Chapter 17: Headache¶
Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Headache is the most common reason for seeking medical attention and causes more disability than any other neurologic problem.
- Primary headaches (Tension-type, Migraine, Cluster, Idiopathic stabbing) form the disorder itself; Secondary headaches are caused by exogenous disorders (Infection, Head injury, Vascular, Tumor).
- Pain-producing cranial structures include scalp, meningeal arteries, dural sinuses, falx cerebri, and proximal segments of large pial arteries.
- The trigeminovascular system mediates pain; cranial autonomic symptoms (lacrimation, nasal congestion) are secondary to activation of cranial parasympathetic pathways.
- New-onset severe headache requires evaluation for meningitis, subarachnoid hemorrhage, epidural/subdural hematoma, glaucoma, tumor, and purulent sinusitis.
- Giant cell arteritis (Temporal arteritis) is common in elderly (>50); normal ESR does not exclude the diagnosis; blindness is a major complication.
- Medication-overuse headache is induced by overuse of analgesics; cessation often leads to improvement but residual symptoms may persist.
- Low CSF volume headache is positional (worse upright, better recumbent); MRI with gadolinium shows diffuse meningeal enhancement.
- Idiopathic intracranial hypertension (Pseudotumor Cerebri) is associated with obesity and female gender; treated with acetazolamide and weight loss.
- New Daily Persistent Headache (NDPH) is a distinct syndrome; subarachnoid hemorrhage must be excluded as a secondary cause.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification of Headache Disorders
- 1.2 Anatomy and Physiology of Headache
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Brain Tumor
- 3.2 Meningitis
- 3.3 Intracranial Hemorrhage
- 3.4 Temporal Arteritis
- 3.5 Glaucoma
- 3.6 Chronic Daily Headache
- 3.7 Medication-Related and Medication-Overuse Headache
- 3.8 New Daily Persistent Headache (NDPH)
- 3.9 Low CSF Volume Headache
- 3.10 Raised CSF Pressure Headache
- 3.11 Posttraumatic Headache
- 4. CLINICAL FEATURES
- 4.1 Red Flags and Warning Signs
- 4.2 Chronic Daily Headache Features
- 4.3 New Daily Persistent Headache Features
- 4.4 Low CSF Volume Headache Features
- 4.5 Raised CSF Pressure Headache Features
- 4.6 Posttraumatic Headache Features
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Primary vs Secondary Headache
- 5.2 Differential Diagnosis of New Daily Persistent Headache
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Imaging Studies
- 6.2 Lumbar Puncture
- 6.3 Laboratory Tests
- 6.4 Diagnostic Algorithm for Acute Headache
- 7. MANAGEMENT & TREATMENT
- 7.1 Management of Medication Overuse: Outpatients
- 7.2 Management of Medication Overuse or Treatment-Refractory Headache: Inpatients
- 7.3 Management of Low CSF Volume Headache
- 7.4 Management of Raised CSF Pressure Headache
- 7.5 Management of New Daily Persistent Headache
- 7.6 Management of Medication Overuse: Drug Regimen
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Prognosis of New Daily Persistent Headache
- 8.2 Complications of Giant Cell Arteritis
- 8.3 Prognosis of Idiopathic Intracranial Hypertension
- 9. SPECIAL CONSIDERATIONS
- 9.1 Idiopathic Intracranial Hypertension (Pseudotumor Cerebri)
- 9.2 Posttraumatic Headache
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Magnetic resonance image showing diffuse meningeal enhancement after gadolinium administration in a... |
1. DEFINITION & OVERVIEW¶
Headache is among the most common reasons patients seek medical attention and is responsible, on a global basis, for more disability than any other neurologic problem. Diagnosis and management are based on a careful clinical approach augmented by an understanding of the anatomy, physiology, and pharmacology of the nervous system pathways mediating the various headache syndromes. A classification system developed by the International Headache Society characterizes headache disorders as primary or secondary. Primary headache often results in considerable disability and a decrease in the patient's quality of life. Life-threatening headache is relatively uncommon, with vigilance required to recognize and appropriately treat such patients.
1.1 Classification of Headache Disorders¶
📖 Harrison's defines this as:
Primary headache disorders are those in which headache and its associated features form the disorder itself, whereas secondary headaches are those caused by exogenous disorders.
Primary headache often results in considerable disability and a decrease in the patient's quality of life. Mild secondary headache, such as that seen in association with upper respiratory tract infections, is common but rarely worrisome.
Table 1 — Table 17-1 Common Causes of Headache¶
| PRIMARY HEADACHE | TYPE | % | SECONDARY HEADACHE | TYPE | % |
|---|---|---|---|---|---|
| Tension-type | 69 | Systemic infection | 63 | ||
| Migraine | 16 | Head injury | 4 | ||
| Idiopathic stabbing | 2 | Vascular disorders | 1 | ||
| Cluster | 0.1 | Subarachnoid hemorrhage | <1 | ||
| Brain tumor | 0.1 |
1.2 Anatomy and Physiology of Headache¶
Pain usually occurs when peripheral nociceptors are stimulated in response to tissue injury, visceral distension, or other factors. Pain perception is a normal physiologic response mediated by a healthy nervous system. Pain can also result when pain-producing pathways of the peripheral or central nervous system (CNS) are damaged or activated inappropriately. Headache may originate from either or both mechanisms. Relatively few cranial structures are pain-producing; these include the scalp, meningeal arteries, dural sinuses, falx cerebri, and proximal segments of the large pial arteries. The ventricular ependyma, choroid plexus, pial veins, and much of the brain parenchyma are not pain-producing.
2. EPIDEMIOLOGY¶
Population-based estimates suggest that about 4% of adults have daily or near-daily headache. The prevalence of migraine among the elderly is substantial, considerably higher than that of giant cell arteritis.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Headache may originate from either or both mechanisms: peripheral nociceptor stimulation or damage/activation of pain-producing pathways. Underlying recurrent headache disorders may be activated by pain that follows otologic or endodontic surgical procedures. Thus, pain about the head as the result of diseased tissue or trauma may reawaken an otherwise quiescent migraine syndrome. Treatment of the headache is largely ineffective until the cause of the primary problem is addressed. Serious underlying conditions that are associated with headache are described below.
3.1 Brain Tumor¶
Brain tumor is a rare cause of isolated headache and even less commonly a cause of severe pain. The vast majority of patients presenting with severe headache have a benign cause, usually migraine. Approximately 30% of patients with brain tumors consider headache to be their chief complaint. The head pain is usually nondescript—an intermittent deep, dull aching of moderate intensity, which may worsen with exertion or change in position and may be associated with nausea and vomiting. This pattern of symptoms results from migraine far more often than brain tumor. The headache of brain tumor disturbs sleep in about 10% of patients. Vomiting that precedes the appearance of headache by weeks is highly characteristic of posterior fossa brain tumors. A history of amenorrhea or galactorrhea with headache suggests a possible prolactin-secreting pituitary adenoma or the polycystic ovary syndrome. Headache arising de novo in a patient with known malignancy suggests either cerebral metastases or carcinomatous meningitis.
