Hypertension¶
Chapter 288 | Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Hypertension is defined as an average of three SBP or DBP readings at or above the 95th percentile or an SBP or DBP ≥130 or 80 mmHg in adults ≥18 years.
- Office BP measurements should be averaged from two or more readings at two or more visits to estimate the patient's usual level of BP.
- White coat hypertension (high office, normal out-of-office) has a CVD risk profile similar to normotensive individuals and may be treated with nonpharmacologic interventions.
- Masked hypertension (normal office, high out-of-office) has a CVD risk profile similar to sustained hypertension and requires pharmacologic therapy.
- Secondary hypertension should be considered in patients with new-onset hypertension, abrupt worsening, disproportionate target organ damage, or unprovoked hypokalemia.
- Obstructive sleep apnea (OSA) is the most common cause of secondary hypertension, associated with overweight, obesity, and sympathetic activation.
- The DASH diet can reduce SBP by ~5 mmHg in patients with hypertension and 2–3 mmHg in those without.
- Weight loss reduces SBP by ~1 mmHg per kilogram of weight loss.
- Reduction of sodium intake by ~25% can reduce SBP by ~5 mmHg.
- Potassium supplementation is contraindicated in patients with hyperkalemia or advanced kidney disease.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Blood Pressure Physiology and Pathophysiology
- 1.2 Blood Pressure Measurement
- 2. EPIDEMIOLOGY
- 2.1 Prevalence in the United States
- 2.2 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Primary Hypertension
- 3.2 Secondary Hypertension
- 4. CLINICAL FEATURES
- 4.1 Target Organ Damage
- 4.2 Complications
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Primary vs. Secondary Hypertension
- 5.2 Medication-Induced Hypertension
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Laboratory and Other Investigations
- 6.2 Diagnostic Criteria
- 7. MANAGEMENT & TREATMENT
- 7.1 Nonpharmacologic Interventions
- 7.2 Pharmacologic Treatment
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Cardiovascular Risk
- 8.2 Target Organ Damage
- 9. SPECIAL CONSIDERATIONS
- 9.1 White Coat and Masked Hypertension
- 9.2 Secondary Hypertension
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Clinical Traps
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Hypertension is a leading risk factor for cardiovascular disease (CVD), including ischemic and hemorrhagic stroke, coronary heart disease (CHD), heart failure (HF), peripheral arterial disease (PAD), chronic kidney disease (CKD)/end-stage kidney disease (ESKD), dementia, and all-cause mortality. It is very common no matter how it is defined and results in a huge burden due to death, morbidity, disability, social and workplace disruption, and cost to the individual and society. Hypertension is defined as an average of three SBP or DBP readings at or above the 95th percentile or an SBP or DBP ≥130 or 80 mmHg, respectively. This chapter is focused on BP in adults ≥18 years.
1.1 Blood Pressure Physiology and Pathophysiology¶
Complex and incompletely understood mechanisms control blood flow in individual organs and the arteriolar system. At the most basic level, arterial BP is controlled by cardiac output and peripheral resistance. However, arterial pressure is largely thought to be controlled by a renal-volume-endocrine pressure control system, in which the blood volume and total peripheral resistance are manipulated slowly to adjust arterial BP. Cardiac output is influenced by stroke volume and heart rate. Peripheral vascular resistance is determined by functional and anatomic changes in small arteries and arterioles. The vascular endothelium regulates exchanges between the bloodstream and surrounding tissues and controls vascular tone by synthesizing and releasing relaxing and contracting factors (e.g., nitric oxide, endothelin, angiotensin II). Endothelial dysfunction may play an important role in the initiation or progression of hypertension and atherosclerosis.
1.2 Blood Pressure Measurement¶
Commonly, BP measurements are used to estimate an individual's average level of BP, estimate their risk of CVD, determine the need for hypertension prevention or treatment. Office and clinic BP measurements are among the most common procedures in clinical practice. Correct classification presumes accurate BP measurement and averaging of two or more readings obtained at two or more occasions. When the SBP and DBP readings are in different categories of BP, the higher classification should be chosen. Errors in BP measurement are common in routine clinical practice. Generally, SBP is overestimated by an average of ~7 mmHg, which results in a 15–20% overestimation of hypertension prevalence. However, underestimation of BP and failure to diagnose hypertension are also common.
2. EPIDEMIOLOGY¶
Prevalence estimates vary depending on the criteria for definition of hypertension, the methods for BP measurement, and the population being studied; hypertension is very common, especially at older age. Age-related increases in BP are noted in almost all countries. Generally, SBP increases progressively until about the eighth decade of life. DBP also increases with age, but less steeply than SBP, until about the fifth decade of life and remains stable or declines thereafter. Isolated systolic hypertension is common late in life due to a widening of the pulse pressure (difference between SBP and DBP). Generally, those who have the highest or lowest BPs early in life tend to 'track' in the same extremes of BP over life, with high pressures early in life providing a crude opportunity to identify those at higher risk for hypertension in adulthood. Little or no age-related change in BP has been observed in many isolated populations and in subsets of populations in countries where age-related increases in BP are common.
