Aortic Regurgitation¶
Chapter 273 | Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Aortic regurgitation (AR) is caused by primary valve disease, aortic root disease, or their combination.
- Chronic severe AR is a state of LV volume overload with increased preload and afterload; compensation occurs via LV dilation and eccentric hypertrophy.
- Classic physical findings include a water-hammer pulse (Corrigan's pulse), Quincke's pulse, Traube's sign, and Duroziez's sign.
- The Austin Flint murmur is a soft, low-pitched, rumbling mid-to-late diastolic murmur caused by diastolic displacement of the anterior mitral leaflet.
- Severe AR echocardiographic criteria: central jet width >65% of LVOT width, regurgitant volume ≥60 mL/beat, regurgitant fraction ≥50%, ERO ≥0.3 cm².
- Surgical intervention is indicated for symptomatic severe AR or asymptomatic severe AR with LV dysfunction (EF ≤55%), LVESD >50 mm (>25 mm/m²), or LVEDD >65 mm.
- Acute severe AR requires urgent surgery (within 24–48 h) due to rapid LV decompensation and risk of cardiogenic shock.
- Medical therapy for chronic AR includes diuretics for symptoms, vasodilators (ACEi, ARBs, CCBs) to reduce afterload, and beta-blockers for hypertension or aortopathy.
- Coexistence of hemodynamically significant aortic stenosis with AR usually excludes rarer forms of AR.
- Valve-sparing aortic root reconstruction (David procedure) is an option for root disease without primary valve involvement.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Etiologies
- 3.2 Pathophysiology
- 4. CLINICAL FEATURES
- 4.1 Physical Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria for Severe AR
- 7. MANAGEMENT & TREATMENT
- 7.1 Surgical Treatment
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Management of patients with aortic regurgitation |
| 1 | 🖼 Figure | Valve-sparing aortic root reconstruction (David procedure) |
| 2 | 🖼 Figure | Echocardiographic and Doppler depiction of severe aortic shows a broad jet of... |
| 3 | 🖼 Figure | Echocardiographic and Doppler depiction of severe aortic shows a broad jet of... |
| 4 | 🖼 Figure | Figure / Illustration |
1. DEFINITION & OVERVIEW¶
Aortic regurgitation (AR) is a valvular heart disease characterized by the retrograde flow of blood from the aorta into the left ventricle during diastole. It may be caused by primary valve disease, aortic root disease, or their combination. AR may be associated with other manifestations of Marfan's syndrome, idiopathic dilation of the aorta, annuloaortic ectasia, osteogenesis imperfecta, and severe, chronic hypertension. Occasionally AR is caused by retrograde dissection of the aorta involving the aortic annulus. Syphilis and ankylosing spondylitis may also affect the aortic leaflets and lead to aortic dilation, aneurysm formation, and severe regurgitation.
1.1 Classification¶
AR is classified based on the primary site of pathology: - Primary Valve Disease: Involves thickening, deformity, and shortening of individual aortic valve cusps. - Primary Aortic Root Disease: Involves marked aortic annular dilation without primary involvement of valve leaflets. - Combined Disease: Involves both valve and root pathology.
2. EPIDEMIOLOGY¶
Approximately three-fourths of patients with pure or predominant valvular AR are men; women predominate among patients with primary valvular AR who have associated rheumatic mitral valve disease. Patients with congenital bicuspid aortic valve (BAV) disease may develop predominant AR, and ~20% of these patients will require aortic valve surgery between 10 and 40 years of age.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
AR may be caused by primary valve disease, aortic root disease, or their combination. The total stroke volume ejected by the left ventricle (LV) is increased in patients with AR. In patients with severe AR, the volume of regurgitant flow may equal the effective forward stroke volume. An increase in the LV end-diastolic volume (increased preload) constitutes the major hemodynamic compensation for AR. The dilation and eccentric hypertrophy of the LV allow this chamber to eject a larger stroke volume without requiring any increase in the relative shortening of each myofibril. Therefore, severe AR may occur with a normal effective forward stroke volume and a normal LV ejection fraction (LVEF), together with an elevated LV end-diastolic pressure and volume. However, through the operation of Laplace's law, LV dilation increases the LV systolic tension required to develop any given level of systolic pressure. Chronic AR is, thus, a state in which LV preload and afterload are both increased. Ultimately, these adaptive measures fail. As LV function deteriorates, the end-diastolic volume rises further and the forward stroke volume and ejection fraction (EF) decline. Deterioration of LV function often precedes the development of symptoms. Considerable thickening of the LV wall also occurs with chronic AR, and at autopsy, the hearts of these patients may be among the largest encountered, sometimes weighing >1000 g.
