Edema¶
Chapter 43 | Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Edema represents an excess of interstitial fluid that has become evident clinically.
- Fluid movement from plasma to interstitium is driven by hydrostatic pressure and opposed by colloid oncotic pressure.
- Reduction of effective arterial volume triggers renal sodium and water retention via RAAS, AVP, and SNS.
- Natriuretic peptides (ANP, BNP) oppose sodium retention by augmenting GFR and inhibiting renin/aldosterone.
- Clubbing is associated with cyanotic congenital heart disease, right-to-left shunting, and pulmonary conditions (lung cancer, bronchiectasis, etc.).
- Peripheral cyanosis is abolished by warming/massage; central cyanosis is not.
- Hepatic cirrhosis edema often begins as ascites due to portal hypertension before peripheral edema develops.
- Drug-induced edema is common with calcium channel antagonists, NSAIDs, and thiazolidinediones.
- Lymphedema is particularly intractable due to increased intracapillary pressure and interstitial protein concentration.
- Refeeding edema may occur due to insulin release increasing tubular sodium reabsorption.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Cyanosis and Clubbing
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Neurohumoral Activation
- 4. CLINICAL FEATURES
- 4.1 Distribution of Edema
- 4.2 Localized Edema
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 7. MANAGEMENT & TREATMENT
- 7.1 Drug-Associated Edema
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- WHAT EXCLUDES THE DIAGNOSIS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Clinical conditions in which a decrease in cardiac output (A) and systemic... |
1. DEFINITION & OVERVIEW¶
- Edema is defined as an excess of interstitial fluid that has become evident clinically.
- There is constant interchange of fluid between the intravascular and interstitial compartments of the extracellular fluid.
- The hydrostatic pressure within the capillaries and the colloid oncotic pressure in the interstitial fluid promote the movement of water and diffusible solutes from plasma to the interstitium.
- Fluid is returned from the interstitial space into the vascular system largely through the lymphatic system.
- A net movement of fluid from the intravascular to the interstitial spaces takes place and may be responsible for the development of edema under the following conditions:
- An increase in intracapillary hydrostatic pressure
- Inadequate lymphatic drainage
- Reductions in the oncotic pressure of plasma
- Damage to or dysfunction of the capillary endothelial barrier
- Increases in the oncotic pressure of the interstitial space
1.1 Cyanosis and Clubbing¶
- Cyanosis can be caused by small quantities of circulating methemoglobin (Hb Fe3+) and by even smaller quantities of sulfhemoglobin or magnetic resonance imaging (MRI).
- Both of these hemoglobin derivatives impair oxygen delivery to the tissues.
- Generally, digital clubbing does not occur with these conditions [abnormal hemoglobin species].
- Clubbing is the selective bulbous enlargement of the distal segments of the fingers and toes due to proliferation of connective tissue, particularly on the dorsal surface.
- There is also increased sponginess of the soft tissue at the base of the clubbed nail.
- Clubbing may be hereditary, idiopathic, or acquired and associated with a variety of disorders.
- In certain circumstances, clubbing is reversible, such as following lung transplantation for cystic fibrosis.
- Clubbing in patients with primary and metastatic lung cancer, mesothelioma, bronchiectasis, or hepatic cirrhosis may be associated with hypertrophic osteoarthropathy.
- In hypertrophic osteoarthropathy, the subperiosteal formation of new bone in the distal diaphyses of the long bones of the extremities causes pain and symmetric arthritis-like changes in the shoulders, knees, ankles, wrists, and elbows.
2. EPIDEMIOLOGY¶
- Peripheral cyanosis is probably the most common cause of peripheral cyanosis.
- The most common cause of peripheral cyanosis is the normal vasoconstriction resulting from exposure to cold air or water.
- When cardiac output is reduced, cutaneous vasoconstriction occurs as a compensatory mechanism so that blood is diverted from the skin to more vital areas such as the CNS and heart.
- Cyanosis of the extremities may result even though the arterial blood is normally saturated.
- The text focuses on clinical approach rather than specific incidence or prevalence statistics.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Reduction of Effective Arterial Volume
- In many forms of edema, the effective arterial blood volume, a parameter that represents the filling of the arterial tree and that effectively perfuses the tissues, is reduced.
