Chapter 298 | Asthma¶
Part 7: Disorders of the Respiratory System · Part 7 – Respiratory Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Asthma is characterized by episodic airway obstruction, airway hyperresponsiveness, and airway inflammation, usually reversible but potentially irreversible in a subset.
- Airway hyperresponsiveness is a hallmark defined as an acute narrowing response to agents that do not elicit responses in nonaffected individuals.
- Type 2 inflammation (IL-4, IL-5, IL-13) is the most common mechanism, but non-type 2 (neutrophilic) inflammation occurs in severe or steroid-resistant asthma.
- FeNO elevation increases the odds of asthma in children >5 years and adults, but tailoring therapy based on FeNO has not been shown to improve outcomes.
- Sweat testing (chloride concentration) is the gold standard for Cystic Fibrosis, with a threshold of ≥60 mmol/L for diagnosis, but is not a primary diagnostic tool for asthma.
- Occupational asthma accounts for 10–25% of adult-onset asthma, with immunologic stimuli (high-molecular-weight) and irritative stimuli (RADS) recognized.
- Allergic bronchopulmonary aspergillosis (ABPA) is characterized by IgE >1000 IU/mL, eosinophils >500/μL, and positive skin test to Aspergillus.
- Obese adults with asthma have more severe symptoms and are 2–4 times more likely to be hospitalized with an exacerbation.
- Beta-blockers may trigger bronchospasm even in ophthalmic preparations, and ACE inhibitors may cause cough attributed to poorly controlled asthma.
- Asthma mortality declined globally from 0.44 per 100,000 in 1993 to 0.19 in 2006, attributed to increased use of inhaled corticosteroids.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification & Nosology
- 1.2 Airway Hyperresponsiveness
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors & Exposures
- 2.2 Triggers of Airway Narrowing
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Airway Inflammation
- 3.2 Airway Remodeling & Structural Changes
- 3.3 Mediators
- 4. CLINICAL FEATURES
- 4.1 Symptoms & Signs
- 4.2 Exacerbations
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Overlap Syndromes
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Allergy Testing
- 6.2 Sweat Testing
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Therapy
- 7.2 Non-Pharmacologic Management
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Mortality Trends
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy & Perinatal
- 9.2 Occupational & Environmental
- 9.3 Comorbidities
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Clinical Traps
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Asthma development pathway |
| 1 | 🖼 Figure | Pathologic changes that can be seen in asthmatic airways |
| 2 | 🖼 Figure | Inflammatory cells and mediators involved in type 2 and non–type 2 inflammatory... |
1. DEFINITION & OVERVIEW¶
- Asthma is a disease characterized by episodic airway obstruction and airway hyperresponsiveness usually accompanied by airway inflammation.
- In most cases, the airway obstruction is reversible, but in a subset of asthmatics, a component of the obstruction may become irreversible.
- In a large proportion of patients, the airway inflammation is eosinophilic, but some patients may present with differing types of airway inflammation, and in some cases, there is no obvious evidence of airway inflammation.
- The pathway to development of asthma involves an interplay between genetic susceptibility and environmental exposure and endogenous developmental factors (e.g., aging and menopause).
- Harrison's defines the disease expression as characterized by airway hyperresponsiveness with varying degrees of airway inflammation and airway structural changes accompanied by varying degrees of symptoms that can be influenced by exposure to triggers that can cause acute deterioration as well as chronic symptoms.
1.1 Classification & Nosology¶
- In the past, asthma had been divided into atopic and nonatopic (or intrinsic) asthma.
- Atopic asthma: Relating to allergen sensitivity and exposure, with production of IgE, occurring more commonly in children.
- Nonatopic asthma: Occurring in individuals with later onset asthma, with or without allergies, but frequently with eosinophilia.
- This paradigm is being superseded by a nosology that favors consideration of whether asthma is associated with type 2 or non–type 2 inflammation.
- This approach to immunologic classification is driven by a developing understanding of the underlying immune processes and by the development of therapeutic approaches that target type 2 inflammation.
1.2 Airway Hyperresponsiveness¶
- Airway hyperresponsiveness is a hallmark of asthma.
- It is defined as an acute narrowing response of the airways in reaction to agents that do not elicit airway responses in nonaffected individuals or an excess narrowing response to inhaled agents as compared to that which would occur in nonaffected individuals.
- A component of the hyperresponsiveness occurs at the level of the airway smooth muscle itself as demonstrated by hyperresponsiveness to direct smooth-muscle–acting agents such as histamine or methacholine.
- In many patients, the apparent hyperresponsiveness is due to airway wall thickening with consequences for hyperresponsiveness.
