Enterococcal Infections¶
Chapter 154 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Enterococci are the third most common isolates from hospital-associated infections in the US, after E. coli and staphylococci.
- E. faecium is the most resistant species; >90% of E. faecium isolates are resistant to ampicillin, and vancomycin resistance ranges from 50–70% in acute care hospitals.
- Synergistic bactericidal activity is achieved by combining a cell-wall active agent (β-lactam or glycopeptide) with an aminoglycoside (gentamicin or streptomycin).
- Linezolid is the only FDA-approved agent for VRE infections but is not bactericidal and carries risks of thrombocytopenia, peripheral neuropathy, and optic neuritis with prolonged use.
- Daptomycin is bactericidal against all enterococci but requires high-dose regimens (8–12 mg/kg) for E. faecium with MIC ≤4 mg/L.
- Enterococcal endocarditis typically presents subacutely; valve replacement may be critical for curing infection caused by multidrug-resistant organisms.
- VRE colonization of the GI tract is a critical step in disease development; patients remain colonized for prolonged periods (sometimes >1 year).
- Cephalosporins are not active as monotherapy against enterococci; ampicillin and amoxicillin are the most active β-lactams.
- Intraabdominal infections in hospitalized patients are increasingly caused by vancomycin-resistant E. faecium, leading to treatment failures.
- Enterococcal meningitis is uncommon (~4% of cases) and associated with neurosurgical interventions or hematogenous seeding from endocarditis.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Microbiology and Taxonomy
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors for VRE Colonization
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Resistance Mechanisms
- 4. CLINICAL FEATURES
- 4.1 Clinical Syndromes
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Colonization vs. Infection
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria
- 7. MANAGEMENT & TREATMENT
- 7.1 Therapeutic Regimens
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Mortality and Relapse
- 9. SPECIAL CONSIDERATIONS
- 9.1 Neonatal and Immunocompromised Hosts
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Board Exam Favorites
- 11. WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- 11.1 Specific Findings
- 12. WHAT EXCLUDES THE DIAGNOSIS
- 12.1 Exclusion Criteria
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | CHAPTER 154 FIGURE 154-1 Gram’s stain of cultured blood from a patient... |
1. DEFINITION & OVERVIEW¶
- Enterococci have been recognized as potential human pathogens for well over a century, but only in recent years have these organisms acquired prominence as important causes of nosocomial infections.
- Enterococci are gram-positive organisms observed as single cells, diplococci, or short chains in clinical specimens.
- Harrison's defines the genus as distinct from streptococci based on DNA hybridization studies and 16S rRNA sequencing.
- Unlike the majority of streptococci, enterococci hydrolyze esculin in the presence of 40% bile salts and grow at high salt concentrations (e.g., 6.5%) and at high temperatures (46°C).
- Enterococci are usually reported by the clinical laboratory to be nonhemolytic on the basis of their inability to lyse the ovine or bovine red blood cells (RBCs) commonly used in agar plates; however, some strains of E. faecalis do lyse RBCs from humans, horses, and rabbits due to the presence of an acquired hemolysin/cytolysin gene.
- The majority of clinically relevant enterococcal species hydrolyze pyrrolidonyl-β-naphthylamide (PYR).
- Enterococci were first mentioned in the French literature in 1899; the first pathologic description of an enterococcal infection dates to the same year.
- A clinical isolate from a patient who died as a consequence of endocarditis was initially designated Micrococcus zymogenes, was later named Streptococcus faecalis subspecies zymogenes, and would now be classified as Enterococcus faecalis.
- Although many species of enterococci have been isolated from human infections, the overwhelming majority of cases are caused by two species, E. faecalis and E. faecium.
- Less frequently isolated species include Enterococcus gallinarum, E. durans, E. hirae, and E. avium.
1.1 Microbiology and Taxonomy¶
- Enterococci are gram-positive organisms.
- In clinical specimens, they are usually observed as single cells, diplococci, or short chains (Fig. 154-1), although long chains are noted with some strains.
- Enterococci were originally classified as streptococci because organisms of the two genera share many morphologic and phenotypic characteristics, including a generally negative catalase reaction.
- Only DNA hybridization studies and later 16S rRNA sequencing clearly demonstrated that enterococci should be grouped as a genus distinct from the streptococci.
- Unlike the majority of streptococci, enterococci hydrolyze esculin in the presence of 40% bile salts and grow at high salt concentrations (e.g., 6.5%) and at high temperatures (46°C).
- Enterococci are usually reported by the clinical laboratory to be nonhemolytic on the basis of their inability to lyse the ovine or bovine red blood cells (RBCs) commonly used in agar plates; however, some strains of E. faecalis do lyse RBCs from humans, horses, and rabbits due to the presence of an acquired hemolysin/cytolysin gene.
- The majority of clinically relevant enterococcal species hydrolyze pyrrolidonyl-β-naphthylamide (PYR).
2. EPIDEMIOLOGY¶
- According to data collected from 2018 to 2021 by the National Healthcare Safety Network of the Centers for Disease Control and Prevention, enterococci are the third most common isolates (after Escherichia coli and staphylococci) from hospital-associated infections in the United States.
- Although E. faecalis remains the predominant species recovered from nosocomial infections, the isolation of E. faecium has increased substantially in the past 20 years and accounts for approximately one-third of all enterococcal infections identified to the species level.
- E. faecium is by far the most resistant and challenging enterococcal species to treat.
- More than 90% of E. faecium isolates are resistant to ampicillin (historically the most effective β-lactam agent against enterococci), while ampicillin resistance in E. faecalis is uncommon.
- Vancomycin resistance in E. faecium isolates ranges from 50–70% in acute care hospitals in the United States to up to 80% in long-term care facilities.
- Resistance to vancomycin in E. faecalis isolates is less common, with a higher prevalence in long-term care facilities (10–12%) than in acute care hospitals (2–5%).
- In Europe, the emergence of VRE in the mid-1980s was seen primarily in isolates recovered from animals and healthy humans rather than from hospitalized patients.
- The presence of VRE was associated with the use of the glycopeptide avoparcin as a growth promoter in animal feeds; this association prompted the European Union to ban the use of this compound in animal husbandry in 1996.
- Despite regional differences, Europe has seen a general trend of increasing rates of VRE over the past decade, although these rates continue to be much lower than in the United States.
- Recent data have also shown increasing rates of enterococcal resistance to vancomycin in Latin American countries, with 34% of clinical E. faecium isolates found to be resistant in a multicenter study including hospitals from Colombia, Venezuela, Ecuador, and Peru.
- In Asia, rates of vancomycin resistance among enterococci appear to be similar to those in U.S. hospitals.
- The ability to sequence bacterial genomes has increased our understanding of bacterial diversity, evolution, pathogenesis, and mechanisms of antibiotic resistance.
- Ongoing collection of enterococcal isolates as a part of epidemiologic surveillance has allowed researchers to trace the evolutionary trajectory of enterococci from their origin to the emergence of hospital-adapted clones.
- Sequence analysis suggests the genus appeared ~400 million years ago with the advent of terrestrial animals.
- Several key features aided in this transition, including the ability to recombine large portions of chromosomal DNA from the core genome and a malleable accessory genome consisting of plasmids, phages, and mobile genetic elements.
- This genomic plasticity contributes to the rising rates of antibiotic resistance seen within the genus and, in particular, in E. faecium.
- A large proportion of the genomes available for analysis belong to E. faecium, due to its importance as a nosocomial pathogen and the ease of epidemiologic surveillance projects to track the spread of vancomycin-resistant strains.
- The population can be divided into two large groups, or clades, of organisms: a hospital-associated clade A and a community-associated clade B.
- The hospital-associated clade appears to be evolving rapidly via a series of historic and ongoing recombination events.