- Underfilling of the arterial tree may be caused by:
- A reduction of cardiac output and/or systemic vascular resistance
- Pooling of blood in the splanchnic veins (as in cirrhosis)
- Hypoalbuminemia
- As a consequence of this underfilling, a series of physiological responses designed to restore the effective arterial volume to normal are set into motion.
- A key element of these responses is the renal retention of sodium and, therefore, water, thereby restoring effective arterial volume, but sometimes also leading to the development or intensification of edema.
- Renal Factors and the Renin-Angiotensin-Aldosterone System
- The diminished renal blood flow characteristic of states in which the effective arterial blood volume is reduced is translated by the renal efferent arterioles.
- This action reduces the hydrostatic pressure in the peritubular capillaries, increases capillary permeability, and raises the colloid osmotic pressure in these vessels.
- This enhances salt and water reabsorption in the proximal tubule as well as in the ascending limb of the loop of Henle.
- Activation of the Renin-Angiotensin-Aldosterone System (RAAS)
- The renin-angiotensin-aldosterone system (RAAS) operates as both a hormonal and paracrine system.
- Its activation causes sodium and water retention and thereby contributes to edema formation.
- Blockade of the conversion of angiotensin I to AII and blockade of the AII receptors enhance sodium and water excretion and reduce many forms of retention of edema.
- AII that enters the systemic circulation stimulates the production of aldosterone by the zona glomerulosa of the adrenal cortex.
- Aldosterone in turn enhances sodium reabsorption (and potassium excretion) by the collecting tubule, further favoring edema formation.
- Blockade of the action of aldosterone by spironolactone or eplerenone (aldosterone antagonists) or by amiloride (a blocker of epithelial sodium channels) often induces a moderate diuresis in edematous states.
- Arginine Vasopressin (AVP)
- The secretion of arginine vasopressin (AVP) by the posterior pituitary gland occurs in response to increased intracellular osmolar concentration.
- By stimulating V receptors, AVP increases the reabsorption of free water in the distal tubules and collecting ducts of the kidney, thereby increasing total body water.
- Circulating AVP is elevated in many patients with heart failure secondary to a nonosmotic stimulus associated with decreased effective arterial volume and reduced compliance of the left atrium.
- Such patients fail to show the normal reduction of AVP with a reduction of osmolality, contributing to edema formation and hyponatremia.
- Endothelin-1
- This potent peptide vasoconstrictor is released by endothelial cells.
- Its concentration in the plasma is elevated in patients with severe heart failure.
- It contributes to renal vasoconstriction and sodium retention.
- Natriuretic Peptides
- Atrial distention causes release into the circulation of atrial natriuretic peptide (ANP), a 3000-Da polypeptide.
- A high-molecular-weight precursor of ANP is stored in secretory granules within atrial myocytes.
- A closely related natriuretic peptide (pre-prohormone brain natriuretic peptide [BNP]) is stored primarily in ventricular myocytes and is released when ventricular diastolic pressure rises.
- Released ANP and BNP bind to the natriuretic receptor-A, which causes:
- Excretion of sodium and water by augmenting glomerular filtration
- Inhibiting sodium reabsorption in the proximal tubule
- Inhibiting release of renin and aldosterone
- Dilation of arterioles and venules by antagonizing the vasoconstrictor actions of AII, AVP, and sympathetic stimulation.
- Thus, elevated levels of natriuretic peptides have the capacity to oppose sodium retention in hypervolemic and edematous states.
- Although circulating levels of ANP and BNP are elevated in heart failure and in cirrhosis with ascites, these natriuretic peptides are not sufficiently potent to prevent edema formation.
- Indeed, in edematous states, resistance to the actions of natriuretic peptides may be increased, further reducing their effectiveness.
3.1 Neurohumoral Activation¶
- Activation of the sympathetic nervous system and the RAAS (see above) acts in concert to cause renal vasoconstriction and reduction of glomerular filtration and salt and water retention.
- Sodium and water retention continue, and the increment in blood volume accumulates in the venous circulation, raising venous and intracapillary pressure and resulting in edema.
- The presence of overt cardiac disease, as manifested by cardiac enlargement and/or ventricular hypertrophy, together with clinical evidence of cardiac failure, such as dyspnea, basilar rales, venous distention, and hepatomegaly, usually indicates that edema results from heart failure.
- Noninvasive tests such as electrocardiography, echocardiography, and measurements of BNP (or N-terminal proBNP [NT-proBNP]) are helpful in establishing the diagnosis of heart disease.
