Chapter 194: Chlamydial Infections¶
Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Chlamydiae are obligate intracellular bacteria that cause a wide variety of diseases in humans and nonhuman animals.
- C. trachomatis is the most prevalent bacterial sexually transmitted infection (STI) in the world.
- Up to 80–90% of women and >50% of men with C. trachomatis genital infections lack symptoms.
- Untreated infections may lead to pelvic inflammatory disease (PID), tubal factor infertility, ectopic pregnancy, and chronic pelvic pain.
- Lymphogranuloma venereum (LGV) is caused by C. trachomatis serovars L1, L2, and L3 and is an invasive systemic STI.
- Reactive arthritis occurs in 1–2% of cases of nongonococcal urethritis (NGU) and is triggered by C. trachomatis in 4–15% of cases.
- Neonatal transmission during delivery can cause inclusion conjunctivitis and pneumonia in infants.
- Nucleic acid amplification tests (NAATs) are the diagnostic test of choice for chlamydial infection.
- CDC recommends annual screening of all sexually active women <25 years of age and rescreening of previously infected individuals at 3 months.
- Sexually active men who have sex with men (MSM) should undergo at least annual screening at anatomically exposed sites.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Etiologic Agents & Classification
- 1.2 Biology & Growth Cycle
- 2. EPIDEMIOLOGY
- 2.1 Global & U.S. Statistics
- 2.2 Demographic Variations
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Pathogenesis Mechanisms
- 4. CLINICAL FEATURES
- 4.1 Genital Infections
- 4.2 Epididymitis
- 4.3 Reactive Arthritis
- 4.4 Pelvic Inflammatory Disease
- 4.5 Proctitis
- 4.6 Mucopurulent Cervicitis
- 4.7 Urethral Syndrome in Women
- 4.8 Perihepatitis
- 4.9 Infection in Pregnancy and the Neonatal Period
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 NGU Differential
- 5.2 PID Differential
- 5.3 Proctitis Differential
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Methods
- 6.2 Diagnostic Criteria
- 7. MANAGEMENT & TREATMENT
- 7.1 Screening Guidelines
- 7.2 Treatment Principles
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Long-term Sequelae
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy
- 9.2 MSM
- 9.3 HIV Coinfection
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Board Exam Favorites
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Chlamydial intracellular inclusions filled with smaller dense elementary bodies and larger reticulate... |
1. DEFINITION & OVERVIEW¶
Chlamydiae are obligate intracellular bacteria that cause a wide variety of diseases in humans and nonhuman animals. The chlamydiae were originally classified as four species in the genus Chlamydia: C. trachomatis, C. pneumoniae, C. psittaci, and C. pecorum (the last species being found in ruminants). The C. psittaci group has been separated into three species: C. psittaci, C. felis, and C. abortus. The mouse pneumonitis strain (MoPn) is now classified as C. muridarum, and the guinea pig inclusion conjunctivitis strain (GPIC) is now designated C. caviae.
1.1 Etiologic Agents & Classification¶
C. trachomatis is divided into two biovars: trachoma and LGV (lymphogranuloma venereum). The trachoma biovar causes two major types of disease in humans: ocular trachoma, the leading infectious cause of preventable blindness in the developing world; and urogenital infections, which are predominantly sexually transmitted but can be neonatally transmitted. The 18 serovars of C. trachomatis fall into three groups: the trachoma serovars A, B, Ba, and C; the oculogenital serovars D–K; and the LGV serovars L–L. Serovars can be distinguished by serologic typing with monoclonal antibodies or by molecular gene typing. However, serovar identification usually is not important clinically, since the antibiotic susceptibility pattern is the same for all three groups. The one exception applies when LGV is suspected on clinical grounds; in this situation, serovar determination is important because a longer treatment duration is typically required for LGV strains.
Table 1 — C. trachomatis Serovar Classification¶
| Biovar | Serovars | Disease Type |
|---|---|---|
| Trachoma | A, B, Ba, C | Ocular trachoma, Urogenital infections |
| Oculogenital | D–K | Cervicitis, Salpingitis, Urethritis, Epididymitis, Reactive Arthritis, Proctitis |
| LGV | L1, L2, L3 | Lymphogranuloma Venereum (Invasive systemic STI) |
1.2 Biology & Growth Cycle¶
Chlamydiae are nonmotile, gram-negative, obligate intracellular bacteria that replicate within the cytoplasm of host cells, forming the characteristic membrane-bound inclusions that are the basis for some diagnostic tests. Originally considered to be large viruses, chlamydiae differ from viruses in possessing RNA and DNA as well as a cell wall that is quite similar in structure to the cell wall of typical gram-negative bacteria. However, chlamydiae lack peptidoglycan; their structural integrity depends on disulfide binding of outer-membrane proteins. Among the defining characteristics of chlamydiae is a unique growth cycle that involves alternation between two highly specialized morphologic forms: the elementary body, which is the infectious form and is specifically adapted for extracellular survival, and the metabolically active and replicating reticulate body, which is not infectious, is adapted for an intracellular environment, and does not survive well outside the host cell. The biphasic growth cycle begins with attachment of the elementary body (diameter, 0.25–0.35 μm) at specific sites on the surface of the host cell. The elementary body enters the cell through a process similar to receptor-mediated endocytosis and resides in an inclusion, where the entire growth cycle is completed. The chlamydiae prevent phagosome–lysosome fusion. The inclusion membrane is modified by insertion of chlamydial antigens. Once the elementary body has entered the cell, it reorganizes into a reticulate body, which is larger (0.5–1 μm) and contains more RNA. After ~8 h, the reticulate body starts to divide by binary fission. The intracytoplasmic, membrane-bound inclusion body containing the reticulate bodies increases in size as the reticulate bodies multiply. Approximately 18–24 h after infection of the cell, these reticulate bodies begin to become elementary bodies by a reorganization or condensation process that is poorly understood. After rupture of the inclusion body, the elementary bodies are released to initiate another cycle of infection. Chlamydiae are susceptible to many broad-spectrum antibiotics and possess a number of enzymes, but they have a very restricted metabolic capacity. None of these metabolic reactions result in the production of energy. Chlamydiae have thus been considered to be energy parasites that use the ATP produced by the host cell for their own metabolic functions.
