Syncope¶
Chapter 23 | Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Syncope is a transient, self-limited loss of consciousness (TLOC) due to acute global impairment of cerebral blood flow.
- Three main categories: Neurally mediated syncope, Orthostatic hypotension, and Cardiac syncope.
- High-risk features for hospitalization include chest pain, structural heart disease, prolonged QT interval, and history of ventricular arrhythmias (Table 23-1).
- Neurally mediated syncope is the most common cause in young subjects; cardiovascular disease is the next most common cause in older patients.
- Orthostatic hypotension is defined as a reduction in systolic blood pressure of at least 20 mmHg or diastolic blood pressure of at least 10 mmHg after 3 min of standing.
- Management of neurally mediated syncope includes reassurance, education, avoidance of triggers, fluid/salt, and isometric counterpressure maneuvers.
- Cardiac syncope requires evaluation for arrhythmias and structural disease; treatment depends on the underlying disorder (pacing, ablation, drugs).
- Orthostatic hypotension treatment involves removing reversible causes, non-pharmacologic measures, and pharmacologic agents like fludrocortisone or midodrine.
- EEG flattening during syncope is a marker of more severe cerebral hypoperfusion; myoclonic movements do not indicate seizure.
- Fecal incontinence is very rare with syncope, whereas urinary incontinence may occur.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- Classification of Neurally Mediated Syncope
- 4. CLINICAL FEATURES
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 7. MANAGEMENT & TREATMENT
- Cardiac Syncope Treatment
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | A |
| 2 | 🖼 Figure | The baroreflex |
1. DEFINITION & OVERVIEW¶
- Syncope is a transient, self-limited loss of consciousness due to acute global impairment of cerebral blood flow.
- The onset is rapid, duration brief, and recovery spontaneous and complete.
- Other causes of transient loss of consciousness need to be distinguished from syncope; these include seizures, vertebrobasilar ischemia, hypoxemia, and hypoglycemia.
- A syncopal prodrome (presyncope) is common, although loss of consciousness may occur without any warning symptoms.
- Typical presyncopal symptoms include lightheadedness or faintness, dizziness, weakness, fatigue, and visual and auditory disturbances.
- The causes of syncope can be divided into three general categories: (1) neurally mediated syncope (also called reflex or vasovagal syncope), (2) orthostatic hypotension, and (3) cardiac syncope.
- The clinical features, underlying pathophysiologic mechanisms, therapeutic interventions, and prognoses differ markedly among these three causes.
- Syncope is a form of transient loss of consciousness (TLOC) that is a consequence of global cerebral hypoperfusion.
- It represents a failure of cerebral blood flow autoregulatory mechanisms.
- Myogenic factors, local metabolites, and to a lesser extent autonomic neurovascular control are responsible for the autoregulation of cerebral blood flow.
- The latency of the autoregulatory response is 5–10 s.
- Typically, cerebral blood flow ranges from 50–60 mL/min per 100 g brain tissue and remains relatively constant over perfusion pressures ranging from 50–150 mmHg.
- Cessation of blood flow for 6–8 s will result in loss of consciousness, while impairment of consciousness ensues when blood flow decreases to 25 mL/min per 100 g brain tissue.
- From the clinical standpoint, a fall in systemic systolic blood pressure to ~50 mmHg or lower will usually result in syncope.
- A decrease in cardiac output and/or systemic vascular resistance—the determinants of blood pressure—thus underlies the pathophysiology of syncope.
- Common causes of impaired cardiac output include decreased effective circulating blood volume, increased thoracic pressure, massive pulmonary embolus, cardiac brady- and tachyarrhythmias, valvular heart disease, and myocardial dysfunction.
- Systemic vascular resistance may be decreased by central and peripheral autonomic nervous system diseases, sympatholytic medications, and transiently during neurally mediated syncope.
- Increased cerebral vascular resistance, most frequently due to hypocarbia induced by hyperventilation, may also contribute to the pathophysiology of syncope.
2. EPIDEMIOLOGY¶
- Syncope is a common presenting problem, accounting for ~3% of all emergency department (ED) visits and 1% of all hospital admissions.
- The annual cost for syncope-related hospitalization in the United States is ~$2.4 billion.
- Syncope has a lifetime cumulative incidence of up to 40% in the general population.
- A bimodal age distribution exists; the peak incidence in the young occurs between ages 10 and 30 years, with a median peak around 15 years.
- Neurally mediated syncope is the etiology in the vast majority of these cases.
- In older adults, there is a sharp rise in the incidence of syncope after 70 years of age.
- In population-based studies, neurally mediated syncope is the most common cause of syncope.
- The incidence is higher in women than men.
- In young subjects, there is often a family history in first-degree relatives.
- Cardiovascular disease due to structural disease or arrhythmias is the next most common cause in most series, particularly in ED settings and in older patients.
- Orthostatic hypotension also increases in prevalence with age because of the reduced baroreflex responsiveness, decreased cardiac compliance, and attenuation of the vestibulosympathetic reflex associated with aging.