3.2 Meningitis¶
Acute, severe headache with stiff neck and fever suggests meningitis. Often there is striking accentuation of pain with eye movement. Meningitis can be easily mistaken for migraine in that the cardinal symptoms of pounding headache, photophobia, nausea, and vomiting are frequently present, perhaps reflecting the underlying biology of some of the patients.
3.3 Intracranial Hemorrhage¶
Acute, maximal in 5 min with stiff neck but without fever suggests subarachnoid hemorrhage. A ruptured aneurysm, arteriovenous malformation, or intraparenchymal hemorrhage may also present with headache alone. Rarely, if the hemorrhage is small or below the foramen magnum, the head CT scan can be normal. Therefore, LP may be required to diagnose definitively subarachnoid hemorrhage.
3.4 Temporal Arteritis¶
Temporal (giant cell) arteritis is an inflammatory disorder of arteries that frequently involves the extracranial carotid circulation. It is a common disorder of the elderly; its annual incidence is 77 per 100,000 individuals aged ≥50. The average age of onset is 70 years, and women account for 65% of cases. About half of patients with untreated temporal arteritis develop blindness due to involvement of the ophthalmic artery and its branches; indeed, ischemic optic neuropathy induced by giant cell arteritis is the major cause of rapidly developing bilateral blindness in patients >60 years. Because treatment with glucocorticoids is effective in preventing this complication, prompt recognition of the disorder is important.
3.5 Glaucoma¶
Glaucoma may present with a prostrating headache associated with nausea and vomiting. The headache often starts with severe eye pain. On physical examination, the eye is often red with a fixed, moderately dilated pupil.
3.6 Chronic Daily Headache¶
The broad description of chronic daily headache (CDH) can be applied when a patient experiences headache on 15 days or more per month. CDH is not a single entity, nor a diagnosis; it encompasses a number of different headache syndromes, both primary and secondary. For patients with primary headache disorders, diagnosis of the headache type will guide therapy. Preventive treatments such as tricyclics, either amitriptyline or nortriptyline at doses up to 1 mg/kg, are very useful in patients with CDH arising from migraine or tension-type headache or where the secondary cause has activated the underlying primary headache. Scalp tenderness is present, often to a marked degree; brushing the hair or resting the head on a pillow may be impossible because of pain. Headache is usually worse at night and often aggravated by exposure to cold. Additional findings may include reddened, tender nodules or red streaking of the skin overlying the temporal arteries, and tenderness of the temporal or, less commonly, the occipital arteries.
Table 2 — Table 17-3 Classification of Daily or Near-Daily Headache¶
| PRIMARY | >4 H DAILY | <4 H DAILY | SECONDARY |
|---|---|---|---|
| Chronic migraine | Chronic cluster headache | Posttraumatic head injury | Iatrogenic |
| Postinfectious | Chronic tension-type headache | ||
| Chronic paroxysmal hemicrania | Giant cell arteritis | ||
| Hemicrania continua | SUNCT/SUNA | Sarcoidosis | |
| Hypnic headache | Behçet's syndrome | ||
| New daily persistent headache | Chronic CNS infection |
3.7 Medication-Related and Medication-Overuse Headache¶
Overuse of analgesic medication for headache can aggravate headache frequency, markedly impair the effect of preventive medicines, and induce a state of refractory daily or near-daily headache called medication-overuse headache. A proportion of patients who stop taking analgesics will experience substantial improvement in the severity and frequency of their headache. However, even after cessation of analgesic use, many patients continue to have headache, although they may feel clinically improved in some way, especially if they have been using opioids or barbiturates regularly. The residual symptoms probably represent the underlying primary headache disorder, and most commonly, this issue occurs in patients prone to migraine.
3.8 New Daily Persistent Headache (NDPH)¶
New daily persistent headache (NDPH) is a clinically distinct syndrome with important secondary causes. Clinical Presentation NDPH presents with headache on most if not all days, and the patient can clearly, and often vividly, recall the moment of onset. The headache usually begins abruptly, but onset may be more gradual; evolution over 3 days has been proposed as the upper limit for this syndrome. Patients typically recall the exact day and circumstances of the onset of headache; the new, persistent head pain does not remit. The first priority is to distinguish between a primary and a secondary cause of this syndrome. Subarachnoid hemorrhage is the most serious of the secondary causes and must be excluded either by history or appropriate investigation.
Table 3 — Table 17-4 Differential Diagnosis of New Daily Persistent Headache¶
| PRIMARY | SECONDARY |
|---|---|
| Migrainous-type headache | Subarachnoid hemorrhage |
| Featureless (tension-type) headache | Low cerebrospinal fluid (CSF) volume |
| Raised CSF pressure headache | |
| Posttraumatic headache | |
| Chronic meningitis |
3.9 Low CSF Volume Headache¶
In these syndromes, head pain is positional: it begins when the patient sits upright and resolves upon reclining. The pain, which is occipitofrontal, is usually a dull ache but may be throbbing. Patients with chronic low CSF volume headache typically present with a history of headache from one day to the next that is generally not present on waking but worsens during the day. Recumbency usually improves the headache within minutes, and it can take only minutes to an hour for the pain to return when the patient resumes an upright position. The most common cause of headache due to persistent low CSF volume is CSF leak following LP. Post-LP headache usually begins within 48 h but may be delayed for up to 12 days. Its incidence is between 10 and 30%. Beverages with caffeine may provide temporary relief. Besides LP, index events may include epidural injection or a vigorous Valsalva maneuver, such as from lifting, straining, coughing, clearing the eustachian tubes in an airplane, or multiple orgasms. Spontaneous CSF leaks are well recognized, and the diagnosis should be considered whenever the headache history is typical, even when there is no obvious index event. As time passes from the index event, the postural nature may become less apparent; cases in which the index event occurred several years before the eventual diagnosis have been recognized. Symptoms appear to result from low volume rather than low pressure: although low CSF pressures, typically 0–50 mm CSF, are usually identified, a pressure as high as 140 mm CSF has been noted with a documented leak.
3.10 Raised CSF Pressure Headache¶
Raised CSF pressure is well recognized as a cause of headache. Brain imaging can often reveal the cause, such as a space-occupying lesion. Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) due to raised CSF pressure can be the presenting symptom for patients with idiopathic intracranial hypertension, a disorder associated with obesity, female gender, and, on occasion, pregnancy. The syndrome can also occur without visual problems, particularly when the fundi are normal. These patients typically present with a history of generalized headache that is present on awakening, improves as the day goes on, and worsens with recumbency. Transient visual obscurations are frequent and may occur when the headaches are most severe. The diagnosis is relatively straightforward when papilledema is present, but the possibility must be considered even in patients without funduscopic changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine. Other conditions that characteristically produce headache on rising in the morning or nocturnal headache are obstructive sleep apnea or poorly controlled hypertension.
