Blastomycosis¶
Chapter 220 | Harrison's 22e · Part 5 – Infectious Diseases: Fungal
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Blastomyces yeast at 37°C, with broad-based budding between cosis in the United... |
RAW CONTENT¶
[PAGE 1699] Blastomycosis 1699 CHAPTER 220 profoundly hypoxemic and critically ill, many clinicians favor or a positive coccidioidal serology in whom therapy with tumor beginning therapy with an amphotericin B formulation combined necrosis factor-α antagonists or other biological response modifiers with an oral triazole antifungal. The triazole antifungal therapy is is being considered. continued alone once clinical improvement occurs and should be There are recent efforts to develop a vaccine for coccidioido- continued for 6 months to 1 year. mycosis, and a live avirulent product has demonstrated promising The nodules that may occur after primary pulmonary coccidi- results in a canine model. Future studies will determine if this is a oidomycosis do not require treatment. As noted above, these nod- viable strategy for preventing or ameliorating coccidioidal infection ules are not easily distinguished from pulmonary malignancies by in humans. means of radiographic imaging. Close clinical follow-up and biopsy may be required to separate these two entities. Most pulmonary cavities do not require therapy. Antifungal treatment should be con- ■ FURTHER READING sidered in patients with persistent cough, pleuritic chest pain, and Galgiani JN et al: 2016 Infectious Diseases Society of America (IDSA) hemoptysis. Occasionally, pulmonary coccidioidal cavities become clinical practice guideline for the treatment of coccidioidomycosis. secondarily infected (see above). This development is often mani- Clin Infect Dis 63:e112, 2016. fested by an air-fluid level within the cavity. Bacterial oral flora or Gorris ME et al: Expansion of coccidioidomycosis endemic regions Aspergillus species are commonly involved, and therapy directed in the United States in response to climate change. Geohealth 3:308, at these organisms should be considered. Surgical removal of the 2019. cavity may be required in cases of persistent productive cough and Shubitz LF et al: Δcps1 vaccine protects dogs against experimentally hemoptysis or in those cases of a persistently growing cavity. In induced coccidioidomycosis. Vaccine 39:6894, 2021. addition, cavities >4 cm in diameter are unlikely to resolve sponta- Taylor JW, Barker BM: The endozoan, small-mammal reservoir neously, and surgical extirpation should be considered. Surgery is hypothesis and the life cycle of Coccidioides species. Med Mycol always required in cases of pyopneumothorax. For chronic pulmo- 57:S16, 2019. nary coccidioidomycosis, prolonged antifungal therapy—lasting for Troung CN et al: Universal lifelong fungal prophylaxis and risk of at least 1 year—is usually required, with monitoring of symptoms, coccidioidomycosis in lung transplant recipients living in an endemic radiographic changes, sputum cultures, and serologic titers. area. Clin Infect Dis 74:1966, 2021. Most cases of disseminated coccidioidomycosis require pro- longed antifungal therapy. The duration of treatment