2. EPIDEMIOLOGY¶
C. trachomatis genital infections are global in distribution. The World Health Organization (WHO) estimated that in 2020, 50 million (95% uncertainty interval [UI] 36-67) prevalent cases in men and 77 million [UI 67-90] prevalent cases in women and 59 million [95% UI 34-90] new cases of chlamydia in men and 70[95% UI 44-98] new cases in women. These figures make chlamydial infection the most prevalent bacterial STI in the world. There are large differences by WHO region; in 2020 in the Americas, the male incidence (per 1000) was 48 (95% UI, 23–86), compared with 12 (95% UI, 5–25) in Southeast Asia. In women in the Americas, there were 68 (95% UI, 39–104) incident cases (per 1000) compared with 16 (95% UI, 7–28) in Southeast Asia. In the United States, these infections are the most commonly reported of all infectious diseases. Chlamydia is notifiable nationally and is reported to the U.S. Centers for Disease Control and Prevention (CDC). In 2022, 1,649,716 cases were reported to the CDC, representing a 5-year decline of 6.2%. As chlamydial infections are typically asymptomatic, case reports are profoundly influenced by screening coverage. The CDC and other professional organizations recommend annual screening of all sexually active women 25 years who are at increased risk of infection, as well as rescreening of previously infected individuals at 3 months. Additionally, the CDC recommends that all pregnant women aged 25 years who are at increased risk be routinely screened for chlamydia during the first prenatal visit. Women who remain at risk for infection should be retested in the third trimester to prevent maternal complications and neonatal infection. In pregnancy, a test-of-cure is recommended 4 weeks after treatment. The 2022 U.S. total case count corresponds to 495 cases per 100,000 population. Women have the highest infection rates (621.2 cases per 100,000) compared to the rate among men (363.7 cases per 100,000). With the increased availability of urine testing and extragenital testing, men—including gay, bisexual, and other men who have sex with men (MSM)—are increasingly being tested for chlamydial infection. From 2021 to 2022, rates of chlamydial infection in men increased by 1.8%, whereas rates in women fell by 1.2% during this period. Chlamydia rates remain highest among adolescents and young adults; in 2022, 57.7% of all cases were reported among persons aged 15–24 years. Chlamydial infection rates vary considerably among different racial and ethnic populations as well as between states. For example, the rate in Louisiana per 100,000 population in 2022 was 788.6, compared with 198.0 in Vermont; the rate among blacks/African Americans was 1113.3 per 100,000 population compared with 100.6 in Asians.
2.1 Global & U.S. Statistics¶
The prevalence of C. trachomatis in the cervix of pregnant women is approximately six times higher than that of Neisseria gonorrhoeae. The prevalence of genital infection with either agent is highest among women who are between the ages of 20 and 24. Recurrent infections are common in groups with greater vulnerability to STIs and are often acquired from untreated sexual partners. The use of hormonal contraception and the presence of cervical ectopy are also associated with an increased risk. The proportion of infections that are asymptomatic appears to be higher for C. trachomatis (83.9% in men, 87.1% in women) than for N. gonorrhoeae, (41.3% in men, 68.4% in women), and symptomatic C. trachomatis infections are clinically less severe. The costs of C. trachomatis infections and their complications to the U.S. health care system have recently been estimated to be >$516.7 million annually.
Table 2 — U.S. Chlamydia Infection Rates (2022)¶
| Population Group | Cases per 100,000 |
|---|---|
| Women | 621.2 |
| Men | 363.7 |
| Total | 495 |
2.2 Demographic Variations¶
Chlamydia rates remain highest among adolescents and young adults; in 2022, 57.7% of all cases were reported among persons aged 15–24 years. Chlamydial infection rates vary considerably among different racial and ethnic populations as well as between states. For example, the rate in Louisiana per 100,000 population in 2022 was 788.6, compared with 198.0 in Vermont; the rate among blacks/African Americans was 1113.3 per 100,000 population compared with 100.6 in Asians. In a cohort of female college students, incident chlamydial infection was also associated with bacterial vaginosis and high-risk human papillomavirus infection. The prevalence of C. trachomatis cervical infection was 5.9% and 8.8% among asymptomatic male and female college students, respectively between 3.3 and 8.3% among prenatal patients; 7% for women seen in family planning clinics; and >10% for women seen in STI clinics.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Genital infections are primarily caused by C. trachomatis serovars D–K, with serovars D, E, and F involved most frequently. Molecular typing of the major outer-membrane protein gene (omp1) from which serovar differences arise has been used to demonstrate that polymorphisms can occur in isolates from patients who are exposed frequently to multiple infections, while less variation is observed in isolates from less sexually active populations. Polymorphisms in the major outer-membrane protein may provide antigenic variation, and the different forms allow persistence in the community because immunity to one is not protective against the others. The trachoma biovar is essentially a parasite of squamocolumnar epithelial cells; the LGV biovar is more invasive and involves lymphoid cells. As is typical of chlamydiae, C. trachomatis strains are capable of causing chronic, clinically inapparent, asymptomatic infections. Because the duration of the chlamydial growth cycle is ~48–72 h, the incubation period of sexually transmitted chlamydial infections is relatively long—generally 1–3 weeks. C. trachomatis causes cell death as a result of its replicative cycle and can induce cell damage whenever it persists. However, few toxic effects are demonstrated, and cell death because of chlamydial replication is not sufficient to account for disease manifestations, the majority of which are due to immunopathologic mechanisms or nonspecific host responses to the organism or its by-products. Persistent or recurrent chlamydial infections are associated with fibrosis, scarring, and complications following simple squamocolumnar epithelial infections. A common endpoint of these late consequences is scarring of mucous membranes. Genital complications can lead to pelvic inflammatory disease (PID) and its late consequences of tubal factor infertility, ectopic pregnancy, and chronic pelvic pain, while ocular infections may lead to blinding trachoma. High levels of antibody to human heat-shock protein have been associated with tubal factor infertility and ectopic pregnancy. Without adequate therapy, chlamydial infections may persist for several years, although symptoms—if present—usually abate. Pathogenic mechanisms of C. pneumoniae have yet to be completely elucidated. The same is true for C. psittaci, except that this agent infects cells very efficiently and causes disease that may reflect direct cytopathic effects.
