Chapter 256: Paroxysmal Supraventricular Tachycardias¶
Chapter 256 | Part 6: Disorders of the Cardiovascular System II · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- AV nodal reentry tachycardia (AVNRT) is the most common form of paroxysmal supraventricular tachycardia (PSVT), representing approximately 60% of cases referred for catheter ablation.
- Wolff-Parkinson-White (WPW) syndrome is defined as a preexcited QRS during sinus rhythm and episodes of PSVT; concealed accessory pathways allow only retrograde conduction.
- Acute management of stable narrow QRS PSVT utilizes vagal maneuvers, adenosine, or AV nodal blocking agents (beta blockers, calcium channel blockers).
- Preexcited atrial fibrillation with R-R intervals <250 ms is associated with a higher risk of ventricular fibrillation and sudden death.
- Catheter ablation of the slow AV nodal pathway is curative in >95% of patients with AVNRT, with a major risk of AV block requiring permanent pacemaker implantation in <1%.
- Catheter ablation targeting the AT focus is effective in >80% of patients and is recommended for recurrent symptomatic atrial tachycardia or incessant AT causing tachycardia-induced cardiomyopathy.
- Junctional ectopic tachycardia (JET) is rare in adults but frequently encountered as an incessant tachycardia in children, often in the perioperative period of surgery for congenital heart disease.
- Patients with preexcitation but no arrhythmia symptoms have a risk of sudden death estimated to be 1 per 1000 patient-years in adults, but ~2 per 1000 patient-years in children.
- Administration of AV nodal–blocking agents (verapamil, diltiazem, beta blockers, adenosine, amiodarone) is contraindicated during preexcited AF.
- Tachycardia-induced cardiomyopathy can occur with incessant tachycardia; anticoagulation indications for atrial tachycardia are unclear but not considered equivalent to atrial fibrillation.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification of SVT
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Accessory Pathway Locations
- 3.2 Wolff-Parkinson-White (WPW) Syndrome
- 4. CLINICAL FEATURES
- 4.1 Symptoms and Signs
- 4.2 Hemodynamic Instability
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Distinguishing Features
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria
- 6.2 Diagnostic Algorithm
- 7. MANAGEMENT & TREATMENT
- 7.1 Acute Management
- 7.2 Chronic Management
- 7.3 Preexcited AF Management
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Tachycardia-Induced Cardiomyopathy
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pediatric Considerations
- 9.2 Elderly Considerations
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
- Sustained supraventricular tachycardias (SVTs) depend on the atrioventricular (AV) node.
- These include AV nodal reentry tachycardia (AVNRT), junctional tachycardia, AV reciprocating tachycardia (AVRT) utilizing an accessory pathway, and a group of additional various SVTs that involve an accessory pathway.
- The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and technically includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, AVNRT, and atrial fibrillation.
- For the purposes of describing an organized approach to diagnosis and treatment of SVT, a separate discussion for these non-AV nodal–dependent SVTs is provided.
- Paroxysmal supraventricular tachycardias (PSVTs) are rapid heart rates originating above the ventricles.
- The mechanism of SVT is often reentry involving the AV node and the perinodal atrium, made possible by the existence of multiple pathways for conduction from the atrium into the AV node that are capable of conduction in two directions.
- Accessory pathways (APs) are abnormal connections that allow conduction between the atrium and ventricles across the AV ring.
- APs are present from birth and are due to failure of complete partitioning of atrium and ventricle by the fibrous AV rings.
- WPW syndrome is defined as a preexcited QRS during sinus rhythm and episodes of PSVT.
1.1 Classification of SVT¶
- AV nodal reentry tachycardia (AVNRT).
- Junctional tachycardia.
- AV reciprocating tachycardia (AVRT) utilizing an accessory pathway.
- Atrial tachycardia (AT).
- Atrial flutter.
- Atrial fibrillation.
- Preexcited tachycardias (WPW syndrome).
- Concealed accessory pathways.
2. EPIDEMIOLOGY¶
- Accessory pathways occur in 1 in 1500–2000 people.
- APs are associated with a variety of arrhythmias including narrow-complex PSVT, wide-complex tachycardias, and, rarely, sudden death.
- Most patients have structurally normal hearts.
- APs are associated with Ebstein’s anomaly of the tricuspid valve and forms of hypertrophic cardiomyopathy including PRKAG2 mutations, Danon’s disease, and Fabry’s disease.
- AVNRT most commonly manifests in the second to fourth decades of life, more often in women.
- Adults who have preexcitation but no arrhythmia symptoms have a risk of sudden death estimated to be 1 per 1000 patient-years.
- Children are at greater risk of sudden death, ~2 per 1000 patient-years.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- AVNRT mechanism is reentry involving the AV node and the perinodal atrium.
- Multiple pathways for conduction from the atrium into the AV node are capable of conduction in two directions.
- Most forms of AVNRT utilize a slowly conducting AV nodal pathway (right inferior extension) that extends from the compact AV node near the His bundle, inferiorly along the tricuspid valve annulus to the floor of the coronary sinus.
- The reentry wavefront propagates up this slowly conducting pathway to the compact AV node and then exits the fast pathway at the top of the AV node.
- The path back to the atrium is via the fast pathway at the top of the AV node.
- The path back to the atrium is via the fast pathway at the top of the AV node.
- More unusual forms of AVNRT utilize a left inferior extension that connects to the compact AV node through the roof of the coronary sinus or, in extremely rare cases, directly from the mitral valve annulus avoiding the coronary sinus musculature altogether.
- In typical forms, the conduction time from the compact AV node region to the atrium is similar to that from the compact node to the His bundle and ventricles, such that atrial activation occurs at about the same time as ventricular activation.
