Chapter 463: Psychiatric Disorders¶
Part 13: Neurologic Disorders · Part 13 – Neurologic Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Psychiatric disorders are the major cause of life-years lost to disability among all medical illnesses, affecting >300 million individuals worldwide.
- Anxiety disorders are the most prevalent psychiatric illnesses in the general community, present in 15–20% of medical clinic patients.
- Panic disorder is defined by recurrent and unpredictable panic attacks; lifetime prevalence is 2–3%.
- Generalized Anxiety Disorder (GAD) requires excessive worry for at least 6 months; lifetime prevalence is 5–6%.
- SSRIs (e.g., fluoxetine, sertraline) are the cornerstone of drug therapy for anxiety disorders and do not have the adverse effects of TCAs.
- Benzodiazepines should generally not be prescribed for >4–6 weeks due to tolerance and risk of abuse/dependence.
- A diagnosis of panic disorder is made only after a medical etiology for panic attacks has been ruled out.
- PTSD requires exposure to actual or threatened death, serious injury, or sexual violence.
- GAD and panic disorder segregate independently; >80% of patients with GAD also suffer from major depression, dysthymia, or social phobia.
- Beta blockers (e.g., propranolol) are effective for performance anxiety but not general social phobia.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Global Considerations
- 1.2 Nosology & Classification
- 2. EPIDEMIOLOGY
- 2.1 Prevalence by Disorder
- 2.2 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Neurobiology of Anxiety
- 3.2 GABAergic Mechanisms
- 4. CLINICAL FEATURES
- 4.1 Panic Disorder Symptoms
- 4.2 GAD Symptoms
- 4.3 Phobic Disorders Symptoms
- 4.4 PTSD Symptoms
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Medical Rule-Outs
- 5.2 Comorbidities
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Panic Disorder Workup
- 6.2 Diagnostic Criteria: GAD
- 6.3 Diagnostic Criteria: PTSD
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Therapy: Antidepressants
- 7.2 Pharmacologic Therapy: Anxiolytics
- 7.3 Psychotherapy
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Relapse & Remission
- 8.2 Comorbidity Impact
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy & Breast-feeding
- 9.2 Elderly & Hepatic Impairment
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Pitfalls
- 10.2 Treatment Pearls
- WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- 11.1 Panic Disorder Clues
- 11.2 GAD Clues
- 11.3 Phobia Clues
- 11.4 PTSD Clues
- WHAT EXCLUDES THE DIAGNOSIS
- 12.1 Medical Exclusions
- 12.2 Psychiatric Exclusions
- Flowcharts & Algorithms
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | A guideline for the medical management of major depressive disorder |
1. DEFINITION & OVERVIEW¶
- Psychiatric disorders are common in medical practice and may present either as a primary disorder or as a comorbid condition.
- The DSM-5-TR and the tenth revision of the International Classification of Diseases (ICD-10-CM) are used for diagnosis, emphasizing clinical pragmatism.
- An alternative approach, HiTOP (Hierarchical Taxonomy of Psychopathology), has been proposed but lacks adequate validation.
- The Primary Care Evaluation of Mental Disorders (PRIME-MD) and the Patient Health Questionnaire are inventories that require only 10 min to complete.
- Validated patient-based questionnaires systematically probe for signs and symptoms associated with the most prevalent psychiatric diagnoses.
- Primary care physicians should assume responsibility for the initial diagnosis and treatment of the most common mental disorders.
- Harrison's defines this as: 'Psychiatric disorders are common in medical practice and may present either as a primary disorder or as a comorbid condition.'
- Consultation with a psychiatrist is appropriate when physicians encounter evidence of psychotic symptoms, mania, severe depression, or anxiety; symptoms of PTSD; suicidal or homicidal preoccupation; or a failure to respond to first-order treatment.
1.1 Global Considerations¶
- Global burden of disease statistics indicates that 4 of the 10 most important causes of morbidity and attendant health care costs worldwide are psychiatric in origin.
- Recent surveys indicate a dramatic increase in prevalence of mental or substance use disorders in the United States is ~30%, but only one-third of affected individuals are currently receiving treatment.
- Changes in health care delivery underscore the need for primary care physicians to assume responsibility for the initial diagnosis and treatment of the most common mental disorders.
- The need for improved prevention strategies and for more definitive and effective interventional treatments remains a global concern.
1.2 Nosology & Classification¶
- The DSM-5-TR and the tenth revision of the International Classification of Diseases (ICD-10-CM) have taken somewhat differing approaches to the diagnosis of mental illness.
- Both systems are in essence purely descriptive and emphasize clinical pragmatism.
- The Research Domain Criteria (RDOC) proposed by the National Institute of Mental Health aspires to provide a causal framework for classification of behavioral disturbance.
- Large-scale genetic investigations have revealed that differing psychiatric disorders overlap in their genetic risk variants and phenotypic symptoms.
2. EPIDEMIOLOGY¶
- Psychiatric disorders are the major cause of life-years lost to disability among all medical illnesses, affecting >300 million individuals worldwide.
- There is general agreement that high-income countries will need to build capacity in professional training in low- and middle-income countries in order to provide an adequate balanced care model for the delivery of evidence-based therapies for mental disorders.
- Anxiety disorders are present in 15–20% of medical clinic patients.
- The lifetime prevalence of panic disorder is 2–3%.
- The lifetime prevalence of GAD is 5–6%; the risk is higher in first-degree relatives of patients with the diagnosis.
- Phobic disorders are common, affecting ~7–9% of the population.
- Twice as many females are affected than males for phobic disorders.
- Between 5 and 10% of Americans will at some time in their life satisfy criteria for PTSD, with women more likely to be affected than men.
- Twin studies show a substantial genetic influence on all symptoms associated with PTSD, with less evidence for an environmental effect.
2.1 Prevalence by Disorder¶
- Panic Disorder: Lifetime prevalence 2–3%.
- Generalized Anxiety Disorder (GAD): Lifetime prevalence 5–6%.
- Phobic Disorders: Affecting ~7–9% of the population.
- PTSD: 5–10% of Americans at some time in their life.
