Viral Gastroenteritis¶
Chapter 209 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Viral (incl. HIV)
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Viral gastroenteritis is a leading cause of death among children in developing countries (0.5 million deaths/year) and accounts for up to 6–8% of hospitalizations in industrialized countries.
- Norovirus is the most common cause of medically attended gastroenteritis in young children in the US and the leading cause of epidemics worldwide (~50% of outbreaks).
- Rotavirus is the leading cause of severe dehydrating diarrhea in children 70–80% decline in hospitalizations in the US.
- Viral gastroenteritis is typically a diagnosis of exclusion; differentiation from bacterial causes relies on stool leukocytes/blood (absent in viral) and incubation period.
- Treatment is supportive (oral rehydration); antibiotics and antimotility agents are contraindicated.
- Rotavirus vaccines (RotaTeq, Rotarix) are recommended for routine immunization of US infants; herd protection reduces disease in unvaccinated contacts.
- Norovirus shedding can occur before symptoms and for weeks after resolution; immunocompromised individuals may shed virus for prolonged periods.
- Rotavirus infection destroys mature enterocytes in the villous epithelium, leading to secretory diarrhea and malabsorption of carbohydrates/fats.
- In temperate climates, viral gastroenteritis (especially rotavirus) peaks in winter months; in tropical areas, it occurs year-round.
- Intussusception is a rare but serious complication associated with rotavirus vaccination in some high- and middle-income countries, though benefits exceed risks.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Etiologic Agents
- 2. EPIDEMIOLOGY
- 2.1 Rotavirus Epidemiology
- 2.2 Calicivirus Epidemiology
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Rotavirus Pathogenesis
- 3.2 Norovirus Pathogenesis
- 4. CLINICAL FEATURES
- 4.1 Rotavirus Clinical Manifestations
- 4.2 Norovirus Clinical Manifestations
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Viral vs Bacterial Differentiation
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Assays
- 7. MANAGEMENT & TREATMENT
- 7.1 Treatment Guidelines
- 7.2 Prevention Strategies
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Mortality and Morbidity
- 8.2 Vaccine Safety
- 9. SPECIAL CONSIDERATIONS
- 9.1 Immunocompromised Hosts
- 9.2 Resource-Poor Settings
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Clinical Pearls
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Viral agents of gastroenteritis |
| 2 | 🖼 Figure | Rotavirus mortality rates by country, per 100,000 children <5 years of age |
1. DEFINITION & OVERVIEW¶
Acute infectious gastroenteritis is a common illness that affects persons of all ages worldwide. It is a leading cause of death among children in developing countries, accounting for an estimated 0.5 million deaths each year, and is responsible for up to 6–8% of all hospitalizations among children in industrialized countries, including the United States. Elderly persons, especially those with debilitating health conditions, are also at risk of severe complications and death from acute gastroenteritis. Among healthy young adults, acute gastroenteritis is rarely fatal but incurs substantial medical and social costs, including those of time lost from work.
1.1 Etiologic Agents¶
Several enteric viruses have been recognized as important etiologic agents of acute infectious gastroenteritis. Although most viral gastroenteritis is caused by RNA viruses, DNA viruses that are occasionally involved (e.g., adenovirus types 40 and 41) are included in this chapter. Illness caused by these viruses is characterized by the acute onset of vomiting and/or diarrhea, which may be accompanied by fever, nausea, abdominal cramps, anorexia, and malaise.
Table 1 — Table 209-1 Viral Causes of Gastroenteritis among Humans¶
| VIRUS | FAMILY | GENOME | PRIMARY AGE GROUP AT RISK | CLINICAL SEVERITY | DETECTION ASSAYS |
|---|---|---|---|---|---|
| Group A rotavirus | Reoviridae | Double-strand segmented RNA | Children <5 years | + + + | EIA (commercial), RT-PCR, EM, PAGE |
| Norovirus | Caliciviridae | Positive-sense single-strand RNA | All ages | + + | RT-PCR, EM, EIA (commercial) |
| Sapovirus | Caliciviridae | Positive-sense single-strand RNA | Children <5 years | + | RT-PCR, EM |
| Astrovirus | Astroviridae | Positive-sense single-strand RNA | Children <5 years | + | EIA, RT-PCR, EM |
| Adenovirus (mainly types 40 and 41) | Adenoviridae | Double-strand DNA | Children <5 years | +/+ + | EIA (commercial), PCR, EM |
2. EPIDEMIOLOGY¶
Infections with human caliciviruses are common and are worldwide, and most adults have antibodies to these viruses. Antibody is acquired at an earlier age in developing countries—a pattern consistent with the presumed fecal–oral mode of transmission. Infections occur year-round, although, in temperate climates, a distinct increase has been noted in cold-weather months. Noroviruses may be the most common infectious agents of mild gastroenteritis in the community. In the United States and some other developed countries, with the decline in severe rotavirus disease following implementation of a rotavirus vaccination program, norovirus has become the leading cause of medically attended gastroenteritis in young children. Noroviruses are also recognized as the major cause of epidemics of gastroenteritis worldwide. In the United States, ~50% of all reported outbreaks of gastroenteritis are caused by noroviruses.
