UrinaryTract Obstruction¶
Chapter 331 | Harrison's 22e · Part 9 – Renal & Urinary Tract Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Diagnostic approach for urinary tract obstruction in unexplained renal |
RAW CONTENT¶
[PAGE 2453] Urinary Tract Obstruction 2453 CHAPTER 331 Calcium Phosphate Calcium phosphate stones share risk factors acetohydroxamic acid can be considered; however, this agent should with calcium oxalate stones, including higher concentrations of urine be used with caution because of potential side effects. calcium and lower concentrations of urine citrate, but additional fac- tors deserve attention. Higher urine phosphate levels and higher urine ■ LONG-TERM FOLLOW-UP pH (typically ≥6.5) are associated with an increased likelihood of cal- In general, the preventive regimens described above do not cure the cium phosphate stone formation. Calcium phosphate stones are more underlying pathophysiologic process. Thus, these recommendations common in patients with distal renal tubular acidosis and primary typically need to be followed for the patient’s lifetime, and it is essential hyperparathyroidism. to tailor recommendations in a way that is acceptable to the patient. There are no randomized trials on which to base preventive recom- Because the memory of the acute stone event fades and patients often mendations for calcium phosphate stone formers, so the interventions return to old habits (e.g., insufficient fluid intake), long-term follow- are focused on modification of the recognized risk factors. Thiazide up, including repeat 24-h urine collections typically annually, is impor- diuretics (with sodium restriction) may be used to reduce urine cal- tant to ensure that the preventive regimen has been implemented and cium, as described above for calcium oxalate stones. In patients with has resulted in the desired reduction in the risk of new stone formation. low urine citrate levels, alkali supplements (e.g., potassium citrate or Follow-up imaging should be planned thoughtfully. Many patients bicarbonate) may be used to increase urine citrate. However, the urine with recurrent episodes of renal colic that lead to emergency room pH of these patients should be monitored initially because supple- visits often undergo repeat CT studies. While CT does provide the mental alkali can raise urine pH, thereby potentially increasing the best information, the radiation dose is higher than that with plain risk of stone formation. Because these patients tend to have a urinary abdominal radiography (KUB). Small stones may be missed by KUB, acidification defect, reducing the urine pH is not an option. Reduction and ultrasound has a limited ability to determine the size and num- of dietary phosphate may be beneficial by reducing urine phosphate ber of stones. Minimizing radiation exposure should be a goal of the excretion. long-term follow-up plan and must be balanced against the gain in diagnostic information. Uric Acid The two main risk factors for uric acid stones are per- ■ FURTHER READING sistently low urine pH and higher uric acid excretion. Urine pH is the Coe FL: The physiology of kidney stone prevention: A narrative for predominant influence on uric acid solubility; therefore, the mainstay patients and physicians. Available at https://bpb-us-w2.wpmucdn.com/ of prevention of uric acid stone formation entails increasing urine pH. voices.uchicago.edu/dist/c/3637/files/2022/10/KIDNEY-STONES_- Alkalinizing the urine can be achieved by increasing the intake of foods Pathogenesis-and-Prevention.pdf. Accessed November 2, 2023. rich in alkali (e.g., fruits and vegetables) and reducing the intake of Coe FL, Worcester EM, Evan AP, Lingeman JE (eds): Kidney Stones: foods that produce acid (e.g., animal flesh). If necessary, supplementa- Medical and Surgical Management, 2nd ed. New Dehli, Jaypee Brothers tion with bicarbonate or citrate salts (preferably potassium-based) can Medical Publishing, 2019. be used to reach the recommended pH goal of 6.5 throughout the day European Association of Urology Guidelines on Urolithiasis. Available and night. at https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU- Urine uric acid excretion is determined by uric