- Certain regions of the chromosome show a convergence of genomic diversity both within and between clades, suggesting there are several 'hot spots' for recombination.
- Importantly, these regions contain the polysaccharide biosynthesis cluster, which has been implicated in altering the antigenic capsular polysaccharide in streptococci.
- Strains belonging to clade A are more frequently identified as isolates causing invasive disease and are more likely to carry drug resistance determinants, whereas clade B isolates largely retain a susceptible phenotype.
- One reason for the propensity of clade A strains to acquire resistance determinants is that they more frequently lack a functional CRISPR-Cas system (short for clustered regularly interspaced short palindromic repeats).
- These systems serve as a primitive 'immune system' and provide a genome defense for bacteria to protect them from foreign DNA, such as phages, but they also serve to reduce the frequency of acquisition of resistance genes borne on mobile genetic elements.
- Another reason for their survival in the hospital environment is that clade A isolates tend to possess alleles of penicillin-binding protein 5 (PBP5) associated with high-level β-lactam resistance in E. faecium and may express higher levels of this enzyme than commensal strains.
- A notable feature of the distribution of strains in clade A in some studies is that they share a relatively recent common ancestor with E. faecium of livestock origin.
- Use of antibiotics in animal husbandry as both therapeutics and growth promoters has been linked to resistance in several important contexts, including glycopeptides, as mentioned above.
- This phenomenon suggests that continued surveillance, and an expanding understanding of the population structure of enterococci, may help identify potential reservoirs of resistance and inform policy to limit their spread.
2.1 Risk Factors for VRE Colonization¶
- Important factors associated with VRE colonization and persistence in the gut include:
- Prolonged hospitalization
- Long courses of antibiotic therapy
- Hospitalization in long-term care facilities, surgical units, and/or intensive care units
- Organ transplantation
- Renal failure (particularly in patients undergoing hemodialysis) and/or diabetes
- High APACHE (Acute Physiology and Chronic Health Evaluation) scores
- Physical proximity to patients infected or colonized with VRE or these patients' rooms
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Enterococci are normal inhabitants of the large bowel of human adults, although they usually make up <1% of the culturable intestinal microbiota.
- In the healthy human host, enterococci are typical symbionts that coexist with other gastrointestinal bacteria; in fact, the utility of certain enterococcal strains as probiotics in the treatment of diarrhea suggests their possible role in maintaining the homeostatic equilibrium of the bowel.
- These commensals play a role in colonization resistance, or the ability of a healthy gastrointestinal microbiota to impede the establishment of a population of drug-resistant bacteria such as vancomycin-resistant enterococci (VRE).
- Colonization resistance arises from a complex set of metabolic and immunologic interactions between the host, pathogen, and intestinal microbiota, many of which are disrupted in hospitalized or chronically ill patients.
- Physical factors, such as stomach pH and the mucin layer on the interior of the intestinal lumen, provide a barrier and limit pathogen access to the intestinal epithelium.
- In the hospital setting, administration of medications that suppress stomach acid secretion, or degradation of the mucin layer by gut commensals during periods of decreased oral intake, can disrupt these protective layers.
- The availability of specific carbon sources also has been shown to influence the ability of enterococci to colonize the intestine.
- Depletion of fructose by members of the genus Olsenella leads to impaired growth and a decrease in the enteric burden of VRE in a mouse-colonization model, while the presence of lactose favors the outgrowth of enterococci.
- Furthermore, enterococci may potentiate the fitness and virulence of pathogens such as Clostridioides difficile by altering the availability of fermentable amino acids, by promoting C. difficile fitness, and by depletion of arginine, which leads to increased C. difficile toxin production.
- One of the most important factors that promotes increased gastrointestinal colonization by enterococci is the administration of antimicrobial agents since enterococci are intrinsically resistant to a variety of commonly used antibacterial drugs.
- In particular, antibiotics that are excreted in the bile and have broad-spectrum activity (e.g., certain cephalosporins and antimicrobials with anaerobic activity) are usually associated with the recovery of higher numbers of enterococci from feces.
- However, the increased colonization by hospital-associated strains of E. faecium in the presence of antimicrobial agents appears to be due to more than the simple filling of a 'biologic niche.'
- Studies of colonization dynamics in mouse intestines suggest host-derived antimicrobial peptides produced by the innate immune system (such as the lectin of RegIIIγ) and compounds such as lantibiotics or bacteriocins produced by members of the microbiota itself are important mediators of colonization resistance.
- Activation of Toll-like receptors by lipopolysaccharide (an important component of the gram-negative cell envelope) leads, in mice, to increased production of RegIIIγ, and loss of this stimulation by antibiotic-induced disruptions of commensal gram-negative bacteria impairs clearance of VRE from the intestines.
- Similarly, antimicrobial lantibiotics produced by commensal bacteria (such as Blautia producta) are active against VRE in vitro, but this organism may require a cooperative partnership with other members of the microbiota to effectively provide colonization resistance.
- Disruption of these partnerships by antibiotic administration can lead to an environment where VRE can flourish.
- Another factor that may contribute to enterococcal survival in the gastrointestinal tract is the production of bacteriocins (molecules that kill competing bacteria).
- Strains of E. faecalis harboring pheromone-producing plasmids that code for bacteriocins are capable of outcompeting enterococci lacking such plasmids, and conjugative transfer of these elements enhances the survival of recipient enterococci.
- In the absence of antibiotics, hospital-associated lineages of E. faecium seem to be less adapted for survival in the gastrointestinal tract than are commensal E. faecium strains.
- Studies examining the rate of carriage of VRE in patients after discharge from the hospital document a median time to clearance between 2 and 4 months in patients without ongoing risk factors, such as continued antibiotic use, residence in a long-term care facility, or need for hemodialysis.
- Colonization by enterococci may also have important effects on the treatment of noninfectious syndromes.
- In hematopoietic stem cell transplant patients, domination of the gastrointestinal tract by enterococci is associated with increased inflammation and a greater severity of illness and mortality in graft-versus-host disease.
- Certain enterococcal species, such as E. faecium, E. durans, and E. hirae, modulate the host immune response and can potentiate the activity of anti-PD-L1 immune checkpoint inhibitor therapy.
- This effect is mediated by the presence of salA, a gene which encodes a peptidoglycan hydrolase with D,L-endopeptidase activity.
- The muropeptides generated by SalA induce host activation of NF-κB via NOD2, leading to an enhanced antitumor immune response.
- Three main groups of virulence factors may increase the ability of enterococci to colonize the gastrointestinal tract and/or cause disease.
- The first group, enterococcal secreted factors, are molecules released outside the bacterial cell that contribute to the process of infection.
- The best studied of these molecules include enterococcal hemolysin/cytolysin and two enterococcal proteases (gelatinase and serine protease).
- Enterococcal cytolysin is a heterodimeric toxin produced by some strains of E. faecalis that is capable of lysing human (as well as equine but not ovine) RBCs as well as polymorphonuclear leukocytes and macrophages.
- A newly described pore-forming toxin, Epx, specifically targets human leukocyte antigen type 1, and has been shown to be active against peripheral blood mononuclear cells and intestinal organoids in vitro.
- E. faecalis gelatinase and serine protease are thought to mediate virulence by several mechanisms, including the degradation of host tissues and the modification of critical components of the immune system.
- Mutants lacking the genes corresponding to these proteins are highly attenuated in experimental animal models of peritonitis, endocarditis, and endophthalmitis.
- A second group of virulence factors, enterococcal surface components, includes adhesins and is thought to contribute to bacterial attachment to extracellular matrix molecules in the human host.
- Several molecules on the surface of enterococci have been characterized and shown to play a role in the pathogenesis of enterococcal infections.