3.1 Pathogenesis Mechanisms¶
The chlamydial heat-shock protein, which shares antigenic epitopes that with similar proteins of other bacteria and with human heat-shock protein, may sensitize the host, and repeated infections may cause host cell damage. Evidence of exaggerated cell-mediated and humoral immune responses to chlamydial antigens in reactive arthritis supports this hypothesis. Evidence of chlamydial nucleic acids in synovial membranes and chlamydial elementary bodies in joint fluid suggests that chlamydiae may actually spread from genital to joint tissues in these patients—perhaps in macrophages. The pathogenesis of reactive arthritis is unclear, but this condition probably represents an abnormal host response to a number of infectious agents, including those associated with bacterial gastroenteritis (e.g., Salmonella, Shigella, Yersinia, or Campylobacter), or to infection with C. trachomatis or N. gonorrhoeae. An association between reactive arthritis and the HLA-B27 phenotype in white individuals has been described, but not in patients from sub-Saharan Africa, where the prevalence of HLA-B27 is much lower. Since other mucosal infections produce an identical syndrome, chlamydial infection is thought to initiate an aberrant hyperreactive immune response that produces inflammation of the involved target organs in these genetically predisposed individuals.
4. CLINICAL FEATURES¶
Spectrum Although chlamydiae cause a number of human diseases, localized lower genital tract infections caused by C. trachomatis and the sequelae of such infections are the most important in terms of medical and economic impact. Oculogenital infections due to C. trachomatis serovars D–K are transmitted during sexual contact or from mother to baby during childbirth and are associated with many syndromes, including cervicitis, salpingitis, acute urethral syndrome, endometritis, ectopic pregnancy, infertility, and PID in female patients; urethritis, proctitis, and epididymitis in male patients; and reactive arthritis, conjunctivitis, and pneumonia in infants. Women bear the greatest burden of morbidity because of the serious sequelae of these infections. Untreated infections may lead to PID, and multiple episodes of PID can lead to tubal factor infertility and chronic pelvic pain. Studies estimate that up to 80–90% of women and >50% of men with C. trachomatis genital infections lack symptoms; other patients have very mild symptoms. Additionally, extragenital infection in the pharynx and rectum is typically asymptomatic and may persist for years without treatment. Thus, a large reservoir of infected persons continues to transmit infection to sexual partners.
4.1 Genital Infections¶
NONGONOCOCCAL AND POSTGONOCOCCAL URETHRITIS C. trachomatis is the most common cause of nongonococcal urethritis (NGU) and postgonococcal urethritis (PGU). The designation PGU refers to NGU developing in men 2–3 weeks after treatment of gonococcal urethritis with single doses of agents such as penicillin or cephalosporins, which lack antimicrobial activity against chlamydiae. Current treatment regimens for gonorrhea have evolved and now include combination therapy with ceftriaxone and doxycycline unless chlamydia has been excluded; if chlamydia has been excluded, then gonorrhea is treated with ceftriaxone monotherapy. Thus, both the incidence of PGU and the causative role of C. trachomatis in this syndrome have declined. In the United States, most of the estimated 2 million cases of acute urethritis are NGU, and C. trachomatis is implicated in 30–50% of these cases. The cause of most of the remaining cases of NGU is due to Mycoplasma genitalium; Trichomonas vaginalis and herpes simplex virus (HSV) cause some cases. Other etiologies include Haemophilus species, N. meningitidis, and adenovirus. The rate of involvement of C. trachomatis in urethral infection ranges from 3–7% among asymptomatic men to 15–20% among symptomatic men attending STI clinics. One multisite study of men in Baltimore, Seattle, Denver, and San Francisco reported an overall chlamydial prevalence of 7% in urine samples assessed by nucleic acid amplification tests (NAATs)—molecular tests that amplify the nucleic acids in clinical specimens. As in women, infection in men is age related, with young age most strongly associated with chlamydial urethritis. The prevalence among men is highest at 20–24 years of age. In STI clinics, urethritis is usually less prevalent among MSM than among heterosexual men. NGU is diagnosed by documentation of leukocytes on urethral exudate and by exclusion of gonorrhea by Gram's staining, NAAT, or culture. C. trachomatis urethritis is generally less severe than gonococcal urethritis, although in any individual patient, these two forms of urethritis cannot reliably be differentiated solely on clinical grounds. Symptoms include urethral discharge (often whitish and mucoid rather than frankly purulent), dysuria, and urethral itching. Physical examination may reveal meatal erythema and tenderness as well as a urethral exudate that is often demonstrable only by stripping or milking of the urethra. At least one-third of male patients with C. trachomatis urethral infection have no evident signs or symptoms of urethritis. The availability of NAATs for first-void urine specimens has facilitated broader-based testing for asymptomatic infection in male patients. As a result, asymptomatic chlamydial infection has been demonstrated in 5–10% of sexually active male adolescents screened at school-based clinics or community centers. Such patients generally have pyuria (≥15 leukocytes per 400× microscopic field in the sediment of first-void urine), a positive leukocyte esterase test, or an increased number of leukocytes on a Gram-stained smear prepared from a urogenital swab inserted 1–2 cm into the anterior urethra. When specific diagnostic tests for chlamydiae are not available, the examination of an endourethral specimen for increased leukocytes is useful in differentiating between true urethritis and functional symptoms in symptomatic patients. Alternatively, urethritis can be assayed noninvasively by examination of a first-void urine sample for pyuria, either by microscopy or by the leukocyte esterase test. Urine (or a urethral swab) can also be tested directly for chlamydiae by DNA amplification methods (NAATs), as described below (see "Detection Methods"). Urine testing for urethral STIs in men is much more acceptable than endourethral swab collection.
4.2 Epididymitis¶
Chlamydial urethritis may be followed by acute epididymitis (6 weeks' duration) (e.g., tuberculosis) should be excluded when a patient with unilateral intrascrotal pain and swelling does not respond to appropriate antimicrobial therapy.
