Gastrointestinal Bleeding¶
Chapter 51 | Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Gastrointestinal bleeding (GIB) is the most common gastrointestinal condition leading to hospitalization in the United States, accounting for ~530,000 admissions annually.
- The case fatality rate for GIB is approximately 2%; patients generally die from decompensation of underlying illnesses rather than exsanguination.
- Transfusion is recommended when hemoglobin drops below 7 g/dL in acute UGIB, based on a large randomized trial showing this restrictive strategy decreases rebleeding and death compared to a threshold of 9 g/dL.
- Hemoglobin may be normal or only minimally decreased at initial presentation of severe bleeding due to proportionate reductions in plasma and red cell volumes; hemoglobin falls as extravascular fluid enters the vascular space, a process that may take up to 72 h.
- Glasgow-Blatchford score of 0–1 identifies patients with very low risk of requiring transfusion, hemostatic intervention, or death (~1% of such patients).
- High-dose proton pump inhibitor (PPI) given after endoscopic therapy decreases further bleeding and mortality in patients with high-risk ulcers (active bleeding, nonbleeding visible vessel, adherent clot).
- Cirrhotic patients presenting with UGIB should be given an antibiotic (e.g., ceftriaxone) and IV vasoactive medication (e.g., octreotide) upon presentation.
- Patients with bleeding ulcers unrelated to H. pylori or NSAIDs should remain on PPI therapy indefinitely given a 42% incidence of rebleeding at 7 years without protective therapy.
- Patients taking aspirin for secondary prevention should not discontinue aspirin and, if aspirin is held, should restart aspirin once hemostasis is confirmed.
- Thalidomide is supported by evidence for use in small-intestinal vascular ectasias, with a multicenter double-blind randomized trial showing marked reductions in bleeding episodes, transfusions, and hospitalizations.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Epidemiology
- 1.2 Classification by Site
- 2. EPIDEMIOLOGY
- 2.1 Hospitalization Statistics
- 2.2 Mortality
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Upper Gastrointestinal Sources
- 3.2 Lower Gastrointestinal Sources
- 3.3 Small-Intestinal Sources
- 3.4 Portal Hypertension Effects
- 3.5 Other Causes
- 4. CLINICAL FEATURES
- 4.1 Symptoms
- 4.2 Signs
- 4.3 Anemia
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 UGIB vs LGIB Differentiation
- 5.2 Mimics
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Initial Risk Assessment
- 6.2 Endoscopy Timing
- 6.3 Angiography and CT
- 7. MANAGEMENT & TREATMENT
- 7.1 UGIB Management
- 7.2 LGIB Management
- 7.3 Small-Intestinal Management
- 7.4 Cirrhotic Patients
- 7.5 Drug Dosing
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Rebleeding Rates
- 8.2 Mortality
- 9. SPECIAL CONSIDERATIONS
- 9.1 Aspirin Management
- 9.2 NSAID Management
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Transfusion Threshold
- 10.2 Nasogastric Aspirate
- Flowcharts & Algorithms
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Suggested algorithm for patients with acute upper gastrointestinal (80 mg) followed by... |
| 2 | 🔀 Flowchart | Suggested algorithm for patients with acute lower gastrointestinal (GI) blood on toilet... |
1. DEFINITION & OVERVIEW¶
Gastrointestinal bleeding (GIB) presents as either overt or occult bleeding. Overt GIB is manifested by hematemesis, vomitus of red blood or 'coffee-grounds' material; melena, black, tarry stool; and/or hematochezia, passage of red or maroon blood from the rectum. In the absence of overt bleeding, occult GIB may present with symptoms of blood loss or anemia such as lightheadedness, syncope, angina, or dyspnea; with iron-deficiency anemia; or a positive fecal occult blood test on colorectal cancer screening. GIB is categorized by the site of bleeding as upper, from the esophagus, stomach, or duodenum; lower, from the colon; small intestinal; or obscure GIB if the source is unclear.
1.1 Epidemiology¶
GIB is the most common gastrointestinal condition leading to hospitalization in the United States, accounting for ~530,000 admissions annually and a case fatality of ~2%. Patients generally die from decompensation of other underlying illnesses rather than exsanguination.
1.2 Classification by Site¶
GIB is categorized by the site of bleeding as upper, from the esophagus, stomach, or duodenum; lower, from the colon; small intestinal; or obscure GIB if the source is unclear.
2. EPIDEMIOLOGY¶
GIB is the most common gastrointestinal condition leading to hospitalization in the United States, accounting for ~530,000 admissions annually and a case fatality of ~2%. Patients generally die from decompensation of other underlying illnesses rather than exsanguination.
