Chapter 84: Breast Cancer¶
Oncology and Hematology · Part 4 – Oncology: Solid Tumors
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Breast cancer is the most common nonskin cancer diagnosed in women; estimated 310,000 new cases in US women in 2024.
- 5-year relative survival in the US is currently 91% due to advances in screening, diagnosis, and treatment.
- About 70% of breast cancer in the US is diagnosed in women 55 years and older; median age of diagnosis is 63.
- Invasive breast cancer is a disease with diverse subtypes: Luminal A, Luminal B, HER2-positive, and Basal-like (TNBC).
- Screening mammography reduced breast cancer mortality by about 20–25% in women ≥50 years.
- Tamoxifen reduces risk of invasive breast cancer in women at higher risk; aromatase inhibitors reduce risk by about 50% in postmenopausal women.
- Prophylactic mastectomy reduces risk of developing breast cancer by about 90% in individuals with germline mutations.
- Neoadjuvant therapy is considered for individuals with HER2-positive tumors ≥2 cm or node-positive disease.
- Complete pathologic response (pCR) to neoadjuvant therapy is associated with better outcomes than no pCR.
- Routine imaging of other types or blood studies have not been shown to enhance well-being or outcome from breast cancer in asymptomatic survivors.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Epidemiology & Survival Statistics
- 2. EPIDEMIOLOGY & RISK FACTORS
- 2.1 Nongenetic Risk Factors
- 2.2 Genetic Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Molecular Subtypes
- 3.2 In Situ Pathology
- 4. CLINICAL FEATURES
- 4.1 Screening Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Algorithm
- 6.2 Biomarker Evaluation
- 7. MANAGEMENT & TREATMENT
- 7.1 General Guidelines for (Neo)Adjuvant Systemic Therapy Selection
- 7.2 Prevention Strategies
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Long-Term Follow-Up
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy & Germline Mutations
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | shows an algorithm for diagnostic abnormalities noted on physical exam or imaging |
| 2 | 🔀 Flowchart | Evaluation and workup of breast lesions |
| 3 | 🔀 Flowchart | Evaluation of new signs or symptoms in a patient with prior history... |
| 1 | 🖼 Figure | Breast cancer continuum conceptual model |
1. DEFINITION & OVERVIEW¶
- Breast cancer is the most common nonskin cancer diagnosed in women in the world.
- In 2024, estimated 310,000 women in the United States will be diagnosed with invasive breast cancer.
- Over 56,000 women will receive a diagnosis of ductal carcinoma in situ (DCIS).
- About 42,250 women will die from breast cancer in 2024 in the United States.
- About 2,800 men will be diagnosed with and 530 men will die from breast cancer in 2024 in the United States.
- 5-year relative survival in the United States is currently 91%.
- Invasive breast cancer is a disease with diverse subtypes, both histologic and molecular.
- Two decades of molecular analyses have documented multiple transcriptional, epigenetic, and genetic changes that characterize invasive breast cancer.
- Staging is carried out according to the guidelines of the American Joint Committee on Cancer (AJCC) eighth edition.
- Conceptually, stages I and II represent early-stage disease, which is confined to breast and ipsilateral nodes.
- Stage III comprises locally advanced breast cancer.
- Stage IV denotes de novo metastatic breast cancer, designated as M1 in the current staging system.
- Common sites for breast cancer metastasis include soft tissues, lung, bone, liver, and brain.
1.1 Epidemiology & Survival Statistics¶
- Incidence is highest in non-Hispanic whites followed by non-Hispanic blacks.
- Incidence is lower in Hispanic, Asian/Pacific Islander, and American Indian/Alaska Native women.
- Mortality is highest in non-Hispanic blacks followed by non-Hispanic whites.
- Incidence and mortality vary considerably around the globe.
- Studies of immigrant populations show that populations who migrate from low-incidence regions to high-incidence regions will attain the breast cancer risk of the higher incidence region within one or two generations.
- Outcomes are directly related to stage at presentation and vary by race and ethnicity in the United States.
Table 1 — Table 84-1 Five-Year Breast Cancer Relative Survival Rate (%) by Stage at Diagnosis and Race/Ethnicity in United States from 2012–2018¶
| STAGE | ALL | WHITE | BLACK | AIAN | HISPANIC | API |
|---|---|---|---|---|---|---|
| >99 | >99 | >99 | >99 | >99 | >99 | |
| 93 | 93 | 89 | 93 | 92 | 94 | |
| 75 | 77 | 64 | 72 | 74 | 77 | |
| 29 | 31 | 20 | 35 | 29 | 34 |
2. EPIDEMIOLOGY & RISK FACTORS¶
- Female gender and increasing age are the most common risk factors for breast cancer.
- About 70% of breast cancer in the United States is diagnosed in women 55 years and older.
- Median age of diagnosis is 63.
- Postmenopausal obesity is also a risk factor, likely because of increased estrogen exposure.
- Alcohol consumption is a risk factor.
- Exposure to ionizing radiation during adolescence is the best documented exogenous risk factor for breast cancer.
- Women diagnosed with some types of benign breast pathology also have a higher risk of subsequent invasive breast cancer diagnosis.
- Diagnosis of atypical ductal or lobular hyperplasia increases risk about four- to fivefold.
- Diagnosis of lobular carcinoma in situ (LCIS) increases risk 7- to 12-fold.
- Women with high breast density on mammography may be at increased risk of breast cancer.
- Family history is a critical risk factor, although only 20% of women diagnosed with breast cancer have a family history.