2.1 Rotavirus Epidemiology¶
In tropical settings, rotavirus disease occurs year-round, with less pronounced seasonal peaks than in temperate settings, where rotavirus disease occurs predominantly during the cooler fall and winter months. Before the introduction of rotavirus vaccine in the United States, the rotavirus season each year began in the Southwest during the autumn and early winter (October through December) and migrated across the continent, peaking in the Northeast during late winter and spring (March through May). The reasons for this characteristic pattern are not clear but may be correlated with state-specific differences in birth rates, which could influence the rate of accumulation of susceptible infants after each rotavirus season. After the implementation of routine vaccination of U.S. infants against rotavirus in 2006, the characteristic prevaccine geotemporal pattern of U.S. rotavirus was dramatically altered, and these changes were accompanied by substantial declines in rotavirus detections by a national network of sentinel laboratories. Worldwide, nearly all children are infected with rotavirus by 3–5 years of age. Neonatal infections are common but are often asymptomatic or mild, presumably because of protection by maternal antibody or breast milk. Compared with rotavirus disease in industrialized countries, disease in developing countries occurs at a younger age, is less seasonal, is more frequently caused by uncommon or multiple rotavirus strains, and is more often fatal. Moreover, because of suboptimal access to hydration therapy, rotavirus is a leading cause of diarrheal death among children in the developing world.
Table 2 — Rotavirus Mortality Rates by Country¶
| Rates per 100,000 PY | 0 to <10 | 50 to <100 | ≥100 |
|---|---|---|---|
| Sub-Saharan Africa and Southern Asia | High | High | Highest |
2.2 Calicivirus Epidemiology¶
Noroviruses are transmitted predominantly by the fecal–oral route but is also present in vomitus. Because an inoculum with very few viruses can be infectious, transmission can occur by aerosolization, by contact with contaminated fomites, and by person-to-person contact. Viral shedding and infectivity are greatest during the acute illness, but challenge studies with Norwalk virus in volunteers indicate that viral antigen may be shed by asymptomatically infected persons and also by symptomatic persons before the onset of symptoms and for several weeks after the resolution of illness. Viral shedding can be prolonged in immunocompromised individuals.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Human Caliciviruses: Norovirus is the prototype strain of a group of small (27–40 nm), nonenveloped, round, icosahedral viruses with relatively amorphous surface features on visualization by electron microscopy. Molecular cloning and characterization have demonstrated that the viruses have a single, positive-strand RNA genome ~7.5 kb in length and possess a single virion-associated protein—similar to that of typical caliciviruses—with a molecular mass of 60 kDa. On the basis of these molecular characteristics, these viruses are presently classified into two genera belonging to the family Caliciviridae, the noroviruses and the sapoviruses, which are further classified into genogroups and genotypes. Of the 10 recognized norovirus genogroups in humans and animals, 35 different genotypes belonging to 5 genogroups (GI, GII, GIV, GVIII, and GIX) are known to infect humans. Pathogenesis: The exact sites and cellular receptors for attachment of viral particles have not been determined. Data suggest that carbohydrates that are similar to human histo-blood group antigens (HBGA) present on the gastroduodenal epithelium of individuals with the secretor phenotype may serve as ligands for the attachment of norovirus. Additional studies must more fully elucidate norovirus–carbohydrate interactions, including strain-specific variations. After the infection of volunteers, reversible lesions are noted in the upper jejunum, with broadening and blunting of the villi, shortening of the microvilli, vacuolization of the lining epithelium, crypt hyperplasia, and infiltration of the lamina propria by polymorphonuclear neutrophils and lymphocytes. The lesions persist for at least 4 days after the resolution of symptoms and are associated with malabsorption of carbohydrates and fats and a decreased level of brush-border enzymes. Adenylate cyclase activity is not altered. No histopathologic changes are seen in the stomach or colon, but gastric motor function is delayed, and this alteration is believed to contribute to the nausea and vomiting that are typical of this illness.
