Relapsing Polychondritis¶
Chapter 378 | Part 11: Immune-Mediated, Inflammatory, and Rheumatologic Disorders · Part 11 – Rheumatology & Immunology
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Relapsing polychondritis (RP) is a rare systemic disease characterized by recurrent inflammation in cartilaginous structures.
- Hallmark features involve the ears, nose, respiratory tract, and joints; other organs (eyes, inner ear, nervous system, skin, cardiovascular) can be affected.
- VEXAS syndrome (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) is associated with acquired hematologic mutations in UBA1 in older male patients with severe systemic inflammation and progressive bone marrow failure.
- Diagnosis is based primarily on clinical pattern recognition; there are no circulating or tissue-based biomarkers with adequate performance characteristics.
- McAdam's criteria require presence of three of six symptoms: bilateral auricular chondritis, nonerosive seronegative inflammatory polyarthritis, nasal chondritis, ocular inflammation, respiratory tract chondritis, or vestibular/cochlear dysfunction.
- Damiani and Levine modified McAdam's criteria to include either three clinical features or one clinical feature with histologic evidence of chondritis or two clinical features with clinical response to glucocorticoids, dapsone, or both.
- Michet's criteria propose three major criteria (inflammation of ear, nose, or respiratory tract) and four minor criteria (ocular inflammation, hearing loss, vestibular dysfunction, and seronegative inflammatory arthritis); diagnosis requires two major criteria or one major plus two minor criteria.
- GPA can be differentiated from RP by the presence of antineutrophil cytoplasmic autoantibodies (ANCA) and glomerulonephritis, which are not features of RP.
- Airway involvement (subglottic stenosis, tracheomalacia, tracheal calcification) can result in stridor and requires urgent medical attention to avoid mortality.
- Ocular involvement: Episcleritis is the most frequent type; scleritis mandates urgent ophthalmologic evaluation due to potential vision loss, scleromalacia, or global rupture.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 VEXAS Syndrome
- 4. CLINICAL FEATURES
- 4.1 Ears, Nose, and Throat
- 4.2 Musculoskeletal
- 4.3 Inner Ear
- 4.4 Ocular Involvement
- 4.5 Cardiovascular
- 4.6 Neurologic
- 4.7 Upper and Lower Airway
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Diagnostic Criteria
- 5.2 Differential Diagnosis
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria
- 6.2 Investigations
- 7. MANAGEMENT & TREATMENT
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- WHAT EXCLUDES THE DIAGNOSIS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Airway involvement in relapsing polychondritis |
| 2 | 🖼 Figure | Airway involvement in relapsing polychondritis |
| 3 | 🖼 Figure | Airway involvement in relapsing polychondritis |
| 4 | 🖼 Figure | (Continued) |
| 5 | 🖼 Figure | (Continued) |
| 6 | 🖼 Figure | Representation of ear involvement in relapsing polychondritis |
| 7 | 🖼 Figure | (Continued) |
| 8 | 🖼 Figure | Representation of ear involvement in relapsing polychondritis |
| 9 | 🖼 Figure | (Continued) |
| 10 | 🖼 Figure | Figure / Illustration |
1. DEFINITION & OVERVIEW¶
- Relapsing polychondritis (RP) is a rare systemic disease characterized by recurrent inflammation in cartilaginous structures.
- Involvement of the ears, nose, respiratory tract, and joints are hallmark features of the disease.
- Other organs can be affected including the eyes, inner ear, nervous system, skin, and cardiovascular system.
- Some patients with RP may be concomitantly diagnosed with other rheumatologic diseases, such as Sjögren's syndrome or systemic lupus erythematosus.
- Recurrent chondritis of the ears and nose in older male patients with severe systemic inflammation and progressive bone marrow failure is associated with acquired hematologic mutations in UBA1, a condition now known as the VEXAS (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) syndrome.
- Prompt recognition and accurate diagnosis of RP or VEXAS syndrome are essential to prevent life-threatening complications of these diseases.
2. EPIDEMIOLOGY¶
- The epidemiology of RP is poorly characterized.
- The disease is commonly reported to primarily affect middle-aged adults without a strong sex predilection.
- Some cohort studies report female predilection, however, these findings are not consistent and, therefore, are not routinely measured to guide management in clinical practice.
- Children can be affected; however, these data are limited to case reports.
- Rare instances of familial aggregation have also been reported.
- The estimated incidence rate of disease is 0.7–3.5 cases per million per year.
- Prevalence estimates range from 4.5–25 cases per million.
- Epidemiologic data in RP are limited to older studies, typically evaluating population distributions more than three decades ago in cohorts from Europe and North America.