- Other contributors are reduced fluid intake and vasoactive medications, also more likely in this age group.
- In the elderly, orthostatic hypotension is more common in institutionalized than community-dwelling individuals, most likely explained by a greater prevalence of predisposing neurologic disorders, physiologic impairment, and vasoactive medication use among institutionalized patients.
- Syncope of noncardiac and unexplained origin in younger individuals has an excellent prognosis; life expectancy is unaffected.
- By contrast, syncope due to a cardiac cause, either structural heart disease or a primary arrhythmic disorder, is associated with an increased risk of sudden cardiac death and mortality from other causes.
- Similarly, the mortality rate is increased in individuals with syncope due to orthostatic hypotension related to age and the associated comorbid conditions (Table 23-1).
- The likelihood of hospitalization and mortality risk are higher in older adults.
Table 1 — Table 23-1 High-Risk Features Indicating Hospitalization or Intensive Evaluation of Syncope¶
| Feature |
|---|
| Chest pain suggesting coronary ischemia |
| Features of congestive heart failure |
| Moderate or severe valvular disease |
| Moderate or severe structural cardiac disease |
| Electrocardiographic features of ischemia |
| History of ventricular arrhythmias |
| Prolonged QT interval (>500 ms) |
| Repetitive sinoatrial block or sinus pauses |
| Persistent sinus bradycardia |
| Bi- or trifascicular block or intraventricular conduction delay with QRS duration ≥120 ms |
| Atrial fibrillation |
| Nonsustained ventricular tachycardia |
| Family history of sudden death |
| Preexcitation syndromes |
| Brugada pattern on electrocardiogram |
| Palpitations at time of syncope |
| Syncope at rest or during exercise |
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- The upright posture imposes a unique physiologic stress upon humans; most, although not all, syncopal episodes occur from a standing position.
- Standing results in pooling of 500–1000 mL of blood in the lower extremities, buttocks, and splanchnic circulation.
- The dependent pooling leads to a decrease in venous return to the heart and reduced ventricular filling that result in diminished cardiac output and blood pressure.
- These hemodynamic changes provoke a compensatory reflex response, initiated by the baroreceptors in the carotid sinus and aortic arch, resulting in increased sympathetic outflow and decreased vagal nerve activity.
- The reflex increases peripheral resistance, venous return to the heart, and cardiac output and thus limits the fall in blood pressure.
- If this response fails, as is the case chronically in orthostatic hypotension and transiently in neurally mediated syncope, hypotension and cerebral hypoperfusion occur.
- In order to develop neurally mediated syncope, a functioning autonomic nervous system is necessary, in contrast to syncope resulting from autonomic failure (discussed below).
- Neurally mediated syncope may be subdivided based on the afferent pathway and provocative trigger.
- Vasovagal syncope (the common faint) is provoked by intense emotion, pain, and/or orthostatic stress.
- Situational reflex syncopes have specific localized stimuli that provoke the reflex vasodilation and bradycardia that leads to syncope.
- The afferent trigger may originate in the pulmonary system, gastrointestinal system, urogenital system, heart, and carotid sinus in the carotid artery.
- Neurally mediated syncope may be subdivided based on the predominant efferent pathway.
- Vasodepressor syncope describes predominantly efferent, sympathetic, vasoconstrictor failure.
- Cardioinhibitory syncope describes syncope predominantly associated with bradycardia or asystole due to increased vagal outflow.
- Mixed response syncope describes syncope in which there are both vagal and sympathetic reflex changes.
- Features of Neurally Mediated Syncope include symptoms of orthostatic intolerance such as dizziness, lightheadedness, and fatigue.
- Premonitory features of autonomic activation may be present in patients with neurally mediated syncope. These include diaphoresis, pallor, palpitations, nausea, hyperventilation, and yawning.
- During the syncopal event, proximal and distal myoclonus (typically arrhythmic) may occur, raising the possibility of a seizure.
- The eyes typically remain open and usually deviate upward.
- Pupils are usually dilated.
- Roving eye movements may occur.
- Grunting, moaning, snorting, and stertorous breathing may be present.
- Urinary incontinence may occur.
- Fecal incontinence is very rare, however.
- Postictal confusion is also rare, although visual and auditory hallucinations and near-death and out-of-body experiences are sometimes reported.
- Although some predisposing factors and provocative stimuli are well established (for example, motionless upright posture, warm ambient temperature, intravascular volume depletion, alcohol ingestion, hypoxemia, anemia, pain, the sight of blood, venipuncture, and intense emotion), the underlying basis for the widely different thresholds for syncope among individuals exposed to the same provocative stimulus is not known.
- A genetic basis for neurally mediated syncope may exist.
- Several studies have reported an increased incidence of syncope in first-degree relatives of fainters, and some candidate genes have been identified with sex-specific associations.
- It is likely that environmental, social, and cultural factors play a large role.
