Chapter 80: Oncologic Emergencies¶
Chapter 80 | Part 4: Oncology and Hematology · Part 4 – Oncology: Solid Tumors
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Superior vena cava syndrome (SVCS) is the clinical manifestation of superior vena cava obstruction with severe reduction in venous return from the head, neck, and upper extremities.
- Lung cancer, particularly of small-cell and squamous cell histologies, accounts for ~85% of all cases of malignant origin SVCS.
- Malignant spinal cord compression (MSCC) occurs in 5–10% of patients with cancer; lung cancer is the most common cause.
- Hyperleukocytosis and leukostasis syndrome occur when peripheral blast cell count is >100,000/mL in acute leukemia.
- Dexamethasone is the best initial treatment for all symptomatic patients with brain metastases.
- The 'hot quadrate' sign on CT scan suggests SVC obstruction caused by portosystemic venous shunting.
- Erosion of the pedicles (the 'winking owl' sign) is the earliest radiologic finding of vertebral tumor in plain films.
- Cauda equina syndrome is characterized by low back pain, diminished sensation over the buttocks, and rectal/bladder dysfunction.
- Pericardial effusion containing malignant cells on cytology has a very poor survival prognosis.
- Intestinal obstruction in patients with cancer has a poor prognosis with median survival of 3–4 months.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 4. CLINICAL FEATURES
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Imaging Findings
- 6.2 Diagnostic Criteria
- 7. MANAGEMENT & TREATMENT
- 7.1 SVCS Treatment
- 7.2 MSCC Treatment
- 7.3 Brain Metastases Treatment
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Management of cancer patients with back pain |
| 2 | 🔀 Flowchart | Management of patients at high risk for the tumor lysis syndrome |
| 1 | 🖼 Figure | Superior vena cava syndrome (SVCS) |
| 2 | 🖼 Figure | Abdominal computed tomography (CT) scans of a 72-year-old woman with neutropenic enterocolitis... |
| 3 | 🖼 Figure | Airway obstruction |
| 4 | 🖼 Figure | Abdominal computed tomography (CT) scans of a 72-year-old woman with neutropenic enterocolitis... |
| 5 | 🖼 Figure | A |
| 6 | 🖼 Figure | A |
| 7 | 🖼 Figure | A |
| 8 | 🖼 Figure | A |
| 9 | 🖼 Figure | Superior vena cava syndrome (SVCS) |
| 10 | 🖼 Figure | Airway obstruction |
| 11 | 🖼 Figure | Superior vena cava syndrome (SVCS) |
1. DEFINITION & OVERVIEW¶
- Emergencies in patients with cancer may be classified into three groups:
- Structural-obstructive oncologic emergencies
- Metabolic or hormonal problems (paraneoplastic syndromes, Chap. 98)
- Treatment-related complications
- Patients with cancer should receive all recommended non-live vaccines based on their approved indications.
- Yearly recommendations regarding COVID-19 and influenza vaccines should be followed.
- Patients with solid tumors in general mount greater antibody titers than patients with hematologic malignancies, especially if they have received B cell–depleting agents (e.g., rituximab, BTK inhibitors).
- However, vaccination is still recommended for such patients with the rationale that they may derive some protective benefit even if suboptimal.
- We also stress vaccination of household members, caretakers, and other close contacts to prevent them from viral infection and transmission to the patient.
- Live vaccines should not be given to immunocompromised persons.
- However, household members including children should receive age-appropriate vaccines, including live vaccines such as MMR and varicella.
2. EPIDEMIOLOGY¶
- Superior vena cava syndrome (SVCS) is the clinical manifestation of superior vena cava (SVC) obstruction, with severe reduction in venous return from the head, neck, and upper extremities.
- Malignant tumors, such as lung cancer, lymphoma, and metastatic tumors, are responsible for the majority of SVCS cases.
- With the expanding use of intravascular devices (e.g., permanent central venous access catheters, pacemaker/defibrillator leads), the prevalence of benign causes of SVCS is now increasing, accounting for at least 40% of cases.
- Lung cancer, particularly of small-cell and squamous cell histologies, accounts for ~85% of all cases of malignant origin.
- In young adults, malignant lymphoma is a leading cause of SVCS.
- Hodgkin's lymphoma involves the mediastinum more commonly than other lymphomas but rarely causes SVCS.
- When SVCS is noted in a young man with a mediastinal mass, the differential diagnosis is lymphoma versus primary mediastinal germ cell tumor.
- Metastatic cancers to the mediastinal lymph nodes, such as testicular and breast carcinomas, account for a small proportion of cases.
- Other causes include benign tumors, aortic aneurysm, thyromegaly, thrombosis, and fibrosing mediastinitis from prior irradiation, histoplasmosis, or Behçet's syndrome.
- Malignant spinal cord compression (MSCC) occurs in 5–10% of patients with cancer.
- Epidural tumor is the first manifestation of malignancy in ~10% of patients.
- The thoracic spine is the most common site (70%), followed by the lumbosacral spine (20%) and the cervical spine (10%).
- Involvement of multiple sites is most frequent in patients with breast and prostate carcinoma.
- Tumor involving the leptomeninges is a complication of both primary central nervous system (CNS) tumors and tumors that metastasize to the CNS.
- The incidence is estimated at 3–8% of patients with cancer.
- About 25% of patients with cancer die with intracranial metastases.
- The cancers that most often metastasize to the brain are lung and breast cancers and melanoma.
- Hyperleukocytosis and the leukostasis syndrome associated with it are potentially fatal complications of acute leukemia (particularly myeloid leukemia).
- The frequency of hyperleukocytosis is 5–13% in acute myeloid leukemia (AML) and 10–30% in acute lymphoid leukemia.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- SVCS is the clinical manifestation of superior vena cava (SVC) obstruction, with severe reduction in venous return from the head, neck, and upper extremities.
- Malignant tumors, such as lung cancer, lymphoma, and metastatic tumors, are responsible for the majority of SVCS cases.
- With the expanding use of intravascular devices (e.g., permanent central venous access catheters, pacemaker/defibrillator leads), the prevalence of benign causes of SVCS is now increasing, accounting for at least 40% of cases.
- Lung cancer, particularly of small-cell and squamous cell histologies, accounts for ~85% of all cases of malignant origin.
- In young adults, malignant lymphoma is a leading cause of SVCS.
- Hodgkin's lymphoma involves the mediastinum more commonly than other lymphomas but rarely causes SVCS.
- Metastatic cancers to the mediastinal lymph nodes, such as testicular and breast carcinomas, account for a small proportion of cases.
- Other causes include benign tumors, aortic aneurysm, thyromegaly, thrombosis, and fibrosing mediastinitis from prior irradiation, histoplasmosis, or Behçet's syndrome.
- SVCS as the initial manifestation of Behçet's syndrome may be due to inflammation of the SVC associated with thrombosis.
- Malignant pericardial disease is found at autopsy in 5–10% of patients with cancer, most frequently with lung cancer, breast cancer, leukemias, and lymphomas.
- Cardiac tamponade as the initial presentation of extrathoracic malignancy is rare.
