Tuberculosis¶
Chapter 183 | Harrison's 22e · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
RAW CONTENT¶
[PAGE 1380] 1380 PART 5 Infectious Diseases major or sole pathogen infecting a joint, the duration of treatment ETIOLOGIC AGENT should be similar to that used for arthritis caused by aerobic bacteria Mycobacteria belong to the family Mycobacteriaceae and the order (Chap. 135). Actinomycetales. Of the pathogenic species belonging to the M. tuber- Although not every anaerobe needs to be covered with pathogen- culosis complex, which comprises eight distinct subgroups, the most directed therapy in most polymicrobial infections, several studies common and important agent of human disease by far is M. tuberculosis of Bacteroides bacteremia have clearly demonstrated that patients (sensu stricto). A closely related organism isolated from cases in West, receiving effective therapy have lower mortality rates and more Central, and East Africa is M. africanum. The complex includes some rapid sterilization of blood cultures than patients receiving ineffec- zoonotic members, such as M. bovis (the bovine tubercle bacillus— tive therapy. characteristically resistant to pyrazinamide, once an important cause FAILURE OF THERAPY of TB transmitted by unpasteurized milk, and currently responsible for 140,000 human cases worldwide in 2020, half of them in Africa) and Anaerobic infections that fail to respond to treatment or that relapse M. caprae (related to M. bovis). In addition, other organisms that have should be reassessed. Potential causes include an uncontrolled been reported rarely as causing TB include M. pinnipedii (a bacillus source of infection (e.g., ongoing intestinal leak into the perito- infecting seals and sea lions in the southern hemisphere and recently neum), superinfection with a new organism, and/or antibiotic fail- isolated from humans), M. mungi (isolated from banded mongooses ure. Additional imaging may be useful to discern whether surgical in southern Africa), M. orygis (described in oryxes and other Bovidae drainage or debridement is warranted. Obtaining additional culture in Africa and Asia and a potential cause of infection in humans), and specimens will help identify whether an organism resistant to the M. microti (the “vole” bacillus, a less virulent organism). Finally, antibiotics being used is present. Strong consideration should be M. canetti is a rare isolate from East African cases that produces given to obtaining susceptibility profiles for the isolates. unusual smooth colonies on solid media and is considered closely related to a supposed progenitor type. There is no known environmen- ■ FURTHER READING tal reservoir for any of these organisms. M. tuberculosis is a rod-shaped, non-spore-forming, thin aero- Cooley L, Teng J: Anaerobic resistance: Should we be worried? Curr bic bacterium measuring 0.5 μm by 3 μm. Mycobacteria, including Opin Infect Dis 32:523, 2019. M. tuberculosis, are often neutral on Gram staining. However, once Debreuil LJ: Fifty years devoted to anaerobes: Historical, lessons, and stained, the bacilli cannot be decolorized by acid alcohol; this charac- highlights. Eur J Clin Microbiol Infect Dis 43:1, 2024. teristic justifies their classification as acid-fast bacilli (AFB; Fig. 183-1). Finegold SM: Anaerobes: Problems and controversies in bacteriology, Acid fastness is due mainly to the organisms’ high content of mycolic infections, and susceptibility testing. Rev Infect Dis 12:S223, 1990. acids, long-chain cross-linked fatty acids, and other cell-wall lipids. Reissier S et al: Recent trends in antimicrobial resistance among Microorganisms other than mycobacteria that display some acid fast- anaerobic clinical isolates. Microorganisms 11:1474, 2023. ness include species of Nocardia and Rhodococcus, Legionella micdadei, Styrt B, Gorbach SL: Recent developments in the understanding of and the protozoa Isospora and Cryptosporidium. In the mycobacterial the pathogenesis and treatment of anaerobic infections (2). N Engl J cell wall, lipids (e.g., mycolic acids) are linked to underlying ara- Med 321:240, 1989. binogalactan and peptidoglycan. This structure results in very low Wexler HM: Bacteroides: The good, the bad, and the nitty-gritty. Clin Microbiol Rev 20:593, 2007. Section 8 Mycobacterial Diseases 183 Tuberculosis Mario C. B. Raviglione, Andrea Gori Tuberculosis (TB), which is caused by bacteria of the Mycobacterium tuberculosis complex, is one of the oldest diseases known to affect humans. In 2023, after being replaced by COVID-19 during the three previous years, TB probably returned to be the top cause of infectious death from a single infectious agent. Population genomic studies suggest that M. tuberculosis may have emerged ~70,000 years ago in Africa and subsequently disseminated along with anatomi- cally modern humans, expanding globally during the Neolithic Age as human density started to increase. This disease most often affects the lungs, although other organs are involved in up to one-third of cases. If properly treated, TB caused by drug-susceptible strains is curable in the vast majority of cases. If untreated, the disease may be fatal in more than 70% of people. Transmission usually takes place through the airborne spread of droplet nuclei produced by patients with infectious pulmonary TB. Through pharmacologic prophylaxis, the development of the disease can be prevented in those who have FIGURE 183-1 Acid-fast bacillus smear showing M. tuberculosis bacilli. (Courtesy contracted TB infection. of the Centers for Disease Control and Prevention, Atlanta.)