acid generation. Guidelines-on-Urolithiasis-2023.pdf. Accessed November 22, 2023. Uric acid is the end product of purine metabolism; thus, reduced Pearle MS et al: Medical management of kidney stones: AUA guide- consumption of purine-containing foods can lower urine uric acid line. J Urol 192:316, 2014. excretion. It is noteworthy that the serum uric acid level is dependent on the fractional excretion of uric acid and, therefore, does not provide information on urine uric acid excretion. For example, an individual with high uric acid generation and concurrent high fractional excre- tion of uric acid will have high urine uric acid excretion with a normal (or even low) serum uric acid level. If alkalinization of the urine alone is not successful and if dietary modifications do not reduce urine uric acid sufficiently, then the addition of a xanthine oxidase inhibitor, such 331 Urinary Tract Obstruction as allopurinol or febuxostat, can reduce urine uric acid excretion by 40–50%. Julian L. Seifter Cystine Cystine excretion is not easily modified. Long-term dietary cystine restriction is not feasible and is unlikely to be successful; thus, the focus for cystine stone prevention is on increasing cystine solu- Obstruction to the flow of urine, with attendant stasis and elevation bility. This goal may be achieved by treatment with medication that in urinary tract pressure, impairs renal and urinary conduit functions covalently binds to cystine (tiopronin or penicillamine) and a medica- and is a common cause of acute and chronic kidney disease (obstruc- tion that raises urine pH. Tiopronin is the preferred choice owing to its tive nephropathy). Early recognition and prompt treatment of urinary better adverse event profile. The preferred alkalinizing agent to achieve tract obstruction (UTO) can prevent or reverse devastating effects on a urine pH of 7.5 is potassium citrate or bicarbonate as sodium salts kidney structure and function, and decrease susceptibility to hyperten- may increase cystine excretion. As with all stone types, and especially sion, infection, and stone formation. Chronic obstruction may lead to in patients with cystinuria, maintaining a high urine volume is an permanent loss of renal mass (renal atrophy) and excretory capability. essential component of the preventive regimen. Because obstructive disease may be secondary to serious underlying inflammatory, vascular, or malignant disease, familiarity with clinical Struvite Struvite stones, also known as infection stones or triple- findings, appropriate diagnostic testing, and the therapeutic approach phosphate stones, form only when the upper urinary tract is infected is of great importance to the clinician. with urease-producing bacteria such as Proteus mirabilis, Klebsiella Recent developments have advanced our knowledge of fetal and pneumoniae, or Providencia species. Urease produced by these bacteria genetic causes of lower urinary tract obstruction (LUTO) and chronic hydrolyzes urea and may elevate the urine pH to a supraphysiologic anomalies of the kidneys and urinary tracts (CAKUT), the rubric level (>8.0). Struvite stones may grow quickly and fill the renal pelvis for a cluster of developmental uropathies associated with cysts and (staghorn calculi). obstruction. In the last few years, studies in mice, zebrafish, and plu- Struvite stones require complete removal by a urologist. New stone ripotent stem cells (kidney organoids) have identified possible genetic formation can be avoided by the prevention of UTIs. In patients mutations implicated in cases of CAKUT producing low nephron with recurrent upper UTIs (e.g., some individuals with surgically number, including duplications and deletions (copy number vari- altered urinary drainage or spinal cord injury), the urease inhibitor ants) and familial candidate genes (HFN1β, PAX2, SIX1, GATA3, and
[PAGE 2454] 2454 PART 9 Disorders of the Kidney and Urinary Tract many others). Given that there is no nephrog
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
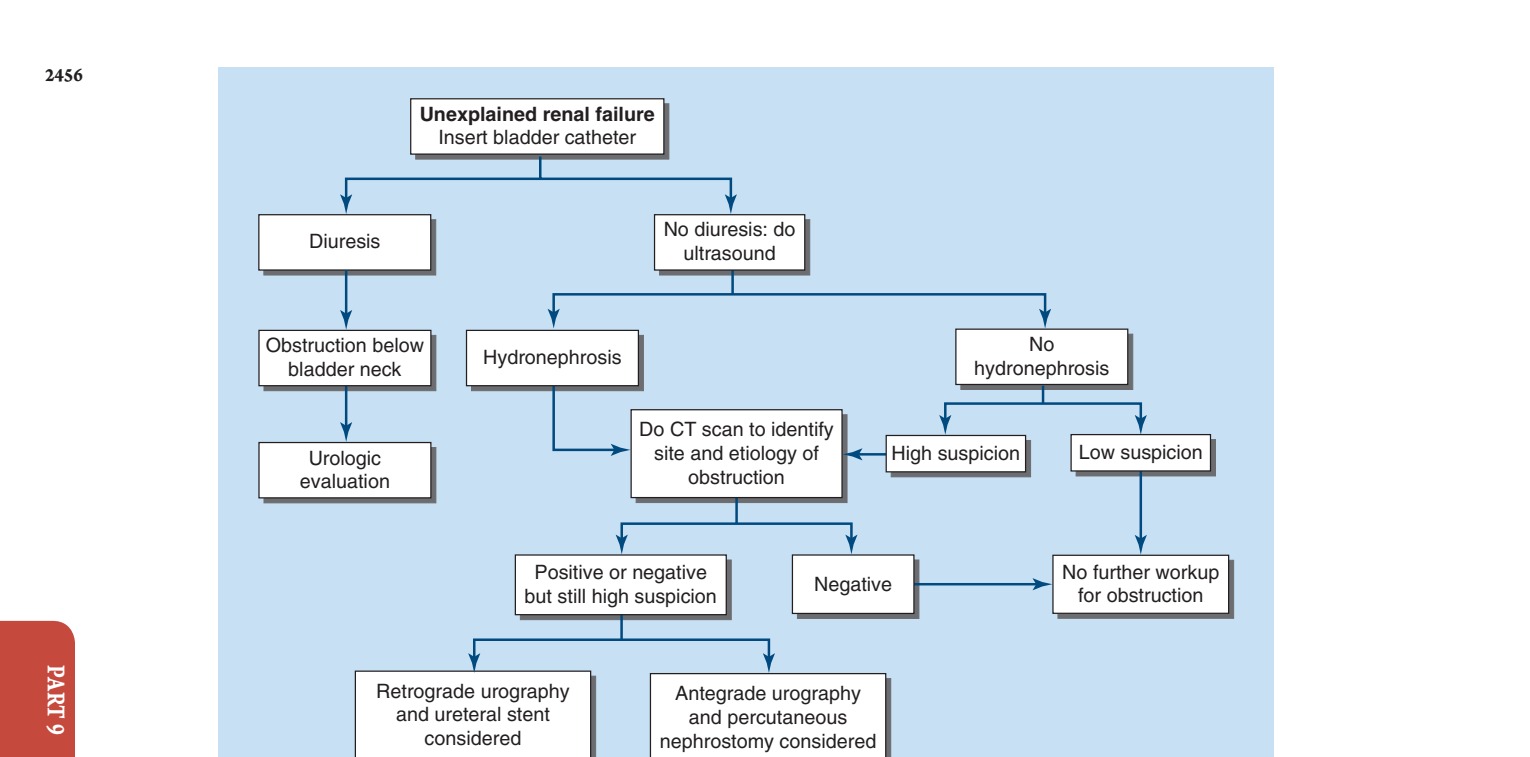
Caption: FIGURE 331-1 Diagnostic approach for urinary tract obstruction in unexplained renal
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.