- The edema of heart failure typically occurs in the dependent portions of the body.
4. CLINICAL FEATURES¶
- Edema is recognized by the persistence of an indentation of the skin after pressure, known as 'pitting' edema.
- In its more subtle form, edema may be detected by noting that after the stethoscope is removed from the chest wall, the rim of the bell leaves an indentation on the skin of the chest for a few minutes.
- Edema may be present when the ring on a finger fits more snugly than in the past or when a patient complains of difficulty putting on shoes, particularly in the evening when dependent edema is greatest.
- Edema may also be recognized by puffiness of the face (most prominent upon awakening), which is most readily apparent in the periorbital areas owing to relative tissue laxity.
- Anasarca refers to gross, generalized edema.
- Ascites (Chap. 53) and hydrothorax refer to accumulation of excess fluid in the peritoneal and pleural cavities, respectively, and are considered special forms of edema.
- Edema of Renal Disease
- The edema that occurs during the acute phase of glomerulonephritis is characteristically associated with hematuria, proteinuria, and hypertension.
- In most instances, the edema results from primary retention of sodium and water by the kidney owing to renal dysfunction.
- This state differs from most forms of heart failure in that it is characterized by a normal (or sometimes even increased) cardiac output.
- Patients with chronic renal failure may also develop edema due to primary renal retention of sodium and water.
- Nephrotic Syndrome and Other Hypoalbuminemic States
- The primary alteration in the nephrotic syndrome is a diminished colloid oncotic pressure due to losses of large quantities (≥3.5 g/d) of protein into the urine and hypoalbuminemia (<3.0 g/dL).
- As a result of the reduced colloid osmotic pressure, the sodium and water that are retained cannot be confined within the vascular compartment, and total and effective arterial blood volumes decline.
- This process initiates the edema-forming sequence of events described above, including activation of the RAAS.
- The nephrotic syndrome may occur during the course of a variety of kidney diseases, including glomerulonephritis, diabetic glomerulosclerosis, and hypersensitivity reactions.
- The edema is diffuse, symmetric, and most prominent in the dependent areas; periorbital edema is most prominent in the morning.
- Hepatic Cirrhosis
- This condition is characterized, in part, by hepatic venous outflow obstruction, which in turn expands the splanchnic blood volume, and hepatic lymph formation.
- Intrahepatic hypertension acts as a stimulus for renal sodium retention and causes a reduction of effective arterial blood volume.
- These alterations are frequently complicated by hypoalbuminemia secondary to reduced hepatic synthesis, as well as peripheral arterial vasodilation.
- These effects reduce the effective arterial blood volume, leading to activation of the sodium- and water-retaining mechanisms described above.
- The concentration of circulating aldosterone often is elevated by the failure of the liver to metabolize this hormone.
- Initially, the excess interstitial fluid is localized preferentially proximal (upstream) to the congested portal venous system, causing ascites.
- In later stages, particularly when there is severe hypoalbuminemia, peripheral edema may develop.
- A sizable accumulation of ascitic fluid may increase intraabdominal pressure and impede venous return from the lower extremities, thereby contributing to the accumulation of the edema.
- Edema of Nutritional Origin
- A diet grossly deficient in calories and particularly in protein over a prolonged period may produce hypoproteinemia and edema.
- The latter may be intensified by the development of beriberi heart disease, which also is of nutritional origin, in which multiple peripheral arteriovenous fistulae result in reduced effective systemic perfusion and effective arterial blood volume, thereby enhancing edema formation.
- Edema develops or becomes intensified when famished subjects are first provided with an adequate diet.
- The ingestion of more food may increase the quantity of sodium ingested, which is then retained along with water.
- So-called refeeding edema also may be linked to increased release of insulin, which directly increases tubular sodium reabsorption.
- In addition to hypoalbuminemia, hypokalemia and caloric deficits may be involved in the edema of starvation.
- Drug-Induced Edema
- A large number of widely used drugs can cause edema.
- Mechanisms include renal vasoconstriction (nonsteroidal anti-inflammatory drugs and cyclosporine), arteriolar dilation (vasodilators), augmented renal sodium reabsorption (steroid hormones), and capillary damage.
- Other Causes of Edema
- These causes include hypothyroidism (myxedema) due to tissue deposition of hyaluronic acid.