[PAGE 1381] Tuberculosis 1381 CHAPTER 183 permeability of the cell wall, thus reducing the effectiveness of most rates (per 100,000 population) in 2022 are depicted in Figs. 183-2 and antibiotics. 183-3, respectively). The complete genome sequence of M. tuberculosis comprises During the past few years, numbers of reported cases have stabilized 4.4 million base pairs, 4043 genes encoding 3993 proteins, and or are slowly declining in most high-income countries. In the United States, 50 genes encoding stable RNAs; its high guanine-plus-cytosine TB cases and incidence rates steadily decreased from 1992 to 2021. In content (65.6%) is indicative of an aerobic “lifestyle.” A large propor- 2022, 8300 cases of TB (2.5 cases per 100,000 population) were reported tion of genes are devoted to the production of enzymes involved in cell to the U.S. Centers for Disease Control and Prevention (CDC), a slight wall metabolism. Substantial genetic variability exists among the innu- increase from the 7882 cases reported in 2021. In the United States, merable M. tuberculosis strains from different parts of the world. Based TB is uncommon among young white adults of European descent, on such genetic variability it is possible to distinguish and compare who have only rarely been exposed to M. tuberculosis infection during different strains. Their distinction is important to study transmission recent decades. In contrast, because of a high risk of transmission in dynamics and identify outbreaks. Starting in the 1990s, reproducible the past, the prevalence of M. tuberculosis infection is relatively high genotyping methods were developed to type the bacterium. Initially, among elderly whites; overall, 13 million