Sustained VentricularTachycardia¶
Chapter 261 | Harrison's 22e · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Algorithm for differentiation of ventricular tachycardia (VT) from supraventricular tachycardia with aberration |
| 1 | 🖼 Figure | Cardiac magnetic resonance image (MRI) |
| 2 | 🖼 Figure | Idiopathic monomorphic ventricular tachycardia (VT) |
| 3 | 🖼 Figure | Monomorphic ventricular tachycardia in a patient with prior myocardial narrower and are... |
| 4 | 🖼 Figure | Accelerated idioventricular rhythm |
RAW CONTENT¶
[PAGE 1963] Sustained Ventricular Tachycardia 1963 CHAPTER 261 I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 V1 FIGURE 260-4 Accelerated idioventricular rhythm. Shown is an example of a slow regular wide-complex rhythm. Fusion beats are seen on complexes 4 and 10, which are more positive in lead V and narrower than the rest of the beats. These features are consistent with an accelerated idioventricular rhythm. 1 myocardium can cause AIVR. Idioventricular rhythms are common during acute MI and may emerge during sinus bradycardia. Often, they 261 Sustained Ventricular are not symptomatic, but hemodynamic compromise may occur with Tachycardia the loss of atrioventricular synchrony in susceptible patients. Atropine may be administered to increase the sinus rates if this is a concern. This rhythm is also common in patients with cardiomyopathies or sleep William H. Sauer, Usha B. Tedrow apnea. It can also be idiopathic, often emerging when the sinus rate slows during sleep. Therapy should target any underlying cause and correction of bradycardia. Specific antiarrhythmic therapy for asymp- Sustained monomorphic ventricular tachycardia (VT) is a ventricular tomatic idioventricular rhythm is not necessary. arrhythmia with a wide QRS lasting for at least 30 s or requiring an intervention such as antitachycardia pacing from a defibrillator or FUTURE DIRECTIONS a cardioversion for termination. Each QRS complex resembles the Recently, it has been appreciated that inflammation plays a role in others, indicating either a focal site of origin or a repetitive exit from the genesis of PVCs in specific patients with inflammatory cardiomy- a fixed arrhythmia reentry circuit. In structural heart disease, the opathies and even in inherited cardiomyopathies. The roles of early arrhythmia substrate is most often an area of patchy replacement fibro- identification of this process and targeted treatment are areas of active sis due to infarction, fibrosis, inflammation, or prior cardiac surgery research. that creates anatomic or functional reentrant pathways. Less com- ■ FURTHER READING monly, VT is related to reentry or automaticity in diseased conduction pathways in the Purkinje system. While scar-related reentrant VTs are Al-Khatib SM et al: 2017 AHA/ACC/HRS guideline for manage- associated with risk of sudden death, idiopathic VT is a more benign ment of patients with ventricular arrhythmias and the prevention form of VT that occurs in structurally normal hearts and can be due to of sudden