Rickettsial Diseases¶
Chapter 192 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Doxycycline is the drug of choice for all rickettsial diseases; immediate empirical administration is strongly considered in endemic settings.
- Rash appears late (day 6 or later in 20% of cases) and is absent in ~10% of cases; do not wait for rash to treat.
- Eschar (tache noire) is a hallmark of tick-borne spotted fevers (RMSF, MSF, African tick-bite fever) and rickettsialpox.
- Hyponatremia is a common laboratory finding (56% of RMSF cases) due to ADH secretion in response to hypovolemia.
- Thrombocytopenia is common (32–52% of RMSF cases) but DIC is rare.
- Serologic diagnosis (IFA) is usually negative in the first 5–6 days; treat empirically without waiting for serology.
- Skin biopsy with immunohistochemistry is the most useful diagnostic test during acute illness (70% sensitive, 100% specific).
- Mortality rate for RMSF is ~3–5% in postantibiotic era but higher in children (70 years).
- Q fever (Coxiella burnetii) is the only rickettsial agent documented to cause chronic illness.
- R. prowazekii and R. rickettsii are bioterrorism threats due to high infectivity and aerosol transmission capability.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification
- 2. EPIDEMIOLOGY
- 2.1 Vector and Reservoir
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Pathogenesis
- 4. CLINICAL FEATURES
- 4.1 Rash Progression
- 4.2 Eschar
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Viral Mimics
- 5.2 Bacterial Mimics
- 5.3 Hematologic Mimics
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Serology
- 6.2 Biopsy and PCR
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Therapy
- 7.2 Supportive Care
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Mortality and Sequelae
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy
- 9.2 Pediatrics
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Board Favorites
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Peripheral-blood smear from a patient with human granulocytotropic anaplasmosis |
| 2 | 🖼 Figure | Eschar at the site of the mite bite in a patient with... |
| 3 | 🖼 Figure | A |
| 4 | 🖼 Figure | A |
| 5 | 🖼 Figure | A |
| 6 | 🖼 Figure | A |
1. DEFINITION & OVERVIEW¶
- Rickettsial diseases are caused by organisms of the genera Rickettsia and Orientia in the family Rickettsiaceae.
- Rickettsiae are a heterogeneous group of small, obligately intracellular, gram-negative coccobacilli and short bacilli.
- Most are transmitted by a tick, mite, flea, or louse vector.
- Except in the case of louse-borne typhus, humans are incidental hosts.
- Coxiella burnetii, Rickettsia prowazekii, and Rickettsia typhi have the well-documented ability to survive for an extended period outside the reservoir or vector and to be extremely infectious.
- Clinical infections with rickettsiae can be classified according to (1) the taxonomy and diverse microbial characteristics of the agents, (2) epidemiology, or (3) clinical manifestations.
- The clinical manifestations of all the acute presentations are similar during the first 5 days: fever, headache, and myalgias with or without nausea, vomiting, and cough.
- As the course progresses, clinical manifestations—including a macular, maculopapular, or vesicular rash; eschar; pneumonitis; and meningoencephalitis—vary from one disease to another.
- Establishing the etiologic diagnosis of rickettsioses is very difficult during the acute stage of illness, and definitive diagnosis usually requires the examination of serum samples during the acute and convalescent phases of illness.
- Heightened clinical suspicion is based on epidemiologic data, history of exposure to vectors or reservoir animals, travel to endemic locations, clinical manifestations (sometimes including rash or eschar), and characteristic laboratory findings (including thrombocytopenia, normal or low white blood cell [WBC] counts, elevated hepatic enzyme levels, and hyponatremia).
- Such suspicion should prompt empirical treatment.
- Doxycycline is the empirical drug of choice for most of these infections.
- Only one agent, C. burnetii, has been documented to cause chronic illness.
- One other species, R. prowazekii, causes recrudescent illness (Brill-Zinsser disease) when latent infection is reactivated years after resolution of the acute illness.
1.1 Classification¶
- Pathogenic rickettsial species are very closely related, have small genomes (as a result of reductive evolution, which eliminated many genes for biosynthesis of intracellularly available molecules), and are traditionally separated into typhus and spotted fever groups on the basis of lipopolysaccharide antigens.
- The Rickettsiaceae that cause life-threatening infections are, in order of decreasing case–fatality rate, R. rickettsii (RMSF); R. prowazekii (louse-borne typhus); Orientia tsutsugamushi (scrub typhus); R. conorii (MSF); R. typhi (murine typhus); and, in rare cases, other spotted fever–group (SFG) organisms.
- Some agents (e.g., R. parkeri, R. africae, Rickettsia 364D, R. akari, R. slovaca, R. honei, R. felis, R. massiliae, R. helvetica, R. heilongjiangensis, R. aeschlimannii, and R. monacensis) have never been documented to cause a fatal illness.
- The most prevalent SFG rickettsia in the United States, R. amblyommatis, has been circumstantially associated with asymptomatic seroconversion in most persons and with self-limited illness in others.
2. EPIDEMIOLOGY¶
- RMSF occurs in 47 states (with the highest prevalence in the south-central and southeastern states) as well as in Canada, Mexico, and Central and South America.
- The infection is transmitted by Dermacentor variabilis, the American dog tick, in the eastern two-thirds of the United States.
- D. andersoni, the Rocky Mountain wood tick, transmits it in the western United States.
- D. similis transmits it in California.
- Rhipicephalus sanguineus, the brown dog tick, transmits it in Mexico, Arizona, and probably Colombia.
- Amblyomma sculptum, A. mixtum, A. patinoi, A. cajennense, A. tonelliae, and A. aureolatum transmit it in Central and/or South America.
- R. conorii is prevalent in southern Europe, Africa, and southwestern and south-central Asia.
- African tick-bite fever, caused by R. africae, occurs in rural areas of sub-Saharan Africa and in the Caribbean islands.
- Maculatum disease, a similar disease caused by the closely related species R. parkeri, is transmitted by A. maculatum and found in a low percentage of A. americanum ticks in the United States.