3.11 Posttraumatic Headache¶
A traumatic event can trigger a headache process that lasts for many months or years after the event. The term trauma is used here in a very broad sense: headache can develop following an injury to the head, but it can also develop after an infectious episode, typically viral meningitis, a flulike illness, or a parasitic infection. Complaints of dizziness, vertigo, and impaired memory can accompany the headache. Symptoms may remit after several weeks or persist for months and even years after the injury. Typically, the neurologic examination is normal and the underlying theme appears to be that a traumatic event involving the pain-producing meninges can trigger a headache process that lasts for many years. Other Causes In one series, one-third of patients with NDPH reported headache beginning after a transient flulike illness characterized by fever, neck stiffness, photophobia, and marked malaise. Evaluation typically reveals no apparent cause for the headache. There is no convincing evidence that persistent Epstein-Barr virus infection plays a role in NDPH. A complicating factor is that many patients undergo LP during the acute illness; iatrogenic low CSF volume headache must be considered in these cases. Post-COVID-19 onset of NDPH is now well documented. CSF-venous fistulas require closure.
4. CLINICAL FEATURES¶
The patient who presents with a new, severe headache has a differential diagnosis that is quite different from the patient with recurrent headaches over many years. In new-onset and severe headache, the probability of finding a potentially serious cause is considerably greater than in recurrent headache. Patients with recent onset of pain require prompt evaluation and appropriate treatment. Serious causes to be considered include meningitis, subarachnoid hemorrhage, epidural or subdural hematoma, glaucoma, tumor, and purulent sinusitis. When worrisome symptoms and signs are present, rapid diagnosis and management are critical. A careful neurologic examination is an essential part of the first step evaluation. In most cases, patients with an abnormal examination, or a history of recent-onset headache, should be evaluated by a computed tomography (CT) or magnetic resonance imaging (MRI) study of the brain. As an initial screening procedure for intracranial pathology in this setting, CT and MRI methods appear to be equally sensitive. In some circumstances, a lumbar puncture (LP) is also required, unless a benign etiology can be otherwise established. A general evaluation of acute headache might include cranial arteries by palpation; cervical spine by the effect of passive movement of the head and by imaging; the investigation of cardiovascular and renal status by blood pressure monitoring and urine examination; and eyes by funduscopy, intraocular pressure measurement, and refraction. The psychological state of the patient should also be evaluated because a relationship exists between head pain, depression, and anxiety. This is intended to identify comorbidity rather than provide an explanation for the headache, because troublesome headache is seldom simply caused by mood change. Although it is notable that some medicines with antidepressant actions are also effective in the preventive treatment of both tension-type headache and migraine, each symptom must be treated optimally.
4.1 Red Flags and Warning Signs¶
Acute, severe headache with stiff neck and fever suggests meningitis. Often there is striking accentuation of pain with eye movement. Meningitis can be easily mistaken for migraine in that the cardinal symptoms of pounding headache, photophobia, nausea, and vomiting are frequently present, perhaps reflecting the underlying biology of some of the patients. Acute, maximal in 5 min with stiff neck but without fever suggests subarachnoid hemorrhage. A ruptured aneurysm, arteriovenous malformation, or intraparenchymal hemorrhage may also present with headache alone. Rarely, if the hemorrhage is small or below the foramen magnum, the head CT scan can be normal. Therefore, LP may be required to diagnose definitively subarachnoid hemorrhage. Brain tumor is a rare cause of isolated headache and even less commonly a cause of severe pain. The vast majority of patients presenting with severe headache have a benign cause, usually migraine. The headache of brain tumor disturbs sleep in about 10% of patients. Vomiting that precedes the appearance of headache by weeks is highly characteristic of posterior fossa brain tumors. Head pain appearing abruptly after bending, lifting, or coughing can be due to a posterior fossa mass, a Chiari malformation, or low cerebrospinal fluid (CSF) volume.
Table 4 — Table 17-2 Headache Symptoms That Suggest a Serious Underlying Disorder¶
| Disorder | Symptoms |
|---|---|
| Sudden-onset headache | First severe headache |
| Vomiting that precedes headache | Subacute worsening over days or weeks |
| Pain induced by bending, lifting, cough | Pain that disturbs sleep or presents immediately upon awakening |
| Known systemic illness | "Worst" headache ever |
| Onset after age 55 | Fever or unexplained systemic signs |
| Abnormal neurologic examination | Pain associated with local tenderness, e.g., region of temporal artery |
4.2 Chronic Daily Headache Features¶
The broad description of chronic daily headache (CDH) can be applied when a patient experiences headache on 15 days or more per month. CDH is not a single entity, nor a diagnosis; it encompasses a number of different headache syndromes, both primary and secondary. For patients with primary headache disorders, diagnosis of the headache type will guide therapy. Preventive treatments such as tricyclics, either amitriptyline or nortriptyline at doses up to 1 mg/kg, are very useful in patients with CDH arising from migraine or tension-type headache or where the secondary cause has activated the underlying primary headache. Scalp tenderness is present, often to a marked degree; brushing the hair or resting the head on a pillow may be impossible because of pain. Headache is usually worse at night and often aggravated by exposure to cold. Additional findings may include reddened, tender nodules or red streaking of the skin overlying the temporal arteries, and tenderness of the temporal or, less commonly, the occipital arteries. The erythrocyte sedimentation rate (ESR) is often, although not always, elevated; a normal ESR does not exclude giant cell arteritis. A temporal artery biopsy followed by immediate treatment with prednisone 80 mg daily for the first 4–6 weeks should be initiated when clinical suspicion is high. The prevalence of migraine among the elderly is substantial, considerably higher than that of giant cell arteritis. Migraineurs often report amelioration of their headaches with prednisone; thus, caution must be used when interpreting the therapeutic response.
4.3 New Daily Persistent Headache Features¶
New daily persistent headache (NDPH) is a clinically distinct syndrome with important secondary causes. Clinical Presentation NDPH presents with headache on most if not all days, and the patient can clearly, and often vividly, recall the moment of onset. The headache usually begins abruptly, but onset may be more gradual; evolution over 3 days has been proposed as the upper limit for this syndrome. Patients typically recall the exact day and circumstances of the onset of headache; the new, persistent head pain does not remit. The first priority is to distinguish between a primary and a secondary cause of this syndrome. Subarachnoid hemorrhage is the most serious of the secondary causes and must be excluded either by history or appropriate investigation.
4.4 Low CSF Volume Headache Features¶
In these syndromes, head pain is positional: it begins when the patient sits upright and resolves upon reclining. The pain, which is occipitofrontal, is usually a dull ache but may be throbbing. Patients with chronic low CSF volume headache typically present with a history of headache from one day to the next that is generally not present on waking but worsens during the day. Recumbency usually improves the headache within minutes, and it can take only minutes to an hour for the pain to return when the patient resumes an upright position. The most common cause of headache due to persistent low CSF volume is CSF leak following LP. Post-LP headache usually begins within 48 h but may be delayed for up to 12 days. Its incidence is between 10 and 30%. Beverages with caffeine may provide temporary relief. Besides LP, index events may include epidural injection or a vigorous Valsalva maneuver, such as from lifting, straining, coughing, clearing the eustachian tubes in an airplane, or multiple orgasms. Spontaneous CSF leaks are well recognized, and the diagnosis should be considered whenever the headache history is typical, even when there is no obvious index event. As time passes from the index event, the postural nature may become less apparent; cases in which the index event occurred several years before the eventual diagnosis have been recognized. Symptoms appear to result from low volume rather than low pressure: although low CSF pressures, typically 0–50 mm CSF, are usually identified, a pressure as high as 140 mm CSF has been noted with a documented leak.