cardiac death: A report of the American College of a focal region of automaticity in the myocardium or reentry involving Cardiology/American Heart Association Task Force on Clinical a portion of the Purkinje system. Practice Guidelines and the Heart Rhythm Society. Heart Rhythm The clinical presentation varies depending on the rate of the 15:e73, 2018. arrhythmia, underlying cardiac function, and autonomic adaptation in Callans DJ: Josephson’s Clinical Cardiac Electrophysiology: Techniques response to the arrhythmia. Rapid VT can produce hypotension that and Interpretations, 7th ed. Philadelphia, Wolters Kluwer, 2024. may present as syncope, particularly in patients with significant ven- Cronin EM et al: 2019 HRS/EHRA/APHRS/LAHRS expert consensus tricular dysfunction. In contrast, patients with normal cardiac function statement on catheter ablation of ventricular arrhythmias. EP Euro- might tolerate sustained VT, even presenting with simple palpitations, pace 21:1143, 2019. despite rapid rates. Monomorphic VT that is rapid or associated with Jalife J, Stevenson W (eds): Zipes and Jalife’s Cardiac Electrophysiol- structural heart disease may eventually deteriorate to ventricular fibril- ogy: From Cell to Bedside, 8th ed. Philadelphia, Elsevier, 2022. lation (VF), which may be the initial cardiac rhythm recorded at the Zeppenfeld K et al: 2022 ESC Guidelines for the management of time of resuscitation of an out-of-hospital cardiac arrest. patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of DIAGNOSIS patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed Sustained monomorphic VT (Table 261-1) has to be distinguished by the Association for European Paediatric and Congenital Cardiol- from other causes of uniform wide QRS tachycardia. These include ogy (AEPC). Eur Heart J 43:3997, 2022. supraventricular tachycardia with left or right bundle branch block
[PAGE 1964] 1964 PART 6 Disorders of the Cardiovascular System VT versus Supraventricular Tachycardia (SVT) TABLE 261-1 Sustained Ventricular Arrhythmias with Aberrancy 1. Idiopathic ventricular tachycardia (VT) without structural heart disease A. Outflow tract origin - Right ventricular (RV) outflow tract: left bundle branch block pattern in Yes V with inferior axis (tall QRS in inferior leads) and late transition in the AV dissociation VT 1 precordial leads - Left ventricular (LV) outflow tract: similar inferiorly directed axis but No with early precordial transition with prominent R wave in V–V 2 3 aVR aVR B. LV fascicular VT: Typical right bundle branch block pattern in V with sharp Yes 1 aVR = R or Rs VT intrinsicoid deflection and left axis deviation (arising from left posterior fascicle in its most common form) C. Papillary muscle VT No - Posteromedial: atypical right bundle branch block pattern in V with 1 V V V V V V monophasic R wave and left axis deviation Yes 1 2 3 4 5 6 No rS or Rs in VT - Anterolateral: atypical right bundle branch block pattern in V with positive deflection in lead III and negative deflection in lead I 1 any of V 1 