- It is also transmitted by A. triste in South America and Arizona as well as A. tigrinum and A. ovale in South America.
- R. japonica causes Japanese spotted fever, which also occurs in Korea, Thailand, Laos, and China.
- Similar diseases in northern Asia are caused by R. sibirica and R. heilongjiangensis.
- Queensland tick typhus due to R. australis is transmitted by Ixodes holocyclus ticks.
- Flinders Island spotted fever, found on the island for which it is named as well as in Tasmania, mainland Australia, and Asia, is caused by R. honei.
- In Europe, patients infected with R. slovaca by a wintertime Dermacentor tick bite usually manifest an afebrile illness with an eschar.
- R. raoultii causes a similar syndrome in Europe and Asia.
- Rickettsia felis is suspected to cause an emerging rickettsiosis worldwide.
- Maintained transovarially in the geographically widespread cat flea, Ctenocephalides felis, the infection has been described as moderately severe.
- Epidemic typhus haunts regions afflicted by wars and disasters.
- The human body louse (Pediculus humanus humanus) lives in clothing under poor hygienic conditions and usually in impoverished cold areas.
- Lice acquire R. prowazekii when they ingest blood from a rickettsemic patient.
- The rickettsiae multiply in the louse’s midgut epithelial cells and are shed in its feces.
- The infected louse leaves a febrile person and deposits infected feces on its subsequent host during its blood meal; the patient autoinoculates the organisms by scratching.
- The louse is killed by the rickettsiae and does not pass R. prowazekii to its offspring.
- R. typhi is maintained in mammalian host–flea cycles, with rats (Rattus rattus and R. norvegicus) and the Oriental rat flea (Xenopsylla cheopis) as the classic zoonotic niche.
- In the United States, murine typhus occurs mainly in Texas, where the disease is expanding northward, and in southern California.
- Globally, endemic typhus occurs mainly in warm (often coastal) areas throughout the tropics and subtropics.
- Scrub typhus is endemic and reemerging in eastern and southern Asia, northern Australia, and islands of the western Pacific and Indian Ocean.
- O. tsutsugamushi is maintained by transovarial transmission in trombiculid mites.
- Infected chiggers are particularly likely to be found in areas of heavy scrub vegetation during the wet season, when mites lay eggs.
- Q fever is caused by Coxiella burnetii.
- Inhalation of aerosols of infected parturition material (goats, sheep, cattle, cats, others), ingestion of infected milk or milk products.
- Worldwide except New Zealand, Antarctica.
2.1 Vector and Reservoir¶
- Epidemiologic clues to the transmission of a particular pathogen include (1) environmental exposure to ticks, fleas, or mites during the season of activity of the vector species for the disease in the appropriate geographic region (spotted fever and typhus rickettsioses, scrub typhus, ehrlichiosis, anaplasmosis).
- (2) travel to or residence in an endemic geographic region during the incubation period.
- (3) exposure to parturient ruminants, cats, and dogs (Q fever).
- (4) exposure to flying squirrels (R. prowazekii infection).
- (5) history of previous louse-borne typhus (recrudescent typhus).
- Maintained partially by transovarian transmission from one generation of ticks to the next, R. rickettsii can be acquired by uninfected ticks through the ingestion of a blood meal from rickettsemic small mammals or by co-feeding adjacent to an infected tick.
- Humans become infected during tick season (in the Northern Hemisphere, from April to September), although some cases occur in winter.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- These diseases, caused by organisms of the genera Rickettsia and Orientia in the family Rickettsiaceae, result from endothelial cell infection and increased vascular permeability.
- R. rickettsii organisms are inoculated into the dermis along with secretions of the tick’s salivary glands after ≥6 h of feeding.
- The rickettsiae spread lymphohematogenously throughout the body and infect numerous foci of contiguous endothelial cells.
- The dose-dependent incubation period is ~1 week (range, 2–14 days).
- Occlusive thrombosis and ischemic necrosis are not the fundamental pathologic bases for tissue and organ injury.
- Instead, increased vascular permeability, with resulting edema, hypovolemia, and ischemia, is responsible.
- Consumption of platelets results in thrombocytopenia in 32–52% of patients, but disseminated intravascular coagulation (DIC) with hypofibrinogenemia is rare.
- Activation of platelets, generation of thrombin, and activation of the fibrinolytic system all appear to be homeostatic physiologic responses to endothelial injury by nonocclusive hemostatic plugs.
- Hypovolemia leads to prerenal azotemia and (in 17% of cases) hypotension.
- Infection of the pulmonary microcirculation leads to noncardiogenic pulmonary edema.
- 12% of patients have acute respiratory distress syndrome, and 8% require mechanical ventilation.
- Cardiac involvement manifests as dysrhythmia in 7–16% of cases.
- Encephalitis, presenting as confusion or lethargy, is apparent in 26–28% of cases.
- Progressively severe encephalitis manifests as stupor or delirium in 21–26% of cases, ataxia in 18%, coma in 10%, and seizures in 8%.
- Numerous focal neurologic deficits have been reported.
- Acute kidney injury, often reversible with rehydration, is caused by acute tubular necrosis in severe cases with shock.
- Hepatic injury with significant increased serum aminotransferase concentrations (38% of cases) is due to multifocal death of individual hepatocytes without hepatic failure.
- Jaundice is recognized in 9% of cases and an elevated serum bilirubin concentration in 18–30%.
- Life-threatening bleeding is rare.
- Anemia develops in 30% of cases and is severe enough to require transfusions in 11%.
- Blood is detected in the stool or vomitus of 10% of patients, and death has followed massive upper-gastrointestinal hemorrhage.
- Other characteristic clinical laboratory findings include increased plasma levels of proteins of the acute-phase response (C-reactive protein, procalcitonin, fibrinogen, ferritin, and others), hypoalbuminemia, and hyponatremia (in 56% of cases) due to the appropriate secretion of antidiuretic hormone in response to the hypovolemic state.