- Among the adhesins is aggregation substance of E. faecalis, which mediates the attachment of bacterial cells to each other, thereby facilitating conjugative plasmid exchange.
- Several lines of evidence indicate that aggregation substance and enterococcal cytolysin act synergistically to increase the virulence potential of E. faecalis strains in experimental endocarditis.
- The surface protein adhesin of collagen of E. faecalis (Ace) and its E. faecium homologue (Acm) are microbial surface components adhering to matrix molecules (MSCRAMMs); they recognize adhesive matrix molecules involved in bacterial attachment to host proteins such as collagen, fibronectin, and fibrinogen.
- Both Ace and Acm are collagen adhesins that are important in the pathogenesis of experimental endocarditis.
- Pili of both E. faecalis and E. faecium are important mediators of attachment to and invasion of host tissues.
- Mutants of E. faecalis lacking pili are attenuated in biofilm production, experimental endocarditis, and urinary tract infections (UTIs).
- Other surface proteins that share structural homology with MSCRAMMs and appear to play a role in enterococcal attachment to the host and in virulence include the E. faecalis surface protein Esp and its E. faecium homologue Esp, the second collagen adhesin of E. faecium (Scm), the surface proteins of E. faecium (Fms), SgrA (which binds to components of the basal lamina), and EcbA (which binds to collagen type V).
- Additional surface components apparently associated with pathogenicity include the Erl protein (a protein from the WxL family) and polysaccharides, which are thought to interfere with phagocytosis of the organism by host immune cells.
- Teichoic acids on the enterococcal surface appear to be immunogenic, and antibodies to these molecules are protective in some animal models.
- The third group of virulence factors has not been well characterized but includes the E. faecalis stress protein Gls24, which has been associated with enterococcal resistance to bile salts and appears to be important in the pathogenesis of endocarditis, and the hyl-containing plasmids of E. faecium, which are transferable between strains and increase gastrointestinal colonization by E. faecium.
- In mouse peritoneitis, acquisition of these plasmids increased the lethality of a commensal strain of E. faecium and enhanced colonization of the uroepithelium.
- A gene encoding a regulator of oxidative stress (AsrR) has been identified as an important virulence factor of E. faecium.
3.1 Resistance Mechanisms¶
- Enterococci are intrinsically resistant and/or tolerant to several antimicrobial agents.
- Tolerance is defined as lack of killing by drug concentrations 32 times higher than the minimal inhibitory concentration (MIC).
- Monotherapy for endocarditis with a β-lactam antibiotic (to which many enterococci are tolerant) has produced disappointing results, with high relapse rates after the end of therapy.
- However, the addition of an aminoglycoside to a cell wall–active agent (a β-lactam or a glycopeptide) increases cure rates and eradicates the organisms; moreover, this combination is synergistic and bactericidal in vitro.
- Therefore, for many decades, combination therapy with a cell wall–active agent and an aminoglycoside was the standard of care for endovascular infections caused by enterococci.
- This synergistic effect can be explained, at least in part, by the increased penetration of the aminoglycoside into the bacterial cell, presumably as a result of cell-wall alterations produced by the β-lactam (or glycopeptide).
- Nonetheless, attaining synergistic bactericidal activity in the treatment of severe enterococcal infections—particularly those caused by E. faecium—has become increasingly difficult because of the development of resistance to virtually all antibiotics available for this purpose.
4. CLINICAL FEATURES¶
- Enterococci are well-known causes of nosocomial UTI—the most common infection caused by these organisms (Chap. 140).
- Enterococcal UTIs are usually associated with indwelling catheterization, instrumentation, or anatomic abnormalities of the genitourinary tract, and it is often challenging to differentiate between true infection and colonization (particularly in patients with chronic indwelling catheters).
- Their role as pathogens in otherwise healthy premenopausal woman with acute cystitis is less clear, with data from one study suggesting that enterococci recovered from midstream urine cultures were not predictive of bacteriuria in a subsequent catheterized specimen.
- The presence of leukocytes in the urine in conjunction with systemic manifestations (e.g., fever) or local signs and symptoms of infection with no other explanation and a positive urine culture (≥105 CFU/mL) suggests the diagnosis.
- Moreover, enterococcal UTIs often occur in critically or chronically ill patients whose comorbidities may obscure the diagnosis.
- In many cases, removal of the indwelling catheter may suffice to eradicate the organism without specific antimicrobial therapy.
- In rare circumstances, UTIs caused by enterococci may run a complicated course, with the development of pyelonephritis and perinephric abscesses that may be a portal of entry for bloodstream infections (see below).
- Enterococci are also known causes of chronic prostatitis, particularly in men whose urinary tract has been manipulated surgically or endoscopically.
- These infections can be difficult to treat since the agents most potent against enterococci (i.e., aminopenicillins and glycopeptides) penetrate prostatic tissue poorly.
- Chronic prostatic infection can be a source of recurrent enterococcal bacteremia.
- Bacteremia without endocarditis is another frequently encountered presentation of enterococcal disease.
- Intravascular catheters and other devices are commonly associated with these bacteremic episodes (Chap. 147).
- Other well-known sources of enterococcal bacteremia include the gastrointestinal and hepatobiliary tracts; pelvic and intraabdominal foci; and, less frequently, wound infections, UTIs, and bone infections.
- In the United States, enterococci are ranked second (after staphylococci) as etiologic agents of central line–associated bacteremia.
- Patients with enterococcal bacteremia usually have comorbidities and have been in the hospital for prolonged periods; they commonly have received several courses of antibiotics.
- Several studies indicate that the isolation of E. faecium from the blood may lead to worse outcomes and higher mortality rates than when other enterococcal species are isolated; this finding may be related to the higher prevalence of vancomycin and ampicillin resistance in E. faecium than in other enterococcal species, with the consequent reduction of therapeutic options.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- In addition, several cases have been documented in which enterococcal bacteremia was associated with Strongyloides stercoralis hyperinfection syndrome in immunocompromised patients.
- Enterococci are important causes of community- and health care–associated endocarditis, ranking second after staphylococci in the latter infections, and recent studies have implicated E. faecalis as the leading cause of endocarditis after transcatheter aortic valve implantation (TAVI).
- The presumed initial source of bacteremia leading to endocarditis is the gastrointestinal or genitourinary tract—e.g., in patients who have malignant and inflammatory conditions of the gut or have undergone procedures in which these tracts are manipulated.
- The affected patients tend to be male and elderly and to have other debilitating diseases and heart conditions.
- Both prosthetic and native valves can be involved; mitral and aortic valves are affected most often.
- Community-associated endocarditis (usually caused by E. faecalis) also occurs in patients with no apparent risk factors or cardiac abnormalities.
- Endocarditis in women of childbearing age was well described in the past.
- The typical presentation of enterococcal endocarditis is a subacute course of fever, weight loss, malaise, and cardiac murmur; typical stigmata of endocarditis (e.g., petechiae, Osler's nodes, Roth's spots) are found in only a minority of patients.
- Atypical manifestations include arthralgias and manifestations of metastatic disease (splenic abscesses, hiccups, pain in the left flank, pleural effusion, and spondylodiscitis).
- Embolic complications are variable and can affect the brain.
- Heart failure is a common complication of enterococcal endocarditis, and valve replacement may be critical in curing this infection, particularly when multidrug-resistant organisms or major complications are involved.
- A clinical scoring system (DENOVA) has been proposed to help differentiate enterococcal bacteremia from true endocarditis and determine the need for echocardiography.
- The duration of therapy is usually 4–6 weeks, with more prolonged courses suggested for multidrug-resistant isolates in the absence of valvular replacement.
- Risk of relapse for endocarditis due to E. faecalis varies across studies, but it is higher in patients who are treated with antibiotics alone (2–11%) than in those who undergo surgery (0–3%); relapse may occur out to 1-year post-treatment.
