Chapter 338: Irritable Bowel Syndrome¶
Disorders of the Gastrointestinal System · Part 10 – Gastrointestinal Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Rome IV criteria require recurrent abdominal pain at least 1 day/week in the last 3 months, associated with 2 of 3 features: related to defecation, change in stool frequency, or change in stool form.
- Alarm features (age >40 onset, weight loss, nocturnal symptoms, rectal bleeding, anemia) warrant colonoscopy to rule out organic disease.
- Visceral hypersensitivity is a core pathophysiological mechanism; pain thresholds are lower in IBS patients compared to healthy controls.
- Soluble fiber (psyllium) is preferred over insoluble fiber (wheat bran) to avoid exacerbating bloating and pain.
- Tricyclic antidepressants (TCAs) are effective for IBS-D by slowing transit and modulating visceral afferent neural function.
- Low FODMAP diet reduces global IBS symptoms in 50–80% of patients, primarily improving abdominal pain and bloating.
- Rifaximin (550 mg TID for 2 weeks) is effective for IBS-D, particularly in patients with bloating and gas.
- Linaclotide and lubiprostone are secretagogues approved for IBS-C; eluxadoline is approved for IBS-D.
- Postinfectious IBS occurs in >10% of patients with infectious enteritis, with risk 4-fold higher than non-infected individuals.
- Mast cell activation and altered gut permeability contribute to visceral hypersensitivity and subclinical mucosal inflammation.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Rome IV Diagnostic Criteria
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 GI Motor Abnormalities
- 3.2 Visceral Hypersensitivity
- 3.3 Central Neural Dysregulation
- 3.4 Abnormal Psychological Features
- 3.5 Postinfectious IBS
- 3.6 Immune Activation and Mucosal Inflammation
- 3.7 Altered Intestinal Permeability
- 3.8 Altered Gut Flora
- 3.9 Abnormal Serotonin Pathways
- 3.10 Bile Acids
- 4. CLINICAL FEATURES
- 4.1 Altered Bowel Habits
- 4.2 Gas and Flatulence
- 4.3 Upper GI Symptoms
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Approach
- 6.2 Alarm Features
- 7. MANAGEMENT & TREATMENT
- 7.1 Stool-Bulking Agents
- 7.2 Antispasmodics
- 7.3 Antiflatulence Therapy
- 7.4 Antidepressant Drugs
- 7.5 Serotonin Receptor Modulators
- 7.6 Modulation of Gut Flora
- 7.7 Low FODMAP Diet
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Changes in gut microbiota among patients with irritable bowel syndrome (IBS) |
| 2 | 🖼 Figure | Pathophysiology of irritable bowel syndrome (IBS) |
| 3 | 🖼 Figure | Pathogenesis of FODMAP-related symptoms |
| 4 | 🖼 Figure | Gut dysbiosis and irritable bowel syndrome (IBS) |
1. DEFINITION & OVERVIEW¶
- Irritable bowel syndrome (IBS) is a functional bowel disorder characterized by abdominal pain or discomfort and altered bowel habits in the absence of detectable structural abnormalities.
- No clear diagnostic markers exist for IBS; thus, the diagnosis is based on clinical presentation and symptom-based criteria.
- IBS symptoms fluctuate over time and often overlap with other functional disorders such as fibromyalgia, headache, backache, and genitourinary symptoms.
- Severity of symptoms varies and can significantly impair quality of life, resulting in high direct and indirect health care costs.
- In 2016, the Rome III criteria were updated to Rome IV criteria for the diagnosis of IBS.
1.1 Rome IV Diagnostic Criteria¶
- Criteria fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis.
- Recurrent abdominal pain, on average, at least 1 day per week in the last 3 months, associated with ≥2 of the following criteria:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
Table 1 — Table 338-1 Rome IV Diagnostic Criteria for Irritable Bowel Syndrome¶
| Criterion | Requirement |
|---|---|
| Recurrent abdominal pain | On average, at least 1 day per week in the last 3 months |
| Associated with defecation | Pain improves or worsens with bowel movements |
| Associated with change in frequency | Change in stool frequency (diarrhea or constipation) |
| Associated with change in form | Change in stool appearance (hard/loose) |
2. EPIDEMIOLOGY¶
- Worldwide, ~10% of adults and adolescents have symptoms consistent with IBS.
- IBS is a disorder that affects all ages, although most patients have their first symptoms before age 45.
- Women are diagnosed with IBS two to three times as often as men and make up 80% of the population with severe IBS.