3.1 Etiologies¶
AR etiologies are categorized by the primary lesion: - Valvular Lesions: Congenital (bicuspid), Endocarditis, Rheumatic fever, Myxomatous (prolapse), Radiation, Trauma, Syphilis, Ankylosing spondylitis. - Aortic Root Disease: Aortic dissection, Medial degeneration, Marfan syndrome, Bicuspid aortic valve, Nonsyndromic familial aneurysm, Aortitis, Hypertension.
Table 1 — TABLE 273-1 Major Causes of Aortic Regurgitation¶
| Aortic regurgitation | Valvular | Aortic root disease |
|---|---|---|
| Congenital (bicuspid) | Endocarditis | Aortic dissection |
| Rheumatic fever | Myxomatous (prolapse) | Medial degeneration |
| Syphilis | Radiation | Marfan syndrome |
| Ankylosing spondylitis | Trauma | Bicuspid aortic valve |
| Nonsyndromic familial aneurysm | Syphilis | Nonsyndromic familial aneurysm |
| Aortitis | Ankylosing spondylitis | Aortitis |
| Hypertension | Hypertension | Hypertension |
3.2 Pathophysiology¶
- Hemodynamics: The reverse diastolic pressure gradient from aorta to LV, which drives the AR flow, decreases progressively during diastole, accounting for the typical decrescendo nature of the diastolic murmur. Equilibration between aortic and LV pressures may occur toward the end of diastole in patients with chronic severe AR, particularly when the heart rate is slow.
- Acute Severe AR: The LV is unprepared for the regurgitant volume load. LV compliance is normal or reduced, and LV diastolic pressures rise rapidly, occasionally to levels >40 mmHg. The LV pressure may exceed the LA pressure toward the end of diastole, and this reversed pressure gradient closes the mitral valve prematurely.
- Myocardial Ischemia: May occur in patients with AR because myocardial oxygen requirements are elevated by LV dilation, hypertrophy, and elevated LV systolic tension, and coronary blood flow may be compromised. A large fraction (the majority) of coronary blood flow occurs during diastole, when aortic pressure is low, thereby reducing coronary perfusion or driving pressure. This combination of increased oxygen demand and reduced supply may cause myocardial ischemia, particularly of the subendocardium, even in the absence of epicardial coronary artery disease (CAD).
- Chronic Severe AR: The effective forward cardiac output (CO) usually is normal or only slightly reduced at rest, but often it fails to rise normally during exercise. An early sign of LV dysfunction is a reduction in the EF. In advanced stages, there may be considerable elevation of the LA, pulmonary artery (PA) wedge, PA, and right ventricular (RV) pressures and reduced forward CO at rest.
4. CLINICAL FEATURES¶
Chronic severe AR may have a long latent period, and patients may remain relatively asymptomatic for as long as 10–15 years. Uncomfortable awareness of the heartbeat, especially on lying down, may be an early complaint. Sinus tachycardia, during exertion or with emotion, or premature ventricular contractions may produce particularly uncomfortable palpitations as well as head pounding. These complaints may persist for many years before the development of exertional dyspnea, usually the first symptom of diminished cardiac reserve. The dyspnea is followed by orthopnea, paroxysmal nocturnal dyspnea, and excessive diaphoresis. Anginal chest pain even in the absence of CAD may occur in patients with severe AR, even in younger patients. Anginal pain may develop at rest as well as during exertion. Nocturnal angina may be a particularly troublesome symptom, and it may be accompanied by marked diaphoresis. The anginal episodes can be prolonged and often do not respond satisfactorily to sublingual nitroglycerin. Systemic fluid accumulation, including congestive hepatomegaly and ankle edema, may develop late in the course of the disease. In acute severe AR, the elevation of LV end-diastolic pressure may lead to early closure of the mitral valve, a soft S, a pulse pressure that is not particularly wide, and a soft, short, early diastolic murmur of AR.
