Tularemia¶
Chapter 175 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Tularemia is a zoonotic disease caused by Francisella tularensis, a small, facultatively intracellular, aerobic, gram-negative, pleomorphic bacterium.
- Two subspecies of high clinical importance exist: F. tularensis subspecies tularensis (Type A) and F. tularensis subspecies holarctica (Type B).
- Type A strains are significantly more lethal in experimentally infected rabbits and have higher human mortality in the United States.
- Clinical recognition may be challenging; patients often present with an acute fever onset episode with influenza-like illness.
- The incubation period is usually 3–5 days but may range from 1 to 21 days.
- Early specific antimicrobial treatment is essential to avoid complications; antibiotics of choice include ciprofloxacin, levofloxacin, gentamicin, or doxycycline.
- Serology remains the mainstay diagnostic in many laboratories, relying on a significant increase of antibody titers between two samples taken 2–4 weeks apart.
- Prior to antibiotics, case fatality rates were 5%–15% and could be as high as 60% for respiratory/pneumonic tularemia.
- Recent surveillance data (2006–2021) show a 3.0% death rate among 903 patients with illness outcome available.
- Culture of F. tularensis from a clinical specimen is associated with significantly reduced odds of survival (OR, 0.1).
- Treatment duration is usually at least 10 days for adults; relapse occurs in up to 30% of poorly compliant patients.
- Postexposure prophylaxis is recommended for high-risk exposures, including performing aerosol-generating procedures with F. tularensis cultures outside a biologic safety cabinet.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Biosafety & Laboratory Handling
- 2. EPIDEMIOLOGY
- 2.1 Maintenance in Nature
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Immune Response
- 4. CLINICAL FEATURES
- 4.1 Clinical Forms
- 4.2 Laboratory Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Specimen Collection
- 6.2 Imaging Findings
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Treatment
- 7.2 Postexposure Prophylaxis
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Relapse & Follow-up
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
- Tularemia is a zoonotic disease that can naturally be transmitted from vertebrate animals to humans, causing a febrile illness.
- Synonyms include deer-fly fever, rabbit fever, market men’s disease, water-rat trappers’ disease, wild hare disease (yato-byo), Francis’ disease, and Ohara’s disease.
- Tularemia was described by the American researchers McCoy and Chapin as a “plague-like disease of rodents” in California in 1911.
- The bacterium was cultivated and described as “Bacterium tularense,” later named after Edward Francis.
- The disease is endemic to the Northern Hemisphere but has a patchy and geographically uneven distribution.
- In the United States, reported human cases have dropped sharply from several thousand annual cases before 1950 to 200–300 cases annually from 2010–2020.
- Most cases are associated with tick bites in Arkansas, Kansas, Missouri, and Oklahoma.
- In some parts of Europe and Asia, tularemia was relatively more common in 2010–2022, with several hundred to >2000 cases in peak years in Finland, Sweden, and Turkey.
- In the Northern Boreal Forest regions of Sweden, Finland, and Russia, tularemia is primarily associated with mosquito bites, while tick bites are more common in Western and Eastern Europe.
- In the Southern Hemisphere, rare human and animal infections have been documented from Australia.
- It is uncertain whether the lack of reporting from other areas of the Southern Hemisphere is due to a lack of disease or from underreporting.
1.1 Biosafety & Laboratory Handling¶
- F. tularensis is highly virulent for humans and numerous mammals, including rodents, hares, and rabbits.
- It is known to cause airborne laboratory-acquired infection.
- Laboratory work, including culturing of the bacterium, must be performed by trained staff in biologic safety cabinets under biosafety level 3 conditions.
- F. tularensis is a U.S. Department of Health and Human Services (HHS) Tier 1 Select Agent.
- An accurate culture diagnosis in the clinic is challenging.
- Cultivation of F. tularensis requires Biosafety Level 3 (BSL-3) laboratories.
2. EPIDEMIOLOGY¶
- F. tularensis infects humans through bites of arthropods functioning as disease vectors (e.g., mosquitoes, ticks, tabanid flies), inhaling infectious aerosols, handling infected animals, or ingesting contaminated water.
- The reported human cases represent bridging between endemic F. tularensis maintenance in nature, or spillover events from massive amplification in infected rodents, hares, or rabbits during disease outbreaks among animals (epizootics).
- Based on extensive historic field studies performed in the United States and the former Soviet Union during the 1950s–1970s, it is believed that distinct disease ecologies characterize F. tularensis subspecies tularensis (type A) and F. tularensis subspecies holarctica (type B).
- This concept recognizes the association of type A tularemia with rabbits, ticks, domestic cats, and sheep in comparatively dry environments.
- In contrast, type B tularemia is associated with streams, ponds, lakes, rivers, and semiaquatic animals such as muskrats and beavers.
- In Finland and Sweden, cases occur during summer, likely reflecting increased human exposure to blood-feeding arthropods, infected wildlife mammals, or aerosols from carcasses of infected animals during outdoor activities.
- In contrast to this seasonal pattern, most cases occur in the winter months in Turkey, where the predominant infection route to humans in some rural areas is nonchlorinated drinking water from natural springs that may be contaminated by infected rodents.
- Colder temperatures enhance the survival of the bacterium in water during winter.
- F. tularensis is a generalist eukaryotic host-associated microbe that can infect many animals and cell types, including amphibians, birds, rodents, rabbits, carnivores, and ruminant mammals.
- Most of these animals are accidental hosts or rapidly die from septic disease.
- It remains unknown exactly how the bacterium is maintained in nature.
- F. tularensis can infect multiple species of soft and hard ticks, supporting the idea of tularemia as an obligate vector-borne disease with ticks as reservoirs.
- In North America, tularemia in humans is mainly tick-borne, but the role of ticks in maintaining and spreading the disease geographically is more debated compared with other pathogens like Babesia and Borrelia.
- Contemporary well-designed experiments involving mice and American dog ticks have tested F. tularensis type A strains from three main genetic clades and a type B strain.
- They demonstrated rapid F. tularensis acquisition by adult ticks from bacteremic mice, an interrupted blood-feeding behavior, and high transmission efficiency to uninfected mice (58–89%).
- Ticks of the more immature nymph life stage showed low survival after F. tularensis ingestion and low transmission efficiency (0–13.5%), indicating that these are ineffective disease vectors.
- Overall, both older and newer studies suggest that F. tularensis infection poses a high burden for immature tick stages, and the literature is conflicted on the presence of transovarial transmission in ticks.
2.1 Maintenance in Nature¶
- It remains unknown exactly how the bacterium is maintained in nature.