- A major therapeutic objective in asthma is to decrease the degree of airway hyperresponsiveness.
2. EPIDEMIOLOGY¶
- Asthma is the most common chronic disease associated with significant morbidity and mortality, with ~262 million people affected globally.
- Cross-sectional studies suggest that 7.9% of the population in the United States is asthmatic as compared to ~4.3% prevalence worldwide.
- Prevalence continues to increase (starting at 7.3% in 2001 in the United States) and is associated with transition from rural to urban living.
- Asthma is more prevalent among children (8.4%) than adults (7.7%).
- In children, the prevalence is greatest among boys (2:1 male-to-female ratio), with a trend toward greater prevalence in women in adulthood.
- In some patients, asthma resolves as they enter adulthood only to 'recur' later in life.
- In the United States in 2016, prior to the effects of the COVID-19 pandemic, 1.8 million people visited an emergency department for asthma, and 189,000 were hospitalized.
- The total economic cost in the United States in 2013 was estimated at $82 billion.
- In the United States, asthma is more prevalent in blacks than Caucasians, and black race is associated with greater case morbidity.
- The ethnicity with the greatest prevalence in the United States is the Puerto Rican population.
- Asthma mortality increased worldwide in the 1960s, apparently related to overuse of inhaled β-agonists.
- Reduction in mortality since then has been attributed to increased use of inhaled corticosteroids.
- Asthma mortality declined globally from 0.44 per 100,000 people in 1993 to 0.19 in 2006, but further reduction in mortality has not occurred since that time.
2.1 Risk Factors & Exposures¶
- Genetic susceptibility plays a key role in asthma susceptibility.
- Family and twin studies suggest a 25–80% degree of heritability.
- Genetic studies suggest complex polygenic inheritance complicated by interaction with environmental exposures.
- Epigenetic modifications related to environmental exposures may also produce heritable patterns of asthma.
- Many of the genes related to asthma have been associated with risk for atopy.
- The most consistently identified genes include ORMDL3/GSDMB (in the 17q21 chromosomal region), ADAM33, DPP-10, TSLP, IL-12, IL-33, ST2 (IL-33 receptor), HLA-DQB1, HLA-DQB2, TLR1, IL-13, and IL6R.
- Only 7.2% of asthma risk can be explained by the single nucleotide polymorphisms that have been associated with asthma.
- Recently, polygenic risk score analysis has been used as a tool to attempt to improve the prediction of asthma risk.
2.2 Triggers of Airway Narrowing¶
- Almost all asthmatics can identify triggers that will make their asthma worse.
- Many of them overlap with the risk factors and etiologic factors reviewed above.
- In some cases, elimination of these triggers may dramatically reduce the impairment caused by asthma.
- In a minority, abatement can lead to 'remission' so that these patients no longer require asthma medications and do not experience bronchospasm with their daily activities and routines.
- While acute exposures to these triggers generally cause short-lived bronchospasm, the bronchospasm may be severe enough that treatment for an exacerbation is required.
- Chronic exposure may lead to permanent deterioration in asthma control, although this does not appear to be true for exercise or stress.
- It should be noted that evidence suggests that severe asthma exacerbations (those requiring systemic corticosteroids) may, in and of themselves, accelerate lung function decline.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- The pathobiologic processes in the airways that lead to episodic and chronic airway obstruction of asthma are discussed below.
- Their pathologic correlates are highlighted in Fig. 298-2, illustrating the pathologic changes that can occur in asthmatic airways.
- These processes can occur individually or simultaneously.
- There can be temporal variation of these processes in an individual based on exogenous factors, discussed later in this chapter, as well as the aging process itself.
- These processes can involve the entire airway (but not the parenchyma), but there can be significant spatial heterogeneity, as has now been demonstrated using hyperpolarized gas ventilation studies and high-resolution computed tomography (CT) of the thorax.
3.1 Airway Inflammation¶
- Most asthma is accompanied by airway inflammation.
- Most commonly, this inflammation is eosinophilic in nature.
- In some patients, neutrophilic inflammation may be predominant, especially in those with more severe asthma.
- Many inflammatory cells are present in an activated state.
- Type 2 Inflammation: An immune response involving the innate and adaptive arms of the immune system to promote barrier immunity on mucosal surfaces.
- Associated with the type 2 subset of CD4+ T-helper cells, which produce the cytokines interleukin (IL) 4, IL-5, and IL-13.
- IL-4 induces B-cell isotype switching to production of IgE.
- IgE, through its binding to basophils and mast cells, results in environmental sensitivity to allergens as a result of cross-linking of IgE on the surface of these mast cells and basophils.
