Chapter 15: Chest Discomfort¶
Chapter 15 | Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Myocardial ischemia is precipitated by an imbalance between myocardial oxygen requirements and myocardial oxygen supply.
- Acute coronary syndrome (ACS) encompasses unstable angina, non–ST elevation MI (NSTEMI), and ST-elevation MI (STEMI).
- Stable angina is precipitated by exertion, cold, or stress and relieved by rest or nitroglycerin within minutes.
- Unstable angina occurs with progressively lower intensity of physical activity or at rest.
- Levine's sign: patient massaging or clutching their chest with a clenched fist held against the sternum.
- Tearing or ripping pain is often described by patients with acute aortic dissection.
- Radiation to both arms or shoulders has a particularly high association with MI as the etiology.
- Chest wall tenderness does not exclude myocardial ischemia.
- High-sensitivity cardiac troponin assays are preferred for the diagnosis of MI.
- The estimated rate of major cardiovascular events through 30 days in low-risk acute chest pain patients is 2.5%.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification of Myocardial Injury
- 2. EPIDEMIOLOGY
- 2.1 Discharge Diagnosis Distribution
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Mechanisms of Ischemia
- 4. CLINICAL FEATURES
- 4.1 Typical Clinical Features of Major Causes
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Diagnostic Assessment Priorities
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria for AMI Likelihood
- 7. MANAGEMENT & TREATMENT
- 7.1 Physical Examination Findings
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Complications of Ischemic Heart Disease
- 9. SPECIAL CONSIDERATIONS
- 9.1 Risk Factors for Aortic Disease
- 10. KEY PEARLS & CLINICAL TRAPS
- WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- WHAT EXCLUDES THE DIAGNOSIS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
📖 Harrison's defines this as:
Myocardial ischemia causing chest discomfort, termed angina pectoris, is a primary clinical concern in patients presenting with chest symptoms.
- Chest discomfort is among the most common reasons for which patients present for medical attention at either an emergency department (ED) or an outpatient clinic.
- The evaluation of nontraumatic chest discomfort is inherently challenging owing to the broad variety of possible causes.
- Myocardial ischemia is precipitated by an imbalance between myocardial oxygen requirements and myocardial oxygen supply, resulting in insufficient delivery of oxygen to meet the heart's metabolic demands.
- Myocardial oxygen consumption may be elevated by increases in heart rate, ventricular wall stress, and myocardial contractility.
- Myocardial oxygen supply is determined by coronary blood flow and coronary arterial oxygen content.
- When myocardial ischemia is sufficiently severe and prolonged in duration (as little as 20 min), irreversible cellular injury occurs, resulting in MI.
- The term acute coronary syndrome, which encompasses unstable angina, NSTEMI, and STEMI, is in general reserved for ischemia precipitated by acute coronary atherothrombosis.
- Conditions associated with extreme myocardial oxygen demand and impaired endocardial blood flow, such as aortic valve disease, hypertrophic cardiomyopathy, or idiopathic dilated cardiomyopathy, can precipitate myocardial ischemia in patients with or without underlying obstructive atherosclerosis.
- Ischemic causes of chest pain and myocardial injury are additionally distinguished from nonischemic causes of acute myocardial injury, such as myocarditis.
1.1 Classification of Myocardial Injury¶
- Stable angina: Ischemic episodes typically precipitated by a superimposed increase in oxygen demand during physical exertion and relieved upon resting.
- Unstable ischemic heart disease is classified clinically by the presence or absence of detectable acute myocardial injury and the presence or absence of ST-segment elevation on the patient's electrocardiogram (ECG).
- Unstable angina: No detectable acute myocardial injury and either non–ST elevation MI (NSTEMI) or ST-elevation MI (STEMI).
- NSTEMI: Evidence of acute myocardial injury without ST-segment elevation.
- STEMI: Evidence of acute myocardial injury with ST-segment elevation.
- Type 1 MI: MI resulting from acute coronary atherothrombosis.
- Type 2 MI: MI occurring secondary to other imbalances of myocardial oxygen supply and demand.
2. EPIDEMIOLOGY¶
- Chest discomfort is one of the three most common reasons for visits to the ED in the United States.
- Resulting in 6–7 million emergency visits each year.
- More than 60% of patients with this presentation are hospitalized for further testing.
- Most of the remainder undergo additional investigation in the ED.
- Fewer than 15% of evaluated patients are eventually diagnosed with acute coronary syndrome (ACS).
- Rates of ACS are 10–20% in most series of unselected populations.
- Rate as low as 5% in some studies.
- In a large proportion of patients with transient acute chest discomfort, ACS or another acute cardiopulmonary cause is excluded but the cause is not determined.
- Historically, 2–6% of patients with chest discomfort of presumed nonischemic etiology who are discharged from the ED were later deemed to have had a missed myocardial infarction (MI).