- Enterococcal meningitis is an uncommon disease (accounting for only ~4% of meningitis cases) that is usually associated with neurosurgical interventions and conditions such as shunts, central nervous system (CNS) trauma, and cerebrospinal fluid (CSF) leakage.
- In some instances—usually in patients with a debilitating condition, such as cardiovascular or congenital heart disease, chronic renal failure, malignancy, receipt of immunosuppressive therapy, or HIV/AIDS—presumed hematogenous seeding of the meninges is seen in infections such as endocarditis or bacteremia.
- Fever and changes in mental status are common, whereas overt meningeal signs are less so.
- CSF findings are consistent with bacterial infection—i.e., pleocytosis, with a predominance of polymorphonuclear leukocytes (average, ~500/μL), an elevated serum protein level (usually >100 mg/dL), and a decreased glucose concentration (average, 28 mg/dL).
- Gram's staining yields a positive result in about half of cases, with a high rate of organism recovery from CSF cultures; the most common species isolated are E. faecalis and E. faecium.
- Complications include hydrocephalus, brain abscesses, and stroke.
- As mentioned before for bacteremia, an association with Strongyloides hyperinfection also has been documented.
- As mentioned above, enterococci are part of the commensal microbiota of the gastrointestinal tract and can produce spontaneous peritonitis in cirrhotic individuals and in patients undergoing chronic ambulatory peritoneal dialysis (Chap. 137).
- These organisms are commonly found (usually along with other bacteria, including enteric gram-negative species and anaerobes) in clinical samples from intraabdominal and pelvic collections.
- The presence of enterococci in intraabdominal infections is sometimes considered to be of little clinical relevance.
- Several studies have shown that the role of enterococci in intraabdominal infections originating in the community and involving previously healthy patients is minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
- In the past few decades, however, these organisms have become prominent as a cause of intraabdominal infections in hospitalized patients because of the emergence and spread of vancomycin resistance among enterococci and the increase in rates of nosocomial infections due to multidrug-resistant E. faecium isolates.
- In fact, several studies have now documented treatment failures due to enterococci, with consequently increased rates of postoperative complications and death among patients with intraabdominal infections.
- Thus, anti-enterococcal therapy is recommended for nosocomial peritonitis in immunocompromised and severely ill patients who have had a prolonged hospital stay, have undergone multiple procedures, have persistent abdominal sepsis and collections, or have risk factors for the development of endocarditis (e.g., prosthetic or damaged heart valves).
- Conversely, specific treatment for enterococci in the first episode of intraabdominal infection originating in the community and affecting previously healthy patients with no important cardiac risk factors for endocarditis does not appear to be beneficial.
- Enterococci are commonly isolated from soft tissue infections (Chap. 134), particularly those involving surgical wounds (Chap. 147).
- In fact, these organisms rank third as agents of nosocomial surgical-site infections, with E. faecalis the most frequently isolated species.
- The clinical relevance of enterococci in some of these infections—as in intraabdominal infections—is a matter of debate; differentiating between colonization and true infection is sometimes challenging, although in some cases, enterococci have been recovered from lung, liver, and skin abscesses.
- Diabetic foot and decubitus ulcers are often colonized with enterococci and may be the portal of entry for bone infections.
- Enterococci are well-known causes of neonatal infections, including sepsis (mostly late-onset), bacteremia, meningitis, pneumonia, and UTI.
- Outbreaks of enterococcal sepsis in neonatal units have been well documented.
- Risk factors for enterococcal disease in newborns include prematurity, low birth weight, indwelling devices, and abdominal surgery.
- Enterococci have also been described as etiologic agents of bone and joint infections, including vertebral osteomyelitis, usually in patients with underlying conditions such as diabetes or endocarditis.
- Similarly, enterococci have been isolated from bone infections in patients who have undergone arthroplasty or reconstruction of fractures with the placement of hardware.
- Since enterococci can produce a biofilm that is likely to alter the efficacy of anti-enterococcal agents, treatment of infections that involve foreign material is challenging, and removal of the hardware may be necessary to eradicate the infection.
- Rare cases of enterococcal pneumonia, lung abscess, and spontaneous empyema have been described.
4.1 Clinical Syndromes¶
- Urinary Tract Infection and Prostatitis
- Enterococci are well-known causes of nosocomial UTI—the most common infection caused by these organisms (Chap. 140).
- Enterococcal UTIs are usually associated with indwelling catheterization, instrumentation, or anatomic abnormalities of the genitourinary tract, and it is often challenging to differentiate between true infection and colonization (particularly in patients with chronic indwelling catheters).
- Their role as pathogens in otherwise healthy premenopausal woman with acute cystitis is less clear, with data from one study suggesting that enterococci recovered from midstream urine cultures were not predictive of bacteriuria in a subsequent catheterized specimen.
- The presence of leukocytes in the urine in conjunction with systemic manifestations (e.g., fever) or local signs and symptoms of infection with no other explanation and a positive urine culture (≥105 CFU/mL) suggests the diagnosis.
- Moreover, enterococcal UTIs often occur in critically or chronically ill patients whose comorbidities may obscure the diagnosis.
- In many cases, removal of the indwelling catheter may suffice to eradicate the organism without specific antimicrobial therapy.
- In rare circumstances, UTIs caused by enterococci may run a complicated course, with the development of pyelonephritis and perinephric abscesses that may be a portal of entry for bloodstream infections (see below).
- Enterococci are also known causes of chronic prostatitis, particularly in men whose urinary tract has been manipulated surgically or endoscopically.
- These infections can be difficult to treat since the agents most potent against enterococci (i.e., aminopenicillins and glycopeptides) penetrate prostatic tissue poorly.
- Chronic prostatic infection can be a source of recurrent enterococcal bacteremia.
- Bacteremia and Endocarditis
- Bacteremia without endocarditis is another frequently encountered presentation of enterococcal disease.
- Intravascular catheters and other devices are commonly associated with these bacteremic episodes (Chap. 147).
- Other well-known sources of enterococcal bacteremia include the gastrointestinal and hepatobiliary tracts; pelvic and intraabdominal foci; and, less frequently, wound infections, UTIs, and bone infections.
- In the United States, enterococci are ranked second (after staphylococci) as etiologic agents of central line–associated bacteremia.
- Patients with enterococcal bacteremia usually have comorbidities and have been in the hospital for prolonged periods; they commonly have received several courses of antibiotics.
- Several studies indicate that the isolation of E. faecium from the blood may lead to worse outcomes and higher mortality rates than when other enterococcal species are isolated; this finding may be related to the higher prevalence of vancomycin and ampicillin resistance in E. faecium than in other enterococcal species, with the consequent reduction of therapeutic options.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- In addition, several cases have been documented in which enterococcal bacteremia was associated with Strongyloides stercoralis hyperinfection syndrome in immunocompromised patients.
- Enterococci are important causes of community- and health care–associated endocarditis, ranking second after staphylococci in the latter infections, and recent studies have implicated E. faecalis as the leading cause of endocarditis after transcatheter aortic valve implantation (TAVI).
- The presumed initial source of bacteremia leading to endocarditis is the gastrointestinal or genitourinary tract—e.g., in patients who have malignant and inflammatory conditions of the gut or have undergone procedures in which these tracts are manipulated.
- The affected patients tend to be male and elderly and to have other debilitating diseases and heart conditions.
- Both prosthetic and native valves can be involved; mitral and aortic valves are affected most often.
- Community-associated endocarditis (usually caused by E. faecalis) also occurs in patients with no apparent risk factors or cardiac abnormalities.
- Endocarditis in women of childbearing age was well described in the past.
- The typical presentation of enterococcal endocarditis is a subacute course of fever, weight loss, malaise, and cardiac murmur; typical stigmata of endocarditis (e.g., petechiae, Osler's nodes, Roth's spots) are found in only a minority of patients.