- Myositis occurs occasionally, with marked elevations in serum creatine kinase levels and multifocal rhabdomyonecrosis.
- Ocular involvement includes conjunctivitis in 30% of cases and retinal vein engorgement, flame hemorrhages, arterial occlusion, and papilledema with normal CSF pressure in some instances.
- Severe RMSF can present as sepsis or septic shock.
- In untreated fatal cases, death occurs 8–15 days after onset.
- A rare presentation, fulminant RMSF, is fatal within 5 days after onset.
- This fulminant presentation is seen most often in male black patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency and may be related to an undefined effect of hemolysis on the rickettsial infection.
- Although survivors of RMSF usually return to their previous state of health, permanent sequelae, including neurologic deficits and gangrene necessitating amputation of extremities, may follow severe illness.
- Rickettsiae are potential agents of bioterrorism.
- Infections with R. prowazekii and R. rickettsii have high case–fatality ratios.
- These organisms cause difficult-to-diagnose diseases and are highly infectious when inhaled as aerosols.
- Organisms resistant to tetracycline or chloramphenicol have been developed in the laboratory.
3.1 Pathogenesis¶
- R. rickettsii organisms are inoculated into the dermis along with secretions of the tick’s salivary glands after ≥6 h of feeding.
- The rickettsiae spread lymphohematogenously throughout the body and infect numerous foci of contiguous endothelial cells.
- The dose-dependent incubation period is ~1 week (range, 2–14 days).
- Occlusive thrombosis and ischemic necrosis are not the fundamental pathologic bases for tissue and organ injury.
- Instead, increased vascular permeability, with resulting edema, hypovolemia, and ischemia, is responsible.
- Consumption of platelets results in thrombocytopenia in 32–52% of patients, but disseminated intravascular coagulation (DIC) with hypofibrinogenemia is rare.
- Activation of platelets, generation of thrombin, and activation of the fibrinolytic system all appear to be homeostatic physiologic responses to endothelial injury by nonocclusive hemostatic plugs.
4. CLINICAL FEATURES¶
- Early in the illness, when medical attention usually is first sought, RMSF is difficult to distinguish from many self-limiting viral illnesses.
- Fever, headache, malaise, myalgia, nausea, vomiting, and anorexia are the most common symptoms during the first 3 days.
- The patient becomes progressively more ill as vascular infection and injury advance.
- In one large series, only one-third of patients were diagnosed with presumptive RMSF early in the clinical course and treated appropriately as outpatients.
- In the tertiary-care setting, RMSF is difficult to distinguish from many self-limiting viral illnesses.
- At presentation during the first 3 days of illness, only 3% of patients exhibit the classic triad of fever, rash, and history of tick exposure.
- When a rash appears, a diagnosis of RMSF should be considered.
- However, many illnesses considered in the differential diagnosis also can be associated with a rash, including rubeola, rubella, meningococcemia, disseminated gonococcal infection, secondary syphilis, toxic shock syndrome, drug hypersensitivity, immune thrombocytopenic purpura, thrombotic thrombocytopenic purpura, Kawasaki syndrome, and immune complex vasculitis.
- Conversely, any person in an endemic area with a provisional diagnosis of one of the above illnesses could have RMSF.
- Thus, if a viral infection is suspected during RMSF season in an endemic area, it should always be kept in mind that RMSF can mimic viral infection early in the course.
- If the illness worsens over the next couple of days after initial presentation, the patient should return for reevaluation.
- Rash is evident in only 14% of patients on the first day of illness and in only 49% during the first 3 days.
- Erythematous macules (1–5 mm) appear first on the wrists and ankles and then on the remainder of the extremities and the trunk.
- Later, more severe vascular damage results in frank hemorrhage at the center of the maculopapule, producing a petechia that does not disappear upon compression.
- This sequence of events is sometimes delayed or aborted by effective treatment.
- However, the rash is a variable manifestation, appearing on day 6 or later in 20% of cases and not appearing at all in ~10% of cases.
- Petechiae occur in 41–59% of cases, appearing on or after day 6 in 74% of cases that manifest a rash.
- Involvement of the palms and soles, often considered diagnostically important, usually develops relatively late in the course (after day 5 in 43% of cases) and does not develop at all in 18–64% of cases.
- African tick-bite fever, caused by R. africae, occurs in rural areas of sub-Saharan Africa and in the Caribbean islands.
- The mild illness consists of headache, fever, eschar, and regional lymphadenopathy.
- Amblyomma ticks, a high portion of which are infected with R. africae, often feed in groups, with the consequent development of multiple eschars.
- Rash may be vesicular, sparse, or absent altogether.
- Maculatum disease, a similar disease caused by the closely related species R. parkeri, is transmitted by A. maculatum and found in a low percentage of A. americanum ticks in the United States.
- It is also transmitted by A. triste in South America and Arizona as well as A. tigrinum and A. ovale in South America.
- R. japonica causes Japanese spotted fever, which also occurs in Korea, Thailand, Laos, and China.
- Similar diseases in northern Asia are caused by R. sibirica and R. heilongjiangensis.
- Queensland tick typhus due to R. australis is transmitted by Ixodes holocyclus ticks.
- Flinders Island spotted fever, found on the island for which it is named as well as in Tasmania, mainland Australia, and Asia, is caused by R. honei.
- In Europe, patients infected with R. slovaca by a wintertime Dermacentor tick bite usually manifest an afebrile illness with an eschar (usually on the scalp) and painful regional lymphadenopathy.
- R. raoultii causes a similar syndrome in Europe and Asia.
- Rickettsialpox is recognized principally in New York City, but cases have also been reported in other urban and rural locations in the United States and in Ukraine, Croatia, Mexico, and Turkey.
- A papule forms at the site of the mite’s feeding, develops a central vesicle, and becomes a 1- to 2.5-cm painless black crusted eschar surrounded by an erythematous halo.
- Enlargement of the regional lymph nodes draining the eschar suggests initial lymphogenous spread.