4.5 Raised CSF Pressure Headache Features¶
Raised CSF pressure is well recognized as a cause of headache. Brain imaging can often reveal the cause, such as a space-occupying lesion. Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) due to raised CSF pressure can be the presenting symptom for patients with idiopathic intracranial hypertension, a disorder associated with obesity, female gender, and, on occasion, pregnancy. The syndrome can also occur without visual problems, particularly when the fundi are normal. These patients typically present with a history of generalized headache that is present on awakening, improves as the day goes on, and worsens with recumbency. Transient visual obscurations are frequent and may occur when the headaches are most severe. The diagnosis is relatively straightforward when papilledema is present, but the possibility must be considered even in patients without funduscopic changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine. Other conditions that characteristically produce headache on rising in the morning or nocturnal headache are obstructive sleep apnea or poorly controlled hypertension.
4.6 Posttraumatic Headache Features¶
A traumatic event can trigger a headache process that lasts for many months or years after the event. The term trauma is used here in a very broad sense: headache can develop following an injury to the head, but it can also develop after an infectious episode, typically viral meningitis, a flulike illness, or a parasitic infection. Complaints of dizziness, vertigo, and impaired memory can accompany the headache. Symptoms may remit after several weeks or persist for months and even years after the injury. Typically, the neurologic examination is normal and the underlying theme appears to be that a traumatic event involving the pain-producing meninges can trigger a headache process that lasts for many years. Other Causes In one series, one-third of patients with NDPH reported headache beginning after a transient flulike illness characterized by fever, neck stiffness, photophobia, and marked malaise. Evaluation typically reveals no apparent cause for the headache. There is no convincing evidence that persistent Epstein-Barr virus infection plays a role in NDPH. A complicating factor is that many patients undergo LP during the acute illness; iatrogenic low CSF volume headache must be considered in these cases. Post-COVID-19 onset of NDPH is now well documented. CSF-venous fistulas require closure.
5. DIFFERENTIAL DIAGNOSIS¶
The patient who presents with a new, severe headache has a differential diagnosis that is quite different from the patient with recurrent headaches over many years. In new-onset and severe headache, the probability of finding a potentially serious cause is considerably greater than in recurrent headache. Patients with recent onset of pain require prompt evaluation and appropriate treatment. Serious causes to be considered include meningitis, subarachnoid hemorrhage, epidural or subdural hematoma, glaucoma, tumor, and purulent sinusitis. When worrisome symptoms and signs are present, rapid diagnosis and management are critical. A careful neurologic examination is an essential part of the first step evaluation. In most cases, patients with an abnormal examination, or a history of recent-onset headache, should be evaluated by a computed tomography (CT) or magnetic resonance imaging (MRI) study of the brain. As an initial screening procedure for intracranial pathology in this setting, CT and MRI methods appear to be equally sensitive. In some circumstances, a lumbar puncture (LP) is also required, unless a benign etiology can be otherwise established. A general evaluation of acute headache might include cranial arteries by palpation; cervical spine by the effect of passive movement of the head and by imaging; the investigation of cardiovascular and renal status by blood pressure monitoring and urine examination; and eyes by funduscopy, intraocular pressure measurement, and refraction. The psychological state of the patient should also be evaluated because a relationship exists between head pain, depression, and anxiety. This is intended to identify comorbidity rather than provide an explanation for the headache, because troublesome headache is seldom simply caused by mood change. Although it is notable that some medicines with antidepressant actions are also effective in the preventive treatment of both tension-type headache and migraine, each symptom must be treated optimally.
5.1 Primary vs Secondary Headache¶
Primary headache disorders generally manifest as headache and associated features occurring in the absence of any exogenous cause. The most common are migraine, tension-type headache, and the trigeminal autonomic cephalalgias (TACs), notably cluster headache. These entities are discussed in detail in Chap. 441. Primary headaches are those in which headache and its associated features form the disorder itself, whereas secondary headaches are those caused by exogenous disorders (Headache Classification Committee of the International Headache Society, 2018). Primary headache often results in considerable disability and a decrease in the patient's quality of life. Life-threatening headache is relatively uncommon, with vigilance required to recognize and appropriately treat such patients.
5.2 Differential Diagnosis of New Daily Persistent Headache¶
New daily persistent headache (NDPH) is a clinically distinct syndrome with important secondary causes. The first priority is to distinguish between a primary and a secondary cause of this syndrome. Subarachnoid hemorrhage is the most serious of the secondary causes and must be excluded either by history or appropriate investigation.
Table 5 — Table 17-4 Differential Diagnosis of New Daily Persistent Headache¶
| PRIMARY | SECONDARY |
|---|---|
| Migrainous-type headache | Subarachnoid hemorrhage |
| Featureless (tension-type) headache | Low cerebrospinal fluid (CSF) volume |
| Raised CSF pressure headache | |
| Posttraumatic headache | |
| Chronic meningitis |
6. INVESTIGATIONS & DIAGNOSIS¶
A careful neurologic examination is an essential part of the first step evaluation. In most cases, patients with an abnormal examination, or a history of recent-onset headache, should be evaluated by a computed tomography (CT) or magnetic resonance imaging (MRI) study of the brain. As an initial screening procedure for intracranial pathology in this setting, CT and MRI methods appear to be equally sensitive. In some circumstances, a lumbar puncture (LP) is also required, unless a benign etiology can be otherwise established. A general evaluation of acute headache might include cranial arteries by palpation; cervical spine by the effect of passive movement of the head and by imaging; the investigation of cardiovascular and renal status by blood pressure monitoring and urine examination; and eyes by funduscopy, intraocular pressure measurement, and refraction. The psychological state of the patient should also be evaluated because a relationship exists between head pain, depression, and anxiety. This is intended to identify comorbidity rather than provide an explanation for the headache, because troublesome headache is seldom simply caused by mood change. Although it is notable that some medicines with antidepressant actions are also effective in the preventive treatment of both tension-type headache and migraine, each symptom must be treated optimally.
6.1 Imaging Studies¶
In most cases, patients with an abnormal examination, or a history of recent-onset headache, should be evaluated by a computed tomography (CT) or magnetic resonance imaging (MRI) study of the brain. As an initial screening procedure for intracranial pathology in this setting, CT and MRI methods appear to be equally sensitive. When imaging is indicated to identify the source of a presumed leak, an MRI with gadolinium is the initial study of choice. A striking pattern of diffuse meningeal enhancement is so typical that in the appropriate clinical context the diagnosis is established. Chiari malformations may sometimes be noted on MRI; in such cases, surgery to decompress the posterior fossa is not indicated and usually worsens the headache. Spinal MRI with T2 weighting may reveal a leak, and spinal MRI may demonstrate spinal meningeal cysts whose role in these syndromes is yet to be elucidated. The source of CSF leakage may be identified by spinal MRI with appropriate sequences, or by CT, preferably lateral decubitus digital subtraction, myelography. In the absence of a directly identified site of leakage, 111In-DTPA CSF studies may demonstrate early emptying of the tracer into the bladder or slow progress of tracer across the brain suggesting a CSF leak; this procedure is now only rarely employed. CT or MRI studies are unrevealing. Chronic subdural hematoma may on occasion mimic this disorder. Posttraumatic headache may also be seen after carotid dissection and subarachnoid hemorrhage and after intracranial surgery. The underlying theme appears to be that a traumatic event involving the pain-producing meninges can trigger a headache process that lasts for many years.