is based on clinical improvement in conjunction with a significant decline in serum CF antibody titer. Such therapy routinely is continued for at least several years. Relapse occurs in 15–30% of individuals once therapy is discontinued and it is important to continue to monitor such patients on a regular basis (e.g., every 3–4 months) after anti- 220 Blastomycosis fungal therapy is discontinued. Coccidioidal meningitis poses a special challenge. While most patients with this form of disease respond to treatment with oral tri- Gregory M. Gauthier, Bruce S. Klein azoles, 80% experience relapse when therapy is stopped. Therefore, lifelong therapy is recommended. In cases of triazole failure, intra- thecal or intraventricular amphotericin B may be used. Installation ■ DEFINITION requires considerable expertise and should be undertaken only by Blastomycosis is a pyogranulomatous disease that follows the inhalation an experienced health care provider. Shunting of CSF in addition of Blastomyces conidia or hyphal fragments. Typically, Blastomyces causes to appropriate antifungal therapy is required in cases of meningitis pulmonary infection; however, a subset of patients will have dissemi- complicated by hydrocephalus. It is prudent to obtain expert con- nated disease that involves organs such as the skin, bone, brain, or geni- sultation in all cases of coccidioidal meningitis. tourinary system. Blastomycosis is considered a primary fungal infection PREVENTION because it affects persons with either intact or impaired immune systems. A delay in diagnosis is common because blastomycosis mimics other There are no proven methods to reduce the risk of acquiring coccid- diseases such as bacterial pneumonia, tuberculosis, and malignancy. ioidomycosis among residents of an endemic region, but avoidance Diagnosis involves culture- and nonculture-based tests. Amphotericin B of inhalation of uncultivated soil or dust is a reasonable measure. formulations and triazoles are the drugs of choice for treatment. For individuals with suppressed cellular immunity, the risk of developing symptomatic coccidioidomycosis is greater than that in ■ ETIOLOGY the general population. Among those about to undergo allogeneic Blastomyces is a species complex comprising B. dermatitidis, B. gil- solid-organ transplantation, antifungal therapy is appropriate prior christii, B. helicus, B. percursus, B. emzantsi, B. silverae, and B. parvus. to transplantation when there is evidence of active or recent coc- B. silverae and B. parvus are not known to commonly infect humans. cidioidomycosis. Several transplant centers in the endemic region Blastomyces species exhibit thermal dimorphism, which involves the provide universal antifungal prophylaxis for 6 months to 1 year ability to convert between hyphal and yeast morphologies in response after solid-organ and allogeneic stem cell transplantation, and to temperature. In the soil (22–25°C), Blastomyces grows as septate lifelong universal prophylaxis has been advocated after lung trans- hyphae that produce infectious conidia. Among the Blastomyces spe- plantation to prevent the development of coccidioidomycosis after cies, B. helicus