2.1 Prevalence in the United States¶
Based on the ACC/AHA criteria for diagnosis, >103 million adults in the United States have hypertension, making it one of the most common health conditions reported. Hypertension is present in ~20–30% of U.S. adults aged 20–44 years, but the prevalence increases to 80–85% in those aged 75 years or older. The overall prevalence of hypertension in U.S. adults has remained fairly stable in recent decades (~46% overall). Men have slightly higher BPs compared to women during the first half of life, but the opposite is true in later life. In the United States, non-Hispanic black adults have a prevalence of hypertension (59%) that is substantially higher compared to whites (45%), Hispanics (47%), or Asians (46%). Adjusted estimates of hypertension in adult non-Hispanic black men and women are reported to be 59 and 56%, respectively, whereas the corresponding estimates for non-Hispanic white men and women are 47 and 41%, respectively. In addition, hypertension in non-Hispanic black adults tends to begin at a younger age and result in more CVD and kidney complications compared to the other major racial/ethnic groups in the United States. The prevalence of hypertension and CVD complications (especially stroke) is higher in the southeastern United States compared to other regions of the country, especially the northwest.
2.2 Risk Factors¶
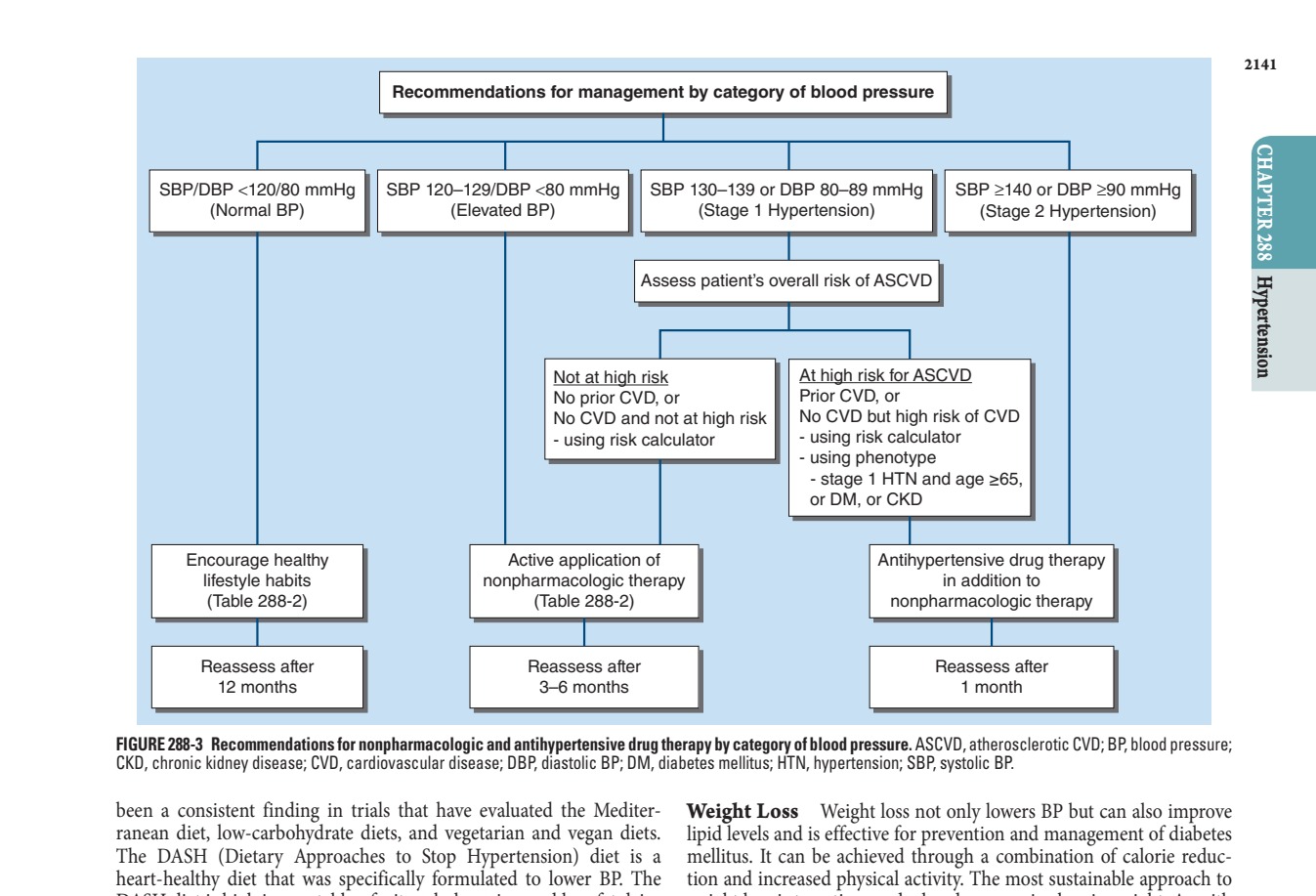
Hypertension is often associated with other CVD risk factors, resulting in a higher risk of complications and related burden of illness. The BP-CVD risk association in observational studies is equally true for men and women. The BP-related slope for relative risk of CVD is steeper at younger age when BP elevation is often an isolated risk predictor. In older adults, the corresponding slope for CVD risk is less steep, but the absolute risk of CVD is far higher because other CVD risk factors are common in those with an elevated BP. At any level of BP, the risk of a CVD complication varies dramatically with more than a 30-fold difference in 10-year predicted risk of CVD for those with an isolated elevation of BP compared to their counterparts with multiple CVD risk factors in addition to an elevated BP. This observation has special relevance for clinical decision-making in patients with a usual SBP between 130 and 139 mmHg. In individuals with stage 1 hypertension as an isolated CVD risk factor, the 5- or 10-year risk of a CVD event may be quite small and limit enthusiasm for introducing antihypertensive drug therapy. However, when stage 1 hypertension is accompanied by other CVD risk factors, the corresponding risk of ASCVD may be quite high and make prescription of antihypertensive drug therapy much more appealing. In antihypertensive clinical trials, the relative risk reductions for CVD events are similar in groups with different levels of underlying CVD risk, but the absolute benefit is much greater in the groups at higher risk for ASCVD. For both these reasons, CVD risk assessment should be part of the initial evaluation.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Most adults have 'primary' hypertension, with no obvious underlying anatomic cause of their high BP. Adoption, twin, clinical, and family studies provide evidence for a heritable component of high BP and hypertension. However, much of this may be due to a shared environment because, with rare exceptions, genetic investigations have only identified modest polygenic associations between multiple genes and BP. While genetic research remains an important area for investigation, the clinical implications of genetic studies for diagnosis and management of high BP are currently very limited. A minority of patients have 'secondary' hypertension, with an overt underlying anatomic or biochemical cause for their high BP. Secondary hypertension should be considered during the evaluation of all patients with new-onset hypertension and in selected patients with prevalent hypertension who have indicators that suggest the possibility of a complicating secondary cause of hypertension, including (1) treatment-resistant hypertension; (2) abrupt worsening of hypertension; (3) disproportionate target organ damage for level of BP; and (4) laboratory or diagnostic findings such as unprovoked hypokalemia, proteinuria, or left ventricular hypertrophy.