- IBS symptoms are prevalent in other functional GI disorders such as noncardiac chest pain patients and esophageal hypersensitivity.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
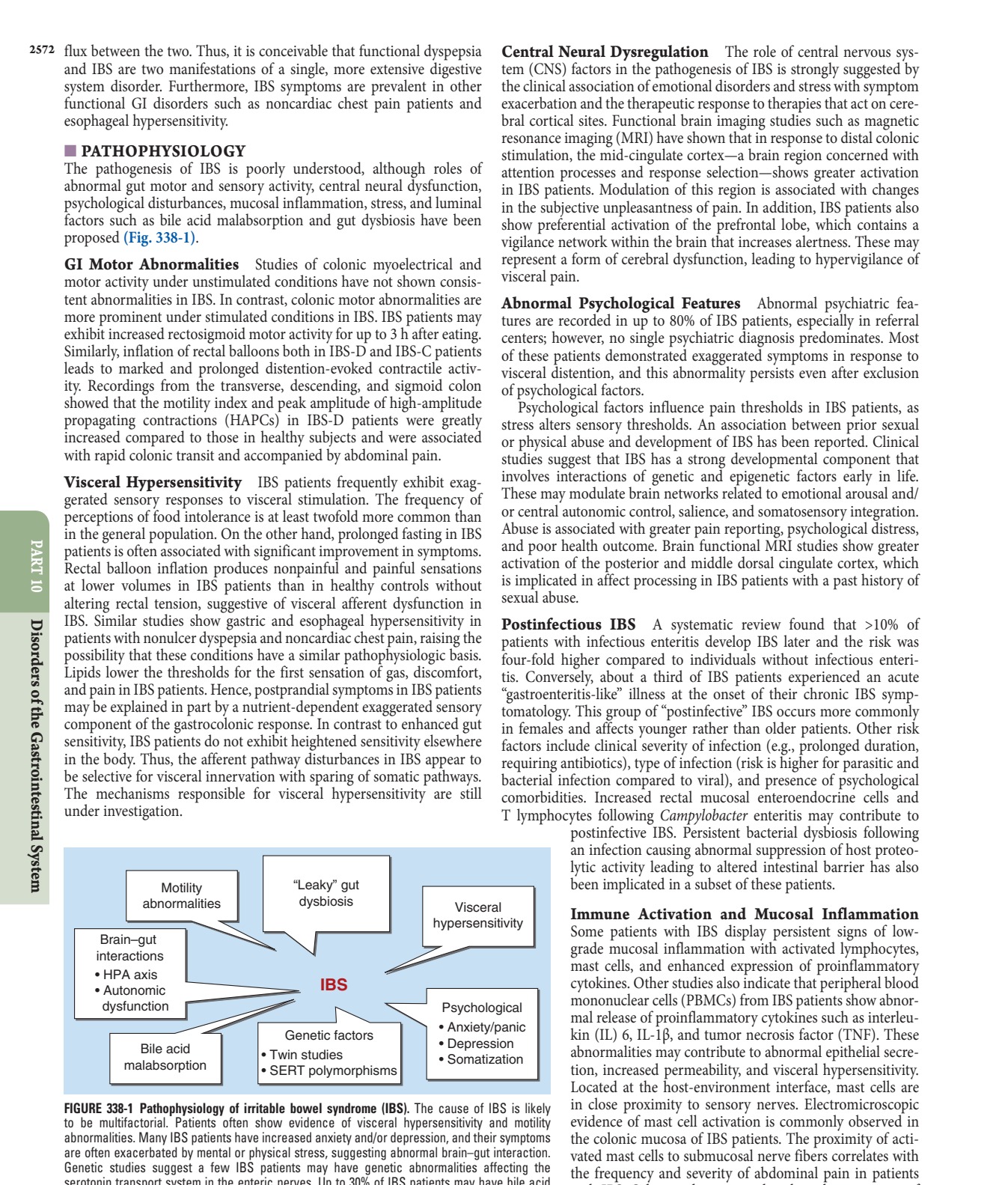
- The pathogenesis of IBS is poorly understood, although roles of abnormal gut motor and sensory activity, central neural dysfunction, psychological disturbances, mucosal inflammation, stress, and luminal factors such as bile acid malabsorption and gut dysbiosis have been proposed.
- The cause of IBS is likely multifactorial, involving genetic susceptibility and environmental insults.
3.1 GI Motor Abnormalities¶
- Studies of colonic myoelectrical and motor activity under unstimulated conditions have not shown consistent abnormalities in IBS.
- In contrast, colonic motor abnormalities are more prominent under stimulated conditions in IBS.
- IBS patients may exhibit increased rectosigmoid motor activity for up to 3 h after eating.
- Inflation of rectal balloons in IBS-D and IBS-C patients leads to marked and prolonged distention-evoked contractile activity.
- Recordings from the transverse, descending, and sigmoid colon showed that the motility index and peak amplitude of high-amplitude propagating contractions (HAPCs) in IBS-D patients were greatly increased compared to healthy subjects and were associated with rapid colonic transit and accompanied by abdominal pain.
3.2 Visceral Hypersensitivity¶
- IBS patients frequently exhibit exaggerated sensory responses to visceral stimulation.
- The frequency of perceptions of food intolerance is at least twofold more common than in the general population.
- Prolonged fasting in IBS patients is often associated with significant improvement in symptoms.
- Rectal balloon inflation produces nonpainful and painful sensations at lower volumes in IBS patients than in healthy controls without altering rectal tension, suggestive of visceral afferent dysfunction in IBS.
- Similar studies show gastric and esophageal hypersensitivity in patients with nonulcer dyspepsia and noncardiac chest pain, raising the possibility that these conditions have a similar pathophysiologic basis.
- Lipids lower the thresholds for the first sensation of gas, discomfort, and pain in IBS patients.
- Hence, postprandial symptoms in IBS patients may be explained in part by a nutrient-dependent exaggerated sensory component of the gastrocolonic response.
- In contrast to enhanced gut sensitivity, IBS patients do not exhibit heightened sensitivity elsewhere in the body. Thus, the afferent pathway disturbances in IBS appear to be selective for visceral innervation with sparing of somatic pathways.
- The mechanisms responsible for visceral hypersensitivity are still under investigation.
- T lymphocytes following Campylobacter enteritis may contribute to postinfective IBS.
- Persistent bacterial dysbiosis following an infection causing abnormal suppression of host proteolytic activity leading to altered intestinal barrier has also been implicated in a subset of these patients.
3.3 Central Neural Dysregulation¶
- The role of central nervous system (CNS) factors in the pathogenesis of IBS is strongly suggested by the clinical association of emotional disorders and stress with symptom exacerbation and the therapeutic response to therapies that act on cerebral cortical sites.
