Exercise Intolerance¶
Chapter 46 | Part 2: Cardiovascular Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Exercise intolerance is defined as the inability to perform physical activity at a level expected for a person of a given age, sex, body mass, and muscle mass.
- Reduced exercise tolerance is a common symptom of many chronic diseases, including ischemic heart disease, valvular heart disease, heart failure, COPD, ILD, cystic fibrosis, pulmonary hypertension, stroke, neuromuscular disorders, and postinfection syndromes.
- Cardiopulmonary exercise testing (CPET) is the important diagnostic test when a singular cause is unclear or multiple causes are present.
- In HFpEF, causes of exercise intolerance include (in decreasing order of frequency): impaired skeletal muscle diffusion of O2, reduced cardiac output (with exercise), decreased alveolar ventilation, reduced lung diffusing capacity, and anemia.
- Long COVID syndrome is associated with exercise intolerance, often heralded by the inability to return to normal activity levels after acute infection.
- Mechanisms for long COVID–associated fatigue and exercise intolerance include oxidative stress, altered energy metabolism, dysbiosis of the gut microbiome, and cardiac deconditioning.
- Precision medicine approach to treatment of exercise intolerance in HFpEF involves ascertaining the set of causes in any individual patient.
- Focused exercise prescriptions guided by patient-specific pathophysiology have been shown to relieve symptoms in many individuals with long COVID.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Epidemiology & Context
- 2. PATHOBIOLOGY
- 2.1 Cardiopulmonary Exercise Testing (CPET)
- 3. SIGNS AND SYMPTOMS
- 3.1 Heart Failure with Preserved Ejection Fraction (HFpEF)
- 3.2 Long COVID Syndrome
- 4. SPECIFIC DISORDERS
- 4.1 Heart Failure
- 4.2 Long COVID
- 5. INVESTIGATIONS
- 5.1 Cardiopulmonary Exercise Testing (CPET)
- 6. MANAGEMENT & TREATMENT
- 6.1 Precision Medicine Approach
- 6.2 Long COVID Management
- 7. WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- 7.1 HFpEF Specific Clues
- 7.2 Long COVID Specific Clues
- Flowcharts & Algorithms
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Oxygen delivery and utilization pathway |
1. DEFINITION & OVERVIEW¶
- Exercise intolerance is defined as the inability to perform physical activity at a level expected for a person of a given age, sex, body mass, and muscle mass.
- Reduced exercise tolerance is a common symptom of many chronic diseases.
- Diseases associated with exercise intolerance include:
- Ischemic heart disease
- Valvular heart disease
- Heart failure
- Chronic obstructive pulmonary disease (COPD)
- Interstitial lung disease
- Cystic fibrosis
- Pulmonary hypertension
- Stroke
- Neuromuscular disorders
- Postinfection syndromes
- While not all patients with these disorders necessarily manifest exercise intolerance, those who do often have an increased rate of disease progression, as well as mortality.
- It reduces quality of life.
1.1 Epidemiology & Context¶
- Reduced exercise tolerance is a common symptom of many chronic diseases.
- It reduces quality of life.
- While not all patients with these disorders necessarily manifest exercise intolerance, those who do often have an increased rate of disease progression, as well as mortality.
2. PATHOBIOLOGY¶
- The pathobiology of exercise intolerance depends on the specific underlying cause but can be physiologically defined by measuring exercise capacity in terms of the rate of oxygen consumption (VO2) at peak exercise (VO2max).
- Any factor that impairs O2 delivery or utilization can reduce VO2max and cause exercise intolerance.
- In natural sequence, the following factors can each lead to decreased exercise capacity and exercise intolerance:
- Reduced inspired O2 concentration
- Reduced alveolar ventilation
- Impaired lung diffusion from alveolus to capillary
- Reduced hemoglobin concentration or transport (loading or release) of O2
- Decreased cardiac output
- Impaired diffusion of O2 into (skeletal) muscle
- Impaired mitochondrial respiration
- In the absence of clear evidence for a singular cause among these specific pathophysiologic abnormalities (such as decreased cardiac output in a patient with heart failure with reduced ejection fraction) or in the setting of multiple causes, cardiopulmonary exercise testing (CPET) can serve as an important diagnostic test.
