Low Back Pain¶
Chapter 18 | Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Pain categorization is critical for treatment decisions: Nociceptive (tissue damage), Neuropathic (nerve injury), and Nociplastic (abnormal processing without tissue damage).
- Nociceptive pain is the most common form of chronic pain in general and LBP in particular, resulting from activity in neural pathways secondary to actual or potentially tissue-damaging stimuli.
- Red flags denote signs or symptoms suggesting serious spinal (e.g., cauda equina syndrome) or nonspinal pathology (e.g., infectious, neoplastic) that may lead to permanent neurologic deficits if not urgently treated.
- Imaging lacks specificity for acute LBP; most studies demonstrate no significant correlation between imaging and symptoms, and a high percentage of abnormalities in populations without back pain.
- The straight leg raising test has a sensitivity of ~80% for L5 and more caudad nerve root involvement, while the crossed straight leg raising test demonstrates consistently high (>85%) specificity.
- Spinal stenosis is characterized by neurogenic claudication, which has a sensitivity of 88% but low specificity; symptoms are exacerbated by activity and improved by rest, especially sitting.
- Herniated disks typically resorb within 2 years but often reherniate; between 38 and 56% of symptomatic individuals report an inciting event.
- Waddell signs (nonanatomic tenderness, sham stimulation pain, distraction, regional disturbances, overreaction) are associated with a greater risk of treatment failure.
- MRI is the gold standard for detecting soft tissue abnormalities including herniation, but CT can provide better spatial contrast and has sensitivity >90% for identifying most lumbar pathology.
- Risk factors for chronic LBP include female sex, African-American race, older age, being unemployed, obesity, and sedentary lifestyle.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Pain Categorization
- 1.2 Epidemiology & Risk Factors
- 2. ETIOLOGY & PATHOPHYSIOLOGY
- 2.1 Myofascial Pain
- 2.2 Discogenic Pain
- 3. CLINICAL FEATURES
- 3.1 Red Flags
- 4. INVESTIGATIONS & DIAGNOSIS
- 4.1 Physical Examination Maneuvers
- 5. MANAGEMENT & TREATMENT
- 5.1 General Principles
- 6. PROGNOSIS & COMPLICATIONS
- 6.1 Red Flag Complications
- 7. SPECIAL CONSIDERATIONS
- 7.1 Imaging Considerations
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Low back pain (LBP) is among the leading causes of years lived with disability worldwide and the principal cause of work-related disability in nearly all industrialized countries. Between 28 and 34% of Americans experienced LBP in the past 3 months, with LBP accounting for >57 million unique patient visits. The all-cause medical costs in the United States are estimated to exceed $300 billion per year.
1.1 Pain Categorization¶
The categorization of pain is important because it predicates treatment decisions at all levels of care. Clinical studies estimate that more than one-third (range <10–55%) of patients with chronic LBP report neuropathic qualities, with 10–20% of the overall back pain population having nociplastic pain. However, different pain categories may occur simultaneously.
Table 1 — Table 18-1: Distinguishing Characteristics of Nociceptive, Neuropathic, and Nociplastic Low Back Pain¶
| CLINICAL CHARACTERISTIC | NOICEPTIVE PAIN | NEUROPATHIC PAIN | NOCIPLASTIC PAIN |
|---|---|---|---|
| Etiology | Cumulative stress; degenerative spondylosis, myofascial pain | Usually preceded by spine degeneration; herniated disk may sometimes occur after inciting event | Usually insidious, but sometimes occurs after physically or psychologically traumatic event |
| Onset | Insidious | Usually insidious | Usually insidious |
| Examples/causes | Degenerative spondylosis, myofascial pain | Herniated disk, spinal stenosis | Nonspecific back pain; may present as mechanical or radicular pain |
| Descriptors | Aching, deep, throbbing | Sharp, shooting, lancinating | Usually similar to neuropathic descriptors, but may include nociceptive ones as well |
| Sensory deficits | Uncommon | Common | Occur sometimes, but often outside of any dermatomal distribution |
| Motor deficits | May be pain-induced | Frequent | Pain-induced weakness, fatigue common |
| Hypersensitivity | Occasionally, with myofascial pain | Common | Extremely common |
| Pain pattern | May be referred into leg (usually proximally) in nondermatomal distribution | Reflects dermatomal pattern | Diffuse, often outside of any anatomic pain patterns |
| Precipitating/relieving factors | Worse with activities that stress structure | More unpredictable; spinal stenosis may be alleviated by forward flexion | Unpredictable, typically worse with stress |
| Autonomic signs | Uncommon | Present in up to 25% of patients | Sympathetic nervous system hyperactivity and postural orthostatic tachycardia syndrome (POTS) very common |
| Accompanying symptoms | Co-existing psychopathology common, and increased rate of neck pain | Higher levels of psychological stress and quality of life decrements than in nociceptive pain | Very high levels of psychological distress and sleep abnormalities; generally co-prevalent with other nociplastic conditions |
| Diagnosis | Imaging correlated with history and physical exam and diagnostic blocks | History and neurologic exam, instruments such as s-LANSS and painDETECT | History (e.g., multiple concomitant nociplastic and nonnociplastic conditions), physical exam (e.g., diffuse tenderness), instruments (central sensitization inventory), and psychophysical tests (conditioned pain modulation) |
1.2 Epidemiology & Risk Factors¶
Risk factors for chronic LBP include female sex, African-American race, older age, being unemployed, obesity, and sedentary lifestyle. Orthopedic populations suggest that over half of individuals may have mixed pain phenotypes.
