Hypothyroidism¶
Chapter 395 | Part 12: Endocrinology · Part 12 – Endocrinology & Metabolism
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- A normal TSH level excludes primary (but not secondary) hypothyroidism.
- Subclinical hypothyroidism refers to biochemical evidence of thyroid hormone deficiency in patients who have few or no apparent clinical features of hypothyroidism.
- In patients of normal body weight who are taking ≥200 μg of LT4 daily, an elevated TSH level is often a sign of poor adherence to treatment.
- In women without evidence of thyroid dysfunction, serum TSH decreases in the late first trimester, and if trimester-specific ranges are not available, an appropriate range for 7–12 weeks' gestation can be used.
- About 10–15% of patients may have persistent symptoms despite restoration of euthyroidism with LT4 for reasons that remain unclear.
- Patients with a suppressed TSH of any cause, including LT4 overtreatment, have an increased risk of atrial fibrillation and reduced bone density.
- Autoimmune hypothyroidism is more common in certain populations, such as the Japanese, probably because of genetic factors and chronic exposure to a high-iodine diet.
- Up to 20% of patients with autoimmune hypothyroidism have antibodies against the TSH-R, which, in contrast to thyroid-stimulating immunoglobulin (TSI), do not stimulate the receptor but prevent the binding of TSH.
- The goal of treatment is to maintain free T4 levels in the upper half of the reference interval because TSH levels cannot be used to monitor therapy in secondary hypothyroidism.
- Early treatment with T4 results in normal IQ levels, but subtle neurodevelopmental abnormalities may occur in those with the most severe hypothyroidism at diagnosis or when treatment is delayed or suboptimal.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification Systems
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Primary Hypothyroidism Causes
- 3.2 Secondary Hypothyroidism Causes
- 3.3 Transient Hypothyroidism Causes
- 3.4 Genetic Causes of Congenital Hypothyroidism
- 4. CLINICAL FEATURES
- 4.1 Symptoms and Signs
- 4.2 Pediatric Manifestations
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Distinguishing Features
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Algorithm
- 6.2 Laboratory Evaluation
- 7. MANAGEMENT & TREATMENT
- 7.1 Drug Therapy
- 7.2 Subclinical Hypothyroidism Management
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Long-term Follow-up
- 9. SPECIAL CONSIDERATIONS
- 9.1 Drug Interactions
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Clinical Clues
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Evaluation of hypothyroidism |
| 1 | 🖼 Figure | Facial appearance in hypothyroidism |
1. DEFINITION & OVERVIEW¶
📖 Harrison's defines this as:
Subclinical hypothyroidism refers to biochemical evidence of thyroid hormone deficiency in patients who have few or no apparent clinical features of hypothyroidism.
- Hypothyroidism is a condition characterized by insufficient production of thyroid hormone.¶
- Harrison's defines this as: Clinical hypothyroidism or overt hypothyroidism.
- Harrison's defines this as: Autoimmune hypothyroidism (Hashimoto’s thyroiditis) may be associated with a goiter (goitrous thyroiditis) or atrophic thyroiditis.
- Harrison's defines this as: Transient hypothyroidism.
- Harrison's defines this as: Secondary or central hypothyroidism.
- Harrison's defines this as: Congenital hypothyroidism.
1.1 Classification Systems¶
- Hypothyroidism is classified based on the site of defect.
- Primary hypothyroidism: Defect in the thyroid gland.
- Secondary hypothyroidism: Defect in the pituitary or hypothalamus.
- Transient hypothyroidism: Temporary dysfunction.
- Congenital hypothyroidism: Present at birth.
- Autoimmune hypothyroidism: Hashimoto’s thyroiditis, atrophic thyroiditis.
2. EPIDEMIOLOGY¶
- The mean annual incidence rate of autoimmune hypothyroidism is up to 4 per 1000 women and 1 per 1000 men.
- It is more common in certain populations, such as the Japanese, probably because of genetic factors and chronic exposure to a high-iodine diet.
- Hypothyroidism typically occurs between 30 and 50 years of age.
- The prevalence of overt hypothyroidism increases with age.
- Subclinical hypothyroidism is found in 6–8% of women (10% over the age of 60) and 3% of men.
- The annual risk of developing clinical hypothyroidism is ~4% when subclinical hypothyroidism is associated with positive thyroid peroxidase (TPO) antibodies.
- The mean age at diagnosis is 60 years.
- Hypothyroidism occurs in about 1 in 2000–4000 newborns.
- Neonatal screening is performed in most industrialized countries.
- The female preponderance of thyroid autoimmunity is most likely due to sex steroid effects on the immune response, but an X chromosome–related genetic factor is also possible and may account for the high frequency of autoimmune hypothyroidism in Turner’s syndrome.