2.2 Risk Factors¶
- Risk factors for the development of PTSD include a past psychiatric history and personality characteristics of high neuroticism and extroversion.
- Panic disorder shows familial aggregation; the disorder is concordant in 30–45% of monozygotic twins.
- Genome-wide screens have identified suggestive risk loci for panic disorder.
- Family studies indicate that GAD and panic disorder segregate independently.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- The etiology of panic disorder is unknown but appears to involve a genetic predisposition, altered autonomic responsivity, and social learning.
- Acute panic attacks appear to be associated with increased noradrenergic discharges in the locus coeruleus.
- Intravenous infusion of sodium lactate evokes an attack in two-thirds of panic disorder patients, as do the α-adrenergic antagonist yohimbine, cholecystokinin tetrapeptide 2 (CCK-4), and carbon dioxide inhalation.
- It is hypothesized that each of these stimuli activates a pathway involving noradrenergic neurons in the locus coeruleus and serotonergic neurons in the dorsal raphe.
- Resting-state functional magnetic resonance imaging (fMRI) has identified abnormalities in the default mode network involving the medial temporal lobe, with greater activation in the sensorimotor cortex in panic disorder and in amygdala-frontal connectivity in social anxiety disorder.
- Most anxiogenic and anxiolytic agents act on the γ-aminobutyric acid (GABA) receptor/chloride ion channel complex, implicating this neurotransmitter system in pathogenesis.
- Benzodiazepines are thought to bind two separate GABA A receptor sites: type I, which has a broad neuroanatomic distribution, and type II, which is concentrated in the hippocampus, striatum, and neocortex.
- The antianxiety effects of the various benzodiazepines are influenced by their relative binding to alpha 2 and 3 subunits of the GABA receptor, and sedation and memory impairment to the alpha 1 subunit.
- Serotonin (5-hydroxytryptamine [5-HT]) and 3α-reduced neuroactive steroids (allosteric modulators of GABA) also appear to have a role in anxiety.
- Animal studies of fear conditioning have indicated that processing of the fear stimulus occurs through the lateral nucleus of the amygdala, extending through the central nucleus and projecting to the periaqueductal gray region, lateral hypothalamus, and paraventricular hypothalamus.
3.1 Neurobiology of Anxiety¶
- Pathway involves noradrenergic neurons in the locus coeruleus and serotonergic neurons in the dorsal raphe.
- Abnormalities in the default mode network involving the medial temporal lobe.
- Greater activation in the sensorimotor cortex in panic disorder.
- Amygdala-frontal connectivity in social anxiety disorder.
3.2 GABAergic Mechanisms¶
- Benzodiazepines bind two separate GABA A receptor sites.
- Type I: Broad neuroanatomic distribution.
- Type II: Concentrated in hippocampus, striatum, and neocortex.
- Antianxiety effects influenced by binding to alpha 2 and 3 subunits.
- Sedation and memory impairment to the alpha 1 subunit.
4. CLINICAL FEATURES¶
- Anxiety, defined as a subjective sense of unease, dread, or foreboding, can indicate a primary psychiatric condition or can be a component of, or reaction to, a primary medical disease.
- Approximately one-third of patients presenting with anxiety have a medical etiology for their psychiatric symptoms, but an anxiety disorder can also present with somatic symptoms in the absence of a diagnosable medical condition.
- Panic Disorder: Panic disorder is defined by the presence of recurrent and unpredictable panic attacks, which are distinct episodes of intense fear and discomfort associated with a variety of physical symptoms, including palpitations, sweating, trembling, shortness of breath, chest pain, dizziness, and a fear of impending doom or death.
- Paresthesias, gastrointestinal distress, and feelings of unreality are also common.
- Panic attacks have a sudden onset, developing within 10 min and usually resolving over the course of an hour, and can occur in an unexpected fashion, such as when waking from sleep.
- The frequency and severity of panic attacks vary, ranging from once a week to clusters of attacks separated by months of well-being.
- The first attack is usually outside the home, and onset is typically in late adolescence to early adulthood.
- In some individuals, anticipatory anxiety develops over time and results in a generalized fear and a progressive avoidance of places or situations in which a panic attack might recur.
- Agoraphobia, which occurs commonly in patients with panic disorder, is an acquired irrational fear of being in places where one might feel trapped or unable to escape.
- Agoraphobia typically leads the patient into a progressive restriction in lifestyle and, in a literal sense, in geography.
- Generalized Anxiety Disorder (GAD): Patients with GAD have persistent, excessive, and/or unrealistic worry associated with muscle tension, impaired concentration, autonomic arousal, feeling “on edge” or restless, and insomnia.
- Onset is usually before age 20 years, and a history of childhood fears and social inhibition may be present.
- Patients with GAD worry excessively over minor matters, with life-disrupting effects; unlike panic disorder, complaints of shortness of breath, palpitations, and tachycardia are relatively rare.
- Phobic Disorders: The cardinal feature of phobic disorders is a marked and persistent fear of objects or situations, exposure to specific situations which results in an immediate anxiety reaction.
- The patient avoids the phobic stimulus, and this avoidance usually impairs occupational or social functioning.
- Social phobia is distinguished by a specific fear of social or performance situations in which the individual is exposed to unfamiliar individuals or to examination and evaluation by others.
- Stress Disorders: Patients may develop anxiety after exposure to extreme traumatic events such as the threat of personal death or injury or the death of a loved one.
- The reaction may occur shortly after the trauma (acute stress disorder) or be delayed and subject to recurrence (PTSD).
- In both syndromes, individuals experience associated symptoms of detachment and loss of emotional responsivity.
- The patient may feel depersonalized and unable to recall specific aspects of the trauma, although typically, it is reexperienced through intrusions in thought, dreams, or flashbacks, particularly when cues of the original event are present.
- Patients often actively avoid stimuli that precipitate recollections of the trauma and demonstrate a resulting increase in vigilance, arousal, and startle response.
4.1 Panic Disorder Symptoms¶
- Palpitations, sweating, trembling.
- Shortness of breath, chest pain, dizziness.