6.2 Lumbar Puncture¶
In some circumstances, a lumbar puncture (LP) is also required, unless a benign etiology can be otherwise established. In the absence of fundal changes, an elevated opening pressure and improvement in headache following removal of CSF are diagnostic. This should be done when the patient is symptomatic so that both the pressure and the response to removal of 20–30 mL of CSF can be determined. An elevated opening pressure and improvement in headache following removal of CSF are diagnostic in the absence of fundal changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine. Other conditions that characteristically produce headache on rising in the morning or nocturnal headache are obstructive sleep apnea or poorly controlled hypertension.
6.3 Laboratory Tests¶
The urinalysis may reveal the state of hydration or rule out severe renal disease, diabetes, or urinary infection. Blood urea nitrogen, glucose, and serum bilirubin levels and liver function tests may be helpful. Serum amylase levels may be increased by many diseases other than pancreatitis, for example, perforated ulcer, strangulating intestinal obstruction, and acute cholecystitis; thus, elevations of serum amylase do not rule in or rule out the need for an operation. Plain and upright or lateral decubitus radiographs of the abdomen have limited utility and may be unnecessary in some patients who have substantial evidence of some diseases such as acute appendicitis or strangulated external hernia. Where the indications for surgical or medical intervention are not clear, low-dose computed tomography is preferred to abdominal radiography when evaluating nontraumatic acute abdominal pain. Very rarely, barium or water-soluble contrast study of the upper part of the gastrointestinal tract is an appropriate radiographic investigation and may demonstrate partial intestinal obstruction that may elude diagnosis by other means. If there is any question of obstruction of the colon, oral administration of barium sulfate should be avoided. On the other hand, in cases of suspected colonic obstruction (without perforation), a contrast enema may be diagnostic. Mild secondary headache, such as that seen in association with upper respiratory tract infections, is common but rarely worrisome. The erythrocyte sedimentation rate (ESR) is often, although not always, elevated; a normal ESR does not exclude giant cell arteritis.
6.4 Diagnostic Algorithm for Acute Headache¶
- Evaluate patient with new, severe headache.
- Perform careful neurologic examination.
- If abnormal examination or history of recent-onset headache: a. Evaluate by CT or MRI study of the brain. b. Consider lumbar puncture (LP) if benign etiology not established.
- General evaluation: a. Cranial arteries by palpation. b. Cervical spine by passive movement and imaging. c. Cardiovascular and renal status by blood pressure monitoring and urine examination. d. Eyes by funduscopy, intraocular pressure measurement, and refraction.
- Evaluate psychological state (depression, anxiety).
- If imaging indicated for leak source: a. MRI with gadolinium (initial study of choice). b. Spinal MRI with T2 weighting. c. CT, preferably lateral decubitus digital subtraction, myelography. d. 111In-DTPA CSF studies if no directly identified site of leakage.
7. MANAGEMENT & TREATMENT¶
The management of secondary headache focuses on diagnosis and treatment of the underlying condition. The management of medically intractable headache is difficult, although recent developments in therapy have proved effective. Monoclonal antibodies to CGRP or its receptor, or CGRP receptor antagonists (gepants), are effective and well-tolerated in chronic migraine and licensed for use in clinical practice. Noninvasive neuromodulatory approaches, such as single-pulse transcranial magnetic stimulation and remote electrical neuromodulation, which respectively, in migraine have been used in clinical practice with success. Noninvasive vagal nerve stimulation has also shown promise, particularly in cluster headache, chronic paroxysmal hemicrania, and hemicrania continua, and possibly in short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT). Other modalities are discussed in Chap. 441. For patients who overuse analgesic medications, it is often helpful to reduce and eliminate them, although this strategy is far from universally effective. One approach is to reduce the medication dose by 10% every 1–2 weeks. Immediate cessation of analgesic use is possible for some patients, provided there is no contraindication. Both approaches are facilitated by use of a medication diary maintained during the month or two before cessation; this helps to identify the scope of the problem. A small dose of a nonsteroidal anti-inflammatory drug (NSAID) such as naproxen, 500 mg bid, if tolerated, will help relieve residual pain as analgesic use is reduced. NSAID overuse is not usually a problem for patients with daily or headache when a NSAID with a longer half-life is taken once or twice daily. Once the patient has substantially reduced analgesic use, a preventive medication should be introduced. Another widely used approach is to commence the preventive at the same time the analgesic reduction is started; both approaches are supported by controlled trial data. A common cause of unresponsiveness to treatment is the use of a preventive when analgesics continue to be used regularly. For some patients, discontinuing analgesics is very difficult; often the best approach is to inform the patient that some degree of pain is inevitable during this initial period. Some patients will require hospitalization for detoxification and management. Such patients have typically failed efforts at outpatient withdrawal or have a significant medical condition, such as diabetes mellitus or epilepsy, that would complicate withdrawal as an outpatient. Following admission to the hospital, medications are withdrawn completely on the first day, in the absence of a contraindication. Antiemetics and fluids are administered as required; clonidine is used for opioid withdrawal symptoms. For acute intolerable pain during the waking hours, aspirin, 1 g IV (not approved in United States), is useful. IM chlorpromazine can be helpful at night; patients must be adequately hydrated. Three to five days into the admission, as the effect of the withdrawn substance wears off, a course of IV dihydroergotamine (DHE) can be used. DHE, administered every 8 h for 5 consecutive days, a treatment that is not stopped short if headache settles, can induce a significant remission that allows a preventive treatment to be established. Serotonin 5-HT receptor antagonists, such as ondansetron or granisetron, or the neurokinin receptor antagonist aprepitant may be required with DHE to prevent significant nausea, and domperidone (not approved in the United States) orally or by suppository can be very helpful. Avoiding sedating or otherwise side effect–prone antiemetics is helpful. Alternatives include a 7- to 10-day course of IV lidocaine or IV divalproex sodium or use of the CGRP antagonist eptinezumab intravenously. Initial treatment for low CSF volume headache is bed rest. For patients with persistent pain, IV caffeine (500 mg in 500 mL of saline administered over 2 h) can be very effective. An electrocardiogram (ECG) to screen for arrhythmia should be performed before administration. It is reasonable to administer at least two infusions of caffeine before embarking on additional tests to identify the source of the CSF leak. Because IV caffeine is safe and can be curative, it spares many patients the need for further investigations. If unsuccessful, an abdominal binder may be helpful. If a leak can be identified, an autologous blood patch is usually curative. A blood patch is also effective for post-LP headache; in this setting, the location is empirically determined to be the site of the LP. In patients with intractable headache, oral theophylline is a useful alternative that can take some months to be effective. Initial treatment is with acetazolamide (250–500 mg bid); the headache may improve within weeks. A plan for weight loss should also be instituted when required. If ineffective, topiramate is the next treatment of choice; it has many actions that may be useful in this setting, including carbonic anhydrase inhibition, weight loss, and neuronal membrane stabilization, likely mediated via effects on phosphorylation pathways. Severely disabled patients who do not respond to medical treatment require intracranial pressure monitoring and may require shunting. After treatment has been initiated, follow-up care is essential to identify whether progress has been made against the headache complaint. Not all headaches will respond to treatment, but, in general, worrisome headaches will progress and will be easier to identify. When a primary care physician feels the diagnosis is a primary headache disorder, it is worth noting that >90% of patients who present to primary care with a complaint of headache will have migraine. In general, patients who do not have a clear diagnosis, have a primary headache disorder other than migraine or tension-type headache, or are unresponsive to two or more standard therapies for the considered headache type should be referred to a specialist. In a practical sense, the threshold for referral is also determined by the experience of the primary care physician in headache medicine and the availability of secondary care options.