persons are estimated to be they included insertion sequence 6110 (IS6110), restriction fragment “latently” infected. In general, adults ≥65 years of age have the highest length polymorphism (RFLP) typing, and spoligotyping. Lately, most incidence rate per capita and children <14 years of age the lowest. Of studies utilize mycobacterial interspersed repetitive unit variable num- the total 7882 cases in 2021, 28% were among U.S.-born persons and ber tandem repeats (MIRU-VNTRs) and whole genome sequencing 71% among non-U.S.-born persons. Non-Hispanic Black or African analysis. American persons accounted for the highest proportion of cases (34%), followed by non-Hispanic White persons (29%), and Hispanic/Latinos EPIDEMIOLOGY (24%). Among non-U.S.-born persons in the United
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
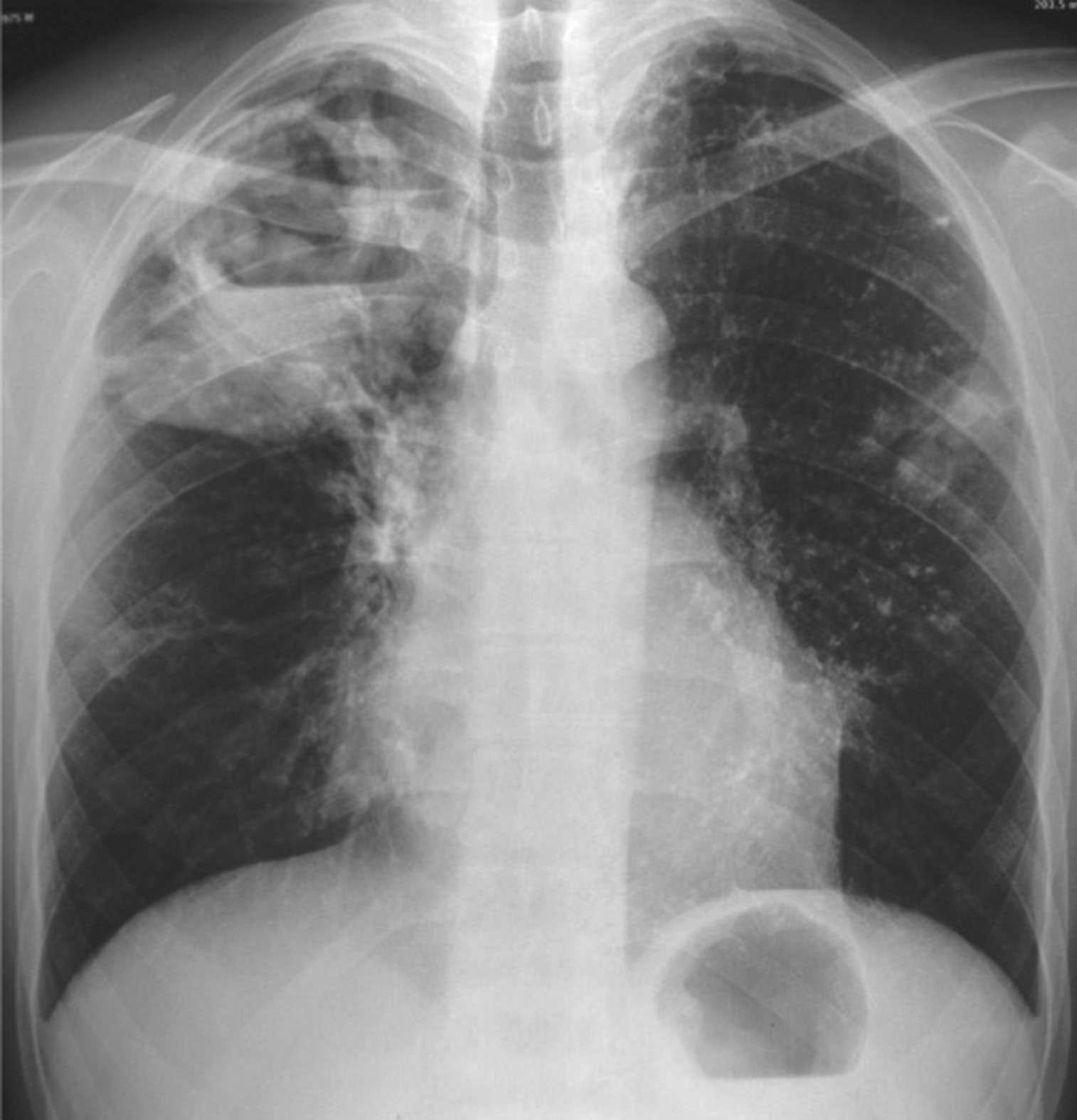
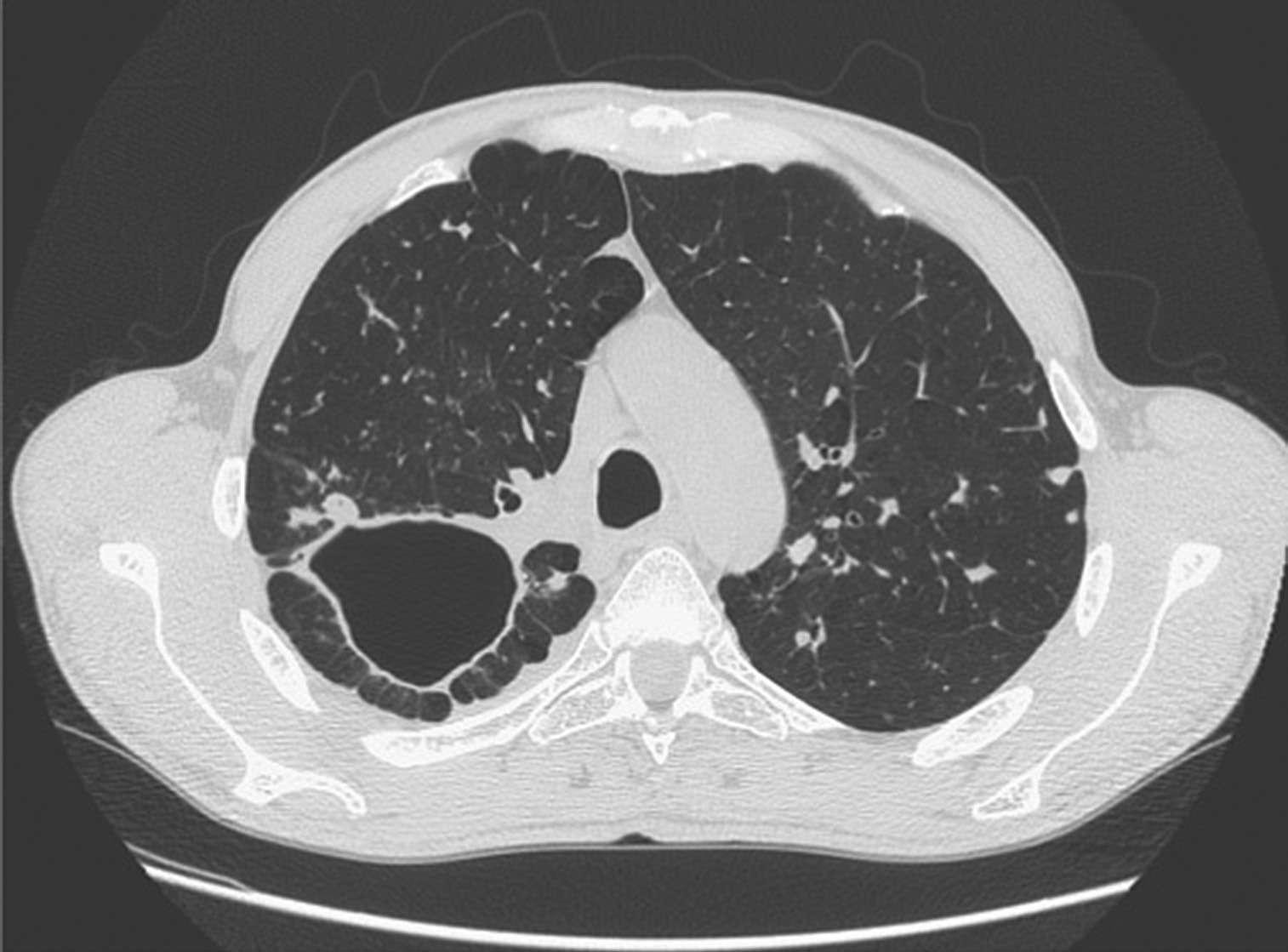
Caption: FIGURE 183-4 Chest radiograph showing right hilar lymph node enlargement with infiltration into the surrounding lung tissue in a child with primary tuberculosis. (Courtesy of Prof. Robert Gie, Department of Paediatrics and Child Health, Stellenbosch University, South Africa; with permission.) FIGURE 183-6 Chest radiograph showing a right-upper-lobe infiltrate and a cavity with an air-fluid level in a patient with active tuberculosis. (Courtesy of Dr. Andrea invariably accompanied by hilar or paratracheal lymphadenopathy due Gori, Infectious Diseases Unit, Fondazione IRCCS Ca’ Granda Ospediale Maggiore to the spread of bacilli from the lung parenchyma through lymphatic Policlinico, University of Milan, Milan, Italy; with permission.) vessels. Enlarged lymph nodes may compress bronchi, causing total obstruction with distal collapse, partial obstruction with large-airway Postprimary (Adult-Type) Disease Also referred to as reacti- wheezing, or a ball-valve effect with segmental/lobar hyperinflation.