- Given the diagnostic challenges encountered in this condition, these data may underestimate the true prevalence of disease.
- Although RP has been reported in many regions of the world, whether racial or ethnic differences are associated with variable clinical features or outcomes is not known.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Although genetic, environmental, and immunologic aspects of the disease have been studied in humans and in animal models, the exact mechanisms that drive the disease are unclear.
- Limited studies in animal models support the concept that autoimmunity to cartilage components may play a role in RP.
- Immunization of specific animals to type II collagen, type IX collagen, or matrillin-1 can recapitulate various aspects of the clinical phenotypes observed in patients with RP.
- However, the performance characteristics of these antibodies in clinical practice are poor to differentiate RP from other diseases.
- Autoantibodies to type II collagen have been reported in small cohorts of patients with RP but are neither sensitive nor specific to be considered as an acceptable diagnostic marker of disease.
- Observational cohort data suggest that B-cell–depleting therapies are not particularly effective to treat the condition, arguing against a strong primary role of antibody-mediated disease.
- Acute phase reactants (e.g., erythrocyte sedimentation rate or C-reactive protein) are not reliably elevated in patients with RP.
- Proinflammatory cytokines and chemokines related to both innate and adaptive immunity have been identified in association with RP.
3.1 VEXAS Syndrome¶
- Recurrent chondritis of the ears and nose in older male patients with severe systemic inflammation and progressive bone marrow failure is associated with acquired hematologic mutations in UBA1.
- This condition is now known as the VEXAS (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) syndrome.
- Presence of cytopenia, most notably macrocytosis and lymphopenia, in older male patients should trigger consideration of genetic testing and bone marrow assessment for VEXAS.
4. CLINICAL FEATURES¶
- RP is associated with a wide range of clinical manifestations.
- In the absence of a diagnostic blood test, a detailed medical history and physical examination are the most essential tools for diagnosis and, most importantly, further management.
- Because disease activity is intermittent and patients may not exhibit clear signs of inflammation during direct evaluation, it is crucial to consider the patient's symptoms over time and to review any provided photographic documentation of disease features.
4.1 Ears, Nose, and Throat¶
- Ear involvement is one of the most common clinical manifestations of relapsing polychondritis, affecting 80–90% of the patients.
- There are no clear definitions of ear chondritis, and patient descriptions of pain and associated symptoms are variable.
- The typical description includes involvement of only the cartilaginous aspect of the ear (pinnae).
- A subset of patients may report pain in the ears with minimal associated findings visualized on physical examination, such as mild swelling or erythema.
- Although damage to the cartilaginous portion of the external ear (i.e., 'cauliflower ear') is observed in RP, it is present only in a small number of patients, usually in the setting of recurrent episodes of ear inflammation.
- Questions that can be helpful to elicit the nature of ear pain include asking about onset, duration, and triggers.
- Common triggers include minimal trauma to the ear (such as from lying on the effected side or wearing glasses) or temperature changes.
- Patients usually describe a sensation of pressure at the bridge of the nose that may not be accompanied by other associated symptoms.
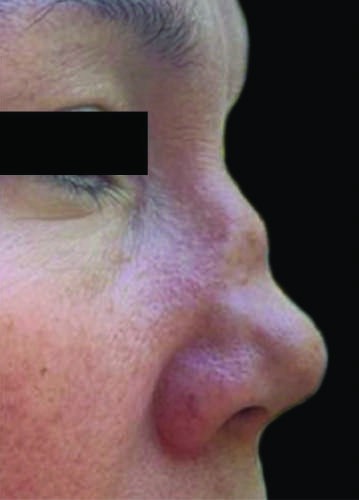
- Some patients may have overt redness and swelling of the bridge or tip of nose, but this is less common.
- While a 'saddle nose' has been described as a typical clinical finding in RP, many patients will not develop an obvious nasal deformity.
- The nasal septum and nasal passages should always be evaluated in patients with suspected RP, as many patients can have septal ulcers and mucosal inflammation.
- In contrast to granulomatosis with polyangiitis (GPA) where a saddle nose deformity is usually associated with a septal perforation, patients with RP who have a saddle nose deformity usually do not have a septal perforation, as most of the nasal perforations in patients with RP are located anteriorly.
- Patients can have complaints of throat pain or a sensation of globus, usually described as a 'choking sensation.'
- Patients can also report pain on the anterior aspect of the neck, in some cases associated with erythema, usually located at the level of the thyroid cartilage.
4.2 Musculoskeletal¶
- RP is associated with a nonerosive inflammatory arthritis that can affect small and large peripheral joints and as well as the axial skeleton.
