Focal Atrial Tachycardia¶
Chapter 255 | Part 12: Endocrinology · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Focal AT accounts for ~10% of paroxysmal supraventricular tachycardia (PSVTs) in patients referred for catheter ablation
- AT mechanisms include abnormal automaticity, triggered automaticity, or small reentry circuit in diseased atrial tissue
- AT will not terminate with AV block, distinguishing it from AV nodal-dependent SVTs
- Warm-up phase when atrial activation rate increases after initiation or cool-down phase when rate slows prior to termination favors AT
- P waves are often discrete with intervening isoelectric segment, in contrast to atrial flutter and macroreentrant AT
- AT with AV block is characteristic of digitalis toxicity
- Incessant AT can cause tachycardia-induced cardiomyopathy
- Treatment strategies aimed at increasing blood pressure will not be appropriate for inappropriate sinus tachycardia
- Sinus node modification will be ineffective for POTS and may exacerbate nontachycardia components
- Areas of fibrosis can act as nidus for abnormal automaticity from injured but partially living cells
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Mechanisms of Focal AT
- 1.2 Anatomical Origins
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Pathophysiological Cascade
- 4. CLINICAL FEATURES
- 4.1 ECG Findings
- 4.2 Symptom Variability
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Distinguishing Features
- 5.2 R-P Relationships
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria
- 6.2 Diagnostic Algorithm
- 7. MANAGEMENT & TREATMENT
- 7.1 Catheter Ablation
- 7.2 Treatment Limitations
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Tachycardia-Induced Cardiomyopathy
- 8.2 Progression to Other Arrhythmias
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
- Focal atrial tachycardia (AT) is a form of supraventricular tachycardia originating from a discrete focus within the atria
- The term focal is used to differentiate this form of AT from typical and atypical atrial flutter but does not define a mechanism of the arrhythmia
- ATs can originate from most regions of the atria, including atrial tissue extending into a pulmonary vein, the coronary sinus, or vena cava
- AT can be sustained, nonsustained, paroxysmal, or incessant
- Focal AT accounts for approximately 10% of paroxysmal supraventricular tachycardia (PSVTs) in patients referred for catheter ablation
- Nonsustained focal AT is commonly observed on ambulatory electrocardiogram (ECG) recordings, and prevalence increases with age
- Asymptomatic nonsustained ATs are often labeled as 'SVT' on monitor reports, prompting patients to seek advice on catheter ablation
- However, treatment is not recommended for asymptomatic nonsustained AT identified on ECG monitoring
- Frequent atrial ectopy and nonsustained AT are often precursors to more significant arrhythmias such as atrial fibrillation and atrial flutter
1.1 Mechanisms of Focal AT¶
- Underlying mechanisms include:
- Abnormal automaticity
- Triggered automaticity
- Small reentry circuit in diseased atrial tissue
- AT typically presents with 1:1 AV conduction or with AV block in a Wenckebach or fixed (e.g., 2:1 or 3:1) pattern
- Because AT is not dependent on AV nodal conduction, the atrial rate will not be affected when AV block occurs
- A so-called warm-up phase when the atrial activation rate increases after initiation or a cool-down phase when the rate slows prior to termination also favors AT rather than AV nodal–dependent SVT
- This warm-up/cool-down phase is a common observation with enhanced automaticity
1.2 Anatomical Origins¶
- AT can originate from most regions of the atria
- AT typically originates in areas of complex atrial anatomy, such as:
- Crista terminalis
- Valve annuli
- Atrial septum
- Atrial muscle extending along cardiac thoracic veins
- Superior vena cava
- Coronary sinus
- Pulmonary veins
- The location can often be approximated by the P-wave morphology
- AT from the atrial septum will frequently have a narrower P-wave duration than sinus rhythm
- AT from the left atrium will usually have a monophasic, positive P wave in lead V and negative P waves in I and aVL, indicating an activation wavefront away from the left atrial free wall
- AT that originates from superior atrial locations, such as the superior vena cava or superior pulmonary veins, will be positive in the inferior limb leads II, III, and aVF
- AT from a more inferior location, such as the ostium of the coronary sinus, will inscribe negative P waves in these same leads
- When the focus is in the superior aspect of the crista terminalis, close to the sinus node, the P wave will resemble that of sinus tachycardia