3.1 Primary Hypertension¶
Primary hypertension is the most common form, with no obvious underlying anatomic cause. It is associated with a heritable component and shared environment. Genetic investigations have only identified modest polygenic associations between multiple genes and BP. The clinical implications of genetic studies for diagnosis and management of high BP are currently very limited.
3.2 Secondary Hypertension¶
Secondary hypertension should be considered during the evaluation of all patients with new-onset hypertension and in selected patients with prevalent hypertension who have indicators that suggest the possibility of a complicating secondary cause of hypertension, including (1) treatment-resistant hypertension; (2) abrupt worsening of hypertension; (3) disproportionate target organ damage for level of BP; and (4) laboratory or diagnostic findings such as unprovoked hypokalemia, proteinuria, or left ventricular hypertrophy.
4. CLINICAL FEATURES¶
Hypertension is often asymptomatic. Symptoms, when present, are usually related to end-organ damage or secondary causes. Common clinical indicators of OSA include snoring, poor quality sleep, breathing pauses during sleep, and daytime sleepiness. Patients with white coat hypertension have a CVD risk profile that is more like those without than those with sustained high BPs in and out of the office. Adults with masked hypertension have a CVD risk profile that is like those with sustained hypertension. Hypertension is very common in all parts of the world, with a progressively increasing prevalence in low- and middle-income countries and a slight decline in high-income countries.
4.1 Target Organ Damage¶
Hypertension is associated with target organ damage, including left ventricular hypertrophy, proteinuria, and retinopathy. Masked hypertension should be suspected especially in adults with an elevated but nonhypertensive office BP and evidence of end-organ damage such as left ventricular hypertrophy or proteinuria. Patients with a history of a prior CVD complication are known to be at high risk for recurrent CVD events. In those without a history of prior CVD, ASCVD risk should be estimated using a risk calculator.
4.2 Complications¶
Hypertension is a leading risk factor for cardiovascular disease (CVD), including ischemic and hemorrhagic stroke, coronary heart disease (CHD), heart failure (HF), peripheral arterial disease (PAD), chronic kidney disease (CKD)/end-stage kidney disease (ESKD), dementia, and all-cause mortality. The BP-CVD risk association in observational studies is equally true for men and women. The BP-related slope for relative risk of CVD is steeper at younger age when BP elevation is often an isolated risk predictor. In older adults, the corresponding slope for CVD risk is less steep, but the absolute risk of CVD is far higher because other CVD risk factors are common in those with an elevated BP. At any level of BP, the risk of a CVD complication varies dramatically with more than a 30-fold difference in 10-year predicted risk of CVD for those with an isolated elevation of BP compared to their counterparts with multiple CVD risk factors in addition to an elevated BP.
5. DIFFERENTIAL DIAGNOSIS¶
The differential diagnosis of hypertension includes primary hypertension and secondary hypertension. Secondary hypertension should be considered in patients with new-onset hypertension, abrupt worsening of hypertension, disproportionate target organ damage for level of BP, or laboratory or diagnostic findings such as unprovoked hypokalemia, proteinuria, or left ventricular hypertrophy. Common causes of secondary hypertension include obstructive sleep apnea (OSA), renal artery stenosis, primary aldosteronism, pheochromocytoma, Cushing syndrome, and thyroid disorders. Medication-induced hypertension is also a common cause.
