Metabolomics¶
Chapter 502 | Part 20: Emerging Topics in Clinical Medicine · Parts 19-20 – Consultative & Emerging Topics
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Metabolomics measures metabolites (small molecules ≤1000 Da) to assess the metabolic state of a cell, tissue, or organism.
- The metabolome is downstream of the genome, epigenome, transcriptome, and proteome, closely reflecting clinical and experimental phenotypes.
- Untargeted metabolomics discovers novel molecules but yields relative quantification; Targeted metabolomics measures predefined subsets with absolute quantification.
- NMR-based approaches are nondestructive and reproducible but have low sensitivity; MS-based approaches are highly sensitive but destructive and require complex sample preparation.
- Magnetic Resonance Spectroscopy (MRS) allows in vivo measurement of metabolites like N-acetylaspartate (NAA) and choline for brain mass diagnosis.
- IDH mutations in gliomas produce 2-hydroxyglutarate (2-HG), a specific biomarker for diagnosis, prognosis, and therapy selection.
- Newborn screening programs use targeted LC–tandem MS to identify inborn errors of metabolism within the first few days of life.
- Sample handling (time, storage, fasting, diet) significantly impacts metabolite levels and must be controlled to avoid false associations.
- Pharmacometabolomics aims to personalize drug dosing by linking baseline metabolomic profiles to pharmacokinetic and pharmacodynamic responses.
- Machine learning and multi-omics integration are expanding the ability to identify metabolic signatures for multifactorial diseases like diabetes and cancer.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 The Metabolome and -omics Hierarchy
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Metabolic Pathways and Confounders
- 4. CLINICAL FEATURES
- 4.1 Biomarkers of Disease
- 4.2 Brain Masses and MRS Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Untargeted vs Targeted Metabolomics
- 6.2 Metabolomics Technologies: NMR vs MS
- 6.3 Chromatography and Mass Spectrometry
- 6.4 Magnetic Resonance Spectroscopy (MRS)
- 6.5 Mass Spectrometry Imaging (MSI)
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacometabolomics
- 7.2 Drug Monitoring and Toxicology
- 7.3 Newborn Screening
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 9.1 Newborns and Children
- 9.2 Sample Handling and Processing
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Metabolism, loosely defined, represents the sum of all biochemical reactions involving small molecules with a molecular mass of ≤1000 Da within a given tissue, cell, or fluid. These small molecules are collectively referred to as metabolites and are involved in the biochemical processes used to create macromolecules and fulfill the energy needs of a cell or organism. Metabolomics, then, represents the measurement of metabolites, either qualitatively or quantitatively, often as a way to gain insight into the metabolism of a cell, tissue, or organism. No one experimental approach can characterize metabolism in its entirety; metabolomics instead strives to measure a portion of the metabolome, which consists of all metabolites in a given biological sample at a given time. Since ChatGPT was introduced in 2022, large language models including GPT-4 have rapidly been applied to diagnostic reasoning, health care documentation, and many other text-based tasks across medical specialties. Modern machine learning offers a powerful set of techniques to learn feature representations directly from data, already performing on par with expert physicians on select tasks.
1.1 The Metabolome and -omics Hierarchy¶
Harrison's defines the metabolome as: all metabolites in a given biological sample at a given time. The metabolome is downstream of the outputs measured by other “-omics” technologies (genome, epigenome, transcriptome, proteome). Thus, the state of the metabolome can more closely reflect clinical and experimental phenotypes. Because metabolic processes are highly connected and interdependent, with individual metabolites often being involved in multiple pathways, levels of a specific metabolite can vary in response to an alteration in either the production or the consumption of that metabolite. Because significant changes in metabolite levels can occur over a very short time frame, the levels measured can be sensitive to perturbations either upstream or downstream of the measured metabolite in a pathway. This sensitivity can make measurement challenging, but it also makes metabolomics a powerful tool with which to assess either acute or chronic changes in cells or tissues. Indeed, the metabolome can be quite dynamic and reflective of the current condition of the material being assessed, as it ultimately represents an integration of outputs from the genome, epigenome, transcriptome, and proteome.