7.1 Management of Medication Overuse: Outpatients¶
For patients who overuse analgesic medications, it is often helpful to reduce and eliminate them, although this strategy is far from universally effective. One approach is to reduce the medication dose by 10% every 1–2 weeks. Immediate cessation of analgesic use is possible for some patients, provided there is no contraindication. Both approaches are facilitated by use of a medication diary maintained during the month or two before cessation; this helps to identify the scope of the problem. A small dose of a nonsteroidal anti-inflammatory drug (NSAID) such as naproxen, 500 mg bid, if tolerated, will help relieve residual pain as analgesic use is reduced.
7.2 Management of Medication Overuse or Treatment-Refractory Headache: Inpatients¶
Some patients will require hospitalization for detoxification and management. Such patients have typically failed efforts at outpatient withdrawal or have a significant medical condition, such as diabetes mellitus or epilepsy, that would complicate withdrawal as an outpatient. Following admission to the hospital, medications are withdrawn completely on the first day, in the absence of a contraindication. Antiemetics and fluids are administered as required; clonidine is used for opioid withdrawal symptoms. For acute intolerable pain during the waking hours, aspirin, 1 g IV (not approved in United States), is useful. IM chlorpromazine can be helpful at night; patients must be adequately hydrated. Three to five days into the admission, as the effect of the withdrawn substance wears off, a course of IV dihydroergotamine (DHE) can be used. DHE, administered every 8 h for 5 consecutive days, a treatment that is not stopped short if headache settles, can induce a significant remission that allows a preventive treatment to be established. Serotonin 5-HT receptor antagonists, such as ondansetron or granisetron, or the neurokinin receptor antagonist aprepitant may be required with DHE to prevent significant nausea, and domperidone (not approved in the United States) orally or by suppository can be very helpful. Avoiding sedating or otherwise side effect–prone antiemetics is helpful. Alternatives include a 7- to 10-day course of IV lidocaine or IV divalproex sodium or use of the CGRP antagonist eptinezumab intravenously.
7.3 Management of Low CSF Volume Headache¶
Initial treatment for low CSF volume headache is bed rest. For patients with persistent pain, IV caffeine (500 mg in 500 mL of saline administered over 2 h) can be very effective. An electrocardiogram (ECG) to screen for arrhythmia should be performed before administration. It is reasonable to administer at least two infusions of caffeine before embarking on additional tests to identify the source of the CSF leak. Because IV caffeine is safe and can be curative, it spares many patients the need for further investigations. If unsuccessful, an abdominal binder may be helpful. If a leak can be identified, an autologous blood patch is usually curative. A blood patch is also effective for post-LP headache; in this setting, the location is empirically determined to be the site of the LP. In patients with intractable headache, oral theophylline is a useful alternative that can take some months to be effective.
7.4 Management of Raised CSF Pressure Headache¶
Initial treatment is with acetazolamide (250–500 mg bid); the headache may improve within weeks. A plan for weight loss should also be instituted when required. If ineffective, topiramate is the next treatment of choice; it has many actions that may be useful in this setting, including carbonic anhydrase inhibition, weight loss, and neuronal membrane stabilization, likely mediated via effects on phosphorylation pathways. Severely disabled patients who do not respond to medical treatment require intracranial pressure monitoring and may require shunting.
7.5 Management of New Daily Persistent Headache¶
Treatment is largely empirical and directed at the headache phenotype. Tricyclic antidepressants, notably amitriptyline, and anticonvulsants, such as topiramate, valproate, candesartan, and gabapentin, have been used with reported benefit, as have CGRP pathway blockers (monoclonal antibodies and gepants). The monoamine oxidase inhibitor phenelzine may also be useful in carefully selected patients. The headache usually resolves within 3–5 years, but it can be quite disabling.
7.6 Management of Medication Overuse: Drug Regimen¶
- Amitriptyline: 10–25 mg daily, up to 1 mg/kg
- Naproxen: 500 mg bid
- Aspirin: 1 g IV (not approved in United States)
- Acetazolamide: 250–500 mg bid
- Prednisone: 80 mg daily for 4–6 weeks
- IV Caffeine: 500 mg in 500 mL saline over 2 h
- Dihydroergotamine (DHE): Every 8 h for 5 consecutive days
- Ondansetron/Granisetron/Aprepitron: With DHE to prevent nausea
- Domperidone: Orally or by suppository (not approved in United States)
- IV Lidocaine: 7- to 10-day course
- IV Divalproex sodium: Alternative
- Eptinezumab: CGRP antagonist intravenously
- Theophylline: Oral alternative for intractable headache
8. PROGNOSIS & COMPLICATIONS¶
The headache usually resolves within 3–5 years, but it can be quite disabling. About half of patients with untreated temporal arteritis develop blindness due to involvement of the ophthalmic artery and its branches; indeed, ischemic optic neuropathy induced by giant cell arteritis is the major cause of rapidly developing bilateral blindness in patients >60 years. Because treatment with glucocorticoids is effective in preventing this complication, prompt recognition of the disorder is important. The syndrome can also occur without visual problems, particularly when the fundi are normal. Transient visual obscurations are frequent and may occur when the headaches are most severe. The diagnosis is relatively straightforward when papilledema is present, but the possibility must be considered even in patients without funduscopic changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine. Other conditions that characteristically produce headache on rising in the morning or nocturnal headache are obstructive sleep apnea or poorly controlled hypertension. Not all headaches will respond to treatment, but, in general, worrisome headaches will progress and will be easier to identify. When a primary care physician feels the diagnosis is a primary headache disorder, it is worth noting that >90% of patients who present to primary care with a complaint of headache will have migraine. In general, patients who do not have a clear diagnosis, have a primary headache disorder other than migraine or tension-type headache, or are unresponsive to two or more standard therapies for the considered headache type should be referred to a specialist. In a practical sense, the threshold for referral is also determined by the experience of the primary care physician in headache medicine and the availability of secondary care options.
8.1 Prognosis of New Daily Persistent Headache¶
The headache usually resolves within 3–5 years, but it can be quite disabling.