2. ETIOLOGY & PATHOPHYSIOLOGY¶
Nociceptive LBP typically worsens with activities that stress the structures responsible for pain, is usually secondary to degenerative changes that occur over time, and with the exception of myofascial pain, tends to be progressive in nature. Mechanical pain can radiate to the upper and sometimes lower leg depending on the structure and level(s) involved and the magnitude of the stimulus (greater stimulation results in more distal radiation). However, referral patterns of mechanical pain tend to be more variable and more proximal than for radicular pain, and do not follow a dermatomal distribution.
2.1 Myofascial Pain¶
Muscles, ligaments, and fascia may be sources of mechanical pain, as they are imbued with nociceptors, collectively comprise a large surface area within spinal structures, are heavily involved in loadbearing and movements, and provide structural support to other potential pain generators. Studies examining muscle histology have found higher levels of neuropeptides (substance P, bradykinin), neurotransmitters (norepinephrine, 5-hydroxytryptamine), and inflammatory cytokines (e.g., tumor necrosis factor α, interleukins); lower pH levels; and more numerous vascular abnormalities in active trigger points than in latent trigger points and normal muscle. Studies using electromyography have also found higher myoelectric tone in patients with back pain compared to controls.
2.2 Discogenic Pain¶
Disk degeneration is reported to account for 26–42% of patients with axial LBP, although selection bias (i.e., only those with suspected discogenic pain are included in discography prevalence studies), concomitant pain generators (e.g., disk degeneration predisposes to facet degeneration), the lack of a reference standard for identifying painful disks (high false-positive rate of discography), and flaws in studies utilizing diagnostic tests to identify painful disks (lack of multiple diagnostic tests with adequate controls) limit the precision of prevalence estimates. In healthy disks, nerve fibers are limited to the outer annulus, but in those with disk degeneration, they populate the inner annulus and even the nucleus pulposus. Disk degeneration is associated with upregulation of inflammatory cytokines and other molecules, which may sensitize intradiscal nerve endings and cause hypermobility, which increases the mechanical stress on disks. Macroscopically, the tearing and degeneration of annular fibers increases the stress on intact annular rings to the point of exceeding the mechanical pain threshold and facilitates contact between intradiscal cytokines and sensitized nerve endings.
3. CLINICAL FEATURES¶
History and physical examination may be used to identify patients who require further diagnostic workup and have indications for advanced therapies, including surgery, but are rarely pathognomonic. Inspection may provide clues of congenital or unusual pathology (e.g., birthmarks and doughy lipomas can indicate spina bifida, and an unusual patch of hair over the spine may indicate underlying bony pathology), while observation of gait can suggest nonspinal pathology (e.g., Parkinson's disease or antipsychotic drug use causing propulsive gait; a central lesion causing spastic gait; muscular dystrophy, spinal or gluteal muscle weakness, or hip pathology causing waddling gait; peroneal neuropathy, a large herniated disk, Guillain-Barré syndrome, multiple sclerosis, or another neurologic condition causing steppage gait or foot drop). Paraspinal tenderness overlying an area of "fullness" or increased muscle tension can indicate muscle spasm or a muscle tear, which can sometimes be distinguished through ultrasound, while midline tenderness may indicate ligamentous injury.