2.1 Hospitalization Statistics¶
GIB accounts for ~530,000 admissions annually in the United States.
2.2 Mortality¶
The case fatality rate is approximately 2%. Patients generally die from decompensation of other underlying illnesses rather than exsanguination.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
GIB sources are classified into Upper Gastrointestinal Sources, Lower Gastrointestinal Sources, Small-Intestinal Sources, and Portal Hypertension effects.
3.1 Upper Gastrointestinal Sources¶
Peptic ulcers are the most common cause of upper GIB (UGIB), accounting for ~50% of UGIB hospitalizations. Approximately 20% of patients with bleeding ulcers have the highest-risk findings of active bleeding or a nonbleeding visible vessel; one-third of such patients have further bleeding that requires urgent surgery if they are treated conservatively. Features of an ulcer at endoscopy provide important prognostic information that guides subsequent management decisions. Mallory-Weiss tears account for ~2–10% of UGIB hospitalizations. Esophageal varices account for ~2–40% of UGIB hospitalizations, depending on the population. Erosions are endoscopically visualized breaks that are confined to the mucosa and do not cause major bleeding because arteries and veins are not present in the mucosa. Erosions in the esophagus, stomach, or duodenum commonly cause mild UGIB, accounting for up to perhaps ~30% of UGIB hospitalizations.
Table 1 — Table: Upper GI Bleeding Sources and Management¶
| Condition | Endoscopic Features | Endoscopic Therapy | Medical Therapy | Diet | Hospital Stay |
|---|---|---|---|---|---|
| Peptic Ulcer | Active bleeding or pigmented spot | Endoscopic therapy | High-dose PPI therapy | Clear liquids for ~2 days | Hospitalize ~3 days |
| Peptic Ulcer | Flat pigmented spot | No endoscopic therapy | Once-daily PPI therapy | Regular diet | Discharge after endoscopy |
| Mallory-Weiss Tear | Active bleeding | Endoscopic therapy | Once-daily PPI therapy | Clear liquids for ~1 day | Discharge after endoscopy |
| Esophageal Varices | Active bleeding | Endoscopic ligation | High-dose octreotide + antibiotic if ongoing nausea | Clear liquids for ~2 days | Hospitalize ~3–5 days |
| Erosions | No active bleeding | Endoscopic therapy | Once-daily PPI therapy | Clear liquids for ~1 day | Discharge after endoscopy |
3.2 Lower Gastrointestinal Sources¶
Hemorrhoids are probably the most common cause of lower GIB (LGIB); anal fissures also cause minor bleeding and pain. If these local anal processes, which rarely require hospitalization, are excluded, the most common cause of LGIB in adults is diverticulosis. Other causes include vascular ectasias (especially in the proximal colon of patients >70 years), neoplasms (primarily adenocarcinoma), colitis (ischemic, infectious, Crohn's or ulcerative colitis, NSAID-induced colitis or ulcers), postpolypectomy bleeding, and radiation proctopathy. Rarer causes include solitary rectal ulcer syndrome, varices (most commonly rectal), lymphoid nodular hyperplasia, vasculitis, trauma, and aortocolic fistulas. In children and adolescents, the most common colonic causes of significant GIB are inflammatory bowel disease and juvenile polyps. Diverticular bleeding is abrupt in onset, usually painless, sometimes massive, and often from the right colon; chronic or occult bleeding is not characteristic. Case series from the United States and Europe suggest colonic diverticula stop bleeding spontaneously in ≥90% of patients, with rebleeding on long-term follow-up as low as ~15% over 4–5 years. Rebleeding is substantially higher in reports from Asia. Bleeding from colonic vascular ectasias may be overt or occult; it tends to be chronic and only occasionally hemodynamically significant. Endoscopic hemostatic therapy may be used in the treatment of vascular ectasias, as well as discrete bleeding ulcers and postpolypectomy bleeding. Transcatheter arterial embolization also may be attempted for persistent bleeding from vascular ectasias and other lesions, although rebleeding is higher in nondiverticular LGIB at ~45%. Surgical therapy is generally required for major persistent or recurrent bleeding from colonic sources that cannot be treated medically, endoscopically, or angiographically.