- Orthostatic hypotension, defined as a reduction in systolic blood pressure of at least 20 mmHg or diastolic blood pressure of at least 10 mmHg after 3 min of standing or head-up tilt on a tilt table, is a manifestation of sympathetic vasoconstrictor (autonomic) failure.
- In many (but not all) cases, there is no compensatory increase in heart rate despite hypotension; with partial autonomic failure, heart rate may increase to some degree but is insufficient to maintain cardiac output.
- A variant of orthostatic hypotension is 'delayed' orthostatic hypotension, which occurs beyond 3 min of standing; this may reflect a mild or early form of sympathetic adrenergic dysfunction.
- In some cases, orthostatic hypotension can occur within 15 s of standing with full resolution within 45 s (so-called initial orthostatic hypotension), a finding that may reflect a transient mismatch between cardiac output and peripheral vascular resistance and does not represent autonomic failure.
- Causes of neurogenic orthostatic hypotension include central and peripheral autonomic nervous system dysfunction.
- Autonomic dysfunction of other organ systems (including the bladder, bowels, sexual organs, and sudomotor system) of varying severity frequently accompanies orthostatic hypotension in these disorders.
- The primary autonomic degenerative disorders are multiple system atrophy (Shy-Drager syndrome), Parkinson's disease, dementia with Lewy bodies, and pure autonomic failure.
- These are often grouped together as 'synucleinopathies' due to the presence of α-synuclein, a protein that aggregates predominantly in the cytoplasm of neurons in the Lewy body disorders and in the glia in multiple system atrophy.
- Peripheral autonomic dysfunction may also accompany small-fiber peripheral neuropathies such as those associated with diabetes mellitus, acquired and hereditary amyloidosis, immune-mediated neuropathies, and hereditary sensory and autonomic neuropathies (HSAN; particularly HSAN type III, familial dysautonomia).
- Less frequently, orthostatic hypotension is associated with the peripheral neuropathies that accompany vitamin B deficiency, neurotoxin exposure, HIV and other infections, and porphyria.
- Patients with autonomic failure and the elderly are susceptible to falls in blood pressure associated with meals.
- The magnitude of the blood pressure fall is exacerbated by large meals, meals high in carbohydrate, and alcohol intake.
- The mechanism of postprandial hypotension, and resultant syncope, is not fully elucidated.
- Orthostatic hypotension is often iatrogenic.
- Drugs from several classes may lower peripheral resistance (e.g., α-adrenoreceptor antagonists used to treat hypertension and prostatic hypertrophy; diuretics, nitrates and other venodilators and vasodilators; other antihypertensive agents of several classes; tricyclic agents and phenothiazines).
- Iatrogenic volume depletion due to diuresis and volume depletion due to medical causes (hemorrhage, vomiting, diarrhea, or decreased fluid intake) may also result in decreased effective circulatory volume, orthostatic hypotension, and syncope.
- Cardiac (or cardiovascular) syncope is caused by arrhythmias and structural heart disease.
- These may occur in combination because structural disease renders the heart more vulnerable to abnormal electrical activity.
- Structural heart disease (e.g., valvular disease, myocardial ischemia, hypertrophic and other cardiomyopathies, cardiac masses such as atrial myxoma, and pericardial effusions) may lead to syncope by compromising cardiac output.
- Structural disease may also contribute to other pathophysiologic mechanisms of syncope.
- For example, cardiac structural disease may predispose to arrhythmogenesis; aggressive treatment of cardiac failure with diuretics and/or vasodilators may lead to orthostatic hypotension; and inappropriate reflex vasodilation may occur with structural disorders such as aortic stenosis and hypertrophic cardiomyopathy, possibly provoked by increased ventricular contractility.
- Two patterns of electroencephalographic (EEG) changes occur in syncopal subjects.
- The first is a 'slow-flat-slow' pattern in which normal background activity is replaced with high-amplitude slow delta waves.
- This is followed by sudden flattening of the EEG—a cessation or attenuation of cortical activity—followed by the return of slow waves, and then normal activity.
- A second pattern, the 'slow pattern,' is characterized by increasing and decreasing slow wave activity only.
- The EEG flattening that occurs in the slow-flat-slow pattern is a marker of more severe cerebral hypoperfusion.
- Despite the presence of myoclonic movements and other motor activity during some syncopal events, EEG seizure discharges are not detected.
Classification of Neurally Mediated Syncope¶
- Neurally mediated syncope comprises a heterogeneous group of disorders that are characterized by a transient change in the reflexes responsible for maintaining cardiovascular homeostasis.
- Episodic vasodilation (or loss of vasoconstrictor tone), decreased cardiac output, and bradycardia occur in varying combinations, resulting in temporary failure of blood pressure control.
- In contrast, in patients with orthostatic hypotension due to autonomic failure, these cardiovascular homeostatic reflexes are chronically impaired.
- Cardiac syncope may be due to arrhythmias or structural cardiac diseases that cause a decrease in cardiac output.
- Neurally mediated syncope may be subdivided based on the afferent pathway and provocative trigger.
