Relapsing Fever¶
Chapter 190 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Relapsing fever is caused by infection with any of several species of Borrelia spirochetes.
- Three clinical forms exist: louse-borne relapsing fever (LBRF), soft tick relapsing fever (STRF), and hard tick relapsing fever (HTRF).
- Antigenic variation of the spirochetes' surface proteins accounts for the infection's relapsing course.
- Diagnosis relies on direct detection of spirochetes by microscopy of the blood or PCR.
- Treatment with antibiotics results in rapid cure but carries the risk of a moderate to severe Jarisch-Herxheimer reaction.
- Penicillin and tetracyclines are the antibiotics of choice for LBRF and STRF; erythromycin is a long-standing alternative.
- Tetracyclines are contraindicated in pregnant women and children; erythromycin is the alternative for these groups.
- Louse-borne relapsing fever is currently limited to Ethiopia, Eritrea, and Somalia.
- Tick-borne relapsing fever is found on most continents, with Africa and Central Asia most affected.
- Hard tick relapsing fever in North America is caused by Borrelia miyamotoi and Borrelia lonestari.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Clinical Forms
- 1.2 Historical Context
- 2. EPIDEMIOLOGY
- 2.1 Geographic Distribution
- 2.2 Reservoirs and Vectors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Borrelia Species
- 3.2 Pathogenesis
- 4. CLINICAL FEATURES
- 4.1 Fever Pattern
- 4.2 Systemic and Neurologic Symptoms
- 4.3 Laboratory Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Tick-Borne Relapsing Fever
- 5.2 Louse-Borne Relapsing Fever
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Microscopy
- 6.2 Molecular and Culture
- 6.3 Serology
- 7. MANAGEMENT & TREATMENT
- 7.1 Antibiotic Choices
- 7.2 Dosing and Administration
- 7.3 Treatment Algorithm
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Recovery and Mortality
- 8.2 Complications
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy and Pediatrics
- 9.2 Prevention
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Pearls
- 10.2 Treatment Pearls
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Photomicrograph of tick-borne relapsing fever spirochete (Borrelia Under conditions of limited resources... |
| 2 | 🖼 Figure | Ornithodoros turicata soft ticks of different ages |
1. DEFINITION & OVERVIEW¶
- Relapsing fever is caused by infection with any of several species of Borrelia spirochetes.
- It occurs in three different clinical and epidemiologic forms: louse-borne relapsing fever (LBRF), soft tick relapsing fever (STRF), and hard tick relapsing fever (HTRF).
- Physicians in ancient Greece distinguished LBRF from other febrile disorders by its characteristic clinical presentation: two or more fever episodes separated by varying periods of well-being.
- In the nineteenth century, LBRF was one of the first diseases to be associated with a specific microbe by virtue of its characteristic laboratory finding: the presence of large numbers of spirochetes of the genus Borrelia in the blood.
- The host responds with systemic inflammation that results in an illness ranging from a flulike syndrome to sepsis.
- Other manifestations are the consequences of central nervous system (CNS) involvement and disordered hemostasis.
- Acquired immunity follows the serial development of antibodies to each of the several variants appearing during an infection.
- Treatment with antibiotics results in rapid cure but at the risk of a moderate to severe Jarisch-Herxheimer reaction.
1.1 Clinical Forms¶
- Louse-borne relapsing fever (LBRF): Caused by Borrelia recurrentis. Humans serve as the sole reservoir in its life cycle.
- Soft tick relapsing fever (STRF): Caused by various Borrelia species transmitted by Ornithodoros ticks.
- Hard tick relapsing fever (HTRF): Caused by Borrelia miyamotoi and Borrelia lonestari transmitted by Ixodes and Amblyomma ticks.
1.2 Historical Context¶
- LBRF caused large epidemics well into the twentieth century.
- Currently occurs in northeastern Africa and among migrants from that area.
- Outbreaks of LBRF, often in association with typhus, can occur under circumstances of famine, refugee migration, war, homelessness, and incarceration.
- At present, however, most cases of relapsing fever are tick-borne in origin, with transmission from either soft-bodied ticks or hard-bodied ticks.
2. EPIDEMIOLOGY¶
- LBRF transmission is currently limited to Ethiopia, Eritrea, and Somalia.
- The disease has had a global distribution in the past, and that potential remains.
- STRF is found on most continents but is absent in arctic environments.
- For most species, the reservoirs of infection are small to medium-sized mammals, usually rodents, but also pigs and other domestic animals living around human habitats.
- One species, Borrelia duttonii in sub-Saharan Africa, is largely maintained by tick transmission between human hosts.
- In North America, the majority of reports of relapsing fever have been from the western United States and Canada and northern Mexico.
- STRF occurs as single cases or small case clusters through transient exposure of persons to tick-infested buildings or caves where mammals have nests or sleep.
