Chapter 187 | Part 5: Infectious Diseases | Syphilis¶
Spirochetal Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Syphilis is a chronic systemic infection caused by Treponema pallidum subspecies pallidum, characterized by active disease episodes interrupted by asymptomatic latency.
- The incubation period averages 2–6 weeks, inversely proportional to the number of organisms transmitted (median ~21 days).
- Primary chancre is typically a single painless papule that erodes, becomes indurated, and heals spontaneously within 4–6 weeks.
- Secondary syphilis manifests with generalized mucosal/cutaneous lesions, generalized nontender lymphadenopathy (85%), and constitutional signs (fever, weight loss, malaise).
- Lipoidal tests (RPR, VDRL) measure IgG/IgM against cardiolipin-lecithin-cholesterol antigen; Treponemal tests (EIA/CIA, TPPA) are specific for current/past infection.
- Argyll Robertson pupil reacts to accommodation but not to light, a feature of tabes dorsalis and paresis.
- Classic congenital stigmata include Hutchinson's teeth (centrally notched incisors), mulberry molars, saddle nose, and saber shins.
- During BPG shortage, nonpregnant patients may be treated with doxycycline, reserving Benzathine Penicillin G (BPG) for seropositive pregnant women.
- CSF abnormalities (pleocytosis, increased protein, reactive VDRL) are found in up to 40% of untreated primary/secondary syphilis cases.
- In the US, P&S syphilis cases increased tenfold from 2000 to 2022, with ~45% of cases in men who have sex with men (MSM).
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification & Subspecies
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors & Transmission
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Pathogenesis of Untreated Syphilis
- 4. CLINICAL FEATURES
- 4.1 Primary Syphilis
- 4.2 Secondary Syphilis
- 4.3 Latent & Tertiary Syphilis
- 4.4 Congenital Syphilis
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Primary Lesion DDx
- 5.2 Congenital Infection DDx
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Serologic Testing Algorithm
- 6.2 CSF Evaluation
- 7. MANAGEMENT & TREATMENT
- 7.1 Current Treatment Context
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Historical & Modern Prognosis
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy & HIV
- 9.2 MSM & Reinfection
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Board Exam Favorites
- WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- 10.2 Specific Findings
- WHAT EXCLUDES THE DIAGNOSIS
- 10.3 Exclusion Criteria
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Primary and secondary syphilis in the United States, 1990–2022, by of sex |
| 2 | 🖼 Figure | Primary syphilis with a firm, nontender chancre |
| 3 | 🖼 Figure | Secondary syphilis |
1. DEFINITION & OVERVIEW¶
- Syphilis, a chronic systemic infection caused by Treponema pallidum subspecies pallidum, is usually sexually transmitted and is characterized by episodes of active disease interrupted by asymptomatic periods (latency).
- After an incubation period averaging 2–6 weeks, a primary lesion appears—often associated with regional lymphadenopathy—and then resolves without treatment.
- The secondary stage, with generalized mucosal and cutaneous lesions and generalized lymphadenopathy, also resolves spontaneously and is followed by a latent period of subclinical infection lasting years or decades.
- Central nervous system (CNS) invasion may occur early in infection, and CNS involvement may be symptomatic or asymptomatic.
- In the preantibiotic era, one-third of untreated patients developed tertiary syphilis, characterized by destructive mucocutaneous, skeletal, or parenchymal lesions; aortitis; or late CNS manifestations.
- Historically, the pathogenic Treponema were distinguished by the clinical syndromes they produce, but phylogenetic analyses yield the three named subspecies groupings: T. pallidum subsp. pallidum (venereal syphilis), T. pallidum subsp. pertenue (yaws), and T. pallidum subsp. endemicum (bejel).
- T. carateum (pinta) is still classified as a separate species, for which no extant strains are available for molecular studies.
- T. pallidum subspecies are thin spiral organisms, with a cell body surrounded by a trilaminar cytoplasmic membrane, a delicate peptidoglycan layer, and a lipid-rich outer membrane.
- Endoflagella wind around the cell body in the periplasmic space and are responsible for motility.
- Historically, T. pallidum subspecies could not be cultured in vitro, but long-term propagation of multiple strains of T. pallidum subsp. pallidum and one strain of subsp. endemicum in complex medium with eukaryotic cells is now possible.
- All T. pallidum subspecies have severely limited metabolic capabilities and are highly dependent on host-derived amino acids, carbohydrates, and lipids.
- Genetic analyses have revealed the existence of a 12-member gene family (tpr) encoding outer-membrane antigens. One member, TprK, has discrete variable regions that undergo antigenic variation during infection, providing a mechanism for immune evasion and persistence.
1.1 Classification & Subspecies¶
- T. pallidum subsp. pallidum (venereal syphilis).
- T. pallidum subsp. pertenue (yaws).
- T. pallidum subsp. endemicum (bejel).
- T. carateum (pinta).
- Whether these groupings represent geographic variation or actual biological differences is unclear.
- The crossing of subspecies boundaries by some 'molecular signatures' and the recent recognition of treponemes of the endemicum genotype in sexually acquired genital ulcers (chancres) and secondary rashes support the concept of a genetic and clinical 'continuum' among strains and subspecies of the pathogenic treponemes.
2. EPIDEMIOLOGY¶
- Nearly all cases of syphilis are acquired by sexual contact with infectious lesions (i.e., the chancre, mucous patch, skin rash, or condylomata lata).
- T. pallidum DNA has also been detected in swabs of normal-appearing oral mucosa, in saliva, in urine, and in semen, raising the possibility of transmission by these routes, but the infectivity of these organisms has not been assessed.
- Less common modes of transmission include nonsexual skin contact, infection in utero, blood transfusion, and organ transplantation.
- ■ SYPHILIS IN THE UNITED STATES
- Following the introduction of penicillin therapy in the 1940s, the number of reported cases of syphilis of all stages in the United States declined 95% to a low of 31,575 cases in 2000, with 5979 reported cases of primary and secondary (P&S) syphilis.
- Since 2000, total cases have increased 6.6-fold to 207,255, and the number of P&S cases has increased tenfold, with 59,061 cases reported in 2022.
- Nationally, ~45% of these cases were in men who have sex with men (MSM), ~40% of whom are co-infected with HIV.
- In two years, from 2020 to 2022, P&S cases rose 31.7% among all men and 85.4% among women, with increases in all racial and ethnic groups and in all geographic regions of the United States.
- Because the incidence of congenital syphilis parallels that of infectious syphilis in women, the striking increase in early syphilis in women has resulted in a dramatic increase in congenital syphilis.