- Fear of impending doom or death.
- Paresthesias, gastrointestinal distress, feelings of unreality.
- Sudden onset, developing within 10 min.
- Usually resolving over the course of an hour.
- Can occur in an unexpected fashion, such as when waking from sleep.
4.2 GAD Symptoms¶
- Persistent, excessive, and/or unrealistic worry.
- Muscle tension.
- Impaired concentration.
- Autonomic arousal.
- Feeling “on edge” or restless.
- Insomnia.
- Onset usually before age 20 years.
- History of childhood fears and social inhibition may be present.
4.3 Phobic Disorders Symptoms¶
- Marked and persistent fear of objects or situations.
- Immediate anxiety reaction upon exposure.
- Avoidance of the phobic stimulus.
- Impairment of occupational or social functioning.
- Social phobia: Specific fear of social or performance situations.
- Exposure to unfamiliar individuals or examination/evaluation by others.
- Examples: Having to converse at a party, using public restrooms, or meeting strangers.
4.4 PTSD Symptoms¶
- Detachment and loss of emotional responsivity.
- Depersonalization.
- Intrusions in thought, dreams, or flashbacks.
- Increase in vigilance, arousal, and startle response.
- Active avoidance of stimuli that precipitate recollections of the trauma.
5. DIFFERENTIAL DIAGNOSIS¶
- A diagnosis of panic disorder is made as after a medical etiology for the panic attacks has been ruled out.
- A variety of cardiovascular, respiratory, endocrine, and neurologic conditions can present with anxiety as the chief complaint.
- Patients with true panic disorder will often focus on one specific feature to the exclusion of others.
- For example, 20% of patients who present with syncope as a primary medical complaint have a primary diagnosis of a mood, anxiety, or substance abuse disorder, the most common being panic disorder.
- When the history is nonspecific, physical examination and focused laboratory testing must be used to rule out anxiety states resulting from medical disorders such as pheochromocytoma, thyrotoxicosis, or hypoglycemia.
- Electrocardiogram (ECG) and echocardiogram may detect some cardiovascular conditions associated with panic, such as paroxysmal atrial tachycardia and mitral valve prolapse.
- In two studies, panic disorder was the primary diagnosis in 43% of patients with chest pain who had normal coronary angiograms and was present in 9% of all outpatients referred for cardiac evaluation.
- Panic disorder has also been diagnosed in many patients referred for pulmonary function testing or with symptoms of irritable bowel syndrome.
- Comorbid substance abuse is common in patients with GAD, particularly alcohol and/or sedative/hypnotic abuse.
- Patients with GAD worry excessively over minor matters, with life-disrupting effects; unlike panic disorder, complaints of shortness of breath, palpitations, and tachycardia are relatively rare.
5.1 Medical Rule-Outs¶
- Pheochromocytoma.
- Thyrotoxicosis.
- Hypoglycemia.
- Paroxysmal atrial tachycardia.
- Mitral valve prolapse.
- Cardiovascular conditions associated with panic.
5.2 Comorbidities¶
- Major depression (75% of panic disorder patients will also satisfy criteria for major depression at some point in their illness).
- Alcohol abuse.
- Benzodiazepine abuse.
- Sedative/hypnotic abuse.
- Social phobia.
- Eating disorders (in social phobia).
- Other psychiatric conditions (e.g., eating disorders in social phobia).
6. INVESTIGATIONS & DIAGNOSIS¶
- When the history is nonspecific, physical examination and focused laboratory testing must be used to rule out anxiety states resulting from medical disorders.
- Electrocardiogram (ECG) and echocardiogram may detect some cardiovascular conditions associated with panic.
- Diagnostic criteria for GAD and PTSD are based on DSM-5-TR.
- A possible validated four-item screen for PTSD (PC-PTSD) is available.
6.1 Panic Disorder Workup¶
- Physical examination and focused laboratory testing.
- Electrocardiogram (ECG).
- Echocardiogram.
- Rule out medical disorders such as pheochromocytoma, thyrotoxicosis, or hypoglycemia.
6.2 Diagnostic Criteria: GAD¶
- A. Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance).
- B. The individual finds it difficult to control the worry.
- C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months):
-
- Restlessness or feeling keyed up or on edge.
-
- Being easily fatigued.
-
- Difficulty concentrating or mind going blank.
-
- Irritability.
-
- Muscle tension.
-
- Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep).
- Note: Only one item is required in children.
- D. The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- E. The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism).
- F. The disturbance is not better explained by another mental disorder (e.g., anxiety or worry about having panic attacks in panic disorder, negative evaluation in social anxiety disorder, contamination or other obsessions in obsessive-compulsive disorder, separation from attachment figures in separation anxiety disorder, reminders of traumatic events in posttraumatic stress disorder, gaining weight in anorexia nervosa, physical complaints in somatic symptom disorder, perceived appearance flaws in body dysmorphic disorder, having a serious illness in illness anxiety disorder, or the content of delusional beliefs in schizophrenia or delusional disorder).
6.3 Diagnostic Criteria: PTSD¶
- A. Exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways:
-
- Directly experiencing the traumatic event(s).
-
- Witnessing, in person, the event(s) as it occurred to others.
-
- Learning that the traumatic event(s) occurred to a close family member or close friend. In cases of actual or threatened death of a family member or friend, the event(s) must have been violent or accidental.
-
- Experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (e.g., first responders collecting human remains; police officers repeatedly exposed to details of child abuse).
- Note: Criterion A4 does not apply to exposure through electronic media, television, movies, or pictures, unless this exposure is work related.
- B. Presence of one (or more) of the following intrusion symptoms associated with the traumatic event(s), beginning after the traumatic event(s) occurred:
-
- Recurrent, involuntary, and intrusive distressing memories of the traumatic event(s).
- Note: In children older than 6 years, repetitive play may occur in which themes or aspects of the traumatic event(s) are expressed.
-
- Recurrent distressing dreams in which the content and/or affect of the dream are related to the traumatic event(s).
- Note: In children, there may be frightening dreams without recognizable content.