- The P wave is therefore inscribed during, slightly before, or slightly after the QRS and can be difficult to discern.
- Accessory pathways (APs) are abnormal connections that allow conduction between the atrium and ventricles across the AV ring.
- APs occur across either an AV valve annulus or the septum, most frequently between the left atrium and free wall of the left ventricle, followed by posteroseptal, right free wall, and anteroseptal locations.
- If the impulse from the sinus node conducts through the AP to the ventricle (antegrade) before the impulse conducts through the AV node and His bundle, then the ventricles are preexcited during sinus rhythm.
- Concealed APs allow only retrograde conduction, from ventricle to atrium, so no preexcitation is present during sinus rhythm, but SVT can occur.
- Fasciculoventricular connections between the His bundle and ventricular septum produce preexcitation but do not cause arrhythmia, probably because the circuit is too short to promote reentry.
- Atriofascicular pathways, also known as Mahaim fibers, probably represent a duplicate AV node and His-Purkinje system that connect the right atrium to fascicles of the right bundle branch and produce a wide-complex tachycardia having a left bundle branch block configuration.
- Preexcitation due to an AP at the diaphragmatic surface of the heart, typically in the paraseptal region, produces delta waves that are negative in leads III and aVF.
3.1 Accessory Pathway Locations¶
- Right-sided pathways preexcite the right ventricle, producing a left bundle branch block–like configuration in lead V, and often create marked preexcitation because of their relatively close proximity of the AP to the sinus node.
- Left-sided pathways preexcite the left ventricle and may produce a right bundle branch–like configuration in lead V and a negative delta wave in aVL, indicating initial depolarization of the lateral portion of the left ventricle that can mimic Q waves of lateral wall infarction.
- Because of the relatively large distance between the sinus node and left free wall APs, preexcitation may be minimal or absent on 12-lead ECG.
- Preexcitation due to an AP at the diaphragmatic surface of the heart, typically in the paraseptal region, produces delta waves that are negative in leads III and aVF.
Table 1 — Accessory Pathway Locations and ECG Morphology¶
| Pathway Location | Preexcitation Characteristics | ECG Findings |
|---|---|---|
| Right-sided | Preexcites right ventricle | Left bundle branch block–like configuration in lead V; marked preexcitation |
| Left-sided | Preexcites left ventricle | Right bundle branch–like configuration in lead V; negative delta wave in aVL |
| Diaphragmatic surface (paraseptal) | Preexcitation | Delta waves negative in leads III and aVF |
3.2 Wolff-Parkinson-White (WPW) Syndrome¶
- WPW syndrome is defined as a preexcited QRS during sinus rhythm and episodes of PSVT.
- There are a number of variations of APs that may not cause preexcitation and/or arrhythmias.
- Concealed APs allow only retrograde conduction, from ventricle to atrium, so no preexcitation is present during sinus rhythm, but SVT can occur.
- Orthodromic AV reentry utilizes retrograde conduction over the AP and antegrade conduction over the AV node.
- Antidromic AV reentry utilizes retrograde conduction over the AV node and antegrade conduction over the AP.
4. CLINICAL FEATURES¶
- AVNRT is usually well tolerated, but rapid tachycardia, particularly in the elderly, may cause angina, pulmonary edema, hypotension, or syncope.
- It is not usually associated with structural heart disease.
- In patients without associated heart disease, AVNRT is not a life-threatening arrhythmia; however, it may cause significant symptoms.
- The rate can vary with sympathetic tone through its effect on the conduction time of AV nodal tissues.
- Simultaneous atrial and ventricular contraction results in atrial contraction against a closed tricuspid valve, producing a cannon A wave visible in the jugular venous pulse often perceived as a fluttering sensation in the neck.
- Elevated venous pressures may also lead to release of natriuretic peptides that cause post-tachycardia diuresis.
- Junctional ectopic tachycardia (JET) presents as a narrow QRS tachycardia, often with ventriculoatrial (VA) block, such that AV dissociation is present.
- JET can occur as a manifestation of increased adrenergic tone and may be seen after administration of isoproterenol, particularly after catheter ablation in the perinodal region.
- It may also occur for a short period of time after ablation for AVNRT.
- Accelerated junctional rhythm is a junctional automatic rhythm between 50 and 100 beats/min.
- Initiation may occur with gradual acceleration in rate, suggesting an automatic focus, or after a premature ventricular contraction, suggesting a focus of triggered automaticity.
- VA conduction is usually present, with P-wave morphology and timing such that it resembles AVNRT at a slow rate.
- It can be related to increased sympathetic tone and may produce palpitations.
- It usually does not require specific therapy.
- Preexcited tachycardia occurs when the ventricles are activated by antegrade conduction over the AP.
- The wide QRS complex is produced entirely via ventricular excitation over the AP because there is no contribution of ventricular activation over more rapidly conducting specialized His-Purkinje fibers.
- This tachycardia is often indistinguishable from monomorphic ventricular tachycardia.
- The presence of preexcitation in sinus rhythm suggests the diagnosis.
- Preexcited AF presents as a wide-complex, very irregular rhythm.
- During AF, the ventricular rate is determined by the conduction properties of the AP and AV node.
- The QRS complex can appear quite bizarre and change on a beat-to-beat basis due to the variability in the degree of fusion from activation over the AV node and AP, or all beats may be due to conduction over the AP.
- Ventricular activation from the Purkinje system may depolarize the ventricular aspect of the AP and prevent atrial wavefront conduction over the AP.
- Slowing AV nodal conduction without slowing AP conduction can thereby facilitate AP conduction and dangerously accelerate the ventricular rate.
4.1 Symptoms and Signs¶
- Palpitations.
- Angina (in elderly).