- The two main Borrelia species involved in North America are Borrelia hermsii and Borrelia nietonii in the mountainous west and Borrelia turicatae in arid southwestern and south-central regions.
- Soft tick vectors typically feed for no more than 30 min, usually while the victim is sleeping, and then leave undetected.
- Transovarial transmission from one generation of ticks to the next means that infection risk may persist in a dwelling long after incriminated mammalian reservoirs have been removed.
- Borrelia miyamotoi is transmitted to humans from other mammals by different species of Ixodes hard ticks (e.g., I. scapularis in the eastern United States and I. ricinus in Europe) that also transmit Lyme disease, babesiosis, anaplasmosis, and a viral encephalitis.
- B. miyamotoi is acquired through outdoor activities and through contact with ticks in forested and shrubby areas during recreation, work, or activities around the home, similarly to Lyme disease.
- Among residents of most areas where B. miyamotoi and Borrelia burgdorferi coexist, the prevalence of antibodies to the former is about one-fourth of that to the latter.
- A less common cause of HTRF is B. lonestari, which is transmitted by Amblyomma americanum ticks of the southern and eastern United States.
2.1 Geographic Distribution¶
- LBRF: Currently limited to Ethiopia, Eritrea, and Somalia.
- STRF: Found on most continents, absent in arctic environments.
- HTRF: North America, Asia, Europe.
- North America: Majority of reports from western United States, Canada, northern Mexico.
- Africa and Central Asia: Most affected for STRF.
2.2 Reservoirs and Vectors¶
- Reservoirs: Small to medium-sized mammals, usually rodents, also pigs and other domestic animals.
- LBRF Vector: Human body louse (Pediculus humanus corporis).
- STRF Vectors: Ornithodoros ticks (soft-bodied).
- HTRF Vectors: Ixodes ticks (hard-bodied), Amblyomma americanum.
- Transovarial transmission: Infection risk may persist in a dwelling long after mammalian reservoirs have been removed.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Coiled, thin microscopic filaments that swim in one direction and then coil up before heading in another were first observed in the blood of patients with relapsing fever in the 1880s.
- These microbes were categorized as spirochetes and assigned to the genus Borrelia.
- The breakthrough cultivation medium was rich in ingredients, ranging from simple (e.g., N-acetylglucosamine) to more complex (e.g., serum).
- The limited biosynthetic capacity of Borrelia cells is accounted for by a genome content one-quarter that of Escherichia coli.
- Like other spirochetes, the helix-shaped Borrelia cells have two membranes, the outer of which is more loosely secured than in other double-membrane bacteria, such as E. coli.
- As a consequence, fixed organisms with damaged membranes can assume a variety of morphologies in smears and histologic preparations.
- The flagella of spirochetes run between the two membranes and are not on the cell surface.
- Although technically gram-negative, the 10- to 20-μm-long Borrelia cells, with a diameter of 0.2–0.3 μm, are too narrow to be seen by microscopy of Gram-stained slides.
- STRF and HTRF spirochetes enter the body in the tick's saliva with the onset of feeding.
- From an inoculum of a few cells, STRF spirochetes proliferate in the blood, doubling every 6 h to numbers of 10^6–10^7/mL or more.
- HTRF spirochetes grow more slowly in a mammalian host and attain lower peak concentrations in the blood.
- Borrelia species are extracellular pathogens; their presence inside cells connotes dead bacteria after phagocytosis.
- Binding of the spirochetes to erythrocytes leads to aggregation of red blood cells, their sequestration in the spleen and liver, and hepatosplenomegaly and anemia.
- A bleeding disorder is probably the consequence of thrombocytopenia, impaired hepatic production of clotting factors, and/or blockage of small vessels by aggregates of spirochetes, erythrocytes, and platelets.
- Some species (e.g., B. turicatae) are neurotropic and enter the brain, where they are comparatively sheltered from host immunity.
- Relapsing fever spirochetes can cross the maternal-fetal barrier and cause placental damage and inflammation, leading to intrauterine growth retardation and congenital infection.
- Although Borrelia species do not have potent exotoxins or a lipopolysaccharide endotoxin, they have abundant lipoproteins that activate Toll-like receptors on host cells, which leads to a proinflammatory process similar to that in endotoxemia.
- This leads to elevations of tumor necrosis factor α, interleukin 6, and interleukin 8 concentrations.
- IgM antibodies specific for the serotype-defining surface lipoprotein appear after a few days of infection and soon reach a concentration that causes lysis of bacteria in the blood through either direct bactericidal action or opsonization.
- The release of lipoproteins and other bacterial products from dying bacteria provokes a 'crisis,' during which there can be an increase in temperature, hypotension, and other signs of shock.
- A similar phenomenon occurring in some patients soon after the initiation of antibiotic treatment is characterized by an abrupt worsening of the patient's condition, which is called a Jarisch-Herxheimer reaction (JHR).