2. EPIDEMIOLOGY¶
While specific incidence and prevalence data for metabolomic biomarkers are not detailed in this chapter, the text notes that metabolomics is used in large prospective cohort studies (e.g., for diabetes, cardiovascular disease, and various cancers). Newborn screening programs are used to identify diseases within the first few days of life such that they can be treated or managed with early intervention. Among the classes of disease targeted by newborn screening programs are many inborn errors of metabolism, which often lead to changes in the levels of specific metabolites in blood or urine.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Metabolomics relies heavily on the intersection of instrumentation, software, and statistical and computational approaches for measurement of metabolite levels and downstream data analysis. The metabolome is dynamic and reflective of the current condition of the material being assessed. Because significant changes in metabolite levels can occur over a very short time frame, the levels measured can be sensitive to perturbations either upstream or downstream of the measured metabolite in a pathway. This sensitivity can make measurement challenging, but it also makes metabolomics a powerful tool with which to assess either acute or chronic changes in cells or tissues.
3.1 Metabolic Pathways and Confounders¶
Metabolites commonly altered with respect to aging are those in antioxidant and redox pathways as well as breakdown products of macromolecules. Sex differences influence a number of different metabolites, most prominently those involved in steroid and lipid metabolism. Diet can also affect the metabolome, and fasting has been shown to impact almost every category of metabolite frequently measured in biological fluids. Differences in sample handling and processing also influence metabolite measurements. Work using metabolomics to analyze material from large prospective cohort studies has shown that changes in metabolite levels introduced by sample handling can lead to falsely positive associations between specific metabolite changes and disease risk. Specific considerations include the large geographic area of distribution from which patients are drawn—e.g., a sample, such as blood, is collected locally and then exposed to variable conditions before being sent to a central lab for further processing. Moreover, because of the costs associated with obtaining and storing samples, often only one sample is available for each individual.
4. CLINICAL FEATURES¶
Tests to assess small molecules are ubiquitous and well established throughout medicine. These include assays to measure select metabolites of known clinical relevance, such as glucose, lactate, and ammonia. Of note, many standard tests assess these metabolites one at a time; however, metabolomics can allow the assessment of many metabolites in a sample and provide more information on metabolic state at a given point in time. In some cases, metabolomics is used to detect molecules for which there is not a robust single analyte test or when multiple species measured in a sample might provide new information.
4.1 Biomarkers of Disease¶
There has been increasing work in prospective human cohort studies on the use of metabolomics, primarily MS-based approaches, to empirically identify small groups of metabolites whose altered levels are associated with the development or progression of disease. Efforts to characterize these “metabolic signatures” have been focused primarily on common, multifactorial diseases such as diabetes, cardiovascular disease, and various cancers that are well represented in large prospective cohort studies. These studies have, for example, identified altered levels of amino acids that are associated with a future diagnosis of diabetes or pancreatic cancer. Similar efforts have proliferated across conditions ranging from chronic lung diseases to neurologic/developmental disorders. Additional efforts have been made to assess the metabolome in patient samples at the time of an acute presentation. Because altered metabolite levels can be associated with a specific clinical diagnosis and/or outcome, the idea is to identify a metabolite signature that facilitates diagnosis or provides prognostic information. This approach has been studied, for example, in the context of sepsis and septic shock, in which blood lactate levels are assessed in combination with the use of clinical tools such as the Acute Physiology and Chronic Health Evaluation (APACHE II) or the Sequential Organ Failure Assessment (SOFA). More recent efforts have identified a strong association between mortality and certain modified amino acids linked to mitochondrial dysfunction, highlighting a potential mechanistic link between sepsis pathogenesis and metabolic alterations.
4.2 Brain Masses and MRS Findings¶
One well-established application is in the diagnosis of brain masses. More specifically, N-acetylaspartate (NAA) is an amino acid derivative that is abundant in neurons, whereas choline is a metabolite whose level, as measured by MRS, correlates with cellularity and/or proliferation. Thus, an increase in the ratio of choline to NAA (and even loss of NAA signal entirely) correlates with cancer; tumors biologically are associated with the properties of increased cellularity from proliferation and the concurrent exclusion of normal neurons. A different process—for example, a brain abscess—does not result in increased choline levels (which instead may actually decrease), but does exclude neurons, resulting in an isolated NAA decrease. Metabolites such as lactate can also be helpful, depending on the clinical context, in providing insight into the metabolism of a tumor or identifying areas of early hypoxic brain injury after a stroke. Finally, among the several amino acids that can be measured, high levels of glutamine/glutamate can be helpful in a patient with altered mental status as changes in these amino acids are associated with hyperammonemia. (Glutamate serves as the central nervous system sink for ammonia, generating glutamine in the process.)