- Pulmonary edema (in elderly).
- Hypotension (in elderly).
- Syncope (in elderly).
- Cannon A wave visible in the jugular venous pulse.
- Fluttering sensation in the neck.
4.2 Hemodynamic Instability¶
- Hypotension with unconsciousness.
- Respiratory distress.
- QRS-synchronous direct current cardioversion is warranted.
5. DIFFERENTIAL DIAGNOSIS¶
- AVNRT vs. AT vs. Atrial Flutter.
- AVNRT vs. WPW vs. Concealed AP.
- Narrow QRS PSVT vs. Wide QRS Tachycardia.
- Monomorphic Ventricular Tachycardia vs. Preexcited Tachycardia.
- Orthodromic AV reentry vs. Atypical AV nodal reentry or AT.
- Permanent junctional reciprocating tachycardia (PJRT) vs. Orthodromic AV reentry.
5.1 Distinguishing Features¶
- AVNRT: P waves at end of QRS, negative in inferior limb leads.
- AT: Discrete P waves with isoelectric segments between, may fall coincident with QRS.
- Atrial Flutter: Sawtooth waves, variable block.
- WPW: Preexcited QRS during sinus rhythm, delta waves.
- Concealed AP: No preexcitation during sinus rhythm, SVT episodes.
- PJRT: Long R-P interval, P waves negative in inferior limb leads.
- Mahaim: Wide-complex tachycardia with left bundle branch block configuration.
- Fasciculoventricular: Preexcitation without arrhythmia.
6. INVESTIGATIONS & DIAGNOSIS¶
- Continuous ECG monitoring should be implemented.
- A 12-lead ECG should always be obtained when possible.
- This may be useful in determining the mechanism.
- In the presence of hypotension with unconsciousness or respiratory distress, QRS-synchronous direct current cardioversion is warranted.
- An echocardiogram is reasonable to exclude Ebstein’s anomaly, forms of hypertrophic cardiomyopathy that can be associated with APs, or tachycardia-mediated cardiomyopathy.
- An invasive electrophysiology study is recommended to assess whether the pathway can support dangerously rapid heart rates if AF were to occur.
- It is usually combined with potentially curative catheter ablation.
- Ambulatory monitoring or exercise testing is often used to gain reassurance that the AP is not high risk.
- Evaluating for abrupt loss of conduction (preexcitation) at physiologic heart rates consistent with a low-risk pathway, but this is not completely reliable.
- Gradual loss of AP conduction with increased sympathetic tone does not reliably indicate low risk since this can occur as AV nodal conduction time shortens, and therefore, the possibility of rapid antegrade AP conduction is not excluded definitively.
- Carotid sinus massage is reasonable provided the risk of carotid vascular disease is low, as indicated by absence of carotid bruits and no prior history of stroke.
- A Valsalva maneuver should be attempted in cooperative individuals, and if effective, the patient can be taught to perform this maneuver as needed.
6.1 Diagnostic Criteria¶
- WPW Syndrome: Preexcited QRS during sinus rhythm and episodes of PSVT.
- AVNRT: P waves at end of QRS, negative in inferior limb leads.
- AT: Discrete P waves with isoelectric segments between.
- JET: Narrow QRS tachycardia, often with VA block.
- PJRT: Long R-P interval, P waves negative in inferior limb leads.
- Concealed AP: No preexcitation during sinus rhythm.
6.2 Diagnostic Algorithm¶
- Step 1: Obtain 12-lead ECG.
- Step 2: Assess for preexcitation (delta waves, short PR).
- Step 3: If preexcitation present, assess for AF or PSVT.
- Step 4: If stable, attempt vagal maneuvers or adenosine.
- Step 5: If unstable, perform cardioversion.
- Step 6: Consider invasive electrophysiology study for high-risk APs or recurrent symptoms.
7. MANAGEMENT & TREATMENT¶
- Acute management of sudden-onset, sustained AT is the same as for other forms of PSVT.
- The response to pharmacologic therapy is variable, likely depending on the mechanism.
- For AT due to reentry, administration of adenosine or vagal maneuvers may transiently increase AV block without terminating tachycardia.
- Some ATs terminate with a sufficient dose of adenosine, consistent with triggered activity as the mechanism.
- Cardioversion can be effective in some but fails in others because of immediate recurrence, suggesting automaticity as the mechanism in these cases.
- Beta blockers and calcium channel blockers may slow the ventricular rate by increasing AV block, which can improve tolerance of the arrhythmias, but large doses are sometimes required.
- Potential precipitating factors and intercurrent illness should be sought and corrected.
- Underlying heart disease should be considered and excluded.
- For patients with recurrent episodes, beta blockers, calcium channel blockers such as diltiazem or verapamil, and antiarrhythmic drugs such as flecainide, propafenone, disopyramide, sotalol, and amiodarone can be effective.
- Potential toxicities and adverse effects often warrant avoidance of long-term use.
- Catheter ablation targeting the AT focus is effective in >80% of patients and is recommended for recurrent symptomatic AT when drugs fail or are not desired or for incessant AT causing tachycardia-induced cardiomyopathy.
- Acute management of orthodromic AV reentry is discussed below for PSVT.
- Patients with WPW syndrome may have wide-complex tachycardia due to antidromic AV reentry, orthodromic AV with bundle branch block, or a preexcited tachycardia, and treatment depends on the underlying rhythm.
- Initial patient evaluation should include assessment for aggravating factors, including intercurrent illness and factors that increase sympathetic tone.
- Examination should focus on excluding underlying heart disease.
- An echocardiogram is reasonable to exclude Ebstein’s anomaly, forms of hypertrophic cardiomyopathy that can be associated with APs, or tachycardia-mediated cardiomyopathy.
- Patients with preexcitation who have symptoms of arrhythmia are at risk for developing AF and sudden death if they have an AP that allows rapid antegrade conduction.
- The risk of cardiac arrest is in the range of 2 per 1000 patients in adults but is likely greater in children.
- An invasive electrophysiology study is recommended to assess whether the pathway can support dangerously rapid heart rates if AF were to occur, and it is usually combined with potentially curative catheter ablation.
- Catheter ablation is warranted for recurrent arrhythmias when drugs are ineffective, not tolerated, or not desired by the patient.
