Meningococcal Infections¶
Chapter 160 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Infection with Neisseria meningitidis most commonly manifests as asymptomatic colonization in the nasopharynx of healthy adolescents and adults.
- Invasive disease occurs rarely, usually presenting as either bacterial meningitis or meningococcal septicemia.
- Patients may also present with occult bacteremia, pneumonia, septic arthritis, conjunctivitis, and chronic meningococcemia.
- In total, 12 capsular groups have been identified (A–C, X–Z, E, W, H–J, and L), but just six of these—A, B, C, X, Y, and W—account for the majority of cases of invasive disease.
- Complement deficiency, chiefly of the terminal complement components (C5–9), properdin, or factor D, increases the risk of disease by up to 600-fold.
- Empirical antibiotic therapy for suspected meningococcal disease consists of a third-generation cephalosporin such as ceftriaxone (75–100 mg/kg per d) or cefotaxime (200 mg/kg per day).
- Mortality rates among children with meningococcal septicemia have been high (25–40%), but early aggressive management may reduce the figure to <10%.
- Purpura fulminans occurs in severe cases and is characterized by multiple large purpuric lesions and signs of peripheral ischemia.
- Chronic meningococcemia presents as repeated episodes of petechial rash associated with fever, joint pain, and arthritis.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 2. EPIDEMIOLOGY
- 2.1 Age Distribution
- 2.2 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Capsular Groups
- 3.2 Pathogenesis
- 4. CLINICAL FEATURES
- 4.1 Septicemia
- 4.2 Meningitis
- 4.3 Chronic Meningococcemia
- 4.4 Postmeningococcal Reactive Disease
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 7. MANAGEMENT & TREATMENT
- 7.1 Antibiotic Therapy
- 7.2 Supportive Care
- 7.3 Adjunctive Therapy
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Global percentage distribution of meningococcal capsular groups groups other than B, C,... |
| 2 | 🖼 Figure | Illustration of meningococcal outer-membrane vesicle containing outer-membrane structures |
| 3 | 🖼 Figure | Age distribution of capsular groups B and ACWY meningococcal 2012–2021 |
| 4 | 🖼 Figure | Cross-section through surface structures of Neisseria (Reproduced with permission from M Sadarangani,... |
| 5 | 🖼 Figure | Electron micrograph of Neisseria meningitidis |
| 6 | 🖼 Figure | A |
| 7 | 🖼 Figure | A |
1. DEFINITION & OVERVIEW¶
- Infection with Neisseria meningitidis most commonly manifests as asymptomatic colonization in the nasopharynx of healthy adolescents and adults.
- Invasive disease occurs rarely, usually presenting as either bacterial meningitis or meningococcal septicemia.
- Patients may also present with occult bacteremia, pneumonia, septic arthritis, conjunctivitis, and chronic meningococcemia.
- N. meningitidis is a gram-negative aerobic diplococcus that colonizes humans only and causes disease after transmission to a susceptible individual.
- Several related neisserial organisms have been recognized, including the pathogen N. gonorrhoeae and the commensals N. lactamica, N. flavescens, N. mucosa, N. sicca, and N. subflava.
- N. meningitidis is a catalase- and oxidase-positive organism that utilizes glucose and maltose to produce acid.
2. EPIDEMIOLOGY¶
- Up to 500,000 cases of meningococcal disease are thought to occur worldwide each year, although the numbers have been declining recently as a result of both immunization programs and secular trends.
- About 10% of affected individuals die.
- There are several patterns of disease: epidemic, outbreak (small clusters of cases), hyperendemic, and sporadic or endemic.
- Epidemics have continued since the original descriptions of meningococcal disease, especially affecting the sub-Saharan meningitis belt of Africa, where tens to hundreds of thousands of cases (caused mainly by capsular group A but also by capsular groups C, W, and X) may be reported over a season and rates may be as high as 1000 cases per 100,000 population.
- Capsular group A epidemics took place in Europe and North America after the First and Second World Wars, and capsular group A outbreaks have been documented over the past 40 years in New Zealand, China, Nepal, Mongolia, India, Pakistan, Poland, and Russia.
- 65% of outbreaks reported in the meningitis belt between 2010 and 2017 were caused by capsular group C and 35% by capsular group W, following an immunization campaign to control capsular group A outbreaks.
- New vaccines covering A, C, W, Y, and X are becoming available globally to extend control of outbreaks.
- Clusters of cases occur where there is an opportunity for increased transmission—i.e., in closed or semi-closed communities such as schools, colleges, universities, military training centers, and refugee camps.
- Over the past 4 decades, such clusters have been especially strongly linked with a particular clone (sequence type 11) that is mainly associated with capsular group C or W but was first described in association with capsular group B.
- Most countries experience predominantly sporadic cases (0.0–2.8 cases per 100,000 population, but recently rates up to 10 cases per 100,000 have been reported in Africa), with many different disease-causing clones involved and usually no clear epidemiologic link between one case and another.
- In the United States, the rate of meningococcal disease fell from 1.2 cases per 100,000 population in 1997 to 0.06 cases per 100,000 in 2021.
- Meningococcal disease in the United States was previously dominated by capsular groups B and C; however, in 2011–2021, group B alone was predominant in children age 5 cases per 100,000 during the 1990s because of an increase in cases caused by the ST11 capsular group C clone.
- A mass immunization program against capsular group C was undertaken beginning in 1999 and resulted in a large impact against the disease, leaving capsular group B meningococci as the predominant cause of infection in the past quarter century.
- Introduction of a group B meningococcal (MenB) vaccine for infants in the United Kingdom in 2015 also led to a significant reduction in group B cases.
- A hyperinvasive ST11 clone bearing a W capsule emerged in South America and spread to various countries in Europe and in Australia with cases peaking in 2016 in the United Kingdom.
- During the same decade, increases in capsular group Y disease were noted in various countries including Europe, Canada, and South Africa.
- The principal determinant of disease susceptibility is age, with the peak incidence in the first year of life.
- The susceptibility of the very young presumably results from an absence of specific adaptive immunity in combination with very close contact with colonized individuals, including parents.
- After early childhood, a second peak of disease occurs among adolescents and young adults (15–25 years of age) in Europe and North America.
- It is thought that this peak relates to social behaviors and the environmental exposures in this age group, as discussed below.
- Most cases of infection with N. meningitidis in developed countries today are sporadic, and the rarity of the disease suggests that individual factors are important.
- Factors that increase the chance of a susceptible individual’s acquiring N. meningitidis via the respiratory route also increase the risk of meningococcal disease.
- Acquisition occurs through close contact with carriers as a result of overcrowding (e.g., in poor socioeconomic settings, in refugee camps, during the Hajj pilgrimage to Mecca, during freshman-year residence in college dormitories), recruitment into the military, and certain social behaviors (e.g., attendance at bars and nightclubs, kissing).
- Secondary cases may occur in close contacts of an index case (e.g., household members, persons kissing the infected individual); the risk to these contacts may be as high as 1000 times the background rate in the population.
- Factors that damage the nasopharyngeal epithelium also increase the risk of both colonization with N. meningitidis and invasive disease.
- The most important of these factors are tobacco smoking (odds ratio, 4.1) and passive exposure to tobacco smoke.
- In addition, recent viral respiratory tract infection, infection with Mycoplasma species, and winter or the dry season (in sub-Saharan Africa) have been associated with meningococcal disease; all of these factors presumably either increase the expression of adhesion molecules in the nasopharynx, thus enhancing meningococcal adhesion, or facilitate meningococcal invasion of the bloodstream.
2.1 Age Distribution¶
- Point-prevalence studies reveal widely divergent rates of carriage for different types of meningococci.
- Despite the high rates of carriage among adolescents and young adults, only ~10% of adults carry meningococci, and colonization is very rare in early childhood.