to V 6 2. Ischemic cardiomyopathy No - Monomorphic VT is common with prior large myocardial infarction V 1 V 2 V 3 V 4 V 5 V 6 - Polymorphic VT and ventricular fibrillation (VF) should prompt ischemia Possible SVT with aberrancy evaluation VT still possible 3. Nonischemic cardiomyopathy FIGURE 261-1 Algorithm for differentiation of ventricular tachycardia (VT) from - Fibrotic scars can cause monomorphic VT, especially with sarcoidosis supraventricular tachycardia with aberration. AV, atrioventricular. or other inflammatory cardiomyopathies, Chagas’ disease, and familial arrhythmogenic cardiomyopathies such as Lamin A/C genetic cardiomyopathy ventriculoatrial (VA) dissociation is a reliable marker for VT, provided - Polymorphic VT and VF can also occur independently or related to the atrial rate is slower than the ventricular rate. Sometimes, P waves degeneration of monomorphic VT can be difficult to define, and the VA relationship cannot be assessed in 4. Arrhythmogenic RV cardiomyopathy a patient with an ongoing atrial arrhythmia such as atrial fibrillation. A - Monomorphic VT usually of RV origin (left bundle branch morphology in V) P wave following each QRS does not exclude VT because 1:1 conduc- 1 - Polymorphic VT and VF can occur independently or related to degeneration tion from ventricle to atrium can occur. A monophasic R wave or Rs of monomorphic VT complex in aVR or concordance from V to V of monophasic R or 1 6 5. Repaired tetralogy of Fallot S waves is also relatively specific for VT (Fig. 261-1). A number of - Monomorphic VT of RV origin (usually left bundle branch morphology in V) other QRS morphology criteria have also been described, but all have 1 6. Hypertrophic cardiomyopathy limitations and are not very reliable in patients with severe heart - Polymorphic VT or ventricular fibrillation disease. In patients with known bundle branch block, the same QRS - Less commonly, monomorphic VT associated with myocardial scars, morphology during tachycardia as during sinus rhythm suggests particularly apical aneurysms supraventricular tachycardia rather than VT, but even this is not abso- 7. Genetic arrhythmia syndromes lutely reliable. Patients with reentry involving the bundle branches of the Purkinje system can have a VT morphology that res
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
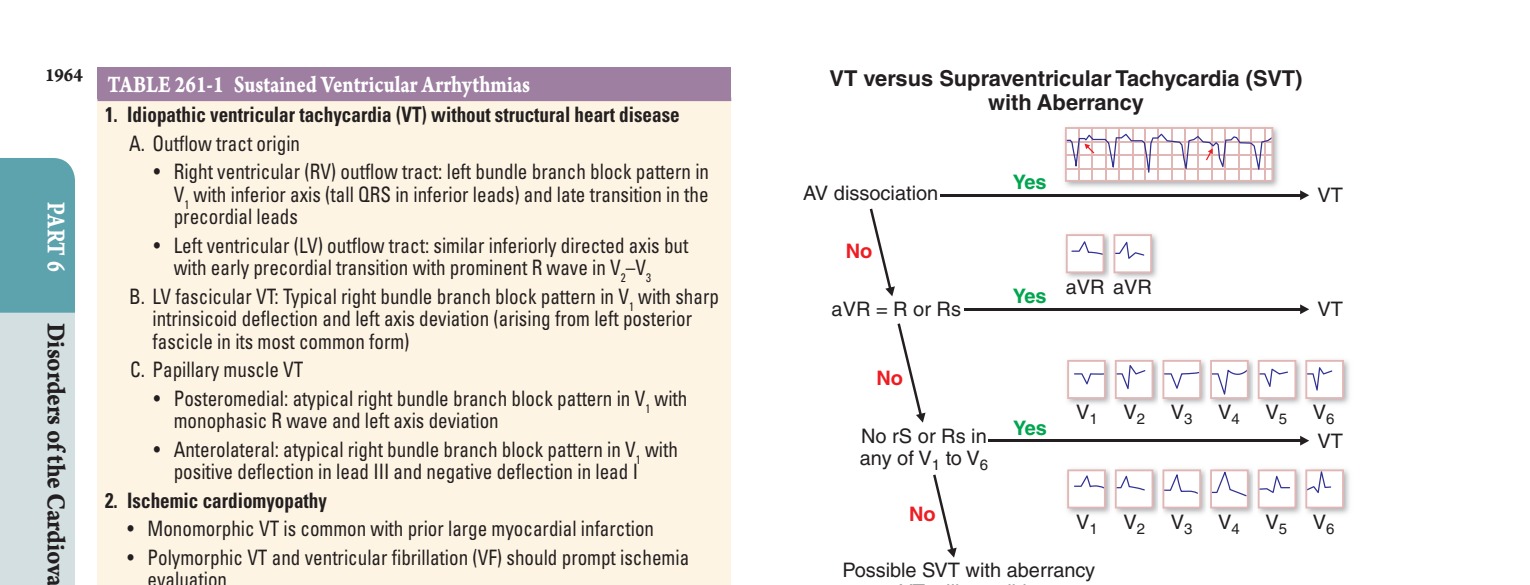
Caption: FIGURE 261-1 Algorithm for differentiation of ventricular tachycardia (VT) from supraventricular tachycardia with aberration. AV, atrioventricular.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
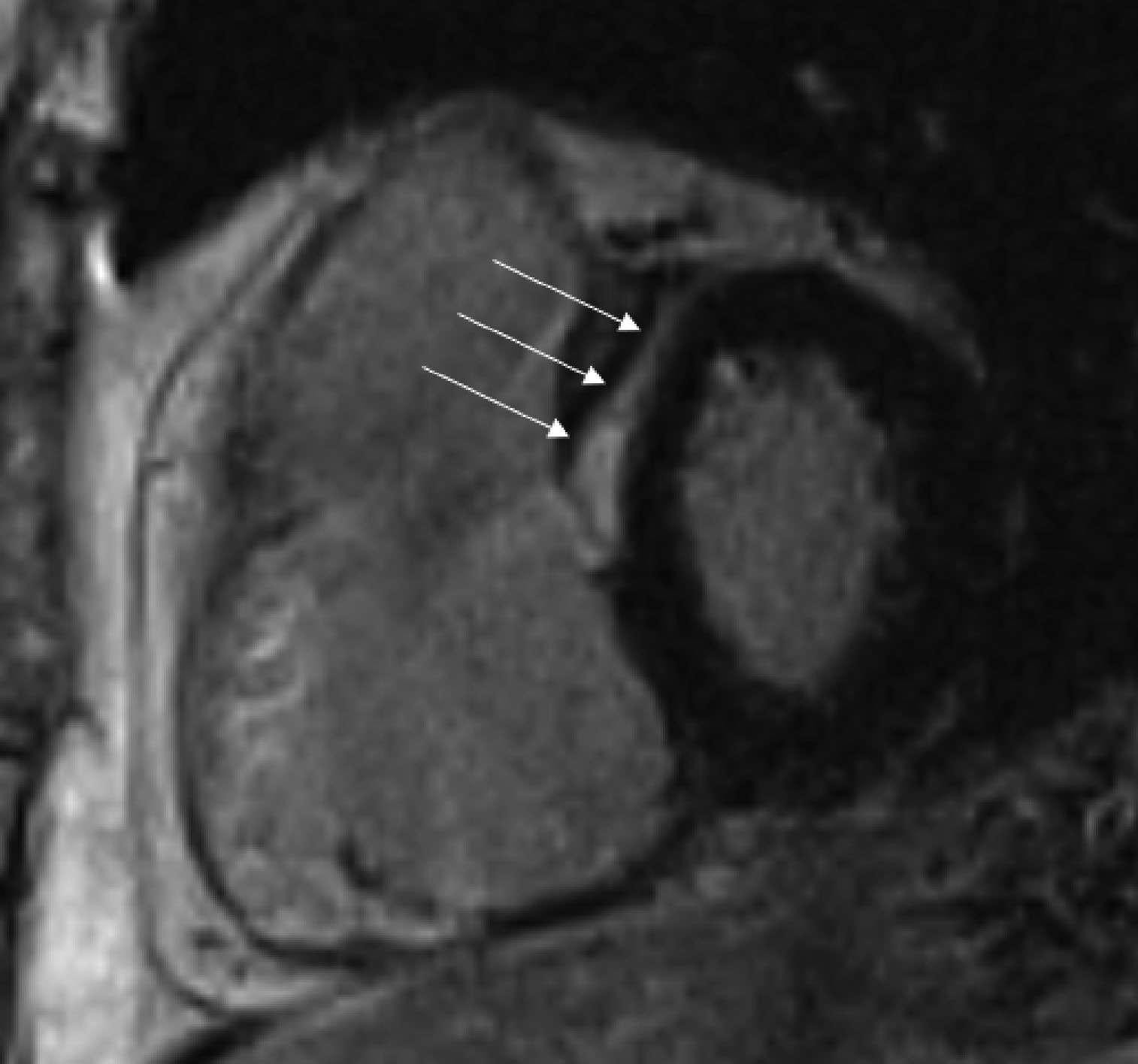
Caption: FIGURE 261-3 Cardiac magnetic resonance image (MRI). Shown is an MRI of the heart with the right ventricle on the left and the left ventricle on the right. Between the ventricles (arrows) is a stripe of late gadolinium enhancement, indicating midmyocardial fibrosis in the interventricular septum. This type of scar pattern is often seen in patients with nonischemic cardiomyopathies and ventricular tachycardia.