3.3 Small-Intestinal Sources¶
Patients without a source of GIB identified on upper endoscopy and colonoscopy were previously labeled as having obscure GIB. With the advent of improved diagnostic modalities, ~75% of GIB previously labeled obscure is estimated to originate in the small intestine beyond the extent of a standard upper endoscopic exam. Small-intestinal GIB may account for ~5% of GIB cases. The most common causes in adults include vascular ectasias, neoplasm (e.g., gastrointestinal stromal tumor, carcinoid, adenocarcinoma, lymphoma, metastases), and NSAID-induced erosions and ulcers. Meckel's diverticulum is the most common cause of significant small-intestinal GIB in children, decreasing in frequency as a cause of bleeding with age. Other less common causes of small-intestinal GIB include Crohn's disease, infection, ischemia, vasculitis, small-bowel varices, diverticula, intussusception, Dieulafoy's lesions, aortoenteric fistulas, and duplication cysts. Small-intestinal vascular ectasias are treated initially with endoscopic therapy, based on observational studies suggesting short-term efficacy. However, rebleeding is common, with pooled rebleeding rates of ~45% over a mean follow-up of ~2 years in systematic reviews, leading guidelines to suggest medical therapy if further bleeding occurs after endoscopic therapy. The best available evidence supports use of thalidomide, with a multicenter double-blind randomized trial showing marked reductions in bleeding episodes, transfusions, and hospitalizations. Monthly intramuscular injection of octreotide long-acting release also is suggested based on observational studies and a small open-label randomized trial.
3.4 Portal Hypertension Effects¶
Portal hypertension is also responsible for bleeding from gastric varices, varices in the small and large intestine, and portal hypertensive gastropathy and enterocolopathy. Bleeding gastric varices are treated with endoscopic injection of tissue adhesive (e.g., n-butyl cyanoacrylate), TIPS, or retrograde transvenous obliteration.
3.5 Other Causes¶
Less common causes of UGIB include neoplasms, Dieulafoy's lesion (in which an aberrant vessel in the mucosa bleeds from a pinpoint mucosal defect), prolapse gastropathy (prolapse of proximal stomach into esophagus with retching), aortoenteric fistulas, and hemobilia or hemosuccus pancreaticus (bleeding from the bile duct or pancreatic duct). Patients with Heyde's syndrome (bleeding vascular ectasias and aortic stenosis) appear to benefit from aortic valve replacement.
4. CLINICAL FEATURES¶
GIB presents as either overt or occult bleeding. Overt GIB is manifested by hematemesis, vomitus of red blood or 'coffee-grounds' material; melena, black, tarry stool; and/or hematochezia, passage of red or maroon blood from the rectum. In the absence of overt bleeding, occult GIB may present with symptoms of blood loss or anemia such as lightheadedness, syncope, angina, or dyspnea; with iron-deficiency anemia; or a positive fecal occult blood test on colorectal cancer screening.
4.1 Symptoms¶
Hematemesis indicates an UGIB source. Melena indicates blood has been present in the gastrointestinal (GI) tract for ≥14 h and as long as 3–5 days. The more proximal the bleeding site, the more likely melena will occur. Hematochezia usually represents a lower GI source of bleeding, although an upper GI lesion may bleed so briskly that blood transits the bowel before melena develops. When hematochezia is the presenting symptom of UGIB, it is associated with hemodynamic instability and dropping hemoglobin. Bleeding lesions of the small bowel may present as melena or hematochezia.
4.2 Signs¶
Measurement of the heart rate and blood pressure is the best way to initially assess a patient with GIB. Clinically significant bleeding now leads to postural changes in heart rate or blood pressure, tachycardia, and, finally, recumbent hypotension. In contrast, hemoglobin does not fall immediately with acute GIB, due to proportionate reductions in plasma and red cell volumes ('people bleed whole blood'). Thus, hemoglobin may be normal or only minimally decreased at initial presentation of a severe bleeding episode. As extravascular fluid enters the vascular space to restore volume, the hemoglobin falls, but this process may take up to 72 h. Other clues to UGIB include hyperactive bowel sounds and elevated blood urea nitrogen (due to volume depletion and blood proteins absorbed in the small intestine). A nonbloody nasogastric aspirate may be seen in ~15% of patients with UGIB who present with clinically serious hematochezia. A bile-stained appearance does not exclude UGIB because reports of bile in the aspirate are incorrect in ~50% of cases. Testing of aspirates that are not grossly bloody for occult blood is not useful.
4.3 Anemia¶
With the development of iron-deficiency anemia, the mean corpuscular volume is low and red-blood-cell distribution width is increased. Patients with slow, chronic GIB may have very low hemoglobin values despite normal blood pressure and heart rate.
5. DIFFERENTIAL DIAGNOSIS¶
Differentiation of UGIB from LGIB is based on the presence of hematemesis (UGIB) vs hematochezia (usually LGIB). Melena indicates blood has been present in the GI tract for ≥14 h and as long as 3–5 days. The more proximal the bleeding site, the more likely melena will occur. Hematochezia usually represents a lower GI source of bleeding, although an upper GI lesion may bleed so briskly that blood transits the bowel before melena develops. When hematochezia is the presenting symptom of UGIB, it is associated with hemodynamic instability and dropping hemoglobin. Bleeding lesions of the small bowel may present as melena or hematochezia.