- Many of the same factors that increase the risk of meningococcal disease also increase the risk of carriage.
- Colonization of the nasopharynx involves a series of interactions of meningococcal adhesins (e.g., Opa proteins and pili) with their ligands on the epithelial mucosa.
- N. meningitidis produces an IgA1 protease that is likely to reduce interruption of colonization by mucosal IgA.
- Colonization should be considered the normal state of meningococcal infection, with an increased risk of invasion being the unfortunate consequence (for both host and organism) of adaptations of hyperinvasive meningococcal lineages to favor their survival.
- The capsule provides resistance to phagocytosis and may be important in preventing desiccation during transmission between hosts.
- Antigenic diversity in surface structures and an ability to vary levels of their expression probably have evolved as important factors in maintaining meningococcal populations within and between individual hosts.
- Invasion through the mucosa into the bloodstream occurs rarely, usually within a few days of acquisition of an invasive strain by a susceptible individual.
- Only occasional cases of prolonged colonization prior to invasion have been documented.
- Once the organism is in the bloodstream, its growth may be limited if the individual is partially immune, although bacteremia may allow seeding of another site, such as the meninges or the joints.
- Alternatively, unchecked proliferation may continue, resulting in high bacterial counts in the circulation.
2.2 Risk Factors¶
- The best-documented genetic association with meningococcal disease is complement deficiency, chiefly of the terminal complement components (C5–9), properdin, or factor D or those treated with complement inhibitors such as eculizumab.
- Such a deficiency increases the risk of disease by up to 600-fold and may result in recurrent attacks.
- Complement components are believed to be important for the bactericidal activity of serum, which is considered the principal mechanism of immunity against invasive meningococcal disease.
- However, when investigated, complement deficiency is found in only a very small proportion of individuals with meningococcal disease (0.3%).
- Conversely, 7–20% of persons whose disease is caused by the less common capsular groups (W, X, Y, Z, E) have a complement deficiency.
- Complement deficiency appears to be associated with capsular group B disease only rarely.
- Individuals with recurrences of meningococcal disease, particularly those caused by non-B capsular groups, should be assessed for complement deficiency by measurement of total hemolytic complement activity.
- There is also limited evidence that hyposplenism (through reduction in phagocytic capacity), hypogammaglobulinemia (through absence of specific antibody), and HIV increase the risk of meningococcal disease.
- Genetic studies have revealed various associations with disease susceptibility, including complement and mannose-binding lectin deficiency, single-nucleotide polymorphisms in Toll-like receptor (TLR) 4 and tumor necrosis factor (TNF) α, complement factor H, and variants of Fc gamma receptors.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Meningococci associated with invasive disease are usually encapsulated with polysaccharide, and the antigenic nature of the capsule determines an organism’s capsular group (serogroup).
- Beneath the capsule, meningococci are surrounded by an outer phospholipid membrane containing lipopolysaccharide (LPS, endotoxin) and multiple outer-membrane proteins.
- Serologic methods for typing meningococci are restricted by the limited availability of serologic reagents that can distinguish among the organisms’ highly variable surface proteins.
- Where available, high-throughput antigen gene sequencing has superseded serology for meningococcal typing.
- A large database of antigen gene sequences for the outer-membrane proteins PorA, PorB, FetA, Opa, NadA, neisserial heparin binding antigen (NHBA), and factor H–binding protein (fHbp) is available online.
- The number of specialized iron-regulated proteins found in the meningococcal outer membrane (e.g., FetA and transferrin-binding proteins) highlights the organisms’ dependence on iron from human sources.
- A thin peptidoglycan cell wall separates the outer membrane from the cytoplasmic membrane.
- N. meningitidis has evolved as an effective colonizer of the human nasopharynx, with asymptomatic infection rates of >25% described in some series of adolescents and young adults and among residents of crowded communities.
- Colonization of the nasopharynx involves a series of interactions of meningococcal adhesins (e.g., Opa proteins and pili) with their ligands on the epithelial mucosa.
- N. meningitidis produces an IgA1 protease that is likely to reduce interruption of colonization by mucosal IgA.
- Invasion through the mucosa into the bloodstream occurs rarely, usually within a few days of acquisition of an invasive strain by a susceptible individual.
- Once the organism is in the bloodstream, its growth may be limited if the individual is partially immune, although bacteremia may allow seeding of another site, such as the meninges or the joints.
- Alternatively, unchecked proliferation may continue, resulting in high bacterial counts in the circulation.
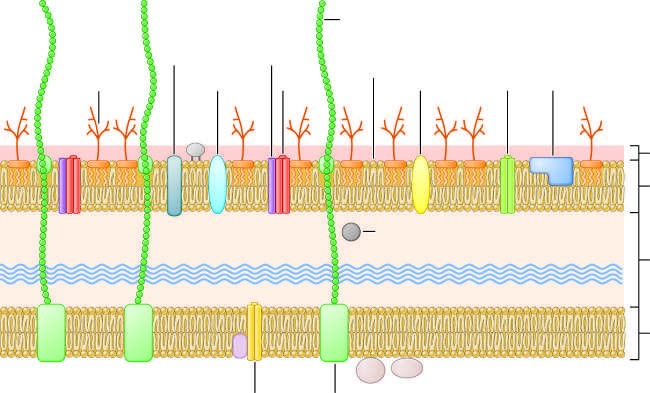
- During growth, meningococci release blebs of outer membrane containing outer-membrane proteins and LPS.
- Endotoxin binds cell-bound CD14 in association with TLR4 to initiate an inflammatory cascade with the release of high levels of various mediators, including soluble TNF receptor, interleukin (IL) 1, IL-1 receptor antagonist, IL-1β, IL-6, IL-8, IL-10, plasminogen-activator inhibitor 1 (PAI-1), and leukemia inhibitory factor.
- Soluble CD14-bound endotoxin acts as a mediator of endothelial activation.
- The severity of meningococcal disease is related both to the levels of endotoxin in the blood and to the magnitude of the inflammatory response.
- The latter is determined to some extent by polymorphisms in inflammatory response genes (and their inhibitors), and the release of the inflammatory cascade heralds the development of meningococcal septicemia (meningococcemia).
- Endothelial injury is central to many clinical features of meningococcemia, including increased vascular permeability, pathologic changes in vascular tone, loss of thromboresistance, intravascular coagulation, and myocardial dysfunction.
- Endothelial injury leads to increased vascular permeability (attributed to loss of glycosaminoglycans and endothelial proteins), with subsequent gross proteinuria.
- Leakage of fluid and electrolytes into the tissues from capillaries ("capillary leak syndrome") leads to hypovolemia, tissue edema, and pulmonary edema.
- Initial compensation results in vasoconstriction and tachycardia, although cardiac output eventually falls.
- While resuscitation fluids may restore circulating volume, tissue edema will continue to increase, and, in the lung, the consequence may be respiratory failure.
- Intravascular thrombosis (caused by activation of procoagulant pathways in association with upregulation of tissue factor on the endothelium) occurs in some patients with meningococcal disease and results in purpura fulminans and infarction of areas of skin or even whole limbs.
- Thrombolysis is also profoundly impaired in meningococcal sepsis through the release of high levels of PAI-1.
- Shock in meningococcal septicemia appears to be attributable to a combination of factors, including hypovolemia, which results from the capillary leak syndrome secondary to endothelial injury, and myocardial depression, which is driven by hypovolemia, hypoxia, metabolic derangements (e.g., hypocalcemia), and cytokines (e.g., IL-6).
- Decreased perfusion of tissues as a result of intravascular thrombosis, vasoconstriction, tissue edema, and reduced cardiac output in meningococcal septicemia can cause widespread organ dysfunction, including renal impairment and—later in the disease—a decreased level of consciousness due to central nervous system involvement.