Figure 2¶
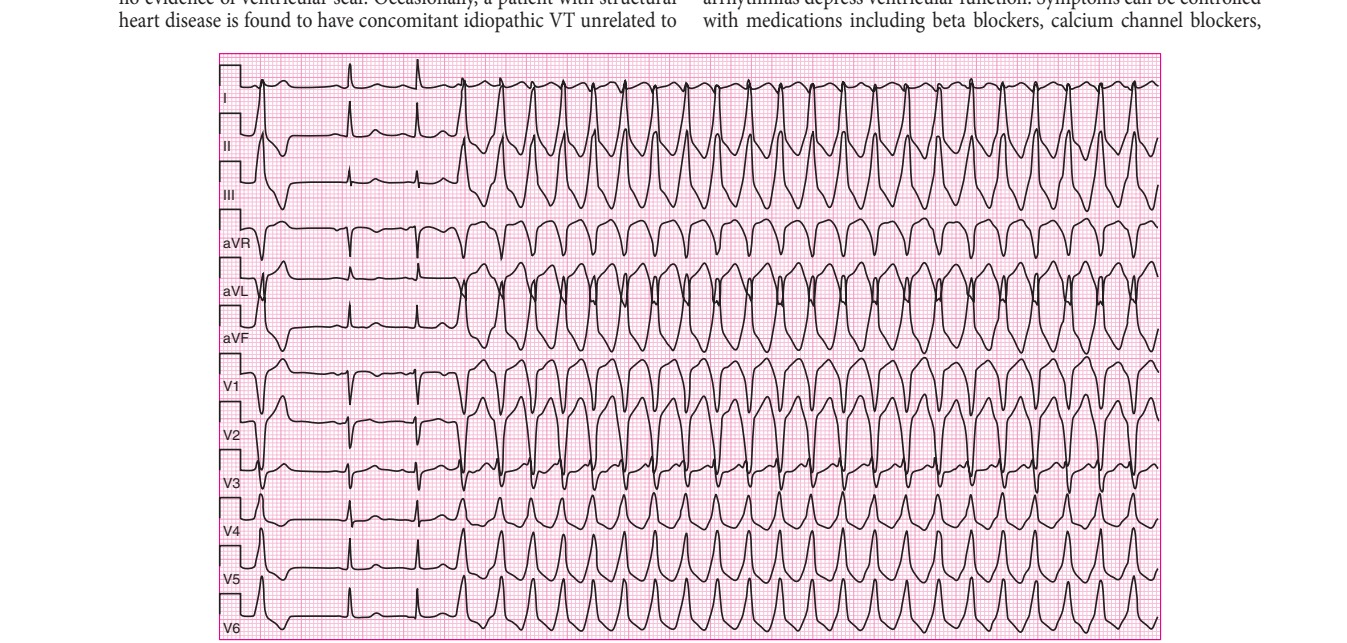
Caption: FIGURE 261-4 Idiopathic monomorphic ventricular tachycardia (VT). This is a 12-lead structural heart disease. The VT has a left bundle branch block configuration in V and an 1 (normal sinus) beats have a normal QRS configuration, consistent with the patient’s lack
Figure 3¶

Caption: FIGURE 261-2 Monomorphic ventricular tachycardia in a patient with prior myocardial narrower and are examples of fusion beats, proving ventriculoatrial (VA) dissociation and SUSTAINED MONOMORPHIC VT IN
Figure 4¶
Caption: FIGURE 260-4 Accelerated idioventricular rhythm. Shown is an example of a slow more positive in lead V and narrower than the rest of the beats. These features are 1
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.