- Efficacy is in the range of 95% depending on the location of the AP.
- Serious complications occur in 95% of patients.
- The major risk is AV block requiring permanent pacemaker implantation, which occurs in <1% of patients.
- Reassurance and instruction as to how to perform the Valsalva maneuver or other vagal nerve–stimulating maneuvers to terminate episodes are sufficient for many patients.
- Administration of an oral beta blocker, verapamil, or diltiazem at the onset of an episode can be used to facilitate termination.
- Chronic therapy with these medications or flecainide is an option if prophylactic therapy is needed.
7.1 Acute Management¶
- Vagal maneuvers.
- Adenosine.
- Beta blockers.
- Calcium channel blockers (verapamil, diltiazem).
- Cardioversion (if unstable).
Table 2 — Management of Focal Atrial Tachycardia¶
| Intervention | Indication | Efficacy | Notes |
|---|---|---|---|
| Adenosine | AT due to reentry | Variable | May transiently increase AV block without terminating tachycardia |
| Vagal maneuvers | Stable PSVT | Variable | First line for stable patients |
| Beta blockers / CCB | Recurrent episodes | Effective | May slow ventricular rate by increasing AV block |
| Catheter ablation | Recurrent symptomatic AT | >80% | Recommended when drugs fail or for incessant AT |
7.2 Chronic Management¶
- Beta blockers.
- Calcium channel blockers (diltiazem, verapamil).
- Antiarrhythmic drugs (flecainide, propafenone, disopyramide, sotalol, amiodarone).
- Catheter ablation (curative in >95% for AVNRT).
- Vagal maneuvers (Valsalva).
- Oral beta blocker, verapamil, or diltiazem at onset of episode.
7.3 Preexcited AF Management¶
- Administration of AV nodal–blocking agents (verapamil, diltiazem, beta blockers, adenosine, amiodarone) is contraindicated during preexcited AF.
- Rapid preexcited tachycardia should be treated with electrical cardioversion or intravenous procainamide or ibutilide.
- These agents may terminate the arrhythmia or slow the ventricular rate.
8. PROGNOSIS & COMPLICATIONS¶
- AVNRT is not usually associated with structural heart disease.
- In patients without associated heart disease, AVNRT is not a life-threatening arrhythmia; however, it may cause significant symptoms.
- Tachycardia-induced cardiomyopathy can occur.
- Preexcited AF presents as a wide-complex, very irregular rhythm.
- Approximately 25% of APs causing preexcitation allow minimum R-to-R intervals of <250 ms during AF and are associated with a higher risk of inducing ventricular fibrillation and sudden death.
- The risk of cardiac arrest is in the range of 2 per 1000 patients in adults but is likely greater in children.
- Procedure mortality is <1 in 1000 patients.
- Serious complications occur in <3% of patients but can include AV block, cardiac tamponade, thromboembolism, coronary artery injury, and vascular access complications.
- The risk of AV block is higher when the AP is located near the AV node and/or His bundle, in the so-called anteroseptal or mid-septal locations.
8.1 Tachycardia-Induced Cardiomyopathy¶
- Can occur with incessant AT.
- Requires cessation of tachycardia.
- Anticoagulation indications for atrial tachycardia are unclear but not considered equivalent to atrial fibrillation.
9. SPECIAL CONSIDERATIONS¶
- Children are at greater risk of sudden death, ~2 per 1000 patient-years.
- JET is rare in adults and more frequently encountered as an incessant tachycardia in children, often in the perioperative period of surgery for congenital heart disease.
- Adults who have preexcitation but no arrhythmia symptoms have a risk of sudden death estimated to be 1 per 1000 patient-years.
- Routine follow-up without therapy is reasonable in others.
- Elderly: Rapid tachycardia may cause angina, pulmonary edema, hypotension, or syncope.
9.1 Pediatric Considerations¶
- JET is more frequently encountered in children.
- Children are at greater risk of sudden death.
- Ambulatory monitoring or exercise testing is often used to gain reassurance that the AP is not high risk.
9.2 Elderly Considerations¶
- Rapid tachycardia may cause angina.
- Pulmonary edema.
- Hypotension.
- Syncope.
10. KEY PEARLS & CLINICAL TRAPS¶
- AVNRT is the most common form of PSVT.
- WPW syndrome is defined as a preexcited QRS during sinus rhythm and episodes of PSVT.
- Preexcited AF with R-R 95% of patients with AVNRT.
- Catheter ablation targeting AT focus is effective in >80% of patients.
- Administration of AV nodal–blocking agents is contraindicated during preexcited AF.
- Vagal maneuvers are first line for stable PSVT.
- Tachycardia-induced cardiomyopathy can occur with incessant tachycardia.
- Concealed APs allow only retrograde conduction, so no preexcitation is present during sinus rhythm.
- Gradual loss of AP conduction with increased sympathetic tone does not reliably indicate low risk.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
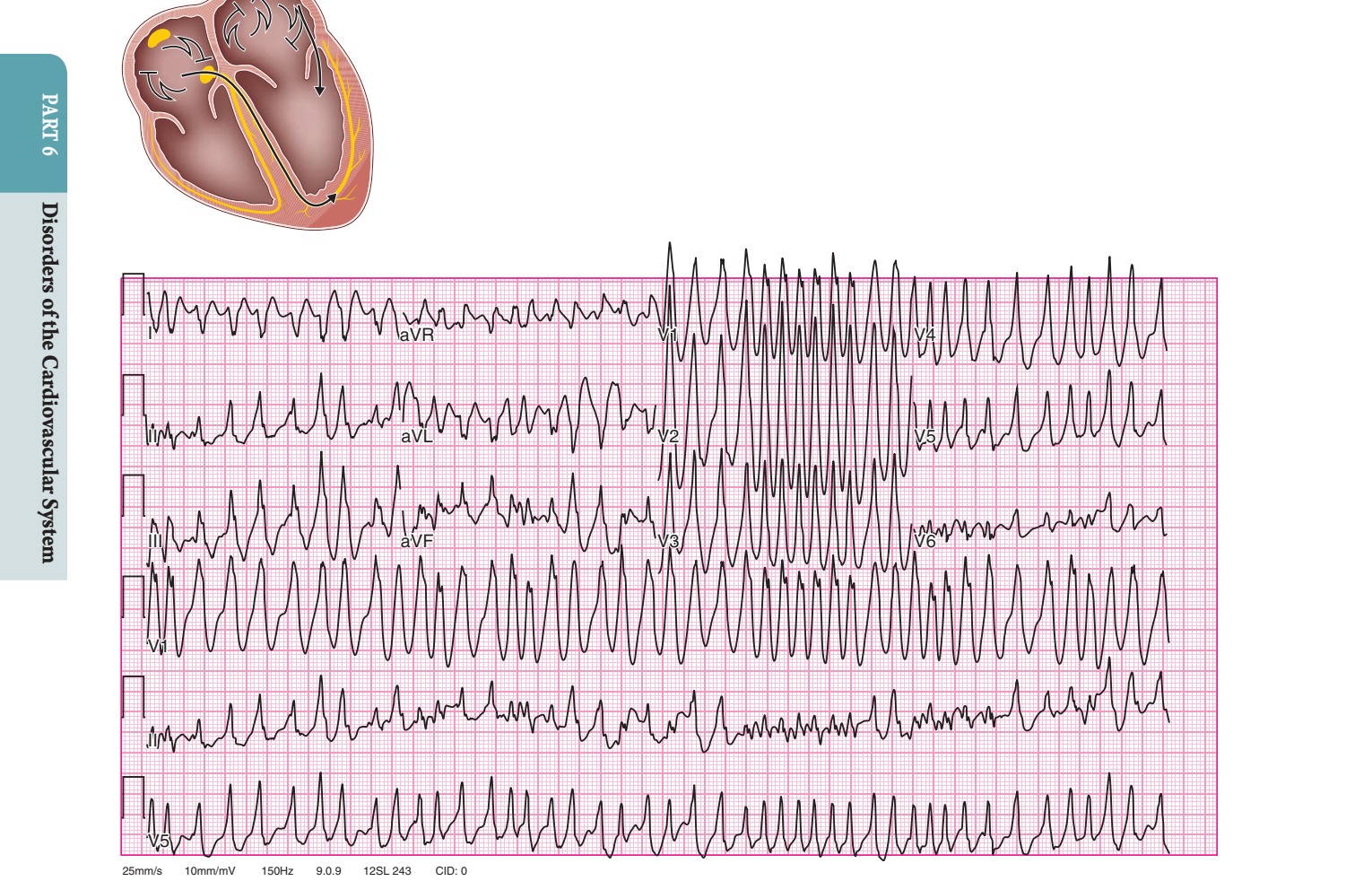
Caption: FIGURE 256-5 Preexcited atrial fibrillation (AF) due to conduction over a left free complexes that represent fusion between conduction over the atrioventricular node and left in this case, indicate a risk of sudden death with this arrhythmia.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 256-3 Wolff-Parkinson-White (WPW) syndrome. A. A 12-lead electrocardiogram in sinus rhythm (SR) of a patient with WPW demonstrating short P-R interval, delta waves, and widened QRS complex. This patient had an anteroseptal location of the accessory pathway (AP). B. Orthodromic atrioventricular (AV) reentry in a patient with WPW syndrome using a posteroseptal AP. Note the P waves in the ST segment (arrows) seen in lead III and normal appearance of QRS of complex. C. Three most common rhythms associated with WPW syndrome: sinus rhythm demonstrating antegrade conduction over the AP and AV node; orthodromic AV reentry tachycardia (AVRT) using retrograde conduction over the AP and antegrade conduction over the AV node; and antidromic AVRT using retrograde conduction over the AV node and antegrade conduction over the AP. — Figure 255-2: Focal atrial tachycardia. Surface 12-lead electrocardiogram showing focal intermittent atrial tachycardia with discrete P waves and isoelectric segments, and electroanatomic map of the anterior interatrial septum showing a focal early site (red) with ablation lesions.
Figure 2¶

