Nephrolithiasis¶
Chapter 330 | Part 9: Disorders of the Kidney and Urinary Tract · Part 9 – Renal & Urinary Tract Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Nephrolithiasis is a global disease with increasing prevalence due to Westernization of lifestyle habits (dietary changes, increasing BMI).
- Up to 20% of men and 10% of women will develop at least one stone during their lifetime.
- Stone composition: Calcium oxalate (~75%), Calcium phosphate (~15%), Uric acid (~8%), Struvite (~1%), Cystine (<1%).
- Supersaturation is the point at which concentration product exceeds solubility product; inhibitors like citrate prevent stone formation.
- Dietary calcium restriction is contraindicated; higher dietary calcium intake is related to a lower risk of stone formation.
- Fluid intake goal: Urine volume should be at least 2 L/d.
- Thiazide diuretics can reduce calcium oxalate stone recurrence by ~50% in patients with hypercalciuria.
- Allopurinol reduced stone recurrence in patients with calcium oxalate stones and high urine uric acid levels.
- NSAIDs (e.g., ketorolac) are just as effective as opioids in relieving renal colic symptoms and have fewer side effects.
- Helical CT is the gold standard diagnostic test; it detects stones as small as 1 mm and allows visualization of uric acid stones.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Stone Composition
- 1.2 Pathogenesis
- 2. EPIDEMIOLOGY
- 2.1 Demographics and Trends
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Dietary Risk Factors
- 3.2 Urinary Risk Factors
- 3.3 Genetic Risk Factors
- 4. CLINICAL FEATURES
- 4.1 Complications
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Differential Diagnosis List
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Laboratory Evaluation
- 6.2 Imaging
- 7. MANAGEMENT & TREATMENT
- 7.1 Acute Management
- 7.2 Prevention of New Stone Formation
- 7.3 Specific Stone Types
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Recurrence Rates
- 9. SPECIAL CONSIDERATIONS
- 9.1 Comorbidities
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Clinical Pearls
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Nephrolithiasis, or kidney stone disease, is a common, painful, and costly condition. Each year, billions of dollars are spent on nephrolithiasis-related activity, with the majority of expenditures on surgical treatment of existing stones. While a stone may form due to crystallization of lithogenic factors in the upper urinary tract, it can subsequently move into the ureter and cause renal colic. Although nephrolithiasis is rarely fatal, patients who have had renal colic report that it is the worst pain they have ever experienced. The evidence on which to base the clinical evaluation is limited, but there are standard approaches to patients with acute and chronic presentations that can reasonably guide the clinical evaluation. Nephrolithiasis is a systemic disorder. Several conditions predispose to stone formation, including gastrointestinal malabsorption (e.g., Crohn's disease, gastric bypass surgery), primary hyperparathyroidism, obesity, type 2 diabetes mellitus, and distal renal tubular acidosis.
1.1 Stone Composition¶
There are several types of kidney stones. It is clinically important to identify the stone type, which informs prognosis and selection of the optimal preventive regimen. Calcium oxalate stones are most common (75%); next, in order, are calcium phosphate (15%), uric acid (8%), struvite (1%), and cystine (<1%) stones. Many stones are a mixture of crystal types (e.g., calcium oxalate and calcium phosphate) and also contain protein in the stone matrix. Rarely, stones are composed of medications, such as acyclovir, atazanavir, and triamterene. Stones that form as a result of an upper tract infection, if not appropriately treated, can have devastating consequences and lead to end-stage renal disease.
Table 1 — Table 1: Stone Types and Prevalence¶
| Stone Type | Percentage of Stones |
|---|---|
| Calcium Oxalate | ~75% |
| Calcium Phosphate | ~15% |
| Uric Acid | ~8% |
| Struvite | ~1% |
| Cystine | <1% |
| Medication-Induced | Rare (e.g., acyclovir, atazanavir, triamterene) |
1.2 Pathogenesis¶
In the consideration of the processes involved in crystal formation, it is helpful to view urine as a complex solution. A clinically useful concept is supersaturation (the point at which the concentration product exceeds the solubility product). However, even though the urine in most individuals is supersaturated with respect to one or more types of crystals, the presence of inhibitors of crystallization prevents the majority of the population from continuously forming stones. The most clinically important inhibitor of calcium-containing stones is urine citrate. While the calculated supersaturation value does not perfectly predict stone formation, it is a useful guide as it integrates the multiple factors that are measured in a 24-h urine collection. Recent studies have changed the paradigm for the site of initiation of stone formation. Renal biopsies of stone formers have revealed calcium phosphate in the renal interstitium. It is hypothesized that this calcium phosphate deposits at the thin limb of the loop of Henle and then extends down to the papilla and erodes through the papillary epithelium, where it provides a site for deposition of calcium oxalate and calcium phosphate crystals. The majority of calcium oxalate stones grow on calcium phosphate at the tip of the renal papilla (Randall's plaque). Tubular plugs of calcium phosphate may be the initiating event in calcium phosphate stone development. Thus, the process of stone formation may begin years before a clinically detectable stone is identified.