- Hyperthyroidism (pretibial myxedema secondary to Graves' disease), in which edema is typically nonpitting.
- Hypercortisolism.
- Pregnancy.
- Administration of estrogens and vasodilators, particularly calcium channel blockers.
4.1 Distribution of Edema¶
- Edema associated with heart failure tends to be more extensive in the legs and to be accentuated in the evening, a feature also determined largely by posture.
- When patients with heart failure are confined to bed, edema may be most prominent in the presacral region.
- Edema resulting from hypoproteinemia, as occurs in the nephrotic syndrome, characteristically is generalized, but it is especially evident in the very soft tissues of the eyelids and face and tends to be most pronounced in the morning owing to the recumbent posture assumed during the night.
- Less common causes of facial edema include trichinosis, allergic reactions, and myxedema.
- Edema limited to one leg or to one or both arms is usually the result of venous and/or lymphatic obstruction.
- Unilateral paralysis reduces lymphatic and venous drainage on the affected side and may also be responsible for unilateral edema.
- In patients with obstruction of the superior vena cava, edema is confined to the face, neck, and upper extremities in which the venous pressure is elevated compared with that in the lower extremities.
4.2 Localized Edema¶
- In thrombophlebitis, varicose veins, and primary venous valve failure, the hydrostatic pressure in the capillary bed upstream (proximal) of the obstruction increases so that an abnormal quantity of fluid is transferred from the vascular to the interstitial space, which may give rise to localized edema.
- The latter may also occur in lymphatic obstruction caused by chronic lymphangitis, resection of regional lymph nodes, filariasis, and genetic (frequently called primary) lymphedema.
- The latter is particularly intractable because restriction of lymphatic flow results in both an increase in intracapillary pressure and increased protein concentration in the interstitial fluid, which act in concert to aggravate fluid retention.
5. DIFFERENTIAL DIAGNOSIS¶
- The differences among the major causes of generalized edema are shown in Table 43-1.
- Cardiac, renal, hepatic, or nutritional disorders are responsible for a large majority of patients with generalized edema.
- Consequently, the differential diagnosis of generalized edema should be directed toward identifying or excluding these several conditions.
- An important first question is whether the edema is localized or generalized.
- If it is localized, the local phenomena that may be responsible should be identified.
- If the edema is generalized, one should determine if there is serious hypoalbuminemia, e.g., serum albumin <3.0 g/dL.
- If so, the history, physical examination, urinalysis, and other laboratory data will help evaluate the question of cirrhosis, severe malnutrition, or the nephrotic syndrome as the underlying disorder.
- If hypoalbuminemia is not present, one should determine if there is evidence of heart failure severe enough to promote generalized edema.
- Finally, it should be ascertained as to whether or not the patient has an adequate urine output or if there is significant oliguria or anuria.
Table 1 — Table 43-1 Principal Causes of Generalized Edema: History, Physical Examination, and Laboratory Findings¶
| ORGAN SYSTEM | HISTORY | PHYSICAL EXAMINATION | LABORATORY FINDINGS |
|---|---|---|---|
| Cardiac | Dyspnea with exertion prominent—often associated with orthopnea—or paroxysmal nocturnal dyspnea | Elevated jugular venous pressure, ventricular (S) gallop; occasionally with displaced or dyskinetic apical impulse; peripheral cyanosis, cool extremities, low pulse pressure when severe | Elevated urea nitrogen-to-creatinine ratio common; serum sodium often decreased; elevated natriuretic peptides |
| Hepatic | Dyspnea uncommon, except if associated with significant degree of ascites; most often a history of ethanol abuse | Frequently associated with ascites; jugular venous pressure normal or low; blood pressure lower than in renal or cardiac disease; one or more additional signs of chronic liver disease (jaundice, palmar erythema, Dupuytren's contracture, spider angiomata, male gynecomastia; asterixis and other signs of encephalopathy) may be present | If severe, reductions in serum albumin, cholesterol, other hepatic proteins (transferrin, fibrinogen); liver enzymes elevated, depending on the cause and acuity of liver injury; tendency toward hypokalemia, respiratory alkalosis; macrocytosis from folate deficiency |
| Renal (CRF) | Usually chronic: may be associated with uremic signs and symptoms, including decreased appetite, altered (metallic or fishy) taste, altered sleep pattern, difficulty concentrating, restless legs, or myoclonus; dyspnea can be present, but generally less prominent than in heart failure | Elevated blood pressure; hypertensive retinopathy; uremic fetor; pericardial friction rub in advanced cases | Elevation of serum creatinine and cystatin C; albuminuria; hyperkalemia, metabolic acidosis, hyperphosphatemia, hypocalcemia, anemia (usually normocytic) |
| Renal (NS) | Childhood diabetes mellitus; plasma cell dyscrasias | Periorbital edema; hypertension | Proteinuria (≥3.5 g/d); hypoalbuminemia; hypercholesterolemia; microscopic hematuria |
6. INVESTIGATIONS & DIAGNOSIS¶
- Noninvasive tests such as electrocardiography, echocardiography, and measurements of BNP (or N-terminal proBNP [NT-proBNP]) are helpful in establishing the diagnosis of heart disease.