- Local endothelial injury may result in cerebral edema and rapid onset of raised intracranial pressure in some cases.
3.1 Capsular Groups¶
- In total, 12 capsular groups have been identified (A–C, X–Z, E, W, H–J, and L), but just six of these—A, B, C, X, Y, and W (formerly W135)—account for the majority of cases of invasive disease.
- Group D is often listed as the thirteenth capsular group but has been identified as an unencapsulated variant of group C.
- Meningococci are commonly isolated from the nasopharynx in studies of carriage; the lack of capsule often is a result of phase variation of capsule expression, but as many as 16% of isolates lack the genes for capsule synthesis and assembly.
- These "capsule-null" meningococci and those that express capsules other than A, B, C, X, Y, and W are only rarely associated with invasive disease and are most commonly identified in the nasopharynx of asymptomatic carriers.
- Hyperinvasive lineages of N. meningitidis have been recognized, persist over decades, and are responsible for the majority of cases of invasive meningococcal disease worldwide.
- Hyperinvasive lineages may be associated with more than one capsular group.
- The apparent genetic stability of these meningococcal clones over decades and during wide geographic spread indicates that they are well adapted to the nasopharyngeal environment of the host and to efficient transmission.
Table 1 — Table 160-1 Structure of the Polysaccharide Capsule of Common Disease-Causing Meningococci¶
| MENINGOCOCCAL CAPSULAR GROUP | CHEMICAL STRUCTURE OF OLIGOSACCHARIDE | CURRENT DISEASE EPIDEMIOLOGY |
|---|---|---|
| A | 2-Acetamido-2-deoxy-D-mannopyranosyl phosphate | Epidemic disease mainly in sub-Saharan Africa; sporadic cases worldwide |
| B | α-2,8-N-acetylneuraminic acid | Sporadic cases worldwide; hyperendemic disease |
| C | α-2,9-O-acetylneuraminic acid | Small outbreaks and sporadic disease |
| W | 4-O-α-D-galactopyranosyl-N-acetylneuraminic acid | Sporadic disease; outbreaks of disease associated with mass gatherings; epidemics in sub-Saharan Africa |
| X | (α1→4) N-acetyl-D-glucosamine-1-phosphate | Sporadic disease and large outbreaks in the meningitis belt of Africa |
| Y | 4-O-α-D-glucopyranosyl-N-acetylneuraminic acid | Sporadic disease and occasional small institutional outbreaks |
3.2 Pathogenesis¶
- N. meningitidis has evolved as an effective colonizer of the human nasopharynx, with asymptomatic infection rates of >25% described in some series of adolescents and young adults and among residents of crowded communities.
- Colonization of the nasopharynx involves a series of interactions of meningococcal adhesins (e.g., Opa proteins and pili) with their ligands on the epithelial mucosa.
- N. meningitidis produces an IgA1 protease that is likely to reduce interruption of colonization by mucosal IgA.
- Invasion through the mucosa into the bloodstream occurs rarely, usually within a few days of acquisition of an invasive strain by a susceptible individual.
- Only occasional cases of prolonged colonization prior to invasion have been documented.
- Once the organism is in the bloodstream, its growth may be limited if the individual is partially immune, although bacteremia may allow seeding of another site, such as the meninges or the joints.
- Alternatively, unchecked proliferation may continue, resulting in high bacterial counts in the circulation.
- During growth, meningococci release blebs of outer membrane containing outer-membrane proteins and LPS.
- Endotoxin binds cell-bound CD14 in association with TLR4 to initiate an inflammatory cascade with the release of high levels of various mediators, including soluble TNF receptor, interleukin (IL) 1, IL-1 receptor antagonist, IL-1β, IL-6, IL-8, IL-10, plasminogen-activator inhibitor 1 (PAI-1), and leukemia inhibitory factor.
- Soluble CD14-bound endotoxin acts as a mediator of endothelial activation.
- The severity of meningococcal disease is related both to the levels of endotoxin in the blood and to the magnitude of the inflammatory response.
- The latter is determined to some extent by polymorphisms in inflammatory response genes (and their inhibitors), and the release of the inflammatory cascade heralds the development of meningococcal septicemia (meningococcemia).
- Endothelial injury is central to many clinical features of meningococcemia, including increased vascular permeability, pathologic changes in vascular tone, loss of thromboresistance, intravascular coagulation, and myocardial dysfunction.
- Endothelial injury leads to increased vascular permeability (attributed to loss of glycosaminoglycans and endothelial proteins), with subsequent gross proteinuria.
- Leakage of fluid and electrolytes into the tissues from capillaries ("capillary leak syndrome") leads to hypovolemia, tissue edema, and pulmonary edema.
- Initial compensation results in vasoconstriction and tachycardia, although cardiac output eventually falls.
- While resuscitation fluids may restore circulating volume, tissue edema will continue to increase, and, in the lung, the consequence may be respiratory failure.
- Intravascular thrombosis (caused by activation of procoagulant pathways in association with upregulation of tissue factor on the endothelium) occurs in some patients with meningococcal disease and results in purpura fulminans and infarction of areas of skin or even whole limbs.
- Thrombolysis is also profoundly impaired in meningococcal sepsis through the release of high levels of PAI-1.
- Shock in meningococcal septicemia appears to be attributable to a combination of factors, including hypovolemia, which results from the capillary leak syndrome secondary to endothelial injury, and myocardial depression, which is driven by hypovolemia, hypoxia, metabolic derangements (e.g., hypocalcemia), and cytokines (e.g., IL-6).
- Decreased perfusion of tissues as a result of intravascular thrombosis, vasoconstriction, tissue edema, and reduced cardiac output in meningococcal septicemia can cause widespread organ dysfunction, including renal impairment and—later in the disease—a decreased level of consciousness due to central nervous system involvement.
- Local endothelial injury may result in cerebral edema and rapid onset of raised intracranial pressure in some cases.
4. CLINICAL FEATURES¶
- As discussed above, the most common form of infection with N. meningitidis is asymptomatic carriage of the organism in the nasopharynx.
- While 30–50% of patients present with a meningitis syndrome alone, up to 40% of meningitis patients also present with some features of septicemia.
- Most deaths from meningococcal meningitis alone (i.e., without septicemia) are associated with raised intracranial pressure presenting as a reduced level of consciousness, relative bradycardia and hypertension, focal neurologic signs, abnormal posturing, and signs of brainstem involvement—e.g., unequal, dilated, or poorly reactive pupils; abnormal eye movement; and impaired corneal responses.
- Septicemia: The most common clinical syndromes are meningitis and meningococcal septicemia.
- In fulminant cases, death may occur within hours of the first symptoms.
- Mortality rates among children with this syndrome have been high (25–40%), but early aggressive management may reduce the figure to 10 years of age.
- A nonblanching rash (petechial or purpuric) develops in >80% of cases of meningococcal disease; however, the rash is often absent early in the illness.
- Usually initially blanching in nature (macules, maculopapules, or urticaria) and indistinguishable from more common viral rashes, the rash of meningococcal infection becomes petechial or frankly purpuric over the hours after onset.
- In the most severe cases, large purpuric lesions develop (purpura fulminans).
- Some patients (including those with overwhelming sepsis) may have no rash.
- While petechial rash and fever are important signs of meningococcal disease, <10% of children (and, in some clinical settings, <1% of patients) with this presentation are found to have meningococcal disease.
- Most patients presenting with a petechial or purpuric rash have a viral infection.
- The skin lesions exhibit widespread endothelial necrosis and occlusion of small vessels in the dermis and subcutaneous tissues, with a neutrophilic infiltrate.