- When an animal dies from a tularemia infection with a high level of bacteria in their bodies, this can potentially help temporarily maintain the bacteria in the environment.
- Over the long term, decaying infectious tissues might also contribute to the bacteria’s persistence under certain conditions.
- Another hypothesis for maintenance of F. tularensis is persistence in water with protozoa such as amoeba serving as host cells.
- Since the 1940s, research has shown that F. tularensis can infect multiple species of soft and hard ticks, supporting the idea of tularemia as an obligate vector-borne disease with ticks as reservoirs.
- To better understand the zoonotic potential and the epidemiology seen in humans, a better understanding of how F. tularensis is maintained between outbreaks will be required.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Tularemia is caused by Francisella tularensis, a small (0.2–0.7 × 0.2 µm), facultatively intracellular, aerobic, gram-negative, pleomorphic bacterium.
- There are two F. tularensis subspecies of high clinical importance: F. tularensis subspecies tularensis (aka Jellison type A) with human disease documentation exclusively from the North American continent, and subspecies holarctica (Jellison type B) with human disease documentation both from North America and from other parts of the world.
- A third subspecies, F. tularensis subspecies mediasiatica, has been isolated from vertebrate animals in Central Asia and Russia, but there is no documented disease in humans.
- The division into type A and type B strains of F. tularensis is based on minor biochemical test differences, with type A strains being significantly more lethal in experimentally infected rabbits.
- Type A but not type B cultures can ferment glycerol and are positive in a citrulline ureidase assay.
- Microbial genome sequencing has revealed an average nucleotide identity >99% between type A and type B strains of F. tularensis, but current and historic epidemiologic studies mirror the experimental findings in rabbits—tularemia mortality among humans is higher with type A in the United States.
- Recent research using high-resolution genetic subtyping, combined with analyses of disease outcomes, shows there is heterogeneity in mortality risks among different type A genetic varieties, with some being less virulent for humans than the type B varieties.
- Genetic neighbors of F. tularensis, including Francisella novicida (sometimes referred to as a fourth subspecies of F. tularensis with a genomic average nucleotide identity of ~97% with other subspecies) and the genetically more distant Francisella philomiragia, are opportunistic pathogens that may cause disease in humans with symptoms varying according to the immune status of the patient.
- Moreover, modern microbiology methods and intense research efforts have resulted in the identification of additional Francisella bacteria, including pathogens of fish, endosymbiont bacteria of ticks, soil bacteria, and bacteria isolated from sea and freshwater, some of which may be opportunistic human pathogens.
- Taxonomists now recognize at least nine distinct Francisella species, including Francisella tularensis, the causative agent of tularemia.
- Natural transmission to humans usually occurs through the skin or by inhalation of aerosols containing F. tularensis, but ingesting infected food or water also may cause infection.
- An extremely low dose of 10–50 bacteria inoculated through microtrauma of the skin or inhaled into the lungs suffices to cause disease in humans.
- In contrast, a dose in the range of 106–108 bacteria is required to infect humans and other primates by the oral route.
- Tissue-resident macrophages, including alveolar macrophages in the lung and Langerhans cells in the skin, are believed to be important in the transport of F. tularensis by blood or lymph vessels to lymph nodes, spleen, and bone marrow.
- In the skin, F. tularensis undergoes phagocytosis by neutrophils at initial stage of infection.
- After the bacteria have been taken up by tissue-resident macrophages and other local phagocytic cells, F. tularensis escapes from the phagosome into the cell cytosol, replicates, leaves the cell, and disseminates throughout the host.
- F. tularensis is a “stealth pathogen,” implying that the bacterium is able to manipulate host-cell signaling, thus rendering itself a safe milieu inside the host cell suitable for its replication.
- In experimental oral infection of mice, there is minimal local gastrointestinal pathology despite the large infection dose required.
- It remains unknown what cell types mediate F. tularensis to cross the intestinal epithelium to cause fatal systemic infection.
- Gross and histopathology findings in nonhuman primates experimentally infected by the inhalation route have shown 0.5- to 1-mm necrotic lesions with live bacteria in the spleen at day 4 after the infection, and subsequent larger foci in liver and lymph nodes at days 5–7, which likely mirror disease events and progression in more severe human tularemia cases.
- At day 6 after infection of nonhuman primates, randomly scattered subacute abscesses and pyogranulomas 6–20 mm in diameter have been observed on the lung surfaces.
- From day 7 and onward, granuloma formation and necrotic lesions in tissues surrounded by layers of macrophages, lymphocytes, and giant cells are typical reaction patterns in lymph nodes, lungs, spleen, kidney, and skin, corroborated by historic reports of similar autopsy findings in fatal human tularemia.
- The immune invasion strategy of F. tularensis—delaying the immune response and permitting rapid systemic distribution—has made studies of early immune responses challenging.
- The mechanisms behind cell-mediated responses against F. tularensis after a primary infection or vaccination by the live vaccine strain of F. tularensis, however, are well described and require both B and T cells, resulting in antigen-specific recall T cell responses persisting 25–30 years after infection or vaccination.
- Nevertheless, although the bacterium can manipulate and delay them, effective early immune responses occur and involve complement, antibodies, neutrophils, inducible NO synthase, phagocyte oxidase, and cytokines such as interferon γ, tumor necrosis factor α, and interleukin 12.
3.1 Immune Response¶
- The immune invasion strategy of F. tularensis—delaying the immune response and permitting rapid systemic distribution—has made studies of early immune responses challenging.
- The mechanisms behind cell-mediated responses against F. tularensis after a primary infection or vaccination by the live vaccine strain of F. tularensis, however, are well described and require both B and T cells, resulting in antigen-specific recall T cell responses persisting 25–30 years after infection or vaccination.
- Nevertheless, although the bacterium can manipulate and delay them, effective early immune responses occur and involve complement, antibodies, neutrophils, inducible NO synthase, phagocyte oxidase, and cytokines such as interferon γ, tumor necrosis factor α, and interleukin 12.
4. CLINICAL FEATURES¶
- Clinical recognition of tularemia may be challenging, especially if the patient does not spontaneously report fever.
- Sporadic cases of patients seeking health care can easily be misdiagnosed with a diversity of other conditions, including lung cancer, head and neck cancer, lymphoma, tuberculosis, or another disease with lymphoid tissue engagement or a suspected tumor.
- Tularemia may not be suspected before extensive and costly medical investigations have already been performed.
- Awareness of the disease and a high index of suspicion is critical.
- Even in high-endemic areas, patients with tularemia often initially are mistakenly managed and treated for other conditions, including unspecified viral infection, common skin and soft tissue infection, common community-acquired pneumonia, or undifferentiated fever or sepsis.