- In 2022, 3755 cases of congenital syphilis were reported, resulting in 282 congenital syphilis-related stillbirths and deaths.
- In the last decade, the number of reported cases in infants <1 year of age has increased from 334 to 3755, or elevenfold.
- The vast majority of these cases resulted from late or no prenatal care, but some were in women who had tested positive for syphilis but were not treated prior to delivery.
- A recent study of substance use in pregnant women with syphilis found that illicit use of opioids and other illicit nonprescription substances was six and four times higher, respectively, in persons with a congenital syphilis outcome than in those without a congenital syphilis outcome.
- Other risk factors include homelessness and unstable housing, transactional sex, and incarceration.
- The populations at highest risk for acquiring syphilis have changed over time, with outbreaks among MSM in the pre-HIV era of the late 1970s and early 1980s, as well as at present.
- The current dramatic decade-long increase in syphilis and other sexually transmitted infections in MSM may be due to unprotected sex between persons who are HIV concordant and to disinhibition facilitated by highly effective antiretroviral therapy (ART) or pre- and postexposure prophylaxis (PrEP and PEP).
- Many MSM diagnosed with syphilis have had syphilis previously, and reinfections may be asymptomatic in persons with multiple past episodes.
- Thus, more frequent (every 3 months) screening for syphilis and other sexually transmitted infections is warranted in high-risk populations.
- Cases of P&S syphilis among African Americans increased 5.5-fold between 2002 and 2022, and the rate (44.4 per 100,000 population) remains higher than rates for other racial/ethnic groups except American Indians/Alaska Natives (67 per 100,000).
- Of individuals named as sexual contacts of persons with early syphilis, some will have developed manifestations of syphilis when they are first seen, and others will develop infectious syphilis if not treated; overall, ~30–60% of persons exposed to P&S syphilis will develop syphilis if not treated.
- Thus, identification and treatment of all recently exposed sexual contacts continue to be important aspects of syphilis control.
- Recent data suggest that PEP with 200 mg of doxycycline (Doxy-PEP), taken within 72 h of exposure, will significantly reduce the likelihood of syphilis (and other) infections in MSM.
- Data from a single study of Doxy-PEP in women have been disappointing, but these results may be due to lack of compliance in the test population.
- Concerns have been raised that widespread use of Doxy-PEP (perhaps misused as PrEP) may result in selection for resistance in sexually transmitted infection pathogens.
- ■ GLOBAL SYPHILIS
- Syphilis remains a significant health problem globally; the number of new infections is estimated at ~8 million per year, with 22.3 million prevalent cases.
- The regions most affected include sub-Saharan Africa, South America, and central and south Asia.
- Rates of P&S syphilis have increased dramatically among MSM in many European, Asian, and South American countries.
- Globally, although efforts by the World Health Organization (WHO) reduced the incidence of congenital syphilis in the 2010s, that progress is being lost as recent increases are reported in nearly all regions of the world.
- In 2022, there were an estimated 700,000 cases of congenital syphilis and 390,000 adverse birth outcomes: 150,000 early fetal deaths and stillbirths, 70,000 neonatal deaths, 55,000 preterm or low-birth-weight infants, and 115,000 infants with clinical evidence of infection.
Table 1 — Table 187-1: Syphilis Cases in the United States (1990–2022)¶
| Year | Total Cases | Primary & Secondary (P&S) Cases | Congenital Cases (2022) |
|---|---|---|---|
| 2000 | 31,575 | 5,979 | N/A |
| 2022 | 207,255 | 59,061 | 3,755 |
2.1 Risk Factors & Transmission¶
- Sexual contact with infectious lesions (chancre, mucous patch, skin rash, condylomata lata).
- Nonsexual skin contact.
- Infection in utero.
- Blood transfusion.
- Organ transplantation.
- Unprotected sex between persons who are HIV concordant.
- Disinhibition facilitated by highly effective ART or PrEP/PEP.
- Homelessness and unstable housing.
- Transactional sex.
- Incarceration.
- Illicit use of opioids and other illicit nonprescription substances.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- The only known natural host for T. pallidum subsp. pallidum (referred to hereafter as T. pallidum) is the human.
- T. pallidum can infect many mammals, but only humans, higher apes, and a few laboratory animals develop syphilitic lesions.
- Rabbits are used to propagate T. pallidum and serve as the animal model that best reflects human disease and immunopathology.
- T. pallidum rapidly penetrates intact mucous membranes or microscopic abrasions in skin and, within a few hours, enters the lymphatics and blood to produce systemic infection and metastatic foci long before the appearance of a primary lesion.
- Blood from a patient with incubating or early syphilis is infectious.
- The generation time of T. pallidum during early disease is estimated to be ~33 h, and the incubation period of syphilis is inversely proportional to the number of organisms transmitted.
- The 50% infectious dose for intradermal inoculation in humans has been calculated to be 57 organisms, and the treponeme concentration generally reaches 10^7/g of tissue before a clinical lesion appears.
- The median incubation period in humans (~21 days) suggests an average inoculum of 500–1000 infectious organisms for naturally acquired disease; the incubation period rarely exceeds 6 weeks.
- The primary lesion appears at the site of inoculation, usually persists for 4–6 weeks, and then heals spontaneously.
- Histopathologic examination shows perivascular infiltration, chiefly by CD4+ and CD8+ T lymphocytes, plasma cells, and macrophages, with capillary endothelial proliferation and subsequent obliteration of small blood vessels.
- The cellular infiltration produces a T 1-type cytokine profile, consistent with the activation of macrophages.
- Phagocytosis of opsonized organisms by activated macrophages ultimately causes their destruction, resulting in spontaneous resolution of the chancre and later the secondary rash.
- The generalized parenchymal, constitutional, mucosal, and cutaneous manifestations of secondary syphilis usually appear ~6–12 weeks after infection, although primary and secondary manifestations may occasionally overlap.
- In contrast, some patients may enter the latent stage without ever recognizing secondary lesions.
- The histopathologic features of secondary maculopapular skin lesions include hyperkeratosis of the epidermis, capillary proliferation with endothelial swelling in the superficial dermis, and—in the deeper dermis—perivascular infiltration by CD8+ and CD4+ T lymphocytes, macrophages, and variable numbers of plasma cells.
- T. pallidum disseminates during the first days to weeks of infection, invading many tissues, including the CNS; cerebrospinal fluid (CSF) abnormalities can be detected in as many as 40% of patients during the secondary stage.
- Clinical hepatitis and immune complex–induced glomerulonephritis are rare, but recognized, manifestations of secondary syphilis.
- Generalized nontender lymphadenopathy is noted in 85% of patients with secondary syphilis.