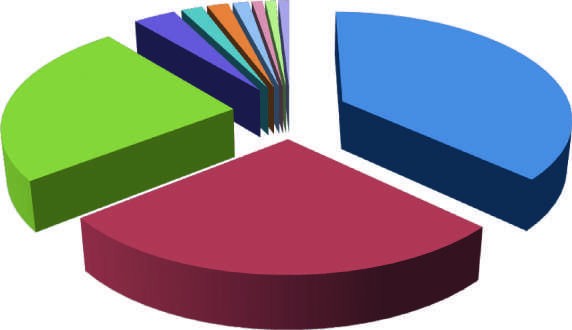
- The most common diagnoses are gastrointestinal causes (Fig. 15-1).
- As few as 5% are other life-threatening cardiopulmonary conditions.
- The estimated rate of major cardiovascular events through 30 days in patients with acute chest pain who had been stratified as low risk was 2.5% in a large population-based study that excluded patients with ST-segment elevation or definite noncardiac chest pain.
2.1 Discharge Diagnosis Distribution¶
- Gastrointestinal causes: 42%
- Ischemic heart disease: 31%
- Chest wall syndrome: 28%
- Pericarditis: 4%
- Pleuritis: 2%
- Pulmonary embolism: 2%
- Lung cancer: 1.5%
- Aortic aneurysm: 1%
- Aortic stenosis: 1%
- Herpes zoster: 1%
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Pathobiology of ischemic heart disease involves the imbalance between myocardial oxygen requirements and supply.
- Irreversible cellular injury occurs when ischemia is sufficiently severe and prolonged (as little as 20 min).
- Acute aortic syndromes encompass a spectrum of acute aortic diseases related to disruption of the media of the aortic wall, including penetrating ulcer and intramural hematoma.
- Pulmonary emboli can produce dyspnea and chest discomfort that is sudden in onset.
- Typically pleuritic in pattern, the chest discomfort associated with pulmonary embolism may result from involvement of the pleural surface of the lung adjacent to a resultant pulmonary infarction, distention of the pulmonary artery, or right ventricular wall stress and/or subendocardial ischemia related to acute pulmonary hypertension.
- Inflammation of the pericardium due to infectious or noninfectious causes can be responsible for acute or chronic chest discomfort.
- The visceral surface and most of the parietal surface of the pericardium are insensitive to pain.
- Pain of pericarditis is thought to arise principally from associated pleural inflammation.
- Acute aortic dissection is a less common cause of chest discomfort but is important because of the catastrophic natural history of certain subsets of cases when recognized late or left untreated.
- Nontraumatic aortic dissections are very rare in the absence of hypertension or conditions associated with deterioration of the elastic or muscular components of the aortic media, including pregnancy, bicuspid aortic disease, or inherited connective tissue diseases, such as Marfan and Ehlers-Danlos syndromes.
3.1 Mechanisms of Ischemia¶
- Increased myocardial oxygen demand: e.g., during intense psychological stress.
- Decreased oxygen delivery: due to anemia, hypoxia, or hypotension.
- Conditions associated with extreme myocardial oxygen demand and impaired endocardial blood flow: aortic valve disease, hypertrophic cardiomyopathy, idiopathic dilated cardiomyopathy.
4. CLINICAL FEATURES¶
- Characteristics of angina pectoris, often referred to simply as angina, are highly similar in quality and location whether the ischemic discomfort is a manifestation of stable ischemic heart disease, unstable angina, or MI.
- Chest discomfort characteristic of myocardial ischemia is typically described as aching, heavy, squeezing, crushing, or constricting.
- In a substantial minority of patients, the quality of discomfort is extremely vague and may be described as a mild to tightness, or merely an uncomfortable feeling, that sometimes is experienced as numbness or a burning sensation.
- The site of the discomfort is usually retrosternal, but radiation is common and generally occurs down the ulnar surface of the left arm.
- The right arm, both arms, neck, jaw, or shoulders may also be involved.
- Stable angina usually begins gradually and reaches its maximal intensity over a period of minutes before dissipating within several minutes with rest or with nitroglycerin.
- The discomfort typically occurs predictably at a characteristic level of exertion or psychological stress.
- By definition, unstable angina is manifest by anginal chest discomfort that occurs with progressively lower intensity of physical activity or even at rest.
- Chest discomfort associated with MI is commonly more severe, is prolonged (usually lasting ≥30 min), and is not relieved by rest.
- Pain that reaches its peak intensity immediately is more suggestive of aortic dissection, pulmonary embolism, or spontaneous pneumothorax.
- Pain that is fleeting (lasting only a few seconds) is rarely ischemic in origin.
- Pain that is constant in intensity for a prolonged period (many hours to days) is unlikely to represent myocardial ischemia if it occurs in the absence of other clinical consequences.
4.1 Typical Clinical Features of Major Causes¶
- Cardiopulmonary Conditions:
- Myocardial ischemia (Stable angina): Pressure, tightness, squeezing, heaviness, burning; Retrosternal; often radiation to neck, jaw, shoulders, or arms; sometimes epigastric; S gallop or mitral regurgitation murmur (rare) during pain; S3 or rales if severe ischemia or complication of myocardial infarction.