2. EPIDEMIOLOGY¶
Nephrolithiasis is a global disease. Data suggest an increasing prevalence, likely due to Westernization of lifestyle habits (e.g., dietary changes, increasing body mass index). National Health and Nutrition Examination Survey data for 2007–2016 indicate that up to 20% of men and 10% of women will develop at least one stone during their lifetime. The prevalence is ~50% lower among black individuals than among whites. The incidence of nephrolithiasis (i.e., the rate at which previously unaffected individuals develop their first stone) also varies by age, sex, and race. Among white men, the peak annual incidence is ~3.5 cases/1000 at age 40 and declines to ~2 cases/1000 by age 70. Among white women in their thirties, the annual incidence is ~2.5 cases/1000; the figure decreases to ~1.5/1000 at age 50 and beyond. In addition to the medical costs associated with nephrolithiasis, this condition also has a substantial economic impact, as those affected are often of working age. Once an individual has had a stone, the prevention of a recurrence is essential.
2.1 Demographics and Trends¶
The incidence of stone disease is highest in middle-aged white men, but stones can form in infants as well as in the elderly. There is geographic variability, with the highest prevalence in the southeastern United States. Weight gain increases the risk of stone formation, and the increasing prevalence of nephrolithiasis in the United States may be due in part to the increasing prevalence of obesity.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Risk factors for nephrolithiasis can be categorized as dietary, nondietary, or urinary. These risk factors vary by stone type and clinical characteristics. Dietary factors that are associated with an increased risk of nephrolithiasis include animal protein, oxalate, sodium, sucrose, and fructose. Dietary factors associated with a lower risk include calcium, potassium, phytate, and higher fluid intake. Despite similar bioavailability, supplemental calcium may increase the risk of stone formation. The discrepancy between the risks from dietary calcium and calcium supplements may be due to the timing of supplemental calcium intake or to higher total calcium consumption leading to higher urinary calcium excretion. Higher intake of animal protein may lead to increased excretion of calcium and uric acid as well as to decreased urinary excretion of citrate, all of which increase the risk of stone formation. Higher sodium and sucrose intake increases calcium excretion independent of calcium intake. Higher potassium intake decreases calcium excretion, and many potassium-rich foods increase urinary citrate excretion due to their alkali content. Vitamin C supplements are associated with an increased risk of calcium oxalate stone formation in men, possibly owing to raised levels of oxalate in urine. Thus, male calcium oxalate stone formers should be advised to avoid high-dose vitamin C supplements.
3.1 Dietary Risk Factors¶
Patients who develop stones often change their diet; therefore, studies that retrospectively assess diet may be hampered by recall bias. Some studies have examined the relation between diet and changes in the lithogenic composition of the urine, often using calculated supersaturation. However, the composition of the urine does not perfectly predict risk, and not all components that modify risk are included in the calculation of supersaturation. Thus, dietary associations are best investigated by prospective studies that examine actual stone formation as the outcome. Dietary factors that are associated with an increased risk of nephrolithiasis include animal protein, oxalate, sodium, sucrose, and fructose. Dietary factors associated with a lower risk include calcium, potassium, phytate, and higher fluid intake.
Table 2 — Table 2: Dietary Risk Factors for Nephrolithiasis¶
| Factor | Effect on Risk | Mechanism |
|---|---|---|
| Animal Protein | Increased | Increased Ca and Uric Acid excretion; Decreased Citrate excretion |
| Oxalate | Increased | Direct lithogenic factor |
| Sodium | Increased | Increased Calcium excretion |
| Sucrose/Fructose | Increased | Increased Calcium excretion |
| Calcium (Dietary) | Decreased | Reduces intestinal oxalate absorption |
| Potassium | Decreased | Decreases Calcium excretion; Increases Citrate excretion |
| Vitamin C (High Dose) | Increased | Raises levels of oxalate in urine |
3.2 Urinary Risk Factors¶
URINE VOLUME: Lower urine volume results in higher concentrations of lithogenic factors and is a common and readily modifiable risk factor. A randomized trial has demonstrated the effectiveness of higher fluid intake in increasing urine volume and reducing the risk of stone recurrence. When the urine output is <1 L/d, the risk of stone formation more than doubles. URINE CALCIUM: Higher urine calcium excretion increases the likelihood of formation of calcium oxalate and calcium phosphate stones. While the term hypercalciuria is often used, there is no cutoff that distinguishes between normal and abnormal urine calcium excretion. Levels of urine calcium excretion are higher in individuals with a history of nephrolithiasis; however, the mechanisms remain poorly understood. Greater gastrointestinal calcium absorption is one important contributor, and greater bone turnover (with a resultant reduction in bone mineral density) may be another. Primary renal calcium loss, with lower serum calcium concentrations and elevated serum levels of parathyroid hormone (PTH) (and a normal 25-hydroxy vitamin D level), is rare. URINE OXALATE: Higher urine oxalate excretion increases the likelihood of calcium oxalate stone formation. As for urine calcium, no definition for "abnormal" urine oxalate excretion is widely accepted. The two sources of urine oxalate are endogenous generation and dietary intake. Dietary oxalate is the major contributor and also the source that can be modified. Notably, higher dietary calcium intake reduces gastrointestinal oxalate absorption and thereby reduces urine oxalate. URINE CITRATE: Urine citrate is a natural inhibitor of calcium-containing stones; thus, lower urine citrate excretion increases the risk of stone formation. Citrate reabsorption is influenced by the intracellular pH of proximal tubular cells. Metabolic acidosis, including that due to higher animal flesh intake, will lead to a reduction in citrate excretion by increasing reabsorption of filtered citrate. However, a notable proportion of patients have lower urine citrate for reasons that remain unclear. URINE URIC ACID: Higher urine levels of uric acid—a risk factor for uric acid stone formation—are found in individuals with excess purine consumption and rare genetic conditions that lead to overproduction of uric acid. This characteristic is not associated with the risk of calcium oxalate stone formation. URINE pH: Urine pH influences the solubility of some crystal types. Uric acid stones form when the urine pH is consistently ≤5.5, whereas calcium phosphate stones are more likely to form when the urine pH is ≥6.5. Cystine is more soluble at higher urine pH. Calcium oxalate stones are not influenced by urine pH.