5.1 UGIB vs LGIB Differentiation¶
Hematemesis indicates an UGIB source. Melena indicates blood has been present in the gastrointestinal (GI) tract for ≥14 h and as long as 3–5 days. The more proximal the bleeding site, the more likely melena will occur. Hematochezia usually represents a lower GI source of bleeding, although an upper GI lesion may bleed so briskly that blood transits the bowel before melena develops. When hematochezia is the presenting symptom of UGIB, it is associated with hemodynamic instability and dropping hemoglobin. Bleeding lesions of the small bowel may present as melena or hematochezia.
5.2 Mimics¶
A nonbloody nasogastric aspirate may be seen in ~15% of patients with UGIB who present with clinically serious hematochezia. A bile-stained appearance does not exclude UGIB because reports of bile in the aspirate are incorrect in ~50% of cases. Testing of aspirates that are not grossly bloody for occult blood is not useful.
6. INVESTIGATIONS & DIAGNOSIS¶
Initial Risk Assessment Baseline characteristics predictive of rebleeding and death include hemodynamic compromise (tachycardia or hypotension), increasing age, and comorbidities. Risk assessment tools may be used to identify patients with very low risk. Discharge from the emergency room with outpatient management is suggested for patients with a Glasgow-Blatchford score (possible range 0–23) of 0–1 because only ~1% of patients who require transfusion, require hemostatic intervention, or die have a score of 0–1.
6.1 Initial Risk Assessment¶
Initial Risk Assessment Baseline characteristics predictive of rebleeding and death include hemodynamic compromise (tachycardia or hypotension), increasing age, and comorbidities. Risk assessment tools may be used to identify patients with very low risk. Discharge from the emergency room with outpatient management is suggested for patients with a Glasgow-Blatchford score (possible range 0–23) of 0–1 because only ~1% of patients who require transfusion, require hemostatic intervention, or die have a score of 0–1.
Table 2 — Table 51-1 Glasgow-Blatchford Score¶
| Risk Factors at Admission | Score |
|---|---|
| Blood urea nitrogen (mg/dL) 18.2 to <22.4 | 2 |
| Blood urea nitrogen (mg/dL) 22.4 to <28.0 | 3 |
| Blood urea nitrogen (mg/dL) 28.0 to <70.0 | 4 |
| Blood urea nitrogen (mg/dL) ≥70.0 | 6 |
| Hemoglobin (g/dL) 12.0 to <13.0 (men); 10.0 to <12.0 (women) | 1 |
| Hemoglobin (g/dL) 10.0 to <12.0 (men) | 3 |
| Hemoglobin (g/dL) <10.0 | 6 |
| Systolic blood pressure (mmHg) 100–109 | 1 |
| Systolic blood pressure (mmHg) 90–99 | 2 |
| Systolic blood pressure (mmHg) <90 | 3 |
| Melena | 1 |
| Syncope | 2 |
| Hepatic disease | 2 |
| Cardiac failure | 2 |
6.2 Endoscopy Timing¶
Pre-Endoscopic Medications PPI infusion may be considered at presentation; it modestly decreases need for endoscopic therapy due to a reduction in high-risk ulcer stigmata (e.g., active bleeding) but does not improve clinical outcomes such as further bleeding or death. The promotility agent erythromycin, 250 mg intravenously ~30–90 min before endoscopy, is suggested to improve visualization features predicting low or high risk of further bleeding and death. Even in high-risk patients, more urgent endoscopy (performed within 6–12 h of gastroenterology consultation) does not improve clinical outcomes, and some observational studies suggest increased mortality with endoscopy within 6–12 h in high-risk patients. Early endoscopy in low-risk patients (e.g., hemodynamically stable without severe comorbidities) identifies low-risk findings (e.g., clean-based ulcers, erosions, nonbleeding Mallory-Weiss tears) that allow discharge in ≥40% of patients, thereby reducing hospital stay.
6.3 Angiography and CT¶
For patients with extrinsic extravasation, angiography is indicated. CT angiography is used for workup for small intestinal/obscure bleeding site. Surgery is indicated if bleeding persists or site has not been identified.
