Frontotemporal Dementia¶
Chapter 443 | Harrison's 22e · Part 13 – Neurologic Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Three major frontotemporal dementia (FTD) clinical syndromes |
| 2 | 🖼 Figure | Frontotemporal dementia syndromes are united by underlying presence of tau, TDP-43, or... |
| 3 | 🖼 Figure | Neuropathology in frontotemporal lobar degeneration (FTLD) |
RAW CONTENT¶
[PAGE 3485] Frontotemporal Dementia 3485 CHAPTER 443 one study), migraine, or cardiac arrhythmias have all been implicated. psychiatric illness. Schizophrenia is usually not difficult to distinguish Approximately one-quarter of patients experience recurrent attacks. from dementia, but occasionally the distinction can be problematic. Rare instances of permanent memory loss have been reported in Schizophrenia generally has a much earlier age of onset (second and patients with TGA-like spells, usually representing ischemic infarction third decades) than most dementing illnesses and is associated with of the hippocampus or dorsomedial thalamic nucleus bilaterally. Sei- intact memory. The delusions and hallucinations of schizophrenia are zure activity due to AD should always be suspected in this syndrome. usually more complex, bizarre, and threatening than those of demen- The ALS/parkinsonian/dementia complex of Guam is a rare degen- tia. Some chronic schizophrenics develop an unexplained progressive erative disease that has occurred in the Chamorro natives on the island dementia late in life that is not related to AD. Conversely, FTD, HD, of Guam. Individuals may have any combination of parkinsonian fea- vascular dementia, DLB, AD, or leukoencephalopathy can begin with tures, dementia, and MND. The most characteristic pathologic features schizophrenia-like features, leading to the misdiagnosis of a psychiatric are the presence of NFTs in degenerating neurons of the cortex and condition. Later age of onset, significant deficits on cognitive testing, or substantia nigra and loss of motor neurons in the spinal cord, although the presence of abnormal neuroimaging suggest a degenerative condi- recent reanalysis has shown that some patients with this illness also tion. Memory loss may also be part of a conversion disorder. In this situ- show coexisting TDP-43 pathology. Epidemiologic evidence supports ation, patients commonly complain bitterly of memory loss, but careful a possible environmental cause, such as exposure to a neurotoxin or cognitive testing either does not confirm the deficits or demonstrates an infectious agent with a long latency period. One interesting but inconsistent or unusual patterns of cognitive problems. The patient’s unproven candidate neurotoxin is the seed of the false palm tree, which behavior and “wrong” answers to questions often indicate that they Guamanians traditionally used to make flour. The amyotrophic lateral understand the question and know the correct answer. sclerosis (ALS) syndrome is no longer present in Guam, but a dement- Clouding of cognition by chronic drug or medication use, often pre- ing illness with rigidity continues to be seen. scribed by physicians, is an important cause of dementia. Sedatives, Rarely, adult-onset leukodystrophies, lysosomal storage diseases, tranquilizers, and analgesics used to treat insomnia, pain, anxiety, or and other genetic disorders can present as a dementia in middle to agitation may cause confusion, memory loss, and lethargy, especially late life. Metachromatic leukodystrophy (MLD) causes a progres- in the elderly. Discontinuation of the offending medication often sive psychiatric or dementia syndrome associated with an extensive, improves mentation. confluent frontal white matter abnormality. MLD is diagnosed by measuring reduced arylsulfatase A enzyme activity in peripheral ■ FURTHER READING white blood cells. Adult-onset presentations of adrenoleukodystrophy Andrews SJ et al: Interpretation of risk loci from genome-wide asso- have been reported in female carriers, and these patients often feature ciation studies of Alzheimer’s disease. Lancet Neurol 19:326, 2020. spinal cord and posterior white matter involvement. Adrenoleuko- Belloy ME et al: A quarter century of APOE and Alzheimer’s disease: dystrophy is diagnosed by demonstrating increased levels of plasma Progress to date and the path forward. Neuron 101:820, 2019. very-long-chain fatty acids. CADASIL (cerebral autosomal dominant Cummings J et al: Progress in pharmacologic management of neu- arteriopathy with