4.3 Reactive Arthritis¶
Reactive arthritis consists of conjunctivitis, urethritis (or, in female patients, cervicitis), arthritis, and characteristic mucocutaneous lesions. It may develop in 1–2% of cases of NGU; the rate of chlamydia-induced arthritis has been estimated to be 4–15% and is thought to be the most common type of peripheral inflammatory arthritis in young men. When reactive arthritis is triggered by an STI, it may also be referred to as sexually acquired reactive arthritis (SARA). C. trachomatis has been recovered from the urethra of 16–44% of patients with reactive arthritis and 69% of men with signs of urogenital inflammation at the time of examination. Antibodies to C. trachomatis have also been detected in 46–67% of patients with reactive arthritis, and Chlamydia-specific cell-mediated immunity has been documented in 72%. In addition, C. trachomatis has been isolated from synovial biopsy samples from 15 of 29 patients in a number of small series and from a smaller proportion of synovial fluid specimens. The pathogenesis of reactive arthritis is unclear, but this condition probably represents an abnormal host response to a number of infectious agents, including those associated with bacterial gastroenteritis (e.g., Salmonella, Shigella, Yersinia, or Campylobacter), or to infection with C. trachomatis or N. gonorrhoeae. An association between reactive arthritis and the HLA-B27 phenotype in white individuals has been described, but not in patients from sub-Saharan Africa, where the prevalence of HLA-B27 is much lower. Since other mucosal infections produce an identical syndrome, chlamydial infection is thought to initiate an aberrant hyperreactive immune response that produces inflammation of the involved target organs in these genetically predisposed individuals. Evidence of exaggerated cell-mediated and humoral immune responses to chlamydial antigens in reactive arthritis supports this hypothesis. Evidence of chlamydial nucleic acids in synovial membranes and chlamydial elementary bodies in joint fluid suggests that chlamydiae may actually spread from genital to joint tissues in these patients—perhaps in macrophages. The initial episode of reactive arthritis usually lasts 2–6 months. The initial lesions—usually papules with a central yellow spot—most often involve the soles and palms and, in ~25% of patients, eventually epithelialize and thicken to produce keratoderma blenorrhagicum. Circinate balanitis is usually painless and occurs in fewer than half of patients. The initial episode of reactive arthritis usually lasts 2–6 months. The knees are most frequently involved; next most commonly affected are the ankles and small joints of the feet. Sacroiliitis, either symmetrical or asymmetrical, is documented in two-thirds of patients. Mild bilateral conjunctivitis, iritis, keratitis, or uveitis is sometimes present but lasts for only a few days. Finally, dermatologic manifestations occur in up to 50% of patients. The urethral discharge may be purulent or mucopurulent, and patients may or may not report dysuria. Accompanying prostatitis, usually asymptomatic, has been described. Arthritis usually begins ~4 weeks after the onset of urethritis but may develop sooner or, in a small percentage of cases, may actually precede urethritis.
4.4 Pelvic Inflammatory Disease¶
Inflammation of sections of the fallopian tube is often referred to as salpingitis or PID. The proportion of acute salpingitis cases caused by C. trachomatis varies geographically and with the population studied. It has been estimated that C. trachomatis causes up to 50% of PID cases in the United States. Recent studies report that the proportions of PID cases attributable to N. gonorrhoeae or C. trachomatis is decreasing; approximately 50% of women diagnosed with acute PID tested positive for either organism. PID occurs via ascending intraluminal spread of C. trachomatis or N. gonorrhoeae from the lower genital tract. Mucopurulent cervicitis is often followed by endometritis, endosalpingitis, and finally pelvic peritonitis. Evidence of mucopurulent cervicitis is often found in women with laparoscopically verified salpingitis. Similarly, endometritis, demonstrated by an endometrial biopsy showing plasma cell infiltration of the endometrial epithelium, is documented in most women with laparoscopy-verified chlamydial (or gonococcal) salpingitis. Chlamydial endometritis can also occur in the absence of clinical evidence of salpingitis. Histologic evidence of endometritis has been correlated with a syndrome consisting of vaginal bleeding, lower abdominal pain, and uterine tenderness in the absence of adnexal tenderness. Chlamydial salpingitis produces milder symptoms than gonococcal salpingitis and may be associated with less marked adnexal tenderness. Thus, mild adnexal or uterine tenderness in a sexually active woman with cervicitis may suggest chlamydial PID. Chronic untreated endometrial and tubal inflammation can result in tubal scarring, impaired tubal function, tubal occlusion, and infertility, even among women who report no prior treatment for chlamydial infection. C. trachomatis has been particularly implicated in "subclinical" PID on the basis of a lack of history of PID among Chlamydia-seropositive women with tubal damage and detection of chlamydial DNA or antigen among asymptomatic women with tubal infertility. These data suggest that the best method to prevent PID and its sequelae is surveillance and control of lower genital tract infections along with diagnosis and treatment of sex partners and prevention of reinfections. Promotion of early symptom recognition and health care presentation may reduce the frequency and severity of sequelae of PID.
4.5 Proctitis¶
Primary anal or rectal infections with C. trachomatis have been described in women and MSM who practice receptive anal intercourse. Symptoms are characterized by anorectal pain, a bloody mucopurulent discharge, and tenesmus. Oculogenital serovars D–K and LGV serovars L1, L2, and L3 have been found to cause proctitis. The LGV serovars are far more invasive and typically cause more severely symptomatic disease, including severe ulcerative proctocolitis that can be clinically confused with HSV proctitis. However, asymptomatic or paucisymptomatic LGV infection is increasingly recognized in MSM. Screening and treating sexually active women for chlamydia and gonorrhea reduce their risk for PID. Histologically, LGV proctitis may resemble Crohn's disease in that giant cell formation and granulomas are detected. In the United States and Europe, cases of LGV proctitis occur almost exclusively in MSM, many of whom have HIV infection and other STI coinfections. The less invasive non-LGV serovars of C. trachomatis cause mild proctitis. Many infected individuals are asymptomatic, and in these cases, infection is diagnosed only by routine NAAT of rectal swabs. The number of fecal leukocytes is usually abnormal in both asymptomatic and symptomatic cases. Sigmoidoscopy may yield normal findings or may reveal mild inflammatory changes or small erosions or follicles in the lower 10 cm of the rectum. Histologic examination of rectal biopsies generally shows anal crypts and prominent follicles as well as neutrophilic infiltration of the lamina propria. Chlamydial proctitis is best diagnosed by isolation of C. trachomatis from the rectum and documentation of a response to appropriate therapy. NAATs are the diagnostic test of choice.