-
- Dissociative reactions (e.g., flashbacks) in which the individual feels or acts as if the traumatic event(s) were recurring. (Such reactions may occur on a continuum, with the most extreme expression being a complete loss of awareness of present surroundings.)
- Note: In children, trauma-specific reenactment may occur in play.
-
- Intense or prolonged psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event(s).
-
- Marked physiological reactions to internal or external cues that symbolize or resemble an aspect of the traumatic event(s).
- C. Persistent avoidance of stimuli associated with the traumatic event(s), beginning after the traumatic event(s) occurred, as evidenced by one or both of the following:
-
- Avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
-
- Avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
- D. Negative alterations in cognitions and mood associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following:
-
- Inability to remember an important aspect of the traumatic event(s) (typically due to dissociative amnesia and not to other factors such as head injury, alcohol, or drugs).
-
- Persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (e.g., “I am bad,” “No one can be trusted,” “The world is completely dangerous,” “My whole nervous system is permanently ruined”).
-
- Persistent, distorted cognitions about the cause or consequences of the traumatic event(s) that lead the individual to
7. MANAGEMENT & TREATMENT¶
- Achievable goals of treatment are to decrease the frequency of panic attacks and to reduce their intensity.
- The cornerstone of drug therapy is antidepressant medication.
- Selective serotonin reuptake inhibitors (SSRIs) benefit the majority of panic disorder patients and do not have the adverse effects of tricyclic antidepressants (TCAs).
- Fluoxetine, paroxetine, sertraline, and the selective serotonin-norepinephrine reuptake inhibitor (SNRI) venlafaxine have received approval from the U.S. Food and Drug Administration (FDA) for this indication.
- These drugs should be started at one-third to one-half of their usual antidepressant dose (e.g., 5–10 mg fluoxetine, 25–50 mg sertraline, 10 mg paroxetine, venlafaxine 37.5 mg).
- Monoamine oxidase inhibitors (MAOIs) are also effective and may specifically benefit patients who have comorbid features of atypical depression (i.e., hypersomnia and weight gain).
- Insomnia, orthostatic hypotension, and the need to maintain a low-tyramine diet (avoidance of cheese and wine) have limited their use, however.
- Antidepressants typically take 2–6 weeks to become effective, and doses may need to be adjusted based on the clinical response.
- Because of anticipatory anxiety and the need for immediate relief of panic symptoms, benzodiazepines are useful early in the course of treatment and sporadically thereafter.
- FDA-approved agents include alprazolam and clonazepam.
- A short course of a benzodiazepine is usually indicated, preferably lorazepam, oxazepam, clonazepam, or alprazolam, although only the last two are FDA approved.
- Treatment should be initiated at the lowest dose possible and prescribed on an as-needed basis as symptoms warrant.
- Benzodiazepines differ in their milligram per kilogram potency, half-life, lipid solubility, metabolic pathways, and presence of active metabolites.
- Agents that are absorbed rapidly and are lipid soluble, such as diazepam, have a rapid onset of action and a higher abuse potential.
- Benzodiazepines should generally not be prescribed for >4–6 weeks because of the development of tolerance and the serious risk of abuse and dependence.
- Withdrawal must be closely monitored as relapses can occur.
- It is important to warn patients that concomitant use of alcohol or other sedating drugs may exacerbate side effects and impair their ability to function.
- Early psychotherapeutic intervention and education aimed at symptom control enhance the effectiveness of drug treatment.
- Patients can be taught breathing techniques, be educated about physiologic changes that occur with panic, and learn to expose themselves voluntarily to precipitating events in a treatment program spanning 12–15 sessions.
- Homework assignments and monitored compliance are important components of successful treatment.
- Once patients have achieved a satisfactory response, drug treatment should be maintained for 1–2 years to prevent relapse.
- Controlled trials indicate a success rate of 75–85%, although the likelihood of complete remission is somewhat lower.
- In treatment-resistant cases, short-term augmentation with aripiprazole, divalproex sodium, or pindolol has some evidence for efficacy.
- There is no clear difference in short-term efficacy between psychotherapeutic therapies and antidepressant or benzodiazepine treatment, alone or in combination.
- Beta blockers (e.g., propranolol, 20–40 mg orally 2 h before the event) are particularly effective in the treatment of “performance anxiety” (but not general social phobia) and appear to work by blocking the peripheral manifestations of anxiety such as perspiration, tachycardia, palpitations, and tremor.
- MAOIs alleviate social phobia independently of their antidepressant activity.
- Paroxetine, sertraline, fluvoxamine CR, and venlafaxine XR have received FDA approval for treatment of social anxiety.
- Benzodiazepines can be helpful in reducing fearful avoidance, but the chronic nature of phobic disorders limits their usefulness.
- Behaviorally focused psychotherapy is an important component of treatment because relapse rates are high when medication is used as the sole treatment.
- Cognitive-behavioral strategies are based on the finding that distorted perceptions and interpretations of fear-producing stimuli play a major role in perpetuation of phobias.
- Individual and group therapy sessions teach the patient to identify specific negative thoughts associated with the anxiety-producing situation and help to reduce the patient’s fear of loss of control.
- In desensitization therapy, hierarchies of feared situations are constructed, and the patient is encouraged to pursue and master gradual exposure to the anxiety-producing stimuli.
- Patients with social phobia, in particular, have a high rate of comorbid alcohol abuse, as well as of other psychiatric conditions (e.g., eating disorders), necessitating the need for parallel management of each disorder if anxiety reduction is to be achieved.
- Benzodiazepines are contraindicated during pregnancy and breast-feeding.
- Patients who were previously responsive to a benzodiazepine are unlikely to rate buspirone as equally effective, but patients with head injury or dementia who are have symptoms of anxiety and/or agitation may do well with this agent.