4.1 Physical Findings¶
- Palpation: In patients with chronic severe AR, the LV impulse is heaving and displaced laterally and inferiorly. The systolic expansion and diastolic retraction of the apex are prominent. A diastolic thrill may be palpable along the left sternal border in thin-chested individuals, and a prominent systolic thrill may be palpable in the suprasternal notch and transmitted upward along the carotid arteries. This systolic thrill and the accompanying murmur do not necessarily signify the coexistence of AS.
- Arterial Pulse: A rapidly rising "water-hammer" pulse, which collapses suddenly as arterial pressure falls rapidly during late systole and diastole (Corrigan's pulse), and capillary pulsations, an alternate flushing and paling of the skin at the root of the nail while pressure is applied to the tip of the nail (Quincke's pulse), are characteristic of chronic severe AR. A booming "pistol-shot" sound can be heard over the femoral arteries (Traube's sign), and a to-and-fro murmur (Duroziez's sign) is audible if the femoral artery is lightly compressed with a stethoscope. The arterial pulse pressure is widened as a result of both systolic hypertension and a lowering of the diastolic pressure.
- Auscultation: In patients with severe AR, the aortic valve closure sound (A) is usually absent. A systolic ejection sound is audible in patients with BAV disease, and occasionally an S also may be heard. The murmur of chronic AR is typically a high-pitched, blowing, decrescendo diastolic murmur, heard best in the third intercostal space along the left sternal border. In patients with mild AR, this murmur is brief, but as the severity increases, it generally becomes louder and longer, indeed holodiastolic. When the murmur is soft, it can be heard best with the diaphragm of the stethoscope and with the patient sitting up, leaning forward, and with the breath held in forced expiration. In patients in whom the AR is caused by primary valvular disease, the diastolic murmur is usually louder along the left than the right sternal border. However, when the murmur is louder along the right sternal border, it suggests that the AR is caused by aneurysmal dilation of the aortic root. "Cooing" or musical diastolic murmurs suggest eversion of an aortic cusp vibrating in the regurgitant stream. A mid-systolic ejection murmur is frequently audible in isolated AR. It is generally heard best at the base of the heart and is transmitted along the carotid arteries. This murmur may be quite loud without signifying aortic valve obstruction. A third murmur sometimes heard in patients with severe AR is the Austin Flint murmur, a soft, low-pitched, rumbling mid-to-late diastolic murmur. It is probably produced by the diastolic displacement of the anterior leaflet of the mitral valve by the AR stream and is not associated with hemodynamically significant mitral valve obstruction. The auscultatory features of AR are intensified by strenuous and sustained handgrip, which augments systemic vascular resistance and increases LV afterload.
5. DIFFERENTIAL DIAGNOSIS¶
The coexistence of hemodynamically significant aortic stenosis (AS) with AR usually excludes all the rarer forms of AR because it occurs almost exclusively in patients with rheumatic or congenital AR. In patients with AR due to primary valvular disease, dilation of the aortic annulus may occur secondarily and lead to worsening regurgitation. The reverse diastolic pressure gradient from aorta to LV, which drives the AR flow, decreases progressively during diastole, accounting for the typical decrescendo nature of the diastolic murmur.
6. INVESTIGATIONS & DIAGNOSIS¶
ECG examination should be directed toward the detection of conditions predisposing to AR, such as bicuspid valve, IE, Marfan's syndrome, or ankylosing spondylitis. In patients with chronic severe AR, ECG signs of LV hypertrophy are common. In addition, these patients frequently exhibit ST-segment depression and T-wave inversion in leads I, aVL, V, and V6 ("LV strain"). Left axis deviation and/or QRS prolongation may also be present.