5.1 Primary vs. Secondary Hypertension¶
Most adults have 'primary' hypertension, with no obvious underlying anatomic cause of their high BP. A minority of patients have 'secondary' hypertension, with an overt underlying anatomic or biochemical cause for their high BP. Secondary hypertension should be considered during the evaluation of all patients with new-onset hypertension and in selected patients with prevalent hypertension who have indicators that suggest the possibility of a complicating secondary cause of hypertension, including (1) treatment-resistant hypertension; (2) abrupt worsening of hypertension; (3) disproportionate target organ damage for level of BP; and (4) laboratory or diagnostic findings such as unprovoked hypokalemia, proteinuria, or left ventricular hypertrophy.
5.2 Medication-Induced Hypertension¶
Prescription and over-the-counter medications, herbal and food additives, and illegal substances are often identified as secondary causes of new-onset hypertension or diminished BP control in patients being treated for hypertension. Typically, the increase in BP results from a direct pressor effect of the agents, but these exposures can also have an indirect effect on BP as a result of drug-drug or drug-nondrug exposure interactions. Some of the most common prescription drugs that can increase BP include amphetamines, angiogenesis inhibitors, antidepressants and antipsychotic agents, decongestants, oral contraceptives, nonsteroidal anti-inflammatory drugs (NSAIDs), and systemic corticosteroids. Examples of illicit drugs that can result in a higher BP include cocaine, marijuana, amphetamines, and methylenedioxymethamphetamine. Herbal treatments that have been reported to raise BP include arnica, ephedra (Ma-Huang), ginseng, guarana, consumption of large quantities of licorice, and St. John's wort. Finally, caffeine and several anesthetic agents can result in short-term elevation of BP.
6. INVESTIGATIONS & DIAGNOSIS¶
In patients with newly diagnosed hypertension, basic laboratory testing is indicated to (1) recognize the presence and extent of target organ damage; (2) facilitate the identification of secondary causes of hypertension, including kidney disease and primary aldosteronism; (3) recognize comorbid conditions, including diabetes mellitus and hyperlipidemia; (4) estimate atherosclerotic CVD (ASCVD) risk in patients without a history of a CVD; and (5) assist in the optimal choice of antihypertensive drug therapy. At a minimum, a complete blood count, serum electrolytes (sodium, potassium, calcium), serum creatinine and estimated GFR (eGFR), lipid profile, glycemic status (hemoglobin A1c or fasting blood glucose), thyroid-stimulating hormone level, urinalysis and urine albumin-to-creatinine ratio, and 12-lead electrocardiogram (ECG) should be obtained. These basic tests can be complemented by other evaluations as clinically indicated. In some countries, it is not possible to obtain the minimally recommended laboratory results. Guidelines written for clinicians in such countries, including the 2021 World Health Organization (WHO) guideline for the treatment of hypertension in adults, recommend that this should not be an impediment to BP reduction.
6.1 Laboratory and Other Investigations¶
In patients with newly diagnosed hypertension, basic laboratory testing is indicated to (1) recognize the presence and extent of target organ damage; (2) facilitate the identification of secondary causes of hypertension, including kidney disease and primary aldosteronism; (3) recognize comorbid conditions, including diabetes mellitus and hyperlipidemia; (4) estimate atherosclerotic CVD (ASCVD) risk in patients without a history of a CVD; and (5) assist in the optimal choice of antihypertensive drug therapy. At a minimum, a complete blood count, serum electrolytes (sodium, potassium, calcium), serum creatinine and estimated GFR (eGFR), lipid profile, glycemic status (hemoglobin A1c or fasting blood glucose), thyroid-stimulating hormone level, urinalysis and urine albumin-to-creatinine ratio, and 12-lead electrocardiogram (ECG) should be obtained. These basic tests can be complemented by other evaluations as clinically indicated. In some countries, it is not possible to obtain the minimally recommended laboratory results. Guidelines written for clinicians in such countries, including the 2021 World Health Organization (WHO) guideline for the treatment of hypertension in adults, recommend that this should not be an impediment to BP reduction.
6.2 Diagnostic Criteria¶
Hypertension is defined as an average of three SBP or DBP readings at or above the 95th percentile or an SBP or DBP ≥130 or 80 mmHg, respectively. This chapter is focused on BP in adults ≥18 years. Correct classification presumes accurate BP measurement and averaging of two or more readings obtained at two or more occasions. When the SBP and DBP readings are in different categories of BP, the higher classification should be chosen. In children and adolescents <13 years of age, hypertension is generally based on a comparison with age-, sex-, and height-specific normative data.
