Chapter 63 | Cutaneous Drug Reactions¶
Harrison's Principles of Internal Medicine, 22nd Edition · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Cutaneous reactions account for 10–15% of reported adverse drug reactions; most are benign, but some are life-threatening.
- Severe cutaneous adverse reactions (SCARs) include SJS/TEN, DRESS, and AGEP; incidence is 1 in 1000 to 2 per million users.
- HLA-B*57:01 screening is recommended before abacavir to prevent hypersensitivity (100% negative predictive value).
- HLA-B*15:02 is associated with carbamazepine-induced SJS/TEN in Han Chinese populations.
- HLA-B*58:01 is associated with allopurinol-induced DRESS/SJS/TEN in Han Chinese populations.
- Morbilliform eruptions are the most common drug reaction (91% of acute cutaneous reactions in hospitalized patients).
- Photosensitivity reactions are usually phototoxic and occur in sun-exposed areas; NSAIDs and fluoroquinolones are common causes.
- Warfarin necrosis occurs in 0.01–0.1% of patients, typically in women, between days 3–10 of therapy.
- Immune checkpoint inhibitors (ICIs) induce immune-related adverse events (irAEs) in 30–60% of patients; management depends on severity.
- Drug-induced hair loss (anagen effluvium) occurs within days of chemotherapy; telogen effluvium occurs 2–4 months after initiation.
- Drug-induced nail changes (onycholysis, onychomadesis) usually involve all 20 nails and need months to resolve.
- Diagnosis of morbilliform eruptions is rarely assisted by laboratory testing or skin biopsy; absence of enanthems supports drug etiology.
- Management of severe reactions requires drug withdrawal, symptomatic treatment (antihistamines, emollients), and systemic corticosteroids for severe cases.
- Nonimmunologic reactions include pigmentation changes, photosensitivity, and exacerbation of preexisting dermatologic diseases.
- Immunologic reactions include Type I (IgE-mediated), Type II (cytotoxic), Type III (immune complex), and Type IV (T-cell mediated).
- Type IV reactions are further subdivided into IVa (macrophage), IVb (eosinophil), and IVc (neutrophil) pathways.
- Genetic factors (HLA alleles) and drug metabolism (e.g., CYP2C9*3) influence risk of severe hypersensitivity reactions.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification of Adverse Drug Reactions
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors
- 2.2 Incidence of Severe Cutaneous Adverse Reactions (SCARs)
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Nonimmunologic Drug Reactions
- 3.2 Immunologic Drug Reactions
- 3.3 Genetic Factors and Cutaneous Drug Reactions
- 3.4 Global Considerations
- 4. CLINICAL FEATURES
- 4.1 Photosensitivity Eruptions
- 4.2 Pigmentation Changes
- 4.3 Drug-Induced Hair Disorders
- 4.4 Drug-Induced Nail Disorders
- 4.5 Warfarin Necrosis of Skin
- 4.6 Toxic Erythema of Chemotherapy
- 4.7 Exacerbation or Induction of Dermatologic Diseases
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Viral Exanthem vs. Drug Eruption
- 5.2 Graft-versus-Host Disease
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Laboratory Testing
- 6.2 Genetic Screening
- 7. MANAGEMENT & TREATMENT
- 7.1 Morbilliform Drug Eruption
- 7.2 Urticaria/Angioedema/Anaphylaxis
- 7.3 Pruritus
- 7.4 Immune Checkpoint Inhibitor irAEs
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Resolution and Sequelae
- 8.2 Risk Populations
- 9. SPECIAL CONSIDERATIONS
- 9.1 Genetic Screening
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Board Exam Favorites
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Cutaneous reactions are the most frequent adverse reactions to medications, representing 10–15% of reported adverse drug reactions. Most are benign, but a few can be life threatening. Prompt recognition of severe reactions, drug withdrawal, and appropriate therapeutic interventions can minimize toxicity. This chapter focuses on adverse cutaneous reactions to systemic medications; it covers their incidence, patterns, and pathogenesis, and provides some practical guidelines on treatment, assessment of causality, and future use of drugs.
1.1 Classification of Adverse Drug Reactions¶
Adverse cutaneous responses to drugs can arise as a result of immunologic or nonimmunologic mechanisms. Immediate reactions depend on the release of mediators of inflammation by tissue mast cells or circulating basophils. Delayed reactions are typically T-cell mediated. The revised classification of adverse drug reactions based on immune pathway is provided in Table 63-1.
Table 1 — Table 63-1 Revised Classification of Adverse Drug Reactions Based on Immune Pathway¶
| TYPE | KEY PATHWAY | KEY IMMUNE MEDIATORS | ADVERSE DRUG REACTION TYPE |
|---|---|---|---|
| Antibody Mediated | Type I | IgE, immediate (IgE, B cells, T2, ILC2; IL-4, IL-5, IL-9, IL-13; Mast cells, basophils) | Acute urticaria, angioedema, anaphylaxis |
| Type II | IgG-mediated cytotoxicity | IgG, B cells, IgM; Phagocytes, neutrophils, macrophages; Complement-dependent cytotoxicity, NK (antibody-dependent cellular cytotoxicity) | Drug-induced cytopenia (e.g. hemolysis, thrombocytopenia secondary to penicillin) |
| Type III | Immune complexes | IgG + antigen (immune complexes); B cells, IgM, IgG; Complement, basophils, mast cells, platelets, Neutrophils, monocytes, macrophages | Serum sickness, Arthus reaction, drug-induced vasculitis and lupus |
| Cell-Mediated (T-cell mediated) (Delayed Hypersensitivity) | Type IVa | T lymphocyte–mediated macrophage inflammation and cytotoxic functions of T cells; T1 cells, ILC1, Tc1, NK; IFN-γ, TNF-α, granzyme B, perforins, granulysin; Macrophages (granulomas) | SJS/TEN, erythema multiforme, allergic contact dermatitis, fixed drug eruption, drug induced liver injury |
| Type IVb | T lymphocyte–mediated eosinophil inflammation | T2 cells, ILC2, Tc2, NK-T; IL-4, IL-5, IL-9, IL-13, IL-31; Eosinophils, B cells, mast cells/basophils | DIHS/DRESS; Morbilliform eruption |
| Type IVc | T lymphocyte–mediated neutrophil inflammation | TH17, ILC3, Tc17; IL17, IL-22, IL-23, CXCL8, GM-CSF; Neutrophils | AGEP |
2. EPIDEMIOLOGY¶
In the United States, more than 6.7 billion prescriptions for >20,000 drug products are dispensed annually. Hospital inpatients alone annually receive about 120 million courses of drug therapy, and approximately two-thirds of adult Americans receive prescription drugs on a regular outpatient basis. Adverse effects of a prescription medication may result in 4.5 million urgent or emergency care visits and over 7000 deaths each year in the United States. Several prospective studies reported that acute cutaneous reactions to drugs affect between 2.2 and 10 per 1000 hospitalized patients. Reactions usually occur a few days to 4 weeks after initiation of therapy. In a series of 48,005 inpatients over a 20-year period, morbilliform rash (91%) and urticaria (6%) were the most frequent skin reactions, and antimicrobials, radiocontrast, and nonsteroidal anti-inflammatory drugs (NSAIDs) were the most common drug associations. Severe hypersensitivity reactions to medications have been reported to occur in between 1 in 1000 and 2 per million users, depending on the reaction type.
2.1 Risk Factors¶
Some populations are at increased risk of drug reactions, including elderly patients, patients with autoimmune disease, hematopoietic stem cell transplant recipients, and those with acute Epstein-Barr virus (EBV) or human immunodeficiency virus (HIV) infection. The pathophysiology underlying this association may be related to immune dysregulation. Individuals with advanced HIV disease that is not virologically suppressed (e.g., CD4+ T lymphocyte count <200 cells/μL) have a 40- to 50-fold increased risk of adverse reactions to sulfamethoxazole and increased risk of severe hypersensitivity reactions to medications overall.
2.2 Incidence of Severe Cutaneous Adverse Reactions (SCARs)¶
Severe cutaneous reactions to drugs have an important impact on health because of significant sequelae; in addition, they may require hospitalization, increase the duration of hospital stay, or be life-threatening. The incidence of SCARs varies by reaction type and population.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
The pathophysiology underlying cutaneous drug reactions is complex and involves immunologic and nonimmunologic mechanisms. Immediate reactions depend on the release of mediators of inflammation by tissue mast cells or circulating basophils. Delayed reactions are typically T-cell mediated. Genetic factors and global considerations also play a role.
3.1 Nonimmunologic Drug Reactions¶
Examples of nonimmunologic cutaneous drug reactions are pigmentationary changes due to dermal accumulation of medications or their metabolites or alteration of hair follicles by antimetabolites and signaling inhibitors. These side effects are predictable and sometimes can be prevented. These reactions usually manifest in the skin and gastrointestinal, respiratory, and cardiovascular systems. Primary symptoms and signs include pruritus, urticaria, nausea, vomiting, abdominal cramps, bronchospasm, laryngeal edema, and, occasionally, anaphylactic or shock with hypotension and death. They occur within minutes of drug exposure. Aspirin, NSAIDs, radiocontrast media, opiates, and some antibiotics (fluoroquinolones, vancomycin) are frequent causes of non–IgE-mediated mast cell activation, which can occur on first exposure, is dose-related, and can be variable in occurrence with multiple exposures over time. Penicillins and cephalosporins (e.g., cefazolin) are the most frequent causes of IgE-dependent reactions to drugs, requiring prior sensitization. When IgE-mediated reactions occur, they typically occur secondary to a haptenated product of the parent drug or metabolite but occasionally can be due to an IgE-mediated response against an inactive excipient of the drug (e.g., polyethylene glycol 3350 in injectable methylprednisolone acetate). Release of mediators is common triggered when polyvalent drug protein conjugates cross-link IgE molecules fixed to sensitized cells. Certain routes of administration favor different clinical patterns (e.g., gastrointestinal effects from oral route, circulatory effects from intravenous route).
3.2 Immunologic Drug Reactions¶
Evidence suggests a direct immunologic basis for most acute drug eruptions. Drug reactions such as urticaria or anaphylaxis may result from immediate release of preformed mediators. Such reactions may be antibody-mediated through an adaptive immune response. Alternatively, they may result from complement activation or direct activation of a mast cell receptor such as the mast-related G-protein–coupled receptor-2 (MRGPRX2) that is not associated with immune memory. T-cell–mediated reactions typically manifest with a delayed exanthem. Drug-specific CD4+ and CD8+ T-cell clones can be derived from the blood or from skin lesions of such patients, suggesting these T cells mediate drug allergy in an antigen-specific manner. For severe cutaneous adverse reactions (SCARs) such as drug-induced hypersensitivity syndrome (DIHS), also known as drug reaction with eosinophilia and systemic symptoms (DRESS), and Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), drug presentation to T cells is major histocompatibility complex (MHC)-restricted and likely involves drug-peptide complex recognition by specific T-cell receptors (TCRs). Once a drug has induced an immune response, the phenotype of the reaction is determined by the nature of effectors: cytotoxic (CD8+) T cells in blistering and certain hypersensitivity reactions, chemokines for reactions mediated by neutrophils or eosinophils, and B-cell collaboration for production of specific antibodies for urticarial reactions. There has been consideration for reclassification of hypersensitivity reactions into antibody and cell-mediated processes that are directly driven by inflammation and the immune system, tissue driven mechanisms, and those mediated through a direct response to chemicals (Table 63-1 and Fig. 63-1).
3.3 Genetic Factors and Cutaneous Drug Reactions¶
Current knowledge suggests that genetic determinants may predispose individuals to severe drug reactions by affecting immune responses to drugs and, in some cases, through altered drug metabolism. Associations between T-cell–mediated delayed drug hypersensitivities and specific class I HLA alleles suggest a key role for immune mechanisms, especially those leading to severe skin or systemic organ involvement, such as SJS/TEN, DIHS/DRESS, abacavir hypersensitivity (AHS), drug-induced liver injury, pancreatitis, or agranulocytosis. Hypersensitivity to the anti-HIV medication abacavir is strongly associated with HLA-B57:01. HLA-B57:01 has 100% negative predictive value for the development of AHS, and routine preprescription screening for HLA-B57:01 has eliminated AHS as a clinical entity. In Taiwan, within a homogeneous Han Chinese population, a strong association was observed between SJS/TEN (but not DIHS/DRESS) related to carbamazepine and HLA-B15:02. In the same population, a strong association was found between HLA-B58:01 and both DIHS/DRESS and SJS/TEN associated with allopurinol. Other notable HLA associations include HLA-B13:01 and dapsone or sulfonamide antibiotic-induced DIHS/DRESS and SJS/TEN, as well as HLA-A32:01 and vancomycin-induced DIHS/DRESS. These associations are drug and phenotype specific; that is, HLA-specific T-cell stimulation by medications leads to distinct reactions. However, while these HLA associations are extremely strong, the presence of a risk HLA allele alone is not sufficient to cause severe drug hypersensitivity reactions. Other factors outside of the MHC, such as drug metabolism (e.g., CYP2C93 slow metabolism status and risk of phenytoin-induced morbilliform drug eruption, DIHS/DRESS, and SJS/TEN), are also important. The entirety of genetic and ecological factors that define why the majority of individuals carrying an HLA risk allele remain drug-tolerant and those factors that drive risk for specific drug hypersensitivity reactions are not known at this time.