Table 3 — Table 3: Urinary Risk Factors and Thresholds¶
| Parameter | Risk Direction | Notes |
|---|---|---|
| Urine Volume | Low (<1 L/d) | Risk more than doubles |
| Urine Calcium | High | No specific cutoff; continuous risk |
| Urine Oxalate | High | Continuous risk; no specific cutoff |
| Urine Citrate | Low | Natural inhibitor |
| Urine Uric Acid | High | Risk for uric acid stones |
| Urine pH | ≤5.5 | Uric acid stones |
| Urine pH | ≥6.5 | Calcium phosphate stones |
| Urine pH | High | Cystine stones (more soluble) |
3.3 Genetic Risk Factors¶
The risk of nephrolithiasis is more than twofold greater in individuals with a family history of stone disease. This association is likely due to a combination of genetic predisposition and similar environmental exposures. While a number of rare monogenic disorders cause nephrolithiasis, genome-wide association studies have begun to reveal genetic contributors to common forms of stone disease. The two most common and well-characterized rare monogenic disorders that lead to stone formation are primary hyperoxaluria and cystinuria. Primary hyperoxaluria is an autosomal recessive disorder that causes excessive endogenous oxalate generation by the liver, with consequent calcium oxalate stone formation and crystal deposition in organs. Intraparenchymal calcium oxalate deposition in the kidney can eventually lead to renal failure. Cystinuria is an autosomal recessive disorder that causes abnormal reabsorption of filtered basic amino acids. The excessive urinary excretion of cystine, which is poorly soluble, leads to cystine stone formation. Cystine stones are visible on plain radiographs and often manifest as staghorn calculi or multiple bilateral stones. Repeat episodes of obstruction and instrumentation can cause a reduction in the glomerular filtration rate (GFR).
4. CLINICAL FEATURES¶
There are two common presentations for individuals with an acute stone event: renal colic and painless gross hematuria. Renal colic is a misnomer because pain typically does not subside completely; rather, it varies in intensity. When a stone moves into the ureter, the discomfort often begins with a sudden onset of unilateral flank pain. The intensity of the pain can increase rapidly, and there are no alleviating factors. This pain, which is accompanied often by nausea and occasionally by vomiting, may radiate, depending on the location of the stone. If the stone lodges in the upper part of the ureter, pain may radiate anteriorly; if the stone is in the lower part of the ureter, pain can radiate to the ipsilateral testicle in men or the ipsilateral labium in women. Occasionally, a patient has gross hematuria without pain. The absence of hematuria does not exclude a stone, particularly when urine flow is completely obstructed by a stone. Other diagnoses may be confused with acute renal colic. If the stone is lodged at the right ureteropelvic junction, symptoms may mimic those of acute cholecystitis. If the stone blocks the ureter as it crosses over the right pelvic brim, symptoms may mimic acute appendicitis, whereas blockage at the left pelvic brim may be confused with acute diverticulitis. If the stone lodges in the ureter at the ureterovesical junction, the patient may experience urinary urgency and frequency. In female patients, the latter symptoms may lead to an incorrect diagnosis of bacterial cystitis; the urine will contain red and white blood cells, but the urine culture will be negative. An obstructing stone with proximal infection may present as acute pyelonephritis. A UTI in the setting of ureteral obstruction is a medical emergency that requires immediate restoration of drainage by placement of either a ureteral stent or a percutaneous nephrostomy tube.
4.1 Complications¶
Although nephrolithiasis does not directly cause upper urinary tract infections (UTIs), a UTI in the setting of an obstructing stone is a urologic emergency ("pus under pressure") and requires urgent intervention to reestablish drainage. Other conditions to consider in the differential diagnosis include muscular or skeletal pain, herpes zoster, duodenal ulcer, abdominal aortic aneurysm, gynecologic conditions, ureteral stricture, and ureteral obstruction by materials other than a stone, such as a blood clot or sloughed papilla. Extraluminal processes can lead to ureteral compression and obstruction; however, because of the gradual onset, these conditions do not typically present with renal colic.
5. DIFFERENTIAL DIAGNOSIS¶
Other diagnoses may be confused with acute renal colic. If the stone is lodged at the right ureteropelvic junction, symptoms may mimic those of acute cholecystitis. If the stone blocks the ureter as it crosses over the right pelvic brim, symptoms may mimic acute appendicitis, whereas blockage at the left pelvic brim may be confused with acute diverticulitis. If the stone lodges in the ureter at the ureterovesical junction, the patient may experience urinary urgency and frequency. In female patients, the latter symptoms may lead to an incorrect diagnosis of bacterial cystitis; the urine will contain red and white blood cells, but the urine culture will be negative. An obstructing stone with proximal infection may present as acute pyelonephritis. Other conditions to consider in the differential diagnosis include muscular or skeletal pain, herpes zoster, duodenal ulcer, abdominal aortic aneurysm, gynecologic conditions, ureteral stricture, and ureteral obstruction by materials other than a stone, such as a blood clot or sloughed papilla.