3.1 Red Flags¶
The term "red flags" has been used to denote signs or symptoms that suggest the potential presence of serious spinal (e.g., cauda equina syndrome) or nonspinal pathology (e.g., infectious, visceral [pelvic and retroperitoneal organs], traumatic, vascular, neoplastic, inflammatory, or endocrine) that may lead to permanent neurologic deficits if not urgently treated. In one review of 9940 patients with a chief complaint of LBP, 92.6% of patients endorsed at least one red flag, with the most common being night pain (58.1%); although the presence of one or more red flags could predict that a neurologic emergency was present, their absence did not meaningfully decrease the likelihood.
4. INVESTIGATIONS & DIAGNOSIS¶
Advanced imaging is often used to associate symptoms with a potential etiology, but lacks specificity, with most studies demonstrating no significant correlation between imaging and symptoms, and a high percentage of abnormalities in populations without back pain. For acute LBP, red flags and serious or progressive neurologic deficits warrant imaging. For chronic LBP, MRI can be considered on a case-to-case basis, especially when considering invasive interventions such as surgery. For lumbar epidural steroid injections (ESIs), a randomized trial failed to demonstrate that MRI improved outcomes or meaningfully affected decision-making. MRI is considered the gold standard for detecting soft tissue abnormalities including herniation, and can reveal active inflammation on certain sequences. Although MRI is superior for contrast resolution between structures, computed tomography (CT) can provide better spatial contrast, is more sensitive for some bone abnormalities, and has sensitivity >90% for identifying most lumbar pathology including disk herniations. Plain films can be used to evaluate scoliosis and spondylolisthesis and detect fractures (including pars interarticularis), although MRI is needed to determine acuity and chronicity (e.g., presence or absence of edema). As a general principle, when pain symptoms persist or worsen despite optimal nonpharmacologic and pharmacologic treatments or if red flag symptoms arise, dedicated imaging (e.g., x-ray, CT, MRI) can clarify potential diagnoses. Focal lesions on radiologic exams that are physiologically or anatomically plausible sources of pain (e.g., disk herniation with nerve root impingement) might be targets for subsequent interventional pain procedures or surgical management, but because symptom severity does not always correlate with imaging findings, a thorough history and physical examination remain the foundation for accurate contextualization. Treatment decisions should rarely be predicted on imaging findings alone.
4.1 Physical Examination Maneuvers¶
Table 18-2 summarizes common physical exam maneuvers for the low back, including tests for lumbar radiculopathy, sacroiliac joint provocation, SI joint mobility/alignment, deep gluteal syndrome/piriformis syndrome, spondyloarthropathy/ankylosing spondylitis, and nonorganic signs/functional disorders.
Table 2 — Table 18-2: Summary of Common Physical Exam Maneuvers for the Low Back¶
| TEST | DESCRIPTION | COMMENTS |
|---|---|---|
| Straight leg raising (SLR) | The patient is in a supine position. The examiner passively flexes the leg of the affected side at the hip, reproducing radicular pain. | SLR has greatest sensitivity (80%) for impingement of the L5 or S1 nerve roots; sensitivity markedly decreases for nerve roots cephalad to L4. Unreliable for eliciting radicular symptoms from spinal stenosis. |
| Crossed SLR | The patient is in a supine position. The examiner passively flexes the leg of the nonaffected (contralateral) side at the hip, reproducing radicular pain in the affected leg. | High specificity (>85%) but low sensitivity. |
| Femoral stretch | The patient is in a prone position. The examiner passively extends the leg of the affected side at the hip, reproducing radicular pain in the thigh. | Modest sensitivity (50%) for L2–L4 nerve root impingement. |
| Compression (SI Joint Provocation) | The patient is in a lateral decubitus position with the affected side up, with hips and knees flexed; the examiner exerts downward pressure on the superior border of the iliac crest. | There are no physical examination maneuvers that reliably distinguish between intraarticular and extraarticular pathologies, but most tests have been studied based on blocks diagnosing intraarticular pathology. |
| Thigh thrust (posterior shear test [POSH]; femoral shear test) | The patient extends their unaffected leg while in a supine position. On the affected side, the examiner flexes the patient's hip to 90° and simultaneously flexes the ipsilateral knee while applying downward pressure along the longitudinal axis of the femur. | Estimated sensitivities and specificities for individual tests vary greatly. The thigh thrust, FABER, and pelvic torsion tests have relatively greater sensitivities (up to 50–80%), whereas the compression and distraction tests have relatively greater specificities (up to 70–80%). |