- The origin is not malignancy in ~50% of cancer patients with symptomatic pericardial disease, but it can be related to irradiation; drug-induced pericarditis, including chemotherapeutic agents such as all-trans retinoic acid, arsenic trioxide, imatinib, and other abl kinase inhibitors; hypothyroidism; idiopathic pericarditis; infection; or autoimmune diseases.
- Pericardial disease has been associated with immune checkpoint inhibitors specifically in patients with advanced non-small-cell lung cancer.
- Intestinal obstruction and reobstruction are common problems in patients with advanced cancer, particularly colorectal or ovarian carcinoma.
- However, other cancers, such as lung or breast cancer and melanoma, can metastasize within the abdomen, leading to intestinal obstruction.
- Metastatic disease from colorectal, ovarian, pancreatic, gastric, and occasionally breast cancer can lead to peritoneal carcinomatosis, with infiltration of the omentum and peritoneal surface, thus limiting bowel motility.
- Typically, obstruction occurs at multiple sites in peritoneal carcinomatosis.
- Melanoma has a predilection to involve the small bowel; this involvement may be isolated, and resection may result in prolonged survival.
- Intestinal pseudoobstruction is caused by infiltration of the mesentery or bowel muscle by tumor, involvement of the celiac plexus, or paraneoplastic neuropathy in patients with small-cell lung cancer.
- Paraneoplastic neuropathy is associated with IgG antibodies reactive to neurons of the myenteric and submucosal plexuses of the jejunum and stomach.
- Ovarian cancer can lead to authentic luminal obstruction or to pseudoobstruction that results when circumferential invasion of a bowel segment arrests the forward progression of peristaltic contractions.
- Urinary obstruction may occur in patients with prostatic or gynecologic malignancies, particularly cervical carcinoma; metastatic disease from other primary sites such as carcinomas of the breast, stomach, lung, colon, and pancreas; or lymphomas.
- Radiation therapy to pelvic tumors may cause fibrosis and subsequent ureteral obstruction.
- Bladder outlet obstruction is usually due to prostate and cervical cancers and may lead to bilateral hydronephrosis and renal failure.
- Malignant spinal cord compression (MSCC) is defined as compression of the spinal cord and/or cauda equina by an extradural tumor mass.
- Metastatic tumor involves the vertebral column more often than any other part of the bony skeleton.
- Lung, breast, and prostate cancers are the most frequent offenders.
- Multiple myeloma also has a high incidence of spine involvement.
- Lymphomas, melanoma, renal cell cancer, and genitourinary cancers also cause cord compression.
- Cord injury develops when metastases to the vertebral body or pedicle enlarge and compress the underlying dura.
- Another cause of cord compression is direct extension of a paravertebral lesion through the intervertebral foramen.
- These cases usually involve a lymphoma, myeloma, or pediatric neoplasm.
- Parenchymal spinal cord metastasis is rare.
- Intramedullary metastases can be seen in lung cancer, breast cancer, renal cancer, melanoma, and lymphoma, and are frequently associated with brain metastases and leptomeningeal disease.
- Expanding extradural tumors induce injury through several mechanisms.
- Expanding extradural tumors induce mechanical injury to axons and myelin.
- Compression compromises blood flow, leading to ischemia and/or infarction.
- Hyperleukocytosis and the leukostasis syndrome associated with it are potentially fatal complications of acute leukemia (particularly myeloid leukemia).
- At such high blast cell counts, blood viscosity is increased, blood flow is slowed by aggregates of tumor cells, and the primitive myeloid leukemic cells are capable of invading through the endothelium and causing hemorrhage.
- Brain and lung are most commonly affected.
- Pulmonary leukostasis may present as respiratory distress and hypoxemia and progress to respiratory failure.
4. CLINICAL FEATURES¶
- Patients with SVCS usually present with neck and facial swelling (especially around the eyes), dyspnea, and cough.
- Other symptoms include hoarseness, tongue swelling, headaches, nasal congestion, epistaxis, hemoptysis, dysphagia, pain, dizziness, syncope, and lethargy.
- Bending forward or lying down may aggravate the symptoms.
- The characteristic physical findings are dilated neck veins; an increased number of collateral veins covering the anterior chest wall; cyanosis; and edema of the face, arms, and chest.
- Facial swelling and plethora are typically exacerbated when the patient is supine.
- More severe cases include proptosis, glossal and laryngeal edema, and obtundation.
- The clinical picture is milder if the obstruction is located above the azygos vein.
- Symptoms are usually progressive, but in some cases, they may improve as collateral circulation develops.
- Signs and symptoms of cerebral and/or laryngeal edema, though rare, are associated with a poorer prognosis and require urgent evaluation.
- Seizures are more likely related to brain metastases than to cerebral edema from venous occlusion.
- Patients with small-cell lung cancer and SVCS have a higher incidence of brain metastases than those without SVCS.
- Cardiorespiratory symptoms at rest, particularly with positional changes, suggest significant airway and vascular obstruction and limited physiologic reserve.
- Cardiac arrest or respiratory failure can occur, particularly in patients receiving sedatives or undergoing general anesthesia.
- Rarely, esophageal varices may develop, particularly in the setting of SVC syndrome due to hemodialysis catheter.
- These are 'downhill' varices based on the direction of blood flow from cephalad to caudad (in contrast to 'uphill' varices associated with caudad to cephalad flow from portal hypertension).
- Variceal bleeding may be a late complication of chronic SVCS.
- SVC obstruction may lead to bilateral breast edema with bilateral enlarged breasts.
- Unilateral breast dilation may be seen as a consequence of axillary or subclavian vein blockage.
- Most patients with pericardial metastasis are asymptomatic.
- However, the common symptoms are dyspnea, cough, chest pain, orthopnea, and weakness.
- Pleural effusion, sinus tachycardia, jugular venous distention, hepatomegaly, peripheral edema, and cyanosis are the most frequent physical findings.
- Relatively specific diagnostic findings, such as paradoxical pulse, diminished heart sounds, pulsus alternans (pulse waves alternating between those of greater and lesser amplitude with successive beats), and friction rub are less common than with nonmalignant pericardial disease.
- The most common initial symptom in patients with MSCC is localized back pain and tenderness due to involvement of vertebrae by tumor.
- Pain is usually present for days or months before other neurologic findings appear.
- It is exacerbated by movement and by coughing or sneezing.
- It can be differentiated from the pain of disk disease by the fact that it worsens when the patient is supine.
- Radicular pain is less common than localized back pain and usually develops later.
- Radicular pain from the thoracic roots is often bilateral and is described by patients as a feeling of tight, band-like constriction around the thorax and abdomen.
- Typical cervical radicular pain radiates down the arm; in the lumbar region, the radiation is down the legs.
- Lhermitte's sign, a tingling or electric sensation down the back and upper and lower limbs upon flexing or extending the neck, may be an early sign of cord compression.
- Loss of bowel or bladder control may be the presenting symptom but usually occurs late in the course.
- Occasionally, patients present with ataxia of gait without motor and sensory involvement due to involvement of the spinocerebellar tract.