- After an incubation period of 10–17 days, during which the eschar and regional lymphadenopathy frequently go unnoticed, disease onset is marked by malaise, chills, fever, headache, and myalgia.
- A macular rash appears 2–6 days after onset and usually evolves sequentially into papules, vesicles, and crusts that heal without scarring.
- In some cases, the rash remains macular or maculopapular.
- Some patients develop nausea, vomiting, abdominal pain, cough, conjunctivitis, or photophobia.
- Without treatment, fever lasts 6–10 days.
- Epidemic typhus is sometimes misdiagnosed as typhoid fever in tropical countries.
- This means even serologic studies are often unavailable in settings of louse-borne typhus.
- Epidemics can be recognized by the serologic or immunohistochemical diagnosis of a single case or by detection of R. prowazekii in a louse found on a patient.
- After an incubation period of ~1–2 weeks, the onset of illness is abrupt, with prostration, severe headache, and fever rising rapidly to 38.8°–40.0°C (102°–104°F).
- Cough is prominent, developing in 70% of patients.
- Myalgias are usually severe.
- A rash often begins on the upper trunk, usually on the fifth day, and then becomes generalized, involving the entire body except the face, palms, and soles.
- Initially, this rash is macular; without treatment, it becomes maculopapular, petechial, and confluent.
- The rash often goes undetected on black skin; 60% of African patients have spotless epidemic typhus.
- Photophobia, with considerable conjunctival injection, is common.
- The tongue may be dry, brown, and furred.
- Confusion and coma associated with meningoencephalitis are common.
- Skin necrosis and gangrene of the digits as well as interstitial pneumonia may occur in severe cases.
- Untreated disease is fatal in 7–40% of cases, with outcome depending primarily on the condition of the host.
- Patients with untreated infections develop renal insufficiency and multiorgan involvement.
- Clinical laboratory studies frequently reveal anemia and leukopenia early in the course, leukocytosis late in the course, thrombocytopenia, hyponatremia, hypoalbuminemia, increased serum levels of hepatic aminotransferases, and prerenal azotemia.
- Complications can include respiratory failure, hematemesis, cerebral hemorrhage, and hemolysis.
- Severe illness necessitates the admission of 10% of hospitalized patients to an intensive care unit.
- Greater severity is generally associated with old age, underlying disease, and treatment with a sulfonamide.
- The case–fatality rate is 0.4%.
- Rickettsialpox is recognized principally in New York City, but cases have also been reported in other urban and rural locations in the United States and in Ukraine, Croatia, Mexico, and Turkey.
- A papule forms at the site of the mite’s feeding, develops a central vesicle, and becomes a 1- to 2.5-cm painless black crusted eschar surrounded by an erythematous halo.
- Enlargement of the regional lymph nodes draining the eschar suggests initial lymphogenous spread.
- After an incubation period of 10–17 days, during which the eschar and regional lymphadenopathy frequently go unnoticed, disease onset is marked by malaise, chills, fever, headache, and myalgia.
- A macular rash appears 2–6 days after onset and usually evolves sequentially into papules, vesicles, and crusts that heal without scarring.
- In some cases, the rash remains macular or maculopapular.
- Some patients develop nausea, vomiting, abdominal pain, cough, conjunctivitis, or photophobia.
- Without treatment, fever lasts 6–10 days.
4.1 Rash Progression¶
- Rash is evident in only 14% of patients on the first day of illness and in only 49% during the first 3 days.
- Erythematous macules (1–5 mm) appear first on the wrists and ankles and then on the remainder of the extremities and the trunk.
- Later, more severe vascular damage results in frank hemorrhage at the center of the maculopapule, producing a petechia that does not disappear upon compression.
- This sequence of events is sometimes delayed or aborted by effective treatment.
- However, the rash is a variable manifestation, appearing on day 6 or later in 20% of cases and not appearing at all in ~10% of cases.
- Petechiae occur in 41–59% of cases, appearing on or after day 6 in 74% of cases that manifest a rash.
- Involvement of the palms and soles, often considered diagnostically important, usually develops relatively late in the course (after day 5 in 43% of cases) and does not develop at all in 18–64% of cases.
4.2 Eschar¶
- Eschar (tache noire) appears before the onset of fever at the site of the tick bite.
- A severe form of the disease (mortality rate, 50%) occurs in patients with diabetes, alcoholism, or heart failure.
- African tick-bite fever, caused by R. africae, occurs in rural areas of sub-Saharan Africa and in the Caribbean islands.
- The mild illness consists of headache, fever, eschar, and regional lymphadenopathy.
- Amblyomma ticks, a high portion of which are infected with R. africae, often feed in groups, with the consequent development of multiple eschars.
- Rash may be vesicular, sparse, or absent altogether.
- Maculatum disease, a similar disease caused by the closely related species R. parkeri, is transmitted by A. maculatum and found in a low percentage of A. americanum ticks in the United States.
- It is also transmitted by A. triste in South America and Arizona as well as A. tigrinum and A. ovale in South America.
- R. japonica causes Japanese spotted fever, which also occurs in Korea, Thailand, Laos, and China.
- Similar diseases in northern Asia are caused by R. sibirica and R. heilongjiangensis.
- Queensland tick typhus due to R. australis is transmitted by Ixodes holocyclus ticks.
- Flinders Island spotted fever, found on the island for which it is named as well as in Tasmania, mainland Australia, and Asia, is caused by R. honei.
- In Europe, patients infected with R. slovaca by a wintertime Dermacentor tick bite usually manifest an afebrile illness with an eschar (usually on the scalp) and painful regional lymphadenopathy.
- R. raoultii causes a similar syndrome in Europe and Asia.
- Rickettsialpox is recognized principally in New York City, but cases have also been reported in other urban and rural locations in the United States and in Ukraine, Croatia, Mexico, and Turkey.
- A papule forms at the site of the mite’s feeding, develops a central vesicle, and becomes a 1- to 2.5-cm painless black crusted eschar surrounded by an erythematous halo.
- Enlargement of the regional lymph nodes draining the eschar suggests initial lymphogenous spread.