3.4 Global Considerations¶
The PREDICT-1 study was a randomized, double-blind clinical trial of real-time preprescription HLA-B57:01 screening versus the previous standard of care of no screening that provided the basis for the utility of HLA-B57:01 screening to prevent AHS. If an HLA risk allele is present, it seems to have the same implication regardless of the population. This generalizability across populations, the fact that self-identified race is a social rather than biological construct, and greater availability of less costly single-HLA assays with a shorter turnaround time argue against targeted genetic screening on the basis of self-identified race. The American College of Rheumatology has recommended HLA-B58:01 screening of Han Chinese patients prescribed allopurinol; however, HLA-B58:01 does not have 100% negative predictive value for allopurinol DIHS/DRESS or SJS/TEN in other populations, and safety monitoring and risk counseling remain imperative. To date, screening for a single HLA (but not multiple HLA haplotypes) in specific populations has been determined to be cost-effective (e.g., HLA-B*1301 screening in Chinese patients with leprosy treated with dapsone). Genetic testing for specific HLA haplotypes is becoming more widely available, and its utility will increase as mechanistic factors driving drug hypersensitivity and tolerance are elucidated. Further data are needed to clarify the role of genetic and other testing beyond screening (e.g., in diagnosis) in order to optimize cost-effectiveness, utility, and benefit.
4. CLINICAL FEATURES¶
A variety of skin diseases can be induced or exacerbated by medications (e.g., pruritus, pigmentation, nail or hair disorders, psoriasis, bullous pemphigoid, photosensitivity, and even cutaneous neoplasms). These drug reactions are not frequent; however, neither their incidence nor their impact on public health has been evaluated. In addition to acute eruptions, a variety of skin diseases can be induced or exacerbated by medications. The hypothesis that a drug may be responsible should always be considered, even after treatment is complete. In addition, reactions may develop in cases of long-term medication therapy due to changes in dosing or host metabolism. Resolution of the cutaneous reaction may be delayed upon discontinuation of the medication.
4.1 Photosensitivity Eruptions¶
Photosensitivity eruptions are usually most marked in sun-exposed areas, but they may extend to sun-protected sites. The mechanism is almost always phototoxicity. Phototoxic reactions resemble sunburn and can occur with first exposure to a drug. Blistering may occur in drug-related pseudoporphyria, most commonly with NSAIDs. The severity of the reaction depends on the tissue level of the drug, its efficiency as a photosensitizer, and the extent of exposure to the activating wavelengths of ultraviolet (UV) light. Common orally administered photosensitizing drugs include fluoroquinolones, tetracycline antibiotics, and trimethoprim/sulfamoxazole. Other drugs less frequently implicated are chlorpromazine, thiazides, NSAIDs, and BRAF inhibitors. Voriconazole may result in severe photosensitivity, accelerated photoaging, and cutaneous carcinogenesis. Hydrochlorothiazide may be associated with increased nonmelanoma skin cancer in some populations. Because UV-A and visible light, which trigger these reactions, are not easily absorbed by nonopaque sunscreens and are transmitted through window glass, photosensitivity reactions may be difficult to prevent. Photosensitivity reactions abate with removal of either the drug or UV radiation, use of sunscreens that block UV-A light, and treatment of the reaction as one would a sunburn. Rarely, individuals develop persistent reactivity to light, necessitating long-term avoidance of sun exposure. Some chemotherapeutic agents, such as methotrexate, can induce a UV-recall reaction characterized by an erythematous, slightly scaly eruption at sites of prior severe photosensitivity reactions.
4.2 Pigmentation Changes¶
Drugs, either systemic or topical, may cause a variety of pigmentary changes in the skin by triggering melanocyte production of melanin (as in the case of oral contraceptives causing melasma) or due to deposition of drug or drug metabolites. Long-term minocycline or amiodarone exposure may cause blue-gray pigmentation. Phenothiazine, gold, and bismuth result in gray-brown pigmentation of sun-exposed areas. Numerous cancer chemotherapeutic agents may be associated with characteristic patterns of pigmentation (e.g., bleomycin, busulfan, daunorubicin, cyclophosphamide, hydroxyurea, fluorouracil, and methotrexate). Clofazimine causes a drug-induced lipofuscinosis with characteristic red-brown coloration. Hyperpigmentation of the face, mucous membranes, and pretibial and subungual areas occurs with antimalarials. Quinacrine causes generalized yellow discoloration. Pigmentation changes may also occur in mucous membranes (busulfan, bismuth), conjunctiva (chlorpromazine, thioridazine, imipramine, clomipramine), nails (zidovudine, doxorubicin, cyclophosphamide, bleomycin, fluorouracil, hydroxyurea), hair, and teeth (tetracyclines).
4.3 Drug-Induced Hair Disorders¶
Medications may affect hair follicles at two different phases of their growth cycle: anagen (growth) or telogen (resting). Anagen effluvium occurs within days of drug administration, especially with antimetabolite or other chemotherapeutic drugs. In contrast, in telogen effluvium, the delay is 2–4 months following initiation of a new medication. Both present as diffuse, nonscarring alopecia, most often reversible after discontinuation of the responsible agent. A considerable number of drugs have been associated with hair loss. These include antineoplastic agents (alkylating agents, bleomycin, vinca alkaloids, platinum compounds), anticonvulsants (carbamazepine, valproate), beta blockers, antidepressants, antithyroid drugs, IFNs, oral contraceptives, and cholesterol-lowering agents. Medications may also cause hair growth. Hirsutism is an excessive growth of terminal hair with masculine hair growth pattern in a female, most often on the face and trunk, due to androgenic stimulation of hormone-sensitive hair follicles (anabolic steroids, oral contraceptives, testosterone, corticotropin). Hypertrichosis is a distinct pattern of hair growth, not in a masculine pattern, typically located on the forehead and temporal regions of the face. Drugs responsible for hypertrichosis include anti-inflammatory drugs, glucocorticoids, vasodilators (diazoxide, minoxidil), diuretics (acetazolamide), anticonvulsants (phenytoin), immunosuppressive agents (cyclosporine A), psoralens, and zidovudine. Changes in hair color or structure are uncommon adverse effects from medications. Hair discoloration may occur with chloroquine, IFN-α, chemotherapeutic agents, and tyrosine kinase inhibitors. Changes in hair structure have been observed in patients given EGFR inhibitors, BRAF inhibitors, tyrosine kinase inhibitors, and acitretin.
4.4 Drug-Induced Nail Disorders¶
Drug-related nail disorders usually involve all 20 nails and need months to resolve after withdrawal of the medication. The pathogenesis is most often toxic. Drug-induced nail changes include Beau lines (transverse depression of the nail plate), onycholysis (detachment of the distal part of the nail plate), onychomadesis (detachment of the proximal part of the nail plate), pigmentation, and paronychia (inflammation of periungual skin). Onycholysis occurs with tetracyclines, fluoroquinolones, retinoids, NSAIDs, and others, including many chemotherapeutic agents, and may be triggered by exposure to sunlight. Onychomadesis is caused by temporary arrest of nail matrix mitotic activity. Common drugs reported to induce onychomadesis include carbamazepine, lithium, retinoids, and chemotherapeutic agents such as taxanes. Paronychia and multiple pyogenic granulomas with progressive and painful periungual abscess of fingers and toes are side effects of systemic retinoids, lamivudine, indinavir, and EGFR inhibitors. Nail discoloration: Some drugs—including anthracyclines, taxanes, fluorouracil, psoralens, and zidovudine—may induce nail bed hyperpigmentation through melanocyte stimulation. It appears to be reversible and dose dependent.
4.5 Warfarin Necrosis of Skin¶
This rare reaction (0.01–0.1%) usually occurs between the third and tenth days of therapy with warfarin, usually in women. Common sites are breasts, thighs, and buttocks. Lesions are sharply demarcated, erythematous, purpuric, and may progress to form large, hemorrhagic bullae with necrosis and eschar formation. Warfarin anticoagulation in protein C or S deficiency causes an additional reduction in already low circulating levels of endogenous anticoagulants, permitting temporary hypercoagulability and thrombosis in the cutaneous microvasculature, with consequent areas of necrosis. Heparin-induced necrosis may have clinically similar features but is probably due to heparin-induced platelet aggregation with subsequent occlusion of blood vessels; it can affect areas adjacent to the injection site or more distant sites if infused. Levamisole-tainted cocaine (and more recently, opiates) can induce similar skin necrosis; however, the distribution tends to involve the ears and cheeks predominantly, with stellate or retiform purpura. Patients may have abnormal white blood cell counts and may be dual P- and C-ANCA positive.
4.6 Toxic Erythema of Chemotherapy¶
Because many agents used in cancer chemotherapy inhibit cell division, rapidly proliferating elements of the skin, including hair, mucous membranes, and appendages, are sensitive to their effects. A broad spectrum of chemotherapy-related skin toxicities has been reported, including neutrophilic eccrine hidradenitis, sterile cellulitis, exfoliative dermatitis, and flexural erythema. These reactions are best characterized under the unifying term “toxic erythema of chemotherapy” (TEC). Acral erythema is marked by dysesthesia and an erythematous, edematous eruption of the palms and soles. Common causes include cytarabine, doxorubicin, methotrexate, hydroxyurea, fluorouracil, and capecitabine. The introduction of many new monoclonal antibody and small-molecule signaling inhibitors for the treatment of cancer has been accompanied by numerous reports of skin and hair toxicity; only the most common of these are mentioned here. EGFR antagonists induce follicular eruptions and nail toxicity after a mean interval of 10 days in a majority of patients. Xerosis, eczematous eruptions, acneiform eruptions, and pruritus are common. Erlotinib is associated with marked hair textural changes. Sorafenib, a tyrosine kinase inhibitor, may result in follicular eruptions and focal bullous eruptions at palmoplantar, flexural sites, or areas of pressure or friction. BRAF inhibitors are associated with photosensitivity, palmoplantar hyperkeratosis, hair curling, dyskeratotic (Grover-like) rash, hyperkeratotic benign cutaneous neoplasms, and keratoacanthoma-like squamous cell carcinomas. The immune checkpoint inhibitor (ICI) class of drugs (including anti-CTLA-4, anti-PD-1, and anti-PD-L1 agents) can induce a wide range of cutaneous eruptions, including lichenoid, eczematous, granulomatous, papulosquamous, bullous, vitiligo-like, alopecic, and panniculitic eruptions. Mucocutaneous immune-related adverse events (irAEs) to ICIs typically occur early and are the most common of potentially multiorgan reactions, occurring in 30–60% of patients. The onset may be as early as a few weeks after initiating the ICI and as late as 1 year or more after initiation. The incidence of irAEs differs between the distinct ICI medications and is most frequent with combination therapy with anti-CTLA-4 and anti-PD-1 agents. Severe irAEs (grade 3 or 4, including DIHS/DRESS, SJS/TEN-like, and bullous reactions involving over 30% body surface area) are rare, occurring in 2–3% of patients with ICI monotherapy and up to 15% with combined ICI therapy. The rates of irAEs may also differ between patient populations depending on the type of malignancy being treated. These reactions are largely T-cell–mediated, which informs the approach to management. Whereas milder reactions may be managed with topical corticosteroids, more severe reactions may require oral corticosteroids or other systemic immunomodulatory or immunosuppressive medications, including biologic agents. In some cases of severe reactions, including lichenoid bullous and SJS/TEN-like reactions, rechallenge of the ICI may be possible. A clear history of all new medications introduced within the few days to 2 months preceding the reaction should be taken, as case reports of ICIs increasing the risk of small-molecule SCAR have emerged. There are some data, largely retrospective studies, supporting the notion that mucocutaneous irAEs may be associated with improved prognosis and survival.