- Patients develop numbness and paresthesias in the extremities or trunk.
- Loss of sensibility to pinprick is as common as loss of sensibility to vibration or position.
- The upper limit of the zone of sensory loss is often one or two vertebrae below the site of compression.
- Motor findings include weakness, spasticity, and abnormal muscle stretching.
- An extensor plantar reflex reflects significant compression.
- Deep tendon reflexes may be brisk.
- Motor and sensory loss usually precedes sphincter disturbance.
- Patients with autonomic dysfunction may present with decreased anal tonus, decreased perineal sensibility, and a distended bladder.
- The absence of the anal wink reflex or the bulbocavernosus reflex confirms cord involvement.
- Autonomic dysfunction is an unfavorable prognostic factor.
- Patients with progressive neurologic symptoms should have frequent neurologic examinations and rapid therapeutic intervention.
- Other illnesses that may mimic cord compression include osteoporotic vertebral collapse, disk disease, pyogenic abscess or vertebral tuberculosis, radiation myelopathy, neoplastic leptomeningitis, benign tumors, epidural hematoma, and spinal lipomatosis.
- Cauda equina syndrome is characterized by low back pain; diminished sensation over the buttocks, posterior-superior thighs, and perineal area in a saddle distribution; rectal and bladder dysfunction; sexual impotence; absent bulbocavernous, patellar, and Achilles' reflexes; and variable amount of lower-extremity weakness.
- This reflects compression of nerve roots as they form the cauda equina after leaving the spinal cord.
- The majority of cauda equina tumors are primary tumors of glial or nerve sheath origin; metastases are very rare.
- The signs and symptoms of a metastatic brain tumor are similar to those of other intracranial expanding lesions: headache, nausea, vomiting, behavioral changes, seizures, and focal, progressive neurologic changes.
- Occasionally the onset is abrupt, resembling a stroke, with the sudden appearance of headache, nausea, vomiting, and neurologic deficits.
- This picture is usually due to hemorrhage into the metastasis.
- Melanoma, germ cell tumors, and renal cell cancers have a particularly high incidence of intracranial bleeding.
- The tumor mass and surrounding edema may cause obstruction of the circulation of CSF, with resulting hydrocephalus.
- Patients with increased intracranial pressure may have papilledema with visual disturbances and neck stiffness.
- As the mass enlarges, brain tissue may be displaced through the fixed cranial openings, producing various herniation syndromes.
- Patients with increased intracranial pressure may have papilledema with visual disturbances and neck stiffness.
- As the mass enlarges, brain tissue may be displaced through the fixed cranial openings, producing various herniation syndromes.
- Patients with painful pathologic compression fractures without spinal instability may benefit from percutaneous vertebroplasty or kyphoplasty, the injection of acrylic cement into a collapsed vertebra to stabilize the fracture.
- Pain palliation is common, and local antitumor effects have been noted.
- Cement leakage may cause symptoms in ~10% of patients.
5. DIFFERENTIAL DIAGNOSIS¶
- When SVCS is noted in a young man with a mediastinal mass, the differential diagnosis is lymphoma versus primary mediastinal germ cell tumor.
- Other causes include benign tumors, aortic aneurysm, thyromegaly, thrombosis, and fibrosing mediastinitis from prior irradiation, histoplasmosis, or Behçet's syndrome.
- SVCS as the initial manifestation of Behçet's syndrome may be due to inflammation of the SVC associated with thrombosis.
- Other illnesses that may mimic cord compression include osteoporotic vertebral collapse, disk disease, pyogenic abscess or vertebral tuberculosis, radiation myelopathy, neoplastic leptomeningitis, benign tumors, epidural hematoma, and spinal lipomatosis.
- Intracranial hypertension ('pseudotumor cerebri') secondary to tretinoin therapy for acute promyelocytic leukemia has been reported as another cause of intracranial pressure in the setting of a malignancy.
- Other causes include benign tumors, aortic aneurysm, thyromegaly, thrombosis, and fibrosing mediastinitis from prior irradiation, histoplasmosis, or Behçet's syndrome.
- SVCS as the initial manifestation of Behçet's syndrome may be due to inflammation of the SVC associated with thrombosis.
6. INVESTIGATIONS & DIAGNOSIS¶
- The diagnosis of SVCS is a clinical one.
- The most significant chest radiographic finding is widening of the superior mediastinum, most commonly on the right side.
- Pleural effusion occurs in only 25% of patients, often on the right side.
- The majority of these effusions are exudative and occasionally chylous.
- However, a normal chest radiograph is still compatible with the diagnosis if other characteristic findings are present.
- Computed tomography (CT) provides the most reliable view of the mediastinal anatomy.
- The diagnosis of SVCS requires diminished or absent opacification of central venous structures with prominent collateral venous circulation.
- The focal hepatic hotspot on CT scan ('hot quadrate') sign suggests SVC obstruction, and it is caused by portosystemic venous shunting between the SVC and portal vein within liver.
- Magnetic resonance imaging (MRI) is increasingly being used to diagnose SVC obstruction with a 100% sensitivity and specificity, but dyspneic SVCS patients may have difficulty remaining supine for the entire imaging process.
- Invasive procedures, including bronchoscopy, percutaneous needle biopsy, mediastinoscopy, and even thoracotomy, can be performed by a skilled clinician without any major risk of bleeding.
- Endobronchial or esophageal ultrasound-guided needle aspiration may establish the diagnosis safely.
- For patients with a known cancer, a detailed workup usually is not necessary, and appropriate treatment may be started after obtaining a CT scan of the thorax.
- For those with no history of malignancy, a detailed evaluation is essential to rule out benign causes and determine a specific diagnosis to direct the appropriate therapy.
- Renal ultrasound is the safest and cheapest way to identify hydronephrosis.
- The function of an obstructed kidney can be evaluated by a nuclear scan.
- CT scan can reveal the point of obstruction and identify a retroperitoneal mass or adenopathy.
- Erect plain abdominal films may reveal multiple air-fluid levels and dilation of the small or large bowel.
- CT scan is useful in defining the extent of disease and the exact nature of the obstruction and differentiating benign from malignant causes of obstruction in patients who have undergone surgery for malignancy.
- Malignant obstruction is suggested by a mass at the site of obstruction or prior surgery, adenopathy, or an abrupt transition zone and irregular bowel thickening at the obstruction site.
- Benign obstruction is more likely when CT shows mesenteric vascular changes, a large volume of ascites, or a smooth transition zone and smooth bowel thickening at the obstruction site.
- In challenging patients with obstructive symptoms, particularly low-grade small-bowel obstruction (SBO), CT enteroclysis often can help establish the diagnosis by providing distention of small-bowel loops.
- In this technique, water-soluble contrast is infused through a nasoenteric tube into the duodenum or proximal small bowel followed by CT images.
- MRI is the imaging procedure of choice.
- Multiple epidural metastases are noted in 25% of patients with cord compression, and their presence influences treatment plans.
- On T1-weighted images, good contrast is noted between the cord, cerebrospinal fluid (CSF), and extradural lesions.