5.1 Differential Diagnosis List¶
- Muscular or skeletal pain
- Herpes zoster
- Duodenal ulcer
- Abdominal aortic aneurysm
- Gynecologic conditions
- Ureteral stricture
- Ureteral obstruction by materials other than a stone (e.g., blood clot, sloughed papilla)
6. INVESTIGATIONS & DIAGNOSIS¶
The diagnosis is often made on the basis of the history, physical examination, and urinalysis. Thus, it may not be necessary to wait for radiographic confirmation before treating the symptoms. The diagnosis is confirmed by an appropriate imaging study—preferably noncontrast helical computed tomography (CT), which is highly sensitive and allows visualization of uric acid stones (traditionally considered "radiolucent"). Helical CT detects stones as small as 1 mm that may be missed by other imaging modalities. While helical CT reveals a ureteral stone or evidence of recent passage (e.g., perinephric stranding or hydronephrosis), a plain abdominal radiograph (kidney/ureter/bladder [KUB]) can miss a stone in the ureter or kidney, even if it is radiopaque, and does not provide information on obstruction. Abdominal ultrasound offers the advantage of avoiding radiation and provides information on hydronephrosis, but it is not as sensitive as CT and images only the kidney and possibly the proximal segment of the ureter; thus, most ureteral stones are not detectable by ultrasound. Serum chemistry findings are typically normal, but the white blood cell count may be elevated. Examination of the urine sediment will usually reveal red and white blood cells and occasionally crystals. The absence of hematuria does not exclude a stone, particularly when urine flow is completely obstructed by a stone. If not recently measured, the following serum levels should be determined: electrolytes (to uncover hypokalemia or renal tubular acidosis), creatinine, calcium, phosphorus, and uric acid. The PTH level should be measured if indicated by elevated, high-normal, or low-normal serum and urine calcium concentrations. 25-Hydroxy vitamin D should be measured in concert with PTH to investigate the possible role of secondarily elevated PTH levels in the setting of vitamin D insufficiency. The urinalysis, including examination of the sediment, can provide useful information. In individuals with asymptomatic residual renal stones, red and white blood cells are frequently present in urine. If there is concern about the possibility of an infection, a urine culture should be performed. The sediment may also reveal crystals, which may help identify the stone type and also provide prognostic information as crystalluria is a strong risk factor for new stone formation. The results from 24-h urine collections serve as the cornerstone on which therapeutic recommendations are based. As a baseline assessment, patients should collect at least two 24-h urine samples while consuming their usual diet and usual volume of fluid. The following factors should be measured: total volume, calcium, oxalate, citrate, uric acid, sodium, potassium, phosphorus, magnesium, pH, and creatinine. When available, the calculated supersaturation is also informative. Stone composition analysis is essential if a stone or fragment is available; patients should be encouraged to retrieve passed stones. The stone type cannot be determined with certainty from 24-h urine results, but pure uric acid stones can be identified by low Hounsfield units on CT.
6.1 Laboratory Evaluation¶
If not recently measured, the following serum levels should be determined: electrolytes (to uncover hypokalemia or renal tubular acidosis), creatinine, calcium, phosphorus, and uric acid. The PTH level should be measured if indicated by elevated, high-normal, or low-normal serum and urine calcium concentrations. 25-Hydroxy vitamin D should be measured in concert with PTH to investigate the possible role of secondarily elevated PTH levels in the setting of vitamin D insufficiency. The urinalysis, including examination of the sediment, can provide useful information. In individuals with asymptomatic residual renal stones, red and white blood cells are frequently present in urine. If there is concern about the possibility of an infection, a urine culture should be performed. The sediment may also reveal crystals, which may help identify the stone type and also provide prognostic information as crystalluria is a strong risk factor for new stone formation.
Table 4 — Table 4: Baseline 24-h Urine Collection Parameters¶
| Parameter | Purpose |
|---|---|
| Total Volume | Assess hydration status |
| Calcium | Assess hypercalciuria |
| Oxalate | Assess hyperoxaluria |
| Citrate | Assess hypocitraturia |
| Uric Acid | Assess hyperuricosuria |
| Sodium | Assess sodium load |
| Potassium | Assess potassium status |
| Phosphorus | Assess phosphaturia |
| Magnesium | Assess magnesium status |
| pH | Assess urine acidity/alkalinity |
| Creatinine | Normalize excretion to body size |
6.2 Imaging¶
The "gold standard" diagnostic test is helical CT without contrast. If not already performed during an acute episode, a low-dose renal-limited noncontrast CT should be considered to establish that definitively the baseline stone burden. A suboptimal imaging study may not detect a residual stone that, if subsequently passed, would be mistaken for a new stone. In this instance, the preventive medical regimen might be unnecessarily changed as the result of a preexisting stone. Recommendations for follow-up imaging should be tailored to the individual patient. While CT provides the best information, the radiation dose is higher than from other modalities; therefore, higher-than-desired CT should be performed only if the results will lead to a change in clinical recommendations. Although less sensitive, renal ultrasound is typically used to minimize radiation exposure, with recognition of the limitations.