Echocardiogram: LV size is increased in chronic AR, and systolic function is normal or even supernormal until myocardial contractility declines, as signaled by a decrease in EF or increase in the end-systolic dimension. A rapid, high-frequency diastolic fluttering of the anterior mitral leaflet produced by the impact of the regurgitant jet is a characteristic finding. The echocardiogram is also useful in determining the cause of AR, by detecting dilation of the aortic annulus and root, aortic dissection or primary leaflet pathology. With severe AR, the central jet width assessed by color flow Doppler imaging exceeds 65% of the width of the LV outflow tract, the regurgitant volume is ≥60 mL/beat, the regurgitant fraction is ≥50%, and there is diastolic flow reversal in the proximal portion of the descending thoracic aorta. The continuous-wave Doppler profile of the AR jet shows a rapid deceleration time in patients with acute severe AR, due to the rapid increase in LV diastolic pressure. Surveillance transthoracic echocardiography (TTE) forms the cornerstone of longitudinal follow-up and allows for the early detection of changes in LV size and/or function. Assessment of LV global longitudinal strain (GLS; a measure of myocardial thickening in systole) with speckle track imaging may demonstrate changes in LV systolic function that precede a fall in EF. There is increasing experience with the use of three-dimensional echocardiography to measure LV volumes. Transesophageal echocardiography (TEE) can provide detailed anatomic assessment of the valve, root, and portions of the aorta. For patients in whom TTE is limited by poor acoustical windows or inadequate characterization of LV function or the cause or severity of the regurgitation, cardiac magnetic resonance (CMR) imaging can be performed. This modality also allows for accurate assessment of LV volumes, as well as aortic size and contour. It can also be utilized to screen for increased LV interstitial (extracellular volume fraction) and replacement fibrosis (late gadolinium enhancement). Both CMR imaging and cardiac computed tomography (CT) can also provide detailed assessment of aortic valve, root, and thoracic aortic anatomy.
Chest X-Ray: In chronic severe AR, the apex is displaced downward and to the left in the frontal projection. In the left anterior oblique and lateral projections, the LV is displaced posteriorly and encroaches on the spine. When AR is caused by primary disease of the aortic root, aneurysmal dilation of the aorta may be noted, and the aorta may fill the retrosternal space in the lateral view. Echocardiography, CMR imaging, and chest CT angiography are more sensitive than a chest x-ray for the detection of root and ascending aortic enlargement.
Cardiac Catheterization and Angiography: When needed, right and left heart catheterization with contrast aortography can provide confirmation of the magnitude of regurgitation and the status of LV function. Coronary angiography is performed routinely in patients at risk of coronary artery disease prior to surgery, although this anatomic information can also be obtained in many patients with coronary CT angiography.
6.1 Diagnostic Criteria for Severe AR¶
Severe AR is defined by the following echocardiographic criteria: - Central jet width >65% of LVOT width. - Regurgitant volume ≥60 mL/beat. - Regurgitant fraction ≥50%. - Effective regurgitant orifice (ERO) ≥0.3 cm². - Diastolic flow reversal in the proximal descending thoracic aorta.
7. MANAGEMENT & TREATMENT¶
Aortic Regurgitation Treatment is divided into Acute and Chronic management.
ACUTE AORTIC REGURGITATION: Patients with acute severe AR may respond to intravenous diuretics and vasodilators (such as sodium nitroprusside), but stabilization is usually short-lived and operation is indicated urgently. Intra-aortic balloon counterpulsation is contraindicated. Beta blockers are best avoided so as not to reduce the CO further or slow the heart rate, thus allowing more time for diastolic filling of the LV. Surgery is the treatment of choice and is usually necessary within 24 h of diagnosis.
CHRONIC AORTIC REGURGITATION: The onset of symptoms, or LV systolic dysfunction, is an indication for surgery. Medical treatment with diuretics and vasodilators (angiotensin-converting enzyme inhibitors, angiotensin receptor blockers [ARBs], dihydropyridine calcium channel blockers, or hydralazine) may be useful as a temporizing measure. Surgery is the treatment of choice and is usually necessary within 24 h of diagnosis for acute cases. For chronic cases, operation should be carried out in asymptomatic patients with severe AR and progressive LV dysfunction defined by an LVEF 50 mm (>25 mm/m²), or an LV diastolic dimension >65 mm. Smaller dimensions may be appropriate thresholds in individuals of smaller stature or when there is evidence of progressively decreasing LV function or increasing LV size on serial studies and the anticipated risks for surgical morbidity and mortality are low. Exercise testing may be helpful to assess effort tolerance more objectively and should be employed whenever questions about symptoms arise. Operation can be deferred as long as the patient both remains asymptomatic and retains normal LV function without severe or progressive chamber dilation.