- Atypical manifestations include arthralgias and manifestations of metastatic disease (splenic abscesses, hiccups, pain in the left flank, pleural effusion, and spondylodiscitis).
- Embolic complications are variable and can affect the brain.
- Heart failure is a common complication of enterococcal endocarditis, and valve replacement may be critical in curing this infection, particularly when multidrug-resistant organisms or major complications are involved.
- A clinical scoring system (DENOVA) has been proposed to help differentiate enterococcal bacteremia from true endocarditis and determine the need for echocardiography.
- The duration of therapy is usually 4–6 weeks, with more prolonged courses suggested for multidrug-resistant isolates in the absence of valvular replacement.
- Risk of relapse for endocarditis due to E. faecalis varies across studies, but it is higher in patients who are treated with antibiotics alone (2–11%) than in those who undergo surgery (0–3%); relapse may occur out to 1-year post-treatment.
- Meningitis
- Enterococcal meningitis is an uncommon disease (accounting for only ~4% of meningitis cases) that is usually associated with neurosurgical interventions and conditions such as shunts, central nervous system (CNS) trauma, and cerebrospinal fluid (CSF) leakage.
- In some instances—usually in patients with a debilitating condition, such as cardiovascular or congenital heart disease, chronic renal failure, malignancy, receipt of immunosuppressive therapy, or HIV/AIDS—presumed hematogenous seeding of the meninges is seen in infections such as endocarditis or bacteremia.
- Fever and changes in mental status are common, whereas overt meningeal signs are less so.
- CSF findings are consistent with bacterial infection—i.e., pleocytosis, with a predominance of polymorphonuclear leukocytes (average, ~500/μL), an elevated serum protein level (usually >100 mg/dL), and a decreased glucose concentration (average, 28 mg/dL).
- Gram's staining yields a positive result in about half of cases, with a high rate of organism recovery from CSF cultures; the most common species isolated are E. faecalis and E. faecium.
- Complications include hydrocephalus, brain abscesses, and stroke.
- As mentioned before for bacteremia, an association with Strongyloides hyperinfection also has been documented.
- Intraabdominal, Pelvic, and Soft Tissue Infections
- As mentioned above, enterococci are part of the commensal microbiota of the gastrointestinal tract and can produce spontaneous peritonitis in cirrhotic individuals and in patients undergoing chronic ambulatory peritoneal dialysis (Chap. 137).
- These organisms are commonly found (usually along with other bacteria, including enteric gram-negative species and anaerobes) in clinical samples from intraabdominal and pelvic collections.
- The presence of enterococci in intraabdominal infections is sometimes considered to be of little clinical relevance.
- Several studies have shown that the role of enterococci in intraabdominal infections originating in the community and involving previously healthy patients is minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
- In the past few decades, however, these organisms have become prominent as a cause of intraabdominal infections in hospitalized patients because of the emergence and spread of vancomycin resistance among enterococci and the increase in rates of nosocomial infections due to multidrug-resistant E. faecium isolates.
- In fact, several studies have now documented treatment failures due to enterococci, with consequently increased rates of postoperative complications and death among patients with intraabdominal infections.
- Thus, anti-enterococcal therapy is recommended for nosocomial peritonitis in immunocompromised and severely ill patients who have had a prolonged hospital stay, have undergone multiple procedures, have persistent abdominal sepsis and collections, or have risk factors for the development of endocarditis (e.g., prosthetic or damaged heart valves).
- Conversely, specific treatment for enterococci in the first episode of intraabdominal infection originating in the community and affecting previously healthy patients with no important cardiac risk factors for endocarditis does not appear to be beneficial.
- Enterococci are commonly isolated from soft tissue infections (Chap. 134), particularly those involving surgical wounds (Chap. 147).
- In fact, these organisms rank third as agents of nosocomial surgical-site infections, with E. faecalis the most frequently isolated species.
- The clinical relevance of enterococci in some of these infections—as in intraabdominal infections—is a matter of debate; differentiating between colonization and true infection is sometimes challenging, although in some cases, enterococci have been recovered from lung, liver, and skin abscesses.
- Diabetic foot and decubitus ulcers are often colonized with enterococci and may be the portal of entry for bone infections.
- Other Infections
- Enterococci are well-known causes of neonatal infections, including sepsis (mostly late-onset), bacteremia, meningitis, pneumonia, and UTI.
- Outbreaks of enterococcal sepsis in neonatal units have been well documented.
- Risk factors for enterococcal disease in newborns include prematurity, low birth weight, indwelling devices, and abdominal surgery.
- Enterococci have also been described as etiologic agents of bone and joint infections, including vertebral osteomyelitis, usually in patients with underlying conditions such as diabetes or endocarditis.
- Similarly, enterococci have been isolated from bone infections in patients who have undergone arthroplasty or reconstruction of fractures with the placement of hardware.
- Since enterococci can produce a biofilm that is likely to alter the efficacy of anti-enterococcal agents, treatment of infections that involve foreign material is challenging, and removal of the hardware may be necessary to eradicate the infection.
- Rare cases of enterococcal pneumonia, lung abscess, and spontaneous empyema have been described.
5. DIFFERENTIAL DIAGNOSIS¶
- Differentiating between colonization and true infection is sometimes challenging, particularly in patients with chronic indwelling catheters.
- Enterococci recovered from midstream urine cultures were not predictive of bacteriuria in a subsequent catheterized specimen in otherwise healthy premenopausal women with acute cystitis.
- Intraabdominal infections originating in the community and involving previously healthy patients are often minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
- The clinical relevance of enterococci in some of these infections—as in intraabdominal infections—is a matter of debate; differentiating between colonization and true infection is sometimes challenging, although in some cases, enterococci have been recovered from lung, liver, and skin abscesses.
- Diabetic foot and decubitus ulcers are often colonized with enterococci and may be the portal of entry for bone infections.
5.1 Colonization vs. Infection¶
- Enterococci are part of the commensal microbiota of the gastrointestinal tract.
- Enterococci are commonly found (usually along with other bacteria, including enteric gram-negative species and anaerobes) in clinical samples from intraabdominal and pelvic collections.
- The presence of enterococci in intraabdominal infections is sometimes considered to be of little clinical relevance.
- Intraabdominal infections originating in the community and involving previously healthy patients are often minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
- The clinical relevance of enterococci in some of these infections—as in intraabdominal infections—is a matter of debate; differentiating between colonization and true infection is sometimes challenging, although in some cases, enterococci have been recovered from lung, liver, and skin abscesses.
- Diabetic foot and decubitus ulcers are often colonized with enterococci and may be the portal of entry for bone infections.
6. INVESTIGATIONS & DIAGNOSIS¶
- Enterococci are usually reported by the clinical laboratory to be nonhemolytic on the basis of their inability to lyse the ovine or bovine red blood cells (RBCs) commonly used in agar plates; however, some strains of E. faecalis do lyse RBCs from humans, horses, and rabbits due to the presence of an acquired hemolysin/cytolysin gene.
- The majority of clinically relevant enterococcal species hydrolyze pyrrolidonyl-β-naphthylamide (PYR).
- Enterococci are usually observed as single cells, diplococci, or short chains (Fig. 154-1), although long chains are noted with some strains.
- Gram's staining yields a positive result in about half of cases, with a high rate of organism recovery from CSF cultures; the most common species isolated are E. faecalis and E. faecium.
- CSF findings are consistent with bacterial infection—i.e., pleocytosis, with a predominance of polymorphonuclear leukocytes (average, ~500/μL), an elevated serum protein level (usually >100 mg/dL), and a decreased glucose concentration (average, 28 mg/dL).