- The products released from these cells include type 2 cytokines as well as direct activators of smooth-muscle constriction and edema.
- IL-5 has a critical role in regulating eosinophils. It controls formation, recruitment, and survival of these cells.
- IL-13 induces airway hyperresponsiveness, mucus hypersecretion, and goblet cell metaplasia.
- Non-Type 2 Processes: Neutrophilic inflammation can also occur.
- This type of inflammation is more commonly seen in severe asthma that has not responded to the common anti-inflammatory therapies, such as corticosteroids, that usually suppress type 2 inflammation.
- In some cases, it may also be associated with chronic infection, occasionally with atypical pathogens such as Mycoplasma, perhaps accounting for the response of some of these patients to macrolide antibiotics.
- It is also commonly seen in reactive airway dysfunction syndrome.
3.2 Airway Remodeling & Structural Changes¶
- The apparent increased responsiveness of the airways in asthma may also have a structural etiology.
- In asthma, airway wall thickness is associated with disease severity and duration.
- This thickening, which may result from a combination of smooth-muscle hypertrophy and hyperplasia, subepithelial collagen deposition, airway edema, and mucosal inflammation, can result in a tendency for the airway to narrow disproportionately in response to stimuli that elicit increased airway muscle tension.
- Airway Smooth Muscle: Can contribute to asthma in three ways.
- First, it can be hyperresponsive to stimuli, as noted above.
- Second, hypertrophy and hyperplasia can lead to airway wall thickening with consequences for hyperresponsiveness.
- Lastly, airway smooth-muscle cells can produce chemokines and cytokines that promote airway inflammation and promote the survival of inflammatory cells, particularly mast cells.
- Subepithelial Collagen Deposition and Matrix Deposition: Thickening of the subepithelial basement membrane occurs as a result of deposition of repair-type collagens and tenascin, periostin, fibronectin, and osteopontin primarily from myofibroblasts under the epithelium.
- The deposition of collagen and matrix stiffens the airway and can result in exaggerated responses to increased circumferential tension stimuli exerted by the smooth muscle.
- Such deposition can also narrow the airway lumen and decrease its ability to relax and thus can contribute to chronic airway obstruction.
- Airway Epithelium: Airway epithelium disruption takes the form of separation of columnar cells from the basal cells.
- The damaged epithelium is hypothesized to form a trophic unit with the underlying mesenchyme.
- This unit elaborates multiple growth factors thought to contribute to airway remodeling.
- The airway epithelium is also a source of multiple cytokines, such as alarmins, and mediators that have been shown to promote a cascade of airway inflammation.
- Vascular Proliferation: In a subset of asthmatics, there is a significant degree of angiogenesis thought to be secondary to elaboration of angiogenic factors in the context of airway inflammation.
- Vascular leakage from postcapillary venules in response to inflammatory mediators can also contribute to the acute and chronic edema of the airways.
- Airway Edema: Submucosal edema can be present as an acute response in asthma and as a chronic contributor to airway wall thickening.
- Epithelial Goblet Cell Metaplasia and Mucus Hypersecretion: Chronic inflammation can result in the proliferation of mucus cells.
- Increased mucus production can reduce the effective airway luminal area.
- Mucus plugs can obstruct medium-size airways and can extend into the small airways.
- These mucus plugs can result in persistent airway obstruction.
- Neuronal Proliferation: Neurotrophins, which can lead to neuronal proliferation, are elaborated by smooth-muscle cells, epithelial cells, and inflammatory cells.
- Neuronal inputs can regulate smooth-muscle tone and mucus production, which may mediate acute bronchospasm and potentially chronically increased airway tone.
3.3 Mediators¶
- Many chemical substances or signaling factors can contribute to the pathobiologic picture of asthma.
- Some of them have been successfully targeted in developing asthma therapies.
- Cytokines: IL-4, IL-5, and IL-13 are the major cytokines associated with type 2 inflammation.
- They have all been targeted successfully in asthma therapies.
- Thymic stromal lymphopoietin (TSLP), IL-25, and IL-33 also play a role in the signaling cascade and are being actively studied as targets for treatment of asthma.
- IL-9 has been implicated as well.
- IL-6, IL-17, tumor necrosis factor α (TNF-α), IL-1β, and IL-8 have been implicated in non–type 2 inflammation.
- Fatty Acid Mediators: Proinflammatory mediators derived from arachidonic acid include leukotrienes and prostaglandins.
- The cysteinyl leukotrienes (leukotrienes C, D, and E) are produced by eosinophils and mast cells.
- They are potent smooth-muscle constrictors.