7. MANAGEMENT & TREATMENT¶
The optimal approach to high BP is to prevent its development, but diagnosis, treatment, and control of hypertension also provide an effective means to reduce the risk of BP-related CVD. Unfortunately, both strategies are poorly implemented worldwide, resulting in a high burden of preventable disease. Most guidelines recommend using an average of two to three measurements obtained in the morning (before taking antihypertensive medications) and evening. In the United States, obtaining home BP measurements for about 3 days prior to an office visit represents a reasonable and practical option for estimating a patient's usual level of home BP. The BP for recognition of hypertension is the same for office and home BP measurements (SBP ≥130 and DBP ≥80 mmHg). Likewise, the BP control is defined as an SBP/DBP <130/80 mmHg in both settings. Many home BP measurement devices allow for storage of the readings on a memory chip and for transfer to the physician's office by use of telemetry. This approach thwarts the potential for bias of more favorable readings that can occur with written patient self-reports. Ambulatory BP measurements are best obtained by practitioners with special expertise in this technique and interpretation and of the results. The equivalent SBP/DBP readings for an office average of 130/80 mmHg are 130/80, 110/65, and 125/75 mmHg for daytime, nighttime, and 24-h ambulatory readings, respectively. Ambulatory BP measurement is relatively expensive and intrusive. Patients in the United States are usually reluctant to undergo repeat ambulatory BP measurements, making this measurement method most useful in confirming the diagnosis of hypertension, especially where uncertainty is a special concern.
7.1 Nonpharmacologic Interventions¶
Nonpharmacologic interventions are the foundation of hypertension management. The six best proven nonpharmacologic interventions that lower blood pressure include diet (DASH diet), body weight reduction, sodium intake reduction, potassium intake increase, physical activity, and alcohol reduction. These interventions are highly prevalent and strongly associated with higher BP and age-related increases in BP. About half of U.S. adults report attempts to eat a heart healthy diet, but this is likely to represent an overestimate. Almost all adults worldwide exceed the intake of dietary sodium and fail to meet the level of dietary potassium recommended by the WHO and national organizations. Likewise, excess body weight is very common in many countries. For example, approximately three-quarters of U.S. adults are either overweight (body mass index [BMI] 25–29 kg/m2) or obese (BMI ≥30 kg/m2). More than a quarter of U.S. adults report no physical activity outside their workplace, and about half report less than the recommended level of physical activity (≥150 min of aerobic exercise/week). About 85% of U.S. adults report consumption of alcohol at some point during their life, with >60% reporting alcohol consumption during the previous year and 25% reporting binge drinking during the previous month. Thus, these six exposures are not only closely related to level of BP and targets for interventions aimed at BP lowering but also extremely common exposures.
7.2 Pharmacologic Treatment¶
Many of the drugs used to manage high BP work through influences on the various BP control mechanisms. Direct vasodilators and calcium channel blockers (CCBs) work by inducing arteriolar vasodilation. Agents that block the RAAS (ACEIs, ARBs, renin inhibitors) act by blocking the vasoconstricting effects of angiotensin II and sodium-retaining effects of aldosterone. ACEIs also inhibit inactivation of the vasodilator bradykinin, resulting in angioedema in some patients. Beta blockers tend to affect BP by impairing the action of sympathetic system neurotransmitters that stimulate vasoconstriction and heart rate. Thiazide and thiazide-like diuretics work to enhance sodium excretion in the distal convoluted tubule and are a mainstay of drug therapy for BP control. Loop diuretics are more potent diuretics that produce sodium excretion in the loop of Henle. Mineralocorticoid receptor antagonists (MRAs) work in the distal tubule to antagonize the action of aldosterone. Carbonic anhydrase inhibitors have a diuretic effect in the proximal tubules, but due to side effects and diminishing efficacy over time, they are rarely used for BP control.
8. PROGNOSIS & COMPLICATIONS¶
Hypertension is a leading risk factor for cardiovascular disease (CVD), including ischemic and hemorrhagic stroke, coronary heart disease (CHD), heart failure (HF), peripheral arterial disease (PAD), chronic kidney disease (CKD)/end-stage kidney disease (ESKD), dementia, and all-cause mortality. The BP-CVD risk association in observational studies is equally true for men and women. The BP-related slope for relative risk of CVD is steeper at younger age when BP elevation is often an isolated risk predictor. In older adults, the corresponding slope for CVD risk is less steep, but the absolute risk of CVD is far higher because other CVD risk factors are common in those with an elevated BP. At any level of BP, the risk of a CVD complication varies dramatically with more than a 30-fold difference in 10-year predicted risk of CVD for those with an isolated elevation of BP compared to their counterparts with multiple CVD risk factors in addition to an elevated BP. This observation has special relevance for clinical decision-making in patients with a usual SBP between 130 and 139 mmHg. In individuals with stage 1 hypertension as an isolated CVD risk factor, the 5- or 10-year risk of a CVD event may be quite small and limit enthusiasm for introducing antihypertensive drug therapy. However, when stage 1 hypertension is accompanied by other CVD risk factors, the corresponding risk of ASCVD may be quite high and make prescription of antihypertensive drug therapy much more appealing. In antihypertensive clinical trials, the relative risk reductions for CVD events are similar in groups with different levels of underlying CVD risk, but the absolute benefit is much greater in the groups at higher risk for ASCVD. For both these reasons, CVD risk assessment should be part of the initial evaluation.