4.6 Mucopurulent Cervicitis¶
Although most women with chlamydial infections of the cervix have no symptoms, almost half generally have local signs of infection on examination. Cervicitis is usually characterized by the presence of a mucopurulent discharge, with >20 neutrophils per microscopic field visible in strands of cervical mucus in a thinly smeared, Gram-stained preparation of endocervical exudate. Hypertrophic ectopy of the cervix may also be evident as an edematous area near the cervical os that is congested and bleeds easily on minor trauma (e.g., when a specimen is collected with a swab). A Papanicolaou smear shows increased numbers of neutrophils as well as a characteristic pattern of mononuclear inflammatory cells, including plasma cells, transformed lymphocytes, and histiocytes. Cervical biopsy shows a predominantly mononuclear cell infiltrate of the subepithelial stroma. Clinical experience and collaborative studies indicate that a cutoff of >30 polymorphonuclear leukocytes (PMNs)/1000× field in a Gram-stained smear of cervical mucus correlates best with chlamydial or gonococcal cervicitis. However, the wide availability of NAATs and limited access to microscopy outside of specialist centers has decreased the role of cervical mucus examination. Clinical recognition of chlamydial cervicitis depends on a high index of suspicion and careful cervical examination. No genital symptoms are specifically correlated with chlamydial cervical infection. The differential diagnosis of a mucopurulent discharge from the endocervical canal in a young, sexually active woman includes gonococcal endocervicitis, salpingitis, endometritis, and intrauterine contraceptive device–induced inflammation. Diagnosis of cervicitis is based on the presence of PMNs on a cervical swab as noted above; the presence of chlamydiae is confirmed by NAAT.
4.7 Urethral Syndrome in Women¶
In the absence of infection with uropathogens such as coliforms or Staphylococcus saprophyticus, C. trachomatis is the pathogen most commonly isolated from college women with dysuria, frequency, and pyuria. Screening studies can recover C. trachomatis at both the cervix and the urethra; in up to 25% of infected women, the organism is isolated only from the urethra. The urethral syndrome in women consists of dysuria and frequency in conjunction with chlamydial urethritis, pyuria, and no bacteriuria or urinary pathogens. Although symptoms of the urethral syndrome may develop in some women with chlamydial infection, the majority of women attending STI clinics for urethral chlamydial infection do not have dysuria or frequency. Even in women with chlamydial urethritis causing the acute urethral syndrome, signs of urethritis such as urethral discharge, meatal redness, and swelling are uncommon. However, mucopurulent cervicitis in a woman presenting with dysuria and frequency strongly suggests C. trachomatis urethritis. Other correlates of chlamydial urethral syndrome include a duration of dysuria of >7–10 days, lack of hematuria, and lack of suprapubic tenderness. Abnormal urethral Gram's stains showing >10 PMNs/1000× field in women with dysuria but without coliform bacteriuria support the diagnosis of chlamydial urethritis. Other possible diagnoses include gonococcal or trichomonal infection of the urethra.
4.8 Perihepatitis¶
Fitz-Hugh–Curtis syndrome was originally described as a complication of gonococcal PID. However, studies over the past several decades have suggested that chlamydial infection is more commonly associated with perihepatitis than is N. gonorrhoeae. Perihepatitis should be suspected in young, sexually active women who develop right-upper-quadrant pain, fever, or nausea. Evidence of salpingitis may or may not be found on examination. Frequently, perihepatitis is strongly associated with extensive tubal scarring, adhesions, and inflammation observed at laparoscopy, and high titers of antibody to the 57-kDa chlamydial heat-shock protein have been documented. Culture and/or serologic evidence of C. trachomatis has been found in three-fourths of women with this syndrome.
4.9 Infection in Pregnancy and the Neonatal Period¶
Infections during pregnancy can be transmitted to infants during delivery. Approximately 20–30% of infants exposed to C. trachomatis in the birth canal develop conjunctivitis, and 10–15% subsequently develop pneumonia. All newborn infants receive ocular prophylaxis at birth to prevent ophthalmia neonatorum. The agents used to prevent gonococcal eye infection are not effective against chlamydial conjunctivitis. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. Inclusions within epithelial cells are often detected in Giemsa-stained conjunctival smears, but these smears are considerably less sensitive than cultures or NAATs for chlamydiae. Gram-stained smears may show gonococci or occasional small gram-negative coccobacilli in Haemophilus conjunctivitis, but smears should be accompanied by cultures or NAATs for these agents. C. trachomatis has also been isolated frequently and persistently from the nasopharynx, rectum, and vagina of infected infants—occasionally for >1 year in the absence of treatment. In some cases, otitis media results from perinatally acquired chlamydial infection. Pneumonia may develop in infants from 2 weeks to 4 months of age. C. trachomatis is estimated to cause 20–30% of pneumonia cases in infants <6 months of age. Epidemiologic studies have linked chlamydial pulmonary infection in infants with increased occurrence of subacute lung disease (bronchitis, asthma, wheezing) in later childhood. The most common presenting picture in heterosexual men and women is the inguinal syndrome, which is characterized by painful inguinal lymphadenopathy beginning 2–6 weeks after presumed exposure; in rare instances, the onset comes after a few months. The inguinal adenopathy is unilateral in two-thirds of cases, and palpable enlargement of the iliac and femoral nodes is often evident on the same side as the enlarged inguinal nodes. The nodes are initially discrete, but progressive periadenitis results in a matted mass of nodes that becomes fluctuant and suppurative. The overlying skin becomes fixed, inflamed, and thin, and multiple draining fistulas finally develop. Extensive enlargement of chains of inguinal nodes above and below the inguinal ligament ("the groove sign") is not specific and, although not uncommon, is documented in only a minority of cases. Spontaneous healing usually takes place after several months; inguinal scars or granulomatous masses of various sizes persist for life. Massive pelvic lymphadenopathy may lead to exploratory laparotomy. C. trachomatis serovars L1, L2, and L3 cause LGV, an invasive systemic STI. The peak incidence of LGV corresponds with the age of greatest sexual activity.
5. DIFFERENTIAL DIAGNOSIS¶
The differential diagnosis of a mucopurulent discharge from the endocervical canal in a young, sexually active woman includes gonococcal endocervicitis, salpingitis, endometritis, and intrauterine contraceptive device–induced inflammation. Diagnosis of cervicitis is based on the presence of PMNs on a cervical swab as noted above; the presence of chlamydiae is confirmed by NAAT. The differential diagnosis of urethritis includes gonococcal urethritis, Mycoplasma genitalium, Trichomonas vaginalis, HSV, Haemophilus species, N. meningitidis, and adenovirus. The differential diagnosis of proctitis includes HSV proctitis, Crohn's disease, and LGV. The differential diagnosis of neonatal conjunctivitis includes N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, and HSV.
5.1 NGU Differential¶
The cause of most of the remaining cases of NGU is due to Mycoplasma genitalium; Trichomonas vaginalis and herpes simplex virus (HSV) cause some cases. Other etiologies include Haemophilus species, N. meningitidis, and adenovirus. C. trachomatis urethritis is generally less severe than gonococcal urethritis, although in any individual patient, these two forms of urethritis cannot reliably be differentiated solely on clinical grounds.