- Meningitis: Meningococcal meningitis commonly presents as nonspecific manifestations, including fever, vomiting, and (especially in infants and young children) irritability, and is indistinguishable from other forms of bacterial meningitis unless there is an associated petechial or purpuric rash, which occurs in two-thirds of cases.
- Headache is rarely reported in early childhood but is more common in later childhood and adulthood.
- When headache is present, the following features, in association with fever or a history of fever, are suggestive of bacterial meningitis: neck stiffness, photophobia, decreased level of consciousness, seizures or status epilepticus, and focal neurologic signs.
- Classic signs of meningitis, such as neck stiffness and photophobia, are often absent in infants and young children with bacterial meningitis, who more usually present with fever and irritability and may have a bulging fontanelle.
- Chronic Meningococcemia: Chronic meningococcemia, which is rarely recognized, presents as repeated episodes of petechial rash (Fig. A1-42) associated with fever, joint pain, features of arthritis, and splenomegaly that may progress to acute meningococcal septicemia if untreated.
- During the relapsing course, bacteremia characteristically clears without treatment and then recurs.
- The differential diagnosis includes bacterial endocarditis, acute rheumatic fever, Henoch-Schönlein purpura, infectious mononucleosis, disseminated gonococcal infection, and immune-mediated vasculitis.
- This condition has been associated with complement deficiencies in some cases and with inadequate sulfonamide therapy in others.
- Postmeningococcal Reactive Disease: In a small proportion of patients, an immune complex disease develops ~4–10 days after the onset of meningococcal disease, with manifestations that include a maculopapular or vasculitic rash (2% of cases), arthritis (up to 8% of cases), iritis (1%), pericarditis, and/or polyserositis associated with fever.
- The immune complexes involve meningococcal polysaccharide antigen and result in immunoglobulin and complement deposition with an inflammatory infiltrate.
- These features resolve spontaneously without sequelae.
- It is important to recognize this condition since a new onset of fever and rash, and/or arthritis, can lead to concerns about relapse of meningococcal disease and unnecessarily prolonged antibiotic treatment.
4.1 Septicemia¶
- Septicemia: The most common clinical syndromes are meningitis and meningococcal septicemia.
- In fulminant cases, death may occur within hours of the first symptoms.
- Mortality rates among children with this syndrome have been high (25–40%), but early aggressive management may reduce the figure to 10 years of age.
- A nonblanching rash (petechial or purpuric) develops in >80% of cases of meningococcal disease; however, the rash is often absent early in the illness.
- Usually initially blanching in nature (macules, maculopapules, or urticaria) and indistinguishable from more common viral rashes, the rash of meningococcal infection becomes petechial or frankly purpuric over the hours after onset.
- In the most severe cases, large purpuric lesions develop (purpura fulminans).
- Some patients (including those with overwhelming sepsis) may have no rash.
- While petechial rash and fever are important signs of meningococcal disease, <10% of children (and, in some clinical settings, <1% of patients) with this presentation are found to have meningococcal disease.
- Most patients presenting with a petechial or purpuric rash have a viral infection.
- The skin lesions exhibit widespread endothelial necrosis and occlusion of small vessels in the dermis and subcutaneous tissues, with a neutrophilic infiltrate.
- Shock is manifested by tachycardia, poor peripheral perfusion, tachypnea, and oliguria.
- Decreased cerebral perfusion leads to confusion, agitation, or decreased level of consciousness.
- With progressive shock, multiorgan failure ensues; hypotension is a late sign in children, who more commonly present with compensated shock (tachycardia, poor peripheral perfusion, and normal blood pressure).
- Poor outcome is associated with an absence of meningism, hypotension, young age, coma, relatively low temperature (<38°C), leukopenia, and thrombocytopenia.
- Spontaneous hemorrhage (pulmonary, gastric, or cerebral) may result from consumption of coagulation factors and thrombocytopenia.
Table 2 — Table 160-2 Common Causes of Petechial or Purpuric Rashes¶
| Cause |
|---|
| Enteroviruses |
| Influenza and other respiratory viruses |
| Measles virus |
| Epstein-Barr virus |
| Cytomegalovirus |
| Parvovirus |
| Deficiency of protein C or S (including post-varicella protein S deficiency) |
| Platelet disorders (e.g., idiopathic thrombocytopenic purpura, drug effects, bone marrow infiltration) |
| Henoch-Schönlein purpura, connective tissue disorders, trauma (including nonaccidental injuries in children) |
| Pneumococcal, streptococcal, staphylococcal, or gram-negative bacterial sepsis |
4.2 Meningitis¶
- Meningitis: Meningococcal meningitis commonly presents as nonspecific manifestations, including fever, vomiting, and (especially in infants and young children) irritability, and is indistinguishable from other forms of bacterial meningitis unless there is an associated petechial or purpuric rash, which occurs in two-thirds of cases.
- Headache is rarely reported in early childhood but is more common in later childhood and adulthood.
- When headache is present, the following features, in association with fever or a history of fever, are suggestive of bacterial meningitis: neck stiffness, photophobia, decreased level of consciousness, seizures or status epilepticus, and focal neurologic signs.
- Classic signs of meningitis, such as neck stiffness and photophobia, are often absent in infants and young children with bacterial meningitis, who more usually present with fever and irritability and may have a bulging fontanelle.
- Most deaths from meningococcal meningitis alone (i.e., without septicemia) are associated with raised intracranial pressure presenting as a reduced level of consciousness, relative bradycardia and hypertension, focal neurologic signs, abnormal posturing, and signs of brainstem involvement—e.g., unequal, dilated, or poorly reactive pupils; abnormal eye movement; and impaired corneal responses.
4.3 Chronic Meningococcemia¶
- Chronic Meningococcemia: Chronic meningococcemia, which is rarely recognized, presents as repeated episodes of petechial rash (Fig. A1-42) associated with fever, joint pain, features of arthritis, and splenomegaly that may progress to acute meningococcal septicemia if untreated.
- During the relapsing course, bacteremia characteristically clears without treatment and then recurs.
- The differential diagnosis includes bacterial endocarditis, acute rheumatic fever, Henoch-Schönlein purpura, infectious mononucleosis, disseminated gonococcal infection, and immune-mediated vasculitis.
- This condition has been associated with complement deficiencies in some cases and with inadequate sulfonamide therapy in others.
4.4 Postmeningococcal Reactive Disease¶
- Postmeningococcal Reactive Disease: In a small proportion of patients, an immune complex disease develops ~4–10 days after the onset of meningococcal disease, with manifestations that include a maculopapular or vasculitic rash (2% of cases), arthritis (up to 8% of cases), iritis (1%), pericarditis, and/or polyserositis associated with fever.
- The immune complexes involve meningococcal polysaccharide antigen and result in immunoglobulin and complement deposition with an inflammatory infiltrate.
- These features resolve spontaneously without sequelae.
- It is important to recognize this condition since a new onset of fever and rash, and/or arthritis, can lead to concerns about relapse of meningococcal disease and unnecessarily prolonged antibiotic treatment.
5. DIFFERENTIAL DIAGNOSIS¶
- Petechial/Purpuric Rash: Most patients presenting with a petechial or purpuric rash have a viral infection.
- Meningitis: Meningococcal meningitis is indistinguishable from other forms of bacterial meningitis unless there is an associated petechial or purpuric rash.
- Chronic Meningococcemia: Differential diagnosis includes bacterial endocarditis, acute rheumatic fever, Henoch-Schönlein purpura, infectious mononucleosis, disseminated gonococcal infection, and immune-mediated vasculitis.
- Postmeningococcal Reactive Disease: Differential diagnosis includes bacterial endocarditis, acute rheumatic fever, Henoch-Schönlein purpura, infectious mononucleosis, disseminated gonococcal infection, and immune-mediated vasculitis.