Caption: FIGURE 256-3 Wolff-Parkinson-White (WPW) syndrome. A. A 12-lead electrocardiogram in sinus rhythm (SR) of a patient with WPW demonstrating short P-R interval, delta waves, and widened QRS complex. This patient had an anteroseptal location of the accessory pathway (AP). B. Orthodromic atrioventricular (AV) reentry in a patient with WPW syndrome using a posteroseptal AP. Note the P waves in the ST segment (arrows) seen in lead III and normal appearance of QRS of complex. C. Three most common rhythms associated with WPW syndrome: sinus rhythm demonstrating antegrade conduction over the AP and AV node; orthodromic AV reentry tachycardia (AVRT) using retrograde conduction over the AP and antegrade conduction over the AV node; and antidromic AVRT using retrograde conduction over the AV node and antegrade conduction over the AP. — Figure 255-3: Clinical approach and treatment algorithm for management of focal atrial tachycardia. Flowchart showing decision nodes for adenosine, cardioversion, calcium channel blockers, beta blockers, antiarrhythmic therapy, and catheter ablation.
Figure 3¶

Caption: FIGURE 255-2 Focal atrial tachycardia. In the right panel, a surface 12-lead isoelectric segments between, as well as the sinus rhythm. The left panel shows an interatrial septum, as viewed in an anterior-posterior (AP) view of the left atrium local electrical activation during each tachycardia atrial activation, showing a focal demonstrating activation of the atrium dispersing from this focal site. Of note, the pink (Adapted from J Brugada et al: 2019 ESC Guidelines for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J every other P wave may fall coincident with the QRS. Maneuvers that increase AV block, such as carotid sinus massage, Valsalva maneuver, or administration of AV nodal–blocking agents, such as adenosine, are — Figure 256-1: Atrioventricular (AV) node reentry. Stylized version of the AV nodal reentry circuit within the triangle of Koch involving AV node and its extensions along with perinodal atrial tissue.
Figure 4¶