- CPET typically involves measurement of breath-by-breath O2 consumption and CO2 production and continuously recording the electrocardiogram during stationary cycle ergometry.
- In more advanced types of CPET, intracardiac (right-heart) pressures are also measured during exercise, as are arterial blood gases and lactate before, during, and after exercise, providing additional diagnostic information to identify the underlying physiologic etiology of exercise limitation.
Table 1 — Table 46-1: Oxygen Delivery and Utilization Pathway (Fig. 46-1)¶
| Step | Physiologic Parameter | Impact on VO2max |
|---|---|---|
| 1 | Reduced inspired O2 concentration | Decreased exercise capacity |
| 2 | Reduced alveolar ventilation | Decreased exercise capacity |
| 3 | Impaired lung diffusion (alveolus to capillary) | Decreased exercise capacity |
| 4 | Reduced hemoglobin concentration or transport | Decreased exercise capacity |
| 5 | Decreased cardiac output | Decreased exercise capacity |
| 6 | Impaired diffusion of O2 into (skeletal) muscle | Decreased exercise capacity |
| 7 | Impaired mitochondrial respiration | Decreased exercise capacity |
2.1 Cardiopulmonary Exercise Testing (CPET)¶
- CPET typically involves measurement of breath-by-breath O2 consumption and CO2 production.
- Continuously recording the electrocardiogram during stationary cycle ergometry.
- In more advanced types of CPET, intracardiac (right-heart) pressures are also measured during exercise.
- Arterial blood gases and lactate are measured before, during, and after exercise.
- Provides additional diagnostic information to identify the underlying physiologic etiology of exercise limitation.
3. SIGNS AND SYMPTOMS¶
- The signs and symptoms of exercise intolerance can vary depending on its severity and etiology.
- Patients with heart failure with reduced ejection fraction following an acute myocardial infarction may be unable to walk up a flight of stairs yet feel comfortable at rest.
- Patients with severe pulmonary arterial hypertension may be short of breath with minimal exertion.
- In some cases, patients who are quite intolerant of exercise may note unusual breathlessness or dyspnea at rest accompanied by tachypnea, (sinus) tachycardia, muscle fatigue, weakness, or frank myalgias.
- A variety of (post)viral syndromes are also associated with exercise intolerance, including Epstein-Barr virus infection and post-COVID-19 (long COVID) syndrome.
- Patients with long COVID often have symptoms that are similar to those of patients with myalgic encephalomyelitis; however, the latter more typically include postexertional malaise.
- In patients following recovery from acute COVID, the inability to return to normal activity levels often heralds the development of long COVID.
- In patients with long COVID, a significant number noted exertional dyspnea, fatigue, and anxiety for up to 3 months after the acute infection, with fatigue remaining as the most common symptom thereafter.
- Orthostatic intolerance and positional tachycardia are common and reflect autonomic dysfunction.
- Among the mechanisms for long COVID–associated fatigue and exercise intolerance are multiple causes, oxidative stress, altered energy metabolism, and dysbiosis of the gut microbiome.
- Cardiac deconditioning is also believed to play a role in the exercise intolerance of long COVID.