6. INVESTIGATIONS & DIAGNOSIS¶
- Like other invasive bacterial infections, meningococcal disease may produce elevations of the white blood cell (WBC) count and of values for inflammatory markers (e.g., C-reactive protein and procalcitonin levels or the erythrocyte sedimentation rate).
- Values may be normal or low in rapidly progressive disease, and a lack of rise in these laboratory test values does not exclude the diagnosis.
- However, in the presence of fever and a petechial rash, these elevations are suggestive of meningococcal disease.
- In patients with severe meningococcal septicemia, common laboratory findings include hypoglycemia, acidosis, hypokalemia, hypocalcemia, or raised intracranial pressure; hypomagnesemia, hypophosphatemia, anemia, and coagulopathy.
- Although meningococcal disease is often diagnosed on clinical grounds, in suspected meningococcal meningitis or meningococcemia, blood should routinely be sent for culture to confirm the diagnosis and to facilitate public health investigations; blood cultures are positive in up to 75% of cases.
- Culture media containing sodium polyanethol sulfonate, which may inhibit meningococcal growth, should be avoided.
- Meningococcal viability is reduced if there is a delay in transport of the specimen to the microbiology laboratory for culture or in plating of the cerebrospinal fluid (CSF) samples.
- In countries where treatment with antibiotics before hospitalization is recommended for meningococcal disease, the majority of clinically suspected cases are culture negative.
- Real-time polymerase chain reaction (PCR) analysis of whole-blood samples increases the diagnostic yield by >40%, and results obtained with this method may remain positive for several days after administration of antibiotics.
- Unless contraindications exist (raised intracranial pressure, uncorrected shock, disordered coagulation, thrombocytopenia, respiratory insufficiency, local infection, ongoing convulsions), lumbar puncture should be undertaken to identify and confirm the etiology of suspected meningococcal meningitis, whose presentation cannot be distinguished from that of meningitis of other bacterial causes.
- Some authorities have recommended a computed tomography (CT) brain scan prior to lumbar puncture because of the risk of cerebral herniation in patients with raised intracranial pressure.
- However, a normal CT scan is not uncommon in the presence of raised intracranial pressure in meningococcal meningitis, and the decision to perform a lumbar puncture should be made on clinical grounds.
- CSF features of meningococcal meningitis (elevated protein level and WBC count, decreased glucose level) are indistinguishable from those of other types of bacterial meningitis unless a gram-negative diplococcus is identified.
- (Gram’s staining is up to 80% sensitive for meningococcal meningitis.)
- CSF should be submitted for culture (sensitivity, 90%) and (where available) PCR analysis.
- CSF antigen testing with latex agglutination is insensitive and should be replaced by molecular diagnosis when possible.
- Lumbar puncture should generally be avoided in meningococcal septicemia, as positioning for the procedure may critically compromise the patient’s circulation in the context of hypovolemic shock.
- Delayed lumbar puncture may still be useful when the diagnosis is uncertain, particularly if molecular diagnostic technology is available.
- In other types of focal infection, culture and PCR analysis of normally sterile body fluids (e.g., synovial fluid) may aid in the diagnosis.
- Although some authorities have recommended cultures of scrapings or aspirates from skin lesions, this procedure adds little to the diagnostic yield when compared with a combination of blood culture and PCR analysis.
- Urinary antigen testing also is insensitive, and serologic testing for meningococcal infection has not been adequately studied.
7. MANAGEMENT & TREATMENT¶
- Death from meningococcal disease is associated most commonly with hypovolemic shock (meningococcemia) and occasionally with raised intracranial pressure (meningococcal meningitis).
- Therefore, management should focus on the treatment of these urgent clinical issues in addition to the administration of specific antibiotic therapy.
- Delayed recognition of meningococcal disease or its associated physiologic derangements, together with inadequate emergency management, is associated with poor outcome.
- Airway patency may be compromised if the level of consciousness is depressed as a result of shock (impaired cerebral perfusion) or raised intracranial pressure; this situation may require intervention.
- In meningococcemia, pulmonary edema and pulmonary oligemia (presenting as hypoxia) require oxygen therapy or elective endotracheal intubation.
- In cases with shock, aggressive fluid resuscitation (with replacement of the circulating volume several times in severe cases) and inotropic support may be necessary to maintain cardiac output.
- If shock persists after volume resuscitation at 40 mL/kg, the risk of pulmonary edema is high, and elective intubation is recommended to improve oxygenation and decrease work of breathing.
- Metabolic derangements, including hypoglycemia, acidosis, hypokalemia, hypocalcemia, hypomagnesemia, hypophosphatemia, anemia, and coagulopathy, should be anticipated and corrected.
- However, aggressive fluid resuscitation with unbuffered electrolyte solutions was found to increase mortality in febrile African children.
- In the presence of raised intracranial pressure, management includes correction of coexistent shock and neurointensive care to maintain cerebral perfusion.
- Empirical antibiotic therapy for suspected meningococcal disease consists of a third-generation cephalosporin such as ceftriaxone (75–100 mg/kg per d [maximum, 4 g/d] in one or two divided IV doses) or cefotaxime (200 mg/kg per day [maximum, 8 g/d] in four divided IV doses) to cover the various other (potentially penicillin-resistant) bacteria that may produce an indistinguishable clinical syndrome.
- In many settings, vancomycin (usually 4–60 mg/kg per d in two to four divided IV doses) is also recommended for the empiric management of sepsis and/or suspected bacterial meningitis.
- Although unusual in most isolates, reduced meningococcal sensitivity to penicillin (a minimal inhibitory concentration of 0.12–1.0 μg/mL) has been reported.
- Use of penicillin is appropriate up once information on antimicrobial resistance patterns is available.
- Both meningococcal meningitis and meningococcal septicemia are conventionally treated for 7 days, although courses of 3–5 days may be equally effective.
- Furthermore, a single dose of ceftriaxone or an oily suspension of chloramphenicol has been used successfully in resource-poor settings.
- No data are available to guide the duration of treatment for meningococcal infection at other foci (e.g., pneumonia, arthritis); antimicrobial therapy is usually continued until clinical and laboratory evidence of infection has resolved.
- Cultures usually become sterile within 24 h of initiation of appropriate antibiotic chemotherapy.
- Eye infections (including keratoconjunctivitis and endophthalmitis) should be treated with a combination of topical and systemic IV therapy, with some small studies suggesting an increased risk of bacteremia when treated with topical therapy alone.
- The use of glucocorticoids for adjunctive treatment of meningococcal meningitis remains controversial since no relevant studies have had sufficient power to determine true efficacy in this condition.
- One large study in adults did indicate a trend toward benefit, and in clinical practice, a decision to use glucocorticoids would best precede a definite microbiologic diagnosis.
- Therapeutic doses of glucocorticoids are not recommended in meningococcal septicemia, but many intensivists recommend them for meningococcal meningitis.
7.1 Antibiotic Therapy¶
- Empirical antibiotic therapy for suspected meningococcal disease consists of a third-generation cephalosporin such as ceftriaxone (75–100 mg/kg per d [maximum, 4 g/d] in one or two divided IV doses) or cefotaxime (200 mg/kg per day [maximum, 8 g/d] in four divided IV doses) to cover the various other (potentially penicillin-resistant) bacteria that may produce an indistinguishable clinical syndrome.
- In many settings, vancomycin (usually 4–60 mg/kg per d in two to four divided IV doses) is also recommended for the empiric management of sepsis and/or suspected bacterial meningitis.
- Although unusual in most isolates, reduced meningococcal sensitivity to penicillin (a minimal inhibitory concentration of 0.12–1.0 μg/mL) has been reported.
- Use of penicillin is appropriate up once information on antimicrobial resistance patterns is available.