Table 1 — Table 463-1 Antidepressants¶
| NAME | USUAL DAILY DOSE (mg) | SIDE EFFECTS | COMMENTS |
|---|---|---|---|
| SSRIs | |||
| Fluoxetine (Prozac) | 10–80 | Headache; nausea and other GI effects; jitteriness; insomnia; sexual dysfunction; can affect plasma levels of other medicines (except sertraline); akathisia rare | Once-daily dosing, usually in the morning; fluoxetine has very long half-life; must not be combined with MAOIs |
| Sertraline (Zoloft) | 50–200 | ||
| Paroxetine (Paxil) | 20–60 | ||
| Fluvoxamine (Luvox) | 100–300 | ||
| Citalopram (Celexa) | 20–60 | ||
| Escitalopram (Lexapro) | 10–30 | ||
| TCAs and Tetracyclics | |||
| Amitriptyline (Elavil) | 150–300 | Anticholinergic (dry mouth, tachycardia, sweating; tremor; postural hypotension; cardiac conduction delay; sedation; weight gain especially by elderly | Once-daily dosing, usually qhs; blood levels of most TCAs available; can be lethal in overdose (lethal dose = 2 g); nortriptyline best tolerated |
| Nortriptyline (Pamelor) | 50–200 | ||
| Imipramine (Tofranil) | 150–300 | ||
| Desipramine (Norpramin) | 150–300 | ||
| Doxepin (Sinequan) | 150–300 | Nausea, anxiety, dry mouth | FDA-approved for OCD |
| Clomipramine (Anafranil) | 150–300 | ||
| Maprotiline (Ludiomil) | 25–150 | ||
| Protriptyline (Vivactil) | 15–40 | ||
| Trimipramine (Surmontil) | 75–200 | Drowsiness, constipation, dry mouth | tid or qid dosing required |
| Amoxapine (Asendin) | 100–300 | Lethality in OD, EPS possible | |
| Mixed Serotonin-Norepinephrine Reuptake Inhibitors (SNRI) and Receptor Blockers | |||
| Venlafaxine (Effexor), XR | 75–375 | Nausea; dizziness; dry mouth; headaches; increased blood pressure; anxiety and insomnia | bid–tid dosing (extended-release available); lower potential for drug interactions than SSRIs; contraindicated with MAOIs |
| Desvenlafaxine (Pristiq) | 50–400 | Nausea, dizziness, insomnia | Primary metabolite of venlafaxine; no increased efficacy with higher dosing |
| Duloxetine (Cymbalta) | 40–60 | Nausea, dizziness, headache, insomnia, constipation and stress incontinence | May have utility in treatment of neuropathic pain and stress incontinence |
| Mirtazapine (Remeron) | 15–45 | Somnolence, weight gain; neutropenia rare | Once-a-day dosing; 5-HT antagonist |
| Vilazodone (Viibryd) | 40 | Nausea, diarrhea, headache; dosage adjustment if given with CYP3A4 inhibitor/stimulator | Also 5-HT receptor partial agonist |
| Vortioxetine (Trintellix) | 5–20 | Nausea, diarrhea, sweating, headache; low incidence of sedation or weight gain | No specific p450 effects; 5-HT and 5-HT receptor antagonist, 5-HT partial agonist, and 5-HT agonist |
| Levomilnacipran (Fetzima) | 40–120 | Nausea, constipation, sweating; rare increase in blood pressure/pulse | Most noradrenergic of SNRIs |
| Mixed-Action Drugs | |||
| Bupropion (Wellbutrin), CR, XR | 250–450 | Jitteriness; flushing; seizures in at-risk patients; anorexia; tachycardia; psychosis | fewer sexual side effects than SSRIs or TCAs; may be useful for adult ADD |
| Trazodone (Desyrel) | 200–600 | Sedation; dry mouth; ventricular irritability; postural hypotension; priapism rare | Useful in low doses for sleep because of sedating effects with no anticholinergic side effects |
| Trazodone extended-release (Oleptro) | 150–375 | Daytime somnolence, dizziness, nausea | |
| Nefazodone | 300–600 | Headache, nausea, dizziness | Rare risk of liver failure, priapism |
| Gepirone extended-release (Exxua) | 18.2–72.6 | Dizziness, nausea, insomnia | Partial agonist/5-HT ; 5-HT antagonist |
| Esketamine (Spravato) | 56–84 | 1–2 times a week | Sedation, dissociation, respiratory depression; Ketamine isomer for treatment-resistant depression and/or suicidal risk |
| Zuranolone (Zurzuvae) | 50 qhs for 14 days | Somnolence, confusion, dizziness | Oral neuroactive steroid for postpartum depression |
| Dextromethorphan-bupropion (Auvelity) | 45/105 bid | Dizziness, headache, diarrhea | Possible increased speed of response |
| MAOIs | |||
| Phenelzine (Nardil) | 45–90 | Insomnia; hypotension; edema; anorgasmia; weight gain; neuropathy; hypertensive crisis; toxic reactions with SSRIs; narcotics | May be more effective in patients with atypical features or treatment-refractory depression |
| Tranylcypromine (Parnate) | 20–50 | ||
| Isocarboxazid (Marplan) | 20–60 | Less weight gain and hypotension than phenelzine | |
| Transdermal selegiline (Emsam) | 6–12 | Local skin reaction, hypertension | No dietary restrictions with 6-mg dose |
Table 2 — Table 463-2 Management of Antidepressant Side Effects¶
| SYMPTOMS | COMMENTS AND MANAGEMENT STRATEGIES |
|---|---|
| Gastrointestinal | |
| Nausea, loss of appetite | Usually short-lived and dose-related; consider temporary dose reduction or administration with food and antacids |
| Diarrhea | Famotidine, 20–40 mg/d |
| Constipation | Wait for tolerance; try diet change, stool softener, exercise; avoid laxatives |
| Sexual dysfunction | Consider dose reduction; drug holiday |
| Anorgasmia/impaired ejaculation | Bethanechol, 10–20 mg, 2 h before activity, or cyproheptadine, 4–8 mg, 2 h before activity, or bupropion, 100 mg bid, or amantadine, 100 mg bid/tid |
| Orthostasis | Tolerance unlikely; increase fluid intake, use calf exercises/support hose; fludrocortisone, 0.025 mg/d |
| Anticholinergic | Wait for tolerance |