7. MANAGEMENT & TREATMENT¶
Treatment of underlying metabolic, social, psychiatric, dental, infectious, or other systemic disorders may be sufficient to restore weight and functional status gradually. Medications that cause nausea or anorexia should be withdrawn or changed, if possible. For those with unexplained UWL, oral nutritional supplements such as high-energy drinks sometimes reverse weight loss. Advising patients to choose appealing foods and to consume supplements between meals rather than with a meal may help minimize appetite suppression and facilitate increased overall intake. Orexigenic, anabolic, and anticytokine agents are not generally recommended. In selected patients, the antidepressant mirtazapine significantly increases body weight, body fat mass, and leptin concentration. However, side effects, including dizziness, fatigue, and somnolence, occur in about 10% of patients. Patients with wasting conditions who can comply with an appropriate exercise program gain muscle protein mass, strength, and endurance and may be more capable of performing ADLs.
7.1 UGIB Management¶
Peptic ulcers are treated conservatively. These patients benefit from endoscopic therapy such as bipolar electrocoagulation, heater probe, injection therapy (e.g., absolute alcohol, 1:10,000 epinephrine), clips, and/or topical hemostatic powder with reductions in bleeding, hospital stay, mortality, and costs. In contrast, patients with clean-based ulcers have rates of serious rebleeding approaching zero. If stable with no other reason for hospitalization, such patients may be discharged home after endoscopy. Endoscopic therapy is indicated for actively bleeding Mallory-Weiss tears. Patients with variceal hemorrhage have poorer outcomes than patients with other sources of UGIB. Esophageal varices are treated with endoscopic ligation and an IV vasoactive medication (octreotide, somatostatin, vapreotide, terlipressin) for 2–5 days. Combination of endoscopic and medical therapy is superior to either therapy alone in decreasing rebleeding. Over the long term, treatment with nonselective beta blockers plus endoscopic ligation is recommended because the combination is more effective than either alone in reduction of recurrent esophageal variceal bleeding. Transjugular intrahepatic portosystemic shunt (TIPS) is recommended in patients who have persistent or recurrent bleeding despite endoscopic and medical therapy. TIPS also is suggested for acute variceal bleeding in patients with advanced liver disease (Child-Pugh class B with score 8–9 and active bleeding at endoscopy, Child-Pugh class C with score 10–13), because randomized trials show significant decreases in rebleeding and mortality compared with standard endoscopic and medical therapy. High-dose, proton pump inhibitor (PPI), given to reduce intragastric acid and thereby enhance clot stability, decreases further bleeding and mortality in patients with high-risk ulcers (active bleeding, nonbleeding visible vessel, adherent clot) when given after endoscopic therapy. Meta-analysis of randomized trials indicates that outcomes are comparable with high-dose PPIs given as a constant infusion or intermittently. Patients with lower-risk findings (flat pigmented spot, clean base) do not require endoscopic therapy and receive standard doses of oral PPI. Approximately 10–50% of patients with bleeding ulcers rebleed within the next year if no preventive strategies are employed. Prevention of recurrent bleeding focuses on the three main factors in ulcer pathogenesis, Helicobacter pylori, nonsteroidal anti-inflammatory drugs (NSAIDs), and acid. Eradication of H. pylori in patients with or bleeding ulcers decreases rebleeding rates to <5%. If a bleeding ulcer develops in a patient taking NSAIDs, the NSAIDs should be discontinued. If NSAIDs must be given, a cyclooxygenase-2 selective NSAID plus a PPI is recommended, based on results of a randomized trial. Patients with established cardiovascular disease who develop bleeding ulcers while taking low-dose aspirin for secondary prevention should not discontinue aspirin and, if aspirin is held, should restart aspirin once hemostasis is confirmed. A randomized trial showed that immediate reinstitution of aspirin was associated with a lower 8-week mortality compared to not restarting aspirin (1% vs 13%; hazard ratio, 0.2; 95% CI, 0.1–0.6). In contrast, aspirin should be discontinued in patients taking aspirin for primary prevention of cardiovascular events who develop UGIB. Patients with bleeding ulcers unrelated to H. pylori or NSAIDs should remain on PPI therapy indefinitely given a 42% incidence of rebleeding at 7 years without protective therapy.