Table 2 — Table 46-2: Determinants of Exercise Intolerance in HFpEF (Fig. 46-2)¶
| Category | Specific Determinant | Frequency/Notes |
|---|---|---|
| Skeletal Muscle | Impaired skeletal muscle diffusion of O2 | Most frequent cause |
| Cardiac | Reduced cardiac output (with exercise) | Common |
| Ventilation | Decreased alveolar ventilation | Common |
| Lung | Reduced lung diffusing capacity | Common |
| Hematologic | Anemia | Common |
| Vascular | Increased large artery stiffness | Associated mechanism |
| Vascular | Chronotropic incompetence | Associated mechanism |
| Vascular | Microvascular dysfunction | Endothelium-dependent and endothelium-independent |
| Comorbidities | Inflammation | Contributing factor |
| Comorbidities | Adipokine signaling | Contributing factor |
| Comorbidities | Insulin resistance | In obese diabetics |
3.1 Heart Failure with Preserved Ejection Fraction (HFpEF)¶
- Exercise intolerance in patients with HFpEF is a well-recognized feature of the syndrome.
- The great majority of patients with HFpEF manifest multiple causes including (in decreasing order of frequency):
- Impaired skeletal muscle diffusion of O2
- Reduced cardiac output (with exercise)
- Decreased alveolar ventilation
- Reduced lung diffusing capacity
- Anemia
- Internal work, a body mass index–related measure of the cost of initiating movement, is higher in patients with HFpEF compared with controls and is associated with rapid increases in cardiac filling pressures (and the pulmonary capillary wedge pressure) early in exercise.
- Other associated mechanisms for these abnormalities include increased large artery stiffness, chronotropic incompetence, and microvascular dysfunction (both endothelium-dependent and endothelium-independent).
- Accompanying comorbid conditions may also contribute to these multifactorial drivers of exercise intolerance in HFpEF, including inflammation, adipokine signaling, and insulin resistance in obese diabetics.
3.2 Long COVID Syndrome¶
- A variety of (post)viral syndromes are also associated with exercise intolerance, including Epstein-Barr virus infection and post-COVID-19 (long COVID) syndrome.
- Patients with long COVID often have symptoms that are similar to those of patients with myalgic encephalomyelitis.
- The latter more typically include postexertional malaise.
- In patients following recovery from acute COVID, the inability to return to normal activity levels often heralds the development of long COVID.
- In patients with long COVID, a significant number noted exertional dyspnea, fatigue, and anxiety for up to 3 months after the acute infection.
- Fatigue remains as the most common symptom thereafter.
- Orthostatic intolerance and positional tachycardia are common and reflect autonomic dysfunction.
- Among the mechanisms for long COVID–associated fatigue and exercise intolerance are multiple causes, oxidative stress, altered energy metabolism, and dysbiosis of the gut microbiome.
- Cardiac deconditioning is also believed to play a role in the exercise intolerance of long COVID.
4. SPECIFIC DISORDERS¶
- Exercise intolerance is a common symptom of many chronic diseases.
- Specific disorders include:
- Ischemic heart disease
- Valvular heart disease
- Heart failure
- Chronic obstructive pulmonary disease (COPD)
- Interstitial lung disease
- Cystic fibrosis
- Pulmonary hypertension
- Stroke
- Neuromuscular disorders
- Postinfection syndromes
- While not all patients with these disorders necessarily manifest exercise intolerance, those who do often have an increased rate of disease progression, as well as mortality.
4.1 Heart Failure¶
- Patients with heart failure with reduced ejection fraction following an acute myocardial infarction may be unable to walk up a flight of stairs yet feel comfortable at rest.
- Patients with severe pulmonary arterial hypertension may be short of breath with minimal exertion.
4.2 Long COVID¶
- A variety of (post)viral syndromes are also associated with exercise intolerance, including Epstein-Barr virus infection and post-COVID-19 (long COVID) syndrome.
- Patients with long COVID often have symptoms that are similar to those of patients with myalgic encephalomyelitis.
- The latter more typically include postexertional malaise.
- In patients following recovery from acute COVID, the inability to return to normal activity levels often heralds the development of long COVID.
- In patients with long COVID, a significant number noted exertional dyspnea, fatigue, and anxiety for up to 3 months after the acute infection, with fatigue remaining as the most common symptom thereafter.
- Orthostatic intolerance and positional tachycardia are common and reflect autonomic dysfunction.