- Vasovagal syncope (the common faint) is provoked by intense emotion, pain, and/or orthostatic stress.
- Situational reflex syncopes have specific localized stimuli that provoke the reflex vasodilation and bradycardia that leads to syncope.
- The afferent trigger may originate in the pulmonary system, gastrointestinal system, urogenital system, heart, and carotid sinus in the carotid artery.
- Neurally mediated syncope may be subdivided based on the predominant efferent pathway.
- Vasodepressor syncope describes predominantly efferent, sympathetic, vasoconstrictor failure.
- Cardioinhibitory syncope describes syncope predominantly associated with bradycardia or asystole due to increased vagal outflow.
- Mixed response syncope describes syncope in which there are both vagal and sympathetic reflex changes.
Table 2 — Table 23-2 Causes of Syncope¶
| Category | Subcategory | Specific Causes |
|---|---|---|
| A. Neurally Mediated Syncope | Vasovagal syncope | Provoked fear, pain, anxiety, intense emotion, sight of blood, unpleasant sights and odors, orthostatic stress |
| Situational reflex syncope | Pulmonary | Cough syncope, wind instrument player's syncope, weightlifter's syncope, 'mess trick' and 'fainting lark,' sneeze syncope, airway instrumentation |
| Urogenital | Postmicturition syncope, urogenital tract instrumentation, prostatic massage | |
| Gastrointestinal | Swallow syncope, glossopharyngeal neuralgia, esophageal stimulation, gastrointestinal tract instrumentation, rectal examination, defecation syncope | |
| Cardiac | Bezold-Jarisch reflex, cardiac outflow obstruction | |
| Carotid sinus | Carotid sinus sensitivity, carotid sinus massage | |
| Ocular | Ocular pressure, ocular examination, ocular surgery | |
| B. Orthostatic Hypotension | Primary autonomic failure due to idiopathic central and peripheral neurodegenerative diseases—the 'synucleinopathies' | Lewy body diseases, Parkinson's disease, Lewy body dementia, Pure autonomic failure, Multiple system atrophy (Shy-Drager syndrome) |
| Secondary autonomic failure due to autonomic peripheral neuropathies | Diabetes, Hereditary amyloidosis (familial amyloid polyneuropathy), Primary amyloidosis (AL amyloidosis; immunoglobulin light chain associated), Hereditary sensory and autonomic neuropathies (HSAN) (especially type III—familial dysautonomia), Idiopathic immune-mediated autonomic neuropathy, Autoimmune autonomic ganglionopathy, Sjögren's syndrome, Paraneoplastic autonomic neuropathy, HIV neuropathy, Postprandial hypotension, Iatrogenic (drug-induced), Volume depletion | |
| C. Cardiac Syncope | Arrhythmias | Sinus node dysfunction, Atrioventricular dysfunction, Supraventricular tachycardias, Ventricular tachycardias, Inherited channelopathies |
| Cardiac structural disease | Valvular disease, Myocardial ischemia, Obstructive and other cardiomyopathies, Atrial myxoma, Pericardial effusions and tamponade |
4. CLINICAL FEATURES¶
- Characteristic symptoms of orthostatic hypotension include light-headedness, dizziness, and presyncope (near-faintness) occurring in response to sudden postural change.
- However, symptoms may be absent or nonspecific such as generalized weakness, fatigue, cognitive slowing, leg buckling, or headache.
- Visual blurring may occur, likely due to retinal or occipital lobe ischemia.
- Neck pain, typically in the suboccipital, posterior cervical, and shoulder region (the 'coat-hanger headache'), most likely due to neck muscle ischemia, may be the only symptom.
- Patients may report orthostatic dyspnea (thought to reflect ventilation-perfusion mismatch due to inadequate perfusion of ventilated lung apices) or angina (attributed to impaired myocardial perfusion even with normal coronary arteries).
- Symptoms may be exacerbated by exertion, prolonged standing, increased ambient temperature, or meals.
- Syncope is usually preceded by warning symptoms, but may occur suddenly, suggesting the possibility of a seizure or cardiac cause.
- Some patients have profound decreases in blood pressure, sometimes without symptoms but placing them at risk for falls and injuries if the autoregulatory threshold is crossed with ensuing cerebral hypoperfusion.
- Supine hypertension is common in patients with orthostatic hypotension due to autonomic failure, affecting >50% of patients in some series.
- Orthostatic hypotension may present after initiation of therapy for hypertension, and supine hypertension may follow treatment of orthostatic hypotension.
- However, in other cases, the association of the two conditions is unrelated to therapy; it may in part be explained by baroreflex dysfunction in the presence of residual sympathetic outflow, particularly in patients with central autonomic degeneration.
- Patients with autonomic failure and the elderly are susceptible to falls in blood pressure associated with meals.
- The magnitude of the blood pressure fall is exacerbated by large meals, meals high in carbohydrate, and alcohol intake.