- The paradoxical appearance of secondary manifestations, even after the development of an immune response that clears primary lesions, likely results from immune evasion due to antigenic variation of exposed portions of the TprK surface protein.
- Secondary lesions generally subside within 2–6 weeks, and the infection enters the latent stage, which is detectable only by serologic testing.
- In the preantibiotic era, up to 25% of untreated patients experienced at least one cutaneous relapse of secondary lesions, usually during the first year.
- Therefore, it is identification and examination of sexual contacts are most important for patients with syphilis of <1 year in duration.
- In the preantibiotic era, about one-third of patients with untreated latent syphilis developed clinically apparent tertiary disease, the most common types being the gumma (a usually benign granulomatous lesion); cardiovascular syphilis (usually involving the vasa vasorum of the ascending aorta and resulting in aneurysm); and late symptomatic neurosyphilis (tabes dorsalis and paresis).
- In Western countries today, specific treatment for early and latent syphilis and coincidental therapy (i.e., therapy with antibiotics active against treponemes, but given for other conditions) have nearly eliminated tertiary syphilis.
- Asymptomatic CNS involvement, however, is still demonstrable in up to 40% of persons with early syphilis and 25% of patients with late latent syphilis, and modern cases of general paresis and tabes dorsalis are being reported from China.
- The factors that contribute to the development and progression of tertiary disease are unknown.
- The course of untreated syphilis was studied retrospectively in a group of nearly 2000 patients with primary or secondary disease diagnosed clinically (the Oslo Study, 1891–1951) and was assessed prospectively in 431 African-American men with seropositive latent syphilis of ≥3 years in duration (the notorious Tuskegee Study, 1932–1972).
- In the Oslo Study, serious late complications were nearly twice as common among men as among women.
- In the Tuskegee Study, untreated syphilis increased the death rate 17% compared to uninfected subjects, largely due to cardiovascular syphilis.
- The ethical issues eventually raised by the Tuskegee Study, begun in the pre-penicillin era but continuing into the early 1970s, had a major influence on the development of current guidelines for protection of human subjects and still contribute to a reluctance of some African Americans to participate in clinical research.
3.1 Pathogenesis of Untreated Syphilis¶
- Primary lesion: Appears at site of inoculation, persists 4–6 weeks, heals spontaneously.
- Secondary stage: Generalized manifestations appear ~6–12 weeks after infection.
- Latent stage: Detectable only by serologic testing.
- Tertiary stage: Develops in ~1/3 of untreated patients in preantibiotic era.
- CNS involvement: May occur early in infection, symptomatic or asymptomatic.
- Relapse: Up to 25% of untreated patients experienced at least one cutaneous relapse of secondary lesions in the first year.
4. CLINICAL FEATURES¶
- ■ PRIMARY SYPHILIS
- The typical primary chancre usually begins as a single painless papule that rapidly erodes and becomes indurated, with a characteristic cartilaginous consistency on palpation of the edge and base of the ulcer.
- Multiple primary lesions are seen in a minority of patients.
- In heterosexual men, the chancre is usually located on the penis, where it is readily seen.
- In MSM, it may also be found in the anal canal, rectum, or mouth.
- Oral sex has been identified as the source of infection in some MSM.
- In women, common primary sites are the cervix, vaginal wall, and labia, as well as anal canal and mouth.
- Consequently, primary syphilis goes unrecognized in women and MSM more often than in heterosexual men.
- Atypical primary lesions are common, and may be multiple, small, or partially resolved.
- Therefore, syphilis should be considered in the evaluation of trivial or atypical dark-field-negative genital lesions.
- The lesions that most commonly must be differentiated from those of primary syphilis include those caused by herpes simplex virus infection, chancroid, traumatic injury, and donovanosis.
- Regional (usually inguinal) lymphadenopathy accompanies the primary syphilitic lesion, appearing within 1 week of lesion onset.
- The nodes are firm, nonsuppurative, and painless.
- Inguinal lymphadenopathy is bilateral and may occur with anal as well as with genital chancres.
- The chancre generally heals within 4–6 weeks (range, 2–12 weeks), but lymphadenopathy may persist for months.
- ■ SECONDARY SYPHILIS
- The classical manifestations of the secondary stage include mucocutaneous or cutaneous lesions and generalized nontender lymphadenopathy.
- The healing primary chancre may still be present in ~15% of cases—more frequently in persons with concurrent HIV infection.
- The skin rash consists of macular, papular, papulosquamous, and occasionally pustular syphilides; often more than one form is present simultaneously.
- The eruption may be very subtle, and 25% of patients with a discernible rash may be unaware that they have dermatologic manifestations.
- Initial lesions are pale red or pink, nonpruritic, discrete macules distributed on the trunk and extremities; these macules progress to papular lesions that are distributed widely and that frequently involve the palms and soles.
- Involvement of the hair follicles may result in patchy alopecia of the scalp hair, eyebrows, or beard in up to 5% of cases.
- In warm, moist, intertriginous areas (commonly the perianal region, vulva, and scrotum), papules can enlarge to produce broad, moist, pink or gray-white, highly infectious lesions (condylomata lata) in 10% of patients with secondary syphilis.
- Superficial mucosal erosions (mucous patches) occur in 10–15% of patients and commonly involve the oral or genital mucosa.
- The typical mucous patch is a painless silver-gray erosion surrounded by a red periphery.
- T. pallidum DNA has been detected in oral mucosal swabs from persons with early and latent syphilis, but who have no visible oral lesions.
- Constitutional signs and symptoms that may accompany or precede secondary syphilis include sore throat (15–30%), fever (5–8%), weight loss (2–20%), malaise (25%), anorexia (2–10%), headache (10%), and meningismus (5%).
- Acute meningitis occurs in only 1–2% of cases, but CSF cell and protein concentrations are increased in up to 40% of early syphilis cases, and viable T. pallidum organisms have been recovered from CSF during primary and secondary syphilis in 30% of cases, sometimes without other CSF abnormalities.
- Persons with current or recent secondary syphilis may present with ocular or otic manifestations.
- Ocular findings include pupillary abnormalities and optic neuritis as well as the classic iritis or uveitis.
- The diagnosis of ocular syphilis is often considered in affected patients only after they fail to respond to topical steroid therapy.
- Anterior uveitis has been reported in 5–10% of patients with secondary syphilis, and T. pallidum has been demonstrated in aqueous humor from such patients.
- Permanent blindness may result without prompt diagnosis and treatment.
- Otic syphilis may present as sensorineural hearing loss, and deafness may result if untreated.