- A careful disease history of a patient with tularemia typically reveals an acute fever onset episode with influenza-like illness.
- If the patient seeks care immediately, an acute fever onset can be easily recollected; if care is sought several weeks after initial symptoms, acute onset of fever may not be mentioned spontaneously.
- The acute illness may be described as “a severe virus” with high fever, muscle pain, headache, and other constitutional symptoms.
- Fever may be persistent or intermittent.
- A tularemia-focused disease history should include risk factors for exposure to F. tularensis and epidemiologic information (e.g., household member or friend having similar symptoms and sharing the same exposure).
- Exposure risk factors or activities include wild animal contact (e.g., rodents, rabbits, hares), contact with or inhalation of dust contaminated with their urine or feces, recent arthropod bites (tick, fly, or mosquitoes), performing brush cutting or grass trimming, handling of wood, handling of hay, and walking or hunting in the forest or other natural habitats of wildlife species.
- When tularemia is suspected it is important to define patient factors with relevance for coping with infection, to define the infection syndrome, and to decide on an appropriate level for patient management.
- Consider factors that may increase the risk of severe infection (e.g., geriatric frailty, immunosuppression, severe lung and/or heart function impairment, other significant comorbidities).
- By physical examination, determine any anatomic location and extent of inflammation (e.g., presence of pneumonitis, lymph node inflammation, skin inflammation including minute ulcers or pustules, pharyngitis).
- Collect information on the rate of progression and judge the severity of infection.
- Determine an appropriate level of care (e.g., localized symptoms likely suitable for outpatient care, multiorgan involvement/hemodynamic instability suggesting inpatient care).
- The most common initial manifestation of tularemia is an influenza-like illness with high fever.
- The incubation period is usually 3–5 days but may range from 1 to 21 days.
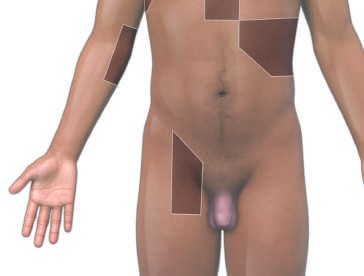
- Inflamed swollen lymphoid tissue is typical for tularemia.
- The initial infection route determines what lymphoid tissue is engaged.
- If bacteria are acquired through skin or oral mucous membranes of the pharynx, palpable enlarged tender regional lymph node(s) can result.
- If bacteria are inhaled, the result will be lymph node enlargement in the mediastinum.
- Different recognized clinical forms of tularemia are the same for type A and type B tularemia and depend on the initial F. tularensis infection route.
- The primary tularemia ulcer is often a small break in the skin, with limited signs of inflammation, and may require careful clinical examination to be detected.
- In some cases, it may not be detectable and the disease form will then be classified as glandular.
- Red, tender, swollen lymph regional nodes are often the most remarkable clinical examination findings in patients with acute ulceroglandular tularemia.
- In oropharyngeal and oculoglandular tularemia, there is more often pronounced local inflammation at the primary site of infection with acute pharyngitis or conjunctivitis, respectively.
- The respiratory or pneumonic form of tularemia acquired by inhalation of F. tularensis may, more often than other clinical forms, be bacteremic and progress to severe disease requiring inpatient care, particularly in patients aged 65 and over and those with comorbidities.
- In the respiratory/pneumonic clinical form of tularemia, onset of dry cough may occur more than 7 days after onset of the influenza-like illness.
- “Typhoidal tularemia” is an older medical classification term referring to a disease syndrome like typhoid fever with prolonged high fever, fatigue, headache, and nausea.
- It is recommended to avoid using this term, if possible, as it is believed that historically, most cases of typhoidal tularemia were acquired by inhalation and were, in fact, respiratory/pneumonic tularemia.
- For type A tularemia, historic disease descriptions suggest that respiratory/pneumonic tularemia or meningitis may also occur as secondary manifestations in severe cases of ulceroglandular disease.
- Data from the United States in 2006–2021 on 1046 cases with primary disease manifestations available showed 47% ulceroglandular, 18% glandular, 17% pneumonic or respiratory, 14% typhoidal, 2% oculoglandular, and 2% oropharyngeal disease.
4.1 Clinical Forms¶
- Ulceroglandular or glandular: Skin inoculation by blood-feeding arthropods or direct contact (touching infected animal or F. tularensis contaminated material).
- Oropharyngeal: Ingestion of contaminated water or food.
- Oculoglandular: Touching the eye with contaminated fingers or exposure to contaminated aerosol.
- Respiratory/pneumonic: Inhalation of contaminated aerosol.
- Typhoidal: Unknown (likely by inhalation, rarely by ingestion).
- Additional less common but well-described clinical invasive manifestations of tularemia exist, including primary tularemia meningitis, endocarditis, and bone and joint infections.
- In patients with immunosuppression, tularemia manifestations may be indolent with few focal symptoms and signs.
4.2 Laboratory Findings¶
- Routine biochemical testing of blood generally is not helpful in tularemia because findings are unspecific and may or may not reveal elevated liver enzymes or red blood cells in the urine.
- In a recent more extensive case series from Sweden of type B tularemia of primarily outpatients, white blood cell counts remained within normal limits for 70% of patients, and the median C-reactive protein level was moderately elevated, peaking at day 7–9 after disease onset at a median of 78 mg/L (range, 30–130).
- A recent analysis of 33 patients hospitalized with severe respiratory type B tularemia showed peak C-reactive protein levels at 100–400 mg/L among patients with F. tularensis growth in blood cultures and 50–220 mg/L among nonbacteremic patients.
5. DIFFERENTIAL DIAGNOSIS¶
- Sporadic cases of patients seeking health care can easily be misdiagnosed with a diversity of other conditions.
- Conditions to consider include lung cancer, head and neck cancer, lymphoma, tuberculosis, or another disease with lymphoid tissue engagement or a suspected tumor.
- Tularemia may not be suspected before extensive and costly medical investigations have already been performed.
- Even in high-endemic areas, patients with tularemia often initially are mistakenly managed and treated for other conditions.
- These include unspecified viral infection, common skin and soft tissue infection, common community-acquired pneumonia, or undifferentiated fever or sepsis.
6. INVESTIGATIONS & DIAGNOSIS¶
- Laboratory confirmation is recommended and may be based on recovery of an F. tularensis isolate, F. tularensis–specific antigens or nucleic acids, or the detection of F. tularensis–specific antibodies in blood by serology testing.