Figure 2¶
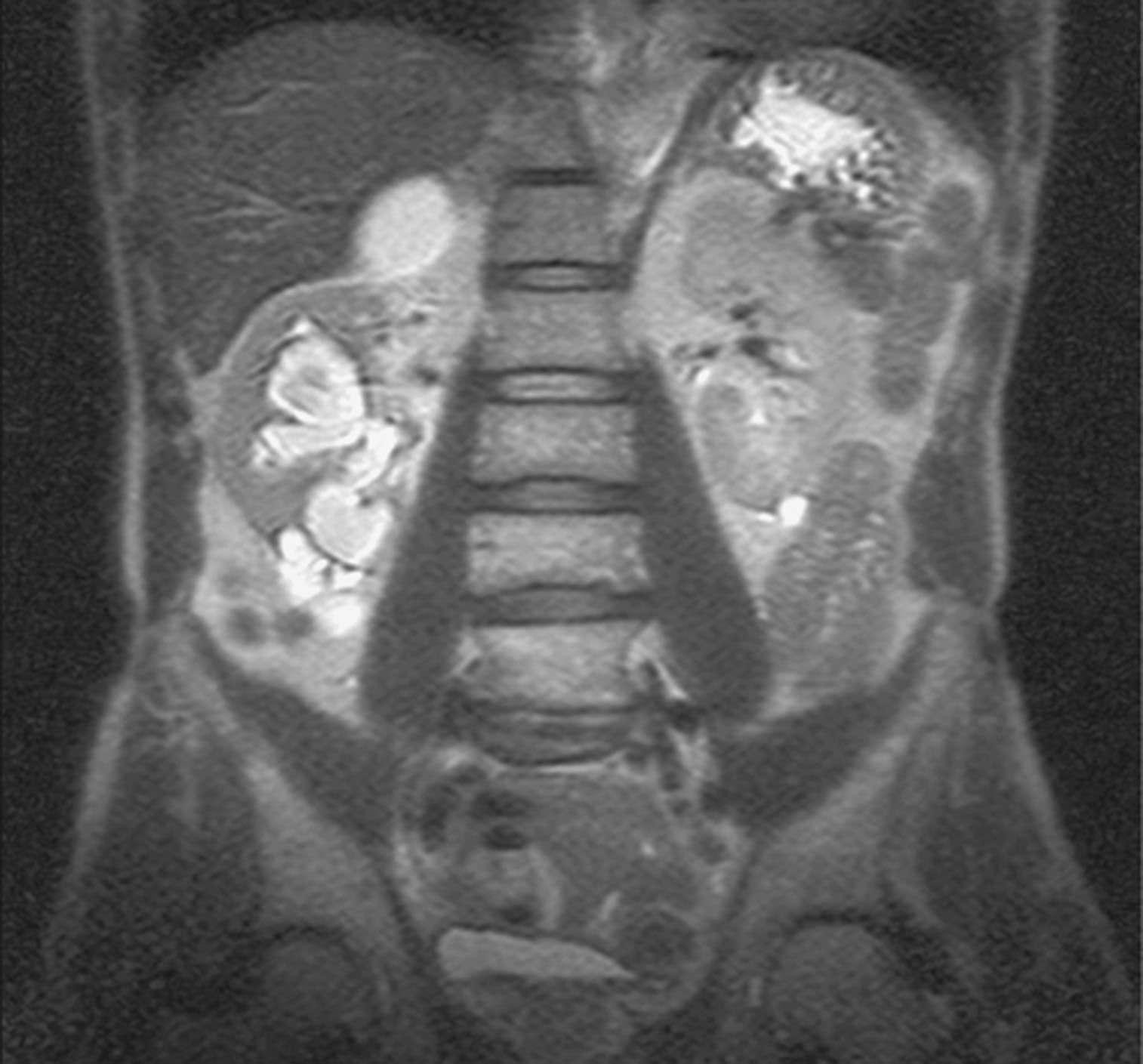
Caption: may involve any portion of the genitourinary tract. Clinical manifesta- FIGURE 183-10 CT scan demonstrating destruction of the right pedicle of T10 due tions are cryptic and protean. Patients may be asymptomatic and their to Pott’s disease. The patient, a 70-year-old Asian woman, presented with back pain disease discovered only after destructive lesions of the kidneys have and weight loss and had biopsy-proven tuberculosis. (Courtesy of Charles L. Daley, developed. Symptoms are often nonspecific and include those of uri- MD, University of California, San Francisco; with permission.) nary tract infection with frequency, dysuria, nocturia and hematuria, and abdominal or flank pain. Without a high index of suspicion, this prostatitis also may develop. In almost half of cases of genitourinary form of TB may result in delayed diagnosis with irreversible organ TB, urinary tract disease is also present. Genitourinary TB responds damage. Up to 75% of patients have abnormalities on CXR suggesting well to chemotherapy. previous or concomitant pulmonary disease. Urinalysis gives abnormal
Figure 3¶

Caption: FIGURE 183-4 Chest radiograph showing right hilar lymph node enlargement with infiltration into the surrounding lung tissue in a child with primary tuberculosis. (Courtesy of Prof. Robert Gie, Department of Paediatrics and Child Health, Stellenbosch University, South Africa; with permission.) FIGURE 183-6 Chest radiograph