subcortical infarcts and leukoencephalopathy) is ropsychiatric syndromes in neurodegenerative disorders: A review. another genetic syndrome associated with white matter disease, often JAMA Neurol 81:645, 2024. frontally and temporally predominant. Diagnosis is made with skin Graff-Radford J et al: New insights into atypical Alzheimer’s disease biopsy, which shows osmophilic granules in arterioles, or increasingly in the era of biomarkers. Lancet Neurol 20:222, 2021. through genetic testing for mutations in Notch 3. The neuronal ceroid Jack CR et al: Revised criteria for the diagnosis and staging of lipofuscinoses are a genetically heterogeneous group of disorders asso- Alzheimer’s disease. Nat Med 30:2121, 2024. ciated with myoclonus, seizures, vision loss, and progressive dementia. Schindler SE et al: Acceptable performance of blood biomarker tests Diagnosis is made by finding eosinophilic curvilinear inclusions within of amyloid pathology: Recommendations from the Global CEO Ini- white blood cells or neuronal tissue. tiative on Alzheimer’s Disease. Nat Rev Neurol 20:426, 2024. Psychogenic amnesia for personally important memories can be Sims JR et al: Donanemab in early symptomatic Alzheimer disease: seen. Whether this results from deliberate avoidance of unpleasant The TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA 330:512, memories, outright malingering, or unconscious repression remains 2023. unknown and probably depends on the patient. Event-specific amnesia Van Dyck CH et al: Lecanemab in early Alzheimer’s disease. N Engl J is more likely to occur after violent crimes such as homicide of a close Med 388:9, 2023. relative or friend or sexual abuse. It may develop in association with severe drug or alcohol intoxication and sometimes with schizophrenia. More prolonged psychogenic amnesia occurs in fugue states that also commonly follow severe emotional stress. The patient with a fugue state suffers from a sudden loss of personal identity and may be found wandering far from home. In contrast to neurologic amnesia, fugue states are associated with amnesia for personal identity and events closely associated with the personal past. At the same time, memory for other 443 Frontotemporal recent events and the ability to learn and use new information are pre- served. The episodes usually last hours or days and occasionally weeks Dementia or months while the patient takes on a new identity. On recovery, there is a residual amnesia gap for the period of the fugue. Very rarely does William W. Seeley, Bruce L. Miller selective loss of autobiographic information reflect a focal injury to the brain areas involved with these functions. Psychiatric diseases may mimic dementia. Severely depressed or anxious individuals may appear demented, a phenomenon sometimes Frontotemporal dementia (FTD) refers to a group of clinical syndromes called pseudodementia. Memory and language are usually intact when united by their links to underlying frontotemporal lobar degenera- carefully tested, and a significant memory disturbance usually suggests tion (FTLD) pathology. FTD, like the other major neurodegenerative an underlying dementia, even if the patient is depressed. Patients in this diseases, is considered a disease of abnormal protein aggregation, with condition may feel confused and unable to accomplish routine tasks. either tau or transactive response DNA-binding protein of 43 kDa Vegetative symptoms, such as insomnia, lack of energy, poor appetite, (TDP-43) implicated in most cases. FTD most often begins in the fifth and concern with bowel function, are common. Onset is often more to seventh decades of life and is nearly as prevalent as Alzheimer’s abrupt, and the psychosocial milieu may suggest prominent reasons disease (AD) in this age group. Early studies suggested that FTD may for depression. Such patients respond to treatment of
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
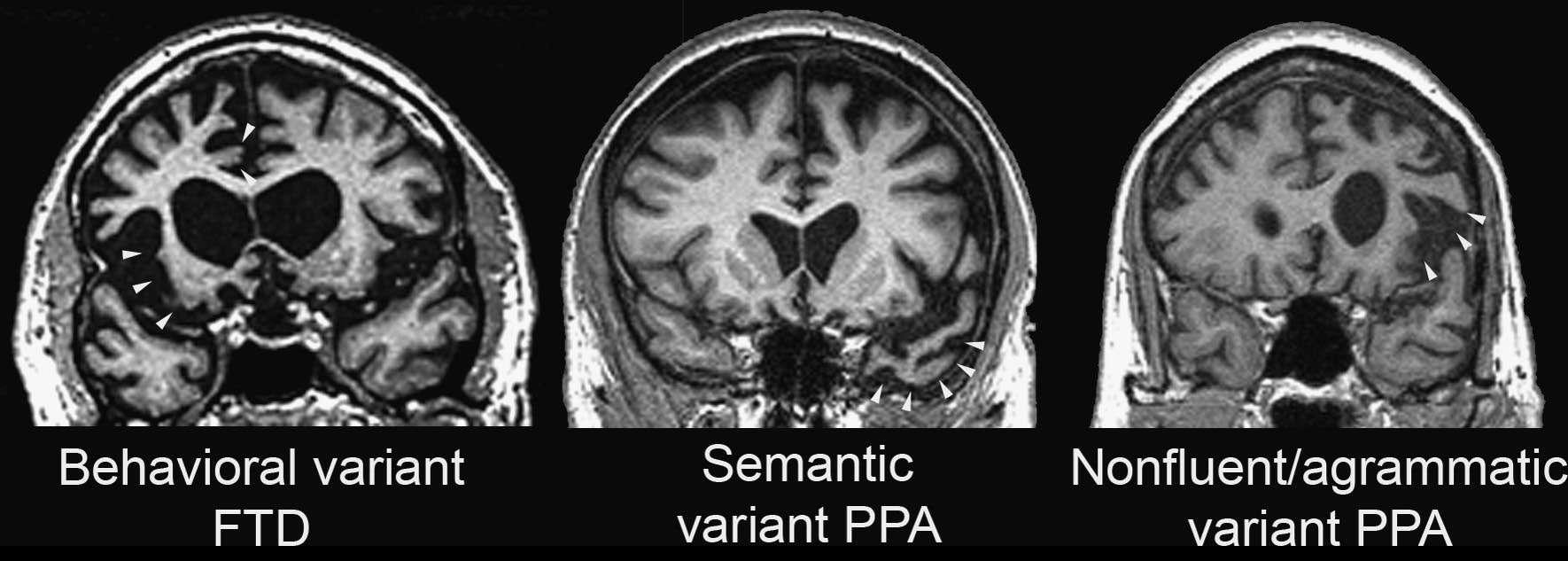
Caption: FIGURE 443-1 Three major frontotemporal dementia (FTD) clinical syndromes. Coronal sections from representative patients with behavioral variant FTD (left) and the agrammatic (right) variants of primary progressive aphasia (PPA). Areas of early and are highlighted (white arrowheads). The behavioral variant features anterior spreading to orbital and dorsolateral prefrontal cortex. Semantic variant PPA shows more often on the left. Nonfluent/agrammatic variant PPA is associated with dominant insula degeneration.