- Functional brain imaging studies such as magnetic resonance imaging (MRI) have shown that in response to distal colonic stimulation, the mid-cingulate cortex—a brain region concerned with attention processes and response selection—shows greater activation in IBS patients.
- Modulation of this region is associated with changes in the subjective unpleasantness of pain.
- In addition, IBS patients also show preferential activation of the prefrontal lobe, which contains a vigilance network within the brain that increases alertness.
- These may represent a form of cerebral dysfunction, leading to hypervigilance of visceral pain.
3.4 Abnormal Psychological Features¶
- Abnormal psychiatric features are recorded in up to 80% of IBS patients, especially in referral centers; however, no single psychiatric diagnosis predominates.
- Most of these patients demonstrated exaggerated symptoms in response to visceral distention, and this abnormality persists even after exclusion of psychological factors.
- Psychological factors influence pain thresholds in IBS patients, as stress alters sensory thresholds.
- An association between prior sexual or physical abuse and development of IBS has been reported.
- Abuse is associated with greater pain reporting, psychological distress, and poor health outcome.
- Brain functional MRI studies show greater activation of the posterior and middle dorsal cingulate cortex, which is implicated in affect processing in IBS patients with a past history of sexual abuse.
3.5 Postinfectious IBS¶
- A systematic review found that >10% of patients with infectious enteritis develop IBS later and the risk was four-fold higher compared to individuals without infectious enteritis.
- Conversely, about a third of IBS patients experienced an acute "gastroenteritis-like" illness at the onset of their chronic IBS symptomatology.
- This group of "postinfective" IBS occurs more commonly in females and affects younger rather than older patients.
- Other risk factors include clinical severity of infection (e.g., prolonged duration, requiring antibiotics), type of infection (risk is higher for parasitic and bacterial infection compared to viral), and presence of psychological comorbidities.
3.6 Immune Activation and Mucosal Inflammation¶
- Some patients with IBS display persistent signs of low-grade mucosal inflammation with activated lymphocytes, mast cells, and enhanced expression of proinflammatory cytokines.
- Other studies also indicate that peripheral blood mononuclear cells (PBMCs) from IBS patients show abnormal release of proinflammatory cytokines such as interleukin (IL) 6, IL-1β, and tumor necrosis factor (TNF).
- These abnormalities may contribute to abnormal epithelial secretion, increased permeability, and visceral hypersensitivity.
- Located at the host-environment interface, mast cells are to be multifactorial.
- Patients often show evidence of visceral hypersensitivity and abnormalities.
- Many IBS patients have increased anxiety and/or depression, and their symptoms are often exacerbated by mental or physical stress, suggesting abnormal brain–gut interaction.
- Genetic studies suggest a few IBS patients may have genetic abnormalities affecting the serotonin transport system in the enteric nerves.
- Up to 30% of IBS patients may have bile acid malabsorption.
- Other studies report that the colonic mucosa of IBS patients. This may lead to subclinical mucosa inflammation.
- HPA, hypothalamic-pituitary-adrenal; SERT, serotonin reuptake transporter.
3.7 Altered Intestinal Permeability¶
- The gut epithelial lining represents a semipermeable barrier that allows nutrient and water absorption while being restrictive against pathogenic molecules, toxins, and bacteria.
- The intestinal barrier is impaired in a subset of patients with IBS.
- This is primarily described in patients with IBS-D and postinfectious IBS.
- It is unclear whether or not those with IBS-C and IBS-M also have increased intestinal permeability.
- There appears to be a correlation between altered intestinal permeability and symptom severity in IBS.
- Studies have not only shown structural changes in barrier function, such as a decrease in gene and protein expression of tight junction proteins, but also functional consequences, such as the increased passage of macromolecules including bacteria across the epithelial barrier in Ussing chamber studies.
- Although the exact etiology of the altered mucosal barrier is not well understood, several factors such as stress, diet, and microbial dysbiosis appear to play a key role.
- Several studies have shown a key role of mast cell activation in mediating barrier dysfunction due to stress and diet-related dysbiosis.
3.8 Altered Gut Flora¶
- IBS patients have fourfold increased odds of having small-intestinal bacterial overgrowth compared to healthy controls based on positive lactulose or glucose hydrogen breath test.
- This finding, however, has been challenged by a number of other studies that found no increased incidence of bacterial overgrowth based on jejunal aspirate culture.
- An abnormal H breath test can occur because of rapid small-bowel transit and may lead to erroneous interpretation.
- It is unclear if an abnormal breath test can predict the response to available treatment options such as nonselective antibiotics, and therefore, the role of testing for small-intestinal bacterial overgrowth in IBS patients remains unclear.
- Many, but not all, studies using culture-independent approaches such as 16S rRNA gene-based analysis found significant differences between the molecular profile of the fecal microbiota of IBS patients and that of healthy subjects.
- Although an IBS-specific microbial signature has not yet been identified, but overall, the diversity of fecal microbiome appears to be significantly lower in IBS patients compared to healthy controls.
- However, the functional significance of this finding is not well understood.
- Despite a lack of consensus on the exact microbial difference between IBS patients and controls, IBS patients generally had decreased proportions of the genera Bifidobacterium and Faecalibacterium and increased abundance of family Enterobacteriaceae (phylum Proteobacteria), family Lactobacillaceae, and genus Bacteroides (phylum Bacteroidetes).
3.9 Abnormal Serotonin Pathways¶
- The serotonin-containing enterochromaffin cells in the colon are increased in a subset of IBS-D patients compared to healthy individuals.
- Furthermore, postprandial plasma serotonin levels were significantly higher in this group of patients compared to healthy controls.
- Tryptophan hydroxylase 1 (TPH1) is the rate-limiting enzyme in enterochromaffin cell serotonin biosynthesis, and functional TPH1 polymorphism has been shown to be associated with IBS subtypes.