3.1 Borrelia Species¶
- B. crocidurae: Soft tick RF (STRF), West Africa, Ornithodoros sonrai.
- B. duttonii: STRF, East Africa, southern and central Africa, O. moubata.
- B. hermsii: STRF, Western North America, O. hermsi.
- B. hispanica: STRF, North Africa, southern Europe, O. erraticus.
- B. kalaharica: STRF, West Africa, southern Africa, O. savignyi.
- B. lonestari: Hard tick RF (HTRF), Southern and eastern United States, Amblyomma americanum.
- B. mazzotti: STRF, Mexico, Central America, O. talaje.
- B. miyamotoi: HTRF, North America, Asia, Europe, Ixodes pacificus, I. persulcatus, I. ricinus, I. scapularis.
- B. nietonii: STRF, Western North America, O. hermsii.
- B. persica: STRF, Central Asia, Middle East, O. tholozani.
- B. puertoricensis: STRF, Central America, O. puertoricensis.
- B. recurrentis: Louse-borne RF, Africa, global, Pediculus humanus corporis (human body louse).
- B. turicatae: STRF, Southwestern United States, northern Mexico, O. turicata.
- B. venezuelensis: STRF, Central America, South America, O. rudis.
3.2 Pathogenesis¶
- Spirochetes enter the body in the tick's saliva with the onset of feeding.
- STRF spirochetes proliferate in the blood, doubling every 6 h.
- HTRF spirochetes grow more slowly in a mammalian host.
- Binding of spirochetes to erythrocytes leads to aggregation and sequestration.
- Hepatosplenomegaly and anemia result from sequestration.
- Bleeding disorder results from thrombocytopenia and impaired hepatic production of clotting factors.
- Neurotropism: Some species enter the brain, sheltered from host immunity.
- Maternal-fetal barrier: Spirochetes can cross, causing placental damage and inflammation.
- Proinflammatory process: Lipoproteins activate Toll-like receptors, leading to TNF-α, IL-6, IL-8 elevations.
- Crisis: Increase in temperature, hypotension, and other signs of shock.
- Jarisch-Herxheimer reaction: Abrupt worsening of patient's condition after antibiotic treatment.
4. CLINICAL FEATURES¶
- STRF and LBRF present with the sudden onset of fever.
- Febrile periods are punctuated by intervening afebrile periods of a few days; this pattern occurs at least twice in STRF.
- The patient's temperature is ≥39°C and may be as high as 43°C.
- The first fever episode often ends in a crisis lasting ~15–30 min and consisting of rigors, a further elevation in temperature, and increases in pulse and blood pressure.
- The crisis phase is followed by profuse diaphoresis, falling temperature, and hypotension, which usually persist for several hours.
- In LBRF, the first episode of fever is unremitting for 3–6 days; it is usually followed by a single milder episode.
- In STRF, multiple febrile periods last 1–3 days each.
- In both forms, the interval between fevers ranges from 4 to 14 days, sometimes with symptoms of malaise and fatigue.
- The symptoms that accompany the fevers are usually nonspecific.
- Headache, neck stiffness, arthralgia, myalgia, and vomiting may accompany the first and subsequent febrile episodes.
- An enlarging spleen and liver cause abdominal pain.
- A nonproductive cough is common during LBRF and—in combination with fever and myalgias—may suggest influenza.
- Acute respiratory distress syndrome may occur during LBRF or STRF.
- On physical examination, the patient with LBRF or STRF may be delirious or apathetic.
- There may be body lice in the patient's clothes or signs of insect bites.
- In regions with B. miyamotoi or B. lonestari infection, a hard tick may be embedded in the skin.
- Jaundice, epistaxis, and subconjunctival hemorrhages are common during LBRF but not in STRF or HTRF.
- Splenomegaly or spleen tenderness is common in LBRF and STRF.
- Localizing neurologic findings are more common in STRF than in LBRF or HTRF.
- In North America, B. turicatae infection has neurologic manifestations, including aseptic meningitis and cranial neuritis, more often than B. hermsii or B. nietonii infection.
- Unilateral or bilateral Bell's palsy is the most common form of cranial neuritis and typically presents in the second or third febrile episode, not the first.
- Visual impairment from unilateral or bilateral iridocyclitis or panophthalmitis may be permanent.
- In LBRF, neurologic manifestations such as altered mental state are thought to be secondary to systemic inflammation or small hemorrhages in the brain rather than to direct invasion of the nervous system.
- Myocarditis in STRF or LBRF is evidenced by gallops on cardiac auscultation, a prolonged QT interval, and cardiomegaly and pulmonary edema on chest radiography.
- General laboratory studies in all forms of relapsing fever are not specific.
- Mild to moderate normocytic anemia is common, but frank hemolysis and hemoglobinuria do not develop.
- Leukocyte counts range from slightly elevated to leukopenic.
- Mild to moderate thrombocytopenia is common; platelet counts may fall below 50,000/μL in some cases.