- Both meningococcal meningitis and meningococcal septicemia are conventionally treated for 7 days, although courses of 3–5 days may be equally effective.
- Furthermore, a single dose of ceftriaxone or an oily suspension of chloramphenicol has been used successfully in resource-poor settings.
- No data are available to guide the duration of treatment for meningococcal infection at other foci (e.g., pneumonia, arthritis); antimicrobial therapy is usually continued until clinical and laboratory evidence of infection has resolved.
- Cultures usually become sterile within 24 h of initiation of appropriate antibiotic chemotherapy.
7.2 Supportive Care¶
- Airway patency may be compromised if the level of consciousness is depressed as a result of shock (impaired cerebral perfusion) or raised intracranial pressure; this situation may require intervention.
- In meningococcemia, pulmonary edema and pulmonary oligemia (presenting as hypoxia) require oxygen therapy or elective endotracheal intubation.
- In cases with shock, aggressive fluid resuscitation (with replacement of the circulating volume several times in severe cases) and inotropic support may be necessary to maintain cardiac output.
- If shock persists after volume resuscitation at 40 mL/kg, the risk of pulmonary edema is high, and elective intubation is recommended to improve oxygenation and decrease work of breathing.
- Metabolic derangements, including hypoglycemia, acidosis, hypokalemia, hypocalcemia, hypomagnesemia, hypophosphatemia, anemia, and coagulopathy, should be anticipated and corrected.
- However, aggressive fluid resuscitation with unbuffered electrolyte solutions was found to increase mortality in febrile African children.
- In the presence of raised intracranial pressure, management includes correction of coexistent shock and neurointensive care to maintain cerebral perfusion.
7.3 Adjunctive Therapy¶
- The use of glucocorticoids for adjunctive treatment of meningococcal meningitis remains controversial since no relevant studies have had sufficient power to determine true efficacy in this condition.
- One large study in adults did indicate a trend toward benefit, and in clinical practice, a decision to use glucocorticoids would best precede a definite microbiologic diagnosis.
- Therapeutic doses of glucocorticoids are not recommended in meningococcal septicemia, but many intensivists recommend them for meningococcal meningitis.
- Eye infections (including keratoconjunctivitis and endophthalmitis) should be treated with a combination of topical and systemic IV therapy, with some small studies suggesting an increased risk of bacteremia when treated with topical therapy alone.
8. PROGNOSIS & COMPLICATIONS¶
- About 10% of affected individuals die.
- Mortality rates among children with this syndrome have been high (25–40%), but early aggressive management may reduce the figure to <10%.
- Poor outcome is associated with an absence of meningism, hypotension, young age, coma, relatively low temperature (<38°C), leukopenia, and thrombocytopenia.
- Spontaneous hemorrhage (pulmonary, gastric, or cerebral) may result from consumption of coagulation factors and thrombocytopenia.
- The Glasgow Meningococcal Septicaemia Prognostic Score (GMSPS) performs well and may be clinically useful for severity assessment in meningococcal disease.
- However, scoring systems do not direct the clinician to specific interventions, and the priority in management should be recognition of compromised airways, breathing, or circulation and direct, urgent intervention.
- Most patients improve rapidly with appropriate antibiotics and supportive therapy.
- Fulminant meningococcemia and delayed recognition of meningococcal disease or its associated physiologic derangements, together with inadequate emergency management, is associated with poor outcome.
9. SPECIAL CONSIDERATIONS¶
- Complement deficiency: The best-documented genetic association with meningococcal disease is complement deficiency, chiefly of the terminal complement components (C5–9), properdin, or factor D or those treated with complement inhibitors such as eculizumab.
- Such a deficiency increases the risk of disease by up to 600-fold and may result in recurrent attacks.
- Complement components are believed to be important for the bactericidal activity of serum, which is considered the principal mechanism of immunity against invasive meningococcal disease.
- However, when investigated, complement deficiency is found in only a very small proportion of individuals with meningococcal disease (0.3%).
- Conversely, 7–20% of persons whose disease is caused by the less common capsular groups (W, X, Y, Z, E) have a complement deficiency.
- Complement deficiency appears to be associated with capsular group B disease only rarely.
- Individuals with recurrences of meningococcal disease, particularly those caused by non-B capsular groups, should be assessed for complement deficiency by measurement of total hemolytic complement activity.
- There is also limited evidence that hyposplenism (through reduction in phagocytic capacity), hypogammaglobulinemia (through absence of specific antibody), and HIV increase the risk of meningococcal disease.
- Genetic studies have revealed various associations with disease susceptibility, including complement and mannose-binding lectin deficiency, single-nucleotide polymorphisms in Toll-like receptor (TLR) 4 and tumor necrosis factor (TNF) α, complement factor H, and variants of Fc gamma receptors.
10. KEY PEARLS & CLINICAL TRAPS¶
- Infection with Neisseria meningitidis most commonly manifests as asymptomatic colonization in the nasopharynx of healthy adolescents and adults.
- Invasive disease occurs rarely, usually presenting as either bacterial meningitis or meningococcal septicemia.
- Patients may also present with occult bacteremia, pneumonia, septic arthritis, conjunctivitis, and chronic meningococcemia.
- In total, 12 capsular groups have been identified (A–C, X–Z, E, W, H–J, and L), but just six of these—A, B, C, X, Y, and W (formerly W135)—account for the majority of cases of invasive disease.
- Group D is often listed as the thirteenth capsular group but has been identified as an unencapsulated variant of group C.
- Meningococci are commonly isolated from the nasopharynx in studies of carriage; the lack of capsule often is a result of phase variation of capsule expression, but as many as 16% of isolates lack the genes for capsule synthesis and assembly.
- These "capsule-null" meningococci and those that express capsules other than A, B, C, X, Y, and W are only rarely associated with invasive disease and are most commonly identified in the nasopharynx of asymptomatic carriers.
- The principal determinant of disease susceptibility is age, with the peak incidence in the first year of life.
- The susceptibility of the very young presumably results from an absence of specific adaptive immunity in combination with very close contact with colonized individuals, including parents.
- After early childhood, a second peak of disease occurs among adolescents and young adults (15–25 years of age) in Europe and North America.
- It is thought that this peak relates to social behaviors and the environmental exposures in this age group, as discussed below.
- Most cases of infection with N. meningitidis in developed countries today are sporadic, and the rarity of the disease suggests that individual factors are important.
- Factors that increase the chance of a susceptible individual’s acquiring N. meningitidis via the respiratory route also increase the risk of meningococcal disease.
- Acquisition occurs through close contact with carriers as a result of overcrowding (e.g., in poor socioeconomic settings, in refugee camps, during the Hajj pilgrimage to Mecca, during freshman-year residence in college dormitories), recruitment into the military, and certain social behaviors (e.g., attendance at bars and nightclubs, kissing).
- Secondary cases may occur in close contacts of an index case (e.g., household members, persons kissing the infected individual); the risk to these contacts may be as high as 1000 times the background rate in the population.
- Factors that damage the nasopharyngeal epithelium also increase the risk of both colonization with N. meningitidis and invasive disease.
- The most important of these factors are tobacco smoking (odds ratio, 4.1) and passive exposure to tobacco smoke.
- In addition, recent viral respiratory tract infection, infection with Mycoplasma species, and winter or the dry season (in sub-Saharan Africa) have been associated with meningococcal disease; all of these factors presumably either increase the expression of adhesion molecules in the nasopharynx, thus enhancing meningococcal adhesion, or facilitate meningococcal invasion of the bloodstream.
- While 30–50% of patients present with a meningitis syndrome alone, up to 40% of meningitis patients also present with some features of septicemia.