- The mechanism of postprandial hypotension, and resultant syncope, is not fully elucidated.
- Orthostatic hypotension is often iatrogenic.
- Drugs from several classes may lower peripheral resistance (e.g., α-adrenoreceptor antagonists used to treat hypertension and prostatic hypertrophy; diuretics, nitrates and other venodilators and vasodilators; other antihypertensive agents of several classes; tricyclic agents and phenothiazines).
- Iatrogenic volume depletion due to diuresis and volume depletion due to medical causes (hemorrhage, vomiting, diarrhea, or decreased fluid intake) may also result in decreased effective circulatory volume, orthostatic hypotension, and syncope.
5. DIFFERENTIAL DIAGNOSIS¶
- Syncope is easily diagnosed when the characteristic features are present; however, several disorders with real or apparent transient loss of consciousness may create diagnostic confusion.
- Generalized and partial seizures may be confused with syncope; however, there are a number of differentiating features.
- Whereas tonic-clonic movements are the hallmark of a generalized seizure, myoclonic and other movements also may occur in up to 90% of syncopal episodes.
- Myoclonic jerks associated with syncope may be multifocal or generalized. They are typically arrhythmic and of short duration (5 min and is associated with prolonged postictal drowsiness and disorientation, whereas reorientation occurs almost immediately after a syncopal event.
- Muscle aches may occur after both syncope and seizures, although they tend to last longer and be more severe following a seizure.
- Seizures, unlike syncope, are rarely provoked by emotions or pain.
- Incontinence of urine may occur with both seizures and syncope; however, fecal incontinence occurs only very rarely with syncope.
- Autonomic manifestations of seizures (autonomic epilepsy) may provide a more difficult diagnostic challenge.
- Autonomic seizures have cardiovascular, gastrointestinal, pulmonary, urogenital, pupillary, and cutaneous manifestations that are similar to the premonitory features of syncope.
- Furthermore, the cardiovascular manifestations of autonomic epilepsy include clinically significant tachycardias and bradycardias that may be of sufficient magnitude to cause loss of consciousness.
- The presence of accompanying non-autonomic auras may help differentiate these episodes from syncope.
- Hypoglycemia may cause transient loss of consciousness, typically in individuals with type 1 or type 2 diabetes treated with insulin.
- The clinical features associated with impending or actual hypoglycemia include tremor, palpitations, anxiety, diaphoresis, hunger, and paresthesias.
- These symptoms are due to autonomic activation to counter the falling blood glucose.
- Hunger, in particular, is not a typical premonitory feature of syncope.
- Hypoglycemia also impairs neuronal function, leading to fatigue, weakness, dizziness, and cognitive and behavioral symptoms.
- Diagnostic difficulties may occur in individuals in strict glycemic control; repeated hypoglycemia impairs the counterregulatory response and leads to a loss of the characteristic warning symptoms that are the hallmark of hypoglycemia.
- Patients with cataplexy experience an abrupt partial or complete loss of muscular tone triggered by strong emotions, typically anger or laughter.
- Unlike syncope, consciousness is maintained throughout the attacks, which typically last between 30 s and 2 min.
- There are no premonitory symptoms.
- Cataplexy occurs in 60–75% of patients with narcolepsy.
- Apparent loss of consciousness can be a manifestation of psychiatric disorders such as generalized anxiety, panic disorders, major depression, and somatization disorder.
- These possibilities should be considered in individuals who faint frequently without prodromal symptoms.
- Such patients are rarely injured despite numerous falls.
- There are no clinically significant hemodynamic changes concurrent with these episodes.
- In contrast, transient loss of consciousness due to vasovagal syncope precipitated by fear, stress, anxiety, and emotional distress is accompanied by hypotension and sometimes bradycardia.
- The clinical interview and interrogation of eyewitnesses (and ancillary cellphone video of the spell, when available) usually allow differentiation of syncope from falls due to vestibular dysfunction, cerebellar disease, extrapyramidal system dysfunction, and other gait disorders.
- A diagnosis of syncope can be particularly challenging in patients with dementia who experience repeated falls and are unable to provide a clear history of the episodes.
- If the fall is accompanied by head trauma, a postconcussive syndrome, amnesia for the precipitating events, and/or a loss or alteration of consciousness, this may also contribute to diagnostic difficulty.
6. INVESTIGATIONS & DIAGNOSIS¶
- ECG monitoring is indicated for patients with a high pretest probability of arrhythmia causing syncope.
- Patients should be monitored in the hospital if the likelihood of a life-threatening arrhythmia is high, e.g., patients with severe coronary artery or structural heart disease, nonsustained ventricular tachycardia, supraventricular tachycardia, paroxysmal atrial fibrillation, trifascicular heart block, prolonged QT interval, Brugada syndrome ECG pattern, syncope during exertion, syncope while seated or supine, and family history of sudden cardiac death (Table 23-1).
- Continuous ambulatory electrocardiographic (Holter) monitoring is recommended for patients who experience frequent syncopal episodes (e.g., daily or almost daily), whereas loop recorders are indicated for patients with infrequent episodes.