- C-reactive protein and procalcitonin levels are elevated.
- Laboratory evidence of hepatitis can be found, with elevated serum concentrations of aminotransferases; the prothrombin and partial thromboplastin times may be moderately prolonged.
- Analysis of the cerebrospinal fluid (CSF) is indicated in all cases of suspected relapsing fever with signs of meningitis or meningoencephalitis.
- The presence of mononuclear pleocytosis and mildly to moderately elevated protein levels justifies intravenous antibiotic therapy in relapsing fever.
4.1 Fever Pattern¶
- STRF and LBRF present with the sudden onset of fever.
- Febrile periods punctuated by intervening afebrile periods of a few days.
- Pattern occurs at least twice in STRF.
- Temperature ≥39°C, may be as high as 43°C.
- First fever episode ends in a crisis lasting ~15–30 min.
- Crisis consists of rigors, further elevation in temperature, and increases in pulse and blood pressure.
- Crisis phase followed by profuse diaphoresis, falling temperature, and hypotension.
- In LBRF, first episode unremitting for 3–6 days, followed by single milder episode.
- In STRF, multiple febrile periods last 1–3 days each.
- Interval between fevers ranges from 4 to 14 days.
4.2 Systemic and Neurologic Symptoms¶
- Headache, neck stiffness, arthralgia, myalgia, and vomiting may accompany fevers.
- An enlarging spleen and liver cause abdominal pain.
- A nonproductive cough is common during LBRF.
- Acute respiratory distress syndrome may occur during LBRF or STRF.
- Patient may be delirious or apathetic.
- Jaundice, epistaxis, and subconjunctival hemorrhages are common during LBRF.
- Splenomegaly or spleen tenderness is common in LBRF and STRF.
- Localizing neurologic findings are more common in STRF.
- Bell's palsy is the most common form of cranial neuritis.
- Visual impairment from iridocyclitis or panophthalmitis may be permanent.
- Myocarditis evidenced by gallops, prolonged QT interval, cardiomegaly, and pulmonary edema.
4.3 Laboratory Findings¶
- Mild to moderate normocytic anemia is common.
- Frank hemolysis and hemoglobinuria do not develop.
- Leukocyte counts range from slightly elevated to leukopenic.
- Mild to moderate thrombocytopenia is common; platelet counts may fall below 50,000/μL.
- C-reactive protein and procalcitonin levels are elevated.
- Elevated serum concentrations of aminotransferases.
- Prothrombin and partial thromboplastin times may be moderately prolonged.
- Mononuclear pleocytosis and mildly to moderately elevated protein levels in CSF.
5. DIFFERENTIAL DIAGNOSIS¶
- Depending on the patient's history of residential, occupational, travel, and recreational exposures, the differential diagnosis of STRF includes one or more of the following infections that feature either periodicity in the fever pattern or an extended single febrile period with nonspecific constitutional symptoms.
- Rocky Mountain spotted fever and other rickettsioses.
- Ehrlichiosis, anaplasmosis, tick-borne viral infection, and babesiosis in North America, Europe, Russia, and northeastern Asia.
- STRF with Bell's palsy may be misdiagnosed as Lyme disease in areas endemic for both diseases.
- Elsewhere in the Americas and Asia and in most of Africa, malaria, typhoid fever, typhus and other rickettsioses, dengue, and leptospirosis also may be considered.
- Other agents transmitted by the body louse are Rickettsia prowazekii, the cause of typhus, and Bartonella quintana, the cause of trench fever.
- There may be co-infections of malaria, typhus, or typhoid with STRF or LBRF.
- B. miyamotoi infection may coexist with Lyme disease.
5.1 Tick-Borne Relapsing Fever¶
- Rocky Mountain spotted fever and other rickettsioses.
- Ehrlichiosis, anaplasmosis, tick-borne viral infection, and babesiosis.
- Lyme disease (in areas endemic for both).
- Malaria, typhoid fever, typhus and other rickettsioses, dengue, and leptospirosis (in Americas, Asia, Africa).
5.2 Louse-Borne Relapsing Fever¶
- Rickettsia prowazekii (typhus).
- Bartonella quintana (trench fever).
- Co-infections of malaria, typhus, or typhoid.
6. INVESTIGATIONS & DIAGNOSIS¶
- STRF or LBRF should be considered in a patient with the characteristic fever pattern and a history of recent exposure—i.e., within 1–2 weeks before illness onset—to body lice or soft ticks in geographic areas with documented current or past transmission.
- Because of the longevity of the ticks and the transovarial transmission of the pathogen in the ticks, a case of relapsing fever may be diagnosed many years after the last case reported in that locale.
- The lice may be on the clothes of a migrant, refugee, or unhoused person.
- While the epidemiologic risks for B. miyamotoi HTRF are similar to those for Lyme disease, prompt removal of an embedded tick upon discovery may not reduce the risk of infection of this pathogen.