- Diagnosis of breast cancer in a first-degree relative (parent, sibling, or daughter) doubles breast cancer risk.
- A personal diagnosis of previous invasive breast cancer also increases the risk of developing a new breast cancer in the ipsilateral or contralateral breast.
- These genes play a role in DNA damage repair, and inherited mutations, which are transmitted in an autosomal dominant fashion, account for 5–10% of breast cancers.
2.1 Nongenetic Risk Factors¶
- Early menarche, late menopause, and late first pregnancy are known risk factors.
- Prolonged exposure to hormone replacement therapy is associated with increased risk.
- Paradoxically, not estrogen replacement therapy is associated with increased risk.
- Current use of oral contraceptives is associated with increased risk.
- Studies of diet and breast cancer risk have not been conclusive.
- Studies of other environmental factors such as pesticide or other chemical exposures have not been convincing.
2.2 Genetic Risk Factors¶
- Germline mutations in BRCA1 (located on chromosome 17q21) or BRCA2 (located on chromosome 13q12) genes impart a 50–80% risk of developing invasive breast cancer by age 80 years.
- Germline mutations in BRCA1/2 also impart a 30% risk of developing ovarian cancer.
- Germline mutations in other genes also lead to a higher risk of breast cancer including TP53 (Li-Fraumeni syndrome), PALB2, ATM, STK11 (Peutz-Jeghers syndrome), and PTEN (Cowden syndrome).
- Certain populations have a higher incidence of BRCA mutations, especially Ashkenazi Jews.
- Testing for germline mutations is readily done using panel testing on DNA obtained from peripheral blood or saliva after appropriate counseling.
- It is not recommended for the general population.
- Evidence-based guidelines from the American Society of Clinical Oncology and Society of Surgical Oncology recommend consideration of testing for high-penetrance breast cancer susceptibility genes in individuals with a personal history of breast cancer with specific features including diagnosis ≤65 years.
- Older patients should be offered testing for clinical features such as Ashkenazi Jewish ancestry; multiple breast cancers; certain types of breast cancer, including breast cancer lacking expression of the estrogen and progesterone receptors and HER2 proteins (triple-negative breast cancer [TNBC]) and lobular breast cancer with personal or family history of diffuse gastric cancer; or close blood relative with early-onset or male breast cancer, ovarian cancer, pancreatic cancer, or metastatic prostate cancer.
- Testing for individuals without a cancer diagnosis should be considered for those with a family member who tests positive or those with a family history as outlined above or those with higher risk based on existing risk assessment tools such as Tyrer-Cuzick score, BRCAPro, or CanRisk.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Breast cancer is predominantly a disease resulting from prolonged generally lead to protein truncation and loss of function of DNA repair proteins.
- The most common mutations are in the BRCA1 or BRCA2 genes.
- Germline mutations in other genes also lead to a higher risk of breast cancer including TP53, PALB2, ATM, STK11, and PTEN.
- Invasive breast cancer is in fact a disease with diverse subtypes, both histologic and molecular.
- Two decades of molecular analyses have documented multiple transcriptional, epigenetic, and genetic changes that characterize invasive breast cancer.
3.1 Molecular Subtypes¶
- Luminal A and B subtypes both express ER and are viewed as generally likely to be responsive to antiestrogen strategies (also called hormonal or endocrine therapies).
- Luminal B tumors are characterized by other findings such as reduced PR expression or increased proliferation, usually measured by expression of Ki67, and are associated with a poorer outcome than luminal A tumors.
- The HER2 subtype expresses HER2 protein at high levels and is more likely to benefit from the use of HER2-targeted therapies.
- Basal tumors tend to lack expression of ER, PR, and HER2 proteins (TNBC).
- TNBCs carry a poorer prognosis and are generally managed with chemotherapy and immunotherapy.
- TNBC can be further divided into at least six subtypes, which may also have therapeutic implications, especially in the metastatic setting.
- Lobular cancers are usually ER positive and HER2 negative.
- Lobular cancers are distinguished by absence of E-cadherin staining or function.
- Lobular cancers have a different natural history, with a propensity to spread to serosal surfaces, including omentum, pleura, and meninges or to various parenchyma, such as ovaries and upper and lower gastrointestinal tracts.
- Mucinous and pure medullary cancers (distinguished by high levels of lymphocytic invasion surrounding the tumor) are associated with very favorable prognoses with local therapy only.
- Metaplastic cancers may present as very poorly differentiated tumors or even as squamous or sarcomatoid differentiations.
- Metaplastic cancers are generally approached as ductal cancers but may be treated in a manner consistent with their relative subtypes, such as squamous or sarcoma-like differentiation.
3.2 In Situ Pathology¶
- Ductal Carcinoma In Situ (DCIS) is confined to the duct without evidence of invasion through the basement membrane into surrounding interstitial tissue.
- Untreated DCIS is associated with a 30% risk of developing a subsequent invasive cancer in the same breast.
- Lobular Carcinoma In Situ (LCIS) is often an incidental finding on a breast biopsy done for abnormalities on physical exam or mammography.
- LCIS is viewed as a marker for increased risk of developing invasive breast cancer as about 25–30% of women with LCIS subsequently develop invasive disease in either breast.
- The primary management is continued breast cancer screening and consideration of chemoprevention with tamoxifen or aromatase inhibitor to decrease risk of invasive disease.
4. CLINICAL FEATURES¶
- Clinical signs and symptoms suggestive of breast cancer may include a breast lump or skin or nipple changes or palpable regional nodes.