- Less often recognized complications of secondary syphilis include hepatitis, nephropathy, gastrointestinal involvement (hypertrophic gastritis, patchy proctitis, or a rectosigmoid mass—sometimes mistakenly assumed to be malignant), arthritis, and periostitis.
- Hepatic involvement is common in syphilis; although it is usually asymptomatic, up to 25% of patients may have abnormal liver function tests.
- Frank syphilitic hepatitis is rare.
- Renal involvement usually results from immune complex deposition and produces proteinuria associated with an acute nephrotic syndrome.
- ■ LATENT SYPHILIS
- Positive serologic tests for syphilis, together with a normal CSF examination and the absence of clinical manifestations of syphilis, indicate a diagnosis of latent syphilis in an untreated person.
- The diagnosis may be made following routine serologic screening or may be suspected due to a history of primary or secondary lesions, a history of exposure to syphilis, or the delivery of an infant with congenital syphilis.
- A previous nonreactive serologic test or clear history of lesions or exposure may help to establish the duration of infection, which is an important factor in the selection of appropriate therapy.
- Early latent syphilis is limited to the first year after infection, whereas late latent syphilis is defined as that of ≥1 year in duration or unknown duration.
- The classical definition of early latent syphilis could include an asymptomatic person whose secondary rash has resolved, as well as a person whose chancre has healed but who has not yet developed secondary manifestations.
- ■ REINFECTION SYPHILIS
- A growing number of individuals, particularly MSM, acquire multiple episodes of syphilis, with important implications for clinical presentation and serologic testing.
- Although no national data are available, 32% of enrollees (mostly MSM) in an 18-year longitudinal study of CNS involvement were known to have had multiple episodes of syphilis.
- It is well recognized that, after treatment, persons with past syphilis are less likely to revert to nonreactive in the Venereal Disease Research Laboratory (VDRL)/rapid plasma reagin (RPR) tests than persons with first episode syphilis, and treponemal tests will remain reactive.
- However, several recent studies also indicate that subsequent episodes of syphilis are more likely to be asymptomatic than initial episodes, less likely to have T. pallidum identified in blood or CSF, and less likely to have laboratory-defined neurosyphilis.
- These cases would be detectable only by serologic screening, reinforcing the utility of frequent screening in high-risk populations to identify reinfection.
- ■ INVOLVEMENT OF THE CNS
- Traditionally, neurosyphilis has been considered a late manifestation of syphilis, but this view is inaccurate.
- CNS syphilis represents a continuum encompassing early invasion (usually within the first weeks of infection), months to years of asymptomatic involvement, and, in some cases, development of early or late neurologic manifestations.
- Early neurosyphilis includes asymptomatic or symptomatic meningitis and meningovascular syphilis; late neurosyphilis includes tabes dorsalis and general paresis.
- Asymptomatic Neurosyphilis
- The diagnosis of asymptomatic neurosyphilis is made in patients who lack neurologic symptoms and signs but who have CSF abnormalities, including mononuclear pleocytosis, increased protein concentration, or reactivity in the CSF VDRL test.
- CSF abnormalities are demonstrated in up to 40% of cases of untreated primary or secondary syphilis and in 25% of cases of untreated latent syphilis.
- T. pallidum has been recovered by inoculation into rabbits of CSF from up to 30% of patients with primary or secondary syphilis but less frequently from patients with syphilis of >1 year in duration.
- The presence of T. pallidum in CSF is often associated with other CSF abnormalities, but organisms can be recovered from patients with otherwise normal CSF.
- Although the prognostic implications of these findings in early syphilis are uncertain, it may be appropriate to conclude that even patients with early syphilis who have CSF abnormalities do indeed have asymptomatic neurosyphilis and should be treated for neurosyphilis; such treatment is particularly important in patients with concurrent untreated HIV infection.
- Before the advent of penicillin, the risk of development of clinical neurosyphilis in untreated asymptomatic persons was roughly proportional to the intensity of CSF changes.
- In several large studies, neurosyphilis was associated with a serum RPR titer of ≥1:32, regardless of clinical stage or HIV infection status.
- Most experts agree that clinical neurosyphilis is more common among persons with untreated HIV infection, and that the immune reconstitution seen with effective ART may have a protective effect against development of clinical neurosyphilis in some HIV-infected persons with syphilis.
- Nonetheless, RPR titer ≥1:32 is still associated with reactive CSF VDRL, even in persons taking effective ART.
- HIV-uninfected persons with untreated latent syphilis and normal CSF probably run a very low risk of subsequent neurosyphilis.
- Symptomatic Neurosyphilis
- The major clinical categories of symptomatic neurosyphilis include early meningeal and meningovascular and late parenchymatous syphilis.
- The last category includes general paresis and tabes dorsalis.
- The onset of symptoms usually occurs 2 years in duration.
- Adequate treatment of the woman before the 16th week of pregnancy should prevent fetal damage, and treatment before the third trimester should adequately treat the infected fetus.
- Untreated maternal infection may result in a rate of fetal loss of up to 40% with second-trimester spontaneous abortion, stillbirth, prematurity, and neonatal death.
- Among infants born alive, only fulminant congenital syphilis is clinically apparent at birth, and these babies have a very poor prognosis.
- The most common clinical problem is the healthy-appearing baby born to a mother with a positive serologic test.
- Routine serologic testing for syphilis in early pregnancy is cost-effective in virtually all populations, even in areas with a low prenatal prevalence of syphilis.
- Low-tech point-of-care tests have been developed and widely implemented to facilitate antenatal testing in resource-poor settings.
- Globally, congenital syphilis incidence has increased dramatically, particularly in Africa, South America, and the United States.
- Periodic lack of benzathine penicillin (BPG) availability in low- and middle-income countries and the current critical shortage in the United States and Europe complicate treatment of seropositive women.
- Globally, integration of programs to prevent congenital syphilis with programs to prevent maternal transmission of HIV would be highly cost-effective but is often hampered by the restrictions placed on HIV-focused funds.
- All pregnant women should be serologically screened at their first antenatal visit.
- Where the prevalence of syphilis in women is high or when the patient is at high risk of reinfection, testing should be repeated at 28 weeks and at delivery.
- Those testing positive should be treated immediately, even before receiving results of confirmatory tests.
- During the current BPG shortage, many clinics are treating nonpregnant patients with doxycycline, thus reserving BPG for seropositive pregnant women.
- Neonatal congenital syphilis must be differentiated from other generalized congenital infections, including rubella, cytomegalovirus or herpes simplex virus infection, and toxoplasmosis, as well as from erythroblastosis fetalis.
- Manifestations of congenital syphilis may appear early (within the first 2 years of life, often at 2–10 weeks of age) or late (after 2 years).