5.2 PID Differential¶
Chlamydial salpingitis produces milder symptoms than gonococcal salpingitis and may be associated with less marked adnexal tenderness. Thus, mild adnexal or uterine tenderness in a sexually active woman with cervicitis may suggest chlamydial PID. The differential diagnosis of a mucopurulent discharge from the endocervical canal in a young, sexually active woman includes gonococcal endocervicitis, salpingitis, endometritis, and intrauterine contraceptive device–induced inflammation.
5.3 Proctitis Differential¶
LGV proctitis may resemble Crohn's disease in that giant cell formation and granulomas are detected. The less invasive non-LGV serovars of C. trachomatis cause mild proctitis. Many infected individuals are asymptomatic, and in these cases, infection is diagnosed only by routine NAAT of rectal swabs. The differential diagnosis includes HSV proctitis and Crohn's disease.
6. INVESTIGATIONS & DIAGNOSIS¶
Culture and PCR are both appropriate methods for the isolation of urogenital mycoplasmas. Culture of these organisms, however, requires special techniques and media that generally are available only at larger medical centers and reference laboratories. Serologic testing is not recommended for the clinical diagnosis of urogenital Mycoplasma infections. Antibiotic resistance testing to guide appropriate therapy is becoming more available to clinical practice. When specific diagnostic tests for chlamydiae are not available, the examination of an endourethral specimen for increased leukocytes is useful in differentiating between true urethritis and functional symptoms in symptomatic patients. Alternatively, urethritis can be assayed noninvasively by examination of a first-void urine sample for pyuria, either by microscopy or by the leukocyte esterase test. Urine (or a urethral swab) can also be tested directly for chlamydiae by DNA amplification methods (NAATs), as described below (see "Detection Methods"). Urine testing for urethral STIs in men is much more acceptable than endourethral swab collection. Inclusions within epithelial cells are often detected in Giemsa-stained conjunctival smears, but these smears are considerably less sensitive than cultures or NAATs for chlamydiae. Gram-stained smears may show gonococci or occasional small gram-negative coccobacilli in Haemophilus conjunctivitis, but smears should be accompanied by cultures or NAATs for these agents. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required.
6.1 Diagnostic Methods¶
NAATs are the diagnostic test of choice. Culture and PCR are both appropriate methods for the isolation of urogenital mycoplasmas. Serologic testing is not recommended for the clinical diagnosis of urogenital Mycoplasma infections. When specific diagnostic tests for chlamydiae are not available, the examination of an endourethral specimen for increased leukocytes is useful in differentiating between true urethritis and functional symptoms in symptomatic patients. Alternatively, urethritis can be assayed noninvasively by examination of a first-void urine sample for pyuria, either by microscopy or by the leukocyte esterase test. Urine (or a urethral swab) can also be tested directly for chlamydiae by DNA amplification methods (NAATs).
6.2 Diagnostic Criteria¶
Diagnosis of cervicitis is based on the presence of PMNs on a cervical swab as noted above; the presence of chlamydiae is confirmed by NAAT. Clinical experience and collaborative studies indicate that a cutoff of >30 polymorphonuclear leukocytes (PMNs)/1000× field in a Gram-stained smear of cervical mucus correlates best with chlamydial or gonococcal cervicitis. However, the wide availability of NAATs and limited access to microscopy outside of specialist centers has decreased the role of cervical mucus examination. Histologic evidence of endometritis has been correlated with a syndrome consisting of vaginal bleeding, lower abdominal pain, and uterine tenderness in the absence of adnexal tenderness. Chlamydial proctitis is best diagnosed by isolation of C. trachomatis from the rectum and documentation of a response to appropriate therapy. NAATs are the diagnostic test of choice.
Table 3 — Diagnostic Criteria for Cervicitis¶
| Criterion | Threshold/Value | Test Method |
|---|---|---|
| PMNs in cervical mucus | >30 PMNs/1000× field | Gram-stained smear |
| PMNs in cervical exudate | >20 neutrophils per microscopic field | Gram-stained preparation |
| Chlamydiae presence | Positive | NAAT |
7. MANAGEMENT & TREATMENT¶
The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. The CDC and other professional organizations recommend annual screening of all sexually active women 25 years who are at increased risk of infection, as well as rescreening of previously infected individuals at 3 months. Additionally, the CDC recommends that all pregnant women aged 25 years who are at increased risk be routinely screened for chlamydia during the first prenatal visit. Women who remain at risk for infection should be retested in the third trimester to prevent maternal complications and neonatal infection. In pregnancy, a test-of-cure is recommended 4 weeks after treatment. The 2022 U.S. total case count corresponds to 495 cases per 100,000 population. Women have the highest infection rates (621.2 cases per 100,000) compared to the rate among men (363.7 cases per 100,000). With the increased availability of urine testing and extragenital testing, men—including gay, bisexual, and other men who have sex with men (MSM)—are increasingly being tested for chlamydial infection. From 2021 to 2022, rates of chlamydial infection in men increased by 1.8%, whereas rates in women fell by 1.2% during this period. Chlamydia rates remain highest among adolescents and young adults; in 2022, 57.7% of all cases were reported among persons aged 15–24 years. Chlamydial infection rates vary considerably among different racial and ethnic populations as well as between states. For example, the rate in Louisiana per 100,000 population in 2022 was 788.6, compared with 198.0 in Vermont; the rate among blacks/African Americans was 1113.3 per 100,000 population compared with 100.6 in Asians. Current treatment regimens for gonorrhea have evolved and now include combination therapy with ceftriaxone and doxycycline unless chlamydia has been excluded; if chlamydia has been excluded, then gonorrhea is treated with ceftriaxone monotherapy. Thus, both the incidence of PGU and the causative role of C. trachomatis in this syndrome have declined. The use of hormonal contraception and the presence of cervical ectopy are also associated with an increased risk. The proportion of infections that are asymptomatic appears to be higher for C. trachomatis (83.9% in men, 87.1% in women) than for N. gonorrhoeae, (41.3% in men, 68.4% in women), and symptomatic C. trachomatis infections are clinically less severe. The costs of C. trachomatis infections and their complications to the U.S. health care system have recently been estimated to be >$516.7 million annually. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required.