- In addition, gut microbes promote colonic serotonin production through an effect of short-chain fatty acids on enterochromaffin cells.
- In IBS patients, the expression of mucosal serotonin reuptake transporter (SERT) is downregulated due to gram-negative gut dysbiosis, leading to abnormal mucosal serotonin levels in IBS.
- Because serotonin plays an important role in the regulation of GI motility and visceral perception, the increased release of serotonin may contribute to the postprandial symptoms of these patients.
3.10 Bile Acids¶
- Up to 25% of patients with IBS-D are found to have evidence of idiopathic bile acid diarrhea.
- Mechanisms leading to increased hepatic synthesis and colonic bile acid levels in idiopathic bile acid diarrhea include reduced synthesis of fibroblast growth factor 19 (FGF-19) by the ileal mucosa or genetic variation in proteins involved in negative feedback of bile acid synthesis.
- Increased colonic bile acid levels in turn influence bowel habit by accelerating colonic transit, intestinal permeability, and visceral hypersensitivity.
4. CLINICAL FEATURES¶
- Abdominal pain is essential for diagnosing IBS.
- This should be associated with defecation and/or have its onset associated with a change in frequency or form of stool.
- Abdominal pain in IBS is highly variable in intensity and location and can occur anywhere in the abdomen.
- It is frequently episodic and crampy, but it may be superimposed on a background of constant ache.
- Pain may be mild enough to be ignored, or it may interfere with daily activities.
- Despite this, malnutrition due to inadequate caloric intake is exceedingly rare with IBS.
- Sleep deprivation is also unusual because abdominal pain is almost uniformly present only during waking hours.
- Pain is often exacerbated by eating or emotional stress and improved by the passage of flatus or stools.
- In addition, female patients with IBS commonly report worsening symptoms during the premenstrual and menstrual phases.
4.1 Altered Bowel Habits¶
- Alteration in bowel habits is the most consistent clinical feature in IBS.
- Based on the predominant bowel type, IBS can be classified into IBS with predominant constipation (IBS-C), IBS with predominant diarrhea (IBS-D), and IBS with both mixed constipation and diarrhea (IBS-M).
- However, bowel pattern subtypes are highly unstable.
- In a patient population with ~33% prevalence rates of IBS-D, IBS-C, and IBS-M forms, 75% of patients change subtypes and 29% switch between IBS-C and IBS-D over 1 year.
- Patients with IBS-C have symptoms of hard stools (often with narrow caliber), infrequent stools (less than three bowel movements per week), incomplete evacuation, straining, sensation of anal blockage, and digitalization.
- On the other hand, those with IBS-D usually have small volumes of loose stools (generally <200 mL).
- This is often associated with fecal urgency, the passage of mucus, and in some cases incontinence.
- Diarrhea may be aggravated by emotional stress or eating.
- Weight loss, nocturnal symptoms, and bleeding per rectum are not common in patients with IBS and, when present, should warrant evaluation for other causes.
4.2 Gas and Flatulence¶
- Patients with IBS frequently complain of bloating, abdominal distention and increased belching or flatulence, all of which they attribute to increased gas.
- Although some patients with these symptoms actually may have a larger amount of gas, quantitative measurements reveal that most patients who complain of increased gas generate no more than a normal amount of intestinal gas.
- Most patients with IBS have impaired transit and intolerance of intestinal gas loads.
- In addition, patients with IBS tend to reflux gas from the distal to the more proximal intestine, which may explain the belching.
- Some patients with bloating may also experience visible distention with increase in abdominal girth.
4.3 Upper GI Symptoms¶
- Between 25 and 50% of patients with IBS complain of dyspepsia, heartburn, nausea, and vomiting.
- This suggests that other areas of the gut apart from the colon may be involved.
- Prolonged ambulant recordings of small-bowel motility in patients with IBS show a high incidence of abnormalities in the small bowel during the diurnal (waking) period; nocturnal motor patterns are not different from those of healthy controls.
- The overlap between dyspepsia and IBS is high.
- The prevalence of IBS is higher among patients with dyspepsia (31.7%) than among those who reported no symptoms of dyspepsia.
- Conversely, among patients with IBS, 55.6% reported symptoms of dyspepsia.
- In addition, the functional abdominal symptoms can change over time.
- Those with predominant dyspepsia or IBS can change over time.
5. DIFFERENTIAL DIAGNOSIS¶
- Because the major symptoms of IBS—abdominal pain, abdominal bloating, and alteration in bowel habits—are common complaints of many GI organic disorders, the list of differential diagnoses is a long one.
- The quality, location, and timing of pain may be helpful to suggest specific disorders.
- Pain due to IBS that occurs in the epigastric or periumbilical area must be differentiated from biliary tract disease, peptic ulcer disorders, intestinal ischemia, and carcinoma of the stomach and pancreas.
- If pain occurs mainly in the lower abdomen, the possibility of diverticular disease of the colon, inflammatory bowel disease (including ulcerative colitis and Crohn’s disease), and carcinoma of the colon must be considered.
- Postprandial pain accompanied by bloating, nausea, and vomiting suggests gastroparesis or partial intestinal obstruction.
- Patients with small intestinal bacteria overgrowth can present with abdominal pain, nausea, and bloating.
- Intestinal infestation with Giardia lamblia or other parasites may cause similar symptoms.
- When diarrhea is the major complaint, the possibility of lactase deficiency, laxative abuse, malabsorption, celiac sprue, hyperthyroidism, inflammatory bowel disease (IBD), and infectious diarrhea must be ruled out.