- The earliest manifestations of congenital syphilis include rhinitis, or 'snuffles' (23%); mucocutaneous lesions (35–41%); bone changes (61%), including periostitis detectable by x-ray examination of long bones; hepatosplenomegaly (50%); lymphadenopathy (32%); anemia (34%); jaundice (30%); thrombocytopenia; and leukocytosis.
- CNS invasion by T. pallidum is detectable in 22% of infected neonates.
- Neonatal death is usually due to pulmonary hemorrhage, secondary bacterial infection, or severe hepatitis.
- Late congenital syphilis (untreated after 2 years of age) is subclinical in 60% of cases; the clinical spectrum in the remainder of cases may include interstitial keratitis (which occurs at 5–25 years of age), eighth-nerve deafness, and recurrent arthropathy.
- Neurosyphilis was documented in about one-quarter of untreated patients with late congenital syphilis in the preantibiotic era.
- Gummatous periostitis occurs at 5–20 years of age and, as in bejel, tends to cause destructive lesions of the palate and nasal septum.
- Classic stigmata include Hutchinson's teeth (centrally notched, widely spaced, peg-shaped upper central incisors), 'mulberry' molars (sixth-year molars with multiple, poorly developed cusps), saddle nose, and saber shins.
Table 2 — Table 187-2: Congenital Syphilis Manifestations¶
| Category | Manifestation | Frequency/Notes |
|---|---|---|
| Early | Rhinitis ('snuffles') | 23% |
| Early | Mucocutaneous lesions | 35–41% |
| Early | Bone changes (periostitis) | 61% |
| Early | Hepatosplenomegaly | 50% |
| Early | Lymphadenopathy | 32% |
| Early | Anemia | 34% |
| Early | Jaundice | 30% |
| Late | Interstitial keratitis | 5–25 years of age |
| Late | Eighth-nerve deafness | N/A |
| Late | Recurrent arthropathy | N/A |
| Stigmata | Hutchinson's teeth | Centrally notched incisors |
| Stigmata | Mulberry molars | Sixth-year molars with multiple cusps |
| Stigmata | Saddle nose | N/A |
| Stigmata | Saber shins | N/A |
4.1 Primary Syphilis¶
- Typical primary chancre: Single painless papule that rapidly erodes and becomes indurated.
- Consistency: Characteristic cartilaginous consistency on palpation of the edge and base of the ulcer.
- Duration: Generally heals within 4–6 weeks (range, 2–12 weeks).
- Lymphadenopathy: Regional (usually inguinal), firm, nonsuppurative, painless, appearing within 1 week of lesion onset.
- Locations: Penis (heterosexual men), anal canal/rectum/mouth (MSM), cervix/vaginal wall/labia (women).
- Differential Diagnosis: Herpes simplex virus infection, chancroid, traumatic injury, donovanosis.
4.2 Secondary Syphilis¶
- Skin rash: Macular, papular, papulosquamous, occasionally pustular syphilides.
- Distribution: Trunk and extremities; frequently involves palms and soles.
- Condylomata lata: Broad, moist, pink or gray-white lesions in warm, moist, intertriginous areas (perianal region, vulva, scrotum).
- Mucous patches: Painless silver-gray erosion surrounded by a red periphery (oral or genital mucosa).
- Constitutional signs: Sore throat (15–30%), fever (5–8%), weight loss (2–20%), malaise (25%), anorexia (2–10%), headache (10%), meningismus (5%).
- Ocular: Pupillary abnormalities, optic neuritis, classic iritis or uveitis (5–10% anterior uveitis).
- Otic: Sensorineural hearing loss, vertigo, tinnitus, deafness.
- Hepatic: Abnormal liver function tests in up to 25% of patients; frank hepatitis rare.
- Renal: Proteinuria associated with acute nephrotic syndrome.
4.3 Latent & Tertiary Syphilis¶
- Latent Syphilis: Positive serologic tests, normal CSF, absence of clinical manifestations.
- Early Latent: <1 year after infection.
- Late Latent: ≥1 year in duration or unknown duration.
- Tertiary Syphilis: Gumma, cardiovascular syphilis, neurosyphilis.
- Gumma: Granulomatous inflammation, central necrosis due to endarteritis obliterans.
- Cardiovascular Syphilis: Endarteritis obliterans of vasa vasorum, aortic regurgitation, saccular aneurysm (ascending aorta), coronary ostial stenosis.
- Neurosyphilis: Meningeal, meningovascular, parenchymatous (general paresis, tabes dorsalis).
- Asymptomatic Neurosyphilis: CSF abnormalities without symptoms.
4.4 Congenital Syphilis¶
- Early Manifestations: Rhinitis ('snuffles'), mucocutaneous lesions, bone changes, hepatosplenomegaly, anemia, jaundice.
- Late Manifestations: Interstitial keratitis, eighth-nerve deafness, recurrent arthropathy, gummatous periostitis.
- Classic Stigmata: Hutchinson's teeth, mulberry molars, saddle nose, saber shins.
5. DIFFERENTIAL DIAGNOSIS¶
- Primary Syphilis Lesions:
- Herpes simplex virus infection.
- Chancroid.
- Traumatic injury.
- Donovanosis.
- Secondary Syphilis Lesions:
- Other generalized rashes (e.g., drug eruptions, viral exanthems).
- Ocular Syphilis:
- Other causes of uveitis/iritis.
- Otic Syphilis:
- Other causes of sensorineural hearing loss.
- Congenital Syphilis:
- Rubella.
- Cytomegalovirus infection.
- Herpes simplex virus infection.
- Toxoplasmosis.
- Erythroblastosis fetalis.
5.1 Primary Lesion DDx¶
- Herpes simplex virus infection.
- Chancroid.
- Traumatic injury.
- Donovanosis.
5.2 Congenital Infection DDx¶
- Rubella.
- Cytomegalovirus infection.
- Herpes simplex virus infection.
- Toxoplasmosis.
- Erythroblastosis fetalis.
6. INVESTIGATIONS & DIAGNOSIS¶
- ■ DEMONSTRATION OF THE ORGANISM
- Historically, dark-field microscopy and immunofluorescence antibody staining have been used to identify T. pallidum in moist lesions such as chancres or condylomata lata, but these tests are rarely available outside of research laboratories.
- Sensitive and specific PCR tests have been developed but are not commercially available, although a number of laboratories perform in-house validated PCR testing.
- The recent advances in cultivation of T. pallidum in a tissue culture system have not yet been implemented in clinical laboratories.