5. DIFFERENTIAL DIAGNOSIS¶
Metabolomics can help differentiate between conditions with similar clinical presentations but distinct metabolic signatures. For example, in the context of brain masses, the ratio of choline to N-acetylaspartate (NAA) helps distinguish cancer (increased ratio, loss of NAA) from abscess (isolated NAA decrease, decreased choline). Inborn errors of metabolism are suggested by abnormal levels of a given metabolite or set of metabolites. Metabolomics can also help identify secondary metabolic defects, such as those that are related to nutritional deficiencies or are acquired in the setting of additional pathology. For example, these measurements are useful in determining the etiology of noncirrhotic hyperammonemia by a catabolic stressor such as sepsis in a patient with a previously unknown subclinical or acquired urea-cycle defect.
6. INVESTIGATIONS & DIAGNOSIS¶
Metabolomics relies heavily on the intersection of instrumentation, software, and statistical and computational approaches for measurement of metabolite levels and downstream data analysis. While the development of new and emerging techniques to assess the metabolome is ongoing, the current, clinically applicable approaches can be separated into two broad categories: nuclear magnetic resonance (NMR)–based approaches and chromatography/mass spectrometry (MS)–based approaches. Each of these two approaches has its own set of advantages and disadvantages.
6.1 Untargeted vs Targeted Metabolomics¶
There are two distinct approaches to measuring metabolites in biological materials: untargeted and targeted metabolomics. These strategies differ in whether a predetermined subset of metabolites is intentionally sought in a sample, with the choice of approach dictated by the question under investigation. Regardless of the method utilized, it is important to recognize that no single metabolomics technique is comprehensive. Technical considerations heavily influence metabolite measurement, even with untargeted metabolomics, and no one method is able to capture the entire metabolome. In this respect, metabolomics contrasts with some other -omics techniques, like genomics or transcriptomics—i.e., in metabolomics, if something is not measured, its absence cannot necessarily be assumed.
6.2 Metabolomics Technologies: NMR vs MS¶
NMR is a technique that, at its core, exploits intrinsic magnetic properties of atomic nuclei to generate data. Nuclei with an odd total number of protons and neutrons (such as 1H, 13C, 15N, and 31P) have a non-zero spin, and this spin generates a magnetic field that can interact with externally applied electromagnetic fields. NMR places compounds into a magnetic field that induces the smaller magnetic fields to align with the larger one. Samples are then exposed to a perpendicular electromagnetic field; the frequency of electromagnetic radiation needed to flip the spin of a nucleus in the exact opposite direction represents the frequency at which an atom “resonates” and can be measured. The resonance frequency of a given atom is affected by adjacent atoms and is ultimately unique for a given arrangement of atoms (i.e., each metabolite). This distribution or “spectrum” of signals is measured and recorded in an NMR experiment. With respect to clinical applications, the primary benefits of NMR-based approaches are that they are nondestructive and can be performed on living samples, such as patients, cells, or tissues. They are also highly reproducible and require minimal sample preparation. Measurements are necessarily quantitative as the signal measured directly reflects concentration. These features ensure that multiple, comparable measurements can be made in a given sample either at a single point in time or across time. In addition, given that spins of different elements require sufficiently disparate resonance-inducing radiofrequencies in order to be entirely distinguishable, multiple elements can be assessed in a sample; this feature allows multidimensional data analysis. Cross-referencing of signals such as hydrogen and carbon. In an untargeted analysis, these multidimensional data can then be used for definitive metabolite identification, with comparison of results to known databases in which spectra for many metabolites in the human metabolome have been systematically recorded. Despite all these benefits, the primary challenge of NMR-based approaches is a lack of sensitivity. Because the time required to detect a signal is proportional to concentration, assessment of less abundant species is impossible or impractical. For example, while a typical NMR-based metabolomics analysis will return data on up to a couple of hundred metabolites at concentrations of >1 μM, the MS-based approaches discussed below can distinguish more than 1000 metabolites at concentrations one to two orders of magnitude lower.