MEDICAL THERAPY: Beta blockers in patients with valvular AR were previously considered relatively contraindicated due to concern that slowing of the heart rate would allow more time for diastolic regurgitation and LV filling. Observational reports, however, have suggested that beta blockers may provide functional benefit in some patients with chronic AR. Beta blockers can sometimes provide incremental blood pressure lowering in patients with chronic AR and hypertension. They can also lessen the sense of forceful heart action that many patients find uncomfortable. Patients with severe AR, particularly those with an associated aortopathy, should avoid isometric exercises. Patients with syphilitic aortitis should receive a full course of penicillin therapy. Beta blockers and the ARB losartan may be useful to retard the rate of aortic root enlargement in young patients with Marfan's syndrome and aortic root dilation. A randomized controlled trial showed no difference in efficacy between atenolol and losartan for this indication. Whether beta blockers or ARBs are useful in retarding the rate of growth of aortic aneurysms in other patient subsets (e.g., BAV disease with aortopathy, Takayasu's disease) has not been demonstrated. Beta blockers in patients with valvular AR were previously considered relatively contraindicated due to concern that slowing of the heart rate would allow more time for diastolic regurgitation and LV filling. Although nitroglycerin and long-acting nitrates are not as helpful in relieving anginal pain as they are in patients with coronary heart disease, they are worth a trial. Patients with severe AR and hypertension should avoid isometric exercises. The use of vasodilators to extend the compensated phase of chronic severe AR in asymptomatic patients before the onset of symptoms or the development of LV dysfunction is not useful, although these agents should be employed to treat hypertension (systolic blood pressure >140 mmHg). It is often difficult to achieve adequate blood pressure control because of the increased stroke volume and enhanced LV ejection that accompany severe AR. Cardiac arrhythmias and systemic infections are poorly tolerated in patients with severe AR and must be treated promptly and vigorously.
7.1 Surgical Treatment¶
Aortic valve replacement (AVR) is indicated for the treatment of severe AR in symptomatic patients irrespective of LV function. In general, the operation should be carried out in asymptomatic patients with severe AR and progressive LV dysfunction defined by an LVEF 50 mm (>25 mm/m²), or an LV diastolic dimension >65 mm. Smaller dimensions may be appropriate thresholds in individuals of smaller stature or when there is evidence of progressively decreasing LV function or increasing LV size on serial studies and the anticipated risks for surgical morbidity and mortality are low. Two case series of patients with severe AR without indications for operation should be followed by clinical and echocardiographic examination every 6–12 months. Transcatheter aortic valve implantation (TAVI) is not recommended for patients with severe AR who are surgical candidates. Technical success with TAVI in patients with chronic AR is limited by the degree of aortic annular dilation and the relative paucity of valvular and annular calcium. Surgical options for management of aortic valve and root disease have expanded considerably over the past decade. AVR with a suitable mechanical or tissue (biological) prosthesis is generally necessary in patients with rheumatic AR and in many patients with other causes of valvular AR. Rarely, when a leaflet has been perforated during IE or torn from its attachments to the aortic annulus by thoracic trauma, primary surgical repair may be possible. When AR is due to aneurysmal dilation of the root or proximal ascending aorta rather than to primary valve involvement, it may be possible to reduce or eliminate the regurgitation by narrowing the annulus or by excising a portion of the aortic root without replacing the valve. Elective, valve-sparing treatment, which may be lifesaving, generally involves reimplantation of the valve in a contoured graft with reattachment of the coronary artery buttons into the side of the graft and is best undertaken in specialized surgical centers by experienced operators. Resuspension of the native aortic valve leaflets is possible in ~50% of patients with acute AR in the setting of type A aortic dissection. In other conditions, however, AR can be effectively eliminated only by replacing the aortic valve, as well as the dilated or aneurysmal ascending aorta with responsible for the regurgitation, often using a composite prosthetic valve-graft conduit. Pure AR is not by itself a contraindication to the Ross procedure, although the presence of aortic annular dilation and/or an associated aortopathy would eliminate this option. As is true in patients with other valvular heart disease, both operative and late mortality risks are largely dependent on the stage of the disease and myocardial function at the time of operation. The overall operative mortality rate for isolated AVR performed for pure AR is ~1–2%. The mortality risk doubles when aortic surgery is added to the operation. Patients with AR, marked cardiac enlargement, and established LV dysfunction experience an operative mortality rate of ~5–10% and a late mortality rate of ~3–5% per year due to LV failure despite a technically satisfactory operation. Nonetheless, because of the very poor prognosis with medical management, even patients with advanced LV systolic dysfunction should be considered for operation. Patients with acute severe AR require prompt (24–48 h) surgical treatment, which may be lifesaving.