showing a right-upper-lobe infiltrate and a cavity with an air-fluid level in a patient with active tuberculosis. (Courtesy of Dr. Andrea invariably accompanied by hilar or paratracheal lymphadenopathy due Gori, Infectious Diseases Unit, Fondazione IRCCS Ca’ Granda Ospediale Maggiore to the spread of bacilli from the lung parenchyma through lymphatic Policlinico, University of Milan, Milan, Italy; with permission.) vessels. Enlarged lymph nodes may compress bronchi, causing total obstruction with distal collapse, partial obstruction with large-airway Postprimary (Adult-Type) Disease Also referred to as reacti- wheezing, or a ball-valve effect with segmental/lobar hyperinflation.
Figure 4¶

Caption: FIGURE 183-4 Chest radiograph showing right hilar lymph node enlargement with infiltration into the surrounding lung tissue in a child with primary tuberculosis. (Courtesy of Prof. Robert Gie, Department of Paediatrics and Child Health, Stellenbosch University, South Africa; with permission.) FIGURE 183-6 Chest radiograph showing a right-upper-lobe infiltrate and a cavity with an air-fluid level in a patient with active tuberculosis. (Courtesy of Dr. Andrea invariably accompanied by hilar or paratracheal lymphadenopathy due Gori, Infectious Diseases Unit, Fondazione IRCCS Ca’ Granda Ospediale Maggiore to the spread of bacilli from the lung parenchyma through lymphatic Policlinico, University of Milan, Milan, Italy; with permission.) vessels. Enlarged lymph nodes may compress bronchi, causing total obstruction with distal collapse, partial obstruction with large-airway Postprimary (Adult-Type) Disease Also referred to as reacti- wheezing, or a ball-valve effect with segmental/lobar hyperinflation.