2.1 Risk Factors¶
- Genetic factors: HLA-DR polymorphisms are the best documented genetic risk factors for autoimmune hypothyroidism, especially HLA-DR3, DR4, and DR5 in Caucasians.
- Environmental factors: A high iodine or low selenium intake and decreased exposure to microorganisms in childhood increase the risk of autoimmune hypothyroidism.
- Smoking cessation transiently increases incidence, whereas alcohol intake seems protective.
- A gene on chromosome 21 may be responsible for the association between autoimmune hypothyroidism and Down’s syndrome.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Susceptibility to autoimmune hypothyroidism is determined by a combination of genetic and environmental factors.
- The risk of either autoimmune hypothyroidism or Graves’ disease is increased among siblings.
- Thyroid cell destruction is primarily mediated by the CD8+ cytotoxic T cells.
- Local production of cytokines, such as tumor necrosis factor (TNF), interleukin-1 (IL-1), and interferon γ (IFN-γ), derived from the inflammatory infiltrate may render thyroid cells more susceptible to apoptosis mediated by death receptors, such as Fas, and by oxidative stress.
- These cytokines also impair thyroid cell function directly and induce the expression of other proinflammatory molecules by the thyroid cells themselves, such as cytokines, human leukocyte antigen (HLA) class I and class II molecules, adhesion molecules, CD40, and nitric oxide.
- Antibodies to TPO and thyroglobulin (Tg) are clinically useful markers of thyroid autoimmunity, but any pathogenic effect is restricted to a secondary role in amplifying an ongoing autoimmune response.
- TPO antibodies fix complement, and complement membrane-attack complexes are present in the thyroid in autoimmune hypothyroidism.
- However, transplacental passage of Tg or TPO antibodies has no effect on the fetal thyroid, which suggests that T cell–mediated injury is required to initiate autoimmune damage to the thyroid.
- Up to 20% of patients with autoimmune hypothyroidism have antibodies against the TSH-R, which, in contrast to thyroid-stimulating immunoglobulin (TSI), do not stimulate the receptor but prevent the binding of TSH.
- These TSH-R-blocking antibodies, therefore, cause hypothyroidism and, especially in Asian patients, thyroid atrophy.
- Their transplacental passage may induce transient neonatal hypothyroidism.
- Rarely, patients have a mixture of TSI and TSH-R-blocking antibodies, and thyroid function can oscillate between hyperthyroidism and hypothyroidism as one or the other antibody becomes dominant.
- Predicting the course of disease in such individuals is difficult, and they require close monitoring of thyroid function.
- Bioassays can be used to document that TSH-R-blocking antibodies reduce the cyclic AMP–inducing effect of TSH on cultured TSH-R-expressing cells, but these assays are difficult to perform.
- Immunoassays for TSH receptor antibodies, which measure whether the patient’s serum contains an antibody that can displace either labeled TSH or a monoclonal TSH receptor antibody from the TSH receptor, do not distinguish between these types of functional antibodies, but a positive result in a patient with spontaneous hypothyroidism is strong evidence for the presence of blocking antibodies.
- The use of these assays does not generally alter clinical management, although it may be useful to confirm the cause of transient neonatal hypothyroidism.
3.1 Primary Hypothyroidism Causes¶
- Autoimmune hypothyroidism: Hashimoto’s thyroiditis, atrophic thyroiditis.
- Iatrogenic: 131I treatment, subtotal or total thyroidectomy, external irradiation of neck for lymphoma or cancer.
- Drugs: iodine excess (including iodine-containing contrast media), amiodarone, lithium, antithyroid drugs, p-aminosalicylic acid, interferon α and other cytokines, aminoglutethimide, tyrosine kinase inhibitors (e.g., sunitinib), immune checkpoint inhibitors (e.g., ipilimumab, nivolumab, pembrolizumab).
- Congenital hypothyroidism: absent or ectopic thyroid gland, dyshormonogenesis, TSH-R mutation.
- Iodine deficiency.
- Infiltrative disorders: amyloidosis, sarcoidosis, hemochromatosis, scleroderma, cystinosis, Riedel’s thyroiditis.
- Overexpression of type 3 deiodinase in infantile hemangioma and other tumors.
3.2 Secondary Hypothyroidism Causes¶
- Hypopituitarism: tumors, pituitary surgery or irradiation, infiltrative disorders, Sheehan’s syndrome, trauma, genetic forms of combined pituitary hormone deficiencies.
- Isolated TSH deficiency or inactivity.
- Drugs: bexarotene, mitotane.
- Hypothalamic disease: tumors, trauma, infiltrative disorders, Prader-Willi syndrome.
3.3 Transient Hypothyroidism Causes¶
- Silent thyroiditis, including postpartum thyroiditis.