- After an incubation period of 10–17 days, during which the eschar and regional lymphadenopathy frequently go unnoticed, disease onset is marked by malaise, chills, fever, headache, and myalgia.
- A macular rash appears 2–6 days after onset and usually evolves sequentially into papules, vesicles, and crusts that heal without scarring.
- In some cases, the rash remains macular or maculopapular.
- Some patients develop nausea, vomiting, abdominal pain, cough, conjunctivitis, or photophobia.
- Without treatment, fever lasts 6–10 days.
5. DIFFERENTIAL DIAGNOSIS¶
- The differential diagnosis for early clinical manifestations of RMSF (fever, headache, and myalgia without a rash) includes influenza, enteroviral infection, infectious mononucleosis, viral hepatitis, leptospirosis, typhoid fever, gram-negative or gram-positive bacterial sepsis, HME, HGA, murine typhus, sylvatic flying-squirrel typhus, and rickettsialpox.
- Enterocolitis may be suggested by nausea, vomiting, and abdominal pain; prominence of abdominal tenderness has resulted in exploratory laparotomy.
- CNS involvement can masquerade as bacterial or viral meningoencephalitis.
- Cough, pulmonary signs, and chest radiographic opacities can lead to a diagnostic consideration of bronchitis or pneumonia.
- At presentation during the first 3 days of illness, only 3% of patients exhibit the classic triad of fever, rash, and history of tick exposure.
- When a rash appears, a diagnosis of RMSF should be considered.
- However, many illnesses considered in the differential diagnosis also can be associated with a rash, including rubeola, rubella, meningococcemia, disseminated gonococcal infection, secondary syphilis, toxic shock syndrome, drug hypersensitivity, immune thrombocytopenic purpura, thrombotic thrombocytopenic purpura, Kawasaki syndrome, and immune complex vasculitis.
- Conversely, any person in an endemic area with a provisional diagnosis of one of the above illnesses could have RMSF.
- Thus, if a viral infection is suspected during RMSF season in an endemic area, it should always be kept in mind that RMSF can mimic viral infection early in the course.
- If the illness worsens over the next couple of days after initial presentation, the patient should return for reevaluation.
5.1 Viral Mimics¶
- Influenza
- Enteroviral infection
- Infectious mononucleosis
- Viral hepatitis
- Leptospirosis
- Typhoid fever
- Rickettsialpox
5.2 Bacterial Mimics¶
- Gram-negative or gram-positive bacterial sepsis
- Meningococcemia
- Disseminated gonococcal infection
- Secondary syphilis
- Toxic shock syndrome
5.3 Hematologic Mimics¶
- Drug hypersensitivity
- Immune thrombocytopenic purpura
- Thrombotic thrombocytopenic purpura
- Kawasaki syndrome
- Immune complex vasculitis
6. INVESTIGATIONS & DIAGNOSIS¶
- The most common serologic test for confirmation of the diagnosis is the indirect immunofluorescence assay.
- Not until 7–10 days after onset is a reactive titer of ≥64 first detectable.
- The sensitivity and specificity of the indirect immunofluorescence IgG assay are 89–100% and 99–100%, respectively.
- Detection of IgM is no more sensitive in early illness and is subject to nonspecific cross-reactivity.
- It is important to understand that serologic tests for RMSF are usually negative at the time of presentation for medical care and that treatment should not be delayed while a positive serologic result is awaited.
- Because of seropositivity in the expanding geographic distribution of Amblyomma americanum ticks, a positive serologic titer in the first 5–6 days of illness represents preexisting antibody unrelated to the current illness.
- The only diagnostic test that has proven useful during the acute illness is immunohistologic examination of a cutaneous biopsy sample from a rash lesion for R. rickettsii.
- Examination of a 3-mm punch biopsy from such a lesion is 70% sensitive and 100% specific.
- Polymerase chain reaction (PCR) on a rash biopsy would likely yield even higher sensitivity.
- PCR amplification for detection of R. rickettsii DNA in peripheral blood is not adequately sensitive.
- Although rickettsiae are present in large quantities in heavily infected foci of endothelial cells, there are relatively low quantities in the circulation.
- Cultivation of rickettsiae in cell culture is feasible but is seldom undertaken because of technical difficulty and biohazard concerns.
- The recent dramatic increase in the reported incidence of RMSF correlates with the use of single-titer SFG cross-reactive enzyme immunoassay serology.
- Few cases are specifically determined to be caused by R. rickettsii.
- Many febrile persons who do not have RMSF present with cross-reactive antibodies, possibly because of previous exposure to the highly prevalent SFG rickettsia R. amblyommatis.
- Diagnosis of these tick-borne spotted fevers is based on clinical and epidemiologic findings and is confirmed by serology, immunohistochemical demonstration of rickettsiae in skin biopsy specimens, cell-culture isolation of rickettsiae, or PCR of skin biopsy, eschar biopsy or swab, or blood samples.
- Serologic diagnosis detects antibodies to antigens shared among SFG rickettsiae, hindering identification of the etiologic species.
- In an endemic area, a possible diagnosis of rickettsial spotted fevers should be considered when patients present with fever, rash, and/or a skin lesion consisting of a black necrotic lesion or a crust surrounded by erythema.
- Epidemic typhus is sometimes misdiagnosed as typhoid fever in tropical countries.
- This means even serologic studies are often unavailable in settings of louse-borne typhus.
- Epidemics can be recognized by the serologic or immunohistochemical diagnosis of a single case or by detection of R. prowazekii in a louse found on a patient.
- Serologic studies of acute- and convalescent-phase serum samples can provide a diagnosis, and an immunohistochemical method for identification of typhus group-specific antigens in biopsy samples has been developed.
- Cultivation is used infrequently and is not widely available.
- PCR of the blood is not adequately sensitive.
- When endemic typhus is suspected, patients should be treated empirically with doxycycline (100 mg twice daily by mouth for 7 days).
- Where available, chloramphenicol is an alternative.