| Dry mouth, eyes | Maintain good oral hygiene; use artificial tears, sugar-free gum |
| Tremor/jitteriness | Antiparkinsonian drugs not effective; use dose reduction/slow increase; lorazepam, 0.5 mg bid, or propranolol, 10–20 mg bid |
| Insomnia | Schedule all doses for the morning; trazodone, 50–100 mg qhs |
| Sedation | Caffeine; schedule all dosing for bedtime; bupropion, 75–100 mg in afternoon |
| Headache | Evaluate diet, stress, other drugs; try dose reduction; amitriptyline, 50 mg/d |
| Weight gain | Decrease carbohydrates; exercise; consider fluoxetine |
| Loss of therapeutic benefit over time | Related to tolerance? Increase dose or drug holiday; add amantadine, 100 mg bid, buspirone, 10 mg tid, or pindolol, 2.5 mg bid |
Table 3 — Table 463-3 Possible Drug Interactions with Selective Serotonin Reuptake Inhibitors¶
| AGENT | EFFECT |
|---|---|
| Monoamine oxidase inhibitors | Serotonin syndrome—absolute contraindication |
| Serotonergic agonists, e.g., tryptophan, fenfluramine, triptans | Potential serotonin syndrome |
| Drugs that are metabolized by P450 isoenzymes: tricyclics, other SSRIs, antipsychotics, beta blockers, codeine, triazolobenzodiazepines, calcium channel blockers | Delayed metabolism resulting in increased blood levels and potential toxicity |
| Drugs that are bound tightly to plasma proteins, e.g., warfarin | Increased bleeding secondary to displacement |
| Drugs that inhibit the metabolism of SSRIs by P450 isoenzymes, e.g., quinidine | Increased SSRI side effects |
Table 4 — Table 463-4 Anxiolytics¶
| NAME | EQUIVALENT PO DOSE (mg) | ONSET OF ACTION | HALF-LIFE (h) | COMMENTS |
|---|---|---|---|---|
| Benzodiazepines | ||||
| Diazepam (Valium) | 5 | Fast | 20–70 | Active metabolites; quite sedating |
| Flurazepam (Dalmane) | 15 | Fast | 30–100 | Flurazepam is a prodrug; metabolites are active; quite sedating |
| Triazolam (Halcion) | 0.25 | Intermediate | 1.5–5 | No active metabolites; can induce confusion and delirium, especially in elderly |
| Lorazepam (Ativan) | 1 | Intermediate | 10–20 | No active metabolites; direct hepatic glucuronide conjugation; quite sedating; FDA-approved for anxiety with depression |
| Alprazolam (Xanax) | 0.5 | Intermediate | 12–15 | Active metabolites; not too sedating; FDA-approved for panic disorder and anxiety with depression; tolerance and dependence develop easily; difficult to withdraw |
| Chlordiazepoxide (Librium) | 10 | Intermediate | 5–30 | Active metabolites; moderately sedating |
| Oxazepam (Serax) | 15 | Slow | 5–15 | No active metabolites; direct glucuronide conjugation; not too sedating |
| Temazepam (Restoril) | 15 | Slow | 9–12 | No active metabolites; moderately sedating |
| Clonazepam (Klonopin) | 0.5 | Slow | 18–50 | No active metabolites; moderately sedating; FDA-approved for panic disorder |
| Clorazepate (Tranxene) | 15 | Fast | 40–200 | Low sedation; unreliable absorption |
| Prazepam (Centrax) | 10–60 | Fast | 29–224 | Less sedating than diazepam |
| Nonbenzodiazepines | ||||
| Buspirone (BuSpar) | 7.5 | 2 weeks | 2–3 | Active metabolites; tid dosing—usual daily dose 10–20 mg tid; nonsedating; no additive effects with alcohol; useful for controlling agitation in demented or brain-injured patients |
7.1 Pharmacologic Therapy: Antidepressants¶
- SSRIs: Fluoxetine, Sertraline, Paroxetine, Fluvoxamine, Citalopram, Escitalopram.
- TCAs and Tetracyclics: Amitriptyline, Nortriptyline, Imipramine, Desipramine, Doxepin, Clomipramine, Maprotiline, Protriptyline, Trimipramine, Amoxapine.
- SNRIs and Receptor Blockers: Venlafaxine, Desvenlafaxine, Duloxetine, Mirtazapine, Vilazodone, Vortioxetine, Levomilnacipran.
- Mixed-Action Drugs: Bupropion, Trazodone, Nefazodone, Gepirone, Esketamine, Zuranolone, Dextromethorphan-bupropion.
- MAOIs: Phenelzine, Tranylcypromine, Isocarboxazid, Transdermal selegiline.
7.2 Pharmacologic Therapy: Anxiolytics¶
- Benzodiazepines: Diazepam, Flurazepam, Triazolam, Lorazepam, Alprazolam, Chlordiazepoxide, Oxazepam, Temazepam, Clonazepam, Clorazepate, Prazepam.
- Nonbenzodiazepines: Buspirone.
7.3 Psychotherapy¶
- Early psychotherapeutic intervention and education aimed at symptom control enhance the effectiveness of drug treatment.
- Patients can be taught breathing techniques.
- Education about physiologic changes that occur with panic.
- Learn to expose themselves voluntarily to precipitating events in a treatment program spanning 12–15 sessions.
- Homework assignments and monitored compliance are important components of successful treatment.
- Behaviorally focused psychotherapy is an important component of treatment because relapse rates are high when medication is used as the sole treatment.
- Cognitive-behavioral strategies are based on the finding that distorted perceptions and interpretations of fear-producing stimuli play a major role in perpetuation of phobias.
- Individual and group therapy sessions teach the patient to identify specific negative thoughts associated with the anxiety-producing situation and help to reduce the patient’s fear of loss of control.
- In desensitization therapy, hierarchies of feared situations are constructed, and the patient is encouraged to pursue and master gradual exposure to the anxiety-producing stimuli.
8. PROGNOSIS & COMPLICATIONS¶
- Controlled trials indicate a success rate of 75–85%, although the likelihood of complete remission is somewhat lower.