- Among the mechanisms for long COVID–associated fatigue and exercise intolerance are multiple causes, oxidative stress, altered energy metabolism, and dysbiosis of the gut microbiome.
- Cardiac deconditioning is also believed to play a role in the exercise intolerance of long COVID.
5. INVESTIGATIONS¶
- In the absence of clear evidence for a singular cause among these specific pathophysiologic abnormalities (such as decreased cardiac output in a patient with heart failure with reduced ejection fraction) or in the setting of multiple causes, cardiopulmonary exercise testing (CPET) can serve as an important diagnostic test.
- CPET typically involves measurement of breath-by-breath O2 consumption and CO2 production and continuously recording the electrocardiogram during stationary cycle ergometry.
- In more advanced types of CPET, intracardiac (right-heart) pressures are also measured during exercise, as are arterial blood gases and lactate before, during, and after exercise, providing additional diagnostic information to identify the underlying physiologic etiology of exercise limitation.
5.1 Cardiopulmonary Exercise Testing (CPET)¶
- CPET typically involves measurement of breath-by-breath O2 consumption and CO2 production.
- Continuously recording the electrocardiogram during stationary cycle ergometry.
- In more advanced types of CPET, intracardiac (right-heart) pressures are also measured during exercise.
- Arterial blood gases and lactate are measured before, during, and after exercise.
- Provides additional diagnostic information to identify the underlying physiologic etiology of exercise limitation.
6. MANAGEMENT & TREATMENT¶
- Ascertaining the set of causes in any individual patient serves as the basis for a precision medicine approach to the treatment of this common symptom in HFpEF, as is the case for other diseases associated with exercise intolerance.
- Focused exercise prescriptions guided by patient-specific pathophysiology have been shown to relieve symptoms in many individuals.
- Treatment strategies depend on the specific underlying cause identified through CPET and other investigations.
6.1 Precision Medicine Approach¶
- Ascertaining the set of causes in any individual patient serves as the basis for a precision medicine approach to the treatment of this common symptom in HFpEF.
- This approach applies to other diseases associated with exercise intolerance.
- Focused exercise prescriptions guided by patient-specific pathophysiology have been shown to relieve symptoms in many individuals.
6.2 Long COVID Management¶
- Focused exercise prescriptions guided by patient-specific pathophysiology have been shown to relieve symptoms in many individuals.
- Mechanisms to address include:
- Oxidative stress management
- Altered energy metabolism correction
- Gut microbiome dysbiosis treatment
- Cardiac deconditioning rehabilitation
7. WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Patients with heart failure with reduced ejection fraction following an acute myocardial infarction may be unable to walk up a flight of stairs yet feel comfortable at rest.
- Patients with severe pulmonary arterial hypertension may be short of breath with minimal exertion.
- In some cases, patients who are quite intolerant of exercise may note unusual breathlessness or dyspnea at rest accompanied by tachypnea, (sinus) tachycardia, muscle fatigue, weakness, or frank myalgias.
- In patients with long COVID, a significant number noted exertional dyspnea, fatigue, and anxiety for up to 3 months after the acute infection, with fatigue remaining as the most common symptom thereafter.
- Orthostatic intolerance and positional tachycardia are common and reflect autonomic dysfunction.
- Internal work, a body mass index–related measure of the cost of initiating movement, is higher in patients with HFpEF compared with controls and is associated with rapid increases in cardiac filling pressures (and the pulmonary capillary wedge pressure) early in exercise.
7.1 HFpEF Specific Clues¶
- Inability to walk up a flight of stairs yet feel comfortable at rest.
- Rapid increases in cardiac filling pressures (and the pulmonary capillary wedge pressure) early in exercise.
- Higher internal work (BMI-related measure of cost of initiating movement) compared with controls.
7.2 Long COVID Specific Clues¶
- Inability to return to normal activity levels after acute infection.
- Exertional dyspnea, fatigue, and anxiety for up to 3 months after the acute infection.