- Subacute thyroiditis.
- Withdrawal of supraphysiologic thyroxine treatment in individuals with an intact thyroid.
- After 131I treatment or subtotal thyroidectomy for Graves’ disease.
3.4 Genetic Causes of Congenital Hypothyroidism¶
- PROP-1: Central, hypothyroidism, Homozygous recessive, Combined pituitary hormone deficiencies, including thyroid-stimulating hormone (TSH), with preservation of adrenocorticotropic hormone.
- PIT-1: Central, hypothyroidism, Homozygous or heterozygous loss of function, Combined deficiencies of growth hormone, prolactin, TSH.
- IGSF1: Central, hypothyroidism, X-linked loss of function, Loss of TSH receptor (TSH-R) expression, testicular enlargement.
- TSHβ: Central, hypothyroidism, Heterozygous loss of function, TSH deficiency.
- TTF-1 (TITF-1): Primary, thyroid dysgenesis, Heterozygous loss of function, Variable thyroid hypoplasia, choreoathetosis, pulmonary problems.
- TTF-2 (FOXE-1): Primary, thyroid dysgenesis, Homozygous recessive, Thyroid agenesis, choanal atresia, spiky hair.
- PAX-8: Primary, thyroid dysgenesis, Heterozygous loss of function, Thyroid dysgenesis, kidney abnormalities.
- NKX2-1: Primary, thyroid dysgenesis, Heterozygous loss of function, Thyroid dysgenesis, brain, lung abnormalities.
- NKX2-5: Primary, thyroid dysgenesis, Heterozygous loss of function, Thyroid dysgenesis, heart abnormalities.
- GLIS3: Primary, thyroid dysgenesis, Homozygous recessive, Thyroid dysgenesis, neonatal diabetes, facial abnormalities.
- JAG-1: Primary, thyroid dysgenesis, Heterozygous loss of function, Thyroid dysgenesis, Alagille syndrome type 1, heart abnormalities.
- TSH receptor: Primary, thyroid dysgenesis and dyshormonogenesis, Homozygous recessive, Resistance to TSH.
- Gαs (Albright hereditary osteodystrophy): Primary, thyroid dyshormonogenesis, Heterozygous loss of function, imprinting, Resistance to TSH.
- Na+/I– symporter (SLC5A5): Primary, thyroid dyshormonogenesis, Homozygous recessive, Inability to transport iodide.
- DUOX2 (THOX2): Primary, thyroid dyshormonogenesis, Heterozygous loss of function, Organification defect.
- DUOXA2: Primary, thyroid dyshormonogenesis, Homozygous recessive, Organification defect.
- Thyroid peroxidase: Primary, thyroid dyshormonogenesis, Homozygous recessive, Defective organification of iodide.
- Thyroglobulin: Primary, thyroid dyshormonogenesis, Homozygous recessive, Defective synthesis of thyroid hormone.
- Pendrin (SLC26A4): Primary, thyroid dyshormonogenesis, Homozygous recessive, Pendred syndrome: sensorineural deafness and partial organification defect in thyroid.
- Dehalogenase 1 (IYD): Primary, thyroid dyshormonogenesis, Homozygous recessive, Loss of iodide reutilization.
4. CLINICAL FEATURES¶
- The onset is usually insidious, and the patient may become aware of symptoms only when euthyroidism is restored.
- Patients with Hashimoto’s thyroiditis may present because of goiter rather than symptoms of hypothyroidism.
- The goiter may not be large, but it is usually irregular and firm in consistency.
- Rarely, uncomplicated Hashimoto’s thyroiditis is associated with pain.
- Patients with atrophic thyroiditis or the later stage of Hashimoto’s thyroiditis present with symptoms and signs of hypothyroidism.
- The skin is dry, and there is decreased sweating, thinning of the epidermis, and hyperkeratosis of the stratum corneum.
- Increased dermal glycosaminoglycan content traps water, giving rise to skin thickening without pitting (myxedema).
- Typical features include a puffy face with edematous eyelids and nonpitting pretibial edema.
- There is pallor, often with a yellow tinge to the skin due to carotene accumulation.
- Nail growth is retarded, and hair is dry, brittle, difficult to manage, and falls out easily.
- In addition to diffuse alopecia, there is thinning of the outer third of the eyebrows, although this is not a specific sign of hypothyroidism.
- Other common features include constipation and weight gain (despite a poor appetite).
- In contrast to popular perception, the weight gain is usually modest and due mainly to fluid retention in the myxedematous tissues.
- Libido is decreased in both sexes, and there may be oligomenorrhea or amenorrhea in long-standing disease, but menorrhagia may occur at an early stage.