4.7 Exacerbation or Induction of Dermatologic Diseases¶
Several medications induce or exacerbate autoimmune disease. Checkpoint inhibitors induce a wide array of systemic autoimmune reactions, including in skin (see below). Interleukin (IL) 2, IFN-α, and anti-TNF-α are associated with new-onset systemic lupus erythematosus (SLE). Drug-induced lupus is classically marked by antinuclear and antihistone antibodies and, in some cases, anti-double-stranded DNA (D-penicillamine, anti-TNF-α) or perinuclear antineutrophil cytoplasmic antibodies (p-ANCA) (minocycline). Subacute cutaneous lupus erythematosus (SCLE) can be induced by a growing list of drugs, including thiazide diuretics, proton pump inhibitors, TNF inhibitors, terbinafine, and minocycline. Drug-induced dermatomyositis may rarely occur with TNF inhibitors or capecitabine, and flares have been reported in association with the herbal supplement spirulina. Hydroxyurea can induce skin findings of dermatomyositis. IFN and TNF inhibitors, as well as BRAF inhibitors and checkpoint inhibitors, can induce granulomatous disease and sarcoidosis. Autoimmune blistering diseases may be drug induced as well: pemphigus by D-penicillamine and ACE inhibitors; bullous pemphigoid by furosemide and, increasingly, by DPP4 inhibitors and PD-1 inhibitors; and linear IgA bullous dermatosis by vancomycin. Other medications may cause highly specific cutaneous reactions. Gadolinium contrast has been associated with nephrogenic systemic fibrosis, a condition of sclerosing skin and rare internal organ involvement, in the setting of renal compromise. Granulocyte colony-stimulating factor, azacitidine, all-trans-retinoic acid, the FLT3 inhibitor class of drugs, and (rarely) levamisole-contaminated cocaine may induce neutrophilic dermatoses.
5. DIFFERENTIAL DIAGNOSIS¶
Diagnosis of morbilliform eruptions is rarely assisted by laboratory testing or skin biopsy. Absence of enanthems; absence of ear, nose, throat, and upper respiratory tract symptoms; and polymorphism of the skin lesions support a drug rather than a viral eruption. A viral exanthem is a differential diagnostic consideration, especially in children, and graft-versus-host disease is also a consideration in the proper clinical setting. Certain medications carry very high rates of morbilliform eruption, including nevirapine and lamotrigine, even in the absence of DIHS/DRESS reactions. Lamotrigine morbilliform rash is associated with higher starting doses, rapid dose escalation, concomitant use of valproate, and in patients with a history of rash to other drugs. Radiocontrast agents are a common cause of urticaria and angioedema. Certain medications carry very high rates of morbilliform eruption, including nevirapine and lamotrigine, even in the absence of DIHS/DRESS reactions. Lamotrigine morbilliform rash is associated with higher starting doses, rapid dose escalation, concomitant use of valproate, and in patients with a history of rash to other drugs.
5.1 Viral Exanthem vs. Drug Eruption¶
A viral exanthem is a differential diagnostic consideration, especially in children, and graft-versus-host disease is also a consideration in the proper clinical setting. Absence of enanthems; absence of ear, nose, throat, and upper respiratory tract symptoms; and polymorphism of the skin lesions support a drug rather than a viral eruption.
5.2 Graft-versus-Host Disease¶
Graft-versus-host disease is also a consideration in the proper clinical setting. This is particularly relevant in patients who have received hematopoietic stem cell transplants.
6. INVESTIGATIONS & DIAGNOSIS¶
Diagnosis of morbilliform eruptions is rarely assisted by laboratory testing or skin biopsy. Absence of enanthems; absence of ear, nose, throat, and upper respiratory tract symptoms; and polymorphism of the skin lesions support a drug rather than a viral eruption. Certain medications carry very high rates of morbilliform eruption, including nevirapine and lamotrigine, even in the absence of DIHS/DRESS reactions. Lamotrigine morbilliform rash is associated with higher starting doses, rapid dose escalation, concomitant use of valproate, and in patients with a history of rash to other drugs. Radiocontrast agents are a common cause of urticaria and angioedema. Certain medications carry very high rates of morbilliform eruption, including nevirapine and lamotrigine, even in the absence of DIHS/DRESS reactions. Lamotrigine morbilliform rash is associated with higher starting doses, rapid dose escalation, concomitant use of valproate, and in patients with a history of rash to other drugs.
6.1 Laboratory Testing¶
Laboratory testing is rarely helpful in diagnosing morbilliform eruptions. However, in cases of suspected DIHS/DRESS, liver function tests, complete blood count with differential, and eosinophil count are recommended. In cases of suspected SJS/TEN, skin biopsy may show full-thickness epidermal necrosis with minimal inflammation. In cases of suspected drug-induced lupus, antinuclear antibodies and anti-histone antibodies are recommended. In cases of suspected drug-induced vasculitis, complement levels and immunofluorescence may be helpful.
6.2 Genetic Screening¶
Genetic testing for specific HLA haplotypes is becoming more widely available, and its utility will increase as mechanistic factors driving drug hypersensitivity and tolerance are elucidated. Further data are needed to clarify the role of genetic and other testing beyond screening (e.g., in diagnosis) in order to optimize cost-effectiveness, utility, and benefit. The PREDICT-1 study was a randomized, double-blind clinical trial of real-time preprescription HLA-B57:01 screening versus the previous standard of care of no screening that provided the basis for the utility of HLA-B57:01 screening to prevent AHS. If an HLA risk allele is present, it seems to have the same implication regardless of the population. This generalizability across populations, the fact that self-identified race is a social rather than biological construct, and greater availability of less costly single-HLA assays with a shorter turnaround time argue against targeted genetic screening on the basis of self-identified race. The American College of Rheumatology has recommended HLA-B58:01 screening of Han Chinese patients prescribed allopurinol; however, HLA-B58:01 does not have 100% negative predictive value for allopurinol DIHS/DRESS or SJS/TEN in other populations, and safety monitoring and risk counseling remain imperative. To date, screening for a single HLA (but not multiple HLA haplotypes) in specific populations has been determined to be cost-effective (e.g., HLA-B*1301 screening in Chinese patients with leprosy treated with dapsone).
7. MANAGEMENT & TREATMENT¶
Prompt recognition of severe reactions, drug withdrawal, and appropriate therapeutic interventions can minimize toxicity. Management of morbilliform eruptions includes discontinuation of the offending drug, symptomatic treatment with antihistamines and emollients, and systemic corticosteroids for severe cases. Management of urticaria/angioedema/anaphylaxis includes discontinuation of the offending drug, antihistamines, and epinephrine for anaphylaxis. Management of ICI irAEs depends on severity; milder reactions may be managed with topical corticosteroids, more severe reactions may require oral corticosteroids or other systemic immunomodulatory or immunosuppressive medications, including biologic agents. In some cases of severe reactions, including lichenoid bullous and SJS/TEN-like reactions, rechallenge of the ICI may be possible. A clear history of all new medications introduced within the few days to 2 months preceding the reaction should be taken, as case reports of ICIs increasing the risk of small-molecule SCAR have emerged. There are some data, largely retrospective studies, supporting the notion that mucocutaneous irAEs may be associated with improved prognosis and survival.
7.1 Morbilliform Drug Eruption¶
Morbilliform or maculopapular drug eruptions (Fig. 63-5) are the most common of all drug-induced reactions, often start on the trunk or intertriginous areas, and consist of blanching erythematous macules and papules that are symmetric and confluent. Nonblanching, dusky, or bright-red macules, as well as mucosal involvement, should raise concern for a more severe reaction. Facial involvement in morbilliform eruptions is also uncommon, and the presence of extensive facial lesions with facial edema suggests DIHS/DRESS. Diagnosis of morbilliform eruptions is rarely assisted by laboratory testing or skin biopsy. Morbilliform drug eruptions may be associated with moderate to severe pruritus and fever. A viral exanthem is a differential diagnostic consideration, especially in children, and graft-versus-host disease is also a consideration in the proper clinical setting. Absence of enanthems; absence of ear, nose, throat, and upper respiratory tract symptoms; and polymorphism of the skin lesions support a drug rather than a viral eruption. Common offenders include aminopenicillins, cephalosporins, antibacterial sulfonamides, allopurinol, and antiepileptic drugs. Beta blockers, calcium channel blockers, and ACE inhibitors are rarely the culprit; however, any drug can cause a morbilliform exanthem. Certain medications carry very high rates of morbilliform eruption, including nevirapine and lamotrigine, even in the absence of DIHS/DRESS reactions. Lamotrigine morbilliform rash is associated with higher starting doses, rapid dose escalation, concomitant use of valproate, and in patients with a history of rash to other drugs. Radiocontrast agents are a common cause of urticaria and angioedema. Certain medications carry very high rates of morbilliform eruption, including nevirapine and lamotrigine, even in the absence of DIHS/DRESS reactions. Lamotrigine morbilliform rash is associated with higher starting doses, rapid dose escalation, concomitant use of valproate, and in patients with a history of rash to other drugs. Management includes discontinuation of the offending drug, symptomatic treatment with antihistamines and emollients, and systemic corticosteroids for severe cases.
7.2 Urticaria/Angioedema/Anaphylaxis¶
Urticaria, the second most frequent type of cutaneous reaction to drugs, is characterized by pruritic, red wheals of varying size rarely lasting more than 24 hours. It has been observed in association with nearly all drugs, most frequently aspirin, NSAIDs, penicillin, and blood products. However, medications account for no more than 10–20% of acute urticaria cases. Deep edema within dermal and subcutaneous tissues is known as angioedema and may involve respiratory and gastrointestinal mucous membranes. Urticaria and angioedema may be part of a life-threatening anaphylactic reaction. Drug-induced urticaria may be caused by three mechanisms: an IgE-dependent mechanism, circulating immune complexes (serum sickness), and nonimmunologic activation of effector pathways. IgE-dependent urticarial reactions usually occur within 36 hours of drug exposure but can occur within minutes. Immune complex–induced urticaria associated with serum sickness reactions usually occurs 6–12 days after first exposure. In this syndrome, the urticarial eruption (typically polycyclic plaques over distal joints) may be accompanied by fever, hematuria, arthralgias, hepatic dysfunction, and neurologic symptoms. Certain drugs, such as NSAIDs, ACE inhibitors, angiotensin II antagonists, radiographic dye, and opiates, may induce urticarial reactions, angioedema, and anaphylaxis in the absence of drug-specific antibodies (non–IgE-mediated mast cell activation) through direct mast cell degranulation. Non–IgE-mediated mast cell activation associated with fluoroquinolones, vancomycin, radiocontrast dye, opiates, and other medications that share a tetrahydroisoquinolone (THIQ) moiety is now thought to be mediated through their interaction and activation of the MRGPRX2 receptor on mast cells. Expression of MRGPRX2 is also increased in the skin of patients with severe chronic spontaneous urticaria (CSU), and patients with CSU are more likely to be labeled as allergic to multiple drugs. Management includes discontinuation of the offending drug, antihistamines, and epinephrine for anaphylaxis.
7.3 Pruritus¶
Pruritus is associated with almost all drug eruptions and, in some cases, may represent the only symptom of the adverse cutaneous reaction. It may be alleviated by antihistamines such as hydroxyzine or diphenhydramine. Pruritus stemming from specific medications may require distinct treatment, such as selective opiate antagonists for opiate-related pruritus.
7.4 Immune Checkpoint Inhibitor irAEs¶