Table 1 — Table 502-1 Comparison of Nuclear Magnetic Resonance (NMR)-Based and Mass Spectrometry (MS)-Based Approaches to Metabolomic Analyses¶
| FEATURE | NMR | MS |
|---|---|---|
| Reproducibility | High | Lower |
| Sensitivity | Low (low μM) | High (low nM) |
| Selectivity | Untargeted | Targeted >> untargeted |
| Sample preparation | Minimal | Complex |
| Metabolites per sample | 50–200 | >1000 |
| Identification | Easy, using one- or two-dimensional databases and additional analyses | Complex; need standards |
| Quantitation | Inherently quantitative; intensity proportional to concentration | Requires standards |
| Sample recovery | Easy, nondestructive | No |
| Living samples | Yes | No |
6.3 Chromatography and Mass Spectrometry¶
A distinguishing feature of chromatography/MS–based approaches is that a multistep process that destroys the material is necessary to generate a sample for analysis. In addition, each step of the sample preparation process involves decisions that influence the metabolites measured at the time of analysis. In general, once a sample to be analyzed is prepared, that material is subjected to a combined chemical and temporal separation of compounds via chromatography, with the output delivered to a device for performance of mass-based detection (technically, measurement of a mass-to-charge [m/z] ratio)—i.e., mass spectrometry. Finally, data collected by the mass spectrometer are analyzed. Sample Preparation Although occasionally a part of NMR-based metabolite detection protocols, MS-based approaches almost uniformly require an initial sample-preparation phase called extraction. This technique destroys the original sample by partitioning metabolites into distinct immiscible phases, such as polar and nonpolar. These phases are then mechanically separated and processed further for analysis. Given the nature of this extraction process, it is critical to determine in advance the general class of metabolites to be measured. This information will help to determine the optimal extraction protocol for specific types of metabolites of interest and to shape further downstream decisions regarding the chromatography/MS technique that also influences metabolite detection. In addition, depending on the metabolites to be analyzed and the method of separation and/or analysis used, extracted samples sometimes are processed further in a preparative step called derivatization: extracted metabolites are chemically modified by the addition or substitution of distinct, known chemical moieties that facilitate separation or detection of types of metabolites. By changing the chemical properties of metabolites, derivatization may improve stability, solubility, or volatility or facilitate separation from closely related compounds, enhancing measurement of specific metabolites.
6.4 Magnetic Resonance Spectroscopy (MRS)¶
Magnetic resonance spectroscopy (MRS) is an adaptation of magnetic resonance imaging (MRI), a widely used technology in clinical practice. MRI, at its core, is essentially proton (1H) NMR with the resulting data rendered spatially to generate an image. Recall that NMR is nondestructive and can be applied to living samples. MRS, then, is a capability built into almost every MRI machine. In practice, radiologists can focus on specific volumes of interest within a patient’s imaging and perform additional sequences to obtain an NMR spectrum in that space that can allow for the identification and quantification of specific metabolites in that space. With this approach, several different metabolites across diverse classes, including lipids, sugars, and amino acids, can be measured at a given time.
6.5 Mass Spectrometry Imaging (MSI)¶
Most clinical metabolomics relies on analysis of bulk material, but in an individual patient, there are areas of normal and diseased tissue, and understanding the differences in metabolism in these areas requires both spatially sensitive resolution (imaging) and interrogation (metabolomics). While MRS can perform some of these functions, it is limited to macroscopic imaging (MRI) and relatively insensitive metabolomics approaches (NMR). In contrast, MS-based approaches, while more sensitive, by their nature rely on specimen destruction and homogenization. The premise of mass spectrometry imaging (MSI) is to overcome these limitations of MRS and mass spectrometry. MSI combines histologic evaluation of tissue with MS-based approaches to assess spatial differences in metabolites. MSI as a technique has been most highly refined in the neurosciences and can provide subcellular resolution. In general, thin slices of tissue are mounted on a slide, and metabolomics is performed at defined points across the slide, yielding spatial information on where in the tissue section metabolites are measured. One specific approach utilizes matrix-assisted laser desorption/ionization (MALDI) coupled to MS. In MALDI, tissues are coated with a special matrix and the MALDI laser scans point-by-point across a tissue slice, ionizing the metabolites at each location for analysis by a mass spectrometer. These data can then be referenced back to an image of the original tissue slice. This approach is being tested for defining tumor margins in real time during resection and thereby providing insight into boundaries between normal and abnormal tissues.