3.1 Rotavirus Pathogenesis¶
Rotaviruses infect and ultimately destroy mature enterocytes in the villous epithelium of the proximal small intestine. The loss of absorptive villous epithelium, coupled with the proliferation of secretory crypt cells, results in secretory diarrhea. Brush-border enzymes characteristic of differentiated cells are reduced, and this change leads to the accumulation of unmetabolized disaccharides and consequent osmotic diarrhea. Studies in mice indicate that a nonstructural rotavirus protein, NSP4, functions as an enterotoxin and contributes to secretory diarrhea by altering epithelial cell function and permeability. In addition, rotavirus may evoke fluid secretion through activation of the enteric nervous system in the intestinal wall. Rotavirus antigenemia and viremia are common among children with acute rotavirus infection, although the antigen and RNA levels in serum are substantially lower than those in stool.
Table 3 — Rotavirus Structure and Classification¶
| Feature | Description |
|---|---|
| Family | Reoviridae |
| Genome | 11 segments of double-strand RNA enclosed in a triple-layered, nonenveloped, icosahedral capsid 75 nm in diameter |
| Major Structural Protein | Viral protein 6 (VP6) — target of commercial immunoassays and determines the group specificity |
| Serotype Specificity | Two outer-capsid proteins, VP7 (G-protein) and VP4 (P-protein), determine serotype specificity, induce neutralizing antibodies, and form the basis for binary classification of rotaviruses (G and P types) |
| Groups | Seven major groups of rotavirus (A through G) exist; human illness is caused primarily by group A and, to a much lesser extent, by groups B and C |
3.2 Norovirus Pathogenesis¶
Rotavirus gastroenteritis can lead to severe dehydration; appropriate treatment should be instituted early. Standard oral rehydration therapy is successful for most children who can take fluids by mouth, but IV fluid replacement may be required for patients who are severely dehydrated or are unable to tolerate oral therapy because of frequent vomiting. The therapeutic roles of probiotics, bismuth subsalicylate, enkephalinase inhibitors, and nitazoxanide have been evaluated in clinical studies but are not clearly defined. Antibiotics and antimotility agents should be avoided. In immunocompromised children with chronic symptomatic rotavirus disease, orally administered immunoglobulins or colostrum may result in the resolution of symptoms, but the best choices regarding agents and their doses have not been well studied, and treatment decisions are often empirical.
4. CLINICAL FEATURES¶
Gastroenteritis caused by human caliciviruses has a sudden onset following an average incubation period of 24 h (range, 12–72 h). The illness generally lasts 12–60 h and is characterized by one or more of the following symptoms: nausea, vomiting, abdominal cramps, and diarrhea. Vomiting is more prevalent among children, whereas a greater proportion of adults develop diarrhea. Constitutional symptoms are common, including headache, fever, chills, and myalgias. The stools are characteristically loose and watery, without blood, mucus, or leukocytes. White cell counts are generally normal; rarely, leukocytosis with relative lymphopenia may be observed. Death is a rare outcome and usually results from severe dehydration in vulnerable persons (e.g., elderly patients with debilitating health conditions).
4.1 Rotavirus Clinical Manifestations¶
The clinical spectrum of rotavirus infection ranges from subclinical infection to severe gastroenteritis leading to life-threatening dehydration. After an incubation period of 1–3 days, the illness has an abrupt onset, with vomiting frequently preceding the onset of diarrhea. Up to one-third of patients may have a temperature of >39°C. The stools are characteristically loose and watery and only infrequently contain red or white cells. Gastrointestinal symptoms generally resolve in 3–7 days. Respiratory and neurologic features in children with rotavirus infection have been reported, but causal associations have not been proven. Moreover, rotavirus infection has been associated with a variety of other clinical conditions (e.g., sudden infant death syndrome, necrotizing enterocolitis, intussusception, Kawasaki disease, and type 1 diabetes), but no causal relationship has been confirmed with any of these syndromes. Rotavirus does not appear to be a major opportunistic pathogen in children with HIV infection. In severely immunodeficient children, the rotavirus can cause protracted diarrhea with prolonged viral excretion and, in rare instances, can disseminate systemically. Persons who are immunosuppressed for bone marrow transplantation also are at risk for severe or even fatal rotavirus disease. The different epidemiology of rotavirus disease and the greater prevalence of co-infection with other enteric pathogens, of comorbidities, and of malnutrition in developing countries may adversely affect the performance of oral rotavirus vaccines, as is the case with oral vaccines against poliomyelitis, cholera, and typhoid in these regions.