The immune checkpoint inhibitor (ICI) class of drugs (including anti-CTLA-4, anti-PD-1, and anti-PD-L1 agents) can induce a wide range of cutaneous eruptions, including lichenoid, eczematous, granulomatous, papulosquamous, bullous, vitiligo-like, alopecic, and panniculitic eruptions. Mucocutaneous immune-related adverse events (irAEs) to ICIs typically occur early and are the most common of potentially multiorgan reactions, occurring in 30–60% of patients. The onset may be as early as a few weeks after initiating the ICI and as late as 1 year or more after initiation. The incidence of irAEs differs between the distinct ICI medications and is most frequent with combination therapy with anti-CTLA-4 and anti-PD-1 agents. Severe irAEs (grade 3 or 4, including DIHS/DRESS, SJS/TEN-like, and bullous reactions involving over 30% body surface area) are rare, occurring in 2–3% of patients with ICI monotherapy and up to 15% with combined ICI therapy. The rates of irAEs may also differ between patient populations depending on the type of malignancy being treated. These reactions are largely T-cell–mediated, which informs the approach to management. Whereas milder reactions may be managed with topical corticosteroids, more severe reactions may require oral corticosteroids or other systemic immunomodulatory or immunosuppressive medications, including biologic agents. In some cases of severe reactions, including lichenoid bullous and SJS/TEN-like reactions, rechallenge of the ICI may be possible. A clear history of all new medications introduced within the few days to 2 months preceding the reaction should be taken, as case reports of ICIs increasing the risk of small-molecule SCAR have emerged. There are some data, largely retrospective studies, supporting the notion that mucocutaneous irAEs may be associated with improved prognosis and survival. It is important to note that the rash may continue to progress for a few days up to 1 week following medication discontinuation. Oral antihistamines and emollients may help relieve pruritus. Short courses of potent topical glucocorticoids can reduce inflammation and symptoms. Systemic glucocorticoid treatment is rarely indicated.
8. PROGNOSIS & COMPLICATIONS¶
Resolution of the cutaneous reaction may be delayed upon discontinuation of the medication. Drug-related nail disorders usually involve all 20 nails and need months to resolve after withdrawal of the medication. Some chemotherapeutic agents, such as methotrexate, can induce a UV-recall reaction characterized by an erythematous, slightly scaly eruption at sites of prior severe photosensitivity reactions. Some populations are at increased risk of drug reactions, including elderly patients, patients with autoimmune disease, hematopoietic stem cell transplant recipients, and those with acute Epstein-Barr virus (EBV) or human immunodeficiency virus (HIV) infection. The pathophysiology underlying this association may be related to immune dysregulation. Individuals with advanced HIV disease that is not virologically suppressed (e.g., CD4+ T lymphocyte count <200 cells/μL) have a 40- to 50-fold increased risk of adverse reactions to sulfamethoxazole and increased risk of severe hypersensitivity reactions to medications overall.
8.1 Resolution and Sequelae¶
Resolution of the cutaneous reaction may be delayed upon discontinuation of the medication. Drug-related nail disorders usually involve all 20 nails and need months to resolve after withdrawal of the medication. Some chemotherapeutic agents, such as methotrexate, can induce a UV-recall reaction characterized by an erythematous, slightly scaly eruption at sites of prior severe photosensitivity reactions.
8.2 Risk Populations¶
Some populations are at increased risk of drug reactions, including elderly patients, patients with autoimmune disease, hematopoietic stem cell transplant recipients, and those with acute Epstein-Barr virus (EBV) or human immunodeficiency virus (HIV) infection. The pathophysiology underlying this association may be related to immune dysregulation. Individuals with advanced HIV disease that is not virologically suppressed (e.g., CD4+ T lymphocyte count <200 cells/μL) have a 40- to 50-fold increased risk of adverse reactions to sulfamethoxazole and increased risk of severe hypersensitivity reactions to medications overall.
9. SPECIAL CONSIDERATIONS¶
The PREDICT-1 study was a randomized, double-blind clinical trial of real-time preprescription HLA-B57:01 screening versus the previous standard of care of no screening that provided the basis for the utility of HLA-B57:01 screening to prevent AHS. If an HLA risk allele is present, it seems to have the same implication regardless of the population. This generalizability across populations, the fact that self-identified race is a social rather than biological construct, and greater availability of less costly single-HLA assays with a shorter turnaround time argue against targeted genetic screening on the basis of self-identified race. The American College of Rheumatology has recommended HLA-B58:01 screening of Han Chinese patients prescribed allopurinol; however, HLA-B58:01 does not have 100% negative predictive value for allopurinol DIHS/DRESS or SJS/TEN in other populations, and safety monitoring and risk counseling remain imperative. To date, screening for a single HLA (but not multiple HLA haplotypes) in specific populations has been determined to be cost-effective (e.g., HLA-B*1301 screening in Chinese patients with leprosy treated with dapsone). Genetic testing for specific HLA haplotypes is becoming more widely available, and its utility will increase as mechanistic factors driving drug hypersensitivity and tolerance are elucidated. Further data are needed to clarify the role of genetic and other testing beyond screening (e.g., in diagnosis) in order to optimize cost-effectiveness, utility, and benefit.
9.1 Genetic Screening¶
Genetic testing for specific HLA haplotypes is becoming more widely available, and its utility will increase as mechanistic factors driving drug hypersensitivity and tolerance are elucidated. Further data are needed to clarify the role of genetic and other testing beyond screening (e.g., in diagnosis) in order to optimize cost-effectiveness, utility, and benefit. The PREDICT-1 study was a randomized, double-blind clinical trial of real-time preprescription HLA-B57:01 screening versus the previous standard of care of no screening that provided the basis for the utility of HLA-B57:01 screening to prevent AHS. If an HLA risk allele is present, it seems to have the same implication regardless of the population. This generalizability across populations, the fact that self-identified race is a social rather than biological construct, and greater availability of less costly single-HLA assays with a shorter turnaround time argue against targeted genetic screening on the basis of self-identified race. The American College of Rheumatology has recommended HLA-B58:01 screening of Han Chinese patients prescribed allopurinol; however, HLA-B58:01 does not have 100% negative predictive value for allopurinol DIHS/DRESS or SJS/TEN in other populations, and safety monitoring and risk counseling remain imperative. To date, screening for a single HLA (but not multiple HLA haplotypes) in specific populations has been determined to be cost-effective (e.g., HLA-B*1301 screening in Chinese patients with leprosy treated with dapsone).
10. KEY PEARLS & CLINICAL TRAPS¶
Cutaneous reactions are the most frequent adverse reactions to medications, representing 10–15% of reported adverse drug reactions. Most are benign, but a few can be life threatening. Prompt recognition of severe reactions, drug withdrawal, and appropriate therapeutic interventions can minimize toxicity. This chapter focuses on adverse cutaneous reactions to systemic medications; it covers their incidence, patterns, and pathogenesis, and provides some practical guidelines on treatment, assessment of causality, and future use of drugs. Some populations are at increased risk of drug reactions, including elderly patients, patients with autoimmune disease, hematopoietic stem cell transplant recipients, and those with acute Epstein-Barr virus (EBV) or human immunodeficiency virus (HIV) infection. The pathophysiology underlying this association may be related to immune dysregulation. Individuals with advanced HIV disease that is not virologically suppressed (e.g., CD4+ T lymphocyte count <200 cells/μL) have a 40- to 50-fold increased risk of adverse reactions to sulfamethoxazole and increased risk of severe hypersensitivity reactions to medications overall. Hypersensitivity to the anti-HIV medication abacavir is strongly associated with HLA-B57:01. HLA-B57:01 has 100% negative predictive value for the development of AHS, and routine preprescription screening for HLA-B57:01 has eliminated AHS as a clinical entity. In Taiwan, within a homogeneous Han Chinese population, a strong association was observed between SJS/TEN (but not DIHS/DRESS) related to carbamazepine and HLA-B15:02. In the same population, a strong association was found between HLA-B58:01 and both DIHS/DRESS and SJS/TEN associated with allopurinol. Other notable HLA associations include HLA-B13:01 and dapsone or sulfonamide antibiotic-induced DIHS/DRESS and SJS/TEN, as well as HLA-A32:01 and vancomycin-induced DIHS/DRESS. These associations are drug and phenotype specific; that is, HLA-specific T-cell stimulation by medications leads to distinct reactions. However, while these HLA associations are extremely strong, the presence of a risk HLA allele alone is not sufficient to cause severe drug hypersensitivity reactions. Other factors outside of the MHC, such as drug metabolism (e.g., CYP2C93 slow metabolism status and risk of phenytoin-induced morbilliform drug eruption, DIHS/DRESS, and SJS/TEN), are also important. The entirety of genetic and ecological factors that define why the majority of individuals carrying an HLA risk allele remain drug-tolerant and those factors that drive risk for specific drug hypersensitivity reactions are not known at this time.
10.1 Board Exam Favorites¶
HLA-B57:01 screening is recommended before abacavir to prevent hypersensitivity (100% negative predictive value). HLA-B15:02 is associated with carbamazepine-induced SJS/TEN in Han Chinese populations. HLA-B*58:01 is associated with allopurinol-induced DRESS/SJS/TEN in Han Chinese populations. Morbilliform eruptions are the most common drug reaction (91% of acute cutaneous reactions in hospitalized patients). Photosensitivity reactions are usually phototoxic and occur in sun-exposed areas; NSAIDs and fluoroquinolones are common causes. Warfarin necrosis occurs in 0.01–0.1% of patients, typically in women, between days 3–10 of therapy. Drug-induced hair loss (anagen effluvium) occurs within days of chemotherapy; telogen effluvium occurs 2–4 months after initiation. Drug-induced nail changes (onycholysis, onychomadesis) usually involve all 20 nails and need months to resolve. Diagnosis of morbilliform eruptions is rarely assisted by laboratory testing or skin biopsy; absence of enanthems supports drug etiology. Management of severe reactions requires drug withdrawal, symptomatic treatment (antihistamines, emollients), and systemic corticosteroids for severe cases.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
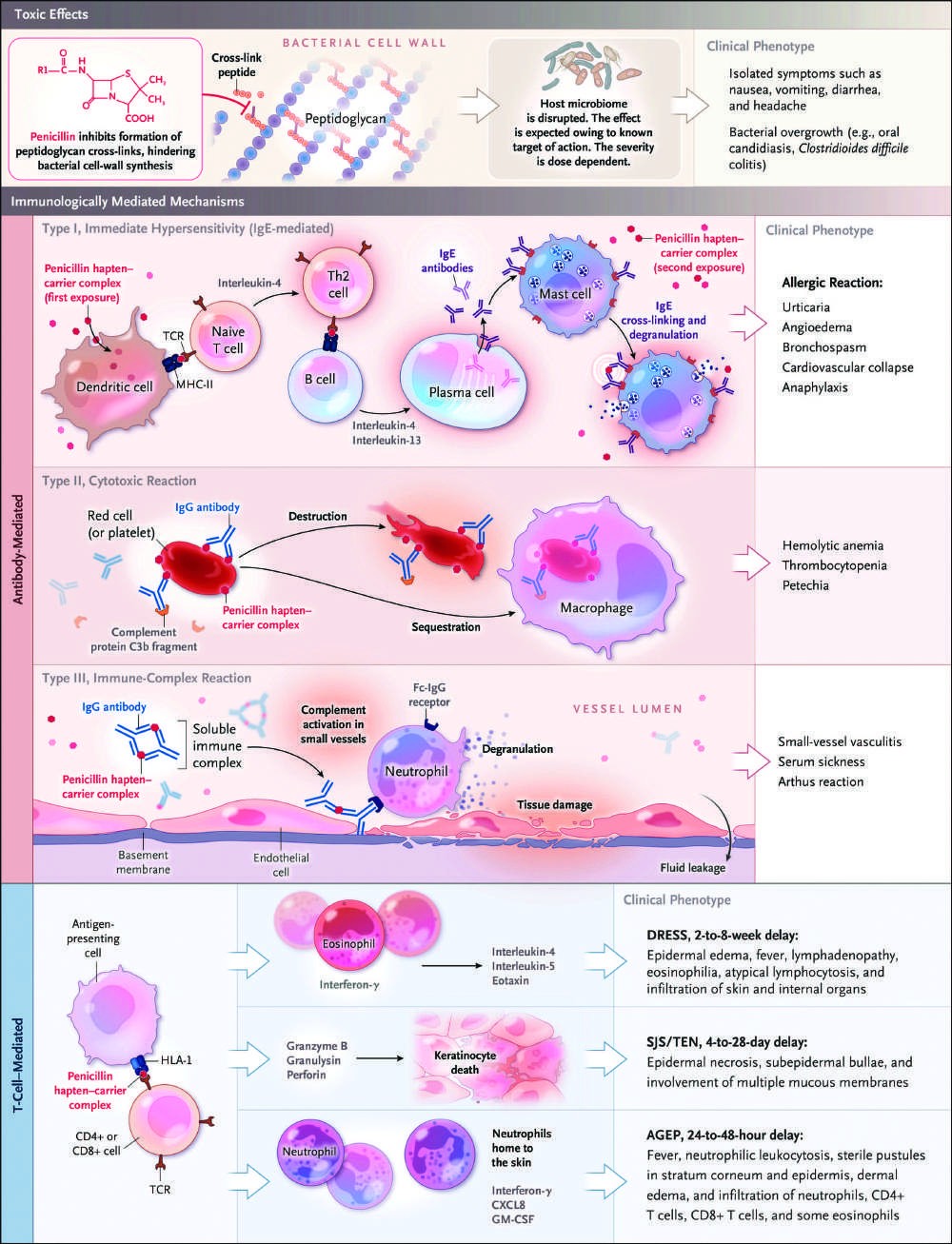
Caption: FIGURE 63-1 Clinical manifestations and mechanisms of immune-mediated cytotoxic reactions, and immune complex reactions. IgE-mediated reactions, also sensitization to a drug (e.g., penicillin). Drug-specific IgE is bound to high-affinity IgE of mast cells and release of mediators including tryptase and histamine, which are anaphylaxis. In type II cytotoxic reactions, antibodies target the cell membrane of red or immune complex reactions, antibodies react with a drug protein carrier forming soluble leading to tissue damage and small vessel vasculitis. Cell- (T-cell) mediated reactions an antigen presenting cell processes peptides modified by the drug and presents them in or CD4+ T cells, which leads to activation of T cells and release of specific cytokines these reactions are shown in Table 63-1, and specific clinical features and causative 381:2338. Copyright © (2019) Massachusetts Medical Society. Reprinted with permission — Figure 62-8: Development of an expressionless, masklike facies in a patient with scleroderma, showing furrowing and matlike telangiectasias on the face and hands.
Figure 2¶
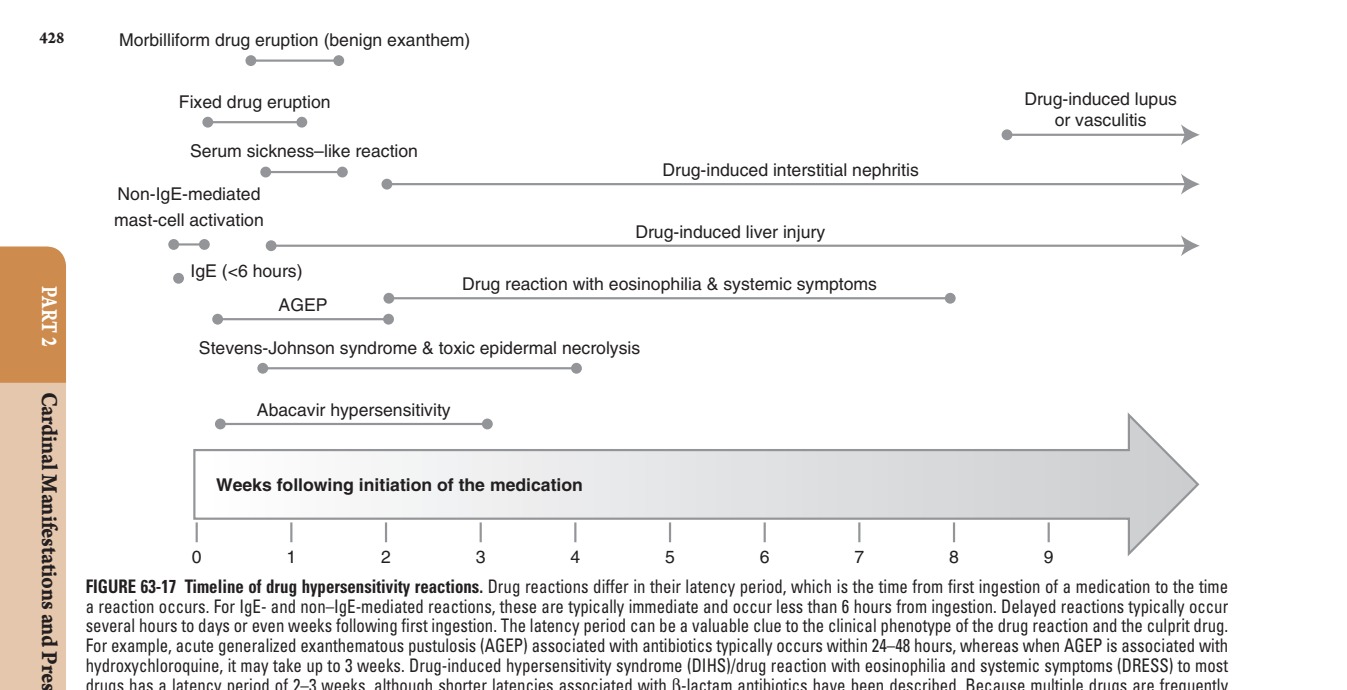
Caption: FIGURE 63-17 Timeline of drug hypersensitivity reactions. Drug reactions differ in their latency period, which is the time from first ingestion of a medication to the time a reaction occurs. For IgE- and non–IgE-mediated reactions, these are typically immediate and occur less than 6 hours from ingestion. Delayed reactions typically occur several hours to days or even weeks following first ingestion. The latency period can be a valuable clue to the clinical phenotype of the drug reaction and the culprit drug. For example, acute generalized exanthematous pustulosis (AGEP) associated with antibiotics typically occurs within 24–48 hours, whereas when AGEP is associated with hydroxychloroquine, it may take up to 3 weeks. Drug-induced hypersensitivity syndrome (DIHS)/drug reaction with eosinophilia and systemic symptoms (DRESS) to most drugs has a latency period of 2–3 weeks, although shorter latencies associated with β-lactam antibiotics have been described. Because multiple drugs are frequently started together in a complex medical patient, a timeline outlining all medications taken at the first time symptoms of a reaction occur and documentation of the evolution of these symptoms in relation to initiation of specific medications are valuable in clinical phenotype and drug causality assessment. (Reproduced with permission from DA Khan et al: Drug allergy: A 2022 practice parameter update. J Allerg Clin Immun 150:1333, 2022, Figure 1.) — Figure 63-1: Clinical manifestations and mechanisms of immune-mediated cutaneous drug reactions, illustrating antibody-mediated (IgE, cytotoxic, immune complex) and cell-mediated (T-cell) pathways.
Figure 3¶