- Erosions have been described in the sacroiliac joints but not in other joints.
- The most common large joint affected is the knees, often presenting with effusions.
- The pattern of small joint involvement emulates rheumatoid arthritis, without erosions or deformities.
- Different tendons can be affected including Achilles and peroneal tendons.
- Located at the rib-sternum junction, costochondral joints are frequently inflamed in RP, producing constant pain that stands out due to its unique severe quality.
- Pain due to costochondritis can be so severe that patients will seek evaluation in the emergency room due to concerns for an acute coronary event.
- The pain is bilateral, reproducible with palpation, and not associated with movement of the affected rib.
4.3 Inner Ear¶
- All patients with RP should undergo hearing tests to evaluate for conductive and sensorineural hearing loss.
- During the physical exam, the ear canal should be evaluated as some patients can have severe inflammation or eustachian tube dysfunction leading to conductive hearing loss.
- The presence of dizziness necessitates further evaluation through maneuvers like finger-to-nose, Romberg, and nystagmus to rule out vestibular involvement.
4.4 Ocular Involvement¶
- Episcleritis is the most frequent type of ocular inflammation in RP.
- It might coincide with other flare symptoms or occur independently.
- Although rare, features suggesting scleritis mandate urgent ophthalmologic evaluation due to its potential catastrophic outcomes, including vision loss, scleromalacia, or global rupture necessitating enucleation.
4.5 Cardiovascular¶
- Patients with mouth and genital ulcers with inflamed cartilage (MAGIC) syndrome may exhibit symptoms seen in Behçet's syndrome, including pathergy and gastrointestinal involvement.
- These patients can also have large-vessel vasculitis involving the aorta.
4.6 Neurologic¶
- The diagnosis of neurologic involvement due to RP is one of exclusion.
- All possible etiologies including infection and malignancy should be ruled out before attributing the clinical findings to RP.
- However, encephalitis and meningitis can be seen in RP.
4.7 Upper and Lower Airway¶
- Conditions like subglottic stenosis may manifest acutely or subacutely, leading to cough, voice changes, or breathlessness.
- Severe narrowing can result in stridor, requiring urgent medical attention to avoid mortality.
- Often misdiagnosed as adult-onset asthma, timely recognition of airway involvement is important to prevent chronic damage to the large airways, which can result in tracheomalacia, bronchomalacia, or tracheal calcification.
- Patients with intermittent episodes of wheezing should be followed closely and further evaluated for lower airway involvement.
- Audiometry to assess hearing loss and dynamic expiratory phase computed tomography of the chest to assess tracheobronchomalacia are critical studies that should be performed in all patients with suspected RP.
5. DIFFERENTIAL DIAGNOSIS¶
- There are no circulating or tissue-based biomarkers with adequate performance characteristics to function as a diagnostic test for RP.
- As such, diagnosis is based primarily on clinical pattern recognition informed by a comprehensive review of systems and physical examination.
- Several diagnostic criteria have been proposed; however, these criteria were developed in small cohorts, are largely based on expert opinion, and have not been formally validated.
5.1 Diagnostic Criteria¶
- McAdam's criteria require presence of three of six symptoms, including bilateral auricular chondritis, nonerosive seronegative inflammatory polyarthritis, nasal chondritis, ocular inflammation, respiratory tract chondritis, or vestibular/cochlear dysfunction.
- Damiani and Levine modified McAdam's criteria to include either three clinical features or one clinical feature with histologic evidence of chondritis or two clinical features with clinical response to glucocorticoids, dapsone, or both.
- Michet's criteria propose three major criteria (inflammation of ear, nose, or respiratory tract) and four minor criteria (ocular inflammation, hearing loss, vestibular dysfunction, and seronegative inflammatory arthritis) and require fulfillment of two major criteria or one major plus two minor criteria to establish the diagnosis.
- Another important limitation of these criteria is the lack of precise definitions of organ involvement.
5.2 Differential Diagnosis¶
- The differential diagnosis for RP includes conditions that mimic chondritis in specific cartilaginous organs and systemic diseases for which chondritis may be a manifestation.
- Ear chondritis can be mimicked by infectious and cutaneous diseases of the external ear, traumatic otohematoma, or red ear syndrome.
- Various infectious diseases and angiocentric centrofacial lymphoma can mimic nasal chondritis.
- Asthma, traumatic airway stenosis, infectious diseases, and congenital disorders involving the airway can mimic airway chondritis.
- Systemic diseases that mimic RP include GPA and autoinflammatory diseases.
- GPA can be differentiated from RP in part by the presence of antineutrophil cytoplasmic autoantibodies (ANCA) and glomerulonephritis, which are not features of RP.