- Fertility is reduced, and the incidence of miscarriage is increased.
- Prolactin levels are often modestly increased and may contribute to alterations in libido and fertility and cause galactorrhea.
- Myocardial contractility and pulse rate are reduced, leading to a reduced stroke volume and bradycardia.
- Increased peripheral resistance may be accompanied by hypertension, particularly diastolic.
- Blood flow is diverted from the skin, producing cool extremities.
- Pericardial effusions occur in up to 30% of patients but rarely compromise cardiac function.
- Although alterations in myosin heavy chain isoform expression have been documented, cardiomyopathy is rare.
- Fluid may also accumulate in other serous cavities and in the middle ear, giving rise to conductive deafness; sensorineural deafness may also occur.
- Pulmonary function is generally normal, but dyspnea may be caused by pleural effusion, impaired respiratory muscle function, diminished ventilatory drive, or sleep apnea.
- Carpal tunnel and other entrapment syndromes are common, as is impairment of muscle function with stiffness, cramps, and pain.
- On examination, there may be slow relaxation of tendon reflexes and pseudomyotonia.
- Memory and concentration are impaired.
- Rare neurologic problems include reversible cerebellar ataxia, dementia, psychosis, and myxedema coma.
- Hashimoto’s encephalopathy has been defined as a steroid-responsive syndrome associated with TPO antibodies, myoclonus, and slow-wave activity on electroencephalography, but the relationship with thyroid autoimmunity or hypothyroidism is not established, and if a patient is euthyroid, levothyroxine (LT4) therapy has not been shown to be efficacious in treatment.
- The hoarse voice and occasionally clumsy speech of hypothyroidism reflect fluid accumulation in the vocal cords and tongue.
- Except when accompanied by iron deficiency or B12 deficiency from concomitant pernicious anemia, the anemia and other abnormalities gradually resolve with thyroxine replacement.
4.1 Symptoms and Signs¶
- Tiredness, weakness.
- Dry skin.
- Feeling cold.
- Hair loss.
- Difficulty concentrating and poor memory.
- Constipation.
- Weight gain with poor appetite.
- Dyspnea.
- Hoarse voice.
- Menorrhagia (later oligomenorrhea or amenorrhea).
- Paresthesia.
- Impaired hearing.
- Dry coarse skin; cool peripheral extremities.
- Puffy face, hands, and feet (myxedema).
- Diffuse alopecia.
- Bradycardia.
- Peripheral edema.
- Delayed tendon reflex relaxation.
- Carpal tunnel syndrome.
- Serous cavity effusions.
4.2 Pediatric Manifestations¶
- Autoimmune hypothyroidism is uncommon in children and usually presents with slow growth and delayed facial and dental maturation.
- The pituitary may be enlarged due to thyrotroph hyperplasia.
- Myopathy, with muscle swelling, is more common in children than in adults.
- In most cases, puberty is delayed, but precocious puberty sometimes occurs.
- There may be intellectual impairment if the onset is before 3 years and the hormone deficiency is severe.
5. DIFFERENTIAL DIAGNOSIS¶
- An asymmetric goiter in Hashimoto’s thyroiditis may be confused with a multinodular goiter (MNG) or thyroid carcinoma, in which thyroid antibodies may also be present.
- Primary thyroid lymphoma is rare but strongly associated with preexisting autoimmune thyroiditis.
- Ultrasound can be used to show the presence of solitary or multiple nodules rather than the thyroid enlargement with heterogeneous echogenicity typical of Hashimoto’s thyroiditis.
- However, ultrasound imaging may also detect pseudonodules, hypoechoic areas likely representing areas of lymphocytic infiltrates, which need to be distinguished from true superimposed nodules as fine-needle aspirate is not warranted for these.
- Fine-needle aspiration biopsy should be performed for all true nodules meeting criteria.
- Other causes of hypothyroidism are discussed in Table 395-1 but rarely cause diagnostic confusion.
5.1 Distinguishing Features¶
- Hashimoto’s thyroiditis: Asymmetric goiter, heterogeneous echogenicity, thyroid antibodies present.
- Multinodular goiter: Multiple nodules, thyroid antibodies may be present.
- Thyroid carcinoma: Nodules, thyroid antibodies may be present.
- Primary thyroid lymphoma: Rare, strongly associated with preexisting autoimmune thyroiditis.
- Pseudonodules: Hypoechoic areas likely representing areas of lymphocytic infiltrates, fine-needle aspirate not warranted.
6. INVESTIGATIONS & DIAGNOSIS¶
- A normal TSH level excludes primary (but not secondary) hypothyroidism.
- If the TSH is elevated, a free or unbound T4 level (FT4) is needed to confirm the presence of clinical hypothyroidism, but T4 is inferior to TSH when used as a screening test because it will not detect subclinical hypothyroidism.