Caption: FIGURE 256-1 Atrioventricular (AV) node reentry. A. Leads II and V are shown. P waves 1 the impression of S waves in the inferior limb leads II, III, and aVF and an R′ in lead 1 (see Fig. 254-1) that involves AV node and its extensions along with perinodal atrial pathway, termed preexcited tachycardias. The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and techni- cally includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, and atrial fibrillation; however, for the purposes of describing an orga- nized approach to diagnosis and treatment of SVT, a separate discus- sion for these non-AV nodal–dependent SVTs are discussed elsewhere. — Figure 256-2: Atrioventricular nodal reentry tachycardia with retrograde P waves before and after adenosine termination. ECG leads showing P waves visible at the end of the QRS complex and negative in lead II.
Figure 5¶

Caption: FIGURE 256-1 Atrioventricular (AV) node reentry. A. Leads II and V are shown. P waves 1 the impression of S waves in the inferior limb leads II, III, and aVF and an R′ in lead 1 (see Fig. 254-1) that involves AV node and its extensions along with perinodal atrial pathway, termed preexcited tachycardias. The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and techni- cally includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, and atrial fibrillation; however, for the purposes of describing an orga- nized approach to diagnosis and treatment of SVT, a separate discus- sion for these non-AV nodal–dependent SVTs are discussed elsewhere. — Figure 256-3: Wolff-Parkinson-White (WPW) syndrome. 12-lead electrocardiogram in sinus rhythm demonstrating short P-R interval, delta waves, and widened QRS complex; orthodromic AV reentry; and antidromic AV reentry.
Figure 6¶