7. MANAGEMENT & TREATMENT¶
Evidence-based guidelines for the evaluation and treatment of nephrolithiasis have been published. Although there is limited evidence for several aspects, there are standard approaches to patients with acute and chronic presentations that can reasonably guide the clinical evaluation. It typically requires weeks to months (and often much longer) for a kidney stone to grow to a clinically detectable size. Although the passage of a stone is a dramatic event, stone formation and growth are characteristically clinically silent. A stone can remain asymptomatic in the kidney for years or even decades before signs (e.g., hematuria) or symptoms (e.g., pain) become apparent. Thus, it is important to remember that the onset of symptoms, typically attributable to a stone moving into the ureter, does not provide insight into when the stone actually formed. The factors that induce stone movement are unknown. Use of an alpha blocker may increase the rate of spontaneous stone passage. Urologic intervention should be postponed unless there is evidence of UTI, a low probability of spontaneous stone passage (e.g., a stone measuring ≥6 mm or an anatomic abnormality), or intractable pain. A ureteral stent may be placed cystoscopically, but this procedure typically requires general anesthesia, and the stent can be quite uncomfortable, may cause gross hematuria, and may increase the risk of UTI. If an intervention is indicated, the selection of the most appropriate intervention is determined by the size, location, and composition of the stone; the urinary tract anatomy; and the experience of the urologist. Extracorporeal shockwave lithotripsy (ESWL), the least invasive option, uses shockwaves generated outside the body to fragment the stone, but is being used less frequently. An endourologic approach, now more frequently used than ESWL, can remove a stone by basket extraction or laser fragmentation. For large upper-tract stones, percutaneous nephrostolithotomy has the highest likelihood of rendering the patient stone-free. Advances and urologic approaches and instruments have nearly eliminated the need for open surgical procedures such as ureterolithotomy or pyelolithotomy. For all stone types, consistently diluted urine reduces the likelihood of crystal formation. The urine volume should be at least 2 L/d. Because of differences in insensible fluid losses and fluid intake from food sources, the required total fluid intake will vary from person to person. Rather than specify how much to drink, it is more helpful to educate patients about how much more they need to drink in light of their 24-h urine volume. For example, if the daily urine volume is 1.5 L, then the patient should be advised to drink consistently at least 0.5 L more per day in order to increase the urine volume to the goal of 2 L/d. Restriction of nondairy animal protein (e.g., meat, chicken, seafood) is a reasonable approach and may result in higher excretion of citrate and lower excretion of calcium. In addition, reducing sodium intake to <2.5 g/d may decrease urinary excretion of calcium. Sucrose and fructose intake should be minimized. For adherence to a dietary pattern that is more manageable for patients than manipulating individual nutrients, the Mediterranean diet or the DASH (Dietary Approaches to Stop Hypertension) diet provides an appropriate and readily available option. Randomized trials have conclusively shown the DASH diet to reduce blood pressure. At present, only data from observational studies are available, but these demonstrate a strong and consistent inverse association between these healthy dietary patterns and risk of stone formation.
7.1 Acute Management¶
Randomized trials have demonstrated that parenterally administered nonsteroidal anti-inflammatory drugs (e.g., ketorolac) are just as effective as opioids in relieving symptoms and have fewer side effects. Excessive fluid administration has not been shown to be beneficial; therefore, the goal should be to maintain euvolemia. If the pain can be adequately controlled and the patient is able to take fluids orally, hospitalization can be avoided. Use of an alpha blocker may increase the rate of spontaneous stone passage. Urologic intervention should be postponed unless there is evidence of UTI, a low probability of spontaneous stone passage (e.g., a stone measuring ≥6 mm or an anatomic abnormality), or intractable pain. A ureteral stent may be placed cystoscopically, but this procedure typically requires general anesthesia, and the stent can be quite uncomfortable, may cause gross hematuria, and may increase the risk of UTI.
Table 5 — Table 5: Acute Management of Renal Colic¶
| Intervention | Indication | Notes |
|---|---|---|
| NSAIDs (e.g., Ketorolac) | Pain control | Preferred over opioids; fewer side effects |
| Alpha Blockers | Spontaneous passage | May increase rate of passage |
| Fluids | Euvolemia | Excessive fluid not beneficial |
| Ureteral Stent/Nephrostomy | UTI, Obstruction, Intractable Pain | Requires general anesthesia; risk of hematuria/UTI |
| ESWL | Stone fragmentation | Least invasive; used less frequently |
| Endourology (Laser/Basket) | Stone removal | More frequently used than ESWL |
| Percutaneous Nephrostolithotomy | Large upper-tract stones | Highest likelihood of stone-free |
7.2 Prevention of New Stone Formation¶
More than half of first-time stone formers will have a recurrence within 10 years. A careful evaluation is indicated to identify predisposing factors, which can then be modified to reduce the risk of new stone formation or growth of existing renal stones. It is appropriate to proceed with an evaluation even after the first stone if the patient is interested because recurrences are common and are usually preventable with inexpensive lifestyle modifications or other treatments. After remediable secondary causes of stone formation (e.g., primary hyperparathyroidism) are excluded, the focus should turn to modification of the urine composition to reduce the risk of new stone formation. The urinary constituents and calculated urine supersaturation are continuous variables, and the associated risk is continuous; thus, there are no definitive thresholds. Dichotomization into "normal" and "abnormal" can be misleading and should be avoided. For all stone types, consistently diluted urine reduces the likelihood of crystal formation. The urine volume should be at least 2 L/d. Because of differences in insensible fluid losses and fluid intake from food sources, the required total fluid intake will vary from person to person. Rather than specify how much to drink, it is more helpful to educate patients about how much more they need to drink in light of their 24-h urine volume. For example, if the daily urine volume is 1.5 L, then the patient should be advised to drink consistently at least 0.5 L more per day in order to increase the urine volume to the goal of 2 L/d. Restriction of nondairy animal protein (e.g., meat, chicken, seafood) is a reasonable approach and may result in higher excretion of citrate and lower excretion of calcium. In addition, reducing sodium intake to <2.5 g/d may decrease urinary excretion of calcium. Sucrose and fructose intake should be minimized. For adherence to a dietary pattern that is more manageable for patients than manipulating individual nutrients, the Mediterranean diet or the DASH (Dietary Approaches to Stop Hypertension) diet provides an appropriate and readily available option. Randomized trials have conclusively shown the DASH diet to reduce blood pressure. At present, only data from observational studies are available, but these demonstrate a strong and consistent inverse association between these healthy dietary patterns and risk of stone formation.