- Appropriate clinical specimens to collect for direct detection of F. tularensis by nucleic acids or culture include ulcer specimens, lower respiratory tract specimens (sputum/tracheal washing/bronchoalveolar lavage), lymph node biopsies or aspirates, and blood cultures.
- Additional clinical specimens with F. tularensis growth reported include pharyngeal and ventricular washings.
- Importantly, sampling from ulcers should be performed from the edge of the wound, preferably selecting a swab with a slightly stiffer stick and some rubbing of the tissue so that it becomes somewhat blood-tinged.
- If there is a scab, this should be removed before sampling.
- If culture specimens are sent to a clinical microbiology laboratory, a suspicion of tularemia must be clearly communicated to the laboratory in advance to minimize the risk of laboratory-acquired infections in lab workers.
- Direct detection of F. tularensis–specific nucleic acid in clinical specimens by polymerase chain reaction or another detection method is a rapid and reliable diagnostic method.
- For ulcer specimens, the method is comparable with culture in sensitivity and specificity.
- There is clinical experience of F. tularensis nucleic acid detection from other specimen types, including sputum, bronchoalveolar lavage, and lymph node biopsies/aspirates, but formal scientific evaluation of the diagnostic performance is lacking.
- With increased availability of molecular methods in some clinical microbiology laboratories, nucleic acid–based subtyping without a prior culture step can be performed directly from clinical specimens and may help clinicians to identify F. tularensis varieties rapidly.
- Identification of the subspecies and genetic variety involved in tularemia infections is currently limited in most laboratories but may be of greatest importance in North America, where type A and type B tularemia exist side by side.
- Cultivation of F. tularensis requires Biosafety Level 3 (BSL-3) laboratories, and because F. tularensis is a U.S. Department of Health and Human Services (HHS) Tier 1 Select Agent, an accurate culture diagnosis in the clinic is challenging.
- However, culture identification provides a definitive diagnosis and allows for subsequent genetic methods to identify different F. tularensis varieties with varying risks of mortality.
- Unexpected findings in blood cultures with matrix-assisted laser desorption/ionization–time-of-flight (MALDI-TOF) mass spectrometry identification of F. tularensis is a scenario that has become more common in recent years with the improvement of blood culture systems and MALDI-TOF reference libraries.
- F. tularensis is a slow-growing bacterium, and an incubation period of 10 days is recommended for optimal sensitivity in blood-culture diagnostics.
- Serology remains commonly used to confirm tularemia and is the mainstay diagnostic in many clinical microbiology laboratories.
- Serology is particularly useful in patients when tularemia is suspected as a differential diagnosis at a later stage—the antibody responses against F. tularensis are generally detectable in the blood of patients 10–20 days post-infection using an enzyme-linked immunosorbent assay or a microagglutination test.
- Some commercial serologic tests may detect F. tularensis–specific antibodies as early as 1–2 weeks after disease onset.
- Importantly, the persistence of F. tularensis antibodies is prolonged, meaning that up to at least 1 year after acute infection, single titers of antibodies remain above the cutoff set by laboratories to detect acute infections.
- Therefore, a reliable serologic diagnosis of tularemia in the acute phase should rely on the demonstration of a significant increase of antibody titers between two samples taken 2–4 weeks apart.
- Chest imaging is useful in respiratory tularemia.
- Single or multifocal consolidation may be present, accompanied by pleural effusion with hilar and mediastinal lymphadenopathy.
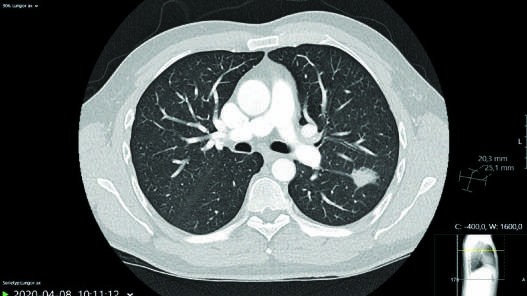
- Computed tomography (CT) scans in the acute phase may reveal multiple rounded consolidations, often in the subpleural region and sometimes with signs of inclusion necrosis with a diffuse marginal zone.
- Lymph node enlargements in the mediastinal and hilar regions on a CT scan may also contain necrotic inclusions.
- A relatively common scenario for sporadic cases of tularemia is pulmonary nodules or dense consolidations, which can mimic lung cancer, resulting in more extensive clinical investigation paths to exclude cancer, including CT and positron emission tomography (PET) scans.
- Endobronchial ultrasound bronchoscopy procedures with biopsy may be performed in some cases before tularemia is suspected.
- The resolution of tularemia pathology on chest imaging may be slow and take months.
6.1 Specimen Collection¶
- Ulcer specimens: Sampling from the edge of the wound, preferably selecting a swab with a slightly stiffer stick and some rubbing of the tissue so that it becomes somewhat blood-tinged.
- If there is a scab, this should be removed before sampling.
- Lower respiratory tract specimens: Sputum/tracheal washing/bronchoalveolar lavage.
- Lymph node biopsies or aspirates.
- Blood cultures.
- Additional clinical specimens with F. tularensis growth reported include pharyngeal and ventricular washings.
6.2 Imaging Findings¶
- Chest imaging is useful in respiratory tularemia.
- Single or multifocal consolidation may be present, accompanied by pleural effusion with hilar and mediastinal lymphadenopathy.
- Computed tomography (CT) scans in the acute phase may reveal multiple rounded consolidations, often in the subpleural region and sometimes with signs of inclusion necrosis with a diffuse marginal zone.
- Lymph node enlargements in the mediastinal and hilar regions on a CT scan may also contain necrotic inclusions.
- A relatively common scenario for sporadic cases of tularemia is pulmonary nodules or dense consolidations, which can mimic lung cancer, resulting in more extensive clinical investigation paths to exclude cancer, including CT and positron emission tomography (PET) scans.
- The resolution of tularemia pathology on chest imaging may be slow and take months.
7. MANAGEMENT & TREATMENT¶
- Specific antimicrobial treatment is highly recommended for tularemia as outlined in Table 175-2.
- The antibiotics of choice are ciprofloxacin, levofloxacin, gentamicin, or doxycycline.
- Early specific antimicrobial treatment is essential to avoid complications irrespective of targeting type A or type B tularemia.
- Several commonly used antimicrobials, including all the β-lactam drugs and clindamycin, lack treatment efficacy against F. tularensis.
- Macrolide antibiotics, including erythromycin and azithromycin, show an in vitro effect against F. tularensis type A and type B varieties known to be present in the United States, but globally there are very scarce treatment outcome data for these drugs in humans.