Caption: essential. Given the severe complications and potentially delayed pre- FIGURE 63-10 SJS-TEN overlap. sentation of myocarditis, patients should undergo cardiac evaluation in cases of severe DIHS/DRESS or if heart involvement is suspected due herpes simplex virus is characterized by painful mucosal erosions and to hypotension or arrhythmia. Patients should be closely monitored target lesions, typically with an acral distribution and limited skin for resolution of organ dysfunction and for development of late-onset detachment. Mycoplasma and other respiratory infections in children autoimmune sequelae, such as thyroiditis, lupus, and diabetes. cause a clinically distinct presentation with prominent mucositis and limited cutaneous involvement. The term reactive infectious mucocuta- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis neous eruption (RIME) is used to help differentiate this clinical entity. SJS/TEN is a disease spectrum characterized by blisters and mucosal/ Patients with SJS/TEN initially present with fever >39°C (102.2°F); epidermal detachment resulting from full-thickness epidermal necro- — Figure 63-2: Subcutaneous lupus erythematosus due to medication, showing characteristic skin lesions.
Figure 4¶

Caption: Drug Reactions FIGURE 63-14 Atypical target-like lesion in SJS. and respiratory support are critical. Early administration of systemic glucocorticoids, intravenous immunoglobulin, cyclosporine, or etaner- cept may improve disease outcomes, but randomized studies to evalu- ate potential therapies are lacking and difficult to perform. FIGURE 63-12 Toxic epidermal necrolysis. Pustular Eruptions AGEP is a rare reaction pattern affecting 3–5 — Figure 63-3: Warfarin necrosis involving the breasts, showing sharply demarcated, erythematous, purpuric lesions that may progress to hemorrhagic bullae.
Figure 5¶