- The presence of leukocytes in the urine in conjunction with systemic manifestations (e.g., fever) or local signs and symptoms of infection with no other explanation and a positive urine culture (≥105 CFU/mL) suggests the diagnosis.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- Intraabdominal infections originating in the community and involving previously healthy patients are often minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
6.1 Diagnostic Criteria¶
- Urine Culture
- Positive urine culture (≥105 CFU/mL) suggests the diagnosis.
- Presence of leukocytes in the urine in conjunction with systemic manifestations (e.g., fever) or local signs and symptoms of infection with no other explanation.
- Enterococci recovered from midstream urine cultures were not predictive of bacteriuria in a subsequent catheterized specimen in otherwise healthy premenopausal women with acute cystitis.
- CSF Analysis
- Pleocytosis, with a predominance of polymorphonuclear leukocytes (average, ~500/μL).
- Elevated serum protein level (usually >100 mg/dL).
- Decreased glucose concentration (average, 28 mg/dL).
- Gram's staining yields a positive result in about half of cases.
- High rate of organism recovery from CSF cultures; the most common species isolated are E. faecalis and E. faecium.
- Blood Culture
- Enterococci are ranked second (after staphylococci) as etiologic agents of central line–associated bacteremia.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- Isolation of E. faecium from the blood may lead to worse outcomes and higher mortality rates than when other enterococcal species are isolated.
7. MANAGEMENT & TREATMENT¶
- Enterococci are intrinsically resistant and/or tolerant to several antimicrobial agents.
- Tolerance is defined as lack of killing by drug concentrations 32 times higher than the minimal inhibitory concentration (MIC).
- Monotherapy for endocarditis with a β-lactam antibiotic (to which many enterococci are tolerant) has produced disappointing results, with high relapse rates after the end of therapy.
- However, the addition of an aminoglycoside to a cell wall–active agent (a β-lactam or a glycopeptide) increases cure rates and eradicates the organisms; moreover, this combination is synergistic and bactericidal in vitro.
- Therefore, for many decades, combination therapy with a cell wall–active agent and an aminoglycoside was the standard of care for endovascular infections caused by enterococci.
- This synergistic effect can be explained, at least in part, by the increased penetration of the aminoglycoside into the bacterial cell, presumably as a result of cell-wall alterations produced by the β-lactam (or glycopeptide).
- Nonetheless, attaining synergistic bactericidal activity in the treatment of severe enterococcal infections—particularly those caused by E. faecium—has become increasingly difficult because of the development of resistance to virtually all antibiotics available for this purpose.
- Among the β-lactams, the most active are the aminopenicillins (ampicillin, amoxicillin); next most active are penicillin G, imipenem, and ureidopenicillins (i.e., piperacillin).
- Cephalosporins are not active as monotherapy.
- The only two aminoglycosides recommended for synergistic therapy in severe enterococcal infections are gentamicin and streptomycin.
- This is because the most common acquired enzyme conferring high-level resistance to gentamicin also is active against tobramycin and amikacin but not streptomycin, and the resistance mechanisms causing high-level resistance to streptomycin do not affect gentamicin.
- The use of amikacin is strongly discouraged because it is infrequently active, and tobramycin should never be used for the treatment of E. faecium infections due to the presence of a chromosomally encoded, species-specific, tobramycin-modifying enzyme.
- Aminoglycoside monotherapy should not be employed.
- Vancomycin is an alternative to β-lactam drugs for the treatment of E. faecalis infections but is less useful in these cases.
- If choosing a β-lactam other than ampicillin for an invasive infection, susceptibility testing for penicillin should be performed to identify penicillin-resistant, ampicillin-susceptible (PRASEF) isolates.
- Limited in vitro data suggest that synergistic killing by dual β-lactams (i.e., ampicillin and ceftriaxone) may be compromised in PRASEF isolates.
- Some suggest caution with the combination of ampicillin and ceftriaxone in PRASEF isolates and would consider an alternate therapy (such as daptomycin plus ampicillin) guided by susceptibility testing in cases of persistent bacteremia or signs of clinical failure.
- Linezolid is the only agent approved by the U.S. Food and Drug Administration (FDA) for the treatment of VRE infections (Table 154-2).
- Linezolid is not bactericidal, and its use in severe endovascular infections has produced mixed results; therefore, it is recommended only as an alternative to other agents for such infections.
- In addition, linezolid may cause significant toxicities (thrombocytopenia, peripheral neuropathy, optic neuritis, and lactic acidosis) when used in regimens given for >2 weeks.
- Nonetheless, linezolid may play a role in the treatment of enterococcal meningitis and other CNS infections, although clinical data are limited.
- The lipopeptide daptomycin is a bactericidal antibiotic with in vitro activity against all enterococci.
- Although daptomycin is not approved by the FDA for the treatment of VRE or E. faecium, simulated dosing regimens (6 mg/kg) in experimental models of VRE infection led the Clinical Laboratory and Standards Institute (CLSI) to change the daptomycin breakpoints in 2019.
- For E. faecium, all isolates with an MIC of ≤4 mg/L are placed in a 'susceptible dose-dependent' category based on a dosing regimen (including endocarditis) of 8–12 mg/kg, while those with an MIC ≥8 mg/L are considered resistant.
- For all other enterococci, isolates are considered susceptible.
- Less severe infections are often related to indwelling intravascular catheters; removal of the catheter increases the likelihood of enterococcal eradication by a subsequent short course of appropriate antimicrobial therapy.
- In selected cases of catheter-associated bacteremia, removal of the catheter and a short course of therapy (~5–7 days) may be sufficient.
- A single positive blood culture that is likely to be associated with a catheter in a patient who is otherwise doing well may not require therapy after removal of the catheter.
- Patients at high risk for endovascular infections or with severe disease may benefit from synergistic combination therapy.
- The addition of intrathecal or intraventricular therapy with gentamicin (2–10 mg/d) if the organism does not exhibit HLR or with vancomycin (10–20 mg/d) when the isolate is susceptible has been suggested by some authorities.
- The addition of systemic rifampin (a good CSF-penetrating agent) may be considered.
- The combination of ampicillin and ceftriaxone may have clinical benefit (by analogy with endocarditis), but no cases treated with this combination have been reported; the authors would use this combination.
- Approved by the U.S. Food and Drug Administration only for uncomplicated urinary tract infections caused by vancomycin-susceptible E. faecalis.
7.1 Therapeutic Regimens¶
- Table 154-1 Suggested Regimens for the Management of Infections Caused by Enterococcus faecalis
- Endovascular infections (including endocarditis)
- Ampicillin (12 g/d IV in divided doses q4h) plus ceftriaxone (2 g IV q12h)
- Ampicillin (12 g/d IV in divided doses q4h or by continuous infusion) or penicillin (18–30 mU/d IV in divided doses q4h or by continuous infusion) plus an aminoglycoside
- Vancomycin (15 mg/kg IV per dose) plus an aminoglycoside
- High-dose daptomycin ± another active agent
- Ampicillin plus imipenem
- Nonendovascular infections
- Ampicillin (12 g/d IV in divided doses q4h) or penicillin (18 mU/d IV in divided doses q4h) ± an aminoglycoside
- Ceftriaxone
- Vancomycin (15 mg/kg IV per dose)
- High-dose daptomycin ± another active agent
- Linezolid (600 mg IV/PO q12h)
- Meningitis
- Ampicillin (20–24 g/d IV in divided doses q4h) or penicillin (24 mU/d IV in divided doses q4h) plus an aminoglycoside and consider adding ceftriaxone (2 g IV q12h)
- Vancomycin (500–750 mg IV q6h) plus an aminoglycoside or rifampin
- Linezolid
- High-dose daptomycin (plus intrathecal daptomycin) ± another active agent
- Urinary tract infections
- Amoxicillin (500 mg PO q8h)
- Fosfomycin (3 g PO, one dose) (uncomplicated)
- Ampicillin (500 mg IV or PO q6h)
- Nitrofurantoin (100 mg PO q6h)
- Table 154-2 Suggested Regimens for the Management of Infections Caused by Vancomycin- and Ampicillin-Resistant Enterococcus faecium
- Endovascular infections (including endocarditis)
- High-dose daptomycin plus another agent ± an aminoglycoside
- Linezolid (600 mg IV q12h)
- High-dose ampicillin (if MIC is ≤64 μg/mL) ± an aminoglycoside
- For E. faecium, all isolates with an MIC of ≤4 mg/L are placed in a 'susceptible dose-dependent' category based on a dosing regimen (including endocarditis) of 8–12 mg/kg, while those with an MIC ≥8 mg/L are considered resistant.