7.1 Screening Guidelines¶
The CDC and other professional organizations recommend annual screening of all sexually active women 25 years who are at increased risk of infection, as well as rescreening of previously infected individuals at 3 months. Additionally, the CDC recommends that all pregnant women aged 25 years who are at increased risk be routinely screened for chlamydia during the first prenatal visit. Women who remain at risk for infection should be retested in the third trimester to prevent maternal complications and neonatal infection. In pregnancy, a test-of-cure is recommended 4 weeks after treatment. Sexually active men who have sex with men (MSM) should undergo at least annual screening at anatomically exposed sites.
7.2 Treatment Principles¶
Current treatment regimens for gonorrhea have evolved and now include combination therapy with ceftriaxone and doxycycline unless chlamydia has been excluded; if chlamydia has been excluded, then gonorrhea is treated with ceftriaxone monotherapy. Thus, both the incidence of PGU and the causative role of C. trachomatis in this syndrome have declined. The use of hormonal contraception and the presence of cervical ectopy are also associated with an increased risk. The proportion of infections that are asymptomatic appears to be higher for C. trachomatis (83.9% in men, 87.1% in women) than for N. gonorrhoeae, (41.3% in men, 68.4% in women), and symptomatic C. trachomatis infections are clinically less severe. The costs of C. trachomatis infections and their complications to the U.S. health care system have recently been estimated to be >$516.7 million annually. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required.
8. PROGNOSIS & COMPLICATIONS¶
Untreated infections may lead to PID, and multiple episodes of PID can lead to tubal factor infertility and chronic pelvic pain. Chronic untreated endometrial and tubal inflammation can result in tubal scarring, impaired tubal function, tubal occlusion, and infertility, even among women who report no prior treatment for chlamydial infection. C. trachomatis has been particularly implicated in "subclinical" PID on the basis of a lack of history of PID among Chlamydia-seropositive women with tubal damage and detection of chlamydial DNA or antigen among asymptomatic women with tubal infertility. These data suggest that the best method to prevent PID and its sequelae is surveillance and control of lower genital tract infections along with diagnosis and treatment of sex partners and prevention of reinfections. Promotion of early symptom recognition and health care presentation may reduce the frequency and severity of sequelae of PID. High levels of antibody to human heat-shock protein have been associated with tubal factor infertility and ectopic pregnancy. Without adequate therapy, chlamydial infections may persist for several years, although symptoms—if present—usually abate. The most common presenting picture in heterosexual men and women is the inguinal syndrome, which is characterized by painful inguinal lymphadenopathy beginning 2–6 weeks after presumed exposure; in rare instances, the onset comes after a few months. The inguinal adenopathy is unilateral in two-thirds of cases, and palpable enlargement of the iliac and femoral nodes is often evident on the same side as the enlarged inguinal nodes. The nodes are initially discrete, but progressive periadenitis results in a matted mass of nodes that becomes fluctuant and suppurative. The overlying skin becomes fixed, inflamed, and thin, and multiple draining fistulas finally develop. Extensive enlargement of chains of inguinal nodes above and below the inguinal ligament ("the groove sign") is not specific and, although not uncommon, is documented in only a minority of cases. Spontaneous healing usually takes place after several months; inguinal scars or granulomatous masses of various sizes persist for life. Massive pelvic lymphadenopathy may lead to exploratory laparotomy. C. trachomatis serovars L1, L2, and L3 cause LGV, an invasive systemic STI. The peak incidence of LGV corresponds with the age of greatest sexual activity. The initial episode of reactive arthritis usually lasts 2–6 months. The initial lesions—usually papules with a central yellow spot—most often involve the soles and palms and, in ~25% of patients, eventually epithelialize and thicken to produce keratoderma blenorrhagicum. Circinate balanitis is usually painless and occurs in fewer than half of patients. The initial episode of reactive arthritis usually lasts 2–6 months. The knees are most frequently involved; next most commonly affected are the ankles and small joints of the feet. Sacroiliitis, either symmetrical or asymmetrical, is documented in two-thirds of patients. Mild bilateral conjunctivitis, iritis, keratitis, or uveitis is sometimes present but lasts for only a few days. Finally, dermatologic manifestations occur in up to 50% of patients. The urethral discharge may be purulent or mucopurulent, and patients may or may not report dysuria. Accompanying prostatitis, usually asymptomatic, has been described. Arthritis usually begins ~4 weeks after the onset of urethritis but may develop sooner or, in a small percentage of cases, may actually precede urethritis.
8.1 Long-term Sequelae¶
Untreated infections may lead to PID, and multiple episodes of PID can lead to tubal factor infertility and chronic pelvic pain. Chronic untreated endometrial and tubal inflammation can result in tubal scarring, impaired tubal function, tubal occlusion, and infertility, even among women who report no prior treatment for chlamydial infection. C. trachomatis has been particularly implicated in "subclinical" PID on the basis of a lack of history of PID among Chlamydia-seropositive women with tubal damage and detection of chlamydial DNA or antigen among asymptomatic women with tubal infertility. These data suggest that the best method to prevent PID and its sequelae is surveillance and control of lower genital tract infections along with diagnosis and treatment of sex partners and prevention of reinfections. Promotion of early symptom recognition and health care presentation may reduce the frequency and severity of sequelae of PID. High levels of antibody to human heat-shock protein have been associated with tubal factor infertility and ectopic pregnancy. Without adequate therapy, chlamydial infections may persist for several years, although symptoms—if present—usually abate.
9. SPECIAL CONSIDERATIONS¶
The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required.
9.1 Pregnancy¶
The CDC and other professional organizations recommend annual screening of all sexually active women 25 years who are at increased risk of infection, as well as rescreening of previously infected individuals at 3 months. Additionally, the CDC recommends that all pregnant women aged 25 years who are at increased risk be routinely screened for chlamydia during the first prenatal visit. Women who remain at risk for infection should be retested in the third trimester to prevent maternal complications and neonatal infection. In pregnancy, a test-of-cure is recommended 4 weeks after treatment.
9.2 MSM¶
With the increased availability of urine testing and extragenital testing, men—including gay, bisexual, and other men who have sex with men (MSM)—are increasingly being tested for chlamydial infection. From 2021 to 2022, rates of chlamydial infection in men increased by 1.8%, whereas rates in women fell by 1.2% during this period. Sexually active men who have sex with men (MSM) should undergo at least annual screening at anatomically exposed sites.