- Thanks to mammographic screening, many patients present with abnormal mammographic findings including a mass, distortion, and/or suspicious microcalcifications without any symptoms or physical exam findings.
- Less than 10% of patients present with de novo metastatic breast cancer.
- Individuals who present with symptoms suggestive of metastatic disease or physical findings of more advanced disease (e.g., large tumor, skin changes, extensive regional adenopathy) should undergo radiologic imaging with computed tomography and radionuclide scanning to look for overt metastatic disease.
- Suspicious lesions should be biopsied whenever possible to confirm a diagnosis of metastatic breast cancer because of the implications for prognosis and selection of therapy.
4.1 Screening Findings¶
- Screening mammography has led to a marked increase in the diagnosis of DCIS and LCIS.
- High breast density on mammography may be at increased risk of breast cancer.
- Women with newly diagnosed breast cancer have unsuspected contralateral disease in up to 3% of cases.
5. DIFFERENTIAL DIAGNOSIS¶
- Breast cancer is a disease with diverse subtypes, both histologic and molecular.
- DCIS vs Invasive Ductal Carcinoma: DCIS is confined to the duct without evidence of invasion through the basement membrane.
- Lobular Carcinoma In Situ (LCIS) vs Invasive Lobular Carcinoma: LCIS is a marker for increased risk of developing invasive breast cancer.
- Metastatic Disease Mimics: Less than 10% of patients present with de novo metastatic breast cancer.
- Metaplastic Cancers: May present as very poorly differentiated tumors or even as squamous or sarcomatoid differentiations.
- Mucinous and Pure Medullary Cancers: Associated with very favorable prognoses with local therapy only.
6. INVESTIGATIONS & DIAGNOSIS¶
- Final diagnosis rests on pathologic confirmation, which is generally carried out by image-guided core biopsy to confirm diagnosis, assess tumor grade and morphology, and carry out biomarker evaluation for expression of estrogen receptor (ER) and progesterone receptor (PR) and HER2 proteins and potentially HER2 gene amplification.
- Suspicious axillary lymph nodes should also be biopsied via image-guided techniques.
- It is important to image both breasts because up to 3% of women with newly diagnosed breast cancer have unsuspected contralateral disease.
- Evaluation of the breasts with MRI after a biopsy-proven diagnosis is controversial.
- MRI is more sensitive than radiologic mammography and will commonly detect previously unidentified disease.
- This observation may lead to additional surgery, including mastectomy, without obvious improvements in outcomes.
- Staging is a cornerstone for breast cancer management because it provides information about natural history and informs decisions about therapy.
- The traditional TNM (tumor-node-metastasis) staging system has evolved to consider molecular testing including biomarkers and certain genomic tests such as the Oncotype 21 gene assay.
- Staging may take place at time of diagnosis (c or clinical staging) or after surgery (p or pathologic staging) or after preoperative systemic therapy followed by surgery (designated with a 'y' prefix).
- For most asymptomatic individuals presenting with early breast cancer, a careful history and physical exam will be sufficient, and testing can be limited to breast imaging and any testing needed to ensure a safe surgical procedure.
- Individuals who present with symptoms suggestive of metastatic disease or physical findings of more advanced disease (e.g., large tumor, skin changes, extensive regional adenopathy) should undergo radiologic imaging with computed tomography and radionuclide scanning to look for overt metastatic disease.
6.1 Diagnostic Algorithm¶
- Suspicious clinical breast finding → Screening breast imaging (mammography, ultrasonography as indicated, MRI if indicated).
- Suspicious breast finding → Diagnostic breast imaging.
- Routine follow-up mammogram as indicated.
- Negative/benign → Routine follow-up screening breast mammogram.
- Confirmed suspicious finding → Biopsy.
- Uncertain or clinical suspicion persists → Follow-up exam.
- Resolved → Routine follow-up screening breast mammogram as indicated.
- Ductal carcinoma in situ → Invasive ductal carcinoma.
- ER positive → PR positive → HER2 negative → Refer to experienced mammogram as indicated.
- Mammographic images courtesy of Drs. Mark Helvie and Colleen Neal, Department of Radiology, Michigan Medicine.
- Photomicrographs courtesy of Dr. Celina Kleer, Department of Pathology, Michigan Medicine.
6.2 Biomarker Evaluation¶
- Biomarker evaluation for expression of estrogen receptor (ER) and progesterone receptor (PR) and HER2 proteins and potentially HER2 gene amplification.
- Positive tumors are commonly defined as those with ≥1% staining by immunohistochemistry.
- Genomic multigene expression testing of the tumor with assays like Oncotype, MammaPrint, ProSigna, EndoPredict, or Breast Cancer Index will identify a substantial portion of patients with zero to three positive nodes who would not benefit from adjuvant chemotherapy.
7. MANAGEMENT & TREATMENT¶
- Multidisciplinary care is a cornerstone for optimal treatment of early breast cancer.
- The current approach to treatment of early-stage breast cancer reflects evolution from the initial concept of breast cancer as an orderly disease that spreads from breast to axillary nodes to systemic disease to our current understanding of breast cancer as a potentially systemic disease almost from onset.
- Therefore, treatment approaches incorporate surgery and radiation to treat local disease and systemic therapy to eliminate or suppress any microscopic distant disease.
- The goal of these treatments in early-stage disease is reduction of subsequent distant recurrence and mortality.
- They are given in a manner to optimize efficacy while minimizing toxicity and avoiding overtreatment.
- Surgery: Six randomized trials have demonstrated equivalent survival with the use of breast-conservation therapy (lumpectomy and, usually, radiotherapy to the remaining breast) or modified radical mastectomy for individuals with early-stage breast cancer.