- The bedrock for laboratory diagnosis of LBRF and STRF remains direct detection of the spirochetes by microscopy of the blood.
- Manual differential counts of white blood cells by Wright, Giemsa, or Giemsa-Wright stain usually reveal spirochetes in thin blood smears if their concentration is ≥10^5/mL and several oil-immersion fields are examined.
- The peak density of B. miyamotoi or B. lonestari in the blood may not be high enough for use of a blood smear alone for diagnosis.
- For LBRF and STRF, the preferred time to obtain a blood specimen is at or just before fever's peak.
- Lower concentrations of spirochetes may be revealed by a thick blood smear that is treated with 0.5% acetic acid before staining.
- An alternative is a wet mount of citrated blood mixed with saline and examined by phase-contrast or dark-field microscopy for motile spirochetes.
- Polymerase chain reaction (PCR) and similar nucleic acid amplification test (NAAT) procedures are increasingly used for examination of blood or CSF in cases of suspected relapsing fever.
- Overall, NAAT is more sensitive than thin blood smear, particularly for samples obtained between febrile episodes.
- PCR is the preferred procedure for direct detection of B. miyamotoi or B. lonestari in blood or CSF.
- Culture of blood or CSF in Barbour-Stoenner-Kelly broth medium or equivalent is an option for isolation of Borrelia species.
- However, visible growth takes several days, and few laboratories offer this service.
- Options for serologic confirmation of infection are limited, and results may be misleading.
- Whole cell–based assays, such as enzyme-linked immunosorbent assay (ELISA) and the C6 peptide ELISA for Lyme disease, may be positive in relapsing fever through antigenic cross-reactivities among these spirochetes.
- A commercially available assay based on GlpQ—a protein antigen of STRF, HTRF, and LBRF but not of any Lyme disease species—has better specificity but commonly is negative at a time when a blood smear or PCR assay would be positive.
- The results of a GlpQ-based assay or an indirect immunofluorescence assay of whole cells cannot be used to differentiate between different Borrelia species as to etiology.
- A positive IgG immunoassay of a single specimen may be the consequence of a past infection and not the present illness.
6.1 Microscopy¶
- Direct detection of spirochetes by microscopy of the blood.
- Manual differential counts of white blood cells by Wright, Giemsa, or Giemsa-Wright stain.
- Spirochetes revealed in thin blood smears if concentration is ≥10^5/mL.
- Preferred time to obtain blood specimen: at or just before fever's peak.
- Thick blood smear treated with 0.5% acetic acid before staining.
- Wet mount of citrated blood mixed with saline and examined by phase-contrast or dark-field microscopy.
6.2 Molecular and Culture¶
- PCR and NAAT procedures for examination of blood or CSF.
- NAAT is more sensitive than thin blood smear, particularly for samples obtained between febrile episodes.
- PCR is the preferred procedure for direct detection of B. miyamotoi or B. lonestari in blood or CSF.
- Culture of blood or CSF in Barbour-Stoenner-Kelly broth medium or equivalent.
- Visible growth takes several days, and few laboratories offer this service.
6.3 Serology¶
- Options for serologic confirmation of infection are limited, and results may be misleading.
- Whole cell–based assays (ELISA, C6 peptide ELISA) may be positive through antigenic cross-reactivities.
- GlpQ-based assay has better specificity but commonly is negative when blood smear or PCR assay would be positive.
- Positive IgG immunoassay of a single specimen may be the consequence of a past infection.
7. MANAGEMENT & TREATMENT¶
- Penicillin and tetracyclines have been the antibiotics of choice for LBRF and STRF for several decades.
- Erythromycin has been a long-standing alternative choice.
- There is no evidence of acquired resistance to these antibiotics.
- Borrelia species are also susceptible to second- and third-generation cephalosporins.
- These spirochetes are relatively resistant to rifampin, sulfonamides, and aminoglycosides.
- Spirochetes are no longer detectable in the blood within a few hours after the first dose of an effective antibiotic.
- Under conditions of limited resources or in the midst of an epidemic, a single dose of antibiotic usually suffices for successful treatment of LBRF.
- For adults, a single dose of oral doxycycline (200 mg), oral tetracycline (500 mg), or intramuscular ceftriaxone 250 mg for adults and 125 mg for children is effective.
- The corresponding doses for children are oral tetracycline at 12.5 mg/kg, oral doxycycline at 5 mg/kg, and intramuscular penicillin G procaine at 200,000–400,000 units.
- When an adult patient is stuporous or nauseated, the intravenous dose of tetracycline is 250–500 mg.
- Tetracyclines are contraindicated in pregnant and nursing women.
- For individuals in these groups who are allergic to penicillin, oral erythromycin (500 mg for adults and 12.5 mg/kg for children) is an alternative.
- While there is little reported experience with other macrolides, such as azithromycin, these are likely to be as effective as erythromycin.