Table 4 — Table 209-2 Characteristics of Gastroenteritis Caused by Viral and Bacterial Agents¶
| FEATURE | VIRAL GASTROENTERITIS | BACTERIAL GASTROENTERITIS |
|---|---|---|
| Setting | Incidence similar in developing and developed countries | More common in settings with poor hygiene and sanitation |
| Infectious dose | Low (10–100 viral particles) for most agents | High (>105 bacteria) for Escherichia coli, Salmonella, Vibrio; medium (102–105 bacteria) for Campylobacter jejuni; low (10–100 bacteria) for Shigella |
| Seasonality | In temperate climates, winter seasonality for most agents; year-round occurrence in tropical areas | More common in summer or rainy months, particularly in developing countries with a high disease burden |
| Incubation period | 1–3 days for most agents; can be shorter for norovirus | 1–7 days for common agents (e.g., Campylobacter, E. coli, Shigella, Salmonella); a few hours for bacteria producing preformed toxins (e.g., Staphylococcus aureus, Bacillus cereus) |
| Reservoir | Primarily humans | Depending on bacterial species, human (e.g., Shigella, Salmonella), animal (e.g., Campylobacter, Salmonella, E. coli), and water (e.g., Vibrio) reservoirs exist |
| Fever | Common with rotavirus and norovirus; uncommon with other agents | Common with agents causing inflammatory diarrhea (e.g., Salmonella, Shigella) |
| Vomiting | Prominent and can be the only presenting feature, especially in children | Common with bacteria producing preformed toxins; less prominent in diarrhea due to other agents |
| Diarrhea | Common; nonbloody in almost all cases | Prominent and occasionally bloody with agents causing inflammatory diarrhea |
| Duration | 1–3 days for norovirus and sapovirus; 2–8 days for other viruses | 1–2 days for bacteria producing preformed toxins; 2–8 days for most other bacteria |
| Diagnosis | This is often a diagnosis of exclusion in clinical practice. Commercial enzyme immunoassays are available for detection of rotavirus and adenovirus, but identification of other agents is limited to research and public health laboratories. | Culture of stool specimens, sometimes on special media, can identify several pathogens. Molecular techniques are useful epidemiologic tools but are not routinely used in most laboratories. |
| Treatment | Supportive therapy to maintain adequate hydration and nutrition should be given. Antibiotics and antimotility agents are contraindicated. | Supportive hydration therapy is adequate for most patients. Antibiotics are recommended for patients with dysentery caused by Shigella or diarrhea caused by Vibrio cholerae and for some patients with Clostridium difficile colitis. |
4.2 Norovirus Clinical Manifestations¶
The disease is self-limited, and oral rehydration therapy is generally adequate. If severe dehydration develops, IV fluid therapy is indicated. No specific antiviral therapy is available.
5. DIFFERENTIAL DIAGNOSIS¶
As shown in Table 209-2, several features can help distinguish gastroenteritis caused by viruses from that caused by bacterial agents. However, the distinction based on clinical and epidemiologic parameters alone is often difficult, and laboratory tests are required to confirm the diagnosis. Fecal examination for leukocytes and blood is helpful in differential diagnosis. Diagnosis of viral gastroenteritis is often a diagnosis of exclusion in clinical practice.
5.1 Viral vs Bacterial Differentiation¶
Viral gastroenteritis is characterized by low infectious dose (10–100 viral particles), winter seasonality in temperate climates, fever common with rotavirus and norovirus, prominent vomiting especially in children, nonbloody diarrhea, and duration of 1–3 days for norovirus and sapovirus. Bacterial gastroenteritis is more common in settings with poor hygiene and sanitation, has a high infectious dose (>105 bacteria for E. coli, Salmonella, Vibrio), is more common in summer or rainy months, fever is common with agents causing inflammatory diarrhea, vomiting is common with bacteria producing preformed toxins, diarrhea is prominent and occasionally bloody, and duration is 1–2 days for bacteria producing preformed toxins or 2–8 days for most other bacteria.