9.3 HIV Coinfection¶
In the United States and Europe, cases of LGV proctitis occur almost exclusively in MSM, many of whom have HIV infection and other STI coinfections.
10. KEY PEARLS & CLINICAL TRAPS¶
Up to 80–90% of women and >50% of men with C. trachomatis genital infections lack symptoms. Untreated infections may lead to PID, and multiple episodes of PID can lead to tubal factor infertility and chronic pelvic pain. C. trachomatis is the most common cause of nongonococcal urethritis (NGU) and postgonococcal urethritis (PGU). Reactive arthritis occurs in 1–2% of cases of NGU; the rate of chlamydia-induced arthritis has been estimated to be 4–15% and is thought to be the most common type of peripheral inflammatory arthritis in young men. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required.
10.1 Board Exam Favorites¶
C. trachomatis is the most prevalent bacterial STI in the world. Up to 80–90% of women and >50% of men with C. trachomatis genital infections lack symptoms. Untreated infections may lead to PID, and multiple episodes of PID can lead to tubal factor infertility and chronic pelvic pain. C. trachomatis is the most common cause of nongonococcal urethritis (NGU) and postgonococcal urethritis (PGU). Reactive arthritis occurs in 1–2% of cases of NGU; the rate of chlamydia-induced arthritis has been estimated to be 4–15% and is thought to be the most common type of peripheral inflammatory arthritis in young men. The most effective measure to prevent neonatal chlamydial conjunctivitis is through screening and treatment of chlamydial infections in pregnant women. Without treatment, conjunctivitis usually develops at 5–19 days of life and often results in a profuse mucopurulent discharge. Roughly half of infected infants develop clinical evidence of inclusion conjunctivitis. However, it is impossible to differentiate chlamydial conjunctivitis from other forms of neonatal conjunctivitis (e.g., that due to N. gonorrhoeae, Haemophilus influenzae, Streptococcus pneumoniae, or HSV) on clinical grounds; thus, laboratory diagnosis is required.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
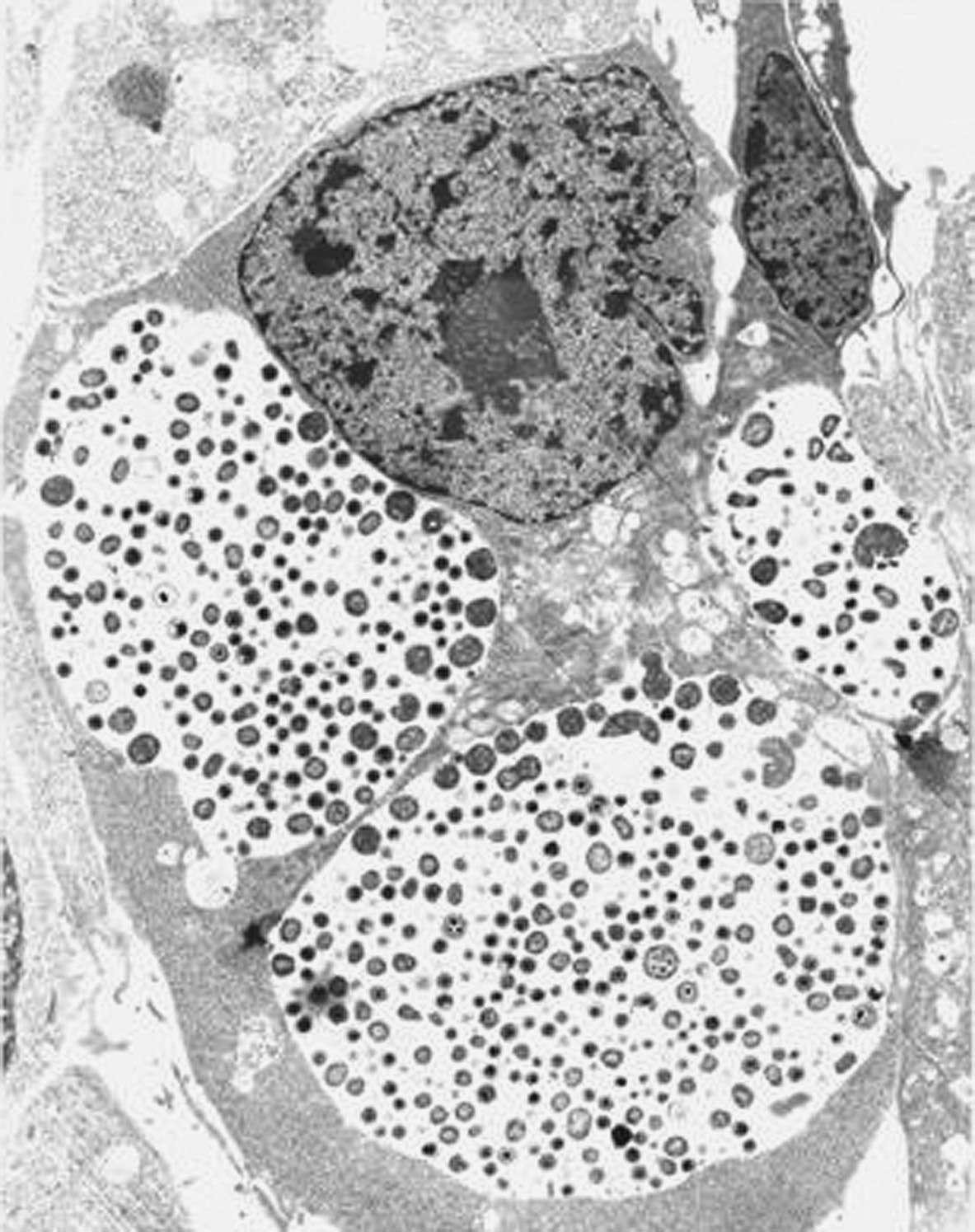
Caption: FIGURE 194-1 Chlamydial intracellular inclusions filled with smaller dense elementary bodies and larger reticulate bodies. (Reprinted with permission from WE Stamm: Chlamydial infections, in Harrison’s Principles of Internal Medicine, 17th ed. AS Fauci et al [eds]. New York, McGraw-Hill, 2008, p 1070.) — FIGURE 194-1 Chlamydial intracellular inclusions filled with smaller dense elementary bodies and larger reticulate bodies. FIGURE 194-2 Chlamydial life cycle showing attachment of elementary bodies, uptake, fusion, multiplication of reticulate bodies, conversion to elementary bodies, and release.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.