- Ciprofloxacin and azithromycin are active in vitro, but clinically, they are less effective than doxycycline.
- Peripheral-blood smear from a patient with human granulocytotropic anaplasmosis shows a neutrophil containing two morulae (vacuoles filled with Anaplasma phagocytophilum).
- Ehrlichia chaffeensis and E. muris subsp. eauclairensis infect predominantly mononuclear phagocytes.
- E. ewingii and A. phagocytophilum infect neutrophils.
- Infections with “Candidatus Neoehrlichia mikurensis,” A. capra, and A. bovis are also described.
6.1 Serology¶
- The most common serologic test for confirmation of the diagnosis is the indirect immunofluorescence assay.
- Not until 7–10 days after onset is a reactive titer of ≥64 first detectable.
- The sensitivity and specificity of the indirect immunofluorescence IgG assay are 89–100% and 99–100%, respectively.
- Detection of IgM is no more sensitive in early illness and is subject to nonspecific cross-reactivity.
- It is important to understand that serologic tests for RMSF are usually negative at the time of presentation for medical care and that treatment should not be delayed while a positive serologic result is awaited.
- Because of seropositivity in the expanding geographic distribution of Amblyomma americanum ticks, a positive serologic titer in the first 5–6 days of illness represents preexisting antibody unrelated to the current illness.
6.2 Biopsy and PCR¶
- The only diagnostic test that has proven useful during the acute illness is immunohistologic examination of a cutaneous biopsy sample from a rash lesion for R. rickettsii.
- Examination of a 3-mm punch biopsy from such a lesion is 70% sensitive and 100% specific.
- Polymerase chain reaction (PCR) on a rash biopsy would likely yield even higher sensitivity.
- PCR amplification for detection of R. rickettsii DNA in peripheral blood is not adequately sensitive.
- Although rickettsiae are present in large quantities in heavily infected foci of endothelial cells, there are relatively low quantities in the circulation.
- Cultivation of rickettsiae in cell culture is feasible but is seldom undertaken because of technical difficulty and biohazard concerns.
7. MANAGEMENT & TREATMENT¶
- The drug of choice for the treatment of both children and adults with RMSF is doxycycline.
- Because of the severity of RMSF, immediate empirical administration of doxycycline should be strongly considered for any patient with a consistent clinical presentation in the appropriate epidemiologic setting.
- Doxycycline is administered orally (or, with coma or vomiting, intravenously) at 100 mg twice daily.
- For children with suspected RMSF, up to five courses of doxycycline may be administered with minimal risk of dental staining.
- In patients with allergy to doxycycline, desensitization should be considered.
- Once considered an alternative during pregnancy, chloramphenicol is not readily available in the United States.
- Although available in much of the world, it is less effective than doxycycline.
- Fortunately, there is little evidence to support the occurrence of tetracycline-associated adverse events in mothers (hepatotoxicity) and fetuses (staining of deciduous teeth and teratogenicity) who receive doxycycline.
- The antirickettsial drug should be administered until the patient is afebrile and improving clinically—usually 3–5 days after defervescence.
- β-Lactam antibiotics, erythromycin, and aminoglycosides have no role in the treatment of RMSF.
- Sulfa-containing drugs are associated with more adverse outcomes than no treatment at all.
- There is little clinical experience with fluoroquinolones, clarithromycin, and azithromycin, which are not recommended.
- The most seriously ill patients are managed in intensive care units, with careful administration of fluids to achieve optimal tissue perfusion without precipitating noncardiogenic pulmonary edema.
- In some severely ill patients, hypoxemia requires intubation and mechanical ventilation.
- Oliguric or anuric acute renal failure requires renal replacement therapy.
- Seizures necessitate the use of antiseizure medication.
- Anemia or severe hemorrhage necessitates transfusions of packed red blood cells.
- Bleeding with severe thrombocytopenia requires platelet transfusions.
- As with RMSF, severe cases should be treated with doxycycline (100 mg bid orally) continued for 3–5 days after defervescence.
- Alternative agents for milder disease include doxycycline (100 mg bid orally for 1–5 days), chloramphenicol (500 mg qid orally for 7–10 days), ciprofloxacin (750 mg bid orally for 7 days), and josamycin (3 g/d orally for 5 days) where available.
- Data on the efficacy of treatment of mildly ill children with clarithromycin or azithromycin should not be extrapolated to adults or to patients with moderate or severe illness.
- Epidemic typhus is sometimes misdiagnosed as typhoid fever in tropical countries.
- This means even serologic studies are often unavailable in settings of louse-borne typhus.
- Epidemics can be recognized by the serologic or immunohistochemical diagnosis of a single case or by detection of R. prowazekii in a louse found on a patient.
- Doxycycline (100 mg bid) is administered orally or—if the patient is comatose or vomiting—intravenously and continued until 3–5 days after defervescence.
- Under epidemic conditions, a single 200-mg oral dose can be tried but fails in some cases.
- Pregnant patients should be evaluated individually and treated with chloramphenicol early in pregnancy or with doxycycline late in pregnancy.
- Prevention of epidemic typhus involves control of body lice.
- Clothes should regularly be changed and laundered in hot water, and insecticides can be used every 6 weeks to control the louse population.
- When endemic typhus is suspected, patients should be treated empirically with doxycycline (100 mg twice daily by mouth for 7 days).
- Where available, chloramphenicol is an alternative.
- Ciprofloxacin and azithromycin are active in vitro, but clinically, they are less effective than doxycycline.
- Rickettsialpox is recognized principally in New York City, but cases have also been reported in other urban and rural locations in the United States and in Ukraine, Croatia, Mexico, and Turkey.
- A papule forms at the site of the mite’s feeding, develops a central vesicle, and becomes a 1- to 2.5-cm painless black crusted eschar surrounded by an erythematous halo.
- Enlargement of the regional lymph nodes draining the eschar suggests initial lymphogenous spread.
- After an incubation period of 10–17 days, during which the eschar and regional lymphadenopathy frequently go unnoticed, disease onset is marked by malaise, chills, fever, headache, and myalgia.