- Sequential therapy vs Single dose therapy algorithm applies.
- If it is not known whether the patient has tick-borne or louse-borne relapsing fever, the patient should be treated for the tick-borne form.
- Central nervous system invasion in louse-borne relapsing fever is uncommon.
7.1 Antibiotic Choices¶
- First choice: Penicillin and tetracyclines.
- Alternative: Erythromycin.
- Susceptible to: Second- and third-generation cephalosporins.
- Resistant to: Rifampin, sulfonamides, and aminoglycosides.
- Rapid cure: Spirochetes no longer detectable in blood within a few hours after first dose.
7.2 Dosing and Administration¶
- Adults: Single dose of oral doxycycline (200 mg), oral tetracycline (500 mg), or intramuscular ceftriaxone 250 mg.
- Children: Intramuscular ceftriaxone 125 mg.
- Children: Oral tetracycline at 12.5 mg/kg, oral doxycycline at 5 mg/kg.
- Children: Intramuscular penicillin G procaine at 200,000–400,000 units.
- Stuporous or nauseated adult: Intravenous dose of tetracycline is 250–500 mg.
- Pregnant and nursing women: Tetracyclines contraindicated.
- Pregnant and nursing women allergic to penicillin: Oral erythromycin (500 mg for adults and 12.5 mg/kg for children).
- Macrolides (e.g., azithromycin): Likely to be as effective as erythromycin.
7.3 Treatment Algorithm¶
- If tick-borne or louse-borne unknown: Treat for tick-borne form.
- Sequential therapy: Intravenous ceftriaxone 2 g qd or Na penicillin G, 5 million U q6h for 14 days.
- First choice sequential: Age ≥9 years, not pregnant: Oral doxycycline 100 mg bid IM 250 mg adults.
- First choice sequential: Age <9 years: Erythromycin 800,000 U adults 12.5 mg/kg per day.
- Second choice sequential: Age ≥9 years, not pregnant: Tetracycline 500 mg qid.
- Second choice sequential: Age <9 years or pregnant: Erythromycin 12.5 mg/kg per day 500 mg qid.
- Third choice sequential: Age ≥9 years: Erythromycin 500 mg qid.
- Duration sequential: 10 days.
- Single dose therapy: Age ≥9 years, not pregnant: Ceftriaxone 250 mg adults and 125 mg children.
- Single dose therapy: Age <9 years or pregnant: Erythromycin 12.5 mg/kg per day 200,000–400,000 U children.
- Duration single dose: 7 days.
8. PROGNOSIS & COMPLICATIONS¶
- Spirochetes are no longer detectable in the blood within a few hours after the first dose of an effective antibiotic.
- Most patients recover.
- Post-leptospirosis symptoms, mainly of a depression-like nature, may occur and persist for years after the acute disease (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Mortality rates are highest among patients who are elderly and those who have severe disease (pulmonary hemorrhage, Weil's syndrome) (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Leptospirosis during pregnancy is associated with high fetal mortality rates (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Long-term follow-up of patients with renal failure and hepatic dysfunction has documented good recovery of both renal and hepatic function (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Jarisch-Herxheimer reaction: Moderate to severe reaction after antibiotic treatment.
- Meningoencephalitis or meningitis was documented in adults with deficiencies in humoral immunity, including the effects of anti–B cell antibodies such as rituximab.
- If the patient has coexisting early Lyme disease, there may be erythema migrans, the localized skin rash.
8.1 Recovery and Mortality¶
- Most patients recover.
- Mortality rates are highest among patients who are elderly and those who have severe disease.
- Jarisch-Herxheimer reaction: Moderate to severe reaction after antibiotic treatment.
8.2 Complications¶
- Meningoencephalitis or meningitis in adults with deficiencies in humoral immunity.
- Coexisting early Lyme disease may present with erythema migrans.
9. SPECIAL CONSIDERATIONS¶
- Tetracyclines are contraindicated in pregnant and nursing women.
- For individuals in these groups who are allergic to penicillin, oral erythromycin is an alternative.
- While there is little reported experience with other macrolides, such as azithromycin, these are likely to be as effective as erythromycin.
- Individuals who may be exposed to Leptospira through their occupations or their involvement in recreational freshwater activities should be informed about the risks (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Measures for controlling leptospirosis include avoidance of exposure to urine and tissues from infected animals through proper eyewear, footwear, and other protective equipment (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Targeted rodent control strategies have a potential benefit (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Vaccines for agricultural and companion animals are generally available, and their use should be encouraged (Note: This text refers to Leptospirosis, not Relapsing Fever).
- The veterinary vaccine used in each area should contain the serovars known to be present in that area in order to prevent vaccine serovar mismatch (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Some vaccinated animals potentially still excrete leptospires in their urine (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Commercial vaccines for human leptospirosis are available in Japan, China, Cuba, and France (Note: This text refers to Leptospirosis, not Relapsing Fever).