8.2 Complications of Giant Cell Arteritis¶
About half of patients with untreated temporal arteritis develop blindness due to involvement of the ophthalmic artery and its branches; indeed, ischemic optic neuropathy induced by giant cell arteritis is the major cause of rapidly developing bilateral blindness in patients >60 years. Because treatment with glucocorticoids is effective in preventing this complication, prompt recognition of the disorder is important.
8.3 Prognosis of Idiopathic Intracranial Hypertension¶
The syndrome can also occur without visual problems, particularly when the fundi are normal. Transient visual obscurations are frequent and may occur when the headaches are most severe. The diagnosis is relatively straightforward when papilledema is present, but the possibility must be considered even in patients without funduscopic changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine.
9. SPECIAL CONSIDERATIONS¶
The syndrome can also occur without visual problems, particularly when the fundi are normal. These patients typically present with a history of generalized headache that is present on awakening, improves as the day goes on, and worsens with recumbency. Transient visual obscurations are frequent and may occur when the headaches are most severe. The diagnosis is relatively straightforward when papilledema is present, but the possibility must be considered even in patients without funduscopic changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine. Other conditions that characteristically produce headache on rising in the morning or nocturnal headache are obstructive sleep apnea or poorly controlled hypertension. Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) due to raised CSF pressure can be the presenting symptom for patients with idiopathic intracranial hypertension, a disorder associated with obesity, female gender, and, on occasion, pregnancy.
9.1 Idiopathic Intracranial Hypertension (Pseudotumor Cerebri)¶
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) due to raised CSF pressure can be the presenting symptom for patients with idiopathic intracranial hypertension, a disorder associated with obesity, female gender, and, on occasion, pregnancy. The syndrome can also occur without visual problems, particularly when the fundi are normal. These patients typically present with a history of generalized headache that is present on awakening, improves as the day goes on, and worsens with recumbency. Transient visual obscurations are frequent and may occur when the headaches are most severe. The diagnosis is relatively straightforward when papilledema is present, but the possibility must be considered even in patients without funduscopic changes. Formal visual field testing should be performed even in the absence of overt ophthalmic involvement. Partial obstructions of the cerebral venous sinuses are found in a small number of cases. In addition, persistently raised intracranial pressure can trigger a syndrome of chronic migraine.
9.2 Posttraumatic Headache¶
A traumatic event can trigger a headache process that lasts for many months or years after the event. The term trauma is used here in a very broad sense: headache can develop following an injury to the head, but it can also develop after an infectious episode, typically viral meningitis, a flulike illness, or a parasitic infection. Complaints of dizziness, vertigo, and impaired memory can accompany the headache. Symptoms may remit after several weeks or persist for months and even years after the injury. Typically, the neurologic examination is normal and the underlying theme appears to be that a traumatic event involving the pain-producing meninges can trigger a headache process that lasts for many years. Other Causes In one series, one-third of patients with NDPH reported headache beginning after a transient flulike illness characterized by fever, neck stiffness, photophobia, and marked malaise. Evaluation typically reveals no apparent cause for the headache. There is no convincing evidence that persistent Epstein-Barr virus infection plays a role in NDPH. A complicating factor is that many patients undergo LP during the acute illness; iatrogenic low CSF volume headache must be considered in these cases. Post-COVID-19 onset of NDPH is now well documented. CSF-venous fistulas require closure.
10. KEY PEARLS & CLINICAL TRAPS¶
Migraine and other primary headache disorders are not "vascular headaches"; these disorders do not reliably manifest vascular changes, and treatment outcomes cannot be predicted by vascular effects. Migraine is a brain disorder and is best understood and managed as such. Cranial autonomic symptoms, such as lacrimation, conjunctival injection, nasal congestion, rhinorrhea, periorbital swelling, aural fullness, and ptosis, are prominent in the trigeminal autonomic cephalalgias (TACs), including cluster headache and paroxysmal hemicrania, and are often seen in migraine, even in children. These cranial autonomic symptoms reflect activation of cranial parasympathetic pathways, and functional imaging studies indicate that vascular changes in migraine and cluster headache, when present, are similarly driven by these cranial autonomic systems. Thus, they are secondary, and not causative, in the headache cascade. Moreover, they can often be mistaken for symptoms or signs of cranial sinus inflammation, which is then overdiagnosed and inappropriately managed. The erythrocyte sedimentation rate (ESR) is often, although not always, elevated; a normal ESR does not exclude giant cell arteritis. A temporal artery biopsy followed by immediate treatment with prednisone 80 mg daily for the first 4–6 weeks should be initiated when clinical suspicion is high. The prevalence of migraine among the elderly is substantial, considerably higher than that of giant cell arteritis. Migraineurs often report amelioration of their headaches with prednisone; thus, caution must be used when interpreting the therapeutic response. Head pain appearing abruptly after bending, lifting, or coughing can be due to a posterior fossa mass, a Chiari malformation, or low cerebrospinal fluid (CSF) volume. Vomiting that precedes the appearance of headache by weeks is highly characteristic of posterior fossa brain tumors. Headache arising de novo in a patient with known malignancy suggests either cerebral metastases or carcinomatous meningitis. About half of patients with untreated temporal arteritis develop blindness due to involvement of the ophthalmic artery and its branches; indeed, ischemic optic neuropathy induced by giant cell arteritis is the major cause of rapidly developing bilateral blindness in patients >60 years. Because treatment with glucocorticoids is effective in preventing this complication, prompt recognition of the disorder is important. The most common cause of headache due to persistent low CSF volume is CSF leak following LP. Post-LP headache usually begins within 48 h but may be delayed for up to 12 days. Its incidence is between 10 and 30%. Beverages with caffeine may provide temporary relief. Besides LP, index events may include epidural injection or a vigorous Valsalva maneuver, such as from lifting, straining, coughing, clearing the eustachian tubes in an airplane, or multiple orgasms. Spontaneous CSF leaks are well recognized, and the diagnosis should be considered whenever the headache history is typical, even when there is no obvious index event. As time passes from the index event, the postural nature may become less apparent; cases in which the index event occurred several years before the eventual diagnosis have been recognized. Symptoms appear to result from low volume rather than low pressure: although low CSF pressures, typically 0–50 mm CSF, are usually identified, a pressure as high as 140 mm CSF has been noted with a documented leak. A striking pattern of diffuse meningeal enhancement is so typical that in the appropriate clinical context the diagnosis is established. Chiari malformations may sometimes be noted on MRI; in such cases, surgery to decompress the posterior fossa is not indicated and usually worsens the headache. Spinal MRI with T2 weighting may reveal a leak, and spinal MRI may demonstrate spinal meningeal cysts whose role in these syndromes is yet to be elucidated. The source of CSF leakage may be identified by spinal MRI with appropriate sequences, or by CT, preferably lateral decubitus digital subtraction, myelography. In the absence of a directly identified site of leakage, 111In-DTPA CSF studies may demonstrate early emptying of the tracer into the