- Most deaths from meningococcal meningitis alone (i.e., without septicemia) are associated with raised intracranial pressure presenting as a reduced level of consciousness, relative bradycardia and hypertension, focal neurologic signs, abnormal posturing, and signs of brainstem involvement—e.g., unequal, dilated, or poorly reactive pupils; abnormal eye movement; and impaired corneal responses.
- A nonblanching rash (petechial or purpuric) develops in >80% of cases of meningococcal disease; however, the rash is often absent early in the illness.
- Usually initially blanching in nature (macules, maculopapules, or urticaria) and indistinguishable from more common viral rashes, the rash of meningococcal infection becomes petechial or frankly purpuric over the hours after onset.
- In the most severe cases, large purpuric lesions develop (purpura fulminans).
- Some patients (including those with overwhelming sepsis) may have no rash.
- While petechial rash and fever are important signs of meningococcal disease, 40%, and results obtained with this method may remain positive for several days after administration of antibiotics.
- Unless contraindications exist (raised intracranial pressure, uncorrected shock, disordered coagulation, thrombocytopenia, respiratory insufficiency, local infection, ongoing convulsions), lumbar puncture should be undertaken to identify and confirm the etiology of suspected meningococcal meningitis, whose presentation cannot be distinguished from that of meningitis of other bacterial causes.
- Some authorities have recommended a computed tomography (CT) brain scan prior to lumbar puncture because of the risk of cerebral herniation in patients with raised intracranial pressure.
- However, a normal CT scan is not uncommon in the presence of raised intracranial pressure in meningococcal meningitis, and the decision to perform a lumbar puncture should be made on clinical grounds.
- CSF features of meningococcal meningitis (elevated protein level and WBC count, decreased glucose level) are indistinguishable from those of other types of bacterial meningitis unless a gram-negative diplococcus is identified.
- (Gram’s staining is up to 80% sensitive for meningococcal meningitis.)
- CSF should be submitted for culture (sensitivity, 90%) and (where available) PCR analysis.
- CSF antigen testing with latex agglutination is insensitive and should be replaced by molecular diagnosis when possible.
- Lumbar puncture should generally be avoided in meningococcal septicemia, as positioning for the procedure may critically compromise the patient’s circulation in the context of hypovolemic shock.
- Delayed lumbar puncture may still be useful when the diagnosis is uncertain, particularly if molecular diagnostic technology is available.
- In other types of focal infection, culture and PCR analysis of normally sterile body fluids (e.g., synovial fluid) may aid in the diagnosis.
- Although some authorities have recommended cultures of scrapings or aspirates from skin lesions, this procedure adds little to the diagnostic yield when compared with a combination of blood culture and PCR analysis.
- Urinary antigen testing also is insensitive, and serologic testing for meningococcal infection has not been adequately studied.
- Death from meningococcal disease is associated most commonly with hypovolemic shock (meningococcemia) and occasionally with raised intracranial pressure (meningococcal meningitis).
- Therefore, management should focus on the treatment of these urgent clinical issues in addition to the administration of specific antibiotic therapy.
- Delayed recognition of meningococcal disease or its associated physiologic derangements, together with inadequate emergency management, is associated with poor outcome.
- Airway patency may be compromised if the level of consciousness is depressed as a result of shock (impaired cerebral perfusion) or raised intracranial pressure; this situation may require intervention.
- In meningococcemia, pulmonary edema and pulmonary oligemia (presenting as hypoxia) require oxygen therapy or elective endotracheal intubation.
- In cases with shock, aggressive fluid resuscitation (with replacement of the circulating volume several times in severe cases) and inotropic support may be necessary to maintain cardiac output.
- If shock persists after volume resuscitation at 40 mL/kg, the risk of pulmonary edema is high, and elective intubation is recommended to improve oxygenation and decrease work of breathing.
- Metabolic derangements, including hypoglycemia, acidosis, hypokalemia, hypocalcemia, hypomagnesemia, hypophosphatemia, anemia, and coagulopathy, should be anticipated and corrected.
- However, aggressive fluid resuscitation with unbuffered electrolyte solutions was found to increase mortality in febrile African children.
- In the presence of raised intracranial pressure, management includes correction of coexistent shock and neurointensive care to maintain cerebral perfusion.
- Empirical antibiotic therapy for suspected meningococcal disease consists of a third-generation cephalosporin such as ceftriaxone (75–100 mg/kg per d [maximum, 4 g/d] in one or two divided IV doses) or cefotaxime (200 mg/kg per day [maximum, 8 g/d] in four divided IV doses) to cover the various other (potentially penicillin-resistant) bacteria that may produce an indistinguishable clinical syndrome.
- In many settings, vancomycin (usually 4–60 mg/kg per d in two to four divided IV doses) is also recommended for the empiric management of sepsis and/or suspected bacterial meningitis.
- Although unusual in most isolates, reduced meningococcal sensitivity to penicillin (a minimal inhibitory concentration of 0.12–1.0 μg/mL) has been reported.
- Use of penicillin is appropriate up once information on antimicrobial resistance patterns is available.
- Both meningococcal meningitis and meningococcal septicemia are conventionally treated for 7 days, although courses of 3–5 days may be equally effective.
- Furthermore, a single dose of ceftriaxone or an oily suspension of chloramphenicol has been used successfully in resource-poor settings.
- No data are available to guide the duration of treatment for meningococcal infection at other foci (e.g., pneumonia, arthritis); antimicrobial therapy is usually continued until clinical and laboratory evidence of infection has resolved.
- Cultures usually become sterile within 24 h of initiation of appropriate antibiotic chemotherapy.
- Eye infections (including keratoconjunctivitis and endophthalmitis) should be treated with a combination of topical and systemic IV therapy, with some small studies suggesting an increased risk of bacteremia when treated with topical therapy alone.
- The use of glucocorticoids for adjunctive treatment of meningococcal meningitis remains controversial since no relevant studies have had sufficient power to determine true efficacy in this condition.
- One large study in adults did indicate a trend toward benefit, and in clinical practice, a decision to use glucocorticoids would best precede a definite microbiologic diagnosis.
- Therapeutic doses of glucocorticoids are not recommended in meningococcal septicemia, but many intensivists recommend them for meningococcal meningitis.
- About 10% of affected individuals die.
- Mortality rates among children with this syndrome have been high (25–40%), but early aggressive management may reduce the figure to <10%.
- Poor outcome is associated with an absence of meningism, hypotension, young age, coma, relatively low temperature (<38°C), leukopenia, and thrombocytopenia.
- Spontaneous hemorrhage (pulmonary, gastric, or cerebral) may result from consumption of coagulation factors and thrombocytopenia.
- The Glasgow Meningococcal Septicaemia Prognostic Score (GMSPS) performs well and may be clinically useful for severity assessment in meningococcal disease.
- However, scoring systems do not direct the clinician to specific interventions, and the priority in management should be recognition of compromised airways, breathing, or circulation and direct, urgent intervention.
- Most patients improve rapidly with appropriate antibiotics and supportive therapy.
- Fulminant meningococcemia and delayed recognition of meningococcal disease or its associated physiologic derangements, together with inadequate emergency management, is associated with poor outcome.
- The best-documented genetic association with meningococcal disease is complement deficiency, chiefly of the terminal complement components (C5–9), properdin, or factor D or those treated with complement inhibitors such as eculizumab.
- Such a deficiency increases the risk of disease by up to 600-fold and may result in recurrent attacks.
- Complement components are believed to be important for the bactericidal activity of serum, which is considered the principal mechanism of immunity against invasive meningococcal disease.
- However, when investigated, complement deficiency is found in only a very small proportion of individuals with meningococcal disease (0.3%).
- Conversely, 7–20% of persons whose disease is caused by the less common capsular groups (W, X, Y, Z, E) have a complement deficiency.
- Complement deficiency appears to be associated with capsular group B disease only rarely.