- T. pallidum can be found in tissue by immunofluorescence or immunohistochemical methods using specific monoclonal antibodies to T. pallidum.
- Some commercial polyclonal antibodies are cross-reactive with other spirochetes and should be avoided.
- Silver stains should be interpreted with caution because artifacts resembling T. pallidum are often seen.
- T. pallidum DNA has been detected by PCR in lesion swabs, tissue samples, blood, CSF, ocular fluid, urine, and oropharyngeal and rectal swabs.
- ■ SEROLOGIC TESTS FOR SYPHILIS
- There are two types of serologic tests for syphilis: lipoidal (formerly called 'nontreponemal') and treponemal.
- Both are reactive in persons with any treponemal infection, including syphilis, yaws, pinta, and bejel.
- The most widely used lipoidal antibody tests are the RPR and VDRL tests, which measure IgG and IgM directed against a cardiolipin-lecithin-cholesterol antigen.
- The RPR test is easier to perform and uses unheated serum or plasma; it is a lipoidal test.
- Treponemal enzyme or chemiluminescence immunoassays (EIAs/CIAs), based largely on reactivity to recombinant antigens, are automated and now used as screening tests by large laboratories.
- When these tests are used for screening, a high proportion of sera reactive by EIA/CIA are nonreactive by subsequent lipoidal tests.
- Such sera should be examined in the TPPA test, which includes different antigens and a different platform.
- If the TPPA test is nonreactive, the patient is unlikely to have syphilis; if it is reactive, the patient is likely to have current or past syphilis.
- Both lipoidal and treponemal tests may be nonreactive in early primary syphilis, although treponemal tests are slightly more sensitive (85–90%) during this stage than lipoidal tests (~80%).
- All tests are reactive during secondary syphilis.
- Fewer than 1% of patients with high titers have a lipoidal test that is nonreactive or weakly reactive with undiluted serum but is reactive with diluted serum—the prozone phenomenon.
- VDRL and RPR sensitivity and titers may decline in untreated persons with late latent syphilis, but treponemal tests remain reactive in late syphilis.
- After treatment for early syphilis, lipoidal test titers will generally decline or the tests will become nonreactive, whereas treponemal tests often remain reactive after therapy and are not helpful in determining the infection status of persons with past syphilis.
- There is some concern in the literature about persons in whom the lipoidal test titer fails to become nonreactive or remains reactive in low titer after treatment; this is more commonly seen in persons with repeated episodes of syphilis.
- The implications in such cases are unclear, but re-treatment rarely achieves the desired goal and is not recommended in the absence of clinical findings.
- False-Positive Serologic Tests for Syphilis
- The lipid antigens of lipoidal tests are similar to those found in human tissues, and these tests may be reactive (usually with titers ≤1:8) in persons without treponemal infection, largely limited to persons with autoimmune conditions or injection drug use.
- Among patients being screened for syphilis because of risk factors, clinical suspicion, or history of exposure, ~1% of reactive lipoidal tests are falsely positive.
- In a patient with a false-positive lipoidal test, syphilis is excluded by a nonreactive treponemal test.
- False-positive reactions may also occur with treponemal tests, particularly the EIA/CIA tests.
- Screening a low-prevalence population for syphilis with a treponemal test may result in true-positive reactions being outnumbered by false-positive reactions, leading to unnecessary treatment.
- Thus, screening with lipoidal tests is highly recommended.
- ■ EVALUATION FOR NEURO-, OCULAR, AND OTIC SYPHILIS
- Involvement of the CNS is detected by examination of CSF for mononuclear pleocytosis (>5 white blood cells/μL), increased protein concentration (>45 mg/dL), or CSF VDRL reactivity.
- Elevated CSF cell counts and protein concentrations are not specific for neurosyphilis.
- Treponemal tests have a very high positive predictive value for diagnosis of syphilis.
Table 3 — Table 187-3: Comparison of Syphilis Serologic Tests¶
| Test Type | Examples | Target Antigen | Sensitivity (Early Primary) | Specificity | Utility |
|---|---|---|---|---|---|
| Lipoidal (Nontreponemal) | RPR, VDRL | Cardiolipin-lecithin-cholesterol | ~80% | High (variable) | Screening, monitoring titers |
| Treponemal | EIA, CIA, TPPA | Recombinant antigens | 85–90% | Very High | Confirmation, diagnosis |
6.1 Serologic Testing Algorithm¶
- Step 1: Screen with Lipoidal Test (RPR or VDRL).
- If Reactive: Confirm with Treponemal Test (EIA/CIA or TPPA).
- If Treponemal Test Nonreactive: False-positive lipoidal test (exclude syphilis).
- If Treponemal Test Reactive: Current or past syphilis.
- Step 2: Early Primary Syphilis.
- Lipoidal tests may be nonreactive.
- Treponemal tests are slightly more sensitive (85–90%) than lipoidal tests (~80%).
- Step 3: Late Latent Syphilis.
- VDRL/RPR titers may decline.
- Treponemal tests remain reactive.
- Step 4: Post-Treatment Monitoring.
- Lipoidal test titers decline or become nonreactive.
- Treponemal tests often remain reactive after therapy.
- Re-treatment not recommended in absence of clinical findings.
6.2 CSF Evaluation¶
- Mononuclear pleocytosis: >5 white blood cells/μL.
- Increased protein concentration: >45 mg/dL.
- CSF VDRL reactivity.
- Note: Elevated CSF cell counts and protein concentrations are not specific for neurosyphilis.
7. MANAGEMENT & TREATMENT¶
- ■ TREATMENT CONSIDERATIONS
- During the current BPG shortage, many clinics are treating nonpregnant patients with doxycycline, thus reserving BPG for seropositive pregnant women.
- Neonatal congenital syphilis must be differentiated from other generalized congenital infections, including rubella, cytomegalovirus or herpes simplex virus infection, and toxoplasmosis, as well as from erythroblastosis fetalis.
- Treatment of mycobacterial infections requires multiple-drug regimens that often exert significant side effects with the potential to limit tolerability.
- The prolonged duration of treatment has vastly improved results over those obtained in past decades, but drugs and regimens that will shorten treatment duration and limit adverse drug effects and interactions are needed.
- Treatment of refractory NTM infections remains unclear.
- Suppressive therapy with periodic parenteral/oral drugs to limit disease progression and control symptoms may be an appropriate alternative to curative treatment.
7.1 Current Treatment Context¶
- Benzathine Penicillin G (BPG) shortage complicates treatment of seropositive women.
- Nonpregnant patients treated with doxycycline during shortage.
- Seropositive pregnant women reserved for BPG.
- Treatment of mycobacterial infections requires multiple-drug regimens (irrelevant to Syphilis but noted in text).