| Distraction (gapping test) | The patient is in a supine position. On the affected side, the examiner applies downward (dorsolateral) pressure on the ipsilateral anterior superior iliac spine (ASIS). | A battery of ≥3 tests is generally accepted as having the greatest overall sensitivity (potentially ≥90%) and specificity (potentially ≥80%). |
| Flexion, abduction, and external rotation (FABER; Patrick's test) | The patient is in a supine position. On the affected side, the examiner flexes the patient's hip and knee and positions the foot under the contralateral knee (abduction). While stabilizing the contralateral ASIS with one hand, the examiner uses their other hand to apply downward pressure on the knee of the affected side (external rotation). | N/A |
| Pelvic torsion (Gaenslen's test) | The patient is in a supine position, usually on the edge of an examining table. The examiner hyperextends the leg of the affected side while maximally flexing the hip and knee of the unaffected side against the patient's abdomen. | N/A |
| Standing hip flexion test (SHFT; Gillet's test; Stork test) | The patient stands upright with both feet on level ground. The patient is instructed to lift one leg by flexing their hip and knee toward the chest. The examiner stands behind the patient and observes the spine and pelvis. The test is repeated in the other leg for comparison. | During hip flexion, the ipsilateral ASIS should rise slightly while the posterior superior iliac spine (PSIS) drops slightly. If these motions are paradoxical (i.e., PSIS rises with hip flexion) or asymmetrical, this suggests SI joint mobility dysfunction. |
| Freiberg's sign | The patient is in a supine position. The examiner passively extends, adducts, and internally rotates the thigh and calf ("log roll") on the affected side. | Assesses potential impingement of the sciatic nerve by nonspine structures (e.g., piriformis muscle, gluteal muscles) by stretching the piriformis and associated (e.g., gemelli) muscles, which can produce symptoms similar to those of lumbar radiculopathy. |
| Flexion, adduction, and internal rotation (FADIR; FAIR test) | The patient is in a supine position. On the affected side, the examiner flexes the patient's hip and knee, and while maximally adducting the thigh, internally rotates the hip. | N/A |
| Pace test | In a sitting position, the patient is asked to abduct and externally rotate their hip, eliciting pain. | N/A |
| Beatty test | The patient is positioned in a lateral decubitus position with the affected side up. Elevating the affected leg elicits pain in the buttocks. | Unlike the FAIR test and Freiberg's sign, this test causes contraction of the piriformis muscle and thus may not reliably elicit sciatic nerve entrapment symptoms. |
| Schober test | The patient stands upright, and horizontal lines are drawn across L5 and 10 cm superior to L5. The patient is asked to bend forward and touch their toes. If the distance between the drawn lines increases <5 cm, this indicates decreased range of motion and is a positive result. | Numerous modifications exist regarding the location of the drawn lines. Nonspecific for inflammatory spinal arthritis (i.e., other conditions such as discogenic pain associated with decreased forward flexion can lead to a positive result). |
| Hoover's sign | The patient is in a supine position. The examiner asks the patient to flex the leg of the affected side at the hip, against resistance. If an organic source of neuropathy or paresis is present, with normal effort, the unaffected leg will involuntarily push downward on the examination table. | A discordant response might suggest malingering or the presence of a functional neurologic disorder (e.g., conversion disorder). |
| Tripod sign | With the patient in a seated position, elevating the affected leg may result in pain in the leg and back. | Leaning back and resting both hands on the table should reduce the pain. Failure to do this may suggest nonorganic pathology or malingering. |
| Waddell signs | Five categories of signs: (1) nonanatomic distribution of tenderness; (2) pain from sham stimulation (i.e., lumbar pain from gentle downward force on the shoulders); (3) distraction (i.e., positive SLR test in supine position but not while sitting, or while preoccupied); (4) regional disturbances (i.e., motor or sensory findings that do not correlate with areas of pathology); and (5) overreaction (i.e., disproportionate physical or emotional responses on exam). | A greater number of positive signs is associated with a greater risk of treatment failure. |
5. MANAGEMENT & TREATMENT¶
Treatment decisions should rarely be predicted on imaging findings alone. When pain symptoms persist or worsen despite optimal nonpharmacologic and pharmacologic treatments or if red flag symptoms arise, dedicated imaging (e.g., x-ray, CT, MRI) can clarify potential diagnoses. Focal lesions on radiologic exams that are physiologically or anatomically plausible sources of pain (e.g., disk herniation with nerve root impingement) might be targets for subsequent interventional pain procedures or surgical management. Nonorganic signs (e.g., overreaction, pain with sham stimulation) may signify underlying psychopathology and are associated with treatment failure. Neurologic and/or psychiatric consultations potentially indicated prior to interventional procedures.