- Once patients have achieved a satisfactory response, drug treatment should be maintained for 1–2 years to prevent relapse.
- Relapse rates are high when medication is used as the sole treatment.
- Comorbid substance abuse is common in these patients, particularly alcohol and/or sedative/hypnotic abuse.
- Patients with social phobia, in particular, have a high rate of comorbid alcohol abuse, as well as of other psychiatric conditions (e.g., eating disorders), necessitating the need for parallel management of each disorder if anxiety reduction is to be achieved.
8.1 Relapse & Remission¶
- Success rate of 75–85%.
- Likelihood of complete remission is somewhat lower.
- Drug treatment should be maintained for 1–2 years to prevent relapse.
8.2 Comorbidity Impact¶
- Comorbid substance abuse is common in patients with GAD.
- Patients with social phobia have a high rate of comorbid alcohol abuse.
- Other psychiatric conditions (e.g., eating disorders) necessitate parallel management.
9. SPECIAL CONSIDERATIONS¶
- Benzodiazepines are contraindicated during pregnancy and breast-feeding.
- Patients with head injury or dementia who are have symptoms of anxiety and/or agitation may do well with buspirone.
- Triazolam can induce confusion and delirium, especially in elderly.
- Benzodiazepines that are metabolized via conjugation rather than oxidation do not accumulate if hepatic function is impaired; the latter also has limited active metabolites.
- Benzodiazepines differ in their milligram per kilogram potency, half-life, lipid solubility, metabolic pathways, and presence of active metabolites.
9.1 Pregnancy & Breast-feeding¶
- Benzodiazepines are contraindicated during pregnancy and breast-feeding.
9.2 Elderly & Hepatic Impairment¶
- Triazolam can induce confusion and delirium, especially in elderly.
- Benzodiazepines that are metabolized via conjugation rather than oxidation do not accumulate if hepatic function is impaired.
- The latter also has limited active metabolites.
10. KEY PEARLS & CLINICAL TRAPS¶
- Primary care physicians should base referrals to a psychiatrist on the presence of signs and symptoms of a mental disorder and not simply to the absence of a physical explanation for a patient’s complaint.
- The physician should discuss with the patient the reasons for requesting the referral or consultation and provide reassurance that they will continue to provide medical care and work collaboratively with the mental health professional.
- Anxiety, defined as a subjective sense of unease, dread, or foreboding, can indicate a primary psychiatric condition or can be a component of, or reaction to, a primary medical disease.
- Approximately one-third of patients presenting with anxiety have a medical etiology for their psychiatric symptoms, but an anxiety disorder can also present with somatic symptoms in the absence of a diagnosable medical condition.
- Panic disorder is defined by the presence of recurrent and unpredictable panic attacks, which are distinct episodes of intense fear and discomfort associated with a variety of physical symptoms.
- A diagnosis of panic disorder is made as after a medical etiology for the panic attacks has been ruled out.
- Benzodiazepines should generally not be prescribed for >4–6 weeks because of the development of tolerance and the serious risk of abuse and dependence.
- SSRIs benefit the majority of panic disorder patients and do not have the adverse effects of tricyclic antidepressants (TCAs).
- Beta blockers (e.g., propranolol, 20–40 mg orally 2 h before the event) are particularly effective in the treatment of “performance anxiety” (but not general social phobia).
- Between 5 and 10% of Americans will at some time in their life satisfy criteria for PTSD, with women more likely to be affected than men.
10.1 Diagnostic Pitfalls¶
- Physicians will fail to recognize the syndrome if direct questioning is not pursued regarding agoraphobia.
- Patients with true panic disorder will often focus on one specific feature to the exclusion of others.
- For example, 20% of patients who present with syncope as a primary medical complaint have a primary diagnosis of a mood, anxiety, or substance abuse disorder, the most common being panic disorder.
10.2 Treatment Pearls¶
- Early psychotherapeutic intervention and education aimed at symptom control enhance the effectiveness of drug treatment.
- Homework assignments and monitored compliance are important components of successful treatment.
- Once patients have achieved a satisfactory response, drug treatment should be maintained for 1–2 years to prevent relapse.
WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Panic Disorder: Recurrent and unpredictable panic attacks, distinct episodes of intense fear and discomfort associated with palpitations, sweating, trembling, shortness of breath, chest pain, dizziness, and a fear of impending doom or death.
- GAD: Persistent, excessive, and/or unrealistic worry associated with muscle tension, impaired concentration, autonomic arousal, feeling “on edge” or restless, and insomnia.
- Phobic Disorders: Marked and persistent fear of objects or situations, exposure to specific situations which results in an immediate anxiety reaction.
- PTSD: Exposure to actual or threatened death, serious injury, or sexual violence.
- Agoraphobia: Acquired irrational fear of being in places where one might feel trapped or unable to escape.
- Social Phobia: Specific fear of social or performance situations in which the individual is exposed to unfamiliar individuals or to examination and evaluation by others.
11.1 Panic Disorder Clues¶
- Recurrent and unpredictable panic attacks.
- Sudden onset, developing within 10 min.
- Usually resolving over the course of an hour.
- Can occur in an unexpected fashion, such as when waking from sleep.
- Anticipatory anxiety develops over time and results in a generalized fear and a progressive avoidance of places or situations in which a panic attack might recur.
11.2 GAD Clues¶
- Persistent, excessive, and/or unrealistic worry.
- Muscle tension.
- Impaired concentration.
- Autonomic arousal.
- Feeling “on edge” or restless.
- Insomnia.
- Onset usually before age 20 years.
- History of childhood fears and social inhibition may be present.
11.3 Phobia Clues¶
- Marked and persistent fear of objects or situations.
- Immediate anxiety reaction upon exposure.
- Avoidance of the phobic stimulus.
- Impairment of occupational or social functioning.
- Social phobia: Specific fear of social or performance situations.
- Exposure to unfamiliar individuals or examination/evaluation by others.
11.4 PTSD Clues¶
- Exposure to actual or threatened death, serious injury, or sexual violence.
- Recurrent, involuntary, and intrusive distressing memories.
- Recurrent distressing dreams.