- Generally, macrolide antibiotics are not recommended for tularemia because macrolide-resistant type B strains are common in Europe and Asia, resulting in total lack of treatment effect and overall little experience using these drugs for tularemia treatment.
- Azithromycin, however, may be an alternative treatment choice for patients with verified type A infection according to recent CDC guidelines.
- Streptomycin, classically used to treat tularemia, has been the drug of choice due to its high cure rate in a U.S. case series reported from 1949–1988, but is now considered a less attractive alternative to gentamicin due to its drawbacks, including the need for intramuscular administration, limited clinical availability, and a higher risk of vestibular and renal toxicity compared with newer aminoglycoside antibiotics.
- Chloramphenicol is another drug with a higher risk of adverse effects that, for this reason, is seldom used systemically in modern medicine.
- Chloramphenicol has an in vitro effect against F. tularensis and was reportedly effective in treating tularemia meningitis in the past.
- Inflamed lymph nodes can progress into an abscess with local and/or systemic reaction and may occur in about one-third of patients, especially if there were delays in F. tularensis–specific antibiotic treatment.
- An antibiotic treatment delay of >2–3 weeks after disease onset has been statistically associated with lymph node abscess formation.
- In some cases, the progression to a lymph node abscess may occur despite ongoing appropriate antibiotic treatment initiated late in the disease course.
- It is unclear if extending the antibiotic treatment duration is of clinical benefit.
- Culture specimens from an abscess at this disease stage are typically F. tularensis negative, but an additional 10–day course of appropriate antibiotic treatment is often used to avoid further disease progression and may be successful.
- If the clinician considers that there is a clear and immediate risk of spontaneous rupture of the skin or the mucus membranes in the pharynx with suppuration of pus, open surgical drainage or needle aspiration is recommended for treatment.
- A more invasive procedure with total surgical excision may be needed in more complicated and long-standing cases.
- Another complication occasionally reported by patients includes postinfectious persisting fatigue and disability.
- Additional complications or disease manifestations of tularemia have been reported, including adult respiratory distress syndrome, myocarditis, pericarditis, endocarditis, meningitis, osteomyelitis, hepatitis, and renal failure.
- Postexposure prophylaxis is recommended for high-risk exposures, including performing aerosol-generating procedures with F. tularensis cultures outside a biologic safety cabinet or handling infected animals.
- There are extensive human data showing that doxycycline is effective.
- For low-risk exposures, preparedness for early treatment may suffice using daily “fever watch”: the patient monitors temperature with instructions to seek immediate treatment if developing a fever.
7.1 Pharmacologic Treatment¶
- Preferred choices: Ciprofloxacin 400 mg every 8 hrs IV or 750 mg every 12 hrs PO, Levofloxacin 750 mg every 24 hrs IV or PO, Gentamicin 5–7 mg/kg IV or IM per day given every 12 hrs or 24 hrs, Doxycycline 200 mg loading dose, then 100 mg every 12 hrs IV or PO.
- Alternative choices having less supporting clinical data are high-dose moxifloxacin, ofloxacin, amikacin, tobramycin, or plazomycin for 10 days.
- In verified type A-infection, azithromycin may be considered based on in vitro susceptibility analysis.
- Doxycycline may safely be included as a preferred choice for patients with nonsevere disease but is associated with a higher frequency of fever relapse and needs a more extended treatment duration.
- Tetracycline 500 mg every 6 hrs IV or PO for 14-21 days is equivalent to doxycycline.
- Patients beginning with IV treatment of ciprofloxacin, levofloxacin, or doxycycline can switch to oral administration when clinically indicated.
7.2 Postexposure Prophylaxis¶
- Doxycycline 100 mg PO twice daily for 14 days.
- Ciprofloxacin 500 mg every 12 hrs PO for 10 days.
- For low-risk exposures, preparedness for early treatment may suffice using daily “fever watch”: the patient monitors temperature with instructions to seek immediate treatment if developing a fever.
- Postexposure prophylaxis is recommended for high-risk exposures, including performing aerosol-generating procedures with F. tularensis cultures outside a biologic safety cabinet or handling infected animals.
8. PROGNOSIS & COMPLICATIONS¶
- Prior to the use of antibiotics to treat tularemia, case fatality rates in the United States were typically 5%–15% and could be as high as 60% for patients with respiratory/pneumonic tularemia.
- Recent surveillance data of tularemia in the United States between 2006 and 2021 show that of 903 patients with illness outcome available, 27 patients (3.0%) died.
- Culture of F. tularensis from a clinical specimen was present in approximately 50% of cases and associated with significantly reduced odds of survival (odds ratio [OR], 0.1; 95% confidence interval [CI], 0.04–0.4).
- Treatment with at least one high-efficacy antimicrobial drug class (aminoglycoside, fluoroquinolone, or tetracycline) was independently associated with increased odds for survival (adjusted OR, 10.4; 95% CI, 4.4–24.5 after controlling for disease severity).
- Notably, previous surveillance data from 1964–2004 considering the modern genetic distinction of three epidemiologically important type A genetic varieties in the United States found a 24% fatality outcome for the most lethal variety.
- Relapse occurs in up to 30% of poorly compliant patients.
- Thus, patients should ideally be followed clinically for up to 2 years to detect relapse, which responds to a prolonged course of the same therapy used originally.
- The general well-being and the body weight of the patient are more useful guides than serology to lack of relapse.
- IgG antibody levels detected by the standard agglutination test and its variants can remain in the diagnostic range for >2 years after successful treatment.
- Complement fixation titers usually fall to normal within 1 year of cure.
- Immunity is not solid; patients can be reinfected after repeated exposures.
- Fewer than 1% of patients die of brucellosis. (Note: This text snippet contains a reference to brucellosis mortality which appears to be a text bleed from the previous chapter; the Tularemia mortality is 3.0% in recent data).
- When the outcome is fatal, death is usually a consequence of cardiac involvement; more rarely, it results from severe neurologic disease.
- Despite the low mortality rate, recovery from tularemia is slow, and the illness can cause prolonged inactivity, with domestic and economic consequences.
- The existence of a prolonged chronic tularemia state after successful treatment remains controversial.
- Evaluation of patients in whom this state is considered (often those with work-related exposure to brucellae) includes careful exclusion of malingering, nonspecific chronic fatigue syndromes, and other causes of excessive sweating, such as alcohol abuse and obesity.
- In the future, the availability of more sensitive assays to detect Brucella antigen or DNA may help to identify patients with ongoing infection. (Note: This text snippet contains a reference to Brucella which appears to be a text bleed from the previous chapter; the Tularemia section focuses on F. tularensis).