- A macular rash appears 2–6 days after onset and usually evolves sequentially into papules, vesicles, and crusts that heal without scarring.
- In some cases, the rash remains macular or maculopapular.
- Some patients develop nausea, vomiting, abdominal pain, cough, conjunctivitis, or photophobia.
- Without treatment, fever lasts 6–10 days.
- Doxycycline is the drug of choice for treatment.
- Prevention Avoidance of tick bites is the only available preventive approach.
- Use of protective clothing and tick repellents, inspection of the body once or twice a day, and removal of ticks before they inoculate rickettsiae reduce the risk of infection.
- Prophylactic doxycycline treatment of tick bites has no proven role in preventing RMSF.
7.1 Pharmacologic Therapy¶
- Drug of choice: Doxycycline.
- Dose: 100 mg twice daily.
- Route: Oral (or intravenously with coma or vomiting).
- Duration: Until afebrile and improving clinically—usually 3–5 days after defervescence.
- Pediatric considerations: Up to five courses may be administered with minimal risk of dental staining.
- Allergy: Desensitization should be considered.
- Pregnancy: Chloramphenicol early in pregnancy or doxycycline late in pregnancy.
- Alternatives for milder disease: Doxycycline (100 mg bid orally for 1–5 days), Chloramphenicol (500 mg qid orally for 7–10 days), Ciprofloxacin (750 mg bid orally for 7 days), Josamycin (3 g/d orally for 5 days).
- Not recommended: Fluoroquinolones, clarithromycin, azithromycin.
- No role: β-Lactam antibiotics, erythromycin, aminoglycosides.
- Adverse outcomes: Sulfa-containing drugs are associated with more adverse outcomes than no treatment at all.
7.2 Supportive Care¶
- Careful administration of fluids to achieve optimal tissue perfusion without precipitating noncardiogenic pulmonary edema.
- Intubation and mechanical ventilation for hypoxemia in some severely ill patients.
- Renal replacement therapy for oliguric or anuric acute renal failure.
- Antiseizure medication for seizures.
- Transfusions of packed red blood cells for anemia or severe hemorrhage.
- Platelet transfusions for bleeding with severe thrombocytopenia.
8. PROGNOSIS & COMPLICATIONS¶
- The mortality rate was 20–25% in the preantibiotic era and has been reported at ~3–5% in the postantibiotic era, principally because of delayed diagnosis and treatment.
- Recent reporting of a relatively low mortality rate (0.4%) for spotted fever rickettsiosis is likely an artifact related to the abundance of less pathogenic SFG rickettsial species likely causing subclinical or undiagnosed infection with cross-reactive anti-SFG antibodies and to a relatively low proportion of diagnostically confirmed cases.
- Indeed, the reported case–fatality rates in confirmed cases in the United States and in parts of Arizona, where R. rickettsii is the sole infecting SFG species, are 9% and 10%, respectively.
- The case–fatality rate is highest among children (70 years).
- For unknown reasons, the case–fatality rate of RMSF in Mexico and Brazil approaches 50%.
- Untreated disease is fatal in 7–40% of cases, with outcome depending primarily on the condition of the host.
- Patients with untreated infections develop renal insufficiency and multiorgan involvement.
- Complications can include respiratory failure, hematemesis, cerebral hemorrhage, and hemolysis.
- Severe illness necessitates the admission of 10% of hospitalized patients to an intensive care unit.
- Greater severity is generally associated with old age, underlying disease, and treatment with a sulfonamide.
- The case–fatality rate is 0.4%.
- Although survivors of RMSF usually return to their previous state of health, permanent sequelae, including neurologic deficits and gangrene necessitating amputation of extremities, may follow severe illness.
- A rare presentation, fulminant RMSF, is fatal within 5 days after onset.
- This fulminant presentation is seen most often in male black patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency and may be related to an undefined effect of hemolysis on the rickettsial infection.
- Rickettsiae are potential agents of bioterrorism.
- Infections with R. prowazekii and R. rickettsii have high case–fatality ratios.
- These organisms cause difficult-to-diagnose diseases and are highly infectious when inhaled as aerosols.
- Organisms resistant to tetracycline or chloramphenicol have been developed in the laboratory.
8.1 Mortality and Sequelae¶
- Mortality rate: 20–25% in preantibiotic era; ~3–5% in postantibiotic era.
- Artifact: Recent reporting of 0.4% mortality likely due to abundance of less pathogenic SFG rickettsial species.
- Confirmed cases: 9% in United States; 10% in parts of Arizona.
- Highest risk: Children (70 years).
- Mexico/Brazil: Approaches 50%.
- Untreated: Fatal in 7–40% of cases.
- Sequelae: Neurologic deficits, gangrene necessitating amputation.
- Fulminant RMSF: Fatal within 5 days after onset.
- G6PD deficiency: Seen in male black patients with fulminant RMSF.
9. SPECIAL CONSIDERATIONS¶
- Pregnant patients should be evaluated individually and treated with chloramphenicol early in pregnancy or with doxycycline late in pregnancy.
- Data on the efficacy of treatment of mildly ill children with clarithromycin or azithromycin should not be extrapolated to adults or to patients with moderate or severe illness.
- For children with suspected RMSF, up to five courses of doxycycline may be administered with minimal risk of dental staining.
- In patients with allergy to doxycycline, desensitization should be considered.
- Once considered an alternative during pregnancy, chloramphenicol is not readily available in the United States.
- Although available in much of the world, it is less effective than doxycycline.
- Fortunately, there is little evidence to support the occurrence of tetracycline-associated adverse events in mothers (hepatotoxicity) and fetuses (staining of deciduous teeth and teratogenicity) who receive doxycycline.
9.1 Pregnancy¶
- Early pregnancy: Chloramphenicol.
- Late pregnancy: Doxycycline.
- Evaluation: Individualized.
9.2 Pediatrics¶
- Dental staining: Minimal risk with up to five courses of doxycycline.