- Contraindications to breast conservation include patient preference, poor cosmesis, multifocal disease, previous chest radiation, and ongoing pregnancy that prevents timely administration of radiotherapy.
- Though not an absolute contraindication, germline mutation in a member of the BRCA gene family can drive a decision for bilateral mastectomy because of the high risk of subsequent disease in either breast.
- Patients who require or choose mastectomy should be informed about availability of immediate or delayed reconstruction options using autologous tissue or implants as clinically appropriate.
- It is clear, though, that most women with early breast cancer are well served by a lumpectomy to negative margins with axillary management, followed by radiation as appropriate.
- Management of the ipsilateral axilla continues to evolve as well.
- For patients with small tumors and clinically negative axillary nodes, sentinel node localization is used to identify clinically relevant nodes for removal and pathologic assessment to finalize staging and inform decisions about extent of radiotherapy and selection of adjuvant systemic therapy.
- Use of axillary dissection (removal of level 1 and 2 lymph nodes) is restricted to individuals with palpable lymph nodes or those with substantial pathologic involvement of sentinel lymph nodes.
- Randomized trials have shown excellent outcomes with omission of any sentinel node evaluation for older women with small biologically favorable tumors and clinically negative axilla who will take adjuvant endocrine therapy as well as omission of axillary dissection for women with low tumor burden in sentinel nodes who will receive radiation.
- Radiation: As with surgery, the use of postoperative radiotherapy to minimize breast recurrence and nodal recurrence has also changed as a result of data accumulated from serial clinical trials.
- Current treatment strategies are tailored to the individual based on age, tumor size, and nodal status.
- Options for external-beam radiotherapy include a standard scheme of daily whole breast radiotherapy (WBR) for 4–6 weeks, hypofractionated schedules lasting 5 days to 3 weeks, or partial breast radiation, usually given in a hypofractionated regimen.
- Clinical trials of the latter have failed to demonstrate its benefit over WBR.
- Extension of the radiotherapy port to include regional and axillary nodes is also considered based on pathology and type of surgery.
- The safety of omitting radiotherapy for women older than 65 with low-risk ER-positive tumors who will take endocrine therapy has been demonstrated.
- Brachytherapy to apply a radiation source directly to the tumor bed is also employed in some cases as a way of shortening duration of therapy.
- Patients who undergo mastectomy may also benefit from chest wall radiotherapy to reduce risk of both local and distant recurrence, thus improving survival.
- Potential candidates include those with large tumors or positive axillary lymph nodes, especially those with four or more involved nodes, while those with one to three positive nodes or close/minimally involved margins are also considered.
- Systemic Therapy: It has been recognized that breast cancer is often a systemic disease at time of diagnosis.
- Enhanced understanding of breast cancer biology, including the concept that resistant clones evolve as a function of random mutations over time, and the identification of multiple targets of therapy have greatly refined our understanding of the role of systemic therapy in early breast cancer.
- Such therapy may be given preoperatively (neoadjuvant) or postoperatively (adjuvant) and may take the form of cytotoxic chemotherapy, endocrine therapy directed toward ER, and other targeted therapies such anti-HER2, poly (ADP-ribose) polymerase (PARP) inhibitors in cancers with BRCA1/2 mutations, and/or immunotherapy directed toward immune checkpoints.
- A targeted agent, olaparib, an oral PARP inhibitor, is also used as an adjunct to chemotherapy for women with high-risk, germline BRCA-mutated, HER2-negative breast cancer who have completed (neo)adjuvant chemotherapy.
- It is particularly active in cancers with DNA repair pathway defects.
- The role of immunotherapy with the checkpoint inhibitors is also under evaluation.
- At present, pembrolizumab for patients with TNBC is the only U.S. Food and Drug Administration (FDA)-approved agent for early-stage breast cancer, but others are under investigation.
- Endocrine therapy is the foundation for adjuvant therapy for women with ER- and/or PR-positive breast cancer.
- Selection is based on menopausal status and consideration of side effect profiles.
- For premenopausal women with low-risk breast cancer, tamoxifen for 5–10 years is the standard.
- Premenopausal women with higher risk tumors are candidates for combined endocrine therapy with an LHRH agonist plus tamoxifen or aromatase inhibitor for 5 years.
- Multiple randomized trials have shown that aromatase inhibitors for 5 years provide modest but statistically significant superior outcome compared with tamoxifen for postmenopausal women.
- Women with ER-positive breast cancers are at risk for distant recurrence long after their original diagnosis, from 10–20 or more years.
- Some trials suggest that up to 10 years of endocrine therapy may be indicated for healthy postmenopausal women with higher risk tumors and good tolerance.
- Tamoxifen is associated with postmenopausal symptoms and a small chance of thromboembolic events or uterine cancer, especially in women over 50 years.
- Aromatase inhibitors are associated with postmenopausal symptoms, arthralgias, and bone loss, while LHRH agonists are associated with postmenopausal symptoms and bone loss.
- Although the three aromatase inhibitors appear to be equally effective, tolerance may vary; patients who are intolerant of one aromatase inhibitor may benefit from change to another member of the family or tamoxifen.
- Estrogen deprivation approaches depend on menopausal status.
- Ovarian suppression by gonadotropin hormone–releasing hormone (GnRH), such as the luteinizing hormone–releasing hormone (LHRH) agonists goserelin or leuprolide, or alternatively surgical oophorectomy, can be used to reduce circulating estradiol levels in premenopausal women to postmenopausal levels.