- On the other hand, constipation may be a side effect of many different drugs, such as anticholinergic, antihypertensive, and antidepressant medications.
- Endocrinopathies such as hypothyroidism and hypoparathyroidism must also be considered in the differential diagnosis of constipation.
- In addition, acute intermittent porphyria and lead poisoning may present in a fashion similar to IBS, with painful constipation as the major complaint.
- These possibilities are suspected on the basis of their clinical presentations and are confirmed by appropriate serum and urine tests.
6. INVESTIGATIONS & DIAGNOSIS¶
- Because IBS is a disorder for which no pathognomonic abnormalities have been identified, its diagnosis relies on recognition of positive clinical features and elimination of other organic diseases.
- Symptom-based criteria have been developed for the purpose of differentiating patients with IBS from those with organic diseases.
- These include the Manning, Rome I, Rome II, Rome III, and Rome IV criteria.
- Rome IV criteria for the diagnosis of IBS were published in 2016 (Table 338-1) and defined IBS on the basis of abdominal pain and altered bowel habits that occur with sufficient frequency in affected patients.
- A careful history and physical examination are frequently helpful in establishing the diagnosis.
- Clinical features suggestive of IBS include recurrence of lower abdominal pain with altered bowel habits over a period of time without progressive deterioration, onset of symptoms during periods of stress or emotional upset, absence of other systemic symptoms such as fever and weight loss, and small-volume stool without any evidence of blood.
- On the other hand, the appearance of the disorder for the first time in old age, progressive course from time of onset, rectal bleeding, significant weight loss persistent diarrhea after a 48-h fast, and presence of nocturnal diarrhea or steatorrheal stools argue against the diagnosis of IBS.
6.1 Diagnostic Approach¶
- Few tests are required for patients who have typical IBS symptoms and no alarm features.
- Unnecessary investigations may be costly and even harmful.
- The American Gastroenterological Association has delineated factors to be considered when determining the aggressiveness of the diagnostic evaluation.
- These include the duration of symptoms, the change in symptoms over time, the age and sex of the patient, the referral status of the patient, prior diagnostic studies, a family history of colorectal malignancy, and the degree of psychosocial dysfunction.
- Thus, a younger individual with mild symptoms requires a minimal diagnostic evaluation, while an older person or an individual with rapidly progressive symptoms should undergo a more thorough exclusion of organic disease.
- Most patients should have a complete blood count and fecal calprotectin (or fecal lactoferrin), and/or C-reactive protein should be checked in patients with IBS-D even in the absence of alarm features to rule out IBD.
- Serologic testing for celiac disease should be performed in patients with symptoms of IBS-D if the prevalence of celiac disease in the general population is 1% or higher.
- Stool examination for ova and parasites is not necessary for all patients with IBS-D but could be helpful in regions where parasitic infections are endemic/common or if history suggests a possibility of parasitic infection (e.g., drinking untreated water).
6.2 Alarm Features¶
- In the presence of alarm features or symptom onset after age 40, or in the absence of response to traditional therapies such as antidiarrheals, colonoscopy is warranted.
- Random biopsies to rule out microscopic colitis should be performed if the patient has persistent or chronic diarrhea.
- If the main symptoms are diarrhea and increased gas, the possibility of lactase deficiency should be ruled out with a hydrogen breath test or with evaluation after a 3-week lactose-free diet.
- Excessive gas with bloating also raises the possibility of small-bowel bacteria overgrowth, and this should be ruled out with a glucose hydrogen breath test.
- In patients with concurrent symptoms of dyspepsia, upper GI radiographs or esophagogastroduodenoscopy may be advisable.
- In patients with postprandial right upper quadrant pain, an ultrasonogram of the gallbladder should be obtained.
- Laboratory features that argue against IBS include evidence of anemia, elevated sedimentation rate, presence of leukocytes or blood in stool, and stool volume >200–300 mL/d.
- These findings would necessitate other diagnostic considerations.
7. MANAGEMENT & TREATMENT¶
- Reassurance and careful explanation of the functional nature of the disorder are of primary importance, along with counseling on how to identify triggers for the patient’s IBS symptoms.
- Stress management may be helpful if stress is a trigger, and identifying obvious food precipitants is an important first step in patient counseling and dietary change.
- As a therapeutic trial, patients should be encouraged to eliminate any foodstuffs that appear to produce symptoms.
- However, patients should avoid nutritionally depleted diets.
- It is unclear if exercise improves overall IBS symptoms, but given its low risk and overall health benefits, it should be encouraged in all IBS patients.
7.1 Stool-Bulking Agents¶
- High-fiber diets and fiber supplementation are frequently used in treating IBS.
- The water-holding action of fibers may contribute to increased stool bulk, and fiber also speeds up colonic transit in most people.
- Furthermore, because of its hydrophilic properties, soluble fiber binds water by soaking up extra water in the colon and therefore can be helpful with diarrhea in some IBS patients.
- Furthermore, fiber supplementation with psyllium has been shown to reduce perception of rectal distention, indicating that fiber may have a positive effect on visceral afferent function.
- Controlled trials of dietary fiber in IBS patients have produced variable results.
- This is not surprising since IBS is a heterogeneous disorder, with some patients being constipated and other having predominant diarrhea.
- Most investigations report increases in stool weight, decreases in colonic transit times, and improvement in constipation.
- Others have noted benefits in patients with alternating diarrhea and constipation, pain, and bloating.
- However, most studies observe no response in patients with diarrhea- or pain-predominant IBS.
- While studies do not support the use of insoluble dietary fiber such as wheat bran in IBS, soluble fibers such as psyllium preparations are often found to be effective in managing IBS symptoms.