- Dissociative reactions (e.g., flashbacks).
- Intense or prolonged psychological distress at exposure to internal or external cues.
- Marked physiological reactions to internal or external cues.
- Persistent avoidance of stimuli associated with the traumatic event(s).
- Negative alterations in cognitions and mood.
- Persistent, distorted cognitions about the cause or consequences of the traumatic event(s).
WHAT EXCLUDES THE DIAGNOSIS¶
- Panic Disorder: A diagnosis of panic disorder is made as after a medical etiology for the panic attacks has been ruled out.
- GAD Criteria E: The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition (e.g., hyperthyroidism).
- GAD Criteria F: The disturbance is not better explained by another mental disorder (e.g., anxiety or worry about having panic attacks in panic disorder, negative evaluation in social anxiety disorder, contamination or other obsessions in obsessive-compulsive disorder, separation from attachment figures in separation anxiety disorder, reminders of traumatic events in posttraumatic stress disorder, gaining weight in anorexia nervosa, physical complaints in somatic symptom disorder, perceived appearance flaws in body dysmorphic disorder, having a serious illness in illness anxiety disorder, or the content of delusional beliefs in schizophrenia or delusional disorder).
- Benzodiazepines: Contraindicated during pregnancy and breast-feeding.
12.1 Medical Exclusions¶
- Pheochromocytoma.
- Thyrotoxicosis.
- Hypoglycemia.
- Paroxysmal atrial tachycardia.
- Mitral valve prolapse.
- Cardiovascular conditions associated with panic.
12.2 Psychiatric Exclusions¶
- Anxiety or worry about having panic attacks in panic disorder.
- Negative evaluation in social anxiety disorder.
- Contamination or other obsessions in obsessive-compulsive disorder.
- Separation from attachment figures in separation anxiety disorder.
- Reminders of traumatic events in posttraumatic stress disorder.
- Gaining weight in anorexia nervosa.
- Physical complaints in somatic symptom disorder.
- Perceived appearance flaws in body dysmorphic disorder.
- Having a serious illness in illness anxiety disorder.
- The content of delusional beliefs in schizophrenia or delusional disorder.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
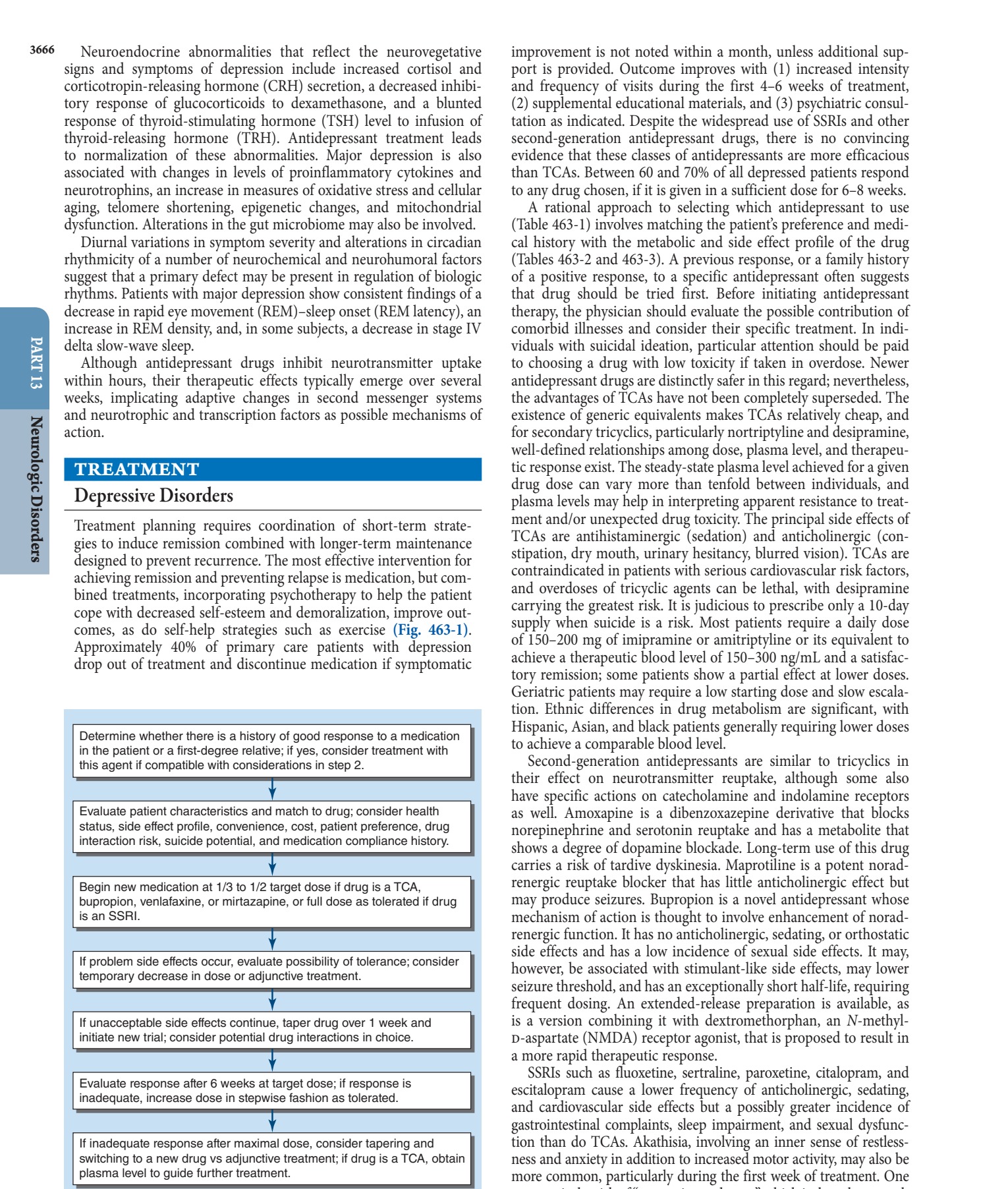
Caption: FIGURE 463-1 A guideline for the medical management of major depressive disorder. SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.