Table 6 — Table 6: Prevention Strategies by Stone Type¶
| Stone Type | Key Risk Factors | Prevention Strategies |
|---|---|---|
| Calcium Oxalate | High Ca, High Oxalate, Low Citrate | Increase fluid; Avoid high-dose Vit C; Maintain dietary Ca; Thiazides if hypercalciuria; Allopurinol if high uric acid; Citrate supplementation if hypocitraturia |
| Uric Acid | Low pH, High Uric Acid | Increase fluid; Alkalinize urine; Allopurinol if high uric acid |
| Struvite | Infection | Treat UTI; Acidify urine |
| Cystine | Low pH, High Cystine | Increase fluid; Alkalinize urine; Chelating agents (e.g., tiopronin) |
| Calcium Phosphate | High pH, High Ca | Increase fluid; Thiazides if hypercalciuria; Citrate supplementation |
7.3 Specific Stone Types¶
Calcium Oxalate: Risk factors for calcium oxalate stones include higher urine calcium, higher urine oxalate, and lower urine citrate. This stone type is insensitive to urine pH in the physiologic range. Individuals with higher urine calcium excretion tend to absorb a higher percentage of ingested calcium. Nevertheless, dietary calcium restriction is not beneficial and, in fact, is likely to be harmful (see "Dietary Risk Factors," above). In a randomized trial in men with high urine calcium and recurrent calcium oxalate stones, a diet containing 1200 mg of calcium and a low intake of sodium and animal protein significantly reduced subsequent stone formation compared with a low-calcium diet (400 mg/d). Excessive calcium intake (>1200 mg/d) should be avoided. A thiazide diuretic, in doses higher than those used to treat hypertension, can substantially lower urine calcium excretion. Several randomized controlled trials, but not all, have demonstrated that thiazide diuretics can reduce calcium oxalate stone recurrence by ~50%. When a thiazide is prescribed, dietary sodium restriction is essential to obtain the desired reduction in urinary calcium excretion and minimize urinary potassium losses. While bisphosphonates may reduce urine calcium excretion in some individuals, there are only observational data to suggest whether this class of medication can reduce stone formation; therefore, bisphosphonates cannot be recommended solely for stone prevention at present, but they can be used to treat those individuals with low bone density. A reduction in urine oxalate will, in turn, reduce the supersaturation of calcium oxalate. In patients with the common form of nephrolithiasis, avoiding high-dose vitamin C supplements is the only known strategy that reduces endogenous oxalate production. In patients with primary hyperoxaluria (type I), an siRNA-based therapy (lumasiran, nedosiran) can reduce oxalate generation in the liver. Oxalate is a metabolic end product; therefore, any dietary oxalate that is absorbed will be excreted in the urine. Reducing absorption of exogenous oxalate involves two approaches. First, the avoidance of foods that contain high amounts of oxalate, such as spinach, rhubarb, almonds, and potatoes, is prudent. However, extreme oxalate restriction has not been demonstrated to reduce stone recurrence and could be harmful to overall health, given other health benefits of many foods that are erroneously considered to be high in oxalate. Second, the absorption of oxalate is reduced by higher calcium intake; therefore, individuals with higher-than-desired urinary oxalate should be counseled to consume adequate calcium. Oxalate absorption can be influenced by the intestinal microbiota, depending on the presence of oxalate-degrading bacteria. Currently, however, there are no available therapies to alter the microbiota that beneficially affect urinary oxalate excretion over the long term. Citrate is a natural inhibitor of calcium oxalate and calcium phosphate stones. Increased consumption of foods rich in alkali (i.e., fruits and vegetables) can increase urine citrate. For patients with lower urine citrate in whom dietary modification does not adequately increase urine citrate, the addition of supplemental alkali (typically potassium citrate or bicarbonate) will lead to an increase in urinary citrate excretion. Sodium salts, such as sodium bicarbonate, while successful in raising urine citrate, are typically avoided due to the adverse effects of sodium on urine calcium excretion. Past reports suggested that higher levels of urine uric acid may increase the risk of calcium oxalate stones, but more recent studies do not support this association. However, allopurinol reduced stone recurrence in one randomized controlled trial in patients with calcium oxalate stones and high urine uric acid levels. The lack of association between urine uric acid level and calcium oxalate stones suggests that a different mechanism underlies the observed beneficial effect of allopurinol in this setting. For patients with the common form of nephrolithiasis, avoiding high-dose vitamin C supplements is the only known strategy that reduces endogenous oxalate production. In patients with primary hyperoxaluria (type I), an siRNA-based therapy (lumasiran, nedosiran) can reduce oxalate generation in the liver. Oxalate is a metabolic end product; therefore, any dietary oxalate that is absorbed will be excreted in the urine. Reducing absorption of exogenous oxalate involves two approaches. First, the avoidance of foods that contain high amounts of oxalate, such as spinach, rhubarb, almonds, and potatoes, is prudent. However, extreme oxalate restriction has not been demonstrated to reduce stone recurrence and could be harmful to overall health, given other health benefits of many foods that are erroneously considered to be high in oxalate. Second, the absorption of oxalate is reduced by higher calcium intake; therefore, individuals with higher-than-desired urinary oxalate should be counseled to consume adequate calcium. Oxalate absorption can be influenced by the intestinal microbiota, depending on the presence of oxalate-degrading bacteria. Currently, however, there are no available therapies to alter the microbiota that beneficially affect urinary oxalate excretion over the long term.