5.1 General Principles¶
The distinction between acute (<3 months' duration) and chronic LBP is important as it is the major factor in determining prognosis. For acute LBP, red flags and serious or progressive neurologic deficits warrant imaging. For chronic LBP, MRI can be considered on a case-to-case basis, especially when considering invasive interventions such as surgery. For lumbar epidural steroid injections (ESIs), a randomized trial failed to demonstrate that MRI improved outcomes or meaningfully affected decision-making.
6. PROGNOSIS & COMPLICATIONS¶
In one systematic review involving 11 studies with acute nonradicular pain, 80% (95% confidence interval [CI], 61–100%), 67% (95% CI, 50–83%), 57% (95% CI, 46–68%), and 65% (95% CI, 54–75%) of patients experienced pain at 1, 3, 6, and 12 months, respectively. In systematic reviews evaluating patients with predominantly chronic LBP, stagnant rates of improvement in pain were reported, with few patients improving dramatically after 6 months and a small percentage worsening. In patients with radicular pain, between 15 and 40% of individuals experience persistent symptoms at 6 months to 1 year, with most studies also finding that herniated disks typically resorb within 2 years but often reherniate. For spinal stenosis, most patients also remain stable, with a small percentage progressing, although unlike disk herniations, the underlying pathology does not recede. Risk factors for pain persistence and poor outcomes for both axial and radicular symptoms include greater disease burden, older age, psychopathology, poor job satisfaction, and secondary gain.
6.1 Red Flag Complications¶
Red flags denote signs or symptoms that suggest the potential presence of serious spinal (e.g., cauda equina syndrome) or nonspinal pathology (e.g., infectious, visceral [pelvic and retroperitoneal organs], traumatic, vascular, neoplastic, inflammatory, or endocrine) that may lead to permanent neurologic deficits if not urgently treated. In one review of 9940 patients with a chief complaint of LBP, 92.6% of patients endorsed at least one red flag, with the most common being night pain (58.1%); although the presence of one or more red flags could predict that a neurologic emergency was present, their absence did not meaningfully decrease the likelihood.
7. SPECIAL CONSIDERATIONS¶
When cauda equina syndrome is suspected, assessing sensation in the perianal area and a rectal exam to evaluate sphincter tone is necessary, and urgent confirmation through MRI might be needed. Nonorganic signs (e.g., overreaction, pain with sham stimulation) may signify underlying psychopathology and are associated with treatment failure. Neurologic and/or psychiatric consultations potentially indicated prior to interventional procedures.