Table 3 — Table: UGIB Management by Endoscopic Findings¶
| Condition | Endoscopic Features | Endoscopic Therapy | Medical Therapy | Diet | Hospital Stay |
|---|---|---|---|---|---|
| Peptic Ulcer | Active bleeding or pigmented spot | Endoscopic therapy | High-dose PPI therapy | Clear liquids for ~2 days | Hospitalize ~3 days |
| Peptic Ulcer | Flat pigmented spot | No endoscopic therapy | Once-daily PPI therapy | Regular diet | Discharge after endoscopy |
| Mallory-Weiss Tear | Active bleeding | Endoscopic therapy | Once-daily PPI therapy | Clear liquids for ~1 day | Discharge after endoscopy |
| Esophageal Varices | Active bleeding | Endoscopic ligation | High-dose octreotide + antibiotic if ongoing nausea | Clear liquids for ~2 days | Hospitalize ~3–5 days |
| Erosions | No active bleeding | Endoscopic therapy | Once-daily PPI therapy | Clear liquids for ~1 day | Discharge after endoscopy |
7.2 LGIB Management¶
Diverticular bleeding is abrupt in onset, usually painless, sometimes massive, and often from the right colon; chronic or occult bleeding is not characteristic. Case series from the United States and Europe suggest colonic diverticula stop bleeding spontaneously in ≥90% of patients, with rebleeding on long-term follow-up as low as ~15% over 4–5 years. Rebleeding is substantially higher in reports from Asia. Case series suggest endoscopic therapy may decrease recurrent bleeding in the uncommon case when colonoscopy identifies the specific bleeding diverticulum. When diverticular bleeding is found at angiography, transcatheter arterial embolization by superselective technique prevents further bleeding in most patients. Segmental surgical resection is recommended for refractory diverticular bleeding. Bleeding from colonic vascular ectasias may be overt or occult; it tends to be chronic and only occasionally hemodynamically significant. Endoscopic hemostatic therapy may be used in the treatment of vascular ectasias, as well as discrete bleeding ulcers and postpolypectomy bleeding. Transcatheter arterial embolization also may be attempted for persistent bleeding from vascular ectasias and other lesions, although rebleeding is higher in nondiverticular LGIB at ~45%. Surgical therapy is generally required for major persistent or recurrent bleeding from colonic sources that cannot be treated medically, endoscopically, or angiographically.
7.3 Small-Intestinal Management¶
Small-intestinal vascular ectasias are treated initially with endoscopic therapy, based on observational studies suggesting short-term efficacy. However, rebleeding is common, with pooled rebleeding rates of ~45% over a mean follow-up of ~2 years in systematic reviews, leading guidelines to suggest medical therapy if further bleeding occurs after endoscopic therapy. The best available evidence supports use of thalidomide, with a multicenter double-blind randomized trial showing marked reductions in bleeding episodes, transfusions, and hospitalizations. Monthly intramuscular injection of octreotide long-acting release also is suggested based on observational studies and a small open-label randomized trial. Other isolated lesions, such as tumors, generally require surgical resection.
7.4 Cirrhotic Patients¶
Cirrhotic patients presenting with UGIB should be given an antibiotic (e.g., ceftriaxone) and IV vasoactive medication (e.g., octreotide) upon presentation. Antibiotics decrease bacterial infections, rebleeding, and mortality, and vasoactive medications improve control of bleeding in the 12 h after presentation.
7.5 Drug Dosing¶
PPI infusion may be considered at presentation; it modestly decreases need for endoscopic therapy due to a reduction in high-risk ulcer stigmata (e.g., active bleeding) but does not improve clinical outcomes such as further bleeding or death. The promotility agent erythromycin, 250 mg intravenously ~30–90 min before endoscopy, is suggested to improve visualization features predicting low or high risk of further bleeding and death. High-dose, proton pump inhibitor (PPI), given to reduce intragastric acid and thereby enhance clot stability, decreases further bleeding and mortality in patients with high-risk ulcers (active bleeding, nonbleeding visible vessel, adherent clot) when given after endoscopic therapy. Meta-analysis of randomized trials indicates that outcomes are comparable with high-dose PPIs given as a constant infusion or intermittently. In contrast, aspirin should be discontinued in patients taking aspirin for primary prevention of cardiovascular events who develop UGIB. Patients with established cardiovascular disease who develop bleeding ulcers while taking low-dose aspirin for secondary prevention should not discontinue aspirin and, if aspirin is held, should restart aspirin once hemostasis is confirmed. A randomized trial showed that immediate reinstitution of aspirin was associated with a lower 8-week mortality compared to not restarting aspirin (1% vs 13%; hazard ratio, 0.2; 95% CI, 0.1–0.6). In contrast, aspirin should be discontinued in patients taking aspirin for primary prevention of cardiovascular events who develop UGIB. Patients with bleeding ulcers unrelated to H. pylori or NSAIDs should remain on PPI therapy indefinitely given a 42% incidence of rebleeding at 7 years without protective therapy.