Caption: FIGURE 256-1 Atrioventricular (AV) node reentry. A. Leads II and V are shown. P waves 1 the impression of S waves in the inferior limb leads II, III, and aVF and an R′ in lead 1 (see Fig. 254-1) that involves AV node and its extensions along with perinodal atrial pathway, termed preexcited tachycardias. The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and techni- cally includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, and atrial fibrillation; however, for the purposes of describing an orga- nized approach to diagnosis and treatment of SVT, a separate discus- sion for these non-AV nodal–dependent SVTs are discussed elsewhere. — Figure 256-4: Potential locations for accessory pathways in patients with Wolff-Parkinson-White syndrome and typical QRS appearance of delta waves that can mimic underlying structural heart disease such as myocardial infarction of bundle branch block.
Figure 7¶

Caption: FIGURE 256-1 Atrioventricular (AV) node reentry. A. Leads II and V are shown. P waves 1 the impression of S waves in the inferior limb leads II, III, and aVF and an R′ in lead 1 (see Fig. 254-1) that involves AV node and its extensions along with perinodal atrial pathway, termed preexcited tachycardias. The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and techni- cally includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, and atrial fibrillation; however, for the purposes of describing an orga- nized approach to diagnosis and treatment of SVT, a separate discus- sion for these non-AV nodal–dependent SVTs are discussed elsewhere. — Figure 256-5: Preexcited atrial fibrillation (AF) due to conduction over a left free wall accessory pathway (AP). Electrocardiogram showing rapid irregular QRS complexes representing fusion between conduction over the AV node and left free wall AP.
Figure 8¶

Caption: FIGURE 256-4 Potential locations for accessory pathways in patients with Wolff- Parkinson-White syndrome and typical QRS appearance of delta waves that can mimic underlying structural heart disease such as myocardial infraction of bundle branch block. AV, aortic valve; MV, mitral valve; PV, pulmonary valve; TV, tricuspid valve. to can occur. Other unusual forms of APs exist. Fasciculoventricular connections between the His bundle and ventricular septum produce preexcitation but do not cause arrhythmia, probably because the circuit — Figure 256-6: AV block with only transient slowing of tachycardia exposing ongoing P waves, indicating AT or atrial flutter as the mechanism. ECG tracing demonstrating the diagnostic utility of AV nodal blockade.
Figure 9¶

Caption: FIGURE 256-4 Potential locations for accessory pathways in patients with Wolff- Parkinson-White syndrome and typical QRS appearance of delta waves that can mimic underlying structural heart disease such as myocardial infraction of bundle branch block. AV, aortic valve; MV, mitral valve; PV, pulmonary valve; TV, tricuspid valve. to can occur. Other unusual forms of APs exist. Fasciculoventricular connections between the His bundle and ventricular septum produce preexcitation but do not cause arrhythmia, probably because the circuit — Figure 256-7: Typical AVNRT ECG. Surface ECG showing P waves at the end of the QRS complex, negative in inferior limb leads, and pseudo-r' in lead V.
Figure 10¶

Caption: FIGURE 256-4 Potential locations for accessory pathways in patients with Wolff- Parkinson-White syndrome and typical QRS appearance of delta waves that can mimic underlying structural heart disease such as myocardial infraction of bundle branch block. AV, aortic valve; MV, mitral valve; PV, pulmonary valve; TV, tricuspid valve. to can occur. Other unusual forms of APs exist. Fasciculoventricular connections between the His bundle and ventricular septum produce preexcitation but do not cause arrhythmia, probably because the circuit — Figure 256-8: Atypical AVNRT ECG. Surface ECG showing P waves falling later between QRS complexes, inverted in inferior limb leads, and inverted P wave seen in the subsequent T wave.
Figure 11¶

Caption: FIGURE 256-4 Potential locations for accessory pathways in patients with Wolff- Parkinson-White syndrome and typical QRS appearance of delta waves that can mimic underlying structural heart disease such as myocardial infraction of bundle branch block. AV, aortic valve; MV, mitral valve; PV, pulmonary valve; TV, tricuspid valve. to can occur. Other unusual forms of APs exist. Fasciculoventricular connections between the His bundle and ventricular septum produce preexcitation but do not cause arrhythmia, probably because the circuit — Figure 256-9: Junctional ectopic tachycardia (JET) ECG. Narrow QRS tachycardia often with ventriculoatrial (VA) block, such that AV dissociation is present.
Figure 12¶