- These vaccines, made with bacterins—inactivated Leptospira—provide short-term, serovar-specific immunity but cause strong adverse side effects (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Both usability and availability remain problematic (Note: This text refers to Leptospirosis, not Relapsing Fever).
- One of the largest-scale trials of vaccine efficacy for leptospirosis in humans has been reported from Cuba (Note: This text refers to Leptospirosis, not Relapsing Fever).
- However, no conclusions can be drawn about efficacy and adverse reactions because of insufficient study design and outcome details (Note: This text refers to Leptospirosis, not Relapsing Fever).
- The efficacy of chemoprophylaxis with doxycycline (200 mg once a week) or azithromycin (in pregnant women and children) is being disputed (Note: This text refers to Leptospirosis, not Relapsing Fever).
- But a cost-effectiveness focused pre- and postexposure administration is indicated in instances of well-defined short-term exposure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Experiments in animal models and a cost-effectiveness focused pre- and postexposure administration is indicated in instances of well-defined short-term exposure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Aggressive supportive care for leptospirosis is essential and can be life-saving (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Patients with nonoliguric renal dysfunction require aggressive fluid and electrolyte resuscitation to prevent dehydration and precipitation of oliguric renal failure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Peritoneal dialysis or hemodialysis should be provided to patients with oliguric renal failure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Rapid initiation of hemodialysis has been shown to reduce mortality risk and typically is necessary only for short periods (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Patients with pulmonary hemorrhage may have reduced pulmonary compliance (as seen in ARDS) and may benefit from mechanical ventilation with low tidal volumes to avoid high ventilation pressures (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Evidence is contradictory for the use of glucocorticoids and desmopressin as adjunct therapy for pulmonary involvement associated with severe leptospirosis (Note: This text refers to Leptospirosis, not Relapsing Fever).
- B. miyamotoi is transmitted to the host soon after the tick begins to feed, and it may be acquired from tick larvae as well as nymphs and adults (Note: This text refers to Relapsing Fever).
- A less common cause of HTRF is B. lonestari, which is transmitted by Amblyomma americanum ticks of the southern and eastern United States (Note: This text refers to Relapsing Fever).
9.1 Pregnancy and Pediatrics¶
- Tetracyclines are contraindicated in pregnant and nursing women.
- For individuals in these groups who are allergic to penicillin, oral erythromycin is an alternative.
- While there is little reported experience with other macrolides, such as azithromycin, these are likely to be as effective as erythromycin.
9.2 Prevention¶
- Individuals who may be exposed to Leptospira through their occupations or their involvement in recreational freshwater activities should be informed about the risks (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Measures for controlling leptospirosis include avoidance of exposure to urine and tissues from infected animals through proper eyewear, footwear, and other protective equipment (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Targeted rodent control strategies have a potential benefit (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Vaccines for agricultural and companion animals are generally available, and their use should be encouraged (Note: This text refers to Leptospirosis, not Relapsing Fever).
- The veterinary vaccine used in each area should contain the serovars known to be present in that area in order to prevent vaccine serovar mismatch (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Some vaccinated animals potentially still excrete leptospires in their urine (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Commercial vaccines for human leptospirosis are available in Japan, China, Cuba, and France (Note: This text refers to Leptospirosis, not Relapsing Fever).
- These vaccines, made with bacterins—inactivated Leptospira—provide short-term, serovar-specific immunity but cause strong adverse side effects (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Both usability and availability remain problematic (Note: This text refers to Leptospirosis, not Relapsing Fever).
- One of the largest-scale trials of vaccine efficacy for leptospirosis in humans has been reported from Cuba (Note: This text refers to Leptospirosis, not Relapsing Fever).
- However, no conclusions can be drawn about efficacy and adverse reactions because of insufficient study design and outcome details (Note: This text refers to Leptospirosis, not Relapsing Fever).
- The efficacy of chemoprophylaxis with doxycycline (200 mg once a week) or azithromycin (in pregnant women and children) is being disputed (Note: This text refers to Leptospirosis, not Relapsing Fever).
- But a cost-effectiveness focused pre- and postexposure administration is indicated in instances of well-defined short-term exposure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Experiments in animal models and a cost-effectiveness focused pre- and postexposure administration is indicated in instances of well-defined short-term exposure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Aggressive supportive care for leptospirosis is essential and can be life-saving (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Patients with nonoliguric renal dysfunction require aggressive fluid and electrolyte resuscitation to prevent dehydration and precipitation of oliguric renal failure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Peritoneal dialysis or hemodialysis should be provided to patients with oliguric renal failure (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Rapid initiation of hemodialysis has been shown to reduce mortality risk and typically is necessary only for short periods (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Patients with pulmonary hemorrhage may have reduced pulmonary compliance (as seen in ARDS) and may benefit from mechanical ventilation with low tidal volumes to avoid high ventilation pressures (Note: This text refers to Leptospirosis, not Relapsing Fever).