8. PROGNOSIS & COMPLICATIONS¶
Approximately 10–50% of patients with bleeding ulcers rebleed within the next year if no preventive strategies are employed. Prevention of recurrent bleeding focuses on the three main factors in ulcer pathogenesis, Helicobacter pylori, nonsteroidal anti-inflammatory drugs (NSAIDs), and acid. Eradication of H. pylori in patients with or bleeding ulcers decreases rebleeding rates to <5%. If a bleeding ulcer develops in a patient taking NSAIDs, the NSAIDs should be discontinued. If NSAIDs must be given, a cyclooxygenase-2 selective NSAID plus a PPI is recommended, based on results of a randomized trial. Patients with established cardiovascular disease who develop bleeding ulcers while taking low-dose aspirin for secondary prevention should not discontinue aspirin and, if aspirin is held, should restart aspirin once hemostasis is confirmed. A randomized trial showed that immediate reinstitution of aspirin was associated with a lower 8-week mortality compared to not restarting aspirin (1% vs 13%; hazard ratio, 0.2; 95% CI, 0.1–0.6). In contrast, aspirin should be discontinued in patients taking aspirin for primary prevention of cardiovascular events who develop UGIB. Patients with bleeding ulcers unrelated to H. pylori or NSAIDs should remain on PPI therapy indefinitely given a 42% incidence of rebleeding at 7 years without protective therapy.
8.1 Rebleeding Rates¶
Approximately 10–50% of patients with bleeding ulcers rebleed within the next year if no preventive strategies are employed. Prevention of recurrent bleeding focuses on the three main factors in ulcer pathogenesis, Helicobacter pylori, nonsteroidal anti-inflammatory drugs (NSAIDs), and acid. Eradication of H. pylori in patients with or bleeding ulcers decreases rebleeding rates to <5%.
8.2 Mortality¶
The case fatality rate for GIB is approximately 2%. Patients generally die from decompensation of other underlying illnesses rather than exsanguination.
9. SPECIAL CONSIDERATIONS¶
Patients with established cardiovascular disease who develop bleeding ulcers while taking low-dose aspirin for secondary prevention should not discontinue aspirin and, if aspirin is held, should restart aspirin once hemostasis is confirmed. A randomized trial showed that immediate reinstitution of aspirin was associated with a lower 8-week mortality compared to not restarting aspirin (1% vs 13%; hazard ratio, 0.2; 95% CI, 0.1–0.6). In contrast, aspirin should be discontinued in patients taking aspirin for primary prevention of cardiovascular events who develop UGIB. Patients with bleeding ulcers unrelated to H. pylori or NSAIDs should remain on PPI therapy indefinitely given a 42% incidence of rebleeding at 7 years without protective therapy.
9.1 Aspirin Management¶
Patients with established cardiovascular disease who develop bleeding ulcers while taking low-dose aspirin for secondary prevention should not discontinue aspirin and, if aspirin is held, should restart aspirin once hemostasis is confirmed. A randomized trial showed that immediate reinstitution of aspirin was associated with a lower 8-week mortality compared to not restarting aspirin (1% vs 13%; hazard ratio, 0.2; 95% CI, 0.1–0.6). In contrast, aspirin should be discontinued in patients taking aspirin for primary prevention of cardiovascular events who develop UGIB.
9.2 NSAID Management¶
If a bleeding ulcer develops in a patient taking NSAIDs, the NSAIDs should be discontinued. If NSAIDs must be given, a cyclooxygenase-2 selective NSAID plus a PPI is recommended, based on results of a randomized trial.
10. KEY PEARLS & CLINICAL TRAPS¶
Hemoglobin may be normal or only minimally decreased at initial presentation of a severe bleeding episode. As extravascular fluid enters the vascular space to restore volume, the hemoglobin falls, but this process may take up to 72 h. Transfusion is recommended when the hemoglobin drops below 7 g/dL, based on a large randomized trial showing this restrictive transfusion strategy decreases rebleeding and death in acute UGIB compared with a transfusion threshold of 9 g/dL. Patients with slow, chronic GIB may have very low hemoglobin values despite normal blood pressure and heart rate. A nonbloody nasogastric aspirate may be seen in ~15% of patients with UGIB who present with clinically serious hematochezia. A bile-stained appearance does not exclude UGIB because reports of bile in the aspirate are incorrect in ~50% of cases. Testing of aspirates that are not grossly bloody for occult blood is not useful.
10.1 Transfusion Threshold¶
Transfusion is recommended when the hemoglobin drops below 7 g/dL, based on a large randomized trial showing this restrictive transfusion strategy decreases rebleeding and death in acute UGIB compared with a transfusion threshold of 9 g/dL.