- Myocardial ischemia (Unstable angina): Increasing pattern or at rest.
- Myocardial ischemia (Myocardial infarction): Usually >30 min.
- Pericarditis: Variable; hours to days; may be episodic; Pleuritic, sharp; Retrosternal or toward cardiac apex; may radiate to left shoulder; May be relieved by sitting up and leaning forward; pericardial friction rub.
- Acute aortic syndrome: Sudden onset of unrelenting pain; Tearing or ripping; knifelike; Anterior chest, often radiating to back, between shoulder blades; Associated with hypertension and/or underlying connective tissue disorder; murmur of aortic insufficiency; loss of peripheral pulses.
- Pulmonary embolism: Sudden onset; Pleuritic; may manifest as heaviness with massive pulmonary embolism; Often lateral, on the side of the embolism; Dyspnea, tachypnea, tachycardia, hypotension.
- Pulmonary hypertension: Variable; often exertional; Pressure; Substernal; Dyspnea, signs of increased venous pressure.
- Pneumonia or pleuritis: Variable; Pleuritic; Unilateral, often localized; Dyspnea, cough, fever, rales, occasional rub.
- Spontaneous pneumothorax: Sudden onset; Pleuritic; Lateral to side of pneumothorax; Dyspnea, decreased breath sounds on side of pneumothorax.
- Noncardiopulmonary Conditions:
- Esophageal reflux: 10–60 min; Burning; Substernal, epigastric; Worsened by postprandial recumbency; relieved by antacids.
- Esophageal spasm: 2–30 min; Pressure, tightness, burning, intense squeezing; Retrosternal; Can closely mimic angina. May be relieved by nitroglycerin or dihydropyridine calcium channel antagonists.
- Esophageal injury: Prolonged; Intense squeezing; Retrosternal; Includes Mallory-Weiss tear or esophageal rupture (Boerhaave's syndrome) from vomiting.
- Peptic ulcer: Prolonged; 60–90 min after meals; Burning; Epigastric (most common), substernal; Relieved with food or antacids.
- Gallbladder disease, including cholecystitis and biliary colic: Prolonged; steady, usually hours; Aching or colicky; Epigastric, right upper quadrant; sometimes to the back, scapula, and lower chest; May follow meal and may subside spontaneously.
- Pancreatitis: Prolonged; Typically aching; Epigastric, radiates to the back.
- Costochondritis: Variable; Aching; Sternal; Sometimes swollen, tender, warm over joint; may be reproduced by localized pressure on examination.
- Cervical disk disease: Variable; may be sudden; Aching; may include numbness; Arms and shoulders; May be exacerbated by movement of neck.
- Trauma or strain: Usually constant; Aching; Localized to area of strain; Reproduced by movement or palpation.
- Herpes zoster: Usually prolonged; Sharp or burning; Dermatomal distribution; Vesicular rash in area of discomfort.
- Emotional and psychiatric conditions: Variable; may be fleeting or prolonged; Variable; often manifests as tightness and dyspnea with feeling of panic or doom; Variable; may be retrosternal; Situational factors may precipitate symptoms; history of panic attacks, anxiety.
5. DIFFERENTIAL DIAGNOSIS¶
- The evaluation of nontraumatic chest discomfort relies heavily on the clinical history and physical examination to direct subsequent diagnostic testing.
- The evaluating clinician should assess the quality, location (including radiation), and pattern (including onset and duration) of the pain as well as any provoking or alleviating factors.
- The presence of associated symptoms may also be useful in establishing a diagnosis.
- The priorities of the initial clinical encounter include assessment of (1) the patient's clinical stability and (2) the probability that the patient has an underlying cause of the discomfort that may be life-threatening.
- The high-risk conditions of principal concern are acute cardiopulmonary processes, including ACS, acute aortic syndrome, pulmonary embolism, tension pneumothorax, and pericarditis with tamponade.
- Fulminant myocarditis also carries a poor prognosis but is usually also manifested by heart failure symptoms.
- Gastrointestinal disorders are the most common cause of nontraumatic chest discomfort and often produce symptoms that are difficult to discern from more serious causes of chest pain.
- Esophageal disorders, in particular, may simulate angina in the character and location of the pain.
- Musculoskeletal discomfort can be produced by any musculoskeletal disorder involving the chest wall or the nerves of the chest wall, neck, or upper limbs.
- Emotional and psychiatric conditions account for as many as 10% of patients who present to EDs with acute chest discomfort.