bladder or slow progress of tracer across the brain suggesting a CSF leak; this procedure is now only rarely employed. CT or MRI studies are unrevealing. Chronic subdural hematoma may on occasion mimic this disorder. Posttraumatic headache may also be seen after carotid dissection and subarachnoid hemorrhage and after intracranial surgery. The underlying theme appears to be that a traumatic event involving the pain-producing meninges can trigger a headache process that lasts for many years. In one series, one-third of patients with NDPH reported headache beginning after a transient flulike illness characterized by fever, neck stiffness, photophobia, and marked malaise. Evaluation typically reveals no apparent cause for the headache. There is no convincing evidence that persistent Epstein-Barr virus infection plays a role in NDPH. A complicating factor is that many patients undergo LP during the acute illness; iatrogenic low CSF volume headache must be considered in these cases. Post-COVID-19 onset of NDPH is now well documented. CSF-venous fistulas require closure. The management of secondary headache focuses on diagnosis and treatment of the underlying condition. The management of medically intractable headache is difficult, although recent developments in therapy have proved effective. Monoclonal antibodies to CGRP or its receptor, or CGRP receptor antagonists (gepants), are effective and well-tolerated in chronic migraine and licensed for use in clinical practice. Noninvasive neuromodulatory approaches, such as single-pulse transcranial magnetic stimulation and remote electrical neuromodulation, which respectively, in migraine have been used in clinical practice with success. Noninvasive vagal nerve stimulation has also shown promise, particularly in cluster headache, chronic paroxysmal hemicrania, and hemicrania continua, and possibly in short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT). Other modalities are discussed in Chap. 441. For patients who overuse analgesic medications, it is often helpful to reduce and eliminate them, although this strategy is far from universally effective. One approach is to reduce the medication dose by 10% every 1–2 weeks. Immediate cessation of analgesic use is possible for some patients, provided there is no contraindication. Both approaches are facilitated by use of a medication diary maintained during the month or two before cessation; this helps to identify the scope of the problem. A small dose of a nonsteroidal anti-inflammatory drug (NSAID) such as naproxen, 500 mg bid, if tolerated, will help relieve residual pain as analgesic use is reduced. NSAID overuse is not usually a problem for patients with daily or headache when a NSAID with a longer half-life is taken once or twice daily. Once the patient has substantially reduced analgesic use, a preventive medication should be introduced. Another widely used approach is to commence the preventive at the same time the analgesic reduction is started; both approaches are supported by controlled trial data. A common cause of unresponsiveness to treatment is the use of a preventive when analgesics continue to be used regularly. For some patients, discontinuing analgesics is very difficult; often the best approach is to inform the patient that some degree of pain is inevitable during this initial period. Some patients will require hospitalization for detoxification and management. Such patients have typically failed efforts at outpatient withdrawal or have a significant medical condition, such as diabetes mellitus or epilepsy, that would complicate withdrawal as an outpatient. Following admission to the hospital, medications are withdrawn completely on the first day, in the absence of a contraindication. Antiemetics and fluids are administered as required; clonidine is used for opioid withdrawal symptoms. For acute intolerable pain during the waking hours, aspirin, 1 g IV (not approved in United States), is useful. IM chlorpromazine can be helpful at night; patients must be adequately hydrated. Three to five days into the admission, as the effect of the withdrawn substance wears off, a course of IV dihydroergotamine (DHE) can be used. DHE, administered every 8 h for 5 consecutive days, a treatment that is not stopped short if headache settles, can induce a significant remission that allows a preventive treatment to be established. Serotonin 5-HT receptor antagonists, such as ondansetron or granisetron, or the neurokinin receptor antagonist aprepitant may be required with DHE to prevent significant nausea, and domperidone (not approved in the United States) orally or by suppository can be very helpful. Avoiding sedating or otherwise side effect–prone antiemetics is helpful. Alternatives include a 7- to 10-day course of IV lidocaine or IV divalproex sodium or use of the CGRP antagonist eptinezumab intravenously. Initial treatment for low CSF volume headache is bed rest. For patients with persistent pain, IV caffeine (500 mg in 500 mL of saline administered over 2 h) can be very effective. An electrocardiogram (ECG) to screen for arrhythmia should be performed before administration. It is reasonable to administer at least two infusions of caffeine before embarking on additional tests to identify the source of the CSF leak. Because IV caffeine is safe and can be curative, it spares many patients the need for further investigations. If unsuccessful, an abdominal binder may be helpful. If a leak can be identified, an autologous blood patch is usually curative. A blood patch is also effective for post-LP headache; in this setting, the location is empirically determined to be the site of the LP. In patients with intractable headache, oral theophylline is a useful alternative that can take some months to be effective. Initial treatment is with acetazolamide (250–500 mg bid); the headache may improve within weeks. A plan for weight loss should also be instituted when required. If ineffective, topiramate is the next treatment of choice; it has many actions that may be useful in this setting, including carbonic anhydrase inhibition, weight loss, and neuronal membrane stabilization, likely mediated via effects on phosphorylation pathways. Severely disabled patients who do not respond to medical treatment require intracranial pressure monitoring and may require shunting. After treatment has been initiated, follow-up care is essential to identify whether progress has been made against the headache complaint. Not all headaches will respond to treatment, but, in general, worrisome headaches will progress and will be easier to identify. When a primary care physician feels the diagnosis is a primary headache disorder, it is worth noting that >90% of patients who present to primary care with a complaint of headache will have migraine. In general, patients who do not have a clear diagnosis, have a primary headache disorder other than migraine or tension-type headache, or are unresponsive to two or more standard therapies for the considered headache type should be referred to a specialist. In a practical sense, the threshold for referral is also determined by the experience of the primary care physician in headache medicine and the availability of secondary care options. The psychological state of the patient should also be evaluated because a relationship exists between head pain, depression, and anxiety. This is intended to identify comorbidity rather than provide an explanation for the headache, because troublesome headache is seldom simply caused by mood change. Although it is notable that some medicines with antidepressant actions are also effective in the preventive treatment of both tension-type headache and migraine, each symptom must be treated optimally. Underlying recurrent headache disorders may be activated by pain that follows otologic or endodontic surgical procedures. Thus, pain about the head as the result of diseased tissue or trauma may reawaken an otherwise quiescent migraine syndrome. Treatment of the headache is largely ineffective until the cause of the primary problem is addressed.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
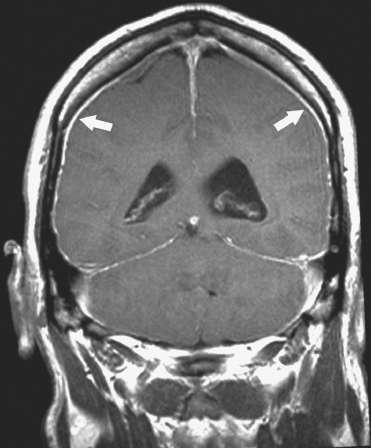
Caption: FIGURE 17-1 Magnetic resonance image showing diffuse meningeal enhancement after gadolinium administration in a patient with low cerebrospinal fluid (CSF) volume headache. — Figure 17-1: Magnetic resonance image showing diffuse meningeal enhancement after gadolinium administration in a patient with low cerebrospinal fluid (CSF) volume headache.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.