- Fiber should be started at a nominal dose and slowly titrated up as tolerated over the course of several weeks to a targeted dose of 20–30 g of total dietary and supplementary fiber per day.
- Even when used judiciously, fiber can exacerbate bloating, flatulence, constipation, and diarrhea.
- Osmotic agents such as magnesium citrate–based products, sodium phosphate–based products, and nonabsorbable carbohydrates are hypertonic products that, through osmosis, extract fluid into the intestinal lumen to soften stool and enhance colonic transit.
- In contrast, polyethylene glycol (PEG)–based solution is iso-osmotic and induces bowel movement by high-volume lavage.
- The osmotic laxatives were better than placebo in improving symptoms of chronic constipation in clinical trials.
- However, chronic use of magnesium hydroxide may result in severe hypermagnesemia in patients with renal impairment.
- Frequent sodium phosphate–based bowel cleansing should be avoided as this is associated with hyperphosphatasemia, hypocalcemia, and hypokalemia.
- In 19 trials, PEG consistently induced more bowel movements than placebo.
- A Cochrane review of 10 randomized trials showed that PEG was superior to lactulose for improving stool frequency and abdominal pain.
- Among the nonabsorbable carbohydrates, lactulose and sorbitol had similar laxative effects.
- However, bacterial metabolism of unabsorbed carbohydrates often leads to gas production and abdominal pain, which can limit long-term use.
- Eluxadoline, a locally acting, mixed µ-opioid receptor agonist, κ-opioid receptor agonist, and δ-opioid receptor antagonist with minimal systemic bioavailability, has been approved for treating abdominal pain and diarrhea by the U.S. Food and Drug administration (FDA) for patients with IBS-D.
- Given a small risk of pancreatitis associated with eluxadoline, it should not be prescribed for patients with prior cholecystectomy or significant alcohol use or prior history of pancreatitis.
- Other antidiarrheal agents that may be used in IBS patients are the bile acid binders cholestyramine or colesevelam because up to 30% of IBS-D patients may have bile acid malabsorption.
7.2 Antispasmodics¶
- Clinicians have observed that anticholinergic drugs may provide temporary relief for symptoms such as painful cramps related to intestinal spasm.
- Although controlled clinical trials have produced mixed results, evidence generally supports the beneficial effects of anticholinergic drugs for pain.
- Physiologic studies demonstrate that anticholinergic drugs inhibit the gastrocolic reflex; hence, postprandial pain is best managed by giving antispasmodics 30 min before meals so that effective blood levels are achieved shortly before the anticipated onset of pain.
- Most anticholinergics contain natural belladonna alkaloids, which may cause xerostomia, urinary hesitancy and retention, blurred vision, and drowsiness.
- They should be used in the elderly with caution.
- Some physicians prefer to use synthetic anticholinergics such as dicyclomine that have less effect on mucous membrane secretion and produce fewer undesirable side effects.
- Peppermint oil appears to reduce abdominal cramps by some undefined mechanism.
- In a meta-analysis of 10 double-blind, randomized controlled trials evaluating 1030 IBS patients, peppermint oil was found to be significantly superior to placebo for global improvement of IBS symptoms and reduction in pain.
- The most commonly reported adverse event was heartburn, which was mild and transient.
7.3 Antiflatulence Therapy¶
- The management of excessive gas is seldom satisfactory, except when there is obvious aerophagia or disaccharidase deficiency.
- Patients should be advised to eat slowly and not chew gum or drink carbonated beverages.
- Bloating may decrease if an associated gut syndrome such as IBS or constipation is improved.
- If bloating is accompanied by diarrhea and worsens after ingesting dairy products, fresh fruits, vegetables, or juices, further investigation or a dietary exclusion trial may be worthwhile.
- Avoiding gas forming foods, exercising, losing excess weight, and taking activated charcoal are safe but unproven remedies.
- A low FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diet has been shown to be quite effective in reducing gas and bloating (see "Low FODMAP Diet").
- Data regarding the use of surfactants such as simethicone are conflicting.
- Antibiotics may help in a subgroup of IBS patients with predominant symptoms of bloating.
- Beano, an over-the-counter oral β-glycosidase solution, may reduce rectal passage of gas without decreasing bloating and abdominal pain.
7.4 Antidepressant Drugs¶
- In addition to their mood-elevating effects, antidepressant medications have several physiologic effects that suggest they may be beneficial in IBS.
- In IBS-D patients, the tricyclic antidepressant imipramine slows jejunal migrating motor complex transit propagation and delays orocecal and whole-gut transit, indicative of a motor inhibitory effect.
- Some studies also suggest that tricyclic agents may alter visceral afferent neural function.
- Tricyclic antidepressants is effective in IBS patients of all subtypes.
- The beneficial effects of the tricyclic compounds in the treatment of IBS appear to be independent of their effects on depression.
- The therapeutic benefits for the bowel symptoms occur faster and at a lower dosage.
- The efficacy of antidepressant agents from other chemical classes in the management of IBS is less well evaluated.
- Selective serotonin reuptake inhibitors (SSRIs) have also been studied in patients with IBS with conflicting results and significant heterogeneity among individual trials.
7.5 Serotonin Receptor Modulators¶
- Serotonin 5-HT and 5-HT receptors are found throughout the GI tract.
- Tegaserod, a 5-HT receptor agonist, exhibits prokinetic activity by stimulating peristalsis.
- Clinical studies involving >4000 IBS-C patients reported reduction in abdominal discomfort and improvements in constipation and bloating compared to placebo.
- Diarrhea is the only major side effect.
- In 2007, the drug was voluntarily withdrawn from the market after a greater number of cardiovascular complications were observed in a database of 18,000 patients receiving tegaserod (0.11 vs 0.01% in placebo).