Caption: essential. Given the severe complications and potentially delayed pre- FIGURE 63-10 SJS-TEN overlap. sentation of myocarditis, patients should undergo cardiac evaluation in cases of severe DIHS/DRESS or if heart involvement is suspected due herpes simplex virus is characterized by painful mucosal erosions and to hypotension or arrhythmia. Patients should be closely monitored target lesions, typically with an acral distribution and limited skin for resolution of organ dysfunction and for development of late-onset detachment. Mycoplasma and other respiratory infections in children autoimmune sequelae, such as thyroiditis, lupus, and diabetes. cause a clinically distinct presentation with prominent mucositis and limited cutaneous involvement. The term reactive infectious mucocuta- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis neous eruption (RIME) is used to help differentiate this clinical entity. SJS/TEN is a disease spectrum characterized by blisters and mucosal/ Patients with SJS/TEN initially present with fever >39°C (102.2°F); epidermal detachment resulting from full-thickness epidermal necro- — Figure 63-4: Toxic erythema of chemotherapy, showing acral erythema marked by dysesthesia and an erythematous, edematous eruption of the palms and soles.
Figure 6¶

Caption: Drug Reactions FIGURE 63-6 Allergic contact dermatitis (bullous) due to adhesive tape. the skin, and T 2 cells express CD134 and produce cytokines such as H IL-4, IL-5, IL-10, IL-13, and eotaxin. Type 2 innate lymphocytes (ILC2) produce IL-5 that promotes activation and migration of eosinophils. Irritant/Allergic Contact Dermatitis Patients using topical Tregs and dendritic cells produce IFN-γ, TNF-α, and CCL17 (serum medications may develop an irritant or allergic contact dermatitis to thymus and activation-regulated chemokine [TARC]), which fuels the the medication itself or to a preservative or other component of the systemic presentation. formulation. Reactions to neomycin sulfate, bacitracin, polymyxin B, Clinically, DIHS/DRESS presents with a prodrome of fever and and benzalkonium are common, and co-sensitization is common due flu-like symptoms for several days, followed by the appearance of to their shared presence in multiple products such as ointments and an extensive rash usually involving the face (Fig. 63-8). The rash of — Figure 63-5: Morbilliform drug eruption, showing blanching erythematous macules and papules that are symmetric and confluent, often starting on the trunk or intertriginous areas.
Figure 7¶