7. MANAGEMENT & TREATMENT¶
The current clinical applications of metabolomics are largely limited to the indications described above. However, ongoing efforts are aimed at expanding the use of metabolomics for detection of biomarkers that can help with disease diagnosis or prognostication. In contrast to the above-described use of metabolomics-based approaches in multifactorial diseases, the application of these approaches in some specific contexts can yield an immediate diagnosis and suggest actionable therapeutic interventions. One specific example in oncology involves an understanding of the pathogenesis of oncogenic mutations in the metabolic enzyme isocitrate dehydrogenase (IDH) isoforms 1 and 2. The normal function of these enzymes is to interconvert isocitrate and α-ketoglutarate; however, cancer-specific point mutations in these enzymes alter the enzymes’ function in a manner conferring neomorphic activity that converts isocitrate into 2-hydroxyglutarate (2-HG). 2-HG is a metabolite that is typically present only at very low levels in cells, but when mutant IDH protein is present, 2-HG is produced and accumulates to high levels. Elevation of 2-HG can promote changes that directly contribute to malignancy; IDH mutations and 2-HG accumulation are found in several human cancers, including specific clinical subsets of acute myeloid leukemia and glioma. Given the unique and specific accumulation of 2-HG in these mutant tumors, detection of this metabolite by LC-MS and NMR-based approaches has been studied both for diagnostic purposes and as a means of assessing drug response. For example, researchers have applied MRS-based approaches to assess the accumulation of 2-HG in gliomas, as this finding can noninvasively identify patients with an IDH-mutant subset of this cancer. This diagnosis provides prognostic information and determines if a patient could benefit from drugs targeting mutant IDH that have been shown to benefit patients with IDH-mutant gliomas. In principle, metabolomics may identify other disease biomarkers to aid with diagnosis or therapy assessments in similar ways.
7.1 Pharmacometabolomics¶
The previous example positions metabolomics as a possible mechanism for achieving a more personalized approach to medicine. The emerging field of pharmacometabolomics aims to take personalization further by making this approach more widely applicable across drugs and disease states. The general idea is to link pharmacokinetics (PK) and pharmacodynamics (PD) data with baseline metabolomic profiling, with the goal of generating a predictive model for individual PK and PD responses based on a naïve patient’s metabolomic profile. Ideally, this approach would allow clinicians to take a baseline set of measurements and then—a priori—choose a specific dose of a specific drug to produce the desired effect in that specific patient. If successful, this method could limit both prolonged titration of medications and medication switching, dramatically shortening and simplifying the current approach to medical therapy.
7.2 Drug Monitoring and Toxicology¶
MS-based metabolomics is used by various athletic organizations for detection of metabolites associated with banned substances and by the pharmaceutical industry for assessment of levels of pharmaceuticals and their metabolites in both blood and tissues. Such analyses can provide key pharmacokinetic information to guide drug dosing and illuminate toxicology. These approaches can also be useful in clinical practice. For example, chronic pain and its management remain a challenge, and the sequelae of opiate/opioid use and abuse are of concern to many providers, their patients, and their patients’ families. Therefore, many electronic medical records systems strive to ensure appropriate and consistent patient access to pain medications, while providers may need a means to ensure that patients are adhering to their prescribed regimens. One way to monitor drug use is to perform targeted LC–tandem MS for detection of specific drug metabolites in patients’ urine. This approach is more sensitive than first-generation immunoassays and can detect a range of metabolites associated with other drugs beyond the one prescribed. Given that the first-generation immunoassays also often rely on confirmatory MS testing, upfront metabolomics reduces lab turnaround time and may also reduce costs by limiting multiple tests on the same sample.
7.3 Newborn Screening¶
Newborn screening programs are used to identify diseases within the first few days of life such that they can be treated or managed with early intervention. Among the classes of disease targeted by newborn screening programs are many inborn errors of metabolism, which often lead to changes in the levels of specific metabolites in blood or urine. One of the first newborn screening programs tested for phenylketonuria, which results from the inability to metabolize phenylalanine resulting in high blood and urine levels of particular metabolites. Since that time, the panel used by programs throughout the United States and around the world has expanded dramatically. The general protocol is to collect a blood sample from infants in the first few days of life (often by heel prick on a piece of paper). These samples are sent to a central lab for analysis, which typically includes metabolomics measurements with targeted LC–tandem MS. Specific inborn errors of metabolism are suggested by abnormal levels of a given metabolite or set of metabolites.