- Owing to its sensitivity in demonstrating the replacement of bone marrow by tumor, MRI can show which parts of a vertebra are involved by tumor.
- MRI also visualizes intraspinal extradural masses compressing the cord.
- T2-weighted images are most useful for the demonstration of intramedullary pathology.
- Gadolinium-enhanced MRI can help to delineate intramedullary disease.
- MRI is as good as or better than myelography plus postmyelogram CT scan in detecting metastatic epidural disease with cord compression.
- Myelography should be reserved for patients who have poor MRIs or who cannot undergo MRI promptly.
- CT scan in conjunction with myelography enhances the detection of small areas of spinal destruction.
- In patients with cord compression and an unknown primary tumor, a simple workup including chest radiography, mammography, measurement of prostate-specific antigen, and abdominal CT usually reveals the underlying malignancy.
- Diagnosis is made by demonstrating malignant cells in the CSF; however, up to 40% of patients may have false-negative CSF cytology.
- An elevated CSF protein level is nearly always present.
- Patients with neurologic signs and symptoms consistent with neoplastic meningitis who have a negative CSF cytology should have the spinal tap repeated at least one more time for cytologic examination.
- MRI findings suggestive of neoplastic meningitis include leptomeningeal, subependymal, dural, or cranial nerve enhancement; superficial cerebral lesions; intradural nodules; and communicating hydrocephalus.
- Spinal cord imaging by radiolabeled CSF flow studies are abnormal in up to 70% of patients with neoplastic meningitis; ventricular outlet obstruction, abnormal flow in the spinal canal, or impaired flow over the cerebral convexities may affect distribution of intrathecal chemotherapy, resulting in decreased efficacy or increased toxicity.
- Radiation therapy may correct CSF flow abnormalities before use of intrathecal chemotherapy.
6.1 Imaging Findings¶
- Chest radiograph: Widening of the superior mediastinum, most commonly on the right side.
- Pleural effusion: Occurs in only 25% of patients, often on the right side; majority are exudative and occasionally chylous.
- CT scan: Diminished or absent opacification of central venous structures with prominent collateral venous circulation.
- CT scan: Focal hepatic hotspot on CT scan ('hot quadrate') sign suggests SVC obstruction, caused by portosystemic venous shunting between the SVC and portal vein within liver.
- MRI: 100% sensitivity and specificity for SVC obstruction.
- MRI: Multiple epidural metastases noted in 25% of patients with cord compression.
- MRI: On T1-weighted images, good contrast is noted between the cord, cerebrospinal fluid (CSF), and extradural lesions.
- MRI: T2-weighted images are most useful for the demonstration of intramedullary pathology.
- MRI: Gadolinium-enhanced MRI can help to delineate intramedullary disease.
- MRI: MRI is as good as or better than myelography plus postmyelogram CT scan in detecting metastatic epidural disease with cord compression.
- MRI: MRI findings suggestive of neoplastic meningitis include leptomeningeal, subependymal, dural, or cranial nerve enhancement; superficial cerebral lesions; intradural nodules; and communicating hydrocephalus.
- CT enteroclysis: Water-soluble contrast is infused through a nasoenteric tube into the duodenum or proximal small bowel followed by CT images.
- Erect plain abdominal films: May reveal multiple air-fluid levels and dilation of the small or large bowel.
Table 1 — SVCS Imaging Findings¶
| Modality | Findings | Sensitivity/Specificity |
|---|---|---|
| Chest Radiograph | Widening of superior mediastinum (most commonly right side); Pleural effusion (25% of patients) | Variable |
| CT Scan | Diminished/absent opacification of central venous structures; Prominent collateral venous circulation; Focal hepatic hotspot ('hot quadrate') | High |
| MRI | 100% sensitivity and specificity for SVC obstruction; Visualizes intraspinal extradural masses | 100% |
6.2 Diagnostic Criteria¶
- SVCS Diagnosis: Clinical one; requires diminished or absent opacification of central venous structures with prominent collateral venous circulation.
- Neoplastic Meningitis Diagnosis: Demonstrating malignant cells in the CSF; elevated CSF protein level is nearly always present.
- Neoplastic Meningitis Diagnosis: MRI findings suggestive of neoplastic meningitis include leptomeningeal, subependymal, dural, or cranial nerve enhancement; superficial cerebral lesions; intradural nodules; and communicating hydrocephalus.
- Intestinal Obstruction Diagnosis: Malignant obstruction suggested by mass at site of obstruction or prior surgery, adenopathy, or abrupt transition zone and irregular bowel thickening.
- Benign Obstruction Diagnosis: CT shows mesenteric vascular changes, large volume of ascites, or smooth transition zone and smooth bowel thickening.
Table 2 — Neoplastic Meningitis MRI Findings¶
| Finding | Description |
|---|---|
| Leptomeningeal enhancement | Suggestive of neoplastic meningitis |
| Subependymal enhancement | Suggestive of neoplastic meningitis |
| Dural enhancement | Suggestive of neoplastic meningitis |
| Cranial nerve enhancement | Suggestive of neoplastic meningitis |
| Intradural nodules | Suggestive of neoplastic meningitis |
| Communicating hydrocephalus | Suggestive of neoplastic meningitis |
7. MANAGEMENT & TREATMENT¶
- Diuretics with a low-salt diet, head elevation, and oxygen may produce temporary symptomatic relief.
- Glucocorticoids have a limited role except in the setting of mediastinal lymphoma masses.
- Radiation therapy is the primary treatment for SVCS caused by non-small-cell lung cancer and other metastatic solid tumors.
- Chemotherapy is effective when the underlying cancer is small-cell carcinoma of the lung, lymphoma, or germ cell tumor.
- SVCS recurs in 10–30% of patients; it may be palliated with the use of intravascular self-expanding stents.
- Endovascular therapy is more frequently used first, to provide rapid relief of clinical symptoms with reduced complications.
- Early stenting may be necessary in patients with severe symptoms, particularly cerebral or laryngeal edema or postural hypotension.
- However, the prompt increase in venous return after stenting may precipitate heart failure and pulmonary edema.
- Other complications of stent placement include hematoma at the insertion site, SVC perforation, stent migration in the right ventricle, stent fracture, and pulmonary embolism.
- Surgery may play role in treatment of SVCS secondary to nonmalignant mediastinal fibrosis.
- Pericardiocentesis with or without the introduction of sclerosing agents, the creation of a pericardial window, complete pericardial stripping, cardiac irradiation, and systemic chemotherapy are effective treatments.
- Acute pericardial tamponade with life-threatening hemodynamic instability requires immediate drainage of fluid.
- This can be quickly achieved by pericardiocentesis.
- The recurrence rate after percutaneous catheter drainage is ~20%.
- Sclerotherapy (pericardial instillation of bleomycin, mitomycin C, or tetracycline) may decrease recurrences.
- Alternatively, subxiphoid pericardiotomy can be performed in 45 min under local anesthesia.
- Thoracoscopic surgical pericardial fenestration can be employed for benign causes.