- Individuals with recurrences of meningococcal disease, particularly those caused by non-B capsular groups, should be assessed for complement deficiency by measurement of total hemolytic complement activity.
- There is also limited evidence that hyposplenism (through reduction in phagocytic capacity), hypogammaglobulinemia (through absence of specific antibody), and HIV increase the risk of meningococcal disease.
- Genetic studies have revealed various associations with disease susceptibility, including complement and mannose-binding lectin deficiency, single-nucleotide polymorphisms in Toll-like receptor (TLR) 4 and tumor necrosis factor (TNF) α, complement factor H, and variants of Fc gamma receptors.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 160-4 Global percentage distribution of meningococcal capsular groups groups other than B, C, W, and Y. (Adapted from C Pardo de Santayana et al: Epidemiology Epidemiol Infect 151:e57, 2023.) — Electron micrograph of Neisseria meningitidis showing gold-labeled polyclonal antibodies binding surface opacity proteins and blebs of outer membrane being released from the bacterial surface.
Figure 2¶
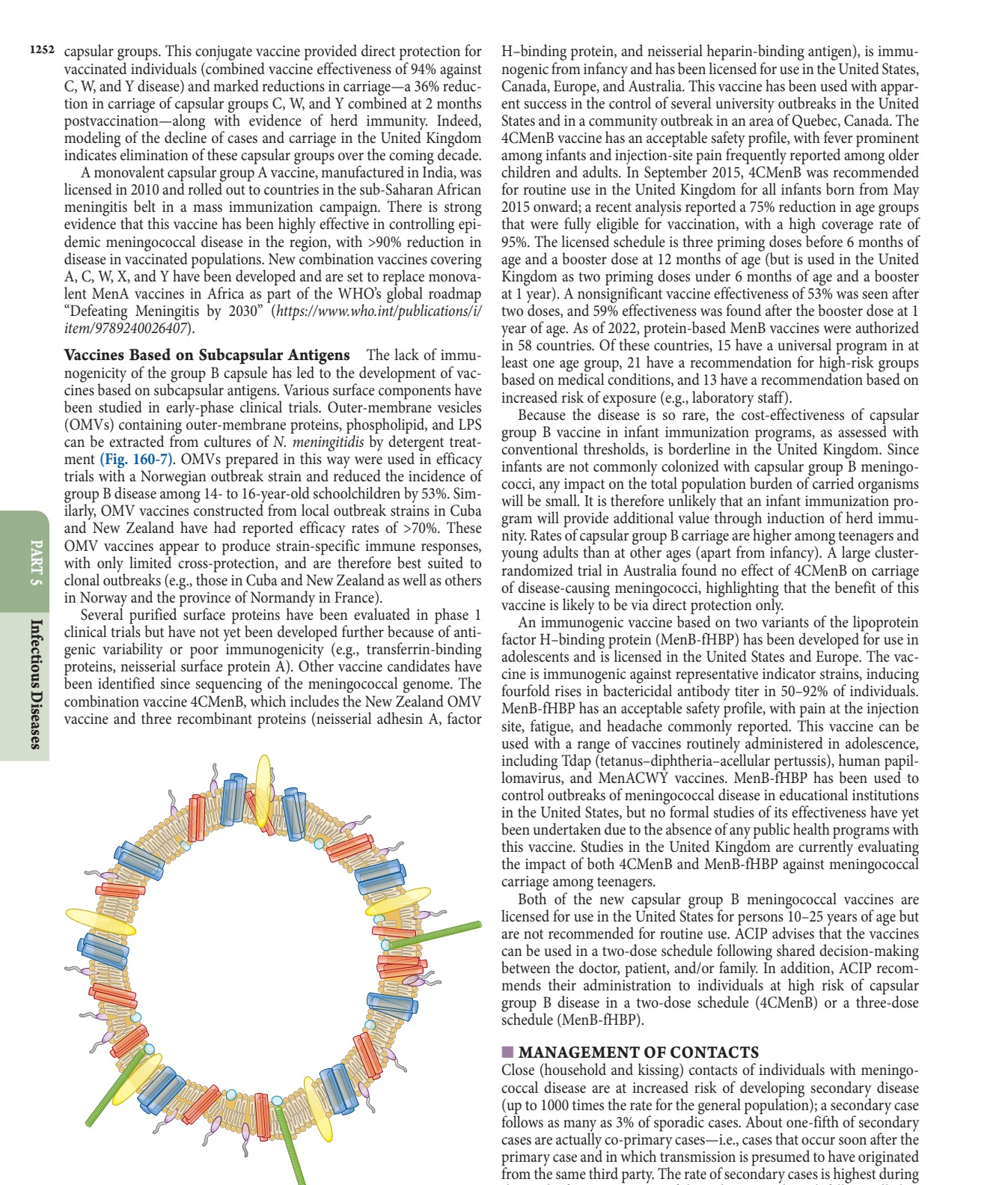
Caption: FIGURE 160-7 Illustration of meningococcal outer-membrane vesicle containing outer-membrane structures. — Cross-section through surface structures of Neisseria meningitidis illustrating LPS, outer membrane proteins (PorA, PorB, Opa, NadA, fHbp), and iron-binding proteins (FetA, RmpM).
Figure 3¶

Caption: FIGURE 160-5 Age distribution of capsular groups B and ACWY meningococcal 2012–2021. (Adapted from https://www.cdc.gov/meningococcal/php/surveillance/.) — Meningococcal disease incidence in the United States from 1997 to 2021, showing a decline from 1.2 cases per 100,000 in 1997 to 0.06 cases per 100,000 in 2021.
Figure 4¶
Caption: FIGURE 160-2 Cross-section through surface structures of Neisseria (Reproduced with permission from M Sadarangani, AJ Pollard: Serogroup B story. Lancet Infect Dis 10:112, 2010.) meningococcal typing. A large database of antigen gene sequences for the outer-membrane proteins PorA, PorB, FetA, Opa, NadA, neisse- rial heparin binding antigen (NHBA), and factor H–binding protein (fHbp) is available online (pubmlst.org/organisms/neisseria-spp). The number of specialized iron-regulated proteins found in the meningo- — Global percentage distribution of meningococcal capsular groups (A, B, C, W, Y, Other) causing invasive meningococcal disease from 2017 to 2019.
Figure 5¶
Caption: FIGURE 160-1 Electron micrograph of Neisseria meningitidis. Black dots are gold-labeled polyclonal antibodies binding surface opacity proteins. Blebs of outer membrane can be seen being released from the bacterial surface (arrow). (Photo courtesy of D. Ferguson, Oxford University.) — Age distribution of capsular groups B and ACWY meningococcal disease in the United States from 2012 to 2021, showing peaks in infants and adolescents.
Figure 6¶

Caption: FIGURE 160-6 A. Polysaccharides from the encapsulated bacteria that cause disease in driving the production of immunoglobulins. There is no production of memory B cells, responses are decreased. B. The carrier protein from protein–polysaccharide presented to carrier peptide–specific T cells, with the consequent production of both T-cell receptor. (Reproduced with permission from AJ Pollard: Maintaining protection Immunol 9:213, 2009.) — Clinical photograph of purpura fulminans, characterized by multiple large purpuric lesions and signs of peripheral ischemia.
Figure 7¶
Caption: FIGURE 160-6 A. Polysaccharides from the encapsulated bacteria that cause disease in driving the production of immunoglobulins. There is no production of memory B cells, responses are decreased. B. The carrier protein from protein–polysaccharide presented to carrier peptide–specific T cells, with the consequent production of both T-cell receptor. (Reproduced with permission from AJ Pollard: Maintaining protection Immunol 9:213, 2009.) — Clinical photograph of chronic meningococcemia presenting as repeated episodes of petechial rash associated with fever and joint pain.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.