- Circulating unbound T4 levels are normal in ~25% of patients, reflecting adaptive deiodinase responses to hypothyroidism.
- T4 measurements are, therefore, not indicated.
- Once clinical or subclinical hypothyroidism is confirmed, the etiology is usually easily established by demonstrating the presence of TPO and Tg antibodies, which are present in >95% of patients with autoimmune hypothyroidism.
- Other abnormal laboratory findings in hypothyroidism may include increased creatine phosphokinase, elevated cholesterol and triglycerides, and anemia (usually normocytic or macrocytic) depending upon the degree and duration of hypothyroidism.
- The diagnosis is confirmed by detecting a low unbound T4 level in secondary hypothyroidism.
- The goal of treatment is to maintain free T4 levels in the upper half of the reference interval because TSH levels cannot be used to monitor therapy in secondary hypothyroidism.
- In patients of normal body weight who are taking ≥200 μg of LT4 daily, an elevated TSH level is often a sign of poor adherence to treatment.
- Such patients often have normal or high free T4 levels, despite an elevated TSH, because they remember to take medication for a few days before testing; this is sufficient to normalize T4, but not TSH levels.
- It is important to consider variable adherence because this pattern of thyroid function tests is otherwise suggestive of disorders associated with inappropriate TSH secretion.
- Because T4 has a long half-life (7 days), patients who miss a dose can be advised to take two doses of the skipped tablets at once.
- Other causes of increased LT4 requirements must be excluded, particularly malabsorption (e.g., celiac disease, small-bowel surgery, atrophic or Helicobacter pylori–related gastritis), oral estrogen-containing medications or selective estrogen receptor modulator therapy, ingestion with a meal, and drugs that interfere with T4 absorption or metabolism such as bile acid sequestrants, ferrous sulfate, calcium supplements, sevelamer, sucralfate, proton pump inhibitors, lovastatin, aluminum hydroxide, rifampicin, amiodarone, carbamazepine, phenytoin, and tyrosine kinase inhibitors.
6.1 Diagnostic Algorithm¶
- Step 1: Measure TSH.
- If Elevated: Measure unbound T4.
- If Normal: Pituitary disease suspected? Yes -> Measure unbound T4. No -> Mild Primary hypothyroidism, no further tests.
- If Normal: Measure unbound T4.
- If Low: Autoimmune hypothyroidism (TPOAb+ or TPOAb–).
- If Normal: Rule out other causes of hypothyroidism.
- If Low: Annual follow-up T4 treatment then evaluate anterior pituitary function.
- If Normal: Rule out drug effects, sick euthyroid syndrome.
6.2 Laboratory Evaluation¶
- TSH: Screening test.
- Unbound T4: Confirm clinical hypothyroidism if TSH elevated.
- TPO antibodies: Present in >95% of patients with autoimmune hypothyroidism.
- Tg antibodies: Present in >95% of patients with autoimmune hypothyroidism.
- Creatine phosphokinase: Increased.
- Cholesterol: Elevated.
- Triglycerides: Elevated.
- Anemia: Normocytic or macrocytic.
7. MANAGEMENT & TREATMENT¶
- If there is no residual thyroid function, the daily replacement dose of LT4 is usually 1.6 μg/kg body weight (typically 100–150 μg), ideally taken at least 30 min before breakfast.
- In many patients, however, lower doses suffice until residual thyroid tissue is destroyed.
- In patients who develop hypothyroidism after the treatment of Graves’ disease, there is often underlying autonomous function, necessitating lower replacement doses (typically 75–125 μg/d).
- Adult patients under 60 years old without evidence of heart disease may be started on 50–100 μg of LT4 daily.
- The dose is adjusted on the basis of TSH levels, with the goal of treatment being a normal TSH, ideally in the lower half of the reference range.
- TSH responses are gradual and should be measured about 6–8 weeks after instituting treatment or after any subsequent change in LT4 dosage.
- The clinical effects of LT4 replacement are slow to appear.
- Patients may not experience full relief from symptoms until several months after normal TSH levels are restored.
- Adjustment of LT4 dosage is made in 12.5- or 25-μg increments if the TSH is high; decrements of the same magnitude should be made if the TSH is suppressed.
- Patients with a suppressed TSH of any cause, including LT4 overtreatment, have an increased risk of atrial fibrillation and reduced bone density.
- About 10–15% of patients may have persistent symptoms despite restoration of euthyroidism with LT4 for reasons that remain unclear.
- Although desiccated animal thyroid preparations (thyroid extract USP) are available, they are not recommended because the ratio of T4 to T3 is nonphysiologic.