2. EPIDEMIOLOGY¶
- Focal AT accounts for approximately 10% of paroxysmal supraventricular tachycardia (PSVTs) in patients referred for catheter ablation
- Nonsustained focal AT is commonly observed on ambulatory electrocardiogram (ECG) recordings
- The prevalence of nonsustained AT increases with age
- Asymptomatic nonsustained ATs are often labeled as 'SVT' on monitor reports
- Treatment is not recommended for asymptomatic nonsustained AT identified on ECG monitoring
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- AT can occur in the absence of structural heart disease
- AT may be associated with any condition that causes atrial fibrosis, including:
- Atrial fibrosis
- Prior catheter ablation (areas of fibrosis can act as a nidus for abnormal automaticity)
- Areas of fibrosis can act as a nidus for abnormal automaticity from injured but partially living cells
- Microreentry in zones of slow conduction within and on the border of fibrotic areas
- Sympathetic stimulation is a promoting factor
- The emergence of AT can be a sign of underlying illness or drug toxicity
- In particular, AT with atrioventricular (AV) block is characteristic of digitalis toxicity
3.1 Pathophysiological Cascade¶
- Abnormal automaticity from injured but partially living cells in fibrotic areas
- Microreentry in zones of slow conduction within and on the border of fibrotic areas
- Sympathetic stimulation promotes emergence of AT
- AT can be sustained, nonsustained, paroxysmal, or incessant
- Incessant AT can cause tachycardia-induced cardiomyopathy
4. CLINICAL FEATURES¶
- Symptoms from AT are highly variable but similar to other supraventricular tachycardias (SVTs)
- Incessant AT can cause tachycardia-induced cardiomyopathy
- AT typically presents with 1:1 AV conduction or with AV block in a Wenckebach or fixed (e.g., 2:1 or 3:1) pattern
- Because AT is not dependent on AV nodal conduction, AT will not terminate with AV block
- A so-called warm-up phase when the atrial activation rate increases after initiation or a cool-down phase when the rate slows prior to termination also favors AT rather than AV nodal–dependent SVT
- P waves are often discrete, with an intervening isoelectric segment, in contrast to atrial flutter and macroreentrant AT because atrial activation from a focal source occurs through a small portion of the tachycardia cycle
- When 1:1 conduction to the ventricles is present, the arrhythmia can resemble sinus tachycardia typically with a P-R interval shorter than the R-P interval, particularly when sympathetic tone results in rapid AV nodal conduction
- It can be distinguished from sinus tachycardia by the P-wave morphology, which usually differs from sinus P waves depending on the location of the focus
4.1 ECG Findings¶
- P waves are often discrete with an intervening isoelectric segment
- P-wave morphology differs from sinus P waves depending on location of the focus
- AT from atrial septum will frequently have a narrower P-wave duration than sinus rhythm
- AT from left atrium will usually have a monophasic, positive P wave in lead V and negative P waves in I and aVL
- AT from superior atrial locations (superior vena cava or superior pulmonary veins) will be positive in inferior limb leads II, III, and aVF
- AT from more inferior location (ostium of coronary sinus) will inscribe negative P waves in these same leads
- When focus is in superior aspect of crista terminalis close to sinus node, P wave will resemble that of sinus tachycardia
- Abrupt onset and offset favor AT rather than sinus tachycardia
- Depending on the atrial rate, the P wave may fall on top of the T wave, or during 2:1 conduction
4.2 Symptom Variability¶
- Symptoms from AT are highly variable
- Symptoms are similar to other supraventricular tachycardias (SVTs)
- Incessant AT can cause tachycardia-induced cardiomyopathy
5. DIFFERENTIAL DIAGNOSIS¶
- Sinus tachycardia
- Inappropriate sinus tachycardia
- Postural orthostatic tachycardia syndrome (POTS)
- Atrioventricular nodal reentry tachycardia (AVNRT)
- Atrioventricular reentry tachycardia (AVRT)
- Atrial flutter
- Macroreentrant AT
5.1 Distinguishing Features¶
- AT vs Sinus Tachycardia:
- AT can be distinguished from sinus tachycardia by P-wave morphology, which usually differs from sinus P waves depending on location of the focus
- When 1:1 conduction to the ventricles is present, the arrhythmia can resemble sinus tachycardia typically with a P-R interval shorter than the R-P interval, particularly when sympathetic tone results in rapid AV nodal conduction
- Abrupt onset and offset favor AT rather than sinus tachycardia
- AT vs AV Nodal-Dependent SVTs:
- AT will not terminate with AV block
- The atrial rate will not be affected when AV block occurs