- Extrapolation: Data on efficacy of clarithromycin or azithromycin in mildly ill children should not be extrapolated to adults or to patients with moderate or severe illness.
10. KEY PEARLS & CLINICAL TRAPS¶
- Doxycycline is the drug of choice for all rickettsial diseases.
- Immediate empirical administration of doxycycline should be strongly considered for any patient with a consistent clinical presentation in the appropriate epidemiologic setting.
- Rash appears late (day 6 or later in 20% of cases) and is absent in ~10% of cases; do not wait for rash to treat.
- Serologic tests for RMSF are usually negative at the time of presentation for medical care; treatment should not be delayed while a positive serologic result is awaited.
- Hyponatremia is a common laboratory finding (56% of RMSF cases) due to ADH secretion in response to hypovolemia.
- Thrombocytopenia is common (32–52% of RMSF cases) but DIC is rare.
- Skin biopsy with immunohistochemistry is the most useful diagnostic test during acute illness (70% sensitive, 100% specific).
- Mortality rate for RMSF is ~3–5% in postantibiotic era but higher in children (70 years).
- R. prowazekii and R. rickettsii are bioterrorism threats due to high infectivity and aerosol transmission capability.
- Eschar (tache noire) is a hallmark of tick-borne spotted fevers (RMSF, MSF, African tick-bite fever) and rickettsialpox.
- Q fever (Coxiella burnetii) is the only rickettsial agent documented to cause chronic illness.
- R. amblyommatis is the most prevalent SFG rickettsia in the United States and has been circumstantially associated with asymptomatic seroconversion in most persons and with self-limited illness in others.
10.1 Board Favorites¶
- Treat empirically without waiting for serology.
- Rash appears late; absence does not rule out RMSF.
- Hyponatremia is a key lab finding.
- Eschar is pathognomonic for tick-borne spotted fevers.
- Doxycycline is safe in pregnancy (late) and pediatrics (dental staining minimal).
- Bioterrorism threat: R. prowazekii and R. rickettsii.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
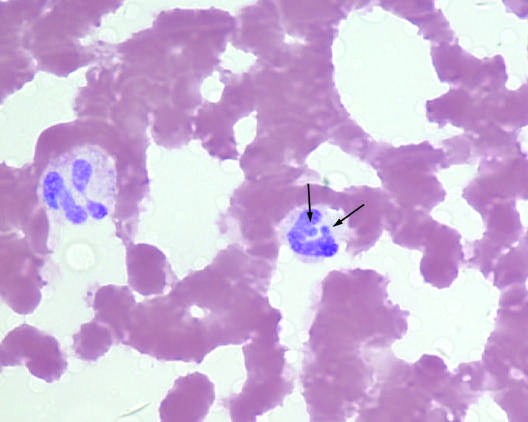
Caption: FIGURE 192-4 Peripheral-blood smear from a patient with human granulocytotropic anaplasmosis. A neutrophil contains two morulae (vacuoles filled with Anaplasma phagocytophilum). (Photo courtesy of Dr. J. Stephen Dumler.) — Peripheral-blood smear from a patient with human granulocytotropic anaplasmosis showing a neutrophil containing two morulae (vacuoles filled with Anaplasma phagocytophilum).
Figure 2¶

Caption: FIGURE 192-2 Eschar at the site of the mite bite in a patient with rickettsialpox. (Reprinted from A Krusell et al: Emerg Infect Dis 8:727, 2002. Photo obtained by Dr. Kenneth Kaye.) — Eschar at the site of the mite bite in a patient with rickettsialpox, showing a 1- to 2.5-cm painless black crusted eschar surrounded by an erythematous halo.
Figure 3¶

Caption: FIGURE 192-3 A. Papulovesicular lesions on the trunk of the patient with rickettsialpox shown in Fig. 192-2. B. Close-up of lesions from the same patient. (Reprinted from A Krusell et al: Emerg Infect Dis 8:727, 2002. Photos obtained in by Dr. Kenneth Kaye.) — Papulovesicular lesions on the trunk of a patient with rickettsialpox, showing the classic progression from macular to papulovesicular to crusts.
Figure 4¶

Caption: FIGURE 192-3 A. Papulovesicular lesions on the trunk of the patient with rickettsialpox shown in Fig. 192-2. B. Close-up of lesions from the same patient. (Reprinted from A Krusell et al: Emerg Infect Dis 8:727, 2002. Photos obtained in by Dr. Kenneth Kaye.) — Close-up of papulovesicular lesions on the trunk of a patient with rickettsialpox, demonstrating the vesicular nature of the rash.
Figure 5¶

Caption: FIGURE 192-1 A. Petechial lesions of Rocky Mountain spotted fever on the lower legs and soles of a young, previously healthy patient. B. Close-up of lesions from the is same patient. (Photos courtesy of Dr. Lindsey Baden; with permission.) — Petechial lesions of Rocky Mountain spotted fever on the lower legs and soles of a young, previously healthy patient, showing the characteristic hemorrhagic rash.
Figure 6¶
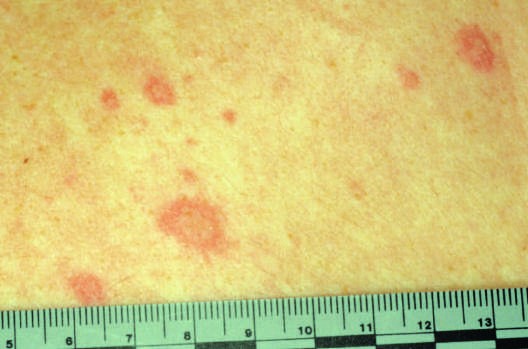
Caption: FIGURE 192-1 A. Petechial lesions of Rocky Mountain spotted fever on the lower legs and soles of a young, previously healthy patient. B. Close-up of lesions from the is same patient. (Photos courtesy of Dr. Lindsey Baden; with permission.) — Close-up of petechial lesions of Rocky Mountain spotted fever on the lower legs and soles, demonstrating the non-blanching hemorrhage at the center of the maculopapule.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.