- The use of LT4 combined with liothyronine (triiodothyronine, T3) has been investigated, but benefit has not been confirmed in prospective studies.
- There is no place for liothyronine alone as long-term replacement, because the short half-life necessitates three or four daily doses and is associated with fluctuating T4 levels.
- Once full replacement is achieved and TSH levels are stable, follow-up measurement of TSH is recommended at annual intervals.
- It is important to ensure ongoing adherence as patients do not feel any symptomatic difference after missing a few doses of LT4, and this sometimes leads to self-discontinuation.
- In patients of normal body weight who are taking ≥200 μg of LT4 daily, an elevated TSH level is often a sign of poor adherence to treatment.
- Such patients often have normal or high free T4 levels, despite an elevated TSH, because they remember to take medication for a few days before testing; this is sufficient to normalize T4, but not TSH levels.
- It is important to consider variable adherence because this pattern of thyroid function tests is otherwise suggestive of disorders associated with inappropriate TSH secretion.
- Because T4 has a long half-life (7 days), patients who miss a dose can be advised to take two doses of the skipped tablets at once.
- Other causes of increased LT4 requirements must be excluded, particularly malabsorption (e.g., celiac disease, small-bowel surgery, atrophic or Helicobacter pylori–related gastritis), oral estrogen-containing medications or selective estrogen receptor modulator therapy, ingestion with a meal, and drugs that interfere with T4 absorption or metabolism such as bile acid sequestrants, ferrous sulfate, calcium supplements, sevelamer, sucralfate, proton pump inhibitors, lovastatin, aluminum hydroxide, rifampicin, amiodarone, carbamazepine, phenytoin, and tyrosine kinase inhibitors.
- A trial of treatment may be considered when young or middle-aged patients have symptoms of hypothyroidism or risk of heart disease.
- It is important to confirm that any elevation of TSH is sustained over a 3-month period before treatment is given.
- Treatment is administered by starting with a low dose of LT4 (25–50 μg/d) with the goal of normalizing TSH.
- In women without evidence of thyroid dysfunction, serum TSH decreases in the late first trimester, and if trimester-specific ranges are not available, an appropriate range for 7–12 weeks' gestation can be used.
- Because maternal hypothyroidism may both adversely affect fetal neural development and be associated with adverse gestational outcomes (miscarriage, preterm delivery), thyroid function should be monitored to preserve euthyroidism in women with a history or high risk of hypothyroidism.
- Although epidemiologic studies have demonstrated the association of miscarriage and preterm delivery with the presence of thyroid autoantibodies detected either during or prior to gestation in euthyroid women, randomized controlled multicenter trials evaluating LT4 therapy prior to conception in this population have not demonstrated benefit.
- Because of the known increase in thyroid hormone requirements during pregnancy in hypothyroid women, LT4 therapy should be targeted to maintain a serum TSH in the normal range but <2.5 mIU/L prior to conception.
- In women without evidence of thyroid dysfunction, serum TSH decreases in the late first trimester, and if trimester-specific ranges are not available, an appropriate range for 7–12 weeks' gestation can be used.
7.1 Drug Therapy¶
- Drug: Levothyroxine (LT4).
- Dose: 1.6 μg/kg body weight (typically 100–150 μg).
- Frequency: Daily, ideally taken at least 30 min before breakfast.
- Monitoring: TSH levels, measured about 6–8 weeks after instituting treatment or after any subsequent change in LT4 dosage.
- Key Side Effects: None specific, but overtreatment can cause atrial fibrillation and reduced bone density.
- Contraindications: None specific, but caution in patients with heart disease.
7.2 Subclinical Hypothyroidism Management¶
- There are no universally accepted recommendations for the management of subclinical hypothyroidism.
- LT4 is recommended if the patient is a woman who wishes to conceive or is pregnant or when TSH levels are >10 mIU/L.
- Most other patients can simply be monitored annually.
- A trial of treatment may be considered when young or middle-aged patients have symptoms of hypothyroidism or risk of heart disease.
- It is important to confirm that any elevation of TSH is sustained over a 3-month period before treatment is given.
8. PROGNOSIS & COMPLICATIONS¶
- Early treatment with T4 results in normal IQ levels, but subtle neurodevelopmental abnormalities may occur in those with the most severe hypothyroidism at diagnosis or when treatment is delayed or suboptimal.
- If transient hypothyroidism is suspected, or the diagnosis is unclear, treatment can be stopped safely after the age of 3 years followed by further evaluation.
- About 10–15% of patients may have persistent symptoms despite restoration of euthyroidism with LT4 for reasons that remain unclear.
- Patients with a suppressed TSH of any cause, including LT4 overtreatment, have an increased risk of atrial fibrillation and reduced bone density.
- Rare neurologic problems include reversible cerebellar ataxia, dementia, psychosis, and myxedema coma.