8. PROGNOSIS & COMPLICATIONS¶
More than half of first-time stone formers will have a recurrence within 10 years. Once an individual has had a stone, the prevention of a recurrence is essential. Published recurrence rates vary by the definitions and diagnostic methods used. Some reports have relied on symptomatic events, while others have been based on imaging. Most experts agree that radiographic evidence of a second stone should be considered to represent a recurrence, even if the stone has not yet caused symptoms. Repeat episodes of obstruction and instrumentation can cause a reduction in the glomerular filtration rate (GFR). Intraparenchymal calcium oxalate deposition in the kidney can eventually lead to renal failure. Cystine stones are visible on plain radiographs and often manifest as staghorn calculi or multiple bilateral stones.
8.1 Recurrence Rates¶
More than half of first-time stone formers will have a recurrence within 10 years. Published recurrence rates vary by the definitions and diagnostic methods used. Some reports have relied on symptomatic events, while others have been based on imaging. Most experts agree that radiographic evidence of a second stone should be considered to represent a recurrence, even if the stone has not yet caused symptoms.
9. SPECIAL CONSIDERATIONS¶
Having previous chronic kidney disease or diabetic nephropathy is a risk factor for developing acute kidney injury with COVID-19. Treatment includes antiviral medications and remdesivir, with these medications needing to be adjusted or avoided based on kidney function. Nephrolithiasis is a systemic disorder. Several conditions predispose to stone formation, including gastrointestinal malabsorption (e.g., Crohn's disease, gastric bypass surgery), primary hyperparathyroidism, obesity, type 2 diabetes mellitus, and distal renal tubular acidosis. A number of other medical conditions are more likely to be present in individuals with a history of nephrolithiasis, including hypertension, gout, cardiovascular disease, cholelithiasis, reduced bone mineral density, and chronic kidney disease. Although nephrolithiasis does not directly cause upper urinary tract infections (UTIs), a UTI in the setting of an obstructing stone is a urologic emergency ("pus under pressure") and requires urgent intervention to reestablish drainage.
9.1 Comorbidities¶
A number of other medical conditions are more likely to be present in individuals with a history of nephrolithiasis, including hypertension, gout, cardiovascular disease, cholelithiasis, reduced bone mineral density, and chronic kidney disease.
10. KEY PEARLS & CLINICAL TRAPS¶
The most clinically important inhibitor of calcium-containing stones is urine citrate. While the calculated supersaturation value does not perfectly predict stone formation, it is a useful guide as it integrates the multiple factors that are measured in a 24-h urine collection. The absence of hematuria does not exclude a stone, particularly when urine flow is completely obstructed by a stone. Dietary calcium restriction is not beneficial and, in fact, is likely to be harmful. Higher dietary calcium intake is related to a lower risk of stone formation. Fluid intake is the main determinant of urine volume, and the importance of fluid intake in preventing stone formation has been demonstrated in observational studies and a randomized controlled trial. When the urine output is <1 L/d, the risk of stone formation more than doubles. NSAIDs (e.g., ketorolac) are just as effective as opioids in relieving symptoms and have fewer side effects. Helical CT detects stones as small as 1 mm that may be missed by other imaging modalities. A UTI in the setting of ureteral obstruction is a medical emergency that requires immediate restoration of drainage by placement of either a ureteral stent or a percutaneous nephrostomy tube.
10.1 Clinical Pearls¶
- Urine citrate is the most clinically important inhibitor of calcium-containing stones.
- Dietary calcium restriction is contraindicated; higher intake reduces risk.
- Fluid intake goal: Urine volume ≥2 L/d.
- NSAIDs preferred over opioids for pain.
- CT detects stones as small as 1 mm.