7.1 Imaging Considerations¶
Advanced imaging is often used to associate symptoms with a potential etiology, but lacks specificity, with most studies demonstrating no significant correlation between imaging and symptoms, and a high percentage of abnormalities in populations without back pain. For acute LBP, red flags and serious or progressive neurologic deficits warrant imaging. For chronic LBP, MRI can be considered on a case-to-case basis, especially when considering invasive interventions such as surgery. For lumbar epidural steroid injections (ESIs), a randomized trial failed to demonstrate that MRI improved outcomes or meaningfully affected decision-making. MRI is considered the gold standard for detecting soft tissue abnormalities including herniation, and can reveal active inflammation on certain sequences. Although MRI is superior for contrast resolution between structures, computed tomography (CT) can provide better spatial contrast, is more sensitive for some bone abnormalities, and has sensitivity >90% for identifying most lumbar pathology including disk herniations. Plain films can be used to evaluate scoliosis and spondylolisthesis and detect fractures (including pars interarticularis), although MRI is needed to determine acuity and chronicity (e.g., presence or absence of edema). As a general principle, when pain symptoms persist or worsen despite optimal nonpharmacologic and pharmacologic treatments or if red flag symptoms arise, dedicated imaging (e.g., x-ray, CT, MRI) can clarify potential diagnoses. Focal lesions on radiologic exams that are physiologically or anatomically plausible sources of pain (e.g., disk herniation with nerve root impingement) might be targets for subsequent interventional pain procedures or surgical management, but because symptom severity does not always correlate with imaging findings, a thorough history and physical examination remain the foundation for accurate contextualization. Treatment decisions should rarely be predicted on imaging findings alone.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
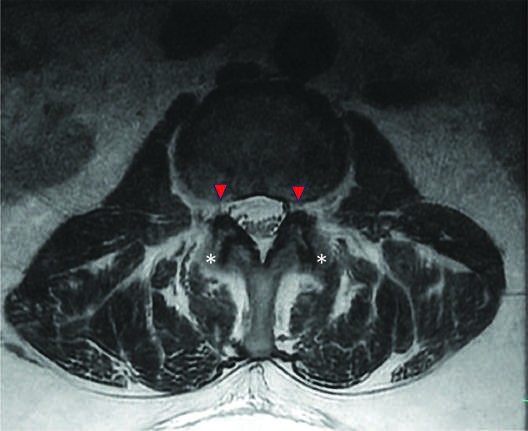
Caption: FIGURE 18-4 In this T2-weighted axial lumbar MRI, bilateral neuroforaminal narrowing secondary to protrusion of the L4–5 disk (arrowheads) and severe bilateral facet joint hypertrophy (asterisks) are visualized. — Figure 18-1: Schematic drawing of a coronal view demonstrating a healthy intervertebral disc (left) and a degenerated disc (right).
Figure 2¶

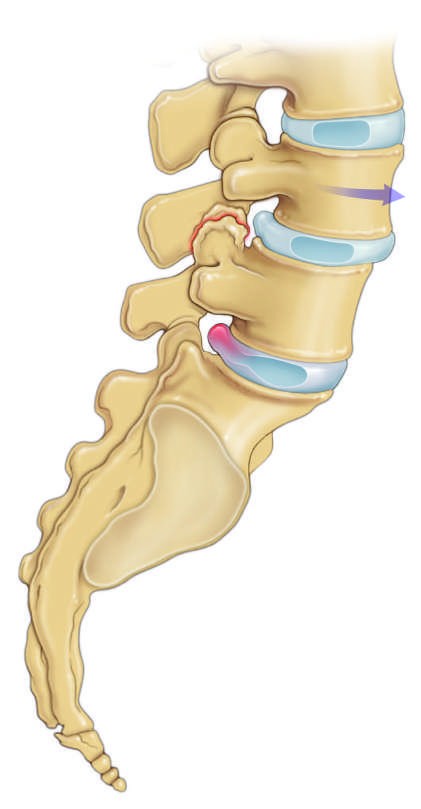
Caption: FIGURE 18-4 In this T2-weighted axial lumbar MRI, bilateral neuroforaminal narrowing secondary to protrusion of the L4–5 disk (arrowheads) and severe bilateral facet joint hypertrophy (asterisks) are visualized. — Figure 18-2: Sagittal view of the lumbar spine depicting L4-5 spinal stenosis secondary to spondylolisthesis, a bulging disc and facet joint hypertrophy, and an L5-S1 herniated nucleus pulposus.
Figure 3¶
Caption: FIGURE 18-4 In this T2-weighted axial lumbar MRI, bilateral neuroforaminal narrowing secondary to protrusion of the L4–5 disk (arrowheads) and severe bilateral facet joint hypertrophy (asterisks) are visualized. — Figure 18-3: T2-weighted sagittal lumbar MRI showing severe central canal stenosis secondary to a disk herniation at L4–5.
Figure 4¶

Caption: FIGURE 18-1 Schematic drawing of a coronal view demonstrating a healthy intervertebral disc (left) and a degenerated disc (right). (Redrawn with permission from Seffrah Jin.) — Figure 18-4: T2-weighted axial lumbar MRI showing bilateral neuroforaminal narrowing secondary to protrusion of the L4–5 disk and severe bilateral facet joint hypertrophy.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.