- These women can then also be treated either with tamoxifen or an AI.
- The CDK4/6 inhibitors abemaciclib and ribociclib may be used in combination with endocrine therapy for high-risk, early-stage, ER-positive breast cancer.
- Multiple cytotoxic agents have shown efficacy for treatment of metastatic breast cancer and are now used in treatment of early-stage disease.
- The most common regimens include cyclophosphamide, doxorubicin, paclitaxel, docetaxel, 5-fluorouracil, methotrexate, and/or one of the platin salt compounds (cisplatin or carboplatin).
- Several anti-HER2 therapies are also available.
- Two monoclonal antibodies, trastuzumab and pertuzumab, and two tyrosine kinase inhibitors, neratinib and lapatinib, are approved for use in early-stage breast cancer.
- Multiple other agents are available for metastatic disease, as discussed below, and are undergoing testing for use in earlier stages of disease.
- Neoadjuvant chemotherapy should be administered to healthy individuals with a large tumor burden or more than three positive nodes, especially premenopausal patients with a primary goal of reducing tumor size.
- However, in ER-positive disease, the likelihood of a pCR is low.
- Regardless, adjuvant chemotherapy (neoadjuvant or standard) is considered for healthy individuals with four or more positive lymph nodes as well as for those with lesser nodal burden who have high genomic signature score.
- Established chemotherapy regimens are outpatient based and use multiple agents for 3–6 months with appropriate supportive care including antiemetics and colony-stimulating factors as appropriate to reduce risk of febrile neutropenia.
- Long-term side effects can include premature menopause in premenopausal women and a small risk of doxorubicin-related cardiomyopathy, taxane-related peripheral neuropathy, or secondary leukemia, and possible cognitive dysfunction.
- Women with node-positive or high-risk node-negative, ER- and/or PR-positive, HER2-negative breast cancer who have completed adjuvant chemotherapy should consider use of a CDK4/6 inhibitor in conjunction with endocrine therapy.
- Current information supports the use of abemaciclib for 2 years or ribociclib for 3 years; addition of palbociclib for 2 years did not improve outcomes.
- Those with HER2-negative germline BRCA-mutated breast cancer who have received (neo)adjuvant chemotherapy should consider a year of oral olaparib.
- When used in conjunction with chemotherapy or anti-HER2 therapy, endocrine therapy is generally delayed until completion of adjuvant chemotherapy to minimize toxicity.
- Follow-Up of Survivors of Early-Stage Breast Cancer: Asymptomatic survivors of early-stage breast cancer should be followed regularly with history and physical examination to look for any evidence of recurrent disease and to assess for toxicities of prior or ongoing treatments.
- These exams are conducted every 3–6 months for the first 3 years and diminish in frequency over time.
- Annual breast imaging to look for ipsilateral or contralateral disease is the only routine testing needed.
- In the absence of symptoms or physical exam findings, routine imaging of other types or blood studies have not been shown to enhance well-being or outcome from breast cancer.
- Current research is focused on use of blood-based assays for circulating tumor cells (CTCs) or circulating free tumor DNA (ctDNA) as markers for early detection of recurrent disease, but these are investigational approaches at present.
- As many patients have long survival, routine follow-up by a primary care provider and adherence to age-appropriate general health guidelines are key.
- Symptom management is a key aspect of follow-up, especially for those on adjuvant endocrine therapy as adherence is a crucial factor.
7.1 General Guidelines for (Neo)Adjuvant Systemic Therapy Selection¶
- Approach to ER- and/or PR-Positive Breast Cancer: Endocrine therapy is the foundation for adjuvant therapy for women with ER- and/or PR-positive breast cancer.
- Selection is based on menopausal status and consideration of side effect profiles.
- For premenopausal women with low-risk breast cancer, tamoxifen for 5–10 years is the standard.
- Premenopausal women with higher risk tumors are candidates for combined endocrine therapy with an LHRH agonist plus tamoxifen or aromatase inhibitor for 5 years.
- Multiple randomized trials have shown that aromatase inhibitors for 5 years provide modest but statistically significant superior outcome compared with tamoxifen for postmenopausal women.
- Women with ER-positive breast cancers are at risk for distant recurrence long after their original diagnosis, from 10–20 or more years.
- Some trials suggest that up to 10 years of endocrine therapy may be indicated for healthy postmenopausal women with higher risk tumors and good tolerance.
- Tamoxifen is associated with postmenopausal symptoms and a small chance of thromboembolic events or uterine cancer, especially in women over 50 years.
- Aromatase inhibitors are associated with postmenopausal symptoms, arthralgias, and bone loss, while LHRH agonists are associated with postmenopausal symptoms and bone loss.
- Although the three aromatase inhibitors appear to be equally effective, tolerance may vary; patients who are intolerant of one aromatase inhibitor may benefit from change to another member of the family or tamoxifen.
- Estrogen deprivation approaches depend on menopausal status.
- Ovarian suppression by gonadotropin hormone–releasing hormone (GnRH), such as the luteinizing hormone–releasing hormone (LHRH) agonists goserelin or leuprolide, or alternatively surgical oophorectomy, can be used to reduce circulating estradiol levels in premenopausal women to postmenopausal levels.
- These women can then also be treated either with tamoxifen or an AI.
- The CDK4/6 inhibitors abemaciclib and ribociclib may be used in combination with endocrine therapy for high-risk, early-stage, ER-positive breast cancer.
- Multiple cytotoxic agents have shown efficacy for treatment of metastatic breast cancer and are now used in treatment of early-stage disease.