- However, 60% of malignant pericardial effusions recur after this procedure.
- In a subset of patients, drainage of the pericardial effusion is paradoxically followed by worsening hemodynamic instability.
- This so-called 'postoperative low cardiac output syndrome' occurs in up to 10% of patients undergoing surgical drainage and carries poor short-term survival.
- The management of intestinal obstruction in patients with advanced malignancy depends on the extent of the underlying malignancy, options for further antineoplastic therapy, estimated life expectancy, the functional status of the major organs, and the extent of the obstruction.
- The initial management should include surgical evaluation.
- Operation is not always successful and may lead to further complications with a substantial mortality rate (10–20%).
- Laparoscopy can diagnose and treat malignant bowel obstruction in some cases.
- Self-expanding metal stents placed in the gastric outlet, duodenum, proximal jejunum, colon, or rectum may palliate obstructive symptoms at those sites without major surgery.
- Patients known to have advanced intraabdominal malignancy should receive a prolonged course of conservative management, including nasogastric decompression.
- Percutaneous endoscopic or surgical gastrostomy tube placement is an option for palliation of nausea and vomiting, the so-called 'venting gastrostomy.'
- Treatment with antiemetics, antispasmodics, and analgesics may allow patients to remain outside the hospital.
- Octreotide may relieve obstructive symptoms through its inhibitory effect on gastrointestinal secretion.
- Glucocorticoids have anti-inflammatory effects and may help the resolution of bowel obstruction.
- Obstruction associated with flank pain, sepsis, or fistula formation due to malignancy is an indication for immediate palliative urinary diversion.
- Internal ureteral stents can be placed under local anesthesia.
- Percutaneous nephrostomy offers an alternative approach for drainage.
- The placement of a nephrostomy is associated with a significant rate of pyelonephritis.
- In the case of bladder outlet obstruction due to malignancy, a suprapubic cystostomy can be used for urinary drainage.
- An aggressive intervention with invasive approaches to improve the obstruction should be weighed against the likelihood of antitumor response, and the ability to reverse renal insufficiency back should be evaluated.
- Radiation therapy plus glucocorticoids is generally the initial treatment of choice for most patients with MSCC.
- The management of MSCC requires a multidisciplinary approach.
- The management decision of SCC involves assessment of neurologic (N), oncologic (O), mechanical (M), and systemic factors (S).
- NOMS was developed by Memorial Sloan Kettering Cancer Center (MSKCC) researchers to provide an algorithm for management of SCC.
- The neurologic assessment is based on the degree of epidural SCC, myelopathy, and/or functional radiculopathy.
- Oncologic assessment involves the radiosensitivity of the tumor type.
- In patients with radioresistant tumors, stereotactic body radiotherapy (SBRT) is the preferred approach if radiation is appropriate.
- Safe delivery of SBRT requires a 2- to 3-mm margin away from the spinal cord.
- Separation surgery followed by SBRT is necessary in patients with high-grade SCC due to radioresistant tumors.
- Separation surgery is the circumferential excision of epidural tumor to reconstitute the thecal sac and provide a 2-mm margin for safe delivery of an ablative radiation dose.
- In patients with mechanical instability or retro-pulsion of bone fragments into the spinal canal or cord, a surgical approach is the treatment of choice.
- Systemic factors that need be considered are the extent of disease and medical comorbidities that determine the patient's ability to tolerate planned therapy.
- Chemotherapy may have a role in patients with chemosensitive tumors who have had prior radiotherapy to the same region and who are not candidates for surgery.
- Patients who previously received radiotherapy for MSCC with an in-field tumor progression can be treated with reirradiation with spine stereotactic radiosurgery (SRS) if they are not surgical candidates.
- Patients with painful pathologic compression fractures without spinal instability may benefit from percutaneous vertebroplasty or kyphoplasty, the injection of acrylic cement into a collapsed vertebra to stabilize the fracture.
- Pain palliation is common, and local antitumor effects have been noted.
- Cement leakage may cause symptoms in ~10% of patients.
- Bisphosphonates and/or denosumab may be helpful in prevention of SCC in patients with bony involvement.
- Dexamethasone is the best initial treatment for all symptomatic patients with brain metastases.
- The current success of immunotherapy approaches for primary and metastatic brain tumors may preclude or limit glucocorticoid use since it may decrease antitumor response.
- Bevacizumab should be considered in patients who are unable to wean completely off of steroids as well as those who have symptomatic brain edema and are on immunotherapy.
- Patients with a single brain metastasis and with controlled extracranial disease may be treated with surgical excision followed by SRS to the resection cavity.
- SRS is recommended in patients with a limited number of brain metastases (one to four) who have stable, systemic disease or reasonable systemic treatment options and in patients who have a small number of metastatic lesions in whom whole-brain radiation therapy has failed.
- The treatment of a larger number of intracranial metastases remains controversial.
- More patients now receive SRS because of cognitive dysfunction associated with whole-brain radiation.
- Some patients with increased intracranial pressure associated with hydrocephalus may benefit from shunt placement.
- If neurologic deterioration is not reversed with medical therapy, ventriculotomy to remove CSF or craniotomy to remove tumors or hematomas may be necessary.
- Patients with painful pathologic compression fractures without spinal instability may benefit from percutaneous vertebroplasty or kyphoplasty, the injection of acrylic cement into a collapsed vertebra to stabilize the fracture.
- Pain palliation is common, and local antitumor effects have been noted.
- Cement leakage may cause symptoms in ~10% of patients.
- Bisphosphonates and/or denosumab may be helpful in prevention of SCC in patients with bony involvement.
- Chemotherapy provided by either intrathecal injection or systemic routes is used to control leptomeningeal disease throughout the entire neuroaxis.
- Intrathecal chemotherapy, usually methotrexate, cytarabine, or thiotepa, is delivered by lumbar puncture or by an intraventricular reservoir (Ommaya).
- Among solid tumors, breast cancer responds best to therapy.
- Focal radiotherapy may have a role in bulky disease and in symptomatic or obstructive lesions.
- Targeted therapy such as systemically administered EGFR tyrosine kinase inhibitors (TKIs) in non-small-cell lung cancer may lead to improvement in some patients with leptomeningeal spread.
- Patients with neoplastic meningitis from either acute leukemia or lymphoma may be cured of their CNS disease if the systemic disease can be eliminated.
- Leukostasis: Hydroxyurea can rapidly reduce a high blast cell count while the diagnostic workup is in progress.
- Leukostasis: Rapid consumption of plasma oxygen by the markedly increased number of white blood cells can cause spuriously low arterial oxygen tension.
- Pulse oximetry is the most accurate way of assessing oxygenation in patients with hyperleukocytosis.
7.1 SVCS Treatment¶
- Diuretics with a low-salt diet, head elevation, and oxygen may produce temporary symptomatic relief.
- Glucocorticoids have a limited role except in the setting of mediastinal lymphoma masses.
- Radiation therapy is the primary treatment for SVCS caused by non-small-cell lung cancer and other metastatic solid tumors.
- Chemotherapy is effective when the underlying cancer is small-cell carcinoma of the lung, lymphoma, or germ cell tumor.