8. PROGNOSIS & COMPLICATIONS¶
In the context of IDH-mutant gliomas, detection of 2-HG provides prognostic information and determines if a patient could benefit from drugs targeting mutant IDH that have been shown to benefit patients with IDH-mutant gliomas. More recent efforts have identified a strong association between mortality and certain modified amino acids linked to mitochondrial dysfunction, highlighting a potential mechanistic link between sepsis pathogenesis and metabolic alterations. One key limitation in all of these studies is that researchers are primarily assessing correlations between blood plasma metabolite levels and complex, multisystem diseases. It remains difficult to obtain a biological understanding of the mechanisms driving these changes or, even more simply, the primary tissue source(s) of these alterations from human data alone, without further experimentation in model systems.
9. SPECIAL CONSIDERATIONS¶
Regardless of the approach used, it is important to consider potential sources of error that can influence the conclusions drawn from a metabolomic analysis. Because of the dynamic nature of the metabolome, numerous biological confounders inherent to the samples themselves can affect levels of the metabolites measured. For this reason, the inclusion of controls or reference populations to account for these confounders can be critical for data interpretation. Established biological confounders for patient-derived material include age, sex, body mass index, time of day collected, fasting status and/or dietary differences, and comorbid conditions such as diabetes or smoking. Differences in sample handling and processing also influence metabolite measurements. Work using metabolomics to analyze material from large prospective cohort studies has shown that changes in metabolite levels introduced by sample handling can lead to falsely positive associations between specific metabolite changes and disease risk. Specific considerations include the large geographic area of distribution from which patients are drawn—e.g., a sample, such as blood, is collected locally and then exposed to variable conditions before being sent to a central lab for further processing. Moreover, because of the costs associated with obtaining and storing samples, often only one sample is available for each individual. Time is a key variable in metabolite measurements, and efforts to assess the impact of sample handling and processing have led to improved analysis pipelines. For example, comparison of metabolites measured in samples undergoing immediate versus delayed processing can provide insight into those metabolites most affected by pre-processing storage under varying conditions. More specifically, because metabolism occurs on a very rapid time scale, some metabolite levels will continue to change after sample collection even if the sample is stored on ice. Therefore, metabolism is ideally halted or “quenched” immediately via rapid freezing or chemical extraction, but practical considerations involved in the collection of material from patients can sometimes make rapid quenching impossible. Therefore, focusing analysis on only those metabolites that are less sensitive to change due to delays in processing time may be important to gain biological insight. Sequential metabolomic analyses of the same type of biological material from a patient can explore how metabolite levels vary over time. It is interesting that, when measured, many metabolites are found to be relatively stable. However, the extensive variability exhibited by some metabolites indicates that findings involving those metabolites should be interpreted with caution.
9.1 Newborns and Children¶
Outside the window of newborn screening, direct clinical measurement of metabolite levels is also used in pediatric and adult patients. In these cases, clinical samples such as serum, cerebrospinal fluid, or even urine are typically subjected to targeted LC–tandem MS to measure metabolites such as amino acids, acylcarnitines, and fatty acids. These measurements can help diagnose milder cases of inborn errors of metabolism that may have been missed by newborn screening. They can also help identify secondary metabolic defects, such as those that are related to nutritional deficiencies or are acquired in the setting of additional pathology. For example, these measurements are useful in determining the etiology of noncirrhotic hyperammonemia by a catabolic stressor such as sepsis in a patient with a previously unknown subclinical or acquired urea-cycle defect.
9.2 Sample Handling and Processing¶
Metabolism is ideally halted or “quenched” immediately via rapid freezing or chemical extraction, but practical considerations involved in the collection of material from patients can sometimes make rapid quenching impossible. Therefore, focusing analysis on only those metabolites that are less sensitive to change due to delays in processing time may be important to gain biological insight. Sequential metabolomic analyses of the same type of biological material from a patient can explore how metabolite levels vary over time. It is interesting that, when measured, many metabolites are found to be relatively stable. However, the extensive variability exhibited by some metabolites indicates that findings involving those metabolites should be interpreted with caution.