- The most common regimens include cyclophosphamide, doxorubicin, paclitaxel, docetaxel, 5-fluorouracil, methotrexate, and/or one of the platin salt compounds (cisplatin or carboplatin).
- Several anti-HER2 therapies are also available.
- Two monoclonal antibodies, trastuzumab and pertuzumab, and two tyrosine kinase inhibitors, neratinib and lapatinib, are approved for use in early-stage breast cancer.
- Multiple other agents are available for metastatic disease, as discussed below, and are undergoing testing for use in earlier stages of disease.
- Neoadjuvant chemotherapy should be administered to healthy individuals with a large tumor burden or more than three positive nodes, especially premenopausal patients with a primary goal of reducing tumor size.
- However, in ER-positive disease, the likelihood of a pCR is low.
- Regardless, adjuvant chemotherapy (neoadjuvant or standard) is considered for healthy individuals with four or more positive lymph nodes as well as for those with lesser nodal burden who have high genomic signature score.
- Established chemotherapy regimens are outpatient based and use multiple agents for 3–6 months with appropriate supportive care including antiemetics and colony-stimulating factors as appropriate to reduce risk of febrile neutropenia.
- Long-term side effects can include premature menopause in premenopausal women and a small risk of doxorubicin-related cardiomyopathy, taxane-related peripheral neuropathy, or secondary leukemia, and possible cognitive dysfunction.
- Women with node-positive or high-risk node-negative, ER- and/or PR-positive, HER2-negative breast cancer who have completed adjuvant chemotherapy should consider use of a CDK4/6 inhibitor in conjunction with endocrine therapy.
- Current information supports the use of abemaciclib for 2 years or ribociclib for 3 years; addition of palbociclib for 2 years did not improve outcomes.
- Those with HER2-negative germline BRCA-mutated breast cancer who have received (neo)adjuvant chemotherapy should consider a year of oral olaparib.
- When used in conjunction with chemotherapy or anti-HER2 therapy, endocrine therapy is generally delayed until completion of adjuvant chemotherapy to minimize toxicity.
- Follow-Up of Survivors of Early-Stage Breast Cancer: Asymptomatic survivors of early-stage breast cancer should be followed regularly with history and physical examination to look for any evidence of recurrent disease and to assess for toxicities of prior or ongoing treatments.
- These exams are conducted every 3–6 months for the first 3 years and diminish in frequency over time.
- Annual breast imaging to look for ipsilateral or contralateral disease is the only routine testing needed.
- In the absence of symptoms or physical exam findings, routine imaging of other types or blood studies have not been shown to enhance well-being or outcome from breast cancer.
- Current research is focused on use of blood-based assays for circulating tumor cells (CTCs) or circulating free tumor DNA (ctDNA) as markers for early detection of recurrent disease, but these are investigational approaches at present.
- As many patients have long survival, routine follow-up by a primary care provider and adherence to age-appropriate general health guidelines are key.
- Symptom management is a key aspect of follow-up, especially for those on adjuvant endocrine therapy as adherence is a crucial factor.
7.2 Prevention Strategies¶
- Current strategies to prevent breast cancer include surgery, chemoprevention, and lifestyle modification; their use and impact will vary depending on the underlying risk of developing breast cancer.
- Prophylactic mastectomy reduces risk of developing breast cancer by about 90% including in individuals who carry a germline breast cancer susceptibility gene mutation.
- Women who opt for prophylactic mastectomy in this setting should be counseled that breast cancer may develop in residual breast tissue.
- However, preventive mastectomy is not likely to improve outcomes in women with low or only modest risk and should be discouraged.
- Though the primary role for prophylactic oophorectomy is for ovarian cancer prevention in germline mutation carriers, it can also reduce breast cancer incidence in premenopausal women by about 50% because of reduction in estrogen exposure.
- Ample evidence exists for the use of chemoprevention approaches that target estrogen signaling pathways in high-risk women.
- Tamoxifen reduces risk of invasive breast cancer in women at higher risk (≥60 years, diagnosis of LCIS, or younger women with risk of developing invasive breast cancer ≥1.67% over 5 years based on current risk assessment tools).
- Newer data suggest that low-dose tamoxifen for 3 years may be effective and well tolerated.
- Side effects include postmenopausal symptoms and increased risk for endometrial cancer and thromboembolic events, especially in women over 50.
- Raloxifene may be an alternative for postmenopausal women.
- Though less effective in reducing breast cancer risk than tamoxifen, it is associated with fewer uterine cancers.
- The aromatase inhibitors, exemestane or anastrozole, also reduce breast cancer incidence by about 50% in postmenopausal women who are at moderate-high risk for breast cancer.
- The U.S. Preventive Services Task Force recommends that clinicians offer risk-reducing medications like tamoxifen, raloxifene, or aromatase inhibitors to women who are at increased risk for breast cancer and at low risk for medication side effects.
- Uptake is low despite the substantial evidence that demonstrates a huge benefit.
- Potential lifestyle modifications to reduce breast cancer risk include maintenance of a normal body mass index, avoidance of alcohol, and minimizing use of hormone replacement therapy.
- Regular exercise, especially during adolescence, may be associated with reduced risk.
- Long-term follow-up from the dietary substudy of the Women’s Health Initiative showed that a low-fat diet in postmenopausal women who previously were cancer-free at the time of study enrollment resulted in a nonsignificant reduction in breast cancer incidence but appeared to reduce risk of death from breast cancer.
- The role of newer GLP-1 agents has not been studied.