- In 2019, the FDA reviewed additional data and approved the use of tegaserod in women younger than 65 years old who do not have a history of ischemic cardiovascular disease and who have no more than one risk factor for cardiovascular disease.
- Lubiprostone, linaclotide, and plecanatide are secretagogues that stimulate net efflux of ions and water into the intestinal lumen and thus enhance transit and facilitate ease of defecation.
- By activating channels on the apical (luminal) enterocyte surface, these secretagogues increase intestinal chloride secretion.
- Other ion channels and transporters secrete sodium into the intestine to maintain electroneutrality, followed by the secretion of water.
- Lubiprostone is a bicyclic fatty acid derived from prostaglandin E that activates type 3 chloride channels in the apical membrane of intestinal epithelial cells.
- Oral lubiprostone was effective in the treatment of patients with IBS-C in large phase 3, randomized, double-blind, placebo-controlled multicenter trials.
- The recommended daily dose is 24 mcg twice daily.
- In general, the drug is well tolerated.
- The major side effects are nausea and diarrhea.
- Linaclotide and plecanatide are minimally absorbed 14-amino-acid peptide guanylate cyclase-C (GC-C) agonists that bind to and activate GC-C on the luminal surface of intestinal epithelium.
- The subsequent increase in cyclic guanosine monophosphate activates the cyclic fibrosis transmembrane regulator and induces fluid secretion into the GI tract.
- These drugs are similar to endogenous peptides secreted by the small intestine (uroguanylin) or colon (guanylin).
- In two 12-week, double-blind, randomized, controlled trials, linaclotide (290 or 145 μg, once daily) reduced constipation and pain.
- A lower dose (72 μg once daily) was also more effective than placebo.
- Linaclotide has been approved by the FDA for treatment of IBS-C.
- Plecanatide (3- and 6-mg doses) also has been shown to be more effective than placebo in two phase 3 trials for IBS-C.
- The 3-mg once-daily dose has been approved by the FDA.
- The only significant side effect was diarrhea, which occurred in <5% of patients.
- Tenapanor, a small-molecule inhibitor of GI sodium-hydrogen exchange-3, is more effective than placebo when given at 50 mg twice daily in patients with IBS-C and has been approved by the FDA for treatment of IBS-C.
7.6 Modulation of Gut Flora¶
- Because altered colonic flora (gut dysbiosis) may contribute to the pathogenesis of IBS, this has led to great interest in using antibiotics, prebiotics, probiotics, and dietary measures to treat IBS.
- Antibiotic treatment benefits a subset of IBS patients.
- In a double-blind, randomized, placebo-controlled study, neomycin dosed at 500 mg twice daily for 10 days was more effective than placebo at improving symptom scores among IBS patients.
- The nonabsorbed oral antibiotic studied antibiotic for the treatment of IBS.
- In two identical double-blind, placebo-controlled studies with >1200 nonconstipated IBS patients, those receiving rifaximin at a dose of 550 mg three times daily for 2 weeks were significantly more likely to report adequate relief of IBS symptoms compared with those taking placebo.
- Currently, rifaximin is approved by the FDA for treatment of IBS-D.
- Moreover, a placebo-controlled randomized clinical trial has shown that patients with IBS-D who respond to rifaximin are more likely to respond to subsequent courses of rifaximin compared to placebo if they experience relapse of symptoms.
- There have been four randomized trials to examine the effects of prebiotics.
- Three of the four studies reported that prebiotics worsened or did not improve IBS symptoms.
- This is not surprising given the adverse effects of a high-carbohydrate diet on IBS symptoms.
- These are defined as live microorganisms that when administered in adequate amounts confer a health benefit on the host.
- Multiple meta-analyses have suggested that probiotics might be an effective strategy in improving global IBS symptoms including abdominal pain and bloating; however, given the limitations of existing studies (small sample size, short duration, lack of rigorous endpoints, single-centered), it is unclear which probiotics to recommend for patients with IBS.
- Given the lack of high-quality data, the American Gastroenterological Association makes no recommendations for use of probiotics in patients with IBS.
- Large-scale studies of well-phenotyped IBS patients are needed to establish the efficacy of probiotics in IBS.
7.7 Low FODMAP Diet¶
- A diet rich in FODMAPs often triggers symptoms in IBS patients.
- FODMAPs are poorly absorbed by the small intestine and fermented by bacteria in the colon to produce gas and osmotically active carbohydrates.
- At the same time, on entering the colon, FODMAPs may serve as nutrients for the colonic bacteria and promote the growth of gram-negative commensal bacteria, which may induce barrier dysfunction and subclinical mucosal inflammation.
- Fructose and fructans induce IBS symptoms in a dose-dependent manner.
- In contrast, a low FODMAP diet reduces IBS symptoms in 50–80% of patients with IBS.
- A network meta-analysis of 13 randomized controlled trials of IBS patients found that a low FODMAP diet was superior to all other dietary interventions in reducing global IBS symptoms and primarily improves abdominal pain and bloating in patients with IBS.