- Inflamed lymph nodes can progress into an abscess with local and/or systemic reaction and may occur in about one-third of patients, especially if there were delays in F. tularensis–specific antibiotic treatment.
- An antibiotic treatment delay of >2–3 weeks after disease onset has been statistically associated with lymph node abscess formation.
- In some cases, the progression to a lymph node abscess may occur despite ongoing appropriate antibiotic treatment initiated late in the disease course.
- It is unclear if extending the antibiotic treatment duration is of clinical benefit.
- Culture specimens from an abscess at this disease stage are typically F. tularensis negative, but an additional 10–day course of appropriate antibiotic treatment is often used to avoid further disease progression and may be successful.
- If the clinician considers that there is a clear and immediate risk of spontaneous rupture of the skin or the mucus membranes in the pharynx with suppuration of pus, open surgical drainage or needle aspiration is recommended for treatment.
- A more invasive procedure with total surgical excision may be needed in more complicated and long-standing cases.
- Another complication occasionally reported by patients includes postinfectious persisting fatigue and disability.
- Additional complications or disease manifestations of tularemia have been reported, including adult respiratory distress syndrome, myocarditis, pericarditis, endocarditis, meningitis, osteomyelitis, hepatitis, and renal failure.
8.1 Relapse & Follow-up¶
- Relapse occurs in up to 30% of poorly compliant patients.
- Thus, patients should ideally be followed clinically for up to 2 years to detect relapse, which responds to a prolonged course of the same therapy used originally.
- The general well-being and the body weight of the patient are more useful guides than serology to lack of relapse.
- IgG antibody levels detected by the standard agglutination test and its variants can remain in the diagnostic range for >2 years after successful treatment.
- Complement fixation titers usually fall to normal within 1 year of cure.
- Immunity is not solid; patients can be reinfected after repeated exposures.
9. SPECIAL CONSIDERATIONS¶
- After significant brucellosis exposure, expert consultation is advised for women who are (or may be) pregnant. (Note: This text snippet contains a reference to brucellosis which appears to be a text bleed from the previous chapter; the Tularemia section does not explicitly detail pregnancy considerations for F. tularensis in the provided text).
- Vaccines based on live attenuated Brucella strains, such as B. abortus strain 19BA or 104M, have been used in some countries to protect high-risk populations but have displayed only short-term efficacy and high reactogenicity. (Note: This text snippet contains a reference to Brucella which appears to be a text bleed from the previous chapter; the Tularemia section does not explicitly detail vaccination for F. tularensis in the provided text).
- Subunit vaccines have been developed but are of uncertain value and cannot be recommended at present.
- Research in this area has been stimulated by interest in biodefense (Chap. S4) and may eventually yield new products.
- The mainstay of veterinary prevention is a national commitment to testing and slaughter of infected herds/flocks (with compensation for owners), control of animal movement, and active immunization of animals.
- These measures are usually sufficient to control human disease as well.
- In their absence, pasteurization of all milk products before consumption is sufficient to prevent nonoccupational animal-to-human transmission.
- All cases of brucellosis in animals and humans should be reported to the appropriate public health authorities. (Note: This text snippet contains a reference to brucellosis which appears to be a text bleed from the previous chapter; the Tularemia section does not explicitly detail reporting for F. tularensis in the provided text).
10. KEY PEARLS & CLINICAL TRAPS¶
- Tularemia may not be suspected before extensive and costly medical investigations have already been performed.
- Even in high-endemic areas, patients with tularemia often initially are mistakenly managed and treated for other conditions, including unspecified viral infection, common skin and soft tissue infection, common community-acquired pneumonia, or undifferentiated fever or sepsis.
- Routine biochemical testing of blood generally is not helpful in tularemia because findings are unspecific and may or may not reveal elevated liver enzymes or red blood cells in the urine.
- In patients with immunosuppression, tularemia manifestations may be indolent with few focal symptoms and signs.
- The primary tularemia ulcer is often a small break in the skin, with limited signs of inflammation, and may require careful clinical examination to be detected.
- In some cases, it may not be detectable and the disease form will then be classified as glandular.
- Red, tender, swollen lymph regional nodes are often the most remarkable clinical examination findings in patients with acute ulceroglandular tularemia.
- In oropharyngeal and oculoglandular tularemia, there is more often pronounced local inflammation at the primary site of infection with acute pharyngitis or conjunctivitis, respectively.
- The respiratory or pneumonic form of tularemia acquired by inhalation of F. tularensis may, more often than other clinical forms, be bacteremic and progress to severe disease requiring inpatient care, particularly in patients aged 65 and over and those with comorbidities.
- In the respiratory/pneumonic clinical form of tularemia, onset of dry cough may occur more than 7 days after onset of the influenza-like illness.
- “Typhoidal tularemia” is an older medical classification term referring to a disease syndrome like typhoid fever with prolonged high fever, fatigue, headache, and nausea.
- It is recommended to avoid using this term, if possible, as it is believed that historically, most cases of typhoidal tularemia were acquired by inhalation and were, in fact, respiratory/pneumonic tularemia.
- For type A tularemia, historic disease descriptions suggest that respiratory/pneumonic tularemia or meningitis may also occur as secondary manifestations in severe cases of ulceroglandular disease.
- Data from the United States in 2006–2021 on 1046 cases with primary disease manifestations available showed 47% ulceroglandular, 18% glandular, 17% pneumonic or respiratory, 14% typhoidal, 2% oculoglandular, and 2% oropharyngeal disease.
- Culture of F. tularensis from a clinical specimen was present in approximately 50% of cases and associated with significantly reduced odds of survival (odds ratio [OR], 0.1; 95% confidence interval [CI], 0.04–0.4).
- Treatment with at least one high-efficacy antimicrobial drug class (aminoglycoside, fluoroquinolone, or tetracycline) was independently associated with increased odds for survival (adjusted OR, 10.4; 95% CI, 4.4–24.5 after controlling for disease severity).
- Notably, previous surveillance data from 1964–2004 considering the modern genetic distinction of three epidemiologically important type A genetic varieties in the United States found a 24% fatality outcome for the most lethal variety.
- Recent surveillance data of tularemia in the United States between 2006 and 2021 show that of 903 patients with illness outcome available, 27 patients (3.0%) died.
- Prior to the use of antibiotics to treat tularemia, case fatality rates in the United States were typically 5%–15% and could be as high as 60% for patients with respiratory/pneumonic tularemia.
- F. tularensis is a slow-growing bacterium, and an incubation period of 10 days is recommended for optimal sensitivity in blood-culture diagnostics.