5.1 Diagnostic Assessment Priorities¶
-
- Could the chest discomfort be due to an acute, potentially life-threatening condition that warrants urgent evaluation and management? (Unstable ischemic heart disease, Aortic dissection, Pneumothorax, Pulmonary embolism)
-
- If not, could the discomfort be due to a chronic condition likely to lead to serious complications? (Stable angina, Aortic stenosis, Pulmonary hypertension)
-
- If not, could the discomfort be due to an acute condition that warrants specific treatment? (Pericarditis, Pneumonia/pleuritis, Herpes zoster)
-
- If not, could the discomfort be due to another treatable chronic condition? (Esophageal reflux, Esophageal spasm, Peptic ulcer disease, Gallbladder disease, Other gastrointestinal conditions, Cervical disk disease, Arthritis of the shoulder or spine, Costochondritis, Other musculoskeletal disorders, Anxiety state)
6. INVESTIGATIONS & DIAGNOSIS¶
- Electrocardiography is crucial in the evaluation of nontraumatic chest discomfort.
- The ECG is pivotal for identifying patients with ongoing ischemia as the principal reason for their presentation as well as secondary cardiac complications of other disorders.
- Professional society guidelines recommend that an ECG be obtained within 10 min of presentation.
- The primary goal of the ECG is identifying patients with ST-segment elevation diagnostic of MI who are candidates for immediate interventions to restore flow in the occluded coronary artery.
- ST-segment depression and symmetric T-wave inversions at least 0.2 mV in depth are useful for detecting myocardial ischemia in the absence of STEMI and are also indicative of higher risk of death or recurrent ischemia.
- Serial performance of ECGs (every 30–60 min) is recommended early in the ED evaluation of suspected ACS.
- An ECG with right-sided lead placement should be considered in patients with clinically suspected ischemia and a nondiagnostic standard 12-lead ECG.
- Despite the value of the resting ECG, its sensitivity for ischemia is poor—as low as 20% in some studies.
- Abnormalities of the ST segment and T wave may occur in a variety of conditions, including pulmonary embolism, ventricular hypertrophy, acute and chronic pericarditis, myocarditis, electrolyte imbalance, and metabolic disorders.
- Notably, hyperventilation associated with panic disorder can also lead to nonspecific ST and T-wave abnormalities.
- Pulmonary embolism is most often associated with sinus tachycardia but can also lead to rightward shift of the ECG axis, manifesting as an S-wave in lead I, with a Q-wave and T-wave in lead III.
- In patients with ST-segment elevation, the presence of diffuse lead involvement not corresponding to a specific coronary anatomic distribution and PR-segment depression can aid in distinguishing pericarditis from acute MI.
- Laboratory testing in patients with acute chest pain is focused on the detection of myocardial injury.
- Cardiac troponin is the preferred biomarker for the diagnosis of MI and should be measured in all patients with suspected ACS.
- It is not necessary or advisable to measure troponin in patients without suspicion of ACS unless this test is being used specifically for risk stratification (e.g., in pulmonary embolism or heart failure).
- High-sensitivity assays are preferred over prior generation troponin assays.
- The greater negative predictive value of a negative troponin result with high-sensitivity assays is an advantage in the evaluation of chest pain in the ED.
- Rapid rule-out protocols that use serial testing and changes in troponin concentration over as short a period as 1–2 h perform well for diagnosis of ACS when using a high-sensitivity troponin assay.
- Troponin should be measured at presentation and repeated at 1–3 h using high-sensitivity troponin and 3–6 h using conventional troponin assays.
- Additional troponin measurements may be warranted beyond 3–6 h when the clinical condition still suggests possible ACS or if there is diagnostic uncertainty.
- In patients presenting more than 2–3 h after symptom onset, a very low concentration of cardiac troponin, at the time of hospital presentation, using a high-sensitivity assay may be sufficient to exclude MI with a negative predictive value >99%.
- With the use of high-sensitivity assays for troponin, myocardial injury is detected in a larger proportion of patients who have non-ACS cardiopulmonary conditions than with previous, less sensitive assays.
- Observation of a change in cardiac troponin concentration between serial samples is necessary for discriminating acute causes of myocardial injury from chronic elevation due to underlying structural heart disease, end-stage renal disease, or the rare presence of interfering antibodies.
- The diagnosis of MI is reserved for acute myocardial injury that is marked by a rising and/or falling pattern—with at least one value exceeding the 99th percentile reference limit—and that is caused by ischemia.
- Other laboratory assessments may include the D-dimer test to aid in exclusion of pulmonary embolism.
- Measurement of a B-type natriuretic peptide is useful when considered in conjunction with the clinical history and exam for the diagnosis of heart failure.
- Plain radiography of the chest is performed routinely when patients present with acute chest discomfort.
- The chest radiograph is most useful for identifying pulmonary processes, such as pneumonia or pneumothorax.
- Findings are often unremarkable in patients with ACS, but pulmonary edema may be evident.
- Other specific findings include widening of the mediastinum in some patients with aortic dissection, Hampton's hump or Westermark's sign in patients with pulmonary embolism, or pericardial calcification in chronic pericarditis.