- Presence of cytopenia, most notably macrocytosis and lymphopenia, in older male patients should trigger consideration of genetic testing and bone marrow assessment for VEXAS.
6. INVESTIGATIONS & DIAGNOSIS¶
- There are no circulating or tissue-based biomarkers with adequate performance characteristics to function as a diagnostic test for RP.
- As such, diagnosis is based primarily on clinical pattern recognition informed by a comprehensive review of systems and physical examination.
- Several diagnostic criteria have been proposed; however, these criteria were developed in small cohorts, are largely based on expert opinion, and have not been formally validated.
6.1 Diagnostic Criteria¶
- McAdam's criteria require presence of three of six symptoms, including bilateral auricular chondritis, nonerosive seronegative inflammatory polyarthritis, nasal chondritis, ocular inflammation, respiratory tract chondritis, or vestibular/cochlear dysfunction.
- Damiani and Levine modified McAdam's criteria to include either three clinical features or one clinical feature with histologic evidence of chondritis or two clinical features with clinical response to glucocorticoids, dapsone, or both.
- Michet's criteria propose three major criteria (inflammation of ear, nose, or respiratory tract) and four minor criteria (ocular inflammation, hearing loss, vestibular dysfunction, and seronegative inflammatory arthritis) and require fulfillment of two major criteria or one major plus two minor criteria to establish the diagnosis.
- Another important limitation of these criteria is the lack of precise definitions of organ involvement.
6.2 Investigations¶
- Acute phase reactants (e.g., erythrocyte sedimentation rate or C-reactive protein) are not reliably elevated in patients with RP.
- Autoantibodies to type II collagen have been reported in small cohorts of patients with RP but are neither sensitive nor specific to be considered as an acceptable diagnostic marker of disease.
- Audiometry to assess hearing loss and dynamic expiratory phase computed tomography of the chest to assess tracheobronchomalacia are critical studies that should be performed in all patients with suspected RP.
- Biopsy of affected cartilage may cause morbidity, and there are no features on histology that are specifically diagnostic for RP.
- Therefore, biopsy is often reserved when there is a high suspicion of conditions that mimic RP, particularly infectious diseases and malignancies.
- Histologic findings from biopsy of affected cartilage are dependent on the timing of tissue sampling.
- In acute disease, a mixed inflammatory infiltrate of myeloid and lymphoid populations is observed at the cartilage interface.
- Over time, cartilage destruction is marked by lacunar breakdown and loss of chondrocytes, replaced by fibrosis.
7. MANAGEMENT & TREATMENT¶
- Management details are not described in the provided source text.
8. PROGNOSIS & COMPLICATIONS¶
- Prompt recognition and accurate diagnosis of RP or VEXAS syndrome are essential to prevent life-threatening complications of these diseases.
9. SPECIAL CONSIDERATIONS¶
- Children can be affected; however, these data are limited to case reports.
- Rare instances of familial aggregation have also been reported.
10. KEY PEARLS & CLINICAL TRAPS¶
- Questions that can be helpful to elicit the nature of ear pain include asking about onset, duration, and triggers.
- Common triggers include minimal trauma to the ear (such as from lying on the effected side or wearing glasses) or temperature changes.
- Patients usually describe a sensation of pressure at the bridge of the nose that may not be accompanied by other associated symptoms.
- While a 'saddle nose' has been described as a typical clinical finding in RP, many patients will not develop an obvious nasal deformity.
- The diagnosis of neurologic involvement due to RP is one of exclusion.
- All possible etiologies including infection and malignancy should be ruled out before attributing the clinical findings to RP.
- However, encephalitis and meningitis can be seen in RP.
WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Hallmark features of the disease involve the ears, nose, respiratory tract, and joints.
- Other organs can be affected including the eyes, inner ear, nervous system, skin, and cardiovascular system.
- Recurrent chondritis of the ears and nose in older male patients with severe systemic inflammation and progressive bone marrow failure is associated with acquired hematologic mutations in UBA1, a condition now known as the VEXAS syndrome.
- Questions that can be helpful to elicit the nature of ear pain include asking about onset, duration, and triggers.
- Common triggers include minimal trauma to the ear (such as from lying on the effected side or wearing glasses) or temperature changes.
- Patients usually describe a sensation of pressure at the bridge of the nose that may not be accompanied by other associated symptoms.
- Although damage to the cartilaginous portion of the external ear (i.e., 'cauliflower ear') is observed in RP, it is present only in a small number of patients, usually in the setting of recurrent episodes of ear inflammation.