- Hashimoto’s encephalopathy has been defined as a steroid-responsive syndrome associated with TPO antibodies, myoclonus, and slow-wave activity on electroencephalography, but the relationship with thyroid autoimmunity or hypothyroidism is not established, and if a patient is euthyroid, levothyroxine (LT4) therapy has not been shown to be efficacious in treatment.
8.1 Long-term Follow-up¶
- Once full replacement is achieved and TSH levels are stable, follow-up measurement of TSH is recommended at annual intervals.
- It is important to ensure ongoing adherence as patients do not feel any symptomatic difference after missing a few doses of LT4, and this sometimes leads to self-discontinuation.
- Because T4 has a long half-life (7 days), patients who miss a dose can be advised to take two doses of the skipped tablets at once.
9. SPECIAL CONSIDERATIONS¶
- Pregnancy: Because maternal hypothyroidism may both adversely affect fetal neural development and be associated with adverse gestational outcomes (miscarriage, preterm delivery), thyroid function should be monitored to preserve euthyroidism in women with a history or high risk of hypothyroidism.
- Although epidemiologic studies have demonstrated the association of miscarriage and preterm delivery with the presence of thyroid autoantibodies detected either during or prior to gestation in euthyroid women, randomized controlled multicenter trials evaluating LT4 therapy prior to conception in this population have not demonstrated benefit.
- Because of the known increase in thyroid hormone requirements during pregnancy in hypothyroid women, LT4 therapy should be targeted to maintain a serum TSH in the normal range but <2.5 mIU/L prior to conception.
- Pediatrics: Autoimmune hypothyroidism is uncommon in children and usually presents with slow growth and delayed facial and dental maturation.
- The pituitary may be enlarged due to thyrotroph hyperplasia.
- Myopathy, with muscle swelling, is more common in children than in adults.
- In most cases, puberty is delayed, but precocious puberty sometimes occurs.
- There may be intellectual impairment if the onset is before 3 years and the hormone deficiency is severe.
- Rarely, LT4 replacement is associated with pseudotumor cerebri in children.
- Presentation appears to be idiosyncratic and occurs months after treatment has begun.
- Elderly: Adult patients under 60 years old without evidence of heart disease may be started on 50–100 μg of LT4 daily.
- Renal/Hepatic Impairment: Not explicitly mentioned in source text.
- Immunocompromised: Not explicitly mentioned in source text.
9.1 Drug Interactions¶
- Drugs that interfere with T4 absorption or metabolism: bile acid sequestrants, ferrous sulfate, calcium supplements, sevelamer, sucralfate, proton pump inhibitors, lovastatin, aluminum hydroxide, rifampicin, amiodarone, carbamazepine, phenytoin, and tyrosine kinase inhibitors.
- Oral estrogen-containing medications or selective estrogen receptor modulator therapy.
- Ingestion with a meal.
10. KEY PEARLS & CLINICAL TRAPS¶
- A normal TSH level excludes primary (but not secondary) hypothyroidism.
- In patients of normal body weight who are taking ≥200 μg of LT4 daily, an elevated TSH level is often a sign of poor adherence to treatment.
- About 10–15% of patients may have persistent symptoms despite restoration of euthyroidism with LT4 for reasons that remain unclear.
- Patients with a suppressed TSH of any cause, including LT4 overtreatment, have an increased risk of atrial fibrillation and reduced bone density.
- Autoimmune hypothyroidism is more common in certain populations, such as the Japanese, probably because of genetic factors and chronic exposure to a high-iodine diet.
- Up to 20% of patients with autoimmune hypothyroidism have antibodies against the TSH-R, which, in contrast to thyroid-stimulating immunoglobulin (TSI), do not stimulate the receptor but prevent the binding of TSH.
- The goal of treatment is to maintain free T4 levels in the upper half of the reference interval because TSH levels cannot be used to monitor therapy in secondary hypothyroidism.
- Early treatment with T4 results in normal IQ levels, but subtle neurodevelopmental abnormalities may occur in those with the most severe hypothyroidism at diagnosis or when treatment is delayed or suboptimal.
- Because T4 has a long half-life (7 days), patients who miss a dose can be advised to take two doses of the skipped tablets at once.
- Other causes of increased LT4 requirements must be excluded, particularly malabsorption (e.g., celiac disease, small-bowel surgery, atrophic or Helicobacter pylori–related gastritis), oral estrogen-containing medications or selective estrogen receptor modulator therapy, ingestion with a meal, and drugs that interfere with T4 absorption or metabolism such as bile acid sequestrants, ferrous sulfate, calcium supplements, sevelamer, sucralfate, proton pump inhibitors, lovastatin, aluminum hydroxide, rifampicin, amiodarone, carbamazepine, phenytoin, and tyrosine kinase inhibitors.