10. KEY PEARLS & CLINICAL TRAPS¶
Modern machine learning offers a powerful set of techniques to learn feature representations directly from data, already performing on par with expert physicians on select tasks. If carefully trained and judiciously applied to key areas of clinician workflow, the representational power of new machine learning methods makes them likely to touch every area of clinical practice. While medical computer vision and natural language processing tasks have been the focus of newer deep learning models due to the extensive structure of imaging and text data, many other application classes exist. For example, cardiologist-level performance has been achieved in deep learning approaches for detecting arrhythmias from ambulatory electrocardiograms, standing in contrast to the rule-based algorithms used traditionally to interpret electrocardiographic signals. In genomics, investigators have analyzed tumor genomes with machine learning methods to predict better survival using both deep learning and other machine learning approaches. Machine learning methods have also been used to characterize the deleteriousness of single nucleotide variants in DNA. Many other applications of machine learning to new patient data streams are emerging, for example, machine learning applied to wearables (e.g., smartwatches).
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 502-3 Metabolite measurement by chromatography/mass spectrometry–based what is measured. First, metabolites are extracted from a biological sample in a manner and creates metabolite samples that can be analyzed, sometimes after a chemical downstream analysis. Second, metabolites in the sample are separated via spectrometry. Each signal detected corresponds to a metabolite’s characteristic mass — Figure 502-1 The metabolome is downstream of the outputs measured by other “-omics” technologies. Thus, the state of the metabolome can more closely reflect clinical and experimental phenotypes.
Figure 2¶
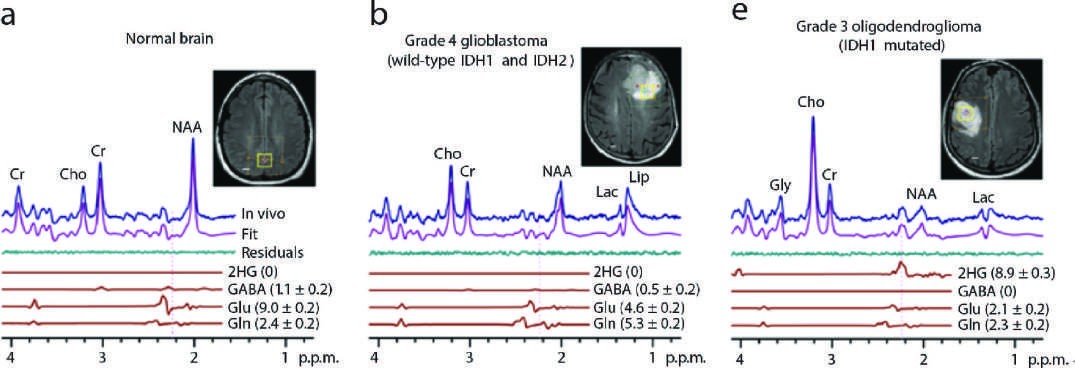
Caption: FIGURE 502-4 In vivo 1H spectra and analysis demonstrating 2-hydroxyglutarate (2-HG) spectra from normal brain (A) and tumors (B–C) are shown. Components of 2-HG, location is indicated by yellow box (voxel). 2-HG is seen only in mutant IDH brain metabolite concentration (mM) ± standard deviation (s.d.). Cho, choline; Cr, creatine; Glu, (Reproduced with permission from C Choi et al: 2012.) — Figure 502-2 Untargeted metabolomics strives to measure as much of the metabolome as possible within a given biological sample, whereas targeted metabolomics focuses on measuring a predetermined subset of the metabolome. In untargeted metabolomics, a large number of signals corresponding to metabolites is generated, and further investigation is often necessary to assign a particular signal to a specific metabolite. Targeted metabolomics allows investigators to definitively measure signals that correspond to specific metabolites of interest.
Figure 3¶
Caption: FIGURE 502-1 The metabolome is downstream of the outputs measured by other and experimental phenotypes. — Figure 502-3 Metabolite measurement by chromatography/mass spectrometry–based approaches involves multiple steps, and decisions made at each step influence what is measured. First, metabolites are extracted from a biological sample in a manner that is destructive of the original sample. This process stops biochemical activity and creates metabolite samples that can be analyzed, sometimes after a chemical derivatization step that alters a subset of metabolites in a manner that facilitates their downstream analysis. Second, metabolites in the sample are separated via chromatography. Finally, the chromatographically separated compounds are analyzed by mass spectrometry. Each signal detected corresponds to a metabolite’s characteristic mass per unit charge while the amplitude of that signal reflects the abundance.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.