Figure 2¶

Caption: FIGURE 443-2 Frontotemporal dementia syndromes are united by underlying presence of tau, TDP-43, or FUS-containing inclusions in neurons and glia. Correlations shading. Despite improvements in clinical syndromic diagnosis, a small percentage of disease neuropathology at autopsy (gray shading). aFTLD-U, atypical frontotemporal disease; BIBD, basophilic inclusion body disease; bvFTD, behavioral variant chronic traumatic encephalopathy; FET, FUS, Ewing sarcoma protein, TAF-15 family of frontotemporal dementia with parkinsonism linked to chromosome 17; FUS, fused in agrammatic variant primary progressive aphasia; NIBD, neurofilament inclusion body supranuclear palsy; PSP-RS, progressive supranuclear palsy–Richardson syndrome; in the pathogenesis of FTLD-TDP and FTLD-FET. As with tau, the
Figure 3¶
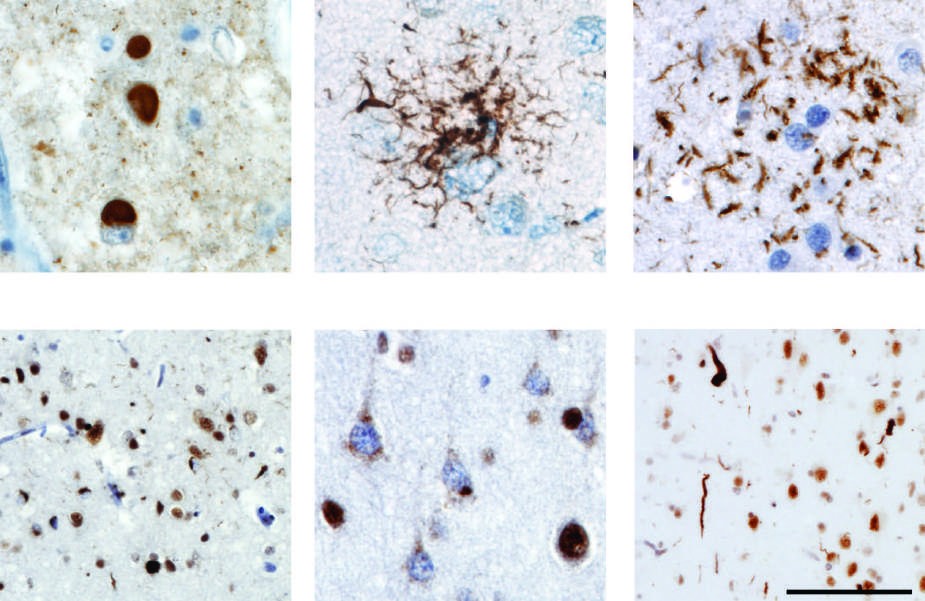
Caption: FIGURE 443-3 Neuropathology in frontotemporal lobar degeneration (FTLD). immunohistochemistry reveals characteristic lesions in each of the major histopathologic in progressive supranuclear palsy; C. an astrocytic plaque in corticobasal degeneration; neuropil threads in FTLD-TDP, type A; E. diffuse/granular neuronal cytoplasmic tortuous dystrophic neurites in FTLD-TDP, type C. TDP can be seen within the nucleus in in FTLD-TDP. Immunostains are 3-repeat tau (A), phospho-tau (B and C), and TDP-43 (D–F). represents 50 μm in A, B, C, and E and 100 μm in D and F. structures. The most prominent involvement is in the subthalamic nucleus, globus pallidus, substantia nigra, periaqueductal gray, tectum, oculomotor nuclei, pontine nuclei, and dentate nucleus of cerebellum. as
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.