is unique because its hyphae grow in a coiled pattern and transplantation. it does not sporulate under in vitro growth conditions. In organs and Cases of donor-transmitted coccidioidomycosis have been tissues (37°C), Blastomyces grows as a pathogenic yeast (Fig. 220-1) reported. Donors who are living or have lived in a coccidioidal that elicits pyogranulomatous inflammation. The yeast form of all Blas- endemic region should be screened serologically for coccidioido- tomyces species grows as broad-based budding yeast cells, with subtle mycosis before transplantation and organ donation deferred if there differences in size among the different species (4–29 μm). is evidence of active infection. Data on the use of antifungal agents for prophylaxis in other ■ EPIDEMIOLOGY situations are limited. The administration of prophylactic anti- Although the majority of Blastomyces infections occur in North America, fungals is not recommended for HIV-1-infected persons who live blastomycosis is a systemic fungal infection of global importance, with in an endemic region. Most experts would administer a triazole infections also occurring in Africa and Asia. In the United States, the antifungal to patients with a history of active coccidioidomycosis traditional geographic range for Blastomyces includes the Mississippi
[PAGE 1700] 1700 PART 5 Infectious Diseases outbreak investigations. The lack of sensitive skin testing and serologic testing, along with difficulty in isolating Blastomyces from the envi- ronment by culture or molecular methods, has limited an in-depth epidemiologic understanding of blastomycosis. In North America, blastomycosis is reportable in five U.S. states (Minnesota, Wisconsin, Michigan, Arkansas, and Louisiana) and two Canadian provinces (Manitoba, Ontario). The annual incidence of blastomycosis in the tra- ditional
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
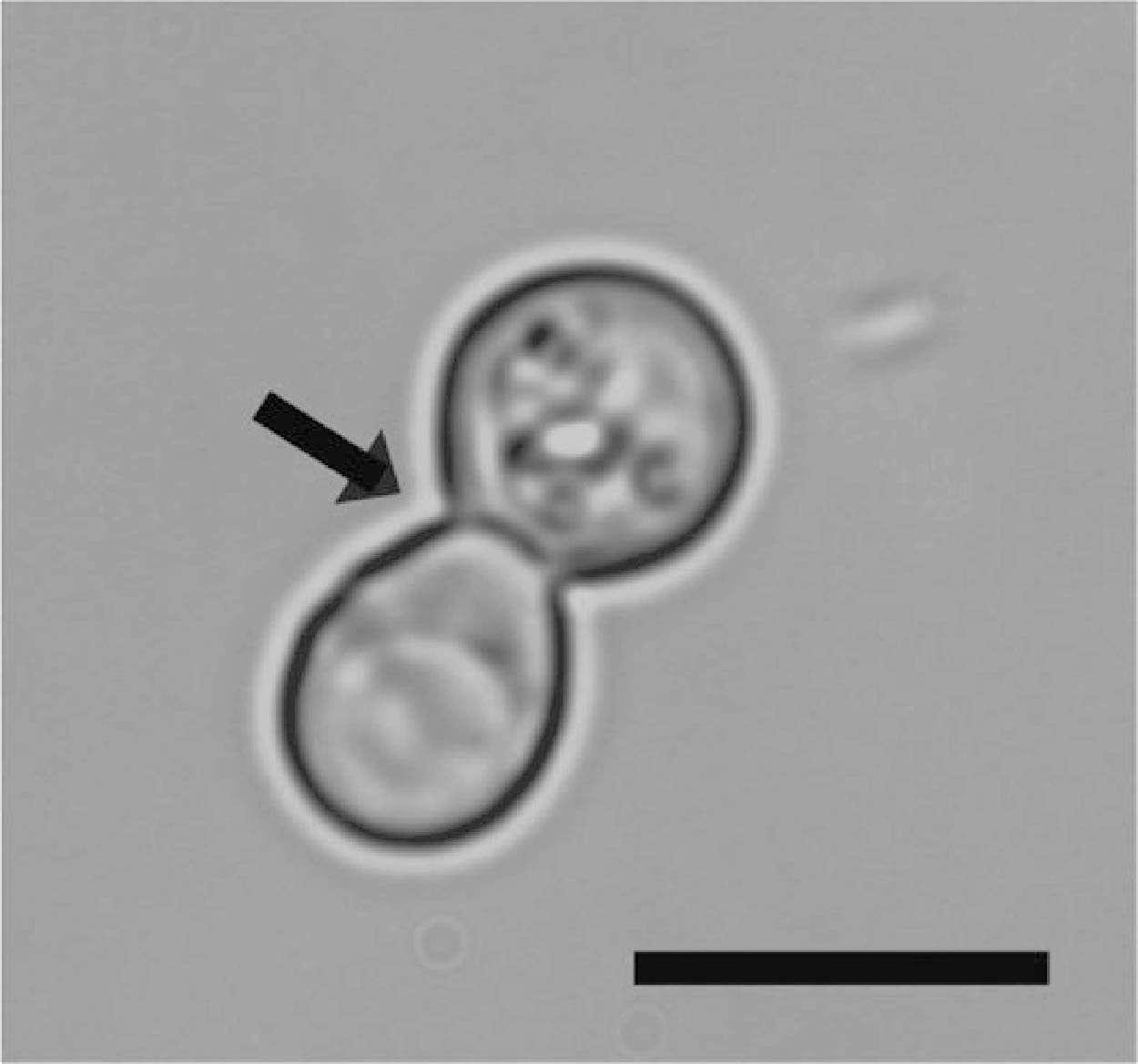
Caption: FIGURE 220-1 Blastomyces yeast at 37°C, with broad-based budding between cosis in the United States since the mid-1950s. Wisconsin, Minnesota, mother and daughter cells (arrow). Bar = 10 μm. (Gregory M. Gauthier, MD, MS.) and North Carolina have had multiple outbreaks. The majority of outbreaks have been in rural areas, but several have occurred in urban and Ohio River basins, the St. Lawrence River basin, states bordering settings. Activities associated with outbreaks include construction (of the Great Lakes, and southeastern states. In Canada, the traditional homes, cabins, factories, and roads), excavation of dirt, participation geographic range includes the provinces of Saskatchewan, Manitoba, in water sports (canoeing, tubing on a river, and fishing), and exposure Ontario, and Quebec. In North America, B. dermatitidis is located to a community compost pile or to beaver dams. Blastomyces infection throughout the traditional geographic range. B. gilchristii is geographi- is typically acquired from disturbed soil, which liberates infectious cally restricted to Minnesota, Wisconsin, Canada, and areas along the particles that are then inhaled into the lungs.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.