- Urinalysis is essential for evaluating nephrotic syndrome or renal failure.
- Liver function tests and serum albumin are required for hepatic causes.
- Spectroscopic examination of the blood should be performed to look for abnormal types of hemoglobin (critical in the differential diagnosis of cyanosis) when the mechanism is obscure.
- Pao and Sao should be determined in patients with cyanosis in whom the mechanism is obscure.
7. MANAGEMENT & TREATMENT¶
- Blockade of the conversion of angiotensin I to AII and blockade of the AII receptors enhance sodium and water excretion and reduce many forms of retention of edema.
- Blockade of the action of aldosterone by spironolactone or eplerenone (aldosterone antagonists) or by amiloride (a blocker of epithelial sodium channels) often induces a moderate diuresis in edematous states.
- Treatment of the underlying cause is paramount.
- Drug-Induced Edema Management
- A large number of widely used drugs can cause edema (Table 43-2).
- Mechanisms include renal vasoconstriction (nonsteroidal anti-inflammatory drugs and cyclosporine), arteriolar dilation (vasodilators), augmented renal sodium reabsorption (steroid hormones), and capillary damage.
- Management of lymphedema is particularly intractable because restriction of lymphatic flow results in both an increase in intracapillary pressure and increased protein concentration in the interstitial fluid, which act in concert to aggravate fluid retention.
Table 2 — Table 43-2 Drugs Associated with Edema Formation¶
| Drug Class/Name |
|---|
| Nonsteroidal anti-inflammatory drugs |
| Antihypertensive agents |
| Direct arterial/arteriolar vasodilators |
| Hydralazine |
| Clonidine |
| Methyldopa |
| Guanethidine |
| Minoxidil |
| Calcium channel antagonists |
| α-Adrenergic antagonists |
| Thiazolidinediones |
| Steroid hormones |
| Glucocorticoids |
| Anabolic steroids |
| Estrogens |
| Progestins |
| Cyclosporine |
| Growth hormone |
| Immunotherapies |
| Interleukin 2 |
| OKT3 monoclonal antibody |
7.1 Drug-Associated Edema¶
- Nonsteroidal anti-inflammatory drugs
- Antihypertensive agents
- Direct arterial/arteriolar vasodilators
- Hydralazine
- Clonidine
- Methyldopa
- Guanethidine
- Minoxidil
- Calcium channel antagonists
- α-Adrenergic antagonists
- Thiazolidinediones
- Steroid hormones
- Glucocorticoids
- Anabolic steroids
- Estrogens
- Progestins
- Cyclosporine
- Growth hormone
- Immunotherapies
- Interleukin 2
- OKT3 monoclonal antibody
8. PROGNOSIS & COMPLICATIONS¶
- Lymphedema is particularly intractable because restriction of lymphatic flow results in both an increase in intracapillary pressure and increased protein concentration in the interstitial fluid, which act in concert to aggravate fluid retention.
- In some instances, clubbing is reversible, such as following lung transplantation for cystic fibrosis.
- Edema of starvation may resolve with adequate diet, though refeeding edema may occur.
- Hepatic cirrhosis edema may progress from ascites to peripheral edema in later stages.
9. SPECIAL CONSIDERATIONS¶
- Pregnancy is listed as a cause of edema under Other Causes of Edema.
- Pediatrics: Nephrotic syndrome may occur in childhood (e.g., childhood diabetes mellitus, plasma cell dyscrasias).
- Nutritional: Edema of starvation and refeeding edema are specific considerations.
- See also Chap. 393 for RAAS details.
- See also Chap. 264 for heart failure details.