- They also stimulate mucus secretion, recruit allergic inflammatory cells, cause microvascular leakage, modulate cytokine production, and influence neural transmission.
- The non-cysteinyl leukotriene, LTB4, is produced primarily from neutrophils but can also be synthesized by macrophages and epithelial cells.
- It is a potent neutrophil chemoattractant.
- Prostaglandins are for the most part proinflammatory.
- Prostaglandin D2 (PGD2) is produced by mast cells.
- Receptors for PGD2 (CRTH2 receptors) are present on T2 cells, ILC2 cells, mast cells, eosinophils, macrophages, and epithelial cells, and the activation of these receptors upregulates type 2 inflammation.
- However, studies with drugs blocking CRTH2 have been relatively disappointing thus far.
- Resolvins and lipoxins: There are several classes of fatty acid–derived mediators that are responsible for the resolution of inflammation.
- Several studies suggest that deficiencies in these moieties may be responsible for the ongoing inflammation in asthma, especially in severe asthma.
- Nitric Oxide: Nitric oxide is a potent vasodilator, and in vitro studies suggest that it can increase mucus production and smooth-muscle proliferation.
- It is produced by epithelial cells, especially in response to IL-13, and by stimulated inflammatory cells including eosinophils, mast cells, and neutrophils.
- Its precise role in the asthmatic diathesis is unclear.
- However, its production is increased in the airways in the presence of IL-13-induced inflammation, and it can be detected in exhaled breath and is reduced by interventions that interfere with IL-13 production or activity.
- Reactive Oxygen Species: When allergens, pollutants, bacteria, and viruses activate inflammatory cells in the airway, they induce respiratory bursts that release reactive oxygen species that result in oxidative stress in the surrounding tissue.
- Increases in oxidative stress have been shown to affect smooth-muscle contraction, increase mucus secretion, produce airway hyperresponsiveness, and result in epithelial shedding.
- Chemokines: A variety of chemokines are secreted by the epithelium (as well as other inflammatory cells) and attract inflammatory cells into the airways.
- Those of particular interest include eotaxin (an eosinophil chemoattractant), TARC and MDC (which attract T2 cells), and RANTES (which has pluripotent pro-phlogistic effects).
4. CLINICAL FEATURES¶
- Asthma most frequently presents as episodic shortness of breath, that can lead to the development of asthma.
- Continued or additional exposures and triggers can affect the progression of disease and the degree of impairment.
- Asthma most frequently presents as episodic shortness of breath, that can lead to the development of asthma.
- These symptoms can occur in combination or separately.
- Other symptoms can include chest tightness and/or mucus production.
- These symptoms can resolve spontaneously or with therapy.
- In some patients, wheezing and/or dyspnea can be persistent.
- Episodes of acute bronchospasm, known as exacerbations, may be severe enough to require emergency medical care or hospitalization and may result in death.
- In some patients, wheezing and/or dyspnea can be persistent.
4.1 Symptoms & Signs¶
- Episodic shortness of breath.
- Wheezing.
- Cough.
- Chest tightness.
- Mucus production.
- Symptoms can occur in relation to triggers but may also occur spontaneously.
- Symptoms can resolve spontaneously or with therapy.
- In some patients, wheezing and/or dyspnea can be persistent.
4.2 Exacerbations¶
- Episodes of acute bronchospasm, known as exacerbations.
- May be severe enough to require emergency medical care or hospitalization.
- May result in death.
- The almost 50% reduction in exacerbations during the COVID-19 pandemic has been attributed to decreased viral infections.
5. DIFFERENTIAL DIAGNOSIS¶
- Review and meta-analysis to help differentiate asthma/chronic obstructive pulmonary disease overlap syndrome.
- Data are conflicting regarding the presence of eosinophils in the sputum and with response to inhaled corticosteroids.
- Evidence suggests that tailoring of asthma therapy based on sputum eosinophil levels was effective in decreasing asthma exacerbations.
- Tailoring of therapy based on FeNO was not beneficial in improving outcomes.
- Insufficient evidence was observed to advocate the use of either sputum analysis or FeNO in clinical practice.
5.1 Overlap Syndromes¶
- Asthma/chronic obstructive pulmonary disease overlap syndrome.
- Data are conflicting regarding the presence of eosinophils in the sputum and with response to inhaled corticosteroids.
6. INVESTIGATIONS & DIAGNOSIS¶
- Skin testing, including patch testing and/or delayed intradermal testing, is available to test exposure to particular allergens and determine reactivity.
- These tests have been shown to aid in clinical phenotyping of type I reactions and potentially in type IV reactions, though their role in type IV assessment remains more controversial.