10.2 Nasogastric Aspirate¶
A nonbloody nasogastric aspirate may be seen in ~15% of patients with UGIB who present with clinically serious hematochezia. A bile-stained appearance does not exclude UGIB because reports of bile in the aspirate are incorrect in ~50% of cases. Testing of aspirates that are not grossly bloody for occult blood is not useful.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
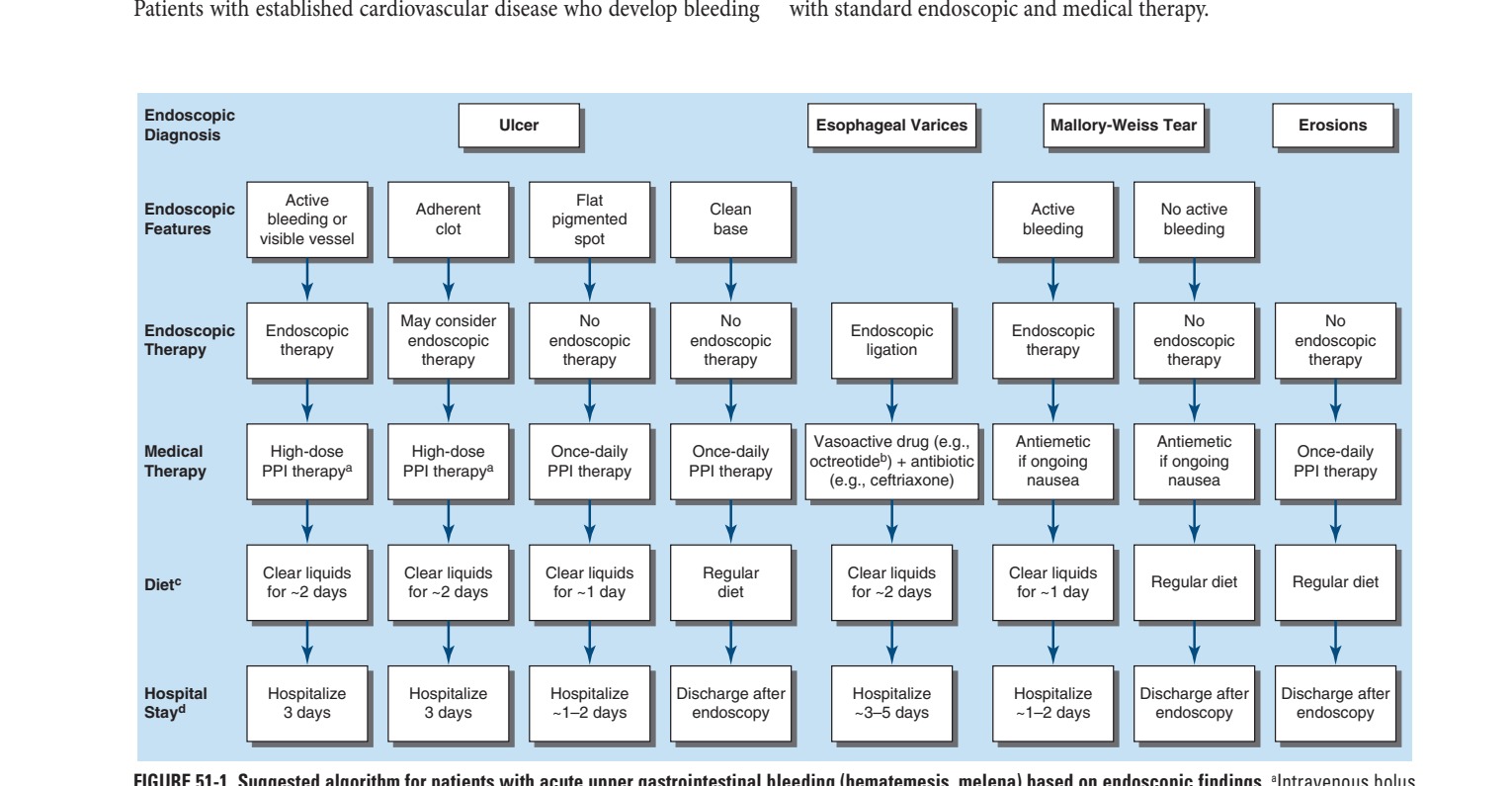
Caption: FIGURE 51-1 Suggested algorithm for patients with acute upper gastrointestinal (80 mg) followed by infusion (8 mg/h) or by intermittent oral or intravenous doses (e.g., infusion for 2–5 days. cDiet after endoscopy, assuming no nausea or vomiting. dDuration medical conditions requiring hospitalization. PPI, proton pump inhibitor.
Flowchart 2¶

Caption: FIGURE 51-2 Suggested algorithm for patients with acute lower gastrointestinal (GI) blood on toilet paper), normal blood pressure and heart rate, normal hemoglobin and sigmoidoscopy is adequate.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.