Figure 5¶
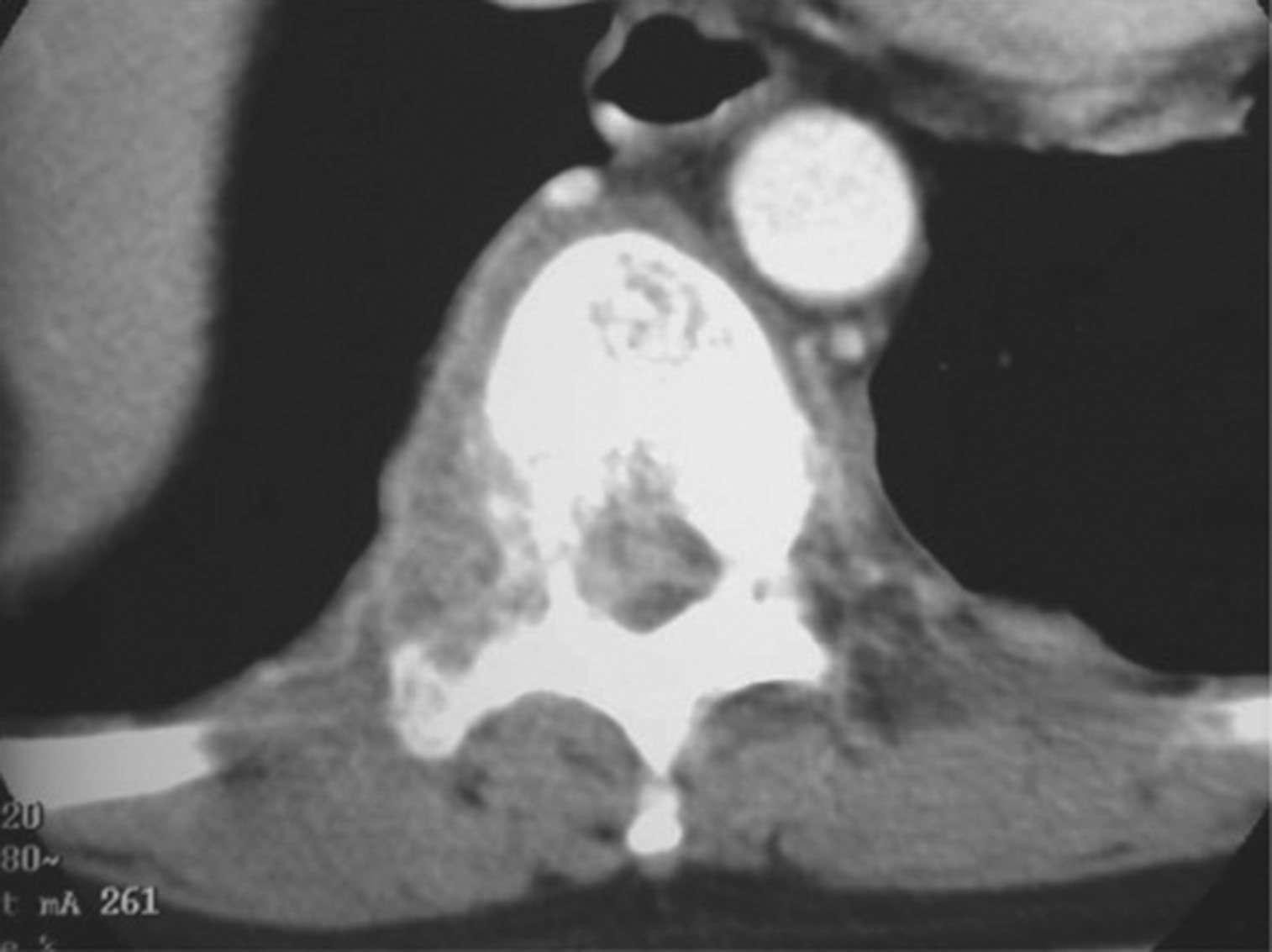
Caption: may involve any portion of the genitourinary tract. Clinical manifesta- FIGURE 183-10 CT scan demonstrating destruction of the right pedicle of T10 due tions are cryptic and protean. Patients may be asymptomatic and their to Pott’s disease. The patient, a 70-year-old Asian woman, presented with back pain disease discovered only after destructive lesions of the kidneys have and weight loss and had biopsy-proven tuberculosis. (Courtesy of Charles L. Daley, developed. Symptoms are often nonspecific and include those of uri- MD, University of California, San Francisco; with permission.) nary tract infection with frequency, dysuria, nocturia and hematuria, and abdominal or flank pain. Without a high index of suspicion, this prostatitis also may develop. In almost half of cases of genitourinary form of TB may result in delayed diagnosis with irreversible organ TB, urinary tract disease is also present. Genitourinary TB responds damage. Up to 75% of patients have abnormalities on CXR suggesting well to chemotherapy. previous or concomitant pulmonary disease. Urinalysis gives abnormal
Figure 6¶
Caption: FIGURE 183-4 Chest radiograph showing right hilar lymph node enlargement with infiltration into the surrounding lung tissue in a child with primary tuberculosis. (Courtesy of Prof. Robert Gie, Department of Paediatrics and Child Health, Stellenbosch University, South