6.1 Diagnostic Criteria for AMI Likelihood¶
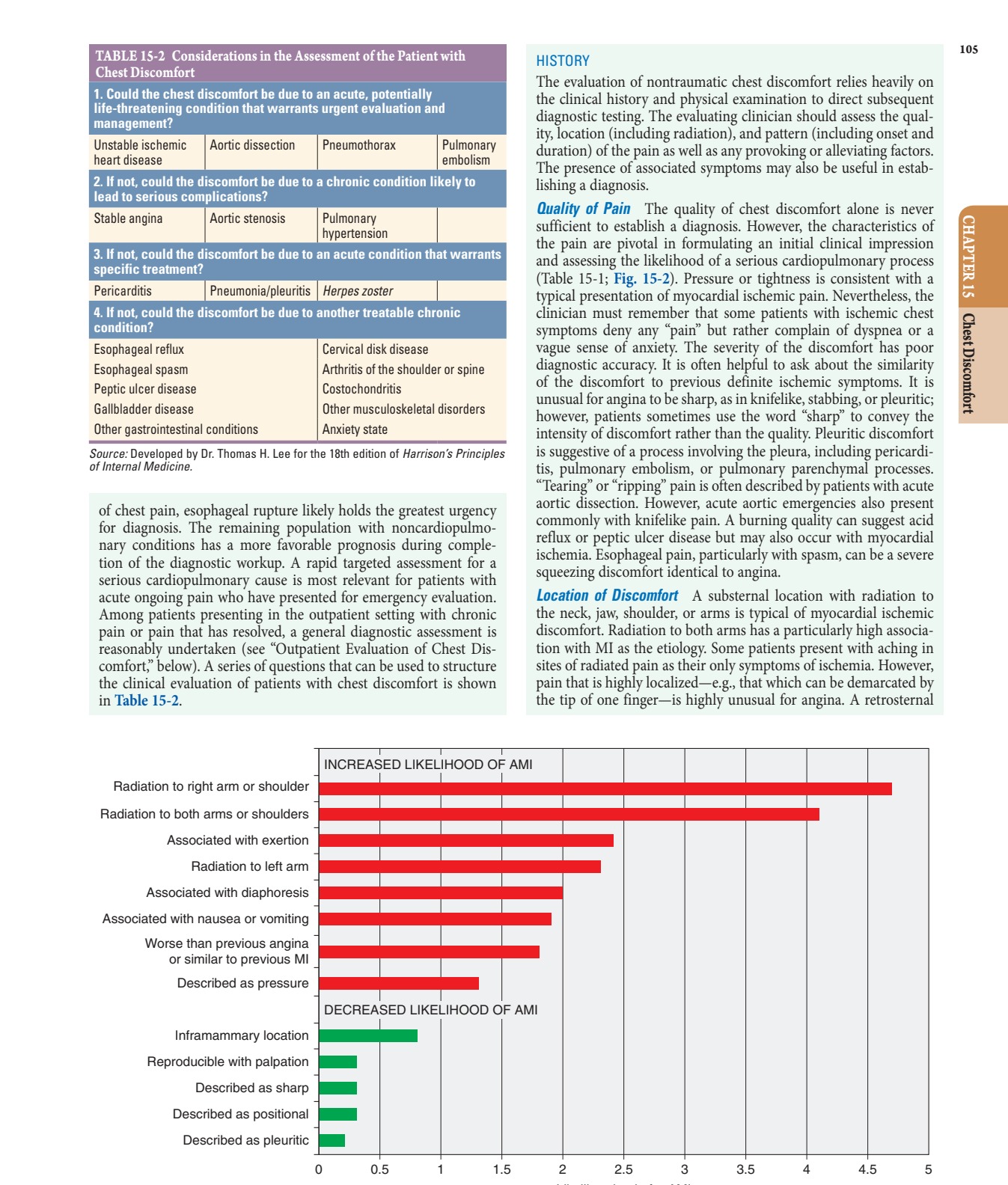
- Increased Likelihood of AMI:
- Radiation to right arm or shoulder
- Radiation to both arms or shoulders
- Associated with exertion
- Radiation to left arm
- Associated with diaphoresis
- Associated with nausea or vomiting
- Worse than previous angina or similar to previous MI
- Described as pressure
- Decreased Likelihood of AMI:
- Inframammary location
- Reproducible with palpation
- Described as sharp
- Described as positional
- Described as pleuritic
7. MANAGEMENT & TREATMENT¶
- Relief of chest discomfort within minutes after administration of nitroglycerin is suggestive of but not sufficiently sensitive or specific for a definitive diagnosis of myocardial ischemia.
- Esophageal spasm may also be relieved promptly with nitroglycerin.
- A delay of >10 min before relief is obtained after nitroglycerin suggests that the symptoms either are not caused by ischemia or are caused by severe ischemia, such as during acute MI.
- Patients with myocardial ischemic pain usually prefer to rest, sit, or stop walking.
- Clinicians should be aware of the phenomenon of warm-up angina in which some patients experience relief of angina as they continue at the same or even a greater level of exertion.
- Alterations in the intensity of pain with changes in position or movement of the upper extremities and neck are less likely with myocardial ischemia and suggest a musculoskeletal etiology.