- In the context of suspected type I reactions, patch testing is more cost effective and may be as effective as intradermal testing in identifying potential causative agents.
- The negative predictive value of intradermal skin testing in assessing for IgE-mediated drug allergies is high.
- However, the high sensitivity of this testing limits its specificity, and results must be interpreted in the context of the pretest probability and the clinical experience of the patient.
- Skin tests have also been demonstrated to assist in identifying the causative agent in type IV reactions and to assess cross-reactivity between structurally related drugs.
- Intradermal testing may be more sensitive than patch testing to assess for type IV drug reactions.
- Though some debate continues regarding a mandatory role for skin testing in the assessment of potential drug allergies, drug provocation testing or rechallenge is generally regarded as safe in low-risk individuals with history of urticaria or immediate rash.
- Skin testing has been proposed as a preliminary assessment in higher-risk individuals with a history of two or more reactions, angioedema, or anaphylaxis, prior to consideration of drug provocation testing.
- Assessment of chloride concentration in sweat using pilocarpine iontophoresis, or sweat testing, remains a key element in the diagnostic framework of cystic fibrosis (CF).
- This method utilizes pilocarpine to stimulate sweat production.
- As patients with CF suffer from alterations to the sodium chloride ion channel, measurement of electrolytes in their secretions such as sweat reveals elevated chloride concentrations.
- This testing has been considered the gold standard in the diagnosis of CF due to its functional nature, its relative noninvasiveness, the establishment of validated standards for its performance, and its ability to discriminate between healthy individuals and those with CF at a chloride concentration of ≥60 mmol/L.
- The likelihood of a diagnosis of CF at a concentration of <40 mmol/L has been observed to be low.
- An indeterminate range was defined as 40–59 mmol/L, which could be consistent with the disease if genetic and clinical manifestations were supportive.
- The Cystic Fibrosis Foundation provided updated guidance for the interpretation of sweat test results, with a decreased lower threshold to define an intermediate range of chloride concentration (changed from 40–50 mmol/L to 30–59 mmol/L), which could be consistent with the diagnosis of CF in the appropriate genetic and clinical context.
- In a subsequent analysis, utilization of the new guidance was found to enhance the probability of identifying patients with CF without increasing the false-positive diagnosis rate in the population.
- Sweat testing is a critical component of the CF diagnostic algorithm but should be interpreted in the context of clinical manifestations of disease and correlated with genetic testing in those suspected of the diagnosis.
Table 1 — TABLE 298-1 Exposures and Risk Factors Related to the Development of Asthma¶
| Risk Factor |
|---|
| Allergen exposure in those with a predisposition to atopy |
| Occupational exposure |
| Air pollution |
| Infections (viral and Mycoplasma) |
| Tobacco |
| Obesity |
| Diet |
| Fungi in allergic airway mycoses |
| Acute irritants and reactive airway dysfunction syndrome (RADS) |
| High-intensity exercise in elite athletes |
Table 2 — TABLE 298-2 Triggers of Airway Narrowing¶
| Trigger Category |
|---|
| Allergens |
| Irritants |
| Viral infections |
| Exercise and cold, dry air |
| Air pollution |
| Drugs |
| Occupational exposures |
| Hormonal changes |
| Pregnancy |
6.1 Allergy Testing¶
- Allergy testing is often considered in the assessment of environmental exposures, including seasonal allergens, food allergens, and drug allergens.
- In the case of drug allergens in particular, drug reactions are often reported based on remote history and are often unconfirmed.
- The hesitancy to re-expose patients with an unconfirmed drug allergy can lead to limited options for treatment, to delay in treatment, and to utilization of treatments with more extended spectrum, potentially influencing the resistance patterns of these agents.
6.2 Sweat Testing¶
- Assessment of chloride concentration in sweat using pilocarpine iontophoresis, or sweat testing, remains a key element in the diagnostic framework of cystic fibrosis (CF).
- This method utilizes pilocarpine to stimulate sweat production.
- As patients with CF suffer from alterations to the sodium chloride ion channel, measurement of electrolytes in their secretions such as sweat reveals elevated chloride concentrations.
- This testing has been considered the gold standard in the diagnosis of CF due to its functional nature, its relative noninvasiveness, the establishment of validated standards for its performance, and its ability to discriminate between healthy individuals and those with CF at a chloride concentration of ≥60 mmol/L.
- The likelihood of a diagnosis of CF at a concentration of <40 mmol/L has been observed to be low.
- An indeterminate range was defined as 40–59 mmol/L, which could be consistent with the disease if genetic and clinical manifestations were supportive.