- SVCS recurs in 10–30% of patients; it may be palliated with the use of intravascular self-expanding stents.
- Endovascular therapy is more frequently used first, to provide rapid relief of clinical symptoms with reduced complications.
- Early stenting may be necessary in patients with severe symptoms, particularly cerebral or laryngeal edema or postural hypotension.
- However, the prompt increase in venous return after stenting may precipitate heart failure and pulmonary edema.
- Other complications of stent placement include hematoma at the insertion site, SVC perforation, stent migration in the right ventricle, stent fracture, and pulmonary embolism.
- Surgery may play role in treatment of SVCS secondary to nonmalignant mediastinal fibrosis.
Table 3 — SVCS Treatment Options¶
| Treatment | Indication | Notes |
|---|---|---|
| Diuretics, low-salt diet, head elevation, oxygen | Temporary symptomatic relief | Limited role |
| Glucocorticoids | Mediastinal lymphoma masses | Limited role |
| Radiation therapy | Non-small-cell lung cancer, metastatic solid tumors | Primary treatment |
| Chemotherapy | Small-cell carcinoma of the lung, lymphoma, germ cell tumor | Effective |
| Intravascular self-expanding stents | Palliation of SVCS | Recurrence 10–30% |
| Endovascular therapy | First-line for rapid relief | Reduced complications |
| Surgery | Nonmalignant mediastinal fibrosis | Role in treatment |
7.2 MSCC Treatment¶
- Radiation therapy plus glucocorticoids is generally the initial treatment of choice for most patients with MSCC.
- The management of MSCC requires a multidisciplinary approach.
- The management decision of SCC involves assessment of neurologic (N), oncologic (O), mechanical (M), and systemic factors (S).
- NOMS was developed by Memorial Sloan Kettering Cancer Center (MSKCC) researchers to provide an algorithm for management of SCC.
- The neurologic assessment is based on the degree of epidural SCC, myelopathy, and/or functional radiculopathy.
- Oncologic assessment involves the radiosensitivity of the tumor type.
- In patients with radioresistant tumors, stereotactic body radiotherapy (SBRT) is the preferred approach if radiation is appropriate.
- Safe delivery of SBRT requires a 2- to 3-mm margin away from the spinal cord.
- Separation surgery followed by SBRT is necessary in patients with high-grade SCC due to radioresistant tumors.
- Separation surgery is the circumferential excision of epidural tumor to reconstitute the thecal sac and provide a 2-mm margin for safe delivery of an ablative radiation dose.
- In patients with mechanical instability or retro-pulsion of bone fragments into the spinal canal or cord, a surgical approach is the treatment of choice.
- Systemic factors that need be considered are the extent of disease and medical comorbidities that determine the patient's ability to tolerate planned therapy.
- Chemotherapy may have a role in patients with chemosensitive tumors who have had prior radiotherapy to the same region and who are not candidates for surgery.
- Patients who previously received radiotherapy for MSCC with an in-field tumor progression can be treated with reirradiation with spine stereotactic radiosurgery (SRS) if they are not surgical candidates.
- Patients with painful pathologic compression fractures without spinal instability may benefit from percutaneous vertebroplasty or kyphoplasty, the injection of acrylic cement into a collapsed vertebra to stabilize the fracture.
- Pain palliation is common, and local antitumor effects have been noted.
- Cement leakage may cause symptoms in ~10% of patients.
- Bisphosphonates and/or denosumab may be helpful in prevention of SCC in patients with bony involvement.
Table 4 — MSCC NOMS Factors¶
| Factor | Assessment | Notes |
|---|---|---|
| Neurologic (N) | Degree of epidural SCC, myelopathy, functional radiculopathy | Initial assessment |
| Oncologic (O) | Radiosensitivity of the tumor type | Determines radiation approach |
| Mechanical (M) | Mechanical instability, retro-pulsion of bone fragments | Surgical approach if present |
| Systemic (S) | Extent of disease, medical comorbidities | Determines ability to tolerate therapy |
7.3 Brain Metastases Treatment¶
- Dexamethasone is the best initial treatment for all symptomatic patients with brain metastases.
- The current success of immunotherapy approaches for primary and metastatic brain tumors may preclude or limit glucocorticoid use since it may decrease antitumor response.
- Bevacizumab should be considered in patients who are unable to wean completely off of steroids as well as those who have symptomatic brain edema and are on immunotherapy.
- Patients with a single brain metastasis and with controlled extracranial disease may be treated with surgical excision followed by SRS to the resection cavity.
- SRS is recommended in patients with a limited number of brain metastases (one to four) who have stable, systemic disease or reasonable systemic treatment options and in patients who have a small number of metastatic lesions in whom whole-brain radiation therapy has failed.
- The treatment of a larger number of intracranial metastases remains controversial.
- More patients now receive SRS because of cognitive dysfunction associated with whole-brain radiation.
- Some patients with increased intracranial pressure associated with hydrocephalus may benefit from shunt placement.
- If neurologic deterioration is not reversed with medical therapy, ventriculotomy to remove CSF or craniotomy to remove tumors or hematomas may be necessary.
- Patients with painful pathologic compression fractures without spinal instability may benefit from percutaneous vertebroplasty or kyphoplasty, the injection of acrylic cement into a collapsed vertebra to stabilize the fracture.
- Pain palliation is common, and local antitumor effects have been noted.
- Cement leakage may cause symptoms in ~10% of patients.
- Bisphosphonates and/or denosumab may be helpful in prevention of SCC in patients with bony involvement.
Table 5 — Brain Metastases Treatment Options¶
| Treatment | Indication | Notes |
|---|---|---|
| Dexamethasone | All symptomatic patients | Best initial treatment |
| Immunotherapy | Primary and metastatic brain tumors | May preclude glucocorticoid use |
| Bevacizumab | Unable to wean off steroids, symptomatic brain edema | Consider in immunotherapy patients |
| Surgical excision + SRS | Single brain metastasis, controlled extracranial disease | Followed by SRS to resection cavity |
| SRS | Limited number of brain metastases (one to four) | Stable systemic disease or whole-brain radiation failure |
| Whole-brain radiation therapy | Larger number of intracranial metastases | Controversial |
| Shunt placement | Increased intracranial pressure associated with hydrocephalus | May benefit patients |
| Ventriculotomy/Craniotomy | Neurologic deterioration not reversed with medical therapy | Remove CSF or tumors/hematomas |
8. PROGNOSIS & COMPLICATIONS¶
- The mortality associated with SVCS does not relate to caval obstruction but rather to the underlying cause.
- Cancer patients with pericardial effusion containing malignant cells on cytology have a very poor survival.
- The prognosis for the patient with cancer who develops intestinal obstruction is poor; median survival is 3–4 months.
- About 25–30% of patients are found to have intestinal obstruction due to causes other than cancer.
- Adhesions from previous operations are a common benign cause.
- Ileus induced by vinca alkaloids, narcotics, or other drugs is another reversible cause.
- Autonomic dysfunction is an unfavorable prognostic factor.