- Suppressive therapy may be an appropriate alternative to curative treatment for refractory cases.
8. PROGNOSIS & COMPLICATIONS¶
- In the Tuskegee Study, untreated syphilis increased the death rate 17% compared to uninfected subjects, largely due to cardiovascular syphilis.
- In the preantibiotic era, about one-third of patients with untreated latent syphilis developed clinically apparent tertiary disease.
- Asymptomatic CNS involvement is still demonstrable in up to 40% of persons with early syphilis and 25% of patients with late latent syphilis.
- Modern cases of general paresis and tabes dorsalis are being reported from China.
- The factors that contribute to the development and progression of tertiary disease are unknown.
- Neonatal death is usually due to pulmonary hemorrhage, secondary bacterial infection, or severe hepatitis.
- Late congenital syphilis (untreated after 2 years of age) is subclinical in 60% of cases.
- Neurosyphilis was documented in about one-quarter of untreated patients with late congenital syphilis in the preantibiotic era.
8.1 Historical & Modern Prognosis¶
- Untreated Syphilis: Increased death rate 17% (Tuskegee Study).
- Tertiary Disease: Gumma, cardiovascular syphilis, neurosyphilis (1/3 of untreated patients in preantibiotic era).
- CNS Involvement: Asymptomatic in up to 40% of early syphilis, 25% of late latent syphilis.
- Modern Cases: General paresis and tabes dorsalis reported from China.
- Congenital Syphilis: Neonatal death due to pulmonary hemorrhage, secondary bacterial infection, or severe hepatitis.
- Late Congenital Syphilis: Subclinical in 60% of cases.
9. SPECIAL CONSIDERATIONS¶
- ■ PREGNANCY
- All pregnant women should be serologically screened at their first antenatal visit.
- Where the prevalence of syphilis in women is high or when the patient is at high risk of reinfection, testing should be repeated at 28 weeks and at delivery.
- Those testing positive should be treated immediately, even before receiving results of confirmatory tests.
- Adequate treatment of the woman before the 16th week of pregnancy should prevent fetal damage.
- Treatment before the third trimester should adequately treat the infected fetus.
- During the current BPG shortage, many clinics are treating nonpregnant patients with doxycycline, thus reserving BPG for seropositive pregnant women.
- ■ HIV CO-INFECTION
- Neurosyphilis is more frequently symptomatic in patients co-infected with untreated HIV, particularly those with low CD4+ T lymphocyte counts.
- Most experts agree that clinical neurosyphilis is more common among persons with untreated HIV infection.
- The immune reconstitution seen with effective ART may have a protective effect against development of clinical neurosyphilis in some HIV-infected persons with syphilis.
- RPR titer ≥1:32 is still associated with reactive CSF VDRL, even in persons taking effective ART.
- ■ MSM & REINFECTION
- A growing number of individuals, particularly MSM, acquire multiple episodes of syphilis.
- After treatment, persons with past syphilis are less likely to revert to nonreactive in the VDRL/RPR tests than persons with first episode syphilis.
- Subsequent episodes of syphilis are more likely to be asymptomatic than initial episodes.
- Less likely to have T. pallidum identified in blood or CSF.
- Less likely to have laboratory-defined neurosyphilis.
- More frequent (every 3 months) screening for syphilis and other sexually transmitted infections is warranted in high-risk populations.
- Recent data suggest that PEP with 200 mg of doxycycline (Doxy-PEP), taken within 72 h of exposure, will significantly reduce the likelihood of syphilis (and other) infections in MSM.
- Concerns have been raised that widespread use of Doxy-PEP (perhaps misused as PrEP) may result in selection for resistance in sexually transmitted infection pathogens.
9.1 Pregnancy & HIV¶
- Pregnancy: Screen at first visit, repeat at 28 weeks and delivery if high risk.
- Treatment: BPG preferred for pregnant women; Doxycycline for nonpregnant during shortage.
- HIV: Neurosyphilis more common in untreated HIV; ART may have protective effect.
- CSF VDRL: Associated with RPR titer ≥1:32 even with ART.
9.2 MSM & Reinfection¶
- Screening: Every 3 months in high-risk populations.
- Reinfection: More likely to be asymptomatic.
- PEP: Doxy-PEP (200 mg within 72 h) reduces likelihood of infection in MSM.
- Resistance: Concerns about widespread use of Doxy-PEP.
10. KEY PEARLS & CLINICAL TRAPS¶
- Primary chancre is typically painless and indurated with cartilaginous consistency.
- Secondary syphilis rash often involves palms and soles.
- Condylomata lata are highly infectious and found in intertriginous areas.
- Mucous patches are painless silver-gray erosions.
- Argyll Robertson pupil reacts to accommodation but not to light.
- Hutchinson's teeth are centrally notched, widely spaced, peg-shaped upper central incisors.
- Mulberry molars are sixth-year molars with multiple, poorly developed cusps.
- CSF abnormalities occur in up to 40% of untreated primary/secondary syphilis cases.
- Lipoidal tests (RPR/VDRL) are recommended for screening due to lower false-positive rate compared to treponemal tests in low-prevalence populations.
- Syphilis is excluded by a nonreactive treponemal test in the setting of a false-positive lipoidal test.
10.1 Board Exam Favorites¶
- Chancre characteristics: Painless, indurated, cartilaginous.
- Rash distribution: Palms and soles.
- Pupil: Argyll Robertson (accommodation yes, light no).
- Teeth: Hutchinson's (notched incisors), Mulberry (molars).
- CSF: Pleocytosis, protein >45 mg/dL, VDRL reactive.
- Screening: Lipoidal first, then Treponemal.
WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Characteristic indurated chancre with cartilaginous consistency.
- Classic iritis or uveitis in ocular syphilis.
- Classic stigmata of congenital syphilis (Hutchinson's teeth, mulberry molars, saddle nose, saber shins).
- Argyll Robertson pupil (reacts to accommodation, not light).
- Generalized nontender lymphadenopathy in secondary syphilis (85%).
- Maculopapular truncal eruption with papules on palms and soles.
- Constitutional signs: Sore throat, fever, weight loss, malaise, anorexia, headache, meningismus.
- Bone changes detectable by x-ray examination of long bones in congenital syphilis.
- Hepatic involvement: Abnormal liver function tests in up to 25% of patients.
10.2 Specific Findings¶
- Chancre: Single painless papule, erodes, indurated.
- Rash: Macular, papular, papulosquamous, pustular.
- Condylomata lata: Broad, moist, pink/gray-white.
- Mucous patches: Painless silver-gray erosion.