- Autonomic testing, including tilt-table testing, can be performed in specialized centers.
- Autonomic testing is helpful to uncover objective evidence of autonomic failure and also to demonstrate a predisposition to neurally mediated syncope.
- Autonomic testing includes assessments of parasympathetic autonomic nervous system function (e.g., heart rate variability to deep respiration and a Valsalva maneuver), sympathetic cholinergic function (e.g., thermoregulatory sweat response and quantitative sudomotor axon reflex test), and sympathetic adrenergic function (e.g., blood pressure response to a Valsalva maneuver and a tilt-table test with beat-to-beat blood pressure measurement).
- The hemodynamic abnormalities demonstrated on the tilt-table test may be useful in distinguishing orthostatic hypotension due to autonomic failure from the hypotensive bradycardic response of neurally mediated syncope.
- Similarly, the tilt-table test may help identify patients with syncope due to immediate or delayed orthostatic hypotension.
- Carotid sinus massage should be considered in patients with symptoms suggestive of carotid sinus syncope and in patients >40 years with recurrent syncope of unknown etiology.
- This test should ideally be carried out under continuous ECG and blood pressure monitoring and should be avoided in patients with carotid bruits, possible or known plaques, or stenosis.
- Cardiac evaluation includes echocardiography and stress testing for structural disease and arrhythmia evaluation.
- Imaging (CT/MRI) may be indicated for structural disease or embolus evaluation.
7. MANAGEMENT & TREATMENT¶
- Reassurance, education, avoidance of provocative stimuli, and plasma volume expansion with fluid and salt are the cornerstones of the management of neurally mediated syncope.
- Isometric counterpressure maneuvers of the limbs (tensing of the abdominal and leg muscles, handgrip and arm tensing, and leg crossing) may raise blood pressure by increasing central blood volume and cardiac output.
- Of these, abdominal and leg muscle tensing is the most effective.
- By maintaining pressure in the autoregulatory zone, these maneuvers, which may be particularly helpful in patients with a long prodrome, avoid or delay the onset of syncope.
- A randomized controlled trial supports this intervention.
- Fludrocortisone, vasoconstricting agents, and β-adrenoreceptor antagonists are widely used by experts to treat refractory patients.
- Of these, only midodrine has been shown to be effective in international, multicenter randomized controlled trials.
- Because vasodilation, decreased central blood volume, decreased stroke volume, and cardiac output are the dominant pathophysiologic syncopal mechanisms in most patients, use of a cardiac pacemaker is rarely beneficial.
- In patients with a cardioinhibitory syncope response during tilt-table testing, however, recent sham-controlled randomized clinical trial data have shown that a dual-chamber pacemaker with a closed-loop stimulation algorithm can decrease syncope recurrence.
- These studies restricted enrollment to older patients (>40 years) with frequent recurrence of syncope and a cardioinhibitory response on tilt-table test.
- In these patients, dual-chamber pacing may be helpful, although this continues to be an area of uncertainty.
- The first step is to remove reversible causes—usually vasoactive medications.
- Next, nonpharmacologic interventions should be introduced.
- These include patient education regarding staged moves from supine to upright; warnings about the hypotensive effects of large meals; instructions about the isometric counterpressure maneuvers that increase intravascular pressure; and raising the head of the bed to reduce supine hypertension and nocturnal diuresis.
- Intravascular volume should be expanded by increasing dietary fluid and salt.
- The rapid ingestion of 500 mL of plain water can often effect a short-term pressor response in these patients.
- If these nonpharmacologic measures fail, pharmacologic intervention with fludrocortisone acetate and vasoconstricting agents such as midodrine or l-dihydroxyphenylserine (droxidopa) should be introduced.
- Some patients with intractable symptoms require additional therapy with supplementary agents that include pyridostigmine, atomoxetine, yohimbine, octreotide, desmopressin acetate (DDAVP), and erythropoietin.
- Treatment of cardiac disease depends on the underlying disorder.
- Therapies for arrhythmias consist of cardiac pacing for bradycardia, including sinus node disease and AV block, and ablation, antiarrhythmic drugs, and cardioverter-defibrillators for atrial and ventricular tachyarrhythmias.
- These disorders are best managed by physicians with specialized skills in this area.
Cardiac Syncope Treatment¶
- Treatment of cardiac disease depends on the underlying disorder.
- Therapies for arrhythmias consist of cardiac pacing for bradycardia, including sinus node disease and AV block, and ablation, antiarrhythmic drugs, and cardioverter-defibrillators for atrial and ventricular tachyarrhythmias.
- These disorders are best managed by physicians with specialized skills in this area.
8. PROGNOSIS & COMPLICATIONS¶
- Syncope of noncardiac and unexplained origin in younger individuals has an excellent prognosis; life expectancy is unaffected.
- By contrast, syncope due to a cardiac cause, either structural heart disease or a primary arrhythmic disorder, is associated with an increased risk of sudden cardiac death and mortality from other causes.