8.1 Cardiovascular Risk¶
Hypertension is a leading risk factor for cardiovascular disease (CVD), including ischemic and hemorrhagic stroke, coronary heart disease (CHD), heart failure (HF), peripheral arterial disease (PAD), chronic kidney disease (CKD)/end-stage kidney disease (ESKD), dementia, and all-cause mortality. The BP-CVD risk association in observational studies is equally true for men and women. The BP-related slope for relative risk of CVD is steeper at younger age when BP elevation is often an isolated risk predictor. In older adults, the corresponding slope for CVD risk is less steep, but the absolute risk of CVD is far higher because other CVD risk factors are common in those with an elevated BP. At any level of BP, the risk of a CVD complication varies dramatically with more than a 30-fold difference in 10-year predicted risk of CVD for those with an isolated elevation of BP compared to their counterparts with multiple CVD risk factors in addition to an elevated BP. This observation has special relevance for clinical decision-making in patients with a usual SBP between 130 and 139 mmHg. In individuals with stage 1 hypertension as an isolated CVD risk factor, the 5- or 10-year risk of a CVD event may be quite small and limit enthusiasm for introducing antihypertensive drug therapy. However, when stage 1 hypertension is accompanied by other CVD risk factors, the corresponding risk of ASCVD may be quite high and make prescription of antihypertensive drug therapy much more appealing. In antihypertensive clinical trials, the relative risk reductions for CVD events are similar in groups with different levels of underlying CVD risk, but the absolute benefit is much greater in the groups at higher risk for ASCVD. For both these reasons, CVD risk assessment should be part of the initial evaluation.
8.2 Target Organ Damage¶
Masked hypertension should be suspected especially in adults with an elevated but nonhypertensive office BP and evidence of end-organ damage such as left ventricular hypertrophy or proteinuria. Patients with a history of a prior CVD complication are known to be at high risk for recurrent CVD events. In those without a history of prior CVD, ASCVD risk should be estimated using a risk calculator.
9. SPECIAL CONSIDERATIONS¶
Hypertension is very common in all parts of the world, with a progressively increasing prevalence in low- and middle-income countries and a slight decline in high-income countries. As in the United States, hypertension prevalence is very age-dependent and varies by region, race/ethnicity, and other factors, including importantly socioeconomic factors, in most countries. No matter how defined, hypertension is very common in all parts of the world, with a progressively increasing prevalence in low- and middle-income countries and a slight decline in high-income countries. Using the hypertension definition of SBP ≥140 mmHg, DBP ≥90 mmHg, or taking antihypertensive medication, the prevalence in adults was estimated to be 31.5% (1.04 billion) in low- and middle-income countries and 28.5% (349 million) in high-income countries in 2010. As in the United States, hypertension prevalence is very age-dependent and varies by region, race/ethnicity, and other factors, including importantly socioeconomic factors, in most countries.
9.1 White Coat and Masked Hypertension¶
White coat hypertension, in which office BPs meet the criteria for hypertension but out-of-office BPs are nonhypertensive, and masked hypertension, in which office BPs are nonhypertensive but out-of-office BPs meet the criteria for hypertension, are common, with prevalence estimates of 15–25% for both conditions. Adults with white coat hypertension have a CVD risk profile that is more like those without than those with sustained high BPs in and out of the office and they may be best treated with nonpharmacologic interventions, with careful monitoring to recognize a transition to sustained hypertension. In contrast, adults with masked hypertension have a CVD risk profile that is like those with sustained hypertension and may be better treated with a combination of antihypertensive drugs in addition to nonpharmacologic therapy. Masked hypertension should be suspected especially in adults with an elevated but nonhypertensive office BP and evidence of end-organ damage such as left ventricular hypertrophy or proteinuria.
9.2 Secondary Hypertension¶
A minority of patients have 'secondary' hypertension, with an overt underlying anatomic or biochemical cause for their high BP. Secondary hypertension should be considered during the evaluation of all patients with new-onset hypertension and in selected patients with prevalent hypertension who have indicators that suggest the possibility of a complicating secondary cause of hypertension, including (1) treatment-resistant hypertension; (2) abrupt worsening of hypertension; (3) disproportionate target organ damage for level of BP; and (4) laboratory or diagnostic findings such as unprovoked hypokalemia, proteinuria, or left ventricular hypertrophy. Obstructive sleep apnea (OSA) is probably the most common cause of secondary hypertension. It is closely associated with overweight, obesity, and other comorbidities. The reported prevalence of OSA varies substantially depending on the criteria used for definition and methods of ascertainment. However, it is very common and may be present in as many as 15–30% of adult men and 10–15% of adult women in the United States. More than half of U.S. adults with OSA have hypertension and >30% of U.S. adults with hypertension have OSA. OSA and hypertension share many common pathophysiologic features, including being overweight, obesity, unhealthy lifestyles, and abnormalities of the renin-angiotensin system and fluid distribution. Sympathetic