- The Cystic Fibrosis Foundation provided updated guidance for the interpretation of sweat test results, with a decreased lower threshold to define an intermediate range of chloride concentration (changed from 40–50 mmol/L to 30–59 mmol/L), which could be consistent with the diagnosis of CF in the appropriate genetic and clinical context.
- In a subsequent analysis, utilization of the new guidance was found to enhance the probability of identifying patients with CF without increasing the false-positive diagnosis rate in the population.
- Sweat testing is a critical component of the CF diagnostic algorithm but should be interpreted in the context of clinical manifestations of disease and correlated with genetic testing in those suspected of the diagnosis.
7. MANAGEMENT & TREATMENT¶
- A major therapeutic objective in asthma is to decrease the degree of airway hyperresponsiveness.
- While acute exposures to these triggers generally cause short-lived bronchospasm, the bronchospasm may be severe enough that treatment for an exacerbation is required.
- Chronic exposure may lead to permanent deterioration in asthma control, although this does not appear to be true for exercise or stress.
- It should be noted that evidence suggests that severe asthma exacerbations (those requiring systemic corticosteroids) may, in and of themselves, accelerate lung function decline.
- Reduction in mortality since then has been attributed to increased use of inhaled corticosteroids.
- The development of anti–IL-5 drugs that dramatically reduce eosinophils has allowed us to determine that, in many asthmatics, eosinophils play a major role in asthma pathobiology.
- They may induce hyperresponsiveness through release of oxidative radicals and major basic protein, which can disrupt the epithelium.
- They produce cysteinyl-leukotrienes that directly stimulate smooth muscle contraction and resulting in airway constriction.
- In addition, recent CT imaging has suggested that mucus plugs, which may contain significant amounts of eosinophil aggregates, may accumulate in the airways and contribute to asthma severity.
- Treatment of symptomatic reflux disease has been shown to produce modest improvement in asthma control.
7.1 Pharmacologic Therapy¶
- The development of anti–IL-5 drugs that dramatically reduce eosinophils has allowed us to determine that, in many asthmatics, eosinophils play a major role in asthma pathobiology.
- They may induce hyperresponsiveness through release of oxidative radicals and major basic protein, which can disrupt the epithelium.
- They produce cysteinyl-leukotrienes that directly stimulate smooth muscle contraction and resulting in airway constriction.
- In addition, recent CT imaging has suggested that mucus plugs, which may contain significant amounts of eosinophil aggregates, may accumulate in the airways and contribute to asthma severity.
- The development of anti–IL-5 drugs that dramatically reduce eosinophils has allowed us to determine that, in many asthmatics, eosinophils play a major role in asthma pathobiology.
- They may induce hyperresponsiveness through release of oxidative radicals and major basic protein, which can disrupt the epithelium.
- They produce cysteinyl-leukotrienes that directly stimulate smooth muscle contraction and resulting in airway constriction.
- In addition, recent CT imaging has suggested that mucus plugs, which may contain significant amounts of eosinophil aggregates, may accumulate in the airways and contribute to asthma severity.
7.2 Non-Pharmacologic Management¶
- In some cases, elimination of these triggers may dramatically reduce the impairment caused by asthma.
- In a minority, abatement can lead to 'remission' so that these patients no longer require asthma medications and do not experience bronchospasm with their daily activities and routines.
- While acute exposures to these triggers generally cause short-lived bronchospasm, the bronchospasm may be severe enough that treatment for an exacerbation is required.
- Chronic exposure may lead to permanent deterioration in asthma control, although this does not appear to be true for exercise or stress.
- It should be noted that evidence suggests that severe asthma exacerbations (those requiring systemic corticosteroids) may, in and of themselves, accelerate lung function decline.
8. PROGNOSIS & COMPLICATIONS¶
- Asthma mortality increased worldwide in the 1960s, apparently related to overuse of inhaled β-agonists.
- Reduction in mortality since then has been attributed to increased use of inhaled corticosteroids.
- Asthma mortality declined globally from 0.44 per 100,000 people in 1993 to 0.19 in 2006, but further reduction in mortality has not occurred since that time.
- In some patients, asthma resolves as they enter adulthood only to 'recur' later in life.
- In a subset of asthmatics, a component of the obstruction may become irreversible.
- Severe asthma exacerbations (those requiring systemic corticosteroids) may, in and of themselves, accelerate lung function decline.
8.1 Mortality Trends¶
- Asthma mortality increased worldwide in the 1960s, apparently related to overuse of inhaled β-agonists.
- Reduction in mortality since then has been attributed to increased use of inhaled corticosteroids.
- Asthma mortality declined globally from 0.44 per 100,000 people in 1993 to 0.19 in 2006, but further reduction in mortality has not occurred since that time.