8. PROGNOSIS & COMPLICATIONS¶
- Outcomes are directly related to stage at presentation and vary by race and ethnicity in the United States.
- Five-year relative survival rates vary by stage and race (see Table 84-1).
- Long-term side effects can include premature menopause in premenopausal women and a small risk of doxorubicin-related cardiomyopathy, taxane-related peripheral neuropathy, or secondary leukemia, and possible cognitive dysfunction.
- As many patients have long survival, routine follow-up by a primary care provider and adherence to age-appropriate general health guidelines are key.
- Symptom management is a key aspect of follow-up, especially for those on adjuvant endocrine therapy as adherence is a crucial factor.
8.1 Long-Term Follow-Up¶
- Asymptomatic survivors of early-stage breast cancer should be followed regularly with history and physical examination to look for any evidence of recurrent disease and to assess for toxicities of prior or ongoing treatments.
- These exams are conducted every 3–6 months for the first 3 years and diminish in frequency over time.
- Annual breast imaging to look for ipsilateral or contralateral disease is the only routine testing needed.
- In the absence of symptoms or physical exam findings, routine imaging of other types or blood studies have not been shown to enhance well-being or outcome from breast cancer.
- Current research is focused on use of blood-based assays for circulating tumor cells (CTCs) or circulating free tumor DNA (ctDNA) as markers for early detection of recurrent disease, but these are investigational approaches at present.
- As many patients have long survival, routine follow-up by a primary care provider and adherence to age-appropriate general health guidelines are key.
- Symptom management is a key aspect of follow-up, especially for those on adjuvant endocrine therapy as adherence is a crucial factor.
9. SPECIAL CONSIDERATIONS¶
- Contraindications to breast conservation include patient preference, poor cosmesis, multifocal disease, previous chest radiation, and ongoing pregnancy that prevents timely administration of radiotherapy.
- Though not an absolute contraindication, germline mutation in a member of the BRCA gene family can drive a decision for bilateral mastectomy because of the high risk of subsequent disease in either breast.
- Patients who require or choose mastectomy should be informed about availability of immediate or delayed reconstruction options using autologous tissue or implants as clinically appropriate.
- It is clear, though, that most women with early breast cancer are well served by a lumpectomy to negative margins with axillary management, followed by radiation as appropriate.
- Evaluation of the breasts with MRI after a biopsy-proven diagnosis is controversial.
- On the one hand, MRI is more sensitive than radiologic mammography and will commonly detect previously unidentified disease.
- On the other hand, this observation may lead to additional surgery, including mastectomy, without obvious improvements in outcomes.
- The role of magnetic resonance imaging (MRI) as a screening modality is less well studied.
- MRI is more sensitive, less specific, and more complex to perform.
- Some guidelines suggest that it be used for women who have a lifetime predicted risk of ≥20%, which includes those with germline pathogenic mutations in the BRCA genes.
- Its use has also been suggested for those with very dense breasts on mammography, but clear evidence of benefit is lacking.
- Screening ultrasound has also been studied, but evidence supporting its routine use is lacking.
- There is considerable interest in the use of multicancer early detection (MCED) tests using circulating DNA as a screening test for diseases like breast cancer.
- Initial studies have not shown that these tests can substitute for or augment conventional mammographic screening, and women who do have MCED assays performed should still undergo mammographic screening, even if the MCED test is negative.
9.1 Pregnancy & Germline Mutations¶
- Ongoing pregnancy that prevents timely administration of radiotherapy is a contraindication to breast conservation.
- Germline mutation in a member of the BRCA gene family can drive a decision for bilateral mastectomy because of the high risk of subsequent disease in either breast.
- Testing for individuals without a cancer diagnosis should be considered for those with a family member who tests positive or those with a family history as outlined above or those with higher risk based on existing risk assessment tools such as Tyrer-Cuzick score, BRCAPro, or CanRisk.
10. KEY PEARLS & CLINICAL TRAPS¶
- Screening mammography reduced breast cancer mortality by about 20–25% in women ≥50 years without an impact on overall mortality.
- The UK Age trial suggested a similar benefit for women who began screening at 40 years.
- Screening frequency has varied from 1–2 years across trials.
- Most recommend that women aged 50–70 years have mammography every 1–3 years, and many recommend screening for women aged 40–50 years as well.
- When to stop is not known, but it is generally accepted that benefits are limited to women with a predicted life expectancy of at least 10 years.
- Uptake of chemoprevention is low despite the substantial evidence that demonstrates a huge benefit.
- Less than 10% of patients present with de novo metastatic breast cancer.
- About 25–30% of women with LCIS subsequently develop invasive disease in either breast.
- Untreated DCIS is associated with a 30% risk of developing a subsequent invasive cancer in the same breast.
- Women with high breast density on mammography may be at increased risk of breast cancer.
- About 70% of breast cancer in the United States is diagnosed in women 55 years and older.
- Median age of diagnosis is 63.
- Invasive breast cancer is a disease with diverse subtypes, both histologic and molecular.
- Two decades of molecular analyses have documented multiple transcriptional, epigenetic, and genetic changes that characterize invasive breast cancer.
- Outcomes are directly related to stage at presentation and vary by race and ethnicity in the United States.
- Five-year relative survival in the United States is currently 91%.
- Breast cancer is the most common nonskin cancer diagnosed in women in the world.
- In 2024, it is estimated that in the United States 310,000 women will be diagnosed with invasive breast cancer, >56,000 women will receive a diagnosis of ductal carcinoma in situ (DCIS), and about 42,250 women will die from breast cancer.