- See also Chap. 326 for renal disease details.
- See also Chap. 355 for hepatic cirrhosis details.
- See also Chap. 53 for ascites details.
- See also Chap. 344 for nutritional origin details.
10. KEY PEARLS & CLINICAL TRAPS¶
- Cyanosis present since birth or infancy is usually due to congenital heart disease.
- Massage or gentle warming of a cyanotic extremity will increase peripheral blood flow and abolish peripheral, but not central, cyanosis.
- The combination of cyanosis and clubbing is frequent in patients with congenital heart disease and right-to-left shunting and is seen occasionally in patients with pulmonary disease, such as lung abscess or pulmonary arteriovenous fistulae.
- In contrast, peripheral cyanosis or acutely developing central cyanosis is not associated with clubbed digits.
- In some instances, clubbing is reversible, such as following lung transplantation for cystic fibrosis.
- Edema of Renal Disease differs from most forms of heart failure in that it is characterized by a normal (or sometimes even increased) cardiac output.
- The edema of heart failure typically occurs in the dependent portions of the body.
- So-called refeeding edema also may be linked to increased release of insulin, which directly increases tubular sodium reabsorption.
WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Certain features are important in arriving at the cause of cyanosis:
- It is important to ascertain the time of onset of cyanosis. Cyanosis present since birth or infancy is usually due to congenital heart disease.
- Central and peripheral cyanosis must be differentiated. Evidence of disorders of the respiratory or cardiovascular systems is helpful.
- The presence or absence of clubbing of the digits should be ascertained.
- PaO2 and SaO2 should be determined, and in patients with cyanosis in whom the mechanism is obscure, spectroscopic examination of the blood should be performed to look for abnormal types of hemoglobin.
- Pathognomonic signs Harrison's explicitly calls out:
- Clubbing in patients with primary and metastatic lung cancer, mesothelioma, bronchiectasis, or hepatic cirrhosis may be associated with hypertrophic osteoarthropathy.
- Edema of Renal Disease is characteristically associated with hematuria, proteinuria, and hypertension.
- Edema resulting from hypoproteinemia, as occurs in the nephrotic syndrome, characteristically is generalized, but it is especially evident in the very soft tissues of the eyelids and face.
- Edema limited to one leg or to one or both arms is usually the result of venous and/or lymphatic obstruction.
- In patients with obstruction of the superior vena cava, edema is confined to the face, neck, and upper extremities.
- Edema associated with heart failure tends to be more extensive in the legs and to be accentuated in the evening.
- When patients with heart failure are confined to bed, edema may be most prominent in the presacral region.
- Less common causes of facial edema include trichinosis, allergic reactions, and myxedema.
WHAT EXCLUDES THE DIAGNOSIS¶
- Generally, digital clubbing does not occur with these conditions [abnormal hemoglobin species].
- In contrast, peripheral cyanosis or acutely developing central cyanosis is not associated with clubbed digits.
- Clubbing may be hereditary, idiopathic, or acquired and associated with a variety of disorders, including cyanotic congenital heart disease, infective endocarditis, and a variety of pulmonary conditions (among them primary and metastatic lung cancer, bronchiectasis, asbestosis, sarcoidosis, lung abscess, cystic fibrosis, tuberculosis, and mesothelioma), as well as with some gastrointestinal diseases (including inflammatory bowel disease and hepatic cirrhosis).