Africa; with permission.) FIGURE 183-6 Chest radiograph showing a right-upper-lobe infiltrate and a cavity with an air-fluid level in a patient with active tuberculosis. (Courtesy of Dr. Andrea invariably accompanied by hilar or paratracheal lymphadenopathy due Gori, Infectious Diseases Unit, Fondazione IRCCS Ca’ Granda Ospediale Maggiore to the spread of bacilli from the lung parenchyma through lymphatic Policlinico, University of Milan, Milan, Italy; with permission.) vessels. Enlarged lymph nodes may compress bronchi, causing total obstruction with distal collapse, partial obstruction with large-airway Postprimary (Adult-Type) Disease Also referred to as reacti- wheezing, or a ball-valve effect with segmental/lobar hyperinflation.
Figure 7¶
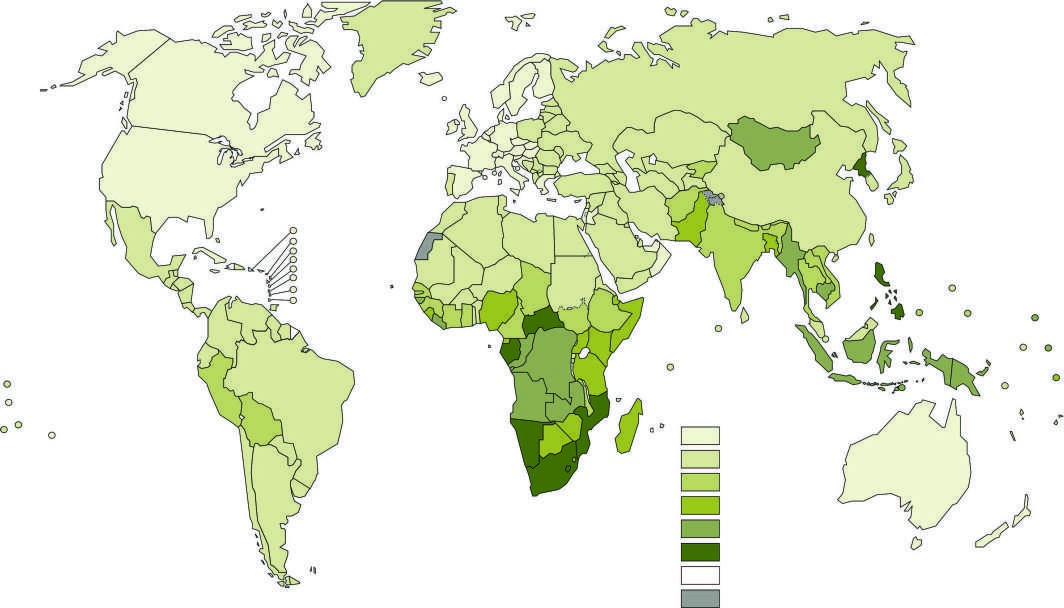
Caption: FIGURE 183-2 Estimated tuberculosis (TB) incidence rates (per 100,000 population) in imply the expression of any opinion whatsoever on the part of the World Health its authorities or concerning the delimitation of its frontiers or boundaries. Dotted, be full agreement. (Reproduced with permission from Global Tuberculosis Report 2023.
Figure 8¶
Caption: FIGURE 183-12 Percentage of new cases of multidrug-resistant/rifampin-resistant Global Drug Resistance Surveillance Project during 1994–2022. Figures are based on the Data reported before the year 2002 are not shown. (See disclaimer in Fig. 183-2. Organization; 2023.)