- While a 'saddle nose' has been described as a typical clinical finding in RP, many patients will not develop an obvious nasal deformity.
- Patients with RP who have a saddle nose deformity usually do not have a septal perforation, as most of the nasal perforations in patients with RP are located anteriorly.
- Features suggesting scleritis mandate urgent ophthalmologic evaluation due to its potential catastrophic outcomes, including vision loss, scleromalacia, or global rupture necessitating enucleation.
WHAT EXCLUDES THE DIAGNOSIS¶
- The diagnosis of neurologic involvement due to RP is one of exclusion.
- All possible etiologies including infection and malignancy should be ruled out before attributing the clinical findings to RP.
- GPA can be differentiated from RP in part by the presence of antineutrophil cytoplasmic autoantibodies (ANCA) and glomerulonephritis, which are not features of RP.
- Presence of cytopenia, most notably macrocytosis and lymphopenia, in older male patients should trigger consideration of genetic testing and bone marrow assessment for VEXAS.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

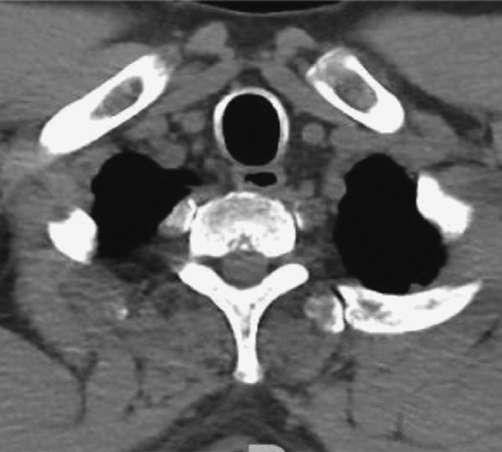
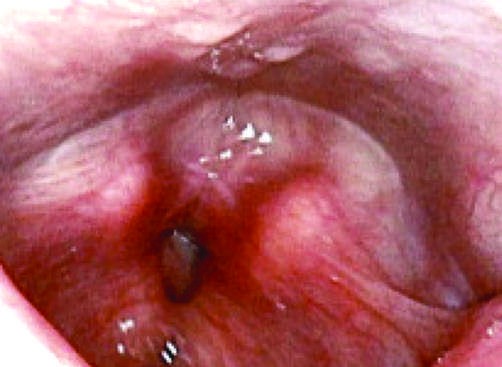
Caption: FIGURE 378-3 Airway involvement in relapsing polychondritis. A. Subglottic stenosis. B and C. Computed tomography demonstrating tracheal calcification and tracheomalacia. — Title page image for Chapter 378: Relapsing Polychondritis.
Figure 2¶
Caption: FIGURE 378-3 Airway involvement in relapsing polychondritis. A. Subglottic stenosis. B and C. Computed tomography demonstrating tracheal calcification and tracheomalacia. — Figure 378-1A and B: Examples of typical ear chondritis in relapsing polychondritis, showing significant inflammation of the pinnae.
Figure 3¶
Caption: FIGURE 378-3 Airway involvement in relapsing polychondritis. A. Subglottic stenosis. B and C. Computed tomography demonstrating tracheal calcification and tracheomalacia. — Figure 378-1C and D: Mild ear cartilage inflammation and cartilage damage (cauliflower ear) in relapsing polychondritis.
Figure 4¶

Caption: FIGURE 378-1 (Continued) — Figure 378-2A: Redness and swelling of the base and tip of the nose in relapsing polychondritis.
Figure 5¶
Caption: FIGURE 378-1 (Continued) — Figure 378-2B: Saddle nose deformity in relapsing polychondritis.
Figure 6¶

Caption: FIGURE 378-1 Representation of ear involvement in relapsing polychondritis. A and B. C. Mild ear cartilage inflammation. D. Cartilage damage. — Figure 378-3A: Subglottic stenosis in relapsing polychondritis.
Figure 7¶

Caption: FIGURE 378-1 (Continued) — Figure 378-3B and C: Computed tomography demonstrating tracheal calcification and tracheomalacia in relapsing polychondritis.
Figure 8¶

Caption: FIGURE 378-1 Representation of ear involvement in relapsing polychondritis. A and B. C. Mild ear cartilage inflammation. D. Cartilage damage. — Figure 378-5A: Ocular inflammation (episcleritis or scleritis) in relapsing polychondritis.
Figure 9¶

Caption: FIGURE 378-1 (Continued) — Figure 378-1 (Continued): Additional views of ear involvement in relapsing polychondritis.
Figure 10¶
Caption: Figure 378-3 (Continued): Additional views of airway involvement in relapsing polychondritis.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.