6. INVESTIGATIONS & DIAGNOSIS¶
Diagnosis of rotavirus is difficult to distinguish clinically from that caused by other enteric viruses. Because large quantities of virus are shed in feces, the diagnosis can usually be confirmed by a wide variety of commercially available EIAs or by techniques for detecting viral RNA, such as gel electrophoresis, probe hybridization, or PCR. Cloning and sequencing of the genomes of Norwalk and several other human caliciviruses have allowed the development of assays based on polymerase chain reaction (PCR) for detection of virus in stool and vomitus. PCR-based detection assays for norovirus combined with those for multiple enteric pathogens are commercially available and are increasingly used in clinical settings. Virus-like particles (VLPs) produced by expression of capsid proteins in a recombinant baculovirus vector have been used to develop enzyme immunoassays (EIAs) for detection of virus in stool or a serologic response to a specific viral antigen. Commercial EIA kits for detection in stool have limited sensitivity and usefulness in clinical practice and are of greatest utility in outbreaks, in which many specimens are tested and only a few need be positive to identify norovirus as the cause.
6.1 Diagnostic Assays¶
Detection assays for viral gastroenteritis include EIA (commercial), RT-PCR, EM (electron microscopy), and PAGE (polyacrylamide gel electrophoresis). Commercial enzyme immunoassays are available for detection of rotavirus and adenovirus, but identification of other agents is limited to research and public health laboratories. PCR-based detection assays for norovirus combined with those for multiple enteric pathogens are commercially available and are increasingly used in clinical settings.
7. MANAGEMENT & TREATMENT¶
Rotavirus gastroenteritis can lead to severe dehydration; appropriate treatment should be instituted early. Standard oral rehydration therapy is successful for most children who can take fluids by mouth, but IV fluid replacement may be required for patients who are severely dehydrated or are unable to tolerate oral therapy because of frequent vomiting. The therapeutic roles of probiotics, bismuth subsalicylate, enkephalinase inhibitors, and nitazoxanide have been evaluated in clinical studies but are not clearly defined. Antibiotics and antimotility agents should be avoided. In immunocompromised children with chronic symptomatic rotavirus disease, orally administered immunoglobulins or colostrum may result in the resolution of symptoms, but the best choices regarding agents and their doses have not been well studied, and treatment decisions are often empirical. Infections with Norwalk and Related Human Caliciviruses: The disease is self-limited, and oral rehydration therapy is generally adequate. If severe dehydration develops, IV fluid therapy is indicated. No specific antiviral therapy is available.
7.1 Treatment Guidelines¶
Standard oral rehydration therapy is successful for most children who can take fluids by mouth. IV fluid replacement may be required for patients who are severely dehydrated or are unable to tolerate oral therapy because of frequent vomiting. Antibiotics and antimotility agents should be avoided. In immunocompromised children with chronic symptomatic rotavirus disease, orally administered immunoglobulins or colostrum may result in the resolution of symptoms, but the best choices regarding agents and their doses have not been well studied, and treatment decisions are often empirical.
7.2 Prevention Strategies¶
Epidemic prevention relies on situation-specific measures, such as control of contamination of food and water, exclusion of ill food handlers, and reduction of person-to-person spread through good personal hygiene and disinfection of contaminated fomites. The role of immunoprophylaxis is not clear, given the lack of long-term immunity from natural disease, but efforts to develop norovirus vaccines are ongoing. Vaccines based on VLPs are being tested in human volunteers. In a proof-of-concept trial, the efficacy of a monovalent GI.1 VLP vaccine was 47% among volunteers who received the vaccine intranasally and were then challenged with a homologous strain. In a second trial, norovirus disease severity was reduced in volunteers who received a bivalent G1.1/GII.4 VLP vaccine intramuscularly (with the GII.4 component including a consensus sequence from three different GII.4 strains) and were subsequently challenged with a GII.4 norovirus strain. Data from the first field efficacy study of this bivalent vaccine conducted in ~4700 healthy U.S. Navy recruits given 1 intramuscular injection of the bivalent vaccine were recently reported. While the primary endpoint of protection against homotypic infection could not be evaluated because only 6 total moderate/severe cases due to GI.1 or GII.4 norovirus strains occurred during the trial, the vaccine efficacy was 61.8% (95.01% confidence interval, 20.8–81.6%) for moderate/severe norovirus acute gastroenteritis due to any type. These initial data are encouraging; however, key issues to be further studied include the duration of protection and the level of heterotypic protection against antigenically distinct strains, particularly given the continuing and rapid natural evolution leading to the emergence of novel norovirus strains.