Table 2 — Table 338-2 Some Common Food Sources of FODMAPs¶
| FOOD TYPE | GALACTO-FREE | FRUCTOSE | LACTOSE | FRUCTANS | OLIGOSACCHARIDES | POLYOLS |
|---|---|---|---|---|---|---|
| Fruits | Apple, cherry, mango, Peach, persimmon, watermelon | Apple, apricot, pear, avocado, pear, watermelon | blackberries, cherry, nectarine, plum, prune | Asparagus, artichokes, Artichokes, beetroot, Brussels sugar snap peas sprout, chicory, fennel, garlic, leek, onion, peas | Cauliflower, mushroom, snow peas | |
| Vegetables | ||||||
| Grains and cereals | Wheat, rye, barley | |||||
| Nuts and seeds | Pistachios | |||||
| Milk and milk products | Milk, yogurt, ice cream, custard, soft cheeses | |||||
| Legumes | Legumes, lentils, chickpeas | Legumes, chickpeas, lentils | ||||
| Other | Honey, high-fructose corn syrup | Chicory drinks | ||||
| Food additives | Inulin, FOS | Sorbitol, mannitol, maltitol, xylitol, isomalt |
8. PROGNOSIS & COMPLICATIONS¶
- Severity of symptoms varies and can significantly impair quality of life, resulting in high direct and indirect health care costs.
- IBS symptoms fluctuate over time and often overlap with other functional disorders such as fibromyalgia, headache, backache, and genitourinary symptoms.
- Sleep deprivation is also unusual because abdominal pain is almost uniformly present only during waking hours.
- Malnutrition due to inadequate caloric intake is exceedingly rare with IBS.
9. SPECIAL CONSIDERATIONS¶
- Anticholinergic drugs should be used in the elderly with caution.
- Frequent sodium phosphate–based bowel cleansing should be avoided as this is associated with hyperphosphatasemia, hypocalcemia, and hypokalemia.
- Chronic use of magnesium hydroxide may result in severe hypermagnesemia in patients with renal impairment.
- Eluxadoline should not be prescribed for patients with prior cholecystectomy or significant alcohol use or prior history of pancreatitis.
- Tegaserod should not be prescribed for patients with a history of ischemic cardiovascular disease and who have no more than one risk factor for cardiovascular disease.
10. KEY PEARLS & CLINICAL TRAPS¶
- Abdominal pain is essential for diagnosing IBS. Painless diarrhea or constipation does not fulfill the diagnostic criteria to be classified as IBS.
- Supportive symptoms that are not part of the diagnostic criteria include straining, urgency or a feeling of incomplete defecation, passing mucus, and bloating.
- Weight loss, nocturnal symptoms, and bleeding per rectum are not common in patients with IBS and, when present, should warrant evaluation for other causes.
- Alarm features (age >40 onset, weight loss, nocturnal symptoms, rectal bleeding, anemia, elevated sedimentation rate, leukocytes or blood in stool, stool volume >200–300 mL/d) argue against IBS and warrant colonoscopy.
- Soluble fiber (psyllium) is preferred over insoluble fiber (wheat bran) to avoid exacerbating bloating and pain.
- Low FODMAP diet reduces global IBS symptoms in 50–80% of patients.
- Rifaximin is effective for IBS-D, particularly in patients with bloating and gas.
- Postinfectious IBS occurs in >10% of patients with infectious enteritis, with risk 4-fold higher than non-infected individuals.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 338-2 Changes in gut microbiota among patients with irritable bowel syndrome (IBS). (Adapted from R Pittayanon et al: Gastroenterology 157:97, 2019.) — Figure 338-1: Pathophysiology of irritable bowel syndrome (IBS). Diagram illustrating multifactorial causes including visceral hypersensitivity, abnormal motility, central neural dysregulation, psychological disturbances, mucosal inflammation, stress, bile acid malabsorption, and gut dysbiosis. Shows connections between the gut-brain axis, HPA axis, autonomic dysfunction, and genetic factors.
Figure 2¶
Caption: FIGURE 338-1 Pathophysiology of irritable bowel syndrome (IBS). The cause of IBS to be multifactorial. Patients often show evidence of visceral hypersensitivity and abnormalities. Many IBS patients have increased anxiety and/or depression, and their are often exacerbated by mental or physical stress, suggesting abnormal brain–gut Genetic studies suggest a few IBS patients may have genetic abnormalities serotonin transport system in the enteric nerves. Up to 30% of IBS patients may have malabsorption. Gut dysbiosis and impaired mucosa permeability also have been reported IBS patients. This may lead to subclinical mucosa inflammation. HPA, adrenal; SERT, serotonin reuptake transporter. — Figure 338-2: Changes in gut microbiota among patients with irritable bowel syndrome (IBS). Bar chart comparing relative abundance of bacterial genera (Lactobacillaceae, Bacteroides, Enterobacteriaceae, Bifidobacterium, Faecalibacterium) in healthy controls versus IBS patients, showing decreased diversity and specific shifts in IBS microbiome.
Figure 3¶

Caption: FIGURE 338-4 Pathogenesis of FODMAP-related symptoms. FODMAPs are poorly osmotically active carbohydrates. These events act in concert to cause bloating, which may induce mucosal changes such as mast cell activation and barrier oligosaccharides, disaccharides, monosaccharides, and polyols; LPS, — Figure 338-3: Gut dysbiosis and irritable bowel syndrome (IBS). Schematic diagram showing how gut dysbiosis acting with genetic and environmental factors alters intestinal permeability, increases antigen presentation, activates mast cells, and releases cytokines/chemokines that alter neuronal and smooth-muscle function causing IBS symptoms.
Figure 4¶

Caption: FIGURE 338-3 Gut dysbiosis and irritable bowel syndrome (IBS). Gut dysbiosis acting in and increase antigen presentation, resulting in mast cell activation. Products of mast symptoms. The cytokines and chemokines generated from mucosal inflammation GI, gastrointestinal. (Adapted from NJ Talley, AA Fodor: Gastroenterology 141:1555, 2011.) — Figure 338-4: Low FODMAP diet mechanism. Illustration of how FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are poorly absorbed in the small intestine, fermented by colonic bacteria to produce gas and osmotically active carbohydrates, leading to symptoms. Shows how a low FODMAP diet reduces these triggers.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.