- This distinguishes AT from most AV nodal–dependent SVTs, such as AV nodal reentry and AV reentry using an accessory pathway
- AT vs Atrial Flutter:
- P waves are often discrete, with an intervening isoelectric segment, in contrast to atrial flutter and macroreentrant AT
- Atrial activation from a focal source occurs through a small portion of the tachycardia cycle
- AT vs Inappropriate Sinus Tachycardia/POTS:
- Recognition of these distinct clinical syndromes is critical for treatment
- Sinus node modification will be ineffective for the treatment of POTS and will possibly exacerbate the nontachycardia components of the condition
- Treatment strategies aimed at increasing blood pressure will not be appropriate for inappropriate sinus tachycardia
5.2 R-P Relationships¶
- AT typically presents with 1:1 AV conduction or with AV block in a Wenckebach or fixed (e.g., 2:1 or 3:1) pattern
- Typical relation of the P wave to QRS, commonly described as the R-P to P-R relationship, for different tachycardia mechanisms:
- AT: R-P P-R
- AV node reentry (uncommon form): R-P > P-R
6. INVESTIGATIONS & DIAGNOSIS¶
- Ambulatory electrocardiogram (ECG) recordings
- Nonsustained focal AT is commonly observed on ambulatory ECG recordings
- The prevalence increases with age
- Asymptomatic nonsustained ATs are often labeled as 'SVT' on monitor reports
- Treatment is not recommended for asymptomatic nonsustained AT identified on ECG monitoring
- ECG findings:
- P-wave morphology differs from sinus P waves depending on location of the focus
- P waves are often discrete, with an intervening isoelectric segment
- AT from atrial septum will frequently have a narrower P-wave duration than sinus rhythm
- AT from left atrium will usually have a monophasic, positive P wave in lead V and negative P waves in I and aVL
- AT from superior atrial locations (superior vena cava or superior pulmonary veins) will be positive in inferior limb leads II, III, and aVF
- AT from more inferior location (ostium of coronary sinus) will inscribe negative P waves in these same leads
- When focus is in superior aspect of crista terminalis close to sinus node, P wave will resemble that of sinus tachycardia
- Abrupt onset and offset favor AT rather than sinus tachycardia
- Depending on the atrial rate, the P wave may fall on top of the T wave, or during 2:1 conduction
- Digitalis toxicity:
- AT with atrioventricular (AV) block is characteristic of digitalis toxicity
6.1 Diagnostic Criteria¶
- Focal AT diagnosis requires:
- Sustained or nonsustained atrial tachycardia
- P-wave morphology differing from sinus P waves
- Location of focus approximated by P-wave morphology
- Absence of AV nodal dependence (AT will not terminate with AV block)
- Warm-up or cool-down phase favors AT rather than AV nodal–dependent SVT
- Asymptomatic nonsustained AT:
- Often labeled as 'SVT' on monitor reports
- Treatment is not recommended for asymptomatic nonsustained AT identified on ECG monitoring
6.2 Diagnostic Algorithm¶
- Step 1: Identify atrial tachycardia on ECG
- Step 2: Assess P-wave morphology to determine focus location
- Step 3: Evaluate for AV nodal dependence
- Step 4: Look for warm-up or cool-down phase
- Step 5: Consider underlying causes (fibrosis, digitalis toxicity, etc.)
- Step 6: Determine if treatment is indicated (symptomatic vs asymptomatic)
7. MANAGEMENT & TREATMENT¶
- Treatment strategy to reduce symptoms
- Catheter ablation:
- Areas of fibrosis can act as a nidus for abnormal automaticity from injured but partially living cells
- Microreentry in zones of slow conduction within and on the border of fibrotic areas
- Targeted with prior catheter ablation
- Sinus node modification:
- Will be ineffective for the treatment of POTS
- Will possibly exacerbate the nontachycardia components of the condition
- Treatment strategies aimed at increasing blood pressure:
- Will not be appropriate for inappropriate sinus tachycardia
- Digitalis toxicity:
- AT with AV block is characteristic of digitalis toxicity
- Requires discontinuation of digitalis and appropriate management of toxicity
7.1 Catheter Ablation¶
- Focal AT accounts for approximately 10% of PSVTs in patients referred for catheter ablation
- Areas of fibrosis can act as a nidus for abnormal automaticity from injured but partially living cells
- Microreentry in zones of slow conduction within and on the border of fibrotic areas
- Targeted with prior catheter ablation
7.2 Treatment Limitations¶
- Sinus node modification:
- Will be ineffective for the treatment of POTS
- Will possibly exacerbate the nontachycardia components of the condition
- Treatment strategies aimed at increasing blood pressure:
- Will not be appropriate for inappropriate sinus tachycardia
8. PROGNOSIS & COMPLICATIONS¶
- Incessant AT can cause tachycardia-induced cardiomyopathy
- Frequent atrial ectopy and nonsustained AT are often precursors to more significant arrhythmias such as atrial fibrillation and atrial flutter
- AT can occur in the absence of structural heart disease or may be associated with any condition that causes atrial fibrosis
- The emergence of AT can be a sign of underlying illness or drug toxicity
8.1 Tachycardia-Induced Cardiomyopathy¶
- Incessant AT can cause tachycardia-induced cardiomyopathy
- Requires appropriate management and treatment strategy to reduce symptoms
8.2 Progression to Other Arrhythmias¶
- Frequent atrial ectopy and nonsustained AT are often precursors to more significant arrhythmias
- Such as atrial fibrillation and atrial flutter
- Areas of fibrosis can act as a nidus for abnormal automaticity from injured but partially living cells
9. SPECIAL CONSIDERATIONS¶
- Digitalis toxicity:
- AT with atrioventricular (AV) block is characteristic of digitalis toxicity
- Requires discontinuation of digitalis and appropriate management of toxicity
- Underlying illness:
- The emergence of AT can be a sign of underlying illness or drug toxicity
- Structural heart disease:
- AT can occur in the absence of structural heart disease
- Or may be associated with any condition that causes atrial fibrosis
10. KEY PEARLS & CLINICAL TRAPS¶
- AT will not terminate with AV block, distinguishing it from AV nodal-dependent SVTs
- A so-called warm-up phase when the atrial activation rate increases after initiation or a cool-down phase when the rate slows prior to termination also favors AT rather than AV nodal–dependent SVT
- P waves are often discrete, with an intervening isoelectric segment, in contrast to atrial flutter and macroreentrant AT
- AT with AV block is characteristic of digitalis toxicity
- Treatment is not recommended for asymptomatic nonsustained AT identified on ECG monitoring
- Sinus node modification will be ineffective for the treatment of POTS and will possibly exacerbate the nontachycardia components of the condition
- Treatment strategies aimed at increasing blood pressure will not be appropriate for inappropriate sinus tachycardia
- Recognition of these distinct clinical syndromes is critical for treatment
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
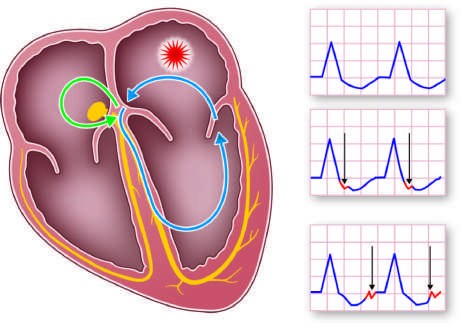
Caption: FIGURE 255-1 Common mechanisms underlying paroxysmal supraventricular view of the heart with atrioventricular (AV) node and specialized conduction tissue tissue. Atrioventricular nodal reentry tachycardia (AVNRT; green circuit) uses AV nodal uses atrial and ventricular tissue, accessory pathway between the ventricle and atrium, the P wave to QRS, commonly described as the R-P to P-R relationship, for the different — Figure 255-1: Common mechanisms underlying paroxysmal supraventricular tachycardia along with typical R-P relationships. Schematic showing four-chamber view of heart with atrioventricular (AV) node and specialized conduction tissue (His-Purkinje) in yellow. Atrial tachycardia (AT; red circuit) confined completely to atrial tissue. Atrioventricular nodal reentry tachycardia (AVNRT; green circuit) uses AV nodal and perinodal atrial tissue. Atrioventricular reentry tachycardia (AVRT; blue circuit) uses atrial and ventricular tissue, accessory pathway between ventricle and atrium, AV node, and His-Purkinje tissue as part of reentry circuit. Typical relation of P wave to QRS, commonly described as R-P to P-R relationship, for different tachycardia mechanisms.
Figure 2¶
Caption: FIGURE 255-1 Common mechanisms underlying paroxysmal supraventricular view of the heart with atrioventricular (AV) node and specialized conduction tissue tissue. Atrioventricular nodal reentry tachycardia (AVNRT; green circuit) uses AV nodal uses atrial and ventricular tissue, accessory pathway between the ventricle and atrium, the P wave to QRS, commonly described as the R-P to P-R relationship, for the different — Figure 255-2: P-wave morphology in focal atrial tachycardia depending on location of focus. AT from atrial septum will frequently have narrower P-wave duration than sinus rhythm. AT from left atrium will usually have monophasic, positive P wave in lead V and negative P waves in I and aVL, indicating activation wavefront away from left atrial free wall. AT from superior atrial locations (superior vena cava or superior pulmonary veins) will be positive in inferior limb leads II, III, and aVF, whereas AT from more inferior location (ostium of coronary sinus) will inscribe negative P waves in these same leads.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.