9. SPECIAL CONSIDERATIONS¶
- Pregnancy may precipitate worsening of asthma in approximately one-third of pregnant patients.
- Preeclampsia and prematurity have been associated with increased risk of asthma in the progeny.
- Babies born by cesarean section are at higher risk for asthma.
- Those with neonatal jaundice are also at increased risk.
- Breast-feeding reduced early wheezing but has a less clear effect on later incidence of asthma.
- Active smoking is estimated to increase the incidence of asthma by up to fourfold in adolescents and young adults.
- Maternal smoking and secondhand smoke exposure are associated with increased childhood asthma.
- Childhood secondhand smoke exposure increased asthma risk twofold.
- Obese adults with asthma have more severe asthma symptoms than lean adults and are two to four times more likely to be hospitalized with an asthma exacerbation.
- Nonrandomized studies have shown an improvement and significant reduction in exacerbations after bariatric surgery.
- The presence of gastroesophageal reflux disease (GERD) predicts poor quality of life and is an independent predictor of asthma exacerbations.
- Treatment of symptomatic reflux disease has been shown to produce modest improvement in asthma control.
- Beta blockers may trigger bronchospasm even when used solely in ophthalmic preparations.
- While the more selective beta blockers are safe for most asthmatics, beta blocker use may be a cause of difficult-to-control asthma.
- Aspirin may precipitate bronchospasm in those with aspirin-exacerbated respiratory disease (see 'Special Considerations').
- Angiotensin-converting enzyme (ACE) inhibitors (and to a lesser extent angiotensin receptor blockers) may cause cough that may be attributed to poorly controlled asthma.
- High-Concentration Irritant Exposure and RADS: A solitary exposure (see 'Occupational Exposures' above) and large-quantity exposures (see discussion of RADS above) can lead to long-lasting or permanent symptoms.
- Causative agents include oxidizing and reducing agents in an aerosol or high levels of particulates.
- The acute pathology usually involves epithelial injury with neutrophilia.
- There is little evidence of type 2 inflammation.
- This syndrome differs from occupational asthma in that these patients have not become sensitized to the provocative agent and can return to work in that environment once they have recovered.
- However, the course of the disease may be variable, with some series showing documented abnormalities and persistent symptoms 10 years after exposure.
- Fungi and Allergic Airway Mycoses: One to 2% of patients with asthma may have an IgE-mediated sensitization to colonization of the airway by fungi, with the most common fungus causing such a reaction being Aspergillus fumigatus.
- So-called allergic bronchopulmonary aspergillosis (ABPA) is characterized by a type 2 airway inflammatory response to aspergillus with IgE >1000 IU/mL, eosinophils >500/μL, positive skin test to Aspergillus, and specific IgE and IgG antibodies to Aspergillus.
- Patients may have intermittent mucus plugging and central bronchiectasis.
- Up to two-thirds of patients will grow Aspergillus from the sputum.
- Treatment involves systemic antifungal treatment with itraconazole or voriconazole and oral corticosteroids.
- A role for biologics has also been suggested.
- Exercise-Induced Symptoms in Elite Athletes: Exercise-induced airway narrowing in elite athletes undertaking extreme exercise in strenuous condition.
- These athletes may have little, or no, airway hyperreactivity or asthma risk factors.
- The condition may involve additional mechanisms including direct epithelial injury.
- Such a syndrome has also been reported in swimmers possibly related to pool chlorination.
9.1 Pregnancy & Perinatal¶
- Pregnancy may precipitate worsening of asthma in approximately one-third of pregnant patients.
- Preeclampsia and prematurity have been associated with increased risk of asthma in the progeny.
- Babies born by cesarean section are at higher risk for asthma.
- Those with neonatal jaundice are also at increased risk.
- Breast-feeding reduced early wheezing but has a less clear effect on later incidence of asthma.
9.2 Occupational & Environmental¶
- Occupational asthma is estimated to account for 10–25% of adult-onset asthma.
- The occupations associated with the most cases in European Community Health Surveys were nursing and cleaning.
- Two types of exposures are recognized: (1) an immunologic stimulus (further subdivided into high-molecular-weight [e.g., proteins, flour] and low-molecular-weight [e.g., formaldehyde, diisocyanate] stimuli based on whether they act as haptens or can directly stimulate a response), and (2) an irritative stimulus.
- The immunologic form is associated with a latency period between time of exposure and development of symptoms.
- The irritative form, known as reactive airway dysfunction syndrome (RADS), will be discussed below.
- A combination of genetic predisposition (including atopy), timing, intensity of exposure, and co-exposure (e.g., smoking) influences whether an individual will develop occupational asthma.