Table 5 — Rotavirus Vaccines¶
| Vaccine | Manufacturer | Recommendation | Efficacy |
|---|---|---|---|
| RotaTeq | Merck, United States | Recommended for routine immunization of all U.S. infants | 85–98% against severe rotavirus disease |
| Rotarix | GlaxoSmithKline, Belgium | Recommended for routine immunization of all U.S. infants | 85–98% against severe rotavirus disease |
| Rotavac | Bharat Biotech, India | Implemented in India’s routine childhood immunization program | 36–66% efficacy in low-income countries |
| Rotasiil | Serum Institute, India | Implemented in India’s routine childhood immunization program | 36–66% efficacy in low-income countries |
8. PROGNOSIS & COMPLICATIONS¶
Death is a rare outcome and usually results from severe dehydration in vulnerable persons (e.g., elderly patients with debilitating health conditions). Reinfections are common, but the severity of disease decreases with each repeat infection. Therefore, severe rotavirus infections are less common among older children and adults than among younger individuals. Nevertheless, rotavirus can cause illness in parents and caretakers of children with rotavirus diarrhea, immunocompromised persons, travelers, and elderly individuals and should be considered in the differential diagnosis of gastroenteritis among adults. Postmarketing surveillance has identified a low risk of intussusception in some high- and middle-income countries; however, the benefits of vaccination exceed the risks, and no changes in vaccine administration policy have been implemented. An intussusception risk has not been identified in several postmarketing evaluations in developing countries to date.
8.1 Mortality and Morbidity¶
Rotavirus is a leading cause of diarrheal death among children in the developing world. Large declines in severe morbidity and mortality from childhood diarrhea have been documented in many countries. Rates per 100,000 PY: 0 to <10, 50 to <100, ≥100. The highest mortality rates among children in sub-Saharan Africa and southern Asia.
8.2 Vaccine Safety¶
Postmarketing surveillance has identified a low risk of intussusception in some high- and middle-income countries; however, the benefits of vaccination exceed the risks, and no changes in vaccine administration policy have been implemented. An intussusception risk has not been identified in several postmarketing evaluations in developing countries to date.
9. SPECIAL CONSIDERATIONS¶
Rotavirus does not appear to be a major opportunistic pathogen in children with HIV infection. In severely immunodeficient children, the rotavirus can cause protracted diarrhea with prolonged viral excretion and, in rare instances, can disseminate systemically. Persons who are immunosuppressed for bone marrow transplantation also are at risk for severe or even fatal rotavirus disease. The different epidemiology of rotavirus disease and the greater prevalence of co-infection with other enteric pathogens, of comorbidities, and of malnutrition in developing countries may adversely affect the performance of oral rotavirus vaccines, as is the case with oral vaccines against poliomyelitis, cholera, and typhoid in these regions. Therefore, evaluation of the efficacy of rotavirus vaccines in resource-poor settings of Africa and Asia was specifically recommended, and these trials have now been completed. As anticipated, the efficacy of rotavirus vaccines was moderate (50–65%) in these settings when compared with that in industrialized countries. Despite modest efficacy, routine use of rotavirus vaccines in low-income African countries with a heavy disease burden has yielded substantial public health benefits.
9.1 Immunocompromised Hosts¶
Rotavirus does not appear to be a major opportunistic pathogen in children with HIV infection. In severely immunodeficient children, the rotavirus can cause protracted diarrhea with prolonged viral excretion and, in rare instances, can disseminate systemically. Persons who are immunosuppressed for bone marrow transplantation also are at risk for severe or even fatal rotavirus disease.