- In some instances, clubbing is reversible, such as following lung transplantation for cystic fibrosis.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
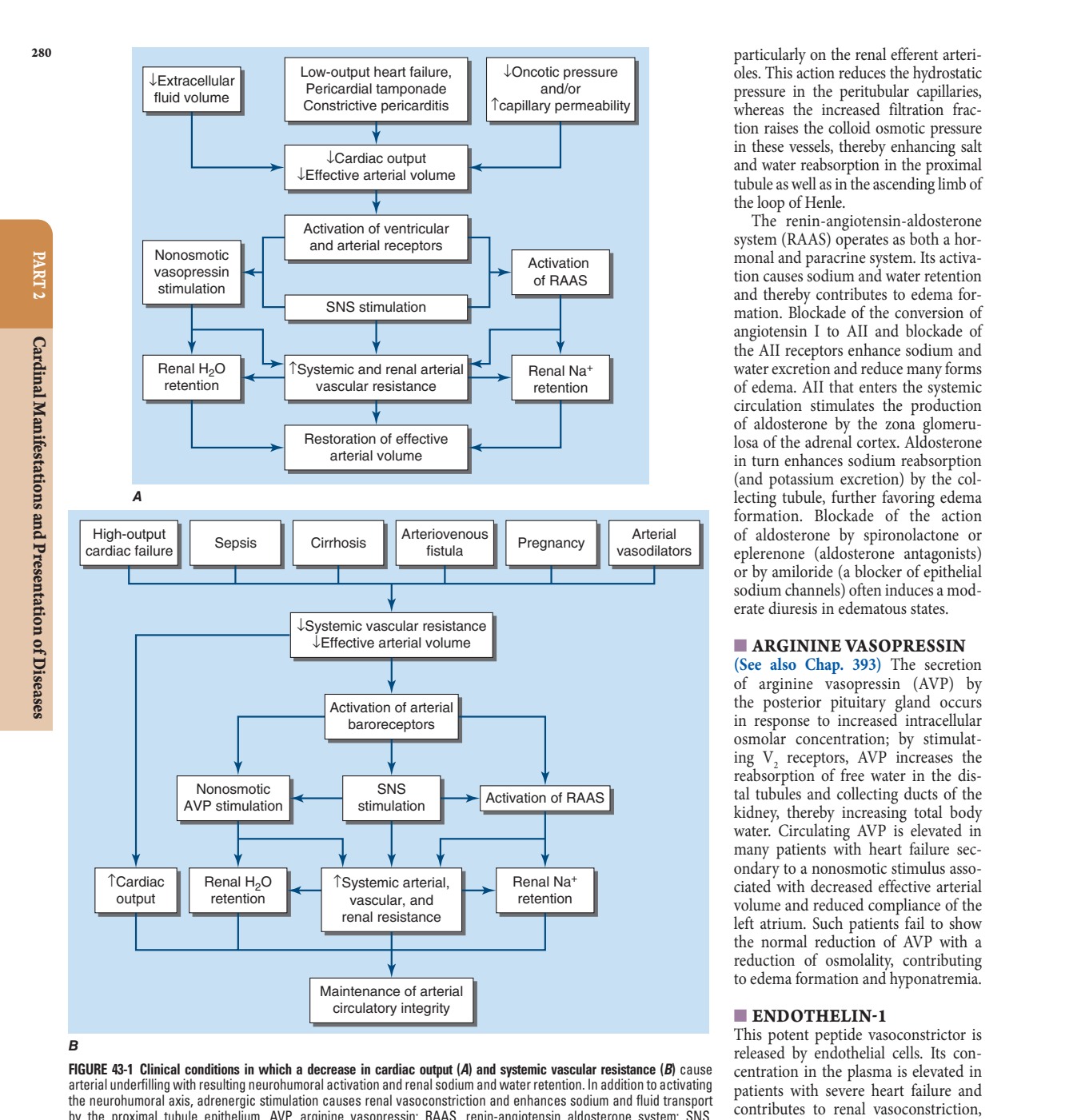
Caption: FIGURE 43-1 Clinical conditions in which a decrease in cardiac output (A) and systemic arterial underfilling with resulting neurohumoral activation and renal sodium and water the neurohumoral axis, adrenergic stimulation causes renal vasoconstriction and by the proximal tubule epithelium. AVP, arginine vasopressin; RAAS, sympathetic nervous system. (From Annals of Internal Medicine, RW Schrier: Body and disease: A unifying hypothesis. 113(2):155-159, 1990. Copyright © 1990, American Reserved. Reprinted with the permission of American College of Physicians, Inc.) — Figure 43-1 Clinical conditions in which a decrease in cardiac output (A) and systemic vascular resistance (B) cause arterial underfilling with resulting neurohumoral activation and renal sodium and water retention. In addition to activating the neurohumoral axis, adrenergic stimulation causes renal vasoconstriction and enhances sodium and fluid transport by the proximal tubule epithelium. AVP, arginine vasopressin; RAAS, renin-angiotensin aldosterone system; SNS, sympathetic nervous system. (From Annals of Internal Medicine, RW Schrier: Body fluid volume regulation in health and disease: A unifying hypothesis. 113(2):155-159, 1990. Copyright © 1990, American College of Physicians. All Rights Reserved. Reprinted with the permission of American College of Physicians, Inc.)
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.