- Evidence is contradictory for the use of glucocorticoids and desmopressin as adjunct therapy for pulmonary involvement associated with severe leptospirosis (Note: This text refers to Leptospirosis, not Relapsing Fever).
10. KEY PEARLS & CLINICAL TRAPS¶
- Jarisch-Herxheimer reaction: Moderate to severe reaction after antibiotic treatment.
- Transovarial transmission: Infection risk may persist in a dwelling long after mammalian reservoirs have been removed.
- Serology limitations: Results may be misleading; positive IgG immunoassay of a single specimen may be the consequence of a past infection.
- GlpQ-based assay: Has better specificity but commonly is negative at a time when a blood smear or PCR assay would be positive.
- Tick-borne relapsing fever: Most cases are tick-borne in origin, with transmission from either soft-bodied ticks or hard-bodied ticks.
- Louse-borne relapsing fever: Currently limited to Ethiopia, Eritrea, and Somalia.
- Hard tick relapsing fever in North America: Caused by Borrelia miyamotoi and Borrelia lonestari.
- Bell's palsy: Most common form of cranial neuritis, typically presents in the second or third febrile episode, not the first.
- Visual impairment: From unilateral or bilateral iridocyclitis or panophthalmitis may be permanent.
- Myocarditis: Evidenced by gallops on cardiac auscultation, a prolonged QT interval, and cardiomegaly and pulmonary edema on chest radiography.
10.1 Diagnostic Pearls¶
- Bedrock for laboratory diagnosis: Direct detection of spirochetes by microscopy of the blood.
- Preferred time to obtain blood specimen: At or just before fever's peak.
- NAAT is more sensitive than thin blood smear, particularly for samples obtained between febrile episodes.
- Serology results may be misleading.
- GlpQ-based assay has better specificity but commonly is negative when blood smear or PCR assay would be positive.
10.2 Treatment Pearls¶
- Penicillin and tetracyclines are the antibiotics of choice for LBRF and STRF.
- Erythromycin is a long-standing alternative choice.
- No evidence of acquired resistance to these antibiotics.
- Spirochetes are no longer detectable in the blood within a few hours after the first dose of an effective antibiotic.
- Under conditions of limited resources or in the midst of an epidemic, a single dose of antibiotic usually suffices for successful treatment of LBRF.
- Tetracyclines are contraindicated in pregnant and nursing women.
- For individuals in these groups who are allergic to penicillin, oral erythromycin is an alternative.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
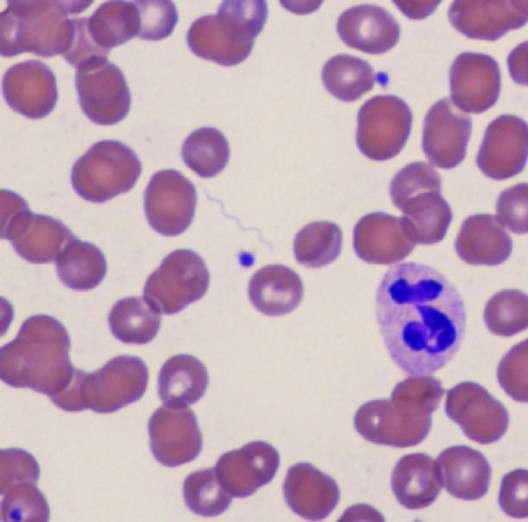
Caption: FIGURE 190-2 Photomicrograph of tick-borne relapsing fever spirochete (Borrelia Under conditions of limited resources or in the turicatae) in a Giemsa-Wright–stained thin blood smear. Included in the figure are a epidemic, a single dose of antibiotic usually suffices for polymorphonuclear leukocyte and two platelets. treatment of LBRF (Fig. 190-3). For adults, a single dose doxycycline (200 mg), oral tetracycline (500 mg), or specificity but commonly is negative at a time when a blood smear or ceftriaxone 250 mg for adults and 125 mg for children is PCR assay would be positive. The results of a GlpQ-based assay or an corresponding doses for children are oral tetracycline at 12.5 indirect immunofluorescence assay of whole cells cannot be used to oral doxycycline at 5 mg/kg, and intramuscular penicillin differentiate between different Borrelia species as to etiology. A positive caine at 200,000–400,000 units. When an adult patient is IgG immunoassay of a single specimen may be the consequence of a or nauseated, the intravenous dose of tetracycline is — FIGURE 190-1 Ornithodoros turicata soft ticks of different ages.
Figure 2¶

Caption: FIGURE 190-1 Ornithodoros turicata soft ticks of different ages. — FIGURE 190-2 Photomicrograph of tick-borne relapsing fever spirochete (Borrelia turicatae) in a Giemsa-Wright–stained thin blood smear. Included in the figure are a polymorphonuclear leukocyte and two platelets.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.