9.2 Resource-Poor Settings¶
The different epidemiology of rotavirus disease and the greater prevalence of co-infection with other enteric pathogens, of comorbidities, and of malnutrition in developing countries may adversely affect the performance of oral rotavirus vaccines, as is the case with oral vaccines against poliomyelitis, cholera, and typhoid in these regions. Therefore, evaluation of the efficacy of rotavirus vaccines in resource-poor settings of Africa and Asia was specifically recommended, and these trials have now been completed. As anticipated, the efficacy of rotavirus vaccines was moderate (50–65%) in these settings when compared with that in industrialized countries. Despite modest efficacy, routine use of rotavirus vaccines in low-income African countries with a heavy disease burden has yielded substantial public health benefits.
10. KEY PEARLS & CLINICAL TRAPS¶
Viral gastroenteritis is a leading cause of death among children in developing countries, accounting for an estimated 0.5 million deaths each year, and is responsible for up to 6–8% of all hospitalizations among children in industrialized countries, including the United States. Norovirus is the most common cause of medically attended gastroenteritis in young children in the US and the leading cause of epidemics worldwide (~50% of outbreaks). Rotavirus is the leading cause of severe dehydrating diarrhea in children 70–80% decline in hospitalizations in the US. Viral gastroenteritis is typically a diagnosis of exclusion; differentiation from bacterial causes relies on stool leukocytes/blood (absent in viral) and incubation period. Treatment is supportive (oral rehydration); antibiotics and antimotility agents are contraindicated. Rotavirus vaccines (RotaTeq, Rotarix) are recommended for routine immunization of US infants; herd protection reduces disease in unvaccinated contacts. Intussusception is a rare but serious complication associated with rotavirus vaccination in some high- and middle-income countries, though benefits exceed risks.
10.1 Clinical Pearls¶
Viral gastroenteritis is a leading cause of death among children in developing countries, accounting for an estimated 0.5 million deaths each year, and is responsible for up to 6–8% of all hospitalizations among children in industrialized countries, including the United States. Norovirus is the most common cause of medically attended gastroenteritis in young children in the US and the leading cause of epidemics worldwide (~50% of outbreaks). Rotavirus is the leading cause of severe dehydrating diarrhea in children 70–80% decline in hospitalizations in the US. Viral gastroenteritis is typically a diagnosis of exclusion; differentiation from bacterial causes relies on stool leukocytes/blood (absent in viral) and incubation period. Treatment is supportive (oral rehydration); antibiotics and antimotility agents are contraindicated. Rotavirus vaccines (RotaTeq, Rotarix) are recommended for routine immunization of US infants; herd protection reduces disease in unvaccinated contacts. Intussusception is a rare but serious complication associated with rotavirus vaccination in some high- and middle-income countries, though benefits exceed risks.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
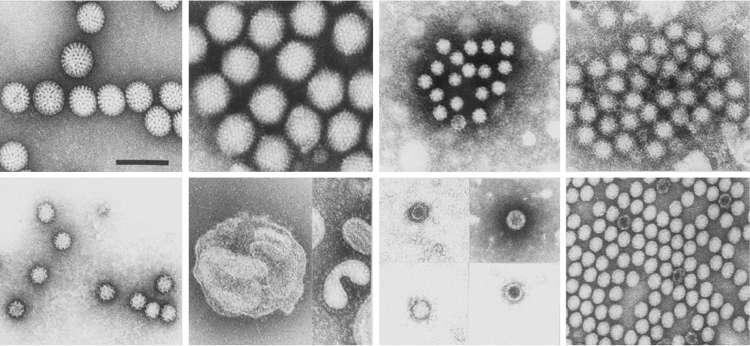
Caption: FIGURE 209-1 Viral agents of gastroenteritis. NV, norovirus; SV, sapovirus. — Figure 209-1: Diagram of viral agents of gastroenteritis. The image displays various viral families and genera associated with human gastroenteritis, including Rotavirus (Reoviridae), Norovirus and Sapovirus (Caliciviridae), Astrovirus (Astroviridae), and Adenovirus (Adenoviridae). NV indicates norovirus; SV indicates sapovirus.
Figure 2¶

Caption: FIGURE 209-2 Rotavirus mortality rates by country, per 100,000 children <5 years of age. in children <5 years of age, 2000–2013. Clin Infect Dis 62:S96, 2016.) — Figure 209-2: Map showing rotavirus mortality rates by country per 100,000 children <5 years of age. The data illustrates the highest mortality rates in sub-Saharan Africa and southern Asia, with rates decreasing in industrialized nations following vaccination programs.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.