system activation due to intermittent hypoxia is also an important component of the underlying pathophysiology in OSA. Almost three-quarters of patients with OSA are overweight or obese. In general, there is a direct association between the severity of OSA and an individual's level of BP as well as their resistance to antihypertensive therapy. Resistant hypertension, snoring, poor quality sleep, breathing pauses during sleep, and daytime sleepiness are common clinical indicators of OSA. Several simple questionnaire-based tests are available to screen for those who should be evaluated more carefully with a sleep study (polysomnography). Lifestyle improvements, especially those resulting in weight loss, are an important component of treatment for both OSA and any associated hypertension. OSA-specific treatment includes continuous positive airway pressure (CPAP), but meta-analyses demonstrate limited BP lowering due to CPAP treatment. As a result, hypertension in patients with OSA should be treated with antihypertensive drug therapy in addition to nonpharmacologic therapy. Prescription and over-the-counter medications, herbal and food additives, and illegal substances are often identified as secondary causes of new-onset hypertension or diminished BP control in patients being treated for hypertension. Typically, the increase in BP results from a direct pressor effect of the agents, but these exposures can also have an indirect effect on BP as a result of drug-drug or drug-nondrug exposure interactions. Some of the most common prescription drugs that can increase BP include amphetamines, angiogenesis inhibitors, antidepressants and antipsychotic agents, decongestants, oral contraceptives, nonsteroidal anti-inflammatory drugs (NSAIDs), and systemic corticosteroids. Examples of illicit drugs that can result in a higher BP include cocaine, marijuana, amphetamines, and methylenedioxymethamphetamine. Herbal treatments that have been reported to raise BP include arnica, ephedra (Ma-Huang), ginseng, guarana, consumption of large quantities of licorice, and St. John's wort. Finally, caffeine and several anesthetic agents can result in short-term elevation of BP. A careful history will identify most of these agents and will allow for use of alternatives or a reduced dosage in most patients. The exact prevalence of exposure to any of these agents is uncertain but high. For example, in the nationally representative 1999–2004 National Health and Nutrition Examination Survey (NHANES), >26% of U.S. adults reported regular NSAID use, and the percentage was much higher in older adults and non-Hispanic whites.
10. KEY PEARLS & CLINICAL TRAPS¶
Hypertension is often asymptomatic. Symptoms, when present, are usually related to end-organ damage or secondary causes. Common clinical indicators of OSA include snoring, poor quality sleep, breathing pauses during sleep, and daytime sleepiness. Patients with white coat hypertension have a CVD risk profile that is more like those without than those with sustained high BPs in and out of the office. Adults with masked hypertension have a CVD risk profile that is like those with sustained hypertension. Hypertension is very common in all parts of the world, with a progressively increasing prevalence in low- and middle-income countries and a slight decline in high-income countries.
10.1 Diagnostic Clues¶
Masked hypertension should be suspected especially in adults with an elevated but nonhypertensive office BP and evidence of end-organ damage such as left ventricular hypertrophy or proteinuria. Resistant hypertension, snoring, poor quality sleep, breathing pauses during sleep, and daytime sleepiness are common clinical indicators of OSA. Several simple questionnaire-based tests are available to screen for those who should be evaluated more carefully with a sleep study (polysomnography).
10.2 Clinical Traps¶
Errors in BP measurement are common in routine clinical practice. Generally, SBP is overestimated by an average of ~7 mmHg, which results in a 15–20% overestimation of hypertension prevalence. However, underestimation of BP and failure to diagnose hypertension are also common. No talking during rest period and between measurements. Apply the cuff to bare upper arm, approximately 2–3 cm above the elbow crease. Arm bare and resting. Mid-arm at heart level. Back supported. Feet flat on floor. Having a trained non-physician staff member obtain routine BP measurements provides an efficient and cost-effective means of obtaining high-quality observations. This is the common practice in research studies and in many large U.S. systems of care.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶

Caption: FIGURE 288-5 Confirmation and management of resistant hypertension. BP, blood OSA, obstructive sleep apnea; SBP, systolic blood pressure.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
Caption: FIGURE 288-3 Recommendations for nonpharmacologic and antihypertensive drug CKD, chronic kidney disease; CVD, cardiovascular disease; DBP, diastolic BP; DM, been a consistent finding in trials that have evaluated the Mediter- ranean diet, low-carbohydrate diets, and vegetarian and vegan diets. The DASH (Dietary Approaches to Stop Hypertension) diet is a heart-healthy diet that was specifically formulated to lower BP. The DASH diet is high in vegetables, fruits, whole grains, and low-fat dairy products and low in fats, saturated fats, and cholesterol. It has been extensively evaluated, and many DASH resources and support systems — FIGURE 288-1: Schematic depiction of factors that influence the control of blood pressure, illustrating the interplay between cardiac output, peripheral resistance, renal-volume-endocrine pressure control systems, and neural/hormonal systems (e.g., sympathetic, RAAS).