Figure 9¶

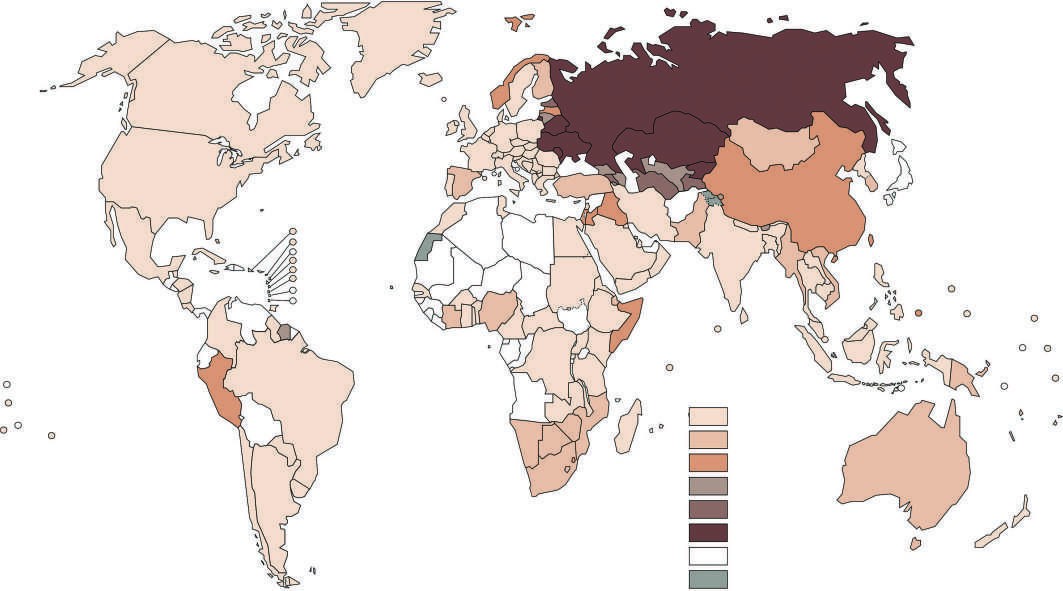
Caption: FIGURE 183-11 Estimated HIV prevalence in new and relapse tuberculosis (TB) cases Tuberculosis Report 2022. Geneva, World Health Organization; 2023.)
Figure 10¶
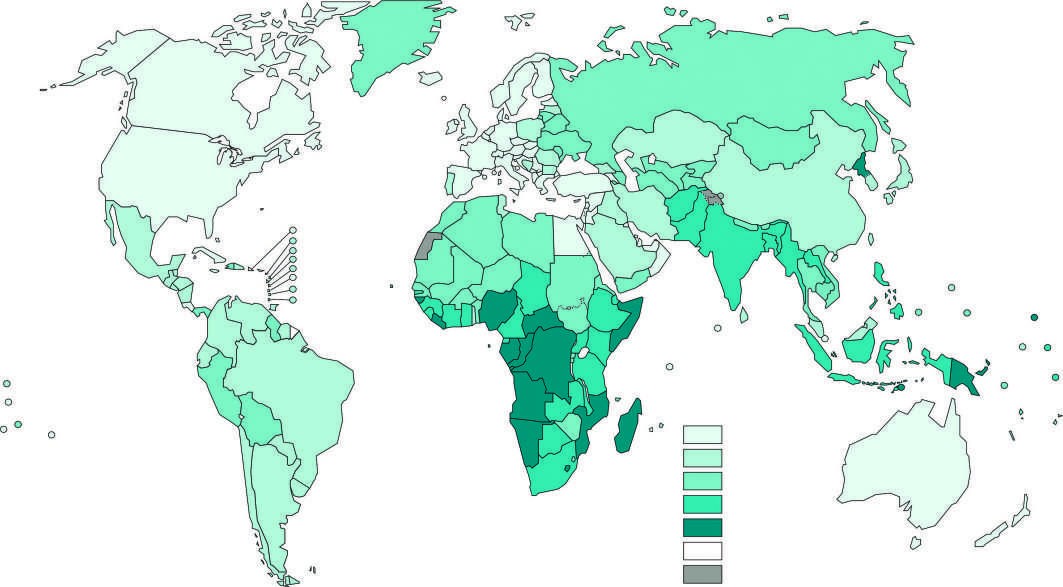
Caption: FIGURE 183-3 Estimated tuberculosis (TB) mortality rates in HIV-negative persons in Tuberculosis Report 2023. Geneva, World Health Organization; 2023.)
Figure 11¶

Caption: FIGURE 183-1 Acid-fast bacillus smear showing M. tuberculosis bacilli. (Courtesy of the Centers for Disease Control and Prevention, Atlanta.)
Figure 12¶

Caption: FIGURE 183-8 Tuberculous lymphadenitis affecting the cervical lymph nodes in a 2-year-old child from Malawi. (Courtesy of Prof. S. Graham, Centre for International Child Health, University of Melbourne, Australia; with permission.)
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.