8. PROGNOSIS & COMPLICATIONS¶
Patients with AR, marked cardiac enlargement, and established LV dysfunction experience an operative mortality rate of ~5–10% and a late mortality rate of ~3–5% per year due to LV failure despite a technically satisfactory operation. Nonetheless, because of the very poor prognosis with medical management, even patients with advanced LV systolic dysfunction should be considered for operation. Abnormal LV GLS (≥ –18%) has been associated with an excess hazard for death in single-center studies. Observational studies using either three-dimensional echocardiography or CMR imaging have also suggested that event-free survival is reduced in asymptomatic patients with an LV end-systolic volume index ≥45 mL/m², compared with patients with an LV end-systolic volume index <45 mL/m².
9. SPECIAL CONSIDERATIONS¶
The text does not provide specific details on pregnancy, pediatrics, elderly, renal/hepatic impairment, or immunocompromised states beyond general management principles for severe AR (e.g., avoiding isometric exercises, treating arrhythmias and infections promptly).
10. KEY PEARLS & CLINICAL TRAPS¶
- Water-hammer pulse (Corrigan's pulse) and Quincke's pulse are characteristic of chronic severe AR.
- Austin Flint murmur is a soft, low-pitched, rumbling mid-to-late diastolic murmur caused by diastolic displacement of the anterior mitral leaflet.
- Coexistence of hemodynamically significant aortic stenosis (AS) with AR usually excludes all the rarer forms of AR.
- Acute severe AR requires urgent surgery (within 24–48 h).
- Severe AR echocardiographic criteria: central jet width >65% of LVOT width, regurgitant volume ≥60 mL/beat, regurgitant fraction ≥50%, ERO ≥0.3 cm².
- Surgical thresholds: EF ≤55%, LVESD >50 mm (>25 mm/m²), or LVEDD >65 mm.
- Beta blockers and ARBs may be useful to retard the rate of aortic root enlargement in young patients with Marfan's syndrome and aortic root dilation.
- Patients with severe AR should avoid isometric exercises.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