- Serology is particularly useful in patients when tularemia is suspected as a differential diagnosis at a later stage—the antibody responses against F. tularensis are generally detectable in the blood of patients 10–20 days post-infection using an enzyme-linked immunosorbent assay or a microagglutination test.
- Some commercial serologic tests may detect F. tularensis–specific antibodies as early as 1–2 weeks after disease onset.
- Importantly, the persistence of F. tularensis antibodies is prolonged, meaning that up to at least 1 year after acute infection, single titers of antibodies remain above the cutoff set by laboratories to detect acute infections.
- Therefore, a reliable serologic diagnosis of tularemia in the acute phase should rely on the demonstration of a significant increase of antibody titers between two samples taken 2–4 weeks apart.
- Chest imaging is useful in respiratory tularemia.
- Single or multifocal consolidation may be present, accompanied by pleural effusion with hilar and mediastinal lymphadenopathy.
- Computed tomography (CT) scans in the acute phase may reveal multiple rounded consolidations, often in the subpleural region and sometimes with signs of inclusion necrosis with a diffuse marginal zone.
- Lymph node enlargements in the mediastinal and hilar regions on a CT scan may also contain necrotic inclusions.
- A relatively common scenario for sporadic cases of tularemia is pulmonary nodules or dense consolidations, which can mimic lung cancer, resulting in more extensive clinical investigation paths to exclude cancer, including CT and positron emission tomography (PET) scans.
- Endobronchial ultrasound bronchoscopy procedures with biopsy may be performed in some cases before tularemia is suspected.
- The resolution of tularemia pathology on chest imaging may be slow and take months.
- Specific antimicrobial treatment is highly recommended for tularemia as outlined in Table 175-2.
- The antibiotics of choice are ciprofloxacin, levofloxacin, gentamicin, or doxycycline.
- Early specific antimicrobial treatment is essential to avoid complications irrespective of targeting type A or type B tularemia.
- Several commonly used antimicrobials, including all the β-lactam drugs and clindamycin, lack treatment efficacy against F. tularensis.
- Macrolide antibiotics, including erythromycin and azithromycin, show an in vitro effect against F. tularensis type A and type B varieties known to be present in the United States, but globally there are very scarce treatment outcome data for these drugs in humans.
- Generally, macrolide antibiotics are not recommended for tularemia because macrolide-resistant type B strains are common in Europe and Asia, resulting in total lack of treatment effect and overall little experience using these drugs for tularemia treatment.
- Azithromycin, however, may be an alternative treatment choice for patients with verified type A infection according to recent CDC guidelines.
- Streptomycin, classically used to treat tularemia, has been the drug of choice due to its high cure rate in a U.S. case series reported from 1949–1988, but is now considered a less attractive alternative to gentamicin due to its drawbacks, including the need for intramuscular administration, limited clinical availability, and a higher risk of vestibular and renal toxicity compared with newer aminoglycoside antibiotics.
- Chloramphenicol is another drug with a higher risk of adverse effects that, for this reason, is seldom used systemically in modern medicine.
- Chloramphenicol has an in vitro effect against F. tularensis and was reportedly effective in treating tularemia meningitis in the past.
- Inflamed lymph nodes can progress into an abscess with local and/or systemic reaction and may occur in about one-third of patients, especially if there were delays in F. tularensis–specific antibiotic treatment.
- An antibiotic treatment delay of >2–3 weeks after disease onset has been statistically associated with lymph node abscess formation.
- In some cases, the progression to a lymph node abscess may occur despite ongoing appropriate antibiotic treatment initiated late in the disease course.
- It is unclear if extending the antibiotic treatment duration is of clinical benefit.
- Culture specimens from an abscess at this disease stage are typically F. tularensis negative, but an additional 10–day course of appropriate antibiotic treatment is often used to avoid further disease progression and may be successful.
- If the clinician considers that there is a clear and immediate risk of spontaneous rupture of the skin or the mucus membranes in the pharynx with suppuration of pus, open surgical drainage or needle aspiration is recommended for treatment.
- A more invasive procedure with total surgical excision may be needed in more complicated and long-standing cases.
- Another complication occasionally reported by patients includes postinfectious persisting fatigue and disability.
- Additional complications or disease manifestations of tularemia have been reported, including adult respiratory distress syndrome, myocarditis, pericarditis, endocarditis, meningitis, osteomyelitis, hepatitis, and renal failure.
- Postexposure prophylaxis is recommended for high-risk exposures, including performing aerosol-generating procedures with F. tularensis cultures outside a biologic safety cabinet or handling infected animals.
- There are extensive human data showing that doxycycline is effective.
- For low-risk exposures, preparedness for early treatment may suffice using daily “fever watch”: the patient monitors temperature with instructions to seek immediate treatment if developing a fever.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 175–3 Patient presenting with ulceroglandular tularemia 3 weeks after onset of high fever and influenza-like illness. Lymph nodes of the left thigh were red, FIGURE 175–2 Characteristic sites of lymphoid tissue engagement in tularemia. tender, and swollen. A tularemia ulcer was present on the left ankle (not shown). (From https://training.seer.cancer.gov/lymphoma/anatomy/lymph-nodes.html.) (Photo from patient care at Region Västerbotten, Sweden.) The primary tularemia ulcer is often a small break in the skin, with limited signs of inflammation, and may require careful clinical examina- days after onset of the influenza-like illness. Bronchoscopy findings may tion to be detected. In some cases, it may not be detectable and the dis- include signs of local tracheitis and pneumonitis, and the lymphoid tissue ease form will then be classified as glandular. Red, tender, swollen lymph engaged will be in the mediastinum or lung hila. “Typhoidal tularemia” is regional nodes are often the most remarkable clinical examination find- an older medical classification term referring to a disease syndrome like — Schematic illustration of the type A and type B disease ecology concepts, showing environmental reservoirs, donors, reservoirs, and vectors for tularemia in North America, Europe, and Asia.
Figure 2¶

Caption: Tularemia CHAPTER 175 FIGURE 175–4 Frontal projection chest x-ray with acute respiratory/pneumonic tularemia (type B) with consolidation at the right side of the lungs with hilar enlargement. Fever and chills started 10 days before. (Photo from patient care at Region Västerbotten, Sweden.) ■ PATHOLOGY Analyses of tularemia skin lesions of humans infected by skinning of rabbits with tularemia have suggested a scenario with accumulation of lymphocytes, plasma cells, and neutrophils at the infection site during the first week after F. tularensis infection of the skin. Microabscesses with — Characteristic sites of lymphoid tissue engagement in tularemia, illustrating the anatomical locations of lymph nodes involved based on the initial infection route.