- Similarly, the mortality rate is increased in individuals with syncope due to orthostatic hypotension related to age and the associated comorbid conditions (Table 23-1).
- The likelihood of hospitalization and mortality risk are higher in older adults.
9. SPECIAL CONSIDERATIONS¶
- In the elderly, orthostatic hypotension is more common in institutionalized than community-dwelling individuals, most likely explained by a greater prevalence of predisposing neurologic disorders, physiologic impairment, and vasoactive medication use among institutionalized patients.
- Orthostatic hypotension is often iatrogenic.
- Drugs from several classes may lower peripheral resistance (e.g., α-adrenoreceptor antagonists used to treat hypertension and prostatic hypertrophy; diuretics, nitrates and other venodilators and vasodilators; other antihypertensive agents of several classes; tricyclic agents and phenothiazines).
- Iatrogenic volume depletion due to diuresis and volume depletion due to medical causes (hemorrhage, vomiting, diarrhea, or decreased fluid intake) may also result in decreased effective circulatory volume, orthostatic hypotension, and syncope.
10. KEY PEARLS & CLINICAL TRAPS¶
- High-risk features for hospitalization include chest pain, structural heart disease, prolonged QT interval, and history of ventricular arrhythmias (Table 23-1).
- EEG flattening during syncope is a marker of more severe cerebral hypoperfusion.
- Myoclonic movements do not indicate seizure.
- Fecal incontinence is very rare with syncope.
- Hunger is not a typical premonitory feature of syncope.
- Supine hypertension is common in autonomic failure.
- Carotid sinus massage should be avoided in patients with carotid bruits, possible or known plaques, or stenosis.
- Midodrine has been shown to be effective in international, multicenter randomized controlled trials.
- Pacemaker is rarely beneficial for vasodepressor syncope.
- Dual-chamber pacemaker with closed-loop stimulation algorithm may help in cardioinhibitory response in older patients with frequent recurrence.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
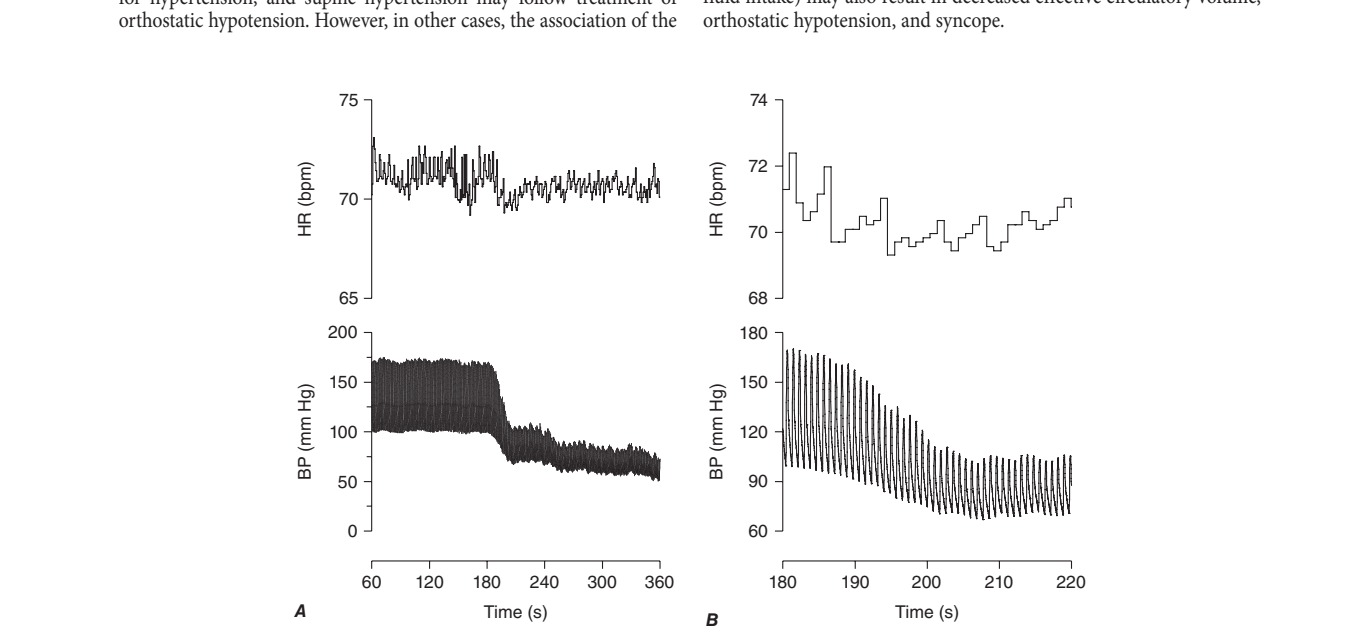
Caption: FIGURE 23-3 A. The gradual fall in blood pressure without a compensatory heart rate Blood pressure and heart rate are shown >5 min (from 60 to 360 s) of an upright tilt on a tilt BP, blood pressure; bpm, beats per minute; HR, heart rate. — FIGURE 23-1 The baroreflex. A decrease in arterial pressure unloads the baroreceptors—the terminals of afferent fibers of the glossopharyngeal and vagus nerves—that are situated in the carotid sinus and aortic arch. This leads to a reduction in the afferent impulses that are relayed from these mechanoreceptors through the glossopharyngeal and vagus nerves to the nucleus of the tractus solitarius (NTS) in the dorsomedial medulla. The reduced baroreceptor afferent activity produces a decrease in vagal nerve input to the sinus node that is mediated via connections of the NTS to the nucleus ambiguus (NA). There is an increase in sympathetic efferent activity that is mediated by the NTS projections to the caudal ventrolateral medulla (CVLM) (an excitatory pathway) and from there to the rostral ventrolateral medulla (RVLM) (an inhibitory pathway). The activation of RVLM presympathetic neurons in response to hypotension is thus predominantly due to disinhibition. In response to a sustained fall in blood pressure, vasopressin release is mediated by projections from the A1 noradrenergic cell group in the ventrolateral medulla. This projection activates vasopressin-synthesizing neurons in the magnocellular portion of the paraventricular nucleus (PVN) and the supraoptic nucleus (SON) of the hypothalamus. Blue denotes sympathetic neurons, and green denotes parasympathetic neurons.