- Fatigue remaining as the most common symptom thereafter.
- Orthostatic intolerance and positional tachycardia.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
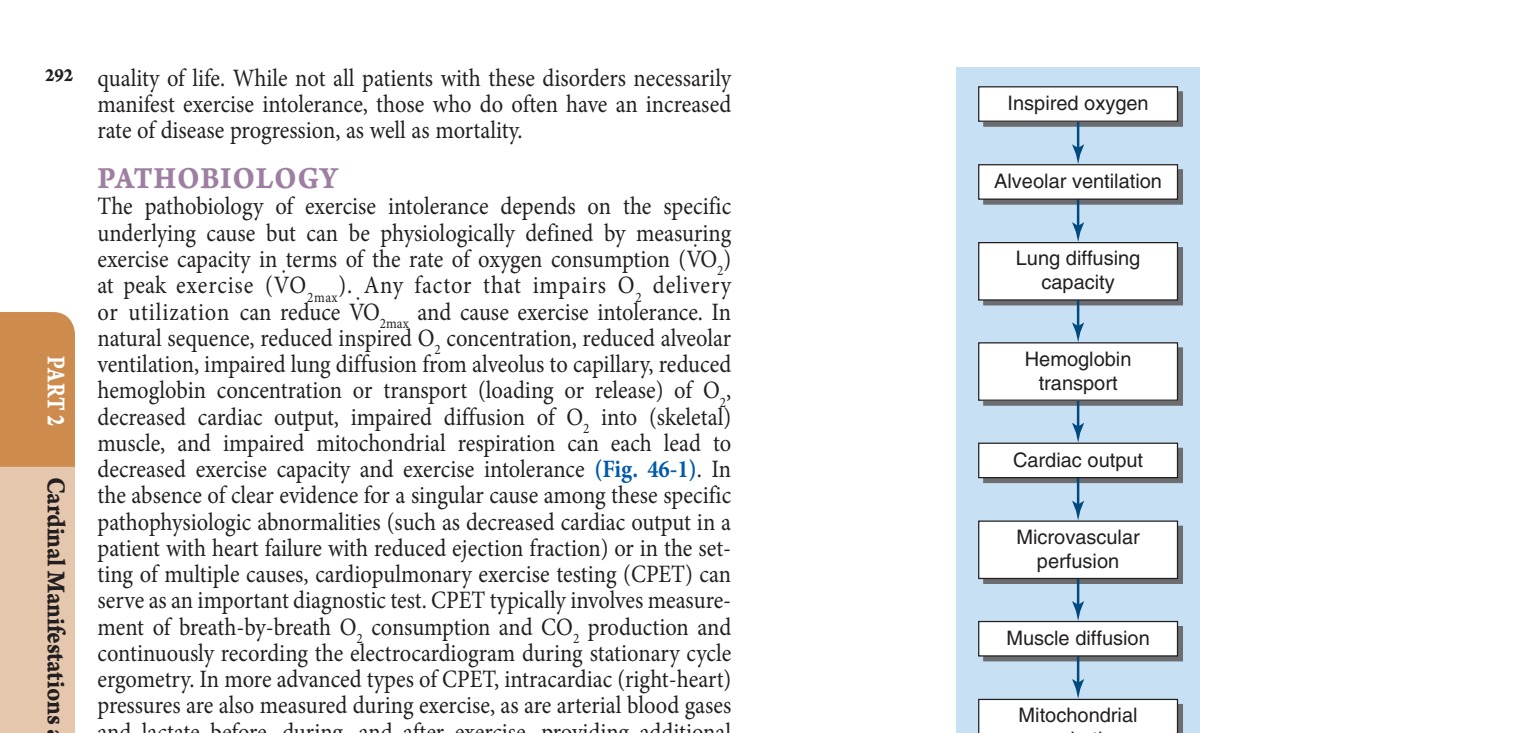
Caption: FIGURE 46-1 Oxygen delivery and utilization pathway.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.