- UTI with obstruction is a urologic emergency.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
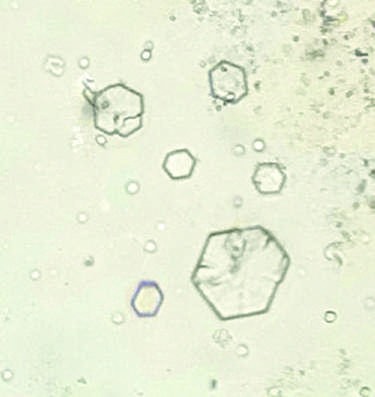
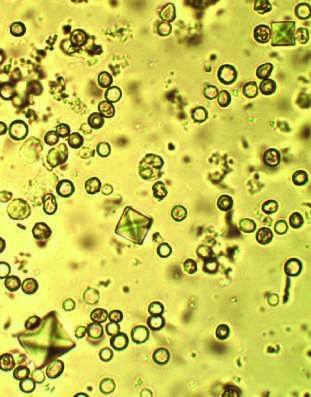
Caption: FIGURE 330-1 Urine sediment from a patient with calcium oxalate stones (left) and a shaped, and cystine crystals are hexagonal. (Left panel image courtesy of Dr. Mark Clinic.) — Figure 330-1: Urine sediment from a patient with calcium oxalate stones (left) and a patient with cystine stones (right). Calcium oxalate dihydrate crystals are bipyramidally shaped, and cystine crystals are hexagonal.
Figure 2¶
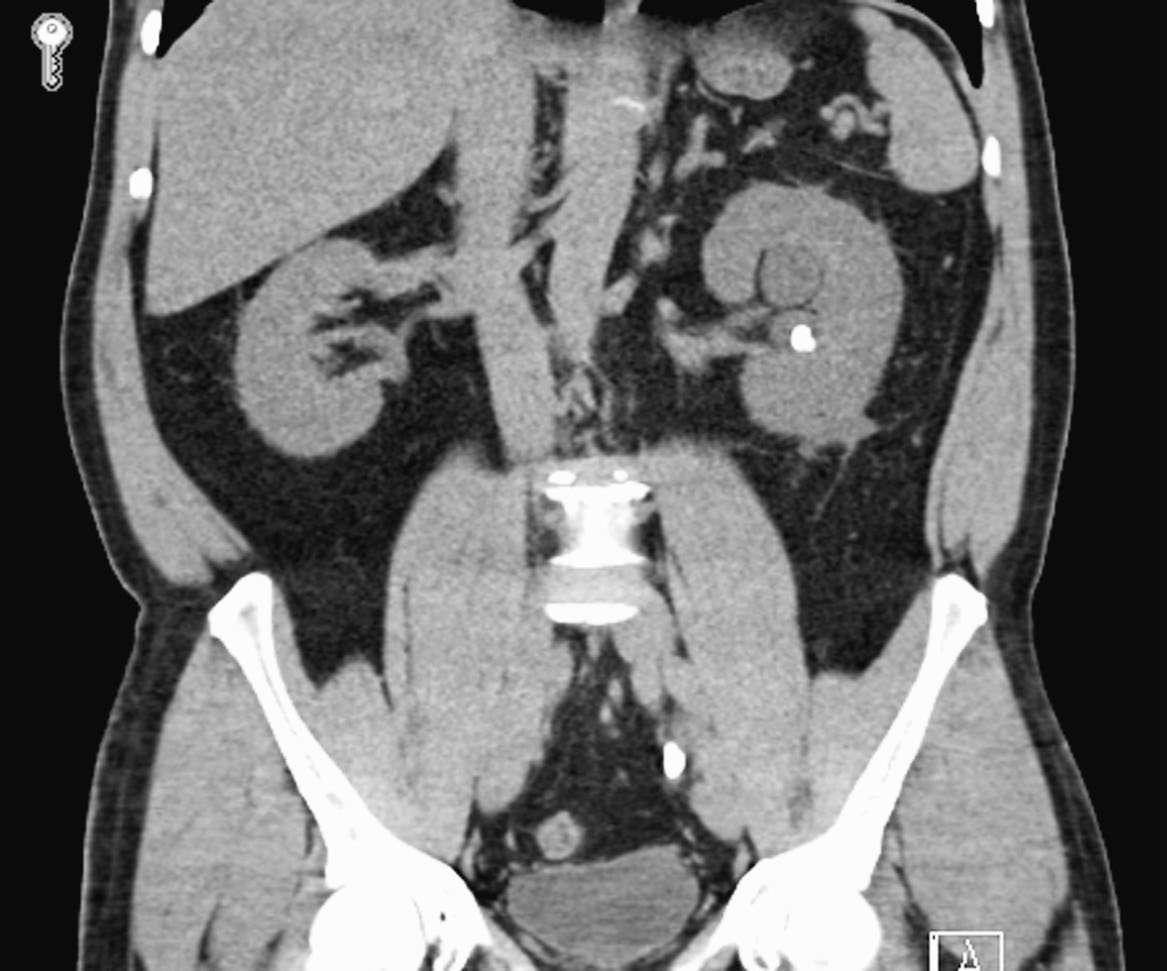
Caption: FIGURE 330-1 Urine sediment from a patient with calcium oxalate stones (left) and a shaped, and cystine crystals are hexagonal. (Left panel image courtesy of Dr. Mark Clinic.) — Figure 330-2: Coronal noncontrast CT image from a patient who presented with left-sided renal colic. An obstructing calculus is present in the distal left ureter at the level of S1, measuring 10 mm in maximal dimension. There is severe left hydroureteronephrosis and associated left perinephric fat stranding.
Figure 3¶
Caption: FIGURE 330-1 Urine sediment from a patient with calcium oxalate stones (left) and a shaped, and cystine crystals are hexagonal. (Left panel image courtesy of Dr. Mark Clinic.) — Figure 330-3: Algorithm for the evaluation and management of nephrolithiasis, including history, physical examination, laboratory evaluation, imaging, and prevention strategies.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.