- Although largely a disease of women, about 2800 men will be diagnosed with and 530 men will die from breast cancer in 2024 in the United States.
- Thanks to advances in understanding of breast cancer biology, screening, diagnosis, treatment, and decreased use of hormone replacement therapy, 5-year relative survival in the United States is currently 91%.
- These advances have also made it possible to conceptualize the evolution of breast cancer and how available interventions can be applied across the continuum of changes to improve outcomes.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
Caption: Figure 84-2 shows an algorithm for diagnostic abnormalities noted on physical exam or imaging. rests on pathologic confirmation, which is generally image-guided core biopsy to confirm diagnosis, assess morphology, and carry out biomarker evaluation for receptor (ER) and progesterone receptor (PR) and potentially HER2 gene amplification. Suspi- nodes should also be biopsied via image-guided important to image both breasts because up to 3% of
Flowchart 2¶
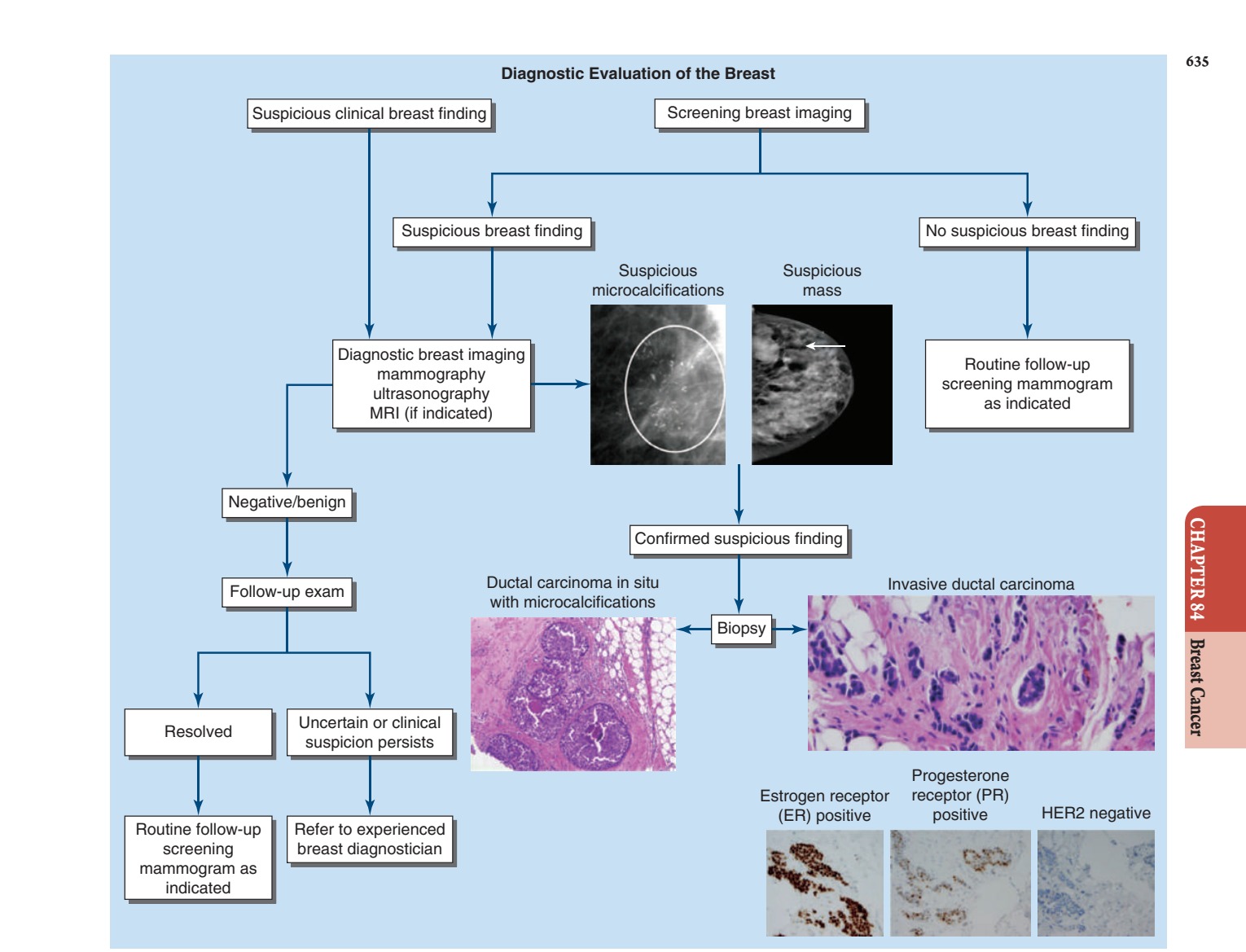
Caption: FIGURE 84-2 Evaluation and workup of breast lesions. For more extensive details, (Mammographic images courtesy of Drs. Mark Helvie and Colleen Neal, Department of Department of Pathology, Michigan Medicine.)
Flowchart 3¶

Caption: FIGURE 84-3 Evaluation of new signs or symptoms in a patient with prior history of carcinoembryonic antigen; ER, estrogen receptor; NGS, next-generation sequencing;
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 84-1 Breast cancer continuum conceptual model. Most breast cancers begin in atypia and hyperplasia to in situ malignancy to invasion into surrounding normal tissues distant organs, culminating in distant metastases. This is a conceptual model. Not all do not progress to the next. — Figure 84-1: Breast cancer continuum conceptual model showing progression from normal epithelial cells through atypia and hyperplasia to in situ malignancy, invasion, metastasis, and mortality.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.