- The pain of pericarditis, however, often is worse in the supine position and relieved by sitting upright and leaning forward.
- Gastroesophageal reflux may be exacerbated by alcohol, some foods, or a reclined position.
- Relief can occur with sitting.
- Exacerbation by eating suggests a gastrointestinal etiology such as peptic ulcer disease, cholecystitis, or pancreatitis.
- Peptic ulcer disease tends to become symptomatic 60–90 min after meals.
- In the setting of severe coronary atherosclerosis, redistribution of blood flow to the splanchnic vasculature after eating can trigger postprandial angina.
- The discomfort of acid reflux and peptic ulcer disease is usually diminished promptly by acid-reducing therapies.
- Physical exertion is very unlikely to alter symptoms from gastrointestinal causes of chest pain.
- Dynamic cTn (significant rise or fall) indicates Ischemia.
- Stable cTn indicates Chronic myocardial injury.
- Multiple clinical algorithms have been developed to aid in decision-making during the evaluation and disposition of patients with acute nontraumatic chest pain.
- Such decision-aids estimate either diagnostic coronary imaging with coronary computed tomographic angiography or eligibility for further testing because of intermediate or undetermined risk.
7.1 Physical Examination Findings¶
- General:
- Patients with acute MI or other acute cardiopulmonary disorders often appear anxious, uncomfortable, pale, cyanotic, or diaphoretic.
- Patients who are massaging or clutching their chests may describe their pain with a clenched fist held against the sternum (Levine's sign).
- Significant tachycardia and hypotension are indicative of important hemodynamic consequences of the underlying cause of chest discomfort.
- Acute aortic emergencies usually present with severe hypertension but may be associated with profound hypotension when there is coronary arterial compromise or dissection into the pericardium.
- Sinus tachycardia is an important manifestation of submassive pulmonary embolism.
- Tachypnea and hypoxemia point toward a pulmonary cause.
- The presence of low-grade fever is nonspecific because it may occur with MI and with thromboembolism in addition to infection.
- Pulmonary:
- Examination of the lungs may localize a primary pulmonary cause of chest discomfort, as in cases of pneumonia, asthma, or pneumothorax.
- Left ventricular dysfunction from severe ischemia/infarction as well as acute valvular complications of MI or aortic dissection can lead to pulmonary edema, which is an indicator of high risk.
- Cardiac:
- The jugular venous pulse is often normal in patients with acute myocardial ischemia but may reveal characteristic patterns with pericardial tamponade or acute right ventricular dysfunction.
- Cardiac auscultation may reveal a third or, more commonly, a fourth heart sound, reflecting myocardial systolic or diastolic dysfunction.
- Murmurs of mitral regurgitation or a ventricular-septal defect may indicate mechanical complications of STEMI.
- A murmur of aortic insufficiency may be a complication of ascending aortic dissection.
- Pericardial friction rubs reflect pericardial inflammation.
- Presentation with syncope or presyncope should prompt consideration of hemodynamically significant pulmonary embolism or aortic dissection as well as ischemic arrhythmias.
- Abdominal:
- Localizing tenderness on the abdominal exam is useful in identifying a gastrointestinal cause of the presenting syndrome.
- Abdominal findings are infrequent with purely acute cardiopulmonary problems, except in the case of right-sided heart failure leading to hepatic congestion.
- Extremities:
- Vascular pulse deficits may reflect underlying atherosclerosis, which increases the likelihood of coronary artery disease.
- Evidence of acute limb ischemia with loss of the pulse and pallor, particularly in the upper extremities, can indicate catastrophic consequences of aortic dissection.
- Unilateral lower-extremity swelling should raise suspicion about venous thromboembolism.
- Musculoskeletal:
- Pain arising from the costochondral and costosternal articulations may be associated with localized swelling, redness, or marked localized tenderness.
- Pain on palpation of these joints is usually well localized and is a useful clinical sign, although deep palpation may elicit pain in the absence of costochondritis.
- Sensory deficits in the upper extremities may be indicative of cervical disk disease.
8. PROGNOSIS & COMPLICATIONS¶
- The estimated rate of major cardiovascular events through 30 days in patients with acute chest pain who had been stratified as low risk was 2.5% in a large population-based study that excluded patients with ST-segment elevation or definite noncardiac chest pain.
- Chest discomfort associated with MI is commonly more severe, is prolonged (usually lasting ≥30 min), and is not relieved by rest.
- Mechanical complications of STEMI include murmurs of mitral regurgitation or a ventricular-septal defect.
- A murmur of aortic insufficiency may be a complication of ascending aortic dissection.
- Pericardial friction rubs reflect pericardial inflammation.
- Presentation with syncope or presyncope should prompt consideration of hemodynamically significant pulmonary embolism or aortic dissection as well as ischemic arrhythmias.
- Fulminant myocarditis also carries a poor prognosis but is usually also manifested by heart failure symptoms.