Caption: Drug Reactions FIGURE 63-14 Atypical target-like lesion in SJS. and respiratory support are critical. Early administration of systemic glucocorticoids, intravenous immunoglobulin, cyclosporine, or etaner- cept may improve disease outcomes, but randomized studies to evalu- ate potential therapies are lacking and difficult to perform. FIGURE 63-12 Toxic epidermal necrolysis. Pustular Eruptions AGEP is a rare reaction pattern affecting 3–5 — Figure 63-6: Drug-induced hair loss (anagen effluvium), showing diffuse, nonscarring alopecia following chemotherapy or other cytotoxic agents.
Figure 8¶

Caption: Cutaneous Drug Reactions FIGURE 63-3 Warfarin necrosis involving the breasts. Toxic Erythema of Chemotherapy and Other Chemotherapy Reactions Because many agents used in cancer chemotherapy or purpuric, and may progress to form large, hemorrhagic bullae with inhibit cell division, rapidly proliferating elements of the skin, includ- necrosis and eschar formation. ing hair, mucous membranes, and appendages, are sensitive to their Warfarin anticoagulation in protein C or S deficiency causes an effects. A broad spectrum of chemotherapy-related skin toxicities has additional reduction in already low circulating levels of endogenous been reported, including neutrophilic eccrine hidradenitis, sterile cel- anticoagulants, permitting temporary hypercoagulability and throm- lulitis, exfoliative dermatitis, and flexural erythema. These reactions bosis in the cutaneous microvasculature, with consequent areas of are best characterized under the unifying term “toxic erythema of necrosis. Heparin-induced necrosis may have clinically similar fea- chemotherapy” (TEC) (Fig. 63-4). Acral erythema is marked by dys- — Figure 63-7: Drug-induced nail changes, showing onycholysis, onychomadesis, pigmentation, or paronychia.
Figure 9¶