Caption: FIGURE 256-3 Wolff-Parkinson-White (WPW) syndrome. A. A 12-lead electrocardiogram in sinus rhythm (SR) of a patient with WPW demonstrating short P-R interval, delta waves, and widened QRS complex. This patient had an anteroseptal location of the accessory pathway (AP). B. Orthodromic atrioventricular (AV) reentry in a patient with WPW syndrome using a posteroseptal AP. Note the P waves in the ST segment (arrows) seen in lead III and normal appearance of QRS of complex. C. Three most common rhythms associated with WPW syndrome: sinus rhythm demonstrating antegrade conduction over the AP and AV node; orthodromic AV reentry tachycardia (AVRT) using retrograde conduction over the AP and antegrade conduction over the AV node; and antidromic AVRT using retrograde conduction over the AV node and antegrade conduction over the AP. — Figure 256-10: Permanent junctional reciprocating tachycardia (PJRT) ECG. ECG showing long R-P interval similar to most ATs, with P waves negative in leads II, III, and aVF.
Figure 13¶

Caption: FIGURE 256-3 Wolff-Parkinson-White (WPW) syndrome. A. A 12-lead electrocardiogram in sinus rhythm (SR) of a patient with WPW demonstrating short P-R interval, delta waves, and widened QRS complex. This patient had an anteroseptal location of the accessory pathway (AP). B. Orthodromic atrioventricular (AV) reentry in a patient with WPW syndrome using a posteroseptal AP. Note the P waves in the ST segment (arrows) seen in lead III and normal appearance of QRS of complex. C. Three most common rhythms associated with WPW syndrome: sinus rhythm demonstrating antegrade conduction over the AP and AV node; orthodromic AV reentry tachycardia (AVRT) using retrograde conduction over the AP and antegrade conduction over the AV node; and antidromic AVRT using retrograde conduction over the AV node and antegrade conduction over the AP. — Figure 256-11: Concealed accessory pathway ECG. Sinus rhythm ECG showing no preexcitation during sinus rhythm but SVT episodes due to retrograde conduction only.
Figure 14¶

Caption: FIGURE 256-3 Wolff-Parkinson-White (WPW) syndrome. A. A 12-lead electrocardiogram in sinus rhythm (SR) of a patient with WPW demonstrating short P-R interval, delta waves, and widened QRS complex. This patient had an anteroseptal location of the accessory pathway (AP). B. Orthodromic atrioventricular (AV) reentry in a patient with WPW syndrome using a posteroseptal AP. Note the P waves in the ST segment (arrows) seen in lead III and normal appearance of QRS of complex. C. Three most common rhythms associated with WPW syndrome: sinus rhythm demonstrating antegrade conduction over the AP and AV node; orthodromic AV reentry tachycardia (AVRT) using retrograde conduction over the AP and antegrade conduction over the AV node; and antidromic AVRT using retrograde conduction over the AV node and antegrade conduction over the AP. — Figure 256-12: Mahaim fiber tachycardia ECG. Wide-complex tachycardia having a left bundle branch block configuration, representing a duplicate AV node and His-Purkinje system.
Figure 15¶

Caption: FIGURE 256-1 Atrioventricular (AV) node reentry. A. Leads II and V are shown. P waves 1 the impression of S waves in the inferior limb leads II, III, and aVF and an R′ in lead 1 (see Fig. 254-1) that involves AV node and its extensions along with perinodal atrial pathway, termed preexcited tachycardias. The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and techni- cally includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, and atrial fibrillation; however, for the purposes of describing an orga- nized approach to diagnosis and treatment of SVT, a separate discus- sion for these non-AV nodal–dependent SVTs are discussed elsewhere. — Figure 256-13: Fasciculoventricular connection ECG. Preexcitation without arrhythmia, showing preexcitation but no reentry circuit due to short circuit length.
Figure 16¶

Caption: FIGURE 256-1 Atrioventricular (AV) node reentry. A. Leads II and V are shown. P waves 1 the impression of S waves in the inferior limb leads II, III, and aVF and an R′ in lead 1 (see Fig. 254-1) that involves AV node and its extensions along with perinodal atrial pathway, termed preexcited tachycardias. The term SVT encompasses a broad group of tachyarrhythmias based on anatomic origin and techni- cally includes sinus tachycardia, atrial tachycardia (AT), atrial flutter, and atrial fibrillation; however, for the purposes of describing an orga- nized approach to diagnosis and treatment of SVT, a separate discus- sion for these non-AV nodal–dependent SVTs are discussed elsewhere. — Figure 256-14: Atrial flutter ECG. ECG showing atrial flutter with variable block, demonstrating the risk of rapid repetitive conduction if AP allows very rapid conduction.
Figure 17¶

Caption: FIGURE 255-2 Focal atrial tachycardia. In the right panel, a surface 12-lead isoelectric segments between, as well as the sinus rhythm. The left panel shows an interatrial septum, as viewed in an anterior-posterior (AP) view of the left atrium local electrical activation during each tachycardia atrial activation, showing a focal demonstrating activation of the atrium dispersing from this focal site. Of note, the pink (Adapted from J Brugada et al: 2019 ESC Guidelines for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J every other P wave may fall coincident with the QRS. Maneuvers that increase AV block, such as carotid sinus massage, Valsalva maneuver, or administration of AV nodal–blocking agents, such as adenosine, are — Figure 256-15: Sinus tachycardia ECG. ECG showing sinus rhythm with increased rate, used as a baseline for comparison with other SVT mechanisms.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.