- For all other enterococci, isolates are considered susceptible.
8. PROGNOSIS & COMPLICATIONS¶
- Several studies indicate that the isolation of E. faecium from the blood may lead to worse outcomes and higher mortality rates than when other enterococcal species are isolated; this finding may be related to the higher prevalence of vancomycin and ampicillin resistance in E. faecium than in other enterococcal species, with the consequent reduction of therapeutic options.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- In addition, several cases have been documented in which enterococcal bacteremia was associated with Strongyloides stercoralis hyperinfection syndrome in immunocompromised patients.
- A clinical scoring system (DENOVA) has been proposed to help differentiate enterococcal bacteremia from true endocarditis and determine the need for echocardiography.
- The duration of therapy is usually 4–6 weeks, with more prolonged courses suggested for multidrug-resistant isolates in the absence of valvular replacement.
- Risk of relapse for endocarditis due to E. faecalis varies across studies, but it is higher in patients who are treated with antibiotics alone (2–11%) than in those who undergo surgery (0–3%); relapse may occur out to 1-year post-treatment.
- Complications include hydrocephalus, brain abscesses, and stroke.
- Intraabdominal infections originating in the community and involving previously healthy patients are often minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
- In the past few decades, however, these organisms have become prominent as a cause of intraabdominal infections in hospitalized patients because of the emergence and spread of vancomycin resistance among enterococci and the increase in rates of nosocomial infections due to multidrug-resistant E. faecium isolates.
- In fact, several studies have now documented treatment failures due to enterococci, with consequently increased rates of postoperative complications and death among patients with intraabdominal infections.
- Thus, anti-enterococcal therapy is recommended for nosocomial peritonitis in immunocompromised and severely ill patients who have had a prolonged hospital stay, have undergone multiple procedures, have persistent abdominal sepsis and collections, or have risk factors for the development of endocarditis (e.g., prosthetic or damaged heart valves).
- Conversely, specific treatment for enterococci in the first episode of intraabdominal infection originating in the community and affecting previously healthy patients with no important cardiac risk factors for endocarditis does not appear to be beneficial.
- Since enterococci can produce a biofilm that is likely to alter the efficacy of anti-enterococcal agents, treatment of infections that involve foreign material is challenging, and removal of the hardware may be necessary to eradicate the infection.
8.1 Mortality and Relapse¶
- Several studies indicate that the isolation of E. faecium from the blood may lead to worse outcomes and higher mortality rates than when other enterococcal species are isolated; this finding may be related to the higher prevalence of vancomycin and ampicillin resistance in E. faecium than in other enterococcal species, with the consequent reduction of therapeutic options.
- Risk of relapse for endocarditis due to E. faecalis varies across studies, but it is higher in patients who are treated with antibiotics alone (2–11%) than in those who undergo surgery (0–3%); relapse may occur out to 1-year post-treatment.
- In fact, several studies have now documented treatment failures due to enterococci, with consequently increased rates of postoperative complications and death among patients with intraabdominal infections.
9. SPECIAL CONSIDERATIONS¶
- Enterococci are well-known causes of neonatal infections, including sepsis (mostly late-onset), bacteremia, meningitis, pneumonia, and UTI.
- Outbreaks of enterococcal sepsis in neonatal units have been well documented.
- Risk factors for enterococcal disease in newborns include prematurity, low birth weight, indwelling devices, and abdominal surgery.
- Enterococci have also been described as etiologic agents of bone and joint infections, including vertebral osteomyelitis, usually in patients with underlying conditions such as diabetes or endocarditis.
- Similarly, enterococci have been isolated from bone infections in patients who have undergone arthroplasty or reconstruction of fractures with the placement of hardware.
- Since enterococci can produce a biofilm that is likely to alter the efficacy of anti-enterococcal agents, treatment of infections that involve foreign material is challenging, and removal of the hardware may be necessary to eradicate the infection.
- Rare cases of enterococcal pneumonia, lung abscess, and spontaneous empyema have been described.
- In hematopoietic stem cell transplant patients, domination of the gastrointestinal tract by enterococci is associated with increased inflammation and a greater severity of illness and mortality in graft-versus-host disease.
- Certain enterococcal species, such as E. faecium, E. durans, and E. hirae, modulate the host immune response and can potentiate the activity of anti-PD-L1 immune checkpoint inhibitor therapy.
- This effect is mediated by the presence of salA, a gene which encodes a peptidoglycan hydrolase with D,L-endopeptidase activity.
- The muropeptides generated by SalA induce host activation of NF-κB via NOD2, leading to an enhanced antitumor immune response.
9.1 Neonatal and Immunocompromised Hosts¶
- Neonatal Infections
- Enterococci are well-known causes of neonatal infections, including sepsis (mostly late-onset), bacteremia, meningitis, pneumonia, and UTI.
- Outbreaks of enterococcal sepsis in neonatal units have been well documented.
- Risk factors for enterococcal disease in newborns include prematurity, low birth weight, indwelling devices, and abdominal surgery.
- Immunocompromised Hosts
- In hematopoietic stem cell transplant patients, domination of the gastrointestinal tract by enterococci is associated with increased inflammation and a greater severity of illness and mortality in graft-versus-host disease.
- Certain enterococcal species, such as E. faecium, E. durans, and E. hirae, modulate the host immune response and can potentiate the activity of anti-PD-L1 immune checkpoint inhibitor therapy.
- This effect is mediated by the presence of salA, a gene which encodes a peptidoglycan hydrolase with D,L-endopeptidase activity.
- The muropeptides generated by SalA induce host activation of NF-κB via NOD2, leading to an enhanced antitumor immune response.
- In some instances—usually in patients with a debilitating condition, such as cardiovascular or congenital heart disease, chronic renal failure, malignancy, receipt of immunosuppressive therapy, or HIV/AIDS—presumed hematogenous seeding of the meninges is seen in infections such as endocarditis or bacteremia.
10. KEY PEARLS & CLINICAL TRAPS¶
- Enterococci are the third most common isolates from hospital-associated infections in the US, after E. coli and staphylococci.
- E. faecium is the most resistant species; >90% of E. faecium isolates are resistant to ampicillin, and vancomycin resistance ranges from 50–70% in acute care hospitals.
- Synergistic bactericidal activity is achieved by combining a cell-wall active agent (β-lactam or glycopeptide) with an aminoglycoside (gentamicin or streptomycin).
- Linezolid is the only FDA-approved agent for VRE infections but is not bactericidal and carries risks of thrombocytopenia, peripheral neuropathy, and optic neuritis with prolonged use.
- Daptomycin is bactericidal against all enterococci but requires high-dose regimens (8–12 mg/kg) for E. faecium with MIC ≤4 mg/L.
- Enterococcal endocarditis typically presents subacutely; valve replacement may be critical for curing infection caused by multidrug-resistant organisms.
- VRE colonization of the GI tract is a critical step in disease development; patients remain colonized for prolonged periods (sometimes >1 year).