Caption: Drug Reactions FIGURE 63-6 Allergic contact dermatitis (bullous) due to adhesive tape. the skin, and T 2 cells express CD134 and produce cytokines such as H IL-4, IL-5, IL-10, IL-13, and eotaxin. Type 2 innate lymphocytes (ILC2) produce IL-5 that promotes activation and migration of eosinophils. Irritant/Allergic Contact Dermatitis Patients using topical Tregs and dendritic cells produce IFN-γ, TNF-α, and CCL17 (serum medications may develop an irritant or allergic contact dermatitis to thymus and activation-regulated chemokine [TARC]), which fuels the the medication itself or to a preservative or other component of the systemic presentation. formulation. Reactions to neomycin sulfate, bacitracin, polymyxin B, Clinically, DIHS/DRESS presents with a prodrome of fever and and benzalkonium are common, and co-sensitization is common due flu-like symptoms for several days, followed by the appearance of to their shared presence in multiple products such as ointments and an extensive rash usually involving the face (Fig. 63-8). The rash of — Figure 63-8: Photosensitivity eruption, showing erythematous, scaly eruption in sun-exposed areas.
Figure 10¶

Caption: Drug Reactions FIGURE 63-6 Allergic contact dermatitis (bullous) due to adhesive tape. the skin, and T 2 cells express CD134 and produce cytokines such as H IL-4, IL-5, IL-10, IL-13, and eotaxin. Type 2 innate lymphocytes (ILC2) produce IL-5 that promotes activation and migration of eosinophils. Irritant/Allergic Contact Dermatitis Patients using topical Tregs and dendritic cells produce IFN-γ, TNF-α, and CCL17 (serum medications may develop an irritant or allergic contact dermatitis to thymus and activation-regulated chemokine [TARC]), which fuels the the medication itself or to a preservative or other component of the systemic presentation. formulation. Reactions to neomycin sulfate, bacitracin, polymyxin B, Clinically, DIHS/DRESS presents with a prodrome of fever and and benzalkonium are common, and co-sensitization is common due flu-like symptoms for several days, followed by the appearance of to their shared presence in multiple products such as ointments and an extensive rash usually involving the face (Fig. 63-8). The rash of — Figure 63-9: Warfarin necrosis, showing necrotic lesions in sun-protected sites or areas of trauma.
Figure 11¶

Caption: FIGURE 62-8 Development of an expressionless, masklike facies in a patient with scleroderma. (Courtesy of Thomas J. Lawley, MD; with permission.) — Figure 63-10: Toxic erythema of chemotherapy, showing flexural erythema and sterile cellulitis.
Figure 12¶

Caption: Drug Reactions FIGURE 63-14 Atypical target-like lesion in SJS. and respiratory support are critical. Early administration of systemic glucocorticoids, intravenous immunoglobulin, cyclosporine, or etaner- cept may improve disease outcomes, but randomized studies to evalu- ate potential therapies are lacking and difficult to perform. FIGURE 63-12 Toxic epidermal necrolysis. Pustular Eruptions AGEP is a rare reaction pattern affecting 3–5 — Figure 63-11: Drug-induced hair loss (telogen effluvium), showing diffuse hair shedding 2–4 months after initiation of medication.
Figure 13¶

Caption: FIGURE 63-16 Cutaneous small-vessel vasculitis (CSVV, leukocytoclastic vasculitis). — Figure 63-12: Drug-induced nail changes, showing Beau lines or transverse depression of the nail plate.
Figure 14¶

Caption: essential. Given the severe complications and potentially delayed pre- FIGURE 63-10 SJS-TEN overlap. sentation of myocarditis, patients should undergo cardiac evaluation in cases of severe DIHS/DRESS or if heart involvement is suspected due herpes simplex virus is characterized by painful mucosal erosions and to hypotension or arrhythmia. Patients should be closely monitored target lesions, typically with an acral distribution and limited skin for resolution of organ dysfunction and for development of late-onset detachment. Mycoplasma and other respiratory infections in children autoimmune sequelae, such as thyroiditis, lupus, and diabetes. cause a clinically distinct presentation with prominent mucositis and limited cutaneous involvement. The term reactive infectious mucocuta- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis neous eruption (RIME) is used to help differentiate this clinical entity. SJS/TEN is a disease spectrum characterized by blisters and mucosal/ Patients with SJS/TEN initially present with fever >39°C (102.2°F); epidermal detachment resulting from full-thickness epidermal necro- — Figure 63-13: Photosensitivity eruption, showing blistering in drug-related pseudoporphyria.
Figure 15¶

Caption: FIGURE 63-5 Morbilliform drug eruption. — Figure 63-14: Warfarin necrosis, showing necrosis in areas of low protein C or S levels.
Figure 16¶

Caption: Cutaneous Drug Reactions FIGURE 63-3 Warfarin necrosis involving the breasts. Toxic Erythema of Chemotherapy and Other Chemotherapy Reactions Because many agents used in cancer chemotherapy or purpuric, and may progress to form large, hemorrhagic bullae with inhibit cell division, rapidly proliferating elements of the skin, includ- necrosis and eschar formation. ing hair, mucous membranes, and appendages, are sensitive to their Warfarin anticoagulation in protein C or S deficiency causes an effects. A broad spectrum of chemotherapy-related skin toxicities has additional reduction in already low circulating levels of endogenous been reported, including neutrophilic eccrine hidradenitis, sterile cel- anticoagulants, permitting temporary hypercoagulability and throm- lulitis, exfoliative dermatitis, and flexural erythema. These reactions bosis in the cutaneous microvasculature, with consequent areas of are best characterized under the unifying term “toxic erythema of necrosis. Heparin-induced necrosis may have clinically similar fea- chemotherapy” (TEC) (Fig. 63-4). Acral erythema is marked by dys- — Figure 63-15: Toxic erythema of chemotherapy, showing neutrophilic eccrine hidradenitis.
Figure 17¶

Caption: Drug Reactions FIGURE 63-14 Atypical target-like lesion in SJS. and respiratory support are critical. Early administration of systemic glucocorticoids, intravenous immunoglobulin, cyclosporine, or etaner- cept may improve disease outcomes, but randomized studies to evalu- ate potential therapies are lacking and difficult to perform. FIGURE 63-12 Toxic epidermal necrolysis. Pustular Eruptions AGEP is a rare reaction pattern affecting 3–5 — Figure 63-16: Drug-induced hair loss, showing hypertrichosis or hirsutism due to androgenic stimulation.
Figure 18¶

Caption: FIGURE 63-2 Subcutaneous lupus erythematosus due to medication. — Figure 63-17: Drug-induced nail changes, showing nail bed hyperpigmentation through melanocyte stimulation.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.