8.1 Complications of Ischemic Heart Disease¶
- Mechanical complications of STEMI:
- Murmurs of mitral regurgitation
- Ventricular-septal defect
- Complications of Aortic Dissection:
- Aortic insufficiency
- Catastrophic consequences of aortic dissection (acute limb ischemia with loss of pulse and pallor)
- Complications of Pulmonary Embolism:
- Right ventricular dysfunction
- Pulmonary edema (in severe cases)
- Syncope or presyncope
9. SPECIAL CONSIDERATIONS¶
- Nontraumatic aortic dissections are very rare in the absence of hypertension or conditions associated with deterioration of the elastic or muscular components of the aortic media.
- These conditions include pregnancy, bicuspid aortic disease, or inherited connective tissue diseases, such as Marfan and Ehlers-Danlos syndromes.
- Aortitis, whether of noninfectious or infectious etiology, in the absence of aortic dissection is a rare cause of chest or back discomfort.
- As many as 10% of patients who present to EDs with acute chest discomfort have a panic disorder or related condition.
- In women and the elderly, anginal equivalents may exist in isolation, particularly dyspnea or a vague sense of anxiety.
- Angina may also occur in an epigastric location.
- Pain that occurs solely above the mandible or below the epigastrium is rarely angina.
9.1 Risk Factors for Aortic Disease¶
- Hypertension
- Connective tissue diseases (Marfan syndrome, Ehlers-Danlos syndromes)
- Pregnancy
- Bicuspid aortic disease
- Inherited connective tissue diseases
10. KEY PEARLS & CLINICAL TRAPS¶
- Levine's sign: patient massaging or clutching their chest with a clenched fist held against the sternum.
- Radiation to both arms has a particularly high association with MI as the etiology.
- Some patients present with aching in sites of radiated pain as their only symptoms of ischemia.
- However, pain that is highly localized—e.g., that which can be demarcated by the tip of one finger—is highly unusual for angina.
- A retrosternal location should prompt consideration of esophageal pain.
- However, other gastrointestinal conditions usually present with pain that is most intense in the abdomen or epigastrium, with possible radiation into the chest.
- Pain that occurs solely above the mandible or below the epigastrium is rarely angina.
- Severe pain radiating to the back, particularly between the shoulder blades, should prompt consideration of acute aortic syndrome.
- Radiation to the trapezius ridge is characteristic of pericardial pain and does not usually occur with angina.
- Warm-up angina: some patients experience relief of angina as they continue at the same or even a greater level of exertion.
- Chest wall tenderness does not exclude myocardial ischemia.
- A negative troponin result with high-sensitivity assays may be sufficient to exclude MI with a negative predictive value >99% in patients presenting more than 2–3 h after symptom onset.
WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Tearing or ripping pain is often described by patients with acute aortic dissection.
- Levine's sign: patient massaging or clutching their chest with a clenched fist held against the sternum.
- Radiation to both arms or shoulders has a particularly high association with MI as the etiology.
- Radiation to the trapezius ridge is characteristic of pericardial pain and does not usually occur with angina.
- Pain that reaches its peak intensity immediately is more suggestive of aortic dissection, pulmonary embolism, or spontaneous pneumothorax.
- Pain that is fleeting (lasting only a few seconds) is rarely ischemic in origin.
- Pain that is constant in intensity for a prolonged period (many hours to days) is unlikely to represent myocardial ischemia if it occurs in the absence of other clinical consequences.
- Sudden onset of significant respiratory distress should lead to consideration of pulmonary embolism and spontaneous pneumothorax.
- Hemoptysis may occur with pulmonary embolism or as blood-tinged frothy sputum in severe heart failure but usually points toward a pulmonary parenchymal etiology of chest symptoms.
- Presentation with syncope or presyncope should prompt consideration of hemodynamically significant pulmonary embolism or aortic dissection as well as ischemic arrhythmias.
- Widening of the mediastinum in some patients with aortic dissection.
- Hampton's hump or Westermark's sign in patients with pulmonary embolism.
- Pericardial calcification in chronic pericarditis.
WHAT EXCLUDES THE DIAGNOSIS¶
- Chest wall tenderness does not exclude myocardial ischemia.
- A negative troponin result with high-sensitivity assays may be sufficient to exclude MI with a negative predictive value >99% in patients presenting more than 2–3 h after symptom onset.
- Pain that is highly localized—e.g., that which can be demarcated by the tip of one finger—is highly unusual for angina.
- Pain that is fleeting (lasting only a few seconds) is rarely ischemic in origin.
- Pain that is constant in intensity for a prolonged period (many hours to days) is unlikely to represent myocardial ischemia if it occurs in the absence of other clinical consequences.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶

Caption: FIGURE 15-4 Examples of decision-aids used in conjunction with serial measurement of modified by the authors in the presented study and omitting the assignment of 0, 1, or 2 composite endpoint of myocardial infarction (MI), cardiogenic shock, cardiac arrest, and artery disease; ECG, electrocardiogram; PCI, percutaneous coronary intervention. (Figure
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
Caption: FIGURE 15-2 Association of chest pain characteristics with the probability of acute nonsignificant association with radiation to the right arm. (Figure prepared from data in — Figure 15-1: Distribution of final discharge diagnoses in patients with nontraumatic acute chest pain, showing Gastrointestinal causes (42%), Ischemic heart disease (31%), Chest wall syndrome (28%), and other conditions.