Figure 2¶
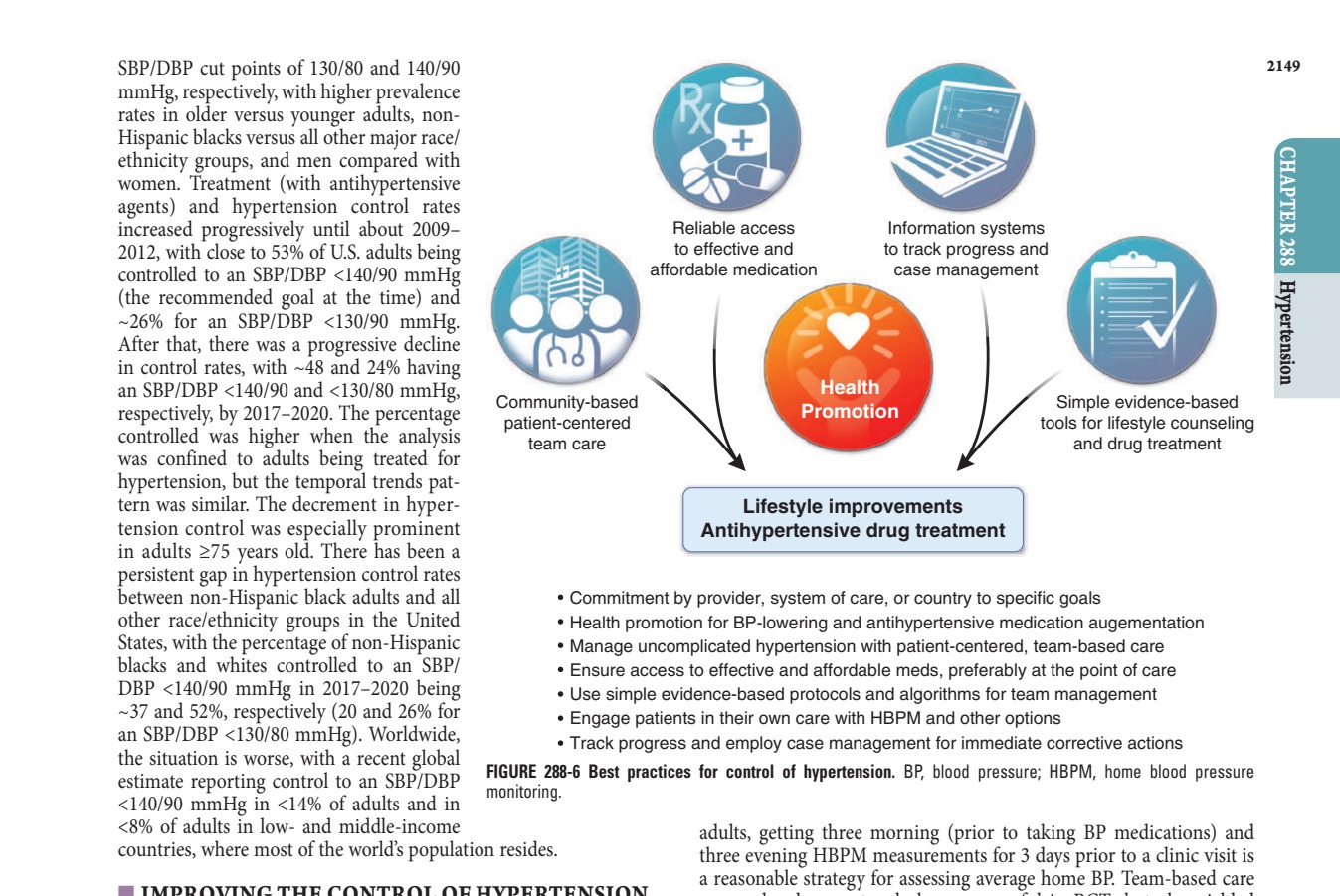
Caption: FIGURE 288-6 Best practices for control of hypertension. BP, blood pressure; monitoring. in adults, getting three morning (prior to taking resides. three evening HBPM measurements for 3 days a reasonable strategy for assessing average HYPERTENSION approaches have not only been successful in rates are unacceptable, and excellent results in clinical practice settings, care for hyper- Northern California reporting an improvement — FIGURE 288-2: Schematic depiction of the important elements for accurate measurement of office blood pressure, including patient positioning (seated, back supported, feet flat), cuff placement (bare arm, mid-brachial level, heart level), and rest period requirements.
Figure 3¶

Caption: FIGURE 288-4 Overview of specific antihypertensive treatments in adults with angiotensin receptor blocker; BP, blood pressure; CCB, calcium channel blocker; DASH, receptor antagonists; SBP, systolic BP. — FIGURE 288-3: Likely depicts the pathophysiology of secondary hypertension or common causes (e.g., renal artery stenosis, pheochromocytoma, primary aldosteronism) based on the text discussion on secondary causes.
Figure 4¶

Caption: FIGURE 288-2 Schematic depiction of the important elements for accurate measurement blood pressure. (Reproduced with permission from AK Cheung et al: International standardized clinic blood pressure measurement: A call to action. Am J Med 136:438, — FIGURE 288-4: Likely depicts target organ damage associated with hypertension (e.g., left ventricular hypertrophy, retinopathy, nephropathy) or the impact of nonpharmacologic interventions on BP.
Figure 5¶
Caption: Hypertension 288 FIGURE 288-1 Schematic depiction of factors that influence the control of blood pressure. handling, primarily by the kidney, and many neural and hormonal systems that influence peripheral resistance by stimulating vascular constriction (e.g., the sympathetic system and the renin-angiotensin- aldosterone system [RAAS]) or inducing vasodilation (e.g., bradykinin system), and by modulating hormones that result in excretion or reten- tion of sodium (natriuretic peptides and aldosterone, respectively). Most vascular beds have the capacity to autoregulate blood flow. — FIGURE 288-5: Likely depicts the management algorithm for hypertension, including risk stratification, drug selection, and monitoring of target organ damage.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.