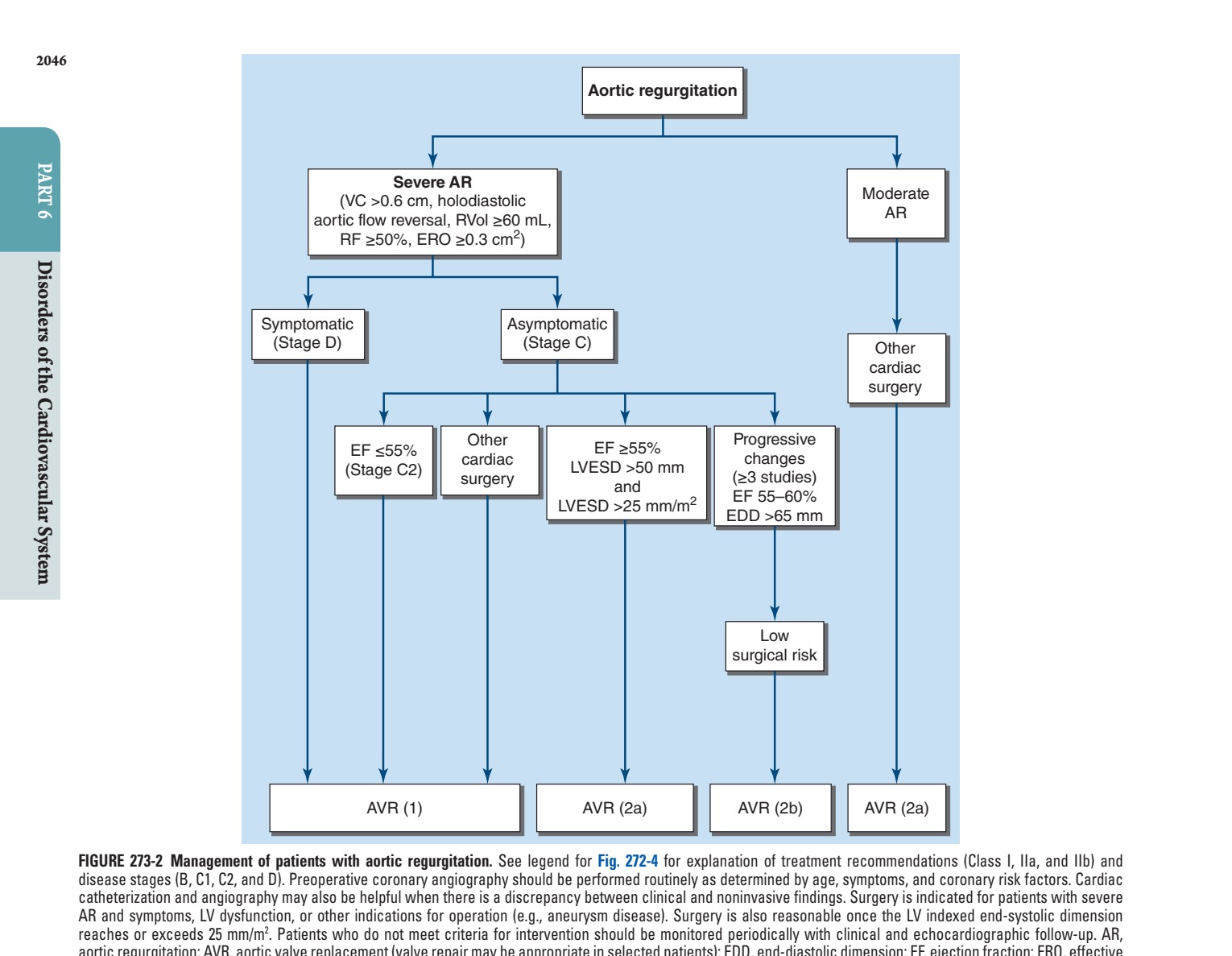
Caption: FIGURE 273-2 Management of patients with aortic regurgitation. See legend for Fig. disease stages (B, C1, C2, and D). Preoperative coronary angiography should be catheterization and angiography may also be helpful when there is a discrepancy AR and symptoms, LV dysfunction, or other indications for operation (e.g., aneurysm reaches or exceeds 25 mm/m2. Patients who do not meet criteria for intervention aortic regurgitation; AVR, aortic valve replacement (valve repair may be appropriate in regurgitant orifice; LV, left ventricular; LVEDD, left ventricular end-diastolic dimension; RF, regurgitant fraction; RVol, regurgitant volume; VC, vena contracta. (Reproduced with with valvular heart disease: A report of the American College of Cardiology/American
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
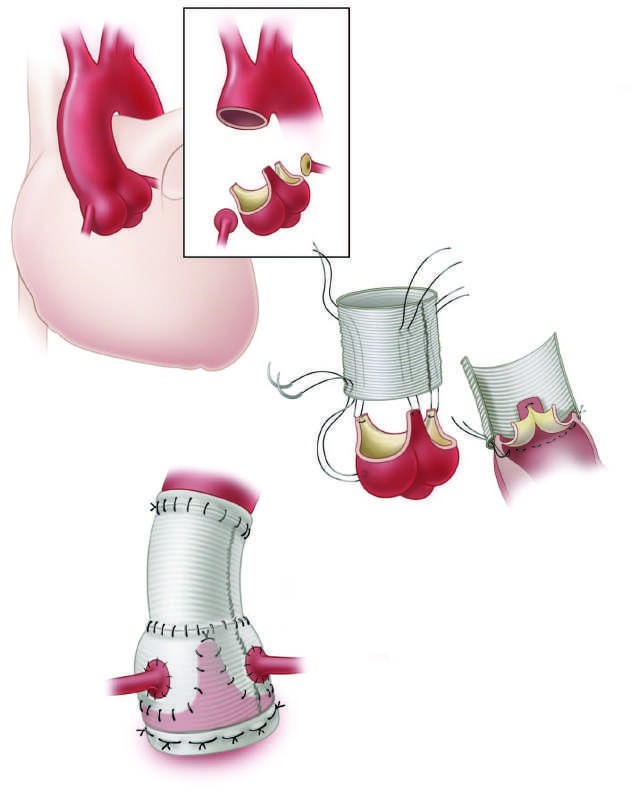
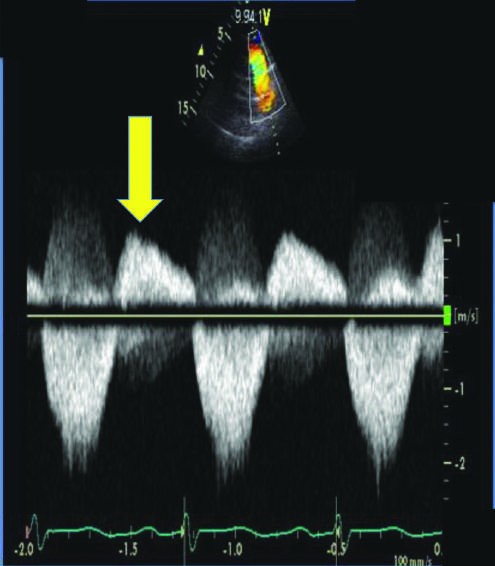
Caption: FIGURE 273-3 Valve-sparing aortic root reconstruction (David procedure). Aortic root mobilized coronary artery buttons remaining. Subannular sutures (C) are placed, through the proximal end of the graft. The annular sutures are tied (D), the valve is appropriate size, and the coronary buttons are attached to the side of the graft. (From P Disease, 3rd ed, Fig. 12-27, p. 200.) — Figure 273-1: Echocardiographic and Doppler depiction of severe aortic regurgitation. (A) Color flow transesophageal echocardiographic long axis image in diastole shows a broad jet of severe aortic regurgitation (AR, yellow arrow) directed into the left ventricle. (B) Continuous wave Doppler tracing obtained from the suprasternal window shows dense, holodiastolic flow reversal in the descending thoracic aorta indicative of severe AR.
Figure 2¶