Figure 2¶
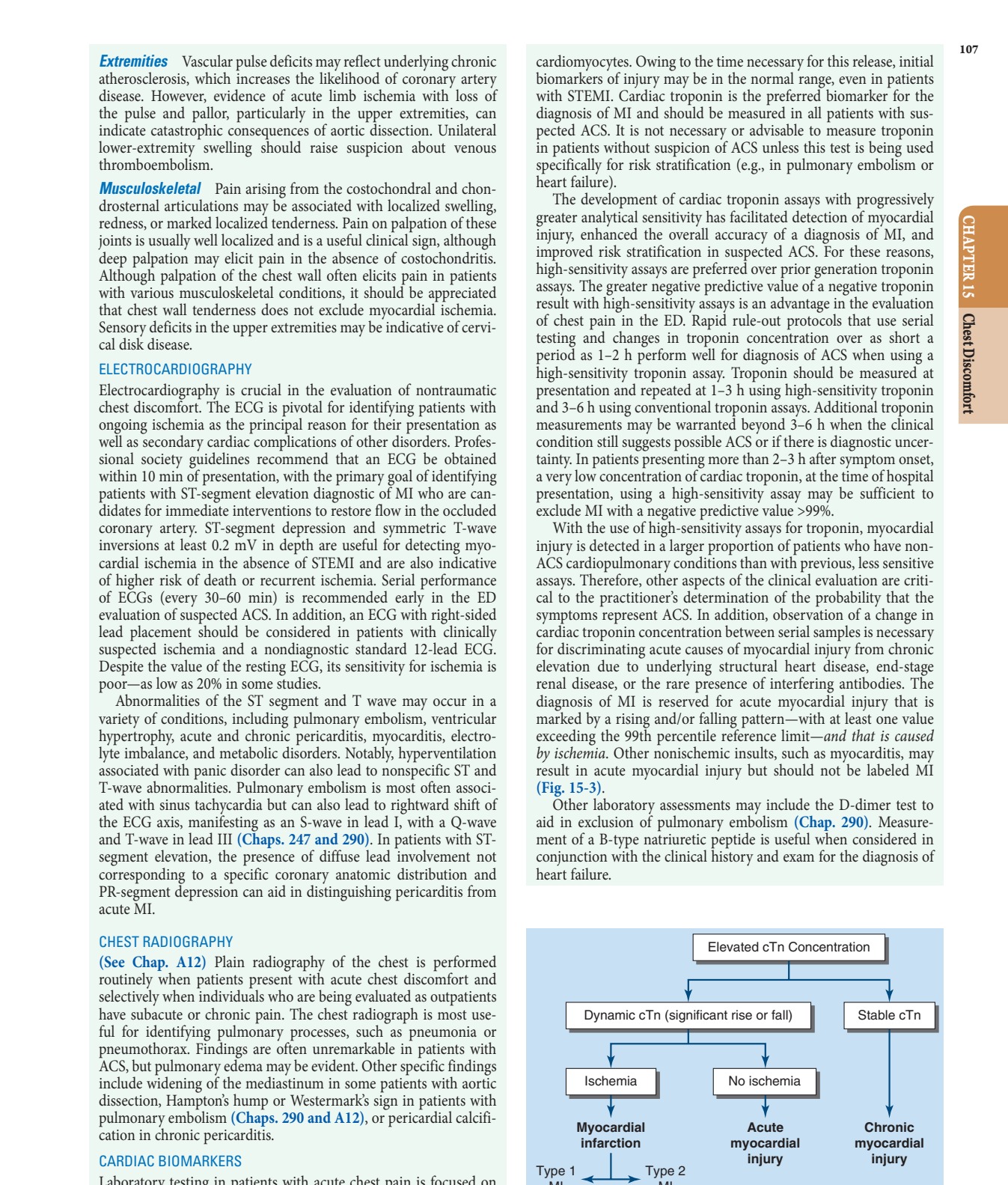
Caption: FIGURE 15-3 Clinical classification of patients with elevated cardiac troponin (cTn). MI, myocardial infarction. — Figure 15-2: Association of chest pain characteristics with the probability of acute myocardial infarction (AMI), illustrating increased likelihood with radiation to right arm, both arms, exertion, diaphoresis, and decreased likelihood with inframammary location, sharp quality, or positional nature.
Figure 3¶
Caption: FIGURE 15-1 Distribution of final discharge diagnoses in patients with nontraumatic acute — Figure 15-3: Clinical classification of patients with elevated cardiac troponin (cTn), distinguishing between Ischemia (Type 1 MI, Type 2 MI), Myocardial Infarction, and Chronic Myocardial Injury based on dynamic cTn changes.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.