- Ocular: Pupillary abnormalities, optic neuritis.
- Otic: Sensorineural hearing loss.
- CNS: Headache, nausea, vomiting, neck stiffness, seizures, mental status changes.
WHAT EXCLUDES THE DIAGNOSIS¶
- Syphilis is excluded by a nonreactive treponemal test in a patient with a false-positive lipoidal test.
- False-positive reactions may also occur with treponemal tests, particularly the EIA/CIA tests.
- Screening a low-prevalence population for syphilis with a treponemal test may result in true-positive reactions being outnumbered by false-positive reactions, leading to unnecessary treatment.
- Re-treatment rarely achieves the desired goal and is not recommended in the absence of clinical findings.
- Lipoidal test titers may fail to become nonreactive or remain reactive in low titer after treatment in persons with repeated episodes of syphilis; implications unclear.
10.3 Exclusion Criteria¶
- Nonreactive treponemal test: Excludes syphilis in false-positive lipoidal test.
- Low-prevalence population: Treponemal test may yield more false-positives than true-positives.
- Post-treatment: Treponemal tests often remain reactive; not helpful for determining infection status of persons with past syphilis.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
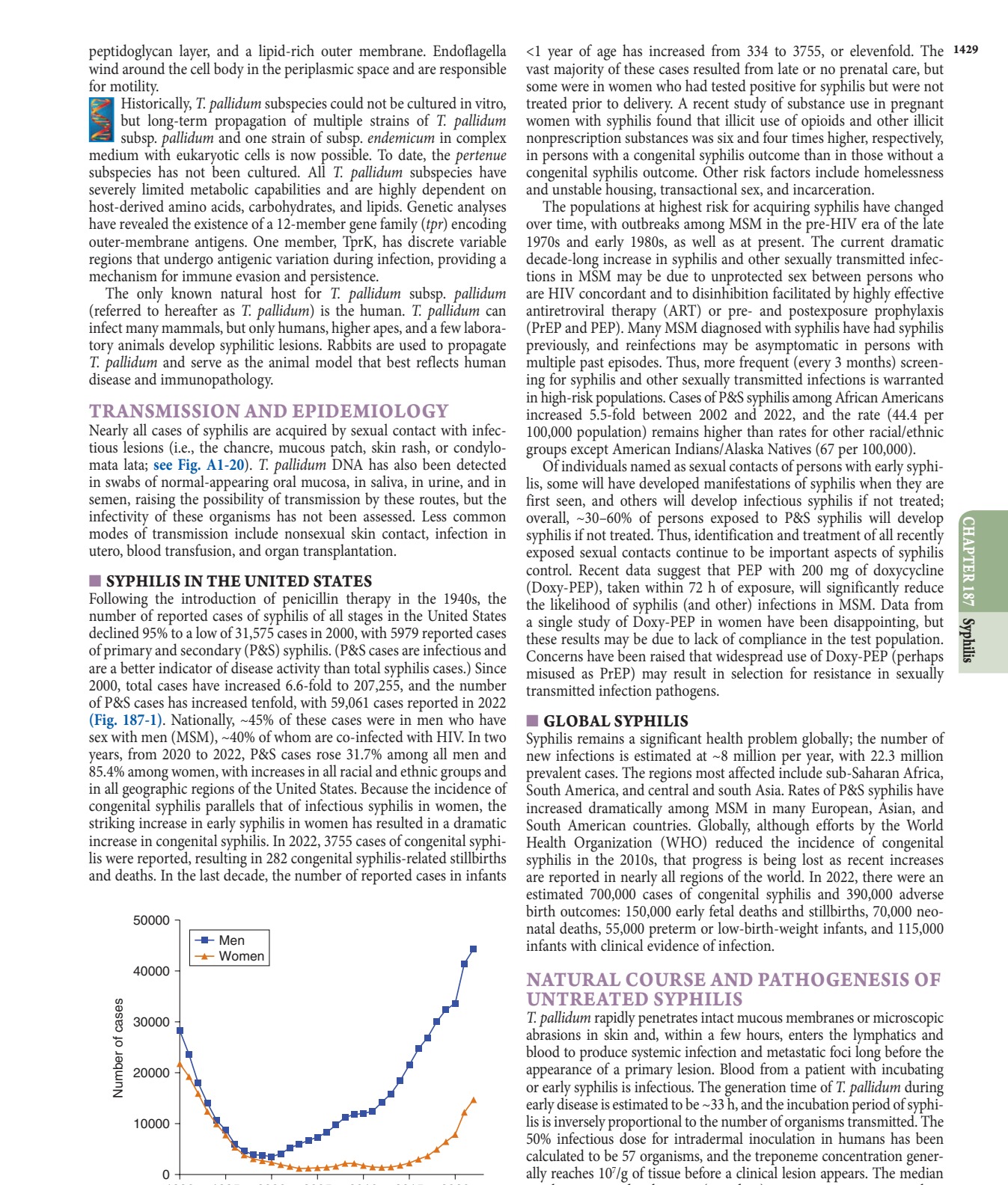
Caption: FIGURE 187-1 Primary and secondary syphilis in the United States, 1990–2022, by of sex. (Data from the Centers for Disease Control and Prevention.) — Figure 187-1: Primary and secondary syphilis in the United States, 1990–2022, by sex. Data from the Centers for Disease Control and Prevention showing a dramatic increase in cases, particularly among men who have sex with men (MSM) and women.
Figure 2¶

Caption: FIGURE 187-2 Primary syphilis with a firm, nontender chancre. — Figure 187-2: Primary syphilis with a firm, nontender chancre. The lesion is typically located on the penis in heterosexual men, but may occur on the anal canal, rectum, or mouth in MSM, and on the cervix, vaginal wall, or labia in women.
Figure 3¶

Caption: FIGURE 187-3 Secondary syphilis. Left: Maculopapular truncal eruption. Middle: Papules on the soles. (Photos courtesy of Jill McKenzie and Christina Marra.) In warm, moist, intertriginous areas (commonly the perianal region, vulva, and scrotum), papules can enlarge to produce broad, moist, pink or gray-white, highly infectious lesions (condylomata lata; see Fig. A1-20) in 10% of patients with secondary syphilis. Superficial mucosal erosions (mucous patches) occur in 10–15% of patients and commonly involve the oral or genital mucosa (see Fig. A1-21). The typical mucous patch is a painless silver-gray erosion surrounded by — Figure 187-3: Secondary syphilis. Left: Maculopapular truncal eruption. Middle: Papules on the palms. Right: Papules on the soles. Lesions are often nonpruritic and may involve the palms and soles.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.