Figure 2¶
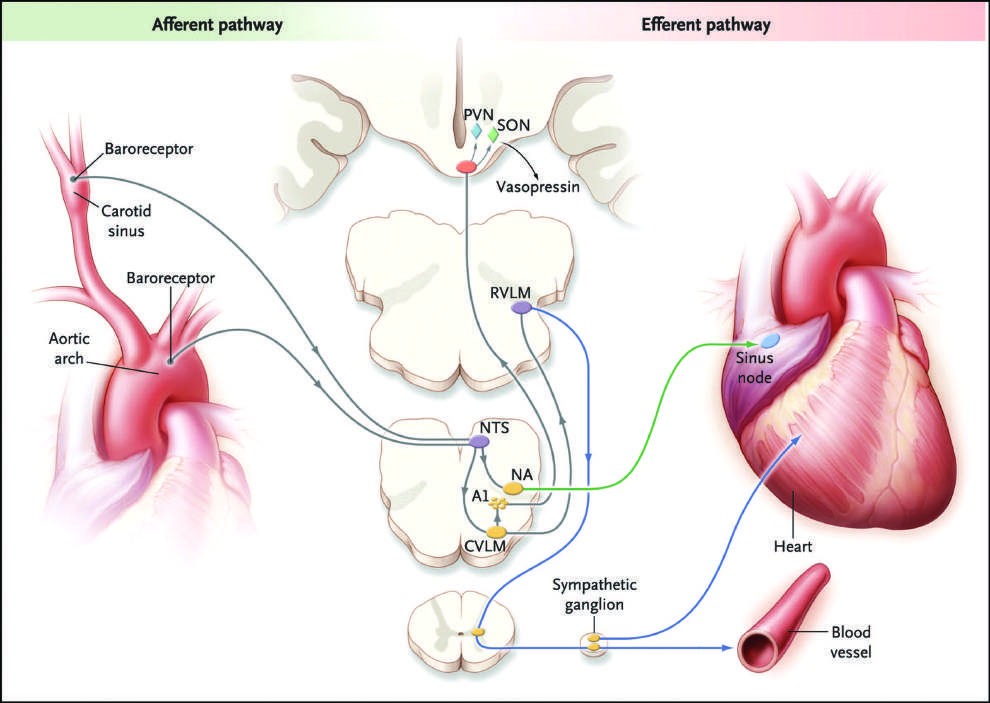
Caption: FIGURE 23-1 The baroreflex. A decrease in arterial pressure unloads the situated in the carotid sinus and aortic arch. This leads to a reduction in the afferent and vagus nerves to the nucleus of the tractus solitarius (NTS) in the dorsomedial input to the sinus node that is mediated via connections of the NTS to the nucleus the NTS projections to the caudal ventrolateral medulla (CVLM) (an excitatory pathway) The activation of RVLM presympathetic neurons in response to hypotension is thus vasopressin release is mediated by projections from the A1 noradrenergic cell group neurons in the magnocellular portion of the paraventricular nucleus (PVN) and the green denotes parasympathetic neurons. (From R Freeman: Neurogenic orthostatic Society. Reprinted with permission.) — FIGURE 23-2 A. The paroxysmal hypotensive-bradycardic response that is characteristic of neurally mediated syncope. Noninvasive beat-to-beat blood pressure and heart rate are shown >5 min (from 60 to 360 s) of an upright tilt on a tilt table. B. The same tracing expanded to show 80 s of the episode (from 80 to 200 s). BP, blood pressure; bpm, beats per minute; HR, heart rate.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.