- Rapid onset and progression of signs and symptoms are poor prognostic features.
- The development of neoplastic meningitis usually occurs in the setting of uncontrolled cancer outside the CNS; thus, prognosis is poor (median survival 10–12 weeks).
- However, treatment of the neoplastic meningitis may successfully alleviate symptoms and control the CNS spread.
- Patients with neoplastic meningitis from either acute leukemia or lymphoma may be cured of their CNS disease if the systemic disease can be eliminated.
9. SPECIAL CONSIDERATIONS¶
- Patients with cancer should receive all recommended non-live vaccines based on their approved indications.
- Yearly recommendations regarding COVID-19 and influenza vaccines should be followed.
- Patients with solid tumors in general mount greater antibody titers than patients with hematologic malignancies, especially if they have received B cell–depleting agents (e.g., rituximab, BTK inhibitors).
- However, vaccination is still recommended for such patients with the rationale that they may derive some protective benefit even if suboptimal.
- We also stress vaccination of household members, caretakers, and other close contacts to prevent them from viral infection and transmission to the patient.
- Live vaccines should not be given to immunocompromised persons.
- However, household members including children should receive age-appropriate vaccines, including live vaccines such as MMR and varicella.
- If the child develops a rash following MMR or varicella vaccination, contact with the cancer patient should be limited until the rash resolves.
- The use of long-term central venous catheters has become common practice in patients with cancer.
- Major vessel thrombosis may occur.
- In these cases, catheter removal should be combined with anticoagulation to prevent embolization.
- SVCS in this setting, if detected early, can be treated by fibrinolytic therapy without sacrificing the catheter.
- When managing patients with transvenous lead-related SVC syndrome, anticoagulation, local and systemic thrombolytic therapy, and surgical intervention can be effective therapy in select patients.
- Endovascular stenting has also been shown to be safe and promising, with minimal procedural or clinical complications.
- The same role of anticoagulation after SVC stent placement is controversial.
10. KEY PEARLS & CLINICAL TRAPS¶
- SVCS: Bending forward or lying down may aggravate the symptoms.
- SVCS: Cardiorespiratory symptoms at rest, particularly with positional changes, suggest significant airway and vascular obstruction and limited physiologic reserve.
- SVCS: Cardiac arrest or respiratory failure can occur, particularly in patients receiving sedatives or undergoing general anesthesia.
- SVCS: Rarely, esophageal varices may develop, particularly in the setting of SVC syndrome due to hemodialysis catheter.
- SVCS: These are 'downhill' varices based on the direction of blood flow from cephalad to caudad (in contrast to 'uphill' varices associated with caudad to cephalad flow from portal hypertension).
- SVCS: Variceal bleeding may be a late complication of chronic SVCS.
- SVCS: SVC obstruction may lead to bilateral breast edema with bilateral enlarged breasts.
- SVCS: Unilateral breast dilation may be seen as a consequence of axillary or subclavian vein blockage.
- MSCC: Pain is usually present for days or months before other neurologic findings appear.
- MSCC: It can be differentiated from the pain of disk disease by the fact that it worsens when the patient is supine.
- MSCC: Loss of bowel or bladder control may be the presenting symptom but usually occurs late in the course.
- MSCC: Autonomic dysfunction is an unfavorable prognostic factor.
- MSCC: Patients with progressive neurologic symptoms should have frequent neurologic examinations and rapid therapeutic intervention.
- MSCC: Other illnesses that may mimic cord compression include osteoporotic vertebral collapse, disk disease, pyogenic abscess or vertebral tuberculosis, radiation myelopathy, neoplastic leptomeningitis, benign tumors, epidural hematoma, and spinal lipomatosis.
- Leukostasis: Hyperleukocytosis and the leukostasis syndrome associated with it are potentially fatal complications of acute leukemia (particularly myeloid leukemia).
- Leukostasis: At such high blast cell counts, blood viscosity is increased, blood flow is slowed by aggregates of tumor cells, and the primitive myeloid leukemic cells are capable of invading through the endothelium and causing hemorrhage.
- Leukostasis: Brain and lung are most commonly affected.
- Leukostasis: Pulmonary leukostasis may present as respiratory distress and hypoxemia and progress to respiratory failure.
- Leukostasis: Rapid consumption of plasma oxygen by the markedly increased number of white blood cells can cause spuriously low arterial oxygen tension.
- Leukostasis: Pulse oximetry is the most accurate way of assessing oxygenation in patients with hyperleukocytosis.
- Pericardial: Relatively specific diagnostic findings, such as paradoxical pulse, diminished heart sounds, pulsus alternans (pulse waves alternating between those of greater and lesser amplitude with successive beats), and friction rub are less common than with nonmalignant pericardial disease.
- Pericardial: Cancer patients with pericardial effusion containing malignant cells on cytology have a very poor survival.
- Pericardial: In a subset of patients, drainage of the pericardial effusion is paradoxically followed by worsening hemodynamic instability.
- Pericardial: This so-called 'postoperative low cardiac output syndrome' occurs in up to 10% of patients undergoing surgical drainage and carries poor short-term survival.
- Intestinal: The prognosis for the patient with cancer who develops intestinal obstruction is poor; median survival is 3–4 months.
- Intestinal: About 25–30% of patients are found to have intestinal obstruction due to causes other than cancer.
- Intestinal: Adhesions from previous operations are a common benign cause.
- Intestinal: Ileus induced by vinca alkaloids, narcotics, or other drugs is another reversible cause.
- Neoplastic Meningitis: Diagnosis is made by demonstrating malignant cells in the CSF; however, up to 40% of patients may have false-negative CSF cytology.
- Neoplastic Meningitis: An elevated CSF protein level is nearly always present.
- Neoplastic Meningitis: Patients with neurologic signs and symptoms consistent with neoplastic meningitis who have a negative CSF cytology should have the spinal tap repeated at least one more time for cytologic examination.
- Neoplastic Meningitis: The development of neoplastic meningitis usually occurs in the setting of uncontrolled cancer outside the CNS; thus, prognosis is poor (median survival 10–12 weeks).
- Neoplastic Meningitis: However, treatment of the neoplastic meningitis may successfully alleviate symptoms and control the CNS spread.
- Neoplastic Meningitis: Patients with neoplastic meningitis from either acute leukemia or lymphoma may be cured of their CNS disease if the systemic disease can be eliminated.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶

Caption: FIGURE 80-2 Management of cancer patients with back pain.