- Cephalosporins are not active as monotherapy against enterococci; ampicillin and amoxicillin are the most active β-lactams.
- Intraabdominal infections in hospitalized patients are increasingly caused by vancomycin-resistant E. faecium, leading to treatment failures.
- Enterococcal meningitis is uncommon (~4% of cases) and associated with neurosurgical interventions or hematogenous seeding from endocarditis.
10.1 Board Exam Favorites¶
- Enterococci are the third most common isolates from hospital-associated infections in the US, after E. coli and staphylococci.
- E. faecium is the most resistant species; >90% of E. faecium isolates are resistant to ampicillin, and vancomycin resistance ranges from 50–70% in acute care hospitals.
- Synergistic bactericidal activity is achieved by combining a cell-wall active agent (β-lactam or glycopeptide) with an aminoglycoside (gentamicin or streptomycin).
- Linezolid is the only FDA-approved agent for VRE infections but is not bactericidal and carries risks of thrombocytopenia, peripheral neuropathy, and optic neuritis with prolonged use.
- Daptomycin is bactericidal against all enterococci but requires high-dose regimens (8–12 mg/kg) for E. faecium with MIC ≤4 mg/L.
- Enterococcal endocarditis typically presents subacutely; valve replacement may be critical for curing infection caused by multidrug-resistant organisms.
- VRE colonization of the GI tract is a critical step in disease development; patients remain colonized for prolonged periods (sometimes >1 year).
- Cephalosporins are not active as monotherapy against enterococci; ampicillin and amoxicillin are the most active β-lactams.
- Intraabdominal infections in hospitalized patients are increasingly caused by vancomycin-resistant E. faecium, leading to treatment failures.
- Enterococcal meningitis is uncommon (~4% of cases) and associated with neurosurgical interventions or hematogenous seeding from endocarditis.
11. WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- The presence of leukocytes in the urine in conjunction with systemic manifestations (e.g., fever) or local signs and symptoms of infection with no other explanation and a positive urine culture (≥105 CFU/mL) suggests the diagnosis.
- Gram's staining yields a positive result in about half of cases, with a high rate of organism recovery from CSF cultures; the most common species isolated are E. faecalis and E. faecium.
- Enterococci are the third most common isolates (after Escherichia coli and staphylococci) from hospital-associated infections in the United States.
- Enterococci are usually reported by the clinical laboratory to be nonhemolytic on the basis of their inability to lyse the ovine or bovine red blood cells (RBCs) commonly used in agar plates; however, some strains of E. faecalis do lyse RBCs from humans, horses, and rabbits due to the presence of an acquired hemolysin/cytolysin gene.
- The majority of clinically relevant enterococcal species hydrolyze pyrrolidonyl-β-naphthylamide (PYR).
- Enterococci are usually observed as single cells, diplococci, or short chains (Fig. 154-1), although long chains are noted with some strains.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- Intraabdominal infections originating in the community and involving previously healthy patients are often minor since surgery and broad-spectrum antimicrobial drugs that do not target enterococci are often sufficient to treat these infections successfully.
- The clinical relevance of enterococci in some of these infections—as in intraabdominal infections—is a matter of debate; differentiating between colonization and true infection is sometimes challenging, although in some cases, enterococci have been recovered from lung, liver, and skin abscesses.
- Diabetic foot and decubitus ulcers are often colonized with enterococci and may be the portal of entry for bone infections.
11.1 Specific Findings¶
- Urine Culture
- Positive urine culture (≥105 CFU/mL) suggests the diagnosis.
- Presence of leukocytes in the urine in conjunction with systemic manifestations (e.g., fever) or local signs and symptoms of infection with no other explanation.
- Enterococci recovered from midstream urine cultures were not predictive of bacteriuria in a subsequent catheterized specimen in otherwise healthy premenopausal women with acute cystitis.
- CSF Analysis
- Pleocytosis, with a predominance of polymorphonuclear leukocytes (average, ~500/μL).
- Elevated serum protein level (usually >100 mg/dL).
- Decreased glucose concentration (average, 28 mg/dL).
- Gram's staining yields a positive result in about half of cases.
- High rate of organism recovery from CSF cultures; the most common species isolated are E. faecalis and E. faecium.
- Blood Culture
- Enterococci are ranked second (after staphylococci) as etiologic agents of central line–associated bacteremia.
- In some cases (usually when the gastrointestinal tract is the source), enterococcal bacteremia may be polymicrobial, with gram-negative organisms isolated at the same time.
- Isolation of E. faecium from the blood may lead to worse outcomes and higher mortality rates than when other enterococcal species are isolated.
12. WHAT EXCLUDES THE DIAGNOSIS¶
- Cephalosporins are not active as monotherapy.
- Tobramycin should never be used for the treatment of E. faecium infections.
- Vancomycin is recommended only as an alternative to β-lactam agents in cases of allergy or toxicity plus the inability to desensitize.
- The use of amikacin is strongly discouraged because it is infrequently active.
- Aminoglycoside monotherapy should not be employed.
- In the absence of antibiotics, hospital-associated lineages of E. faecium seem to be less adapted for survival in the gastrointestinal tract than are commensal E. faecium strains.
- Studies examining the rate of carriage of VRE in patients after discharge from the hospital document a median time to clearance between 2 and 4 months in patients without ongoing risk factors, such as continued antibiotic use, residence in a long-term care facility, or need for hemodialysis.
12.1 Exclusion Criteria¶
- Cephalosporins are not active as monotherapy.
- Tobramycin should never be used for the treatment of E. faecium infections.
- Vancomycin is recommended only as an alternative to β-lactam agents in cases of allergy or toxicity plus the inability to desensitize.
- The use of amikacin is strongly discouraged because it is infrequently active.
- Aminoglycoside monotherapy should not be employed.
- In the absence of antibiotics, hospital-associated lineages of E. faecium seem to be less adapted for survival in the gastrointestinal tract than are commensal E. faecium strains.
- Studies examining the rate of carriage of VRE in patients after discharge from the hospital document a median time to clearance between 2 and 4 months in patients without ongoing risk factors, such as continued antibiotic use, residence in a long-term care facility, or need for hemodialysis.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
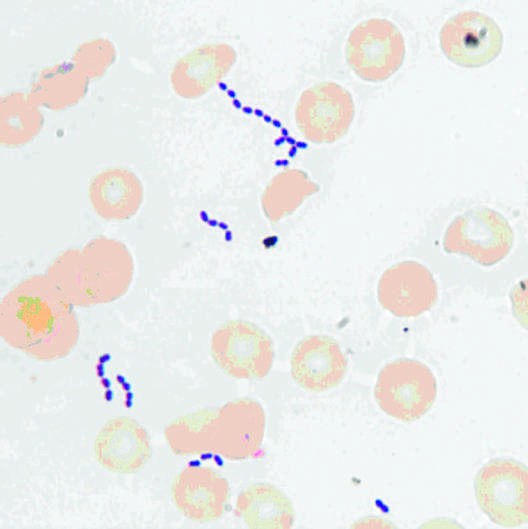
Caption: CHAPTER 154 FIGURE 154-1 Gram’s stain of cultured blood from a patient with enterococcal bacteremia. Oval gram-positive bacterial cells are arranged as diplococci and short chains. (Courtesy of Audrey Wanger, PhD.) this characteristic is helpful in differentiating enterococci from organ- isms of the Streptococcus gallolyticus group (formerly known as S. bovis, which includes S. gallolyticus, S. pasteurianus, and S. infantarius) and from Leuconostoc species. Although many species of enterococci have — Figure 154-1 Gram's stain of cultured blood from a patient with enterococcal bacteremia. Oval gram-positive bacterial cells are arranged as diplococci and short chains.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.