Caption: FIGURE 273-1 Echocardiographic and Doppler depiction of severe aortic shows a broad jet of severe aortic regurgitation (AR, yellow arrow) directed into the left LV, left ventricle. (B) Continuous wave Doppler tracing (middle image) obtained from the dense, holodiastolic flow reversal in the descending thoracic aorta (yellow arrow) Chest X-Ray In chronic severe AR, the apex is displaced down- ward and to the left in the frontal projection. In the left anterior oblique and lateral projections, the LV is displaced posteriorly and encroaches on the spine. When AR is caused by primary disease of the aortic root, aneurysmal dilation of the aorta may be noted, and — Figure 273-2: Management of patients with aortic regurgitation. Algorithm showing indications for surgery based on symptoms, LV dysfunction (EF ≤55%), LV end-systolic dimension (LVESD >50 mm), and LV diastolic dimension (LVEDD >65 mm). Distinguishes between symptomatic (Stage D) and asymptomatic (Stage C) disease.
Figure 3¶
Caption: FIGURE 273-1 Echocardiographic and Doppler depiction of severe aortic shows a broad jet of severe aortic regurgitation (AR, yellow arrow) directed into the left LV, left ventricle. (B) Continuous wave Doppler tracing (middle image) obtained from the dense, holodiastolic flow reversal in the descending thoracic aorta (yellow arrow) Chest X-Ray In chronic severe AR, the apex is displaced down- ward and to the left in the frontal projection. In the left anterior oblique and lateral projections, the LV is displaced posteriorly and encroaches on the spine. When AR is caused by primary disease of the aortic root, aneurysmal dilation of the aorta may be noted, and — Figure 273-3: Valve-sparing aortic root reconstruction (David procedure). Diagram showing resection of aortic root and proximal ascending aorta, mobilization of coronary artery buttons, placement of subannular sutures, reimplantation of the valve inside a contoured graft, and reattachment of coronary buttons.
Figure 4¶
Caption: Figure 246-2C (referenced in text): Carotid arterial pulse bisferiens in aortic regurgitation. Diagram showing two systolic waves separated by a trough in the carotid arterial pulse, which may be seen in patients with AR or combined AS and AR.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.