10.1 Clinical Clues¶
- Puffy face with edematous eyelids and nonpitting pretibial edema.
- Delayed tendon reflex relaxation.
- Myxedema.
- Dry coarse skin; cool peripheral extremities.
- Diffuse alopecia.
- Bradycardia.
- Peripheral edema.
- Carpal tunnel syndrome.
- Serous cavity effusions.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
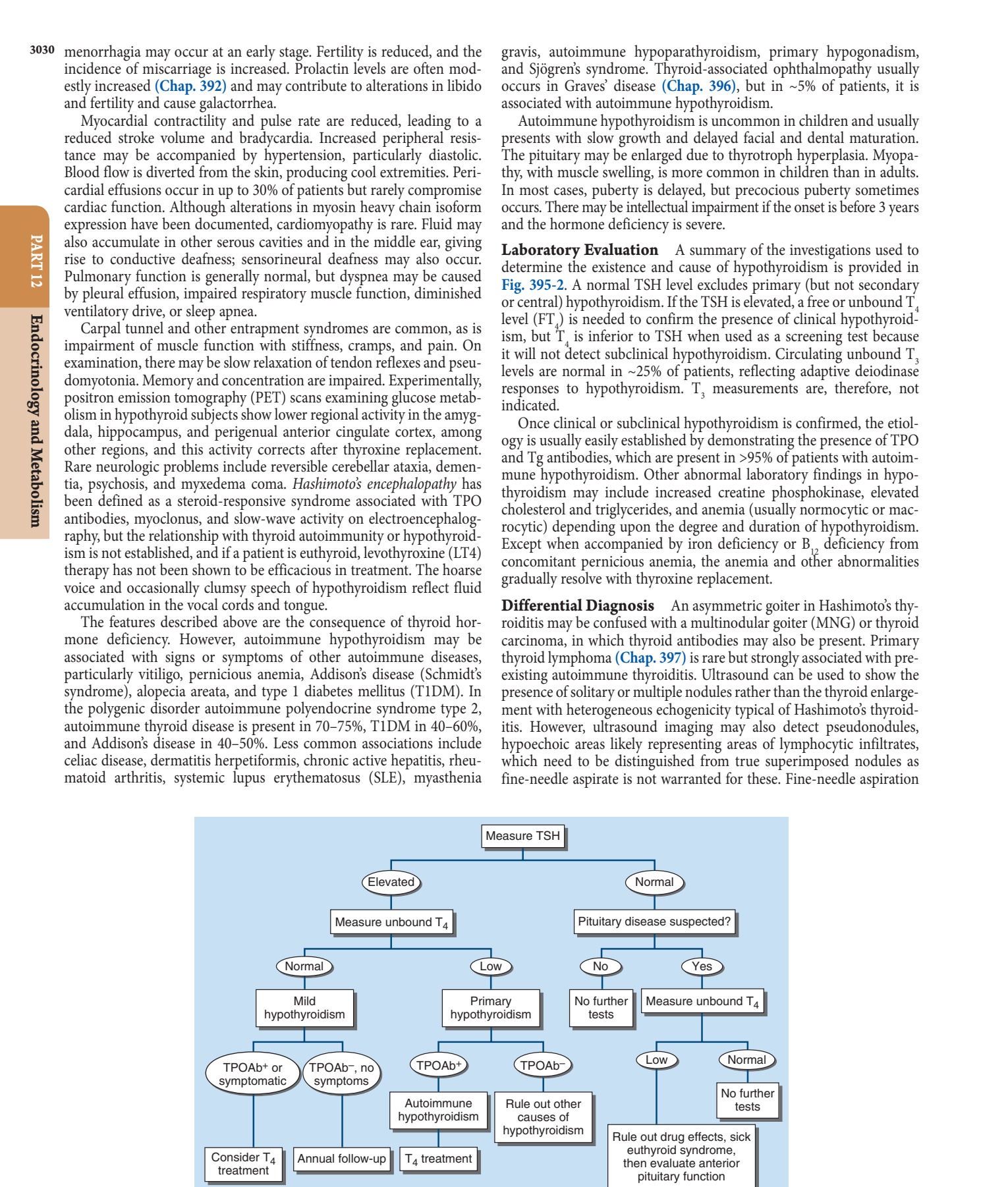
Caption: FIGURE 395-2 Evaluation of hypothyroidism. TPOAb+, thyroid peroxidase antibodies hormone.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 395-1 Facial appearance in hypothyroidism. Note puffy eyes and thickened skin. — FIGURE 395-1 Facial appearance in hypothyroidism. Note puffy eyes and thickened skin.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.