Figure 3¶

Caption: A FIGURE 175–5 Dense consolidation in the left lung of patient with a history of weight in loss and cough for 3–4 months. A. CT scan showed dense consolidation (2.5 × 2.5 × 2.0 cm) in the basal left upper lobe extending to the apical part of the lower lobe and of increased hilar lymphoid tissue. B. Eight days later, PET scan showed increased metabolic activity and progress of the consolidation to 5.0 × 4.5 × 3.5 cm. Tissue biopsy revealed granuloma formation in the adjacent pleura and no malignant cells. C. A tularemia diagnosis was confirmed by serology, the patient was treated with ciprofloxacin, and a CT scan performed 2 months later showed resolution of the consolidation. (Photos from patient care at Region Västerbotten, Sweden.) alternative to gentamicin due to its drawbacks, including the need — Patient presenting with ulceroglandular tularemia 3 weeks after onset of high fever and influenza-like illness, showing red, tender, and swollen lymph nodes of the left thigh and a tularemia ulcer on the left ankle.
Figure 4¶

Caption: A FIGURE 175–5 Dense consolidation in the left lung of patient with a history of weight in loss and cough for 3–4 months. A. CT scan showed dense consolidation (2.5 × 2.5 × 2.0 cm) in the basal left upper lobe extending to the apical part of the lower lobe and of increased hilar lymphoid tissue. B. Eight days later, PET scan showed increased metabolic activity and progress of the consolidation to 5.0 × 4.5 × 3.5 cm. Tissue biopsy revealed granuloma formation in the adjacent pleura and no malignant cells. C. A tularemia diagnosis was confirmed by serology, the patient was treated with ciprofloxacin, and a CT scan performed 2 months later showed resolution of the consolidation. (Photos from patient care at Region Västerbotten, Sweden.) alternative to gentamicin due to its drawbacks, including the need — Frontal projection chest x-ray with acute respiratory/pneumonic tularemia (type B) with consolidation at the right side of the lungs with hilar enlargement.
Figure 5¶
Caption: A FIGURE 175–5 Dense consolidation in the left lung of patient with a history of weight in loss and cough for 3–4 months. A. CT scan showed dense consolidation (2.5 × 2.5 × 2.0 cm) in the basal left upper lobe extending to the apical part of the lower lobe and of increased hilar lymphoid tissue. B. Eight days later, PET scan showed increased metabolic activity and progress of the consolidation to 5.0 × 4.5 × 3.5 cm. Tissue biopsy revealed granuloma formation in the adjacent pleura and no malignant cells. C. A tularemia diagnosis was confirmed by serology, the patient was treated with ciprofloxacin, and a CT scan performed 2 months later showed resolution of the consolidation. (Photos from patient care at Region Västerbotten, Sweden.) alternative to gentamicin due to its drawbacks, including the need — Dense consolidation in the left lung of patient with a history of weight loss and cough for 3–4 months, showing CT scan consolidation, PET scan metabolic activity, and tissue biopsy revealing granuloma formation.
Figure 6¶
Caption: FIGURE 175–3 Patient presenting with ulceroglandular tularemia 3 weeks after onset of high fever and influenza-like illness. Lymph nodes of the left thigh were red, FIGURE 175–2 Characteristic sites of lymphoid tissue engagement in tularemia. tender, and swollen. A tularemia ulcer was present on the left ankle (not shown). (From https://training.seer.cancer.gov/lymphoma/anatomy/lymph-nodes.html.) (Photo from patient care at Region Västerbotten, Sweden.) The primary tularemia ulcer is often a small break in the skin, with limited signs of inflammation, and may require careful clinical examina- days after onset of the influenza-like illness. Bronchoscopy findings may tion to be detected. In some cases, it may not be detectable and the dis- include signs of local tracheitis and pneumonitis, and the lymphoid tissue ease form will then be classified as glandular. Red, tender, swollen lymph engaged will be in the mediastinum or lung hila. “Typhoidal tularemia” is regional nodes are often the most remarkable clinical examination find- an older medical classification term referring to a disease syndrome like — Histopathology of tularemia skin lesions showing accumulation of lymphocytes, plasma cells, and neutrophils at the infection site during the first week after F. tularensis infection of the skin.
Figure 7¶

Caption: FIGURE 175–3 Patient presenting with ulceroglandular tularemia 3 weeks after onset of high fever and influenza-like illness. Lymph nodes of the left thigh were red, FIGURE 175–2 Characteristic sites of lymphoid tissue engagement in tularemia. tender, and swollen. A tularemia ulcer was present on the left ankle (not shown). (From https://training.seer.cancer.gov/lymphoma/anatomy/lymph-nodes.html.) (Photo from patient care at Region Västerbotten, Sweden.) The primary tularemia ulcer is often a small break in the skin, with limited signs of inflammation, and may require careful clinical examina- days after onset of the influenza-like illness. Bronchoscopy findings may tion to be detected. In some cases, it may not be detectable and the dis- include signs of local tracheitis and pneumonitis, and the lymphoid tissue ease form will then be classified as glandular. Red, tender, swollen lymph engaged will be in the mediastinum or lung hila. “Typhoidal tularemia” is regional nodes are often the most remarkable clinical examination find- an older medical classification term referring to a disease syndrome like — Histopathology of tularemia lung lesions showing necrotizing pneumonia characterized by abundant fibrin, cellular debris, and neutrophils within alveolar walls and alveolar spaces.
Figure 8¶

Caption: FIGURE 175–3 Patient presenting with ulceroglandular tularemia 3 weeks after onset of high fever and influenza-like illness. Lymph nodes of the left thigh were red, FIGURE 175–2 Characteristic sites of lymphoid tissue engagement in tularemia. tender, and swollen. A tularemia ulcer was present on the left ankle (not shown). (From https://training.seer.cancer.gov/lymphoma/anatomy/lymph-nodes.html.) (Photo from patient care at Region Västerbotten, Sweden.) The primary tularemia ulcer is often a small break in the skin, with limited signs of inflammation, and may require careful clinical examina- days after onset of the influenza-like illness. Bronchoscopy findings may tion to be detected. In some cases, it may not be detectable and the dis- include signs of local tracheitis and pneumonitis, and the lymphoid tissue ease form will then be classified as glandular. Red, tender, swollen lymph engaged will be in the mediastinum or lung hila. “Typhoidal tularemia” is regional nodes are often the most remarkable clinical examination find- an older medical classification term referring to a disease syndrome like — Close-up view of lymph node enlargement in the mediastinal and hilar regions on a CT scan, which may contain necrotic inclusions in respiratory/pneumonic tularemia.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.