Flowchart 2¶

Caption: FIGURE 80-4 Management of patients at high risk for the tumor lysis syndrome.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

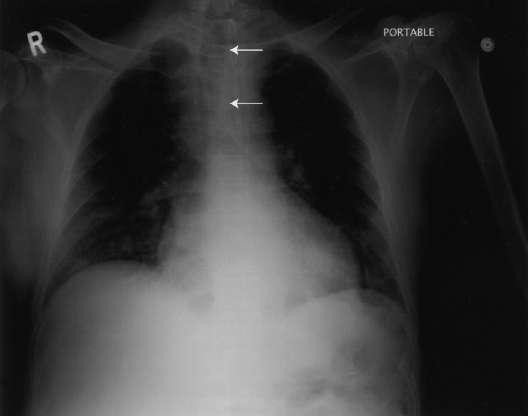
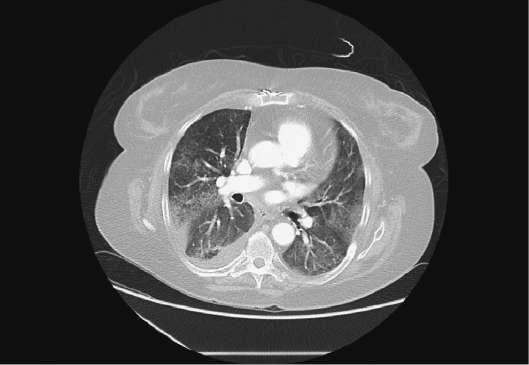
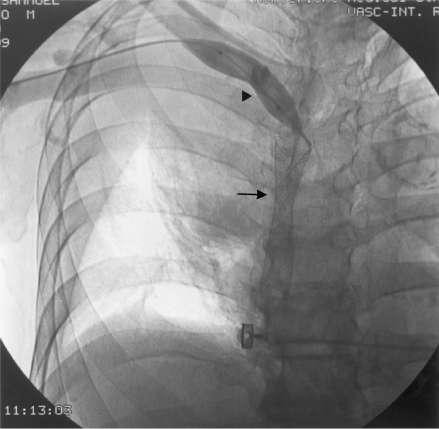
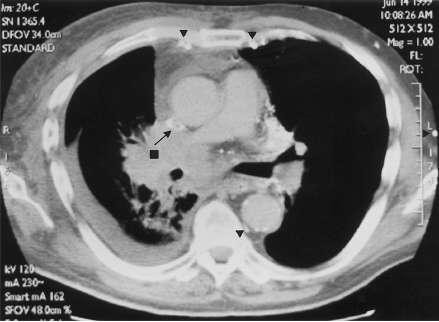
Caption: FIGURE 80-1 Superior vena cava syndrome (SVCS). A. Chest radiographs of a 59-year-old man with recurrent SVCS caused by non-small-cell lung cancer showing right paratracheal mass with right pleural effusion. B. Computed tomography of same patient demonstrating obstruction of the superior vena cava with thrombosis (arrow) by the lung cancer (square) and collaterals (arrowheads). C. Balloon angioplasty (arrowhead) with Wallstent (arrow) in same patient. — Chest radiographs of a 59-year-old man with recurrent SVCS caused by non-small-cell lung cancer showing right paratracheal mass with right pleural effusion.
Figure 2¶

Caption: FIGURE 80-6 Abdominal computed tomography (CT) scans of a 72-year-old woman with neutropenic enterocolitis secondary to chemotherapy. A. Air in inferior mesenteric vein (arrow) and bowel wall with pneumatosis intestinalis. B. CT scan of upper abdomen demonstrating air in portal vein (arrows). — Computed tomography of the same patient demonstrating obstruction of the superior vena cava with thrombosis by the lung cancer and collaterals.
Figure 3¶
Caption: FIGURE 80-3 Airway obstruction. A. Computed tomography scan of a 62-year-old man with tracheal obstruction caused by renal carcinoma showing paratracheal mass with tracheal invasion/obstruction (arrow). B. Chest x-ray of same patient after stent (arrows) placement. — Balloon angioplasty with Wallstent in same patient demonstrating relief of obstruction.
Figure 4¶

Caption: FIGURE 80-6 Abdominal computed tomography (CT) scans of a 72-year-old woman with neutropenic enterocolitis secondary to chemotherapy. A. Air in inferior mesenteric vein (arrow) and bowel wall with pneumatosis intestinalis. B. CT scan of upper abdomen demonstrating air in portal vein (arrows). — Management algorithm for cancer patients with back pain showing steps from evaluation to treatment based on MRI and neurologic status.
Figure 5¶

Caption: FIGURE 80-5 A. Computed tomography scan of a 63-year-old female with metastatic interlobular septal thickening and diffuse ground-glass opacity to nivolumab. B. lung and COVID-19 pneumonia showing peripheral and basilar predominant patchy — Chest radiograph showing widened superior mediastinum, most commonly on the right side, compatible with SVCS diagnosis.
Figure 6¶
Caption: FIGURE 80-5 A. Computed tomography scan of a 63-year-old female with metastatic interlobular septal thickening and diffuse ground-glass opacity to nivolumab. B. lung and COVID-19 pneumonia showing peripheral and basilar predominant patchy — CT scan of chest revealing multiple air-fluid levels and dilation of the small or large bowel in intestinal obstruction.
Figure 7¶

Caption: FIGURE 80-5 A. Computed tomography scan of a 63-year-old female with metastatic interlobular septal thickening and diffuse ground-glass opacity to nivolumab. B. lung and COVID-19 pneumonia showing peripheral and basilar predominant patchy — Ultrasound identifying hydronephrosis in patients with urinary obstruction due to prostatic or gynecologic malignancies.
Figure 8¶

Caption: FIGURE 80-5 A. Computed tomography scan of a 63-year-old female with metastatic interlobular septal thickening and diffuse ground-glass opacity to nivolumab. B. lung and COVID-19 pneumonia showing peripheral and basilar predominant patchy — MRI of spine showing epidural metastases compressing the cord and theca at the level of clinical features.
Figure 9¶
Caption: FIGURE 80-1 Superior vena cava syndrome (SVCS). A. Chest radiographs of a 59-year-old man with recurrent SVCS caused by non-small-cell lung cancer showing right paratracheal mass with right pleural effusion. B. Computed tomography of same patient demonstrating obstruction of the superior vena cava with thrombosis (arrow) by the lung cancer (square) and collaterals (arrowheads). C. Balloon angioplasty (arrowhead) with Wallstent (arrow) in same patient. — MRI of brain showing multiple enhancing lesions of various sizes with surrounding areas of low-density edema in brain metastases.
Figure 10¶

Caption: FIGURE 80-3 Airway obstruction. A. Computed tomography scan of a 62-year-old man with tracheal obstruction caused by renal carcinoma showing paratracheal mass with tracheal invasion/obstruction (arrow). B. Chest x-ray of same patient after stent (arrows) placement. — MRI showing leptomeningeal, subependymal, dural, or cranial nerve enhancement suggestive of neoplastic meningitis.
Figure 11¶
Caption: FIGURE 80-1 Superior vena cava syndrome (SVCS). A. Chest radiographs of a 59-year-old man with recurrent SVCS caused by non-small-cell lung cancer showing right paratracheal mass with right pleural effusion. B. Computed tomography of same patient demonstrating obstruction of the superior vena cava with thrombosis (arrow) by the lung cancer (square) and collaterals (arrowheads). C. Balloon angioplasty (arrowhead) with Wallstent (arrow) in same patient. — Blood gas results showing spuriously low arterial oxygen tension in patients with hyperleukocytosis and leukostasis syndrome.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.