- High-Concentration Irritant Exposure and RADS: A solitary exposure (see 'Occupational Exposures' above) and large-quantity exposures (see discussion of RADS above) can lead to long-lasting or permanent symptoms.
- Causative agents include oxidizing and reducing agents in an aerosol or high levels of particulates.
- The acute pathology usually involves epithelial injury with neutrophilia.
- There is little evidence of type 2 inflammation.
- This syndrome differs from occupational asthma in that these patients have not become sensitized to the provocative agent and can return to work in that environment once they have recovered.
- However, the course of the disease may be variable, with some series showing documented abnormalities and persistent symptoms 10 years after exposure.
9.3 Comorbidities¶
- Obese adults with asthma have more severe asthma symptoms than lean adults and are two to four times more likely to be hospitalized with an asthma exacerbation.
- Nonrandomized studies have shown an improvement and significant reduction in exacerbations after bariatric surgery.
- The presence of gastroesophageal reflux disease (GERD) predicts poor quality of life and is an independent predictor of asthma exacerbations.
- Treatment of symptomatic reflux disease has been shown to produce modest improvement in asthma control.
10. KEY PEARLS & CLINICAL TRAPS¶
- FeNO elevation increased the odds of having asthma in both children above the age of 5 years and adults.
- In another systematic review of FeNO utilization in the management of adults with asthma, the assessment was helpful in the management of severe exacerbations but had no significant impact on overall exacerbations or inhaled corticosteroid use.
- Moreover, evidence suggests that tailoring of asthma therapy based on sputum eosinophil levels was effective in decreasing asthma exacerbations, but tailoring of therapy based on FeNO was not beneficial in improving outcomes, and insufficient evidence was observed to advocate the use of either sputum analysis or FeNO in clinical practice.
- FeNO has also been shown to be influenced by ethnicity, and appropriate reference standards for different ethnic groups have yet to be established.
- While FeNO has been proposed as a potential clinical guide to management, its use has not been incorporated into all guideline recommendations, and it has not been formally approved for clinical use.
- Beta blockers may trigger bronchospasm even when used solely in ophthalmic preparations.
- While the more selective beta blockers are safe for most asthmatics, beta blocker use may be a cause of difficult-to-control asthma.
- Aspirin may precipitate bronchospasm in those with aspirin-exacerbated respiratory disease (see 'Special Considerations').
- Angiotensin-converting enzyme (ACE) inhibitors (and to a lesser extent angiotensin receptor blockers) may cause cough that may be attributed to poorly controlled asthma.
- Asthma mortality increased worldwide in the 1960s, apparently related to overuse of inhaled β-agonists.
- Reduction in mortality since then has been attributed to increased use of inhaled corticosteroids.
- Asthma mortality declined globally from 0.44 per 100,000 people in 1993 to 0.19 in 2006, but further reduction in mortality has not occurred since that time.
10.1 Diagnostic Clues¶
- FeNO elevation increased the odds of having asthma in both children above the age of 5 years and adults.
- In another systematic review of FeNO utilization in the management of adults with asthma, the assessment was helpful in the management of severe exacerbations but had no significant impact on overall exacerbations or inhaled corticosteroid use.
- Moreover, evidence suggests that tailoring of asthma therapy based on sputum eosinophil levels was effective in decreasing asthma exacerbations, but tailoring of therapy based on FeNO was not beneficial in improving outcomes, and insufficient evidence was observed to advocate the use of either sputum analysis or FeNO in clinical practice.
- FeNO has also been shown to be influenced by ethnicity, and appropriate reference standards for different ethnic groups have yet to be established.
- While FeNO has been proposed as a potential clinical guide to management, its use has not been incorporated into all guideline recommendations, and it has not been formally approved for clinical use.
10.2 Clinical Traps¶
- Beta blockers may trigger bronchospasm even when used solely in ophthalmic preparations.
- While the more selective beta blockers are safe for most asthmatics, beta blocker use may be a cause of difficult-to-control asthma.
- Aspirin may precipitate bronchospasm in those with aspirin-exacerbated respiratory disease (see 'Special Considerations').
- Angiotensin-converting enzyme (ACE) inhibitors (and to a lesser extent angiotensin receptor blockers) may cause cough that may be attributed to poorly controlled asthma.
- Asthma mortality increased worldwide in the 1960s, apparently related to overuse of inhaled β-agonists.
- Reduction in mortality since then has been attributed to increased use of inhaled corticosteroids.
- Asthma mortality declined globally from 0.44 per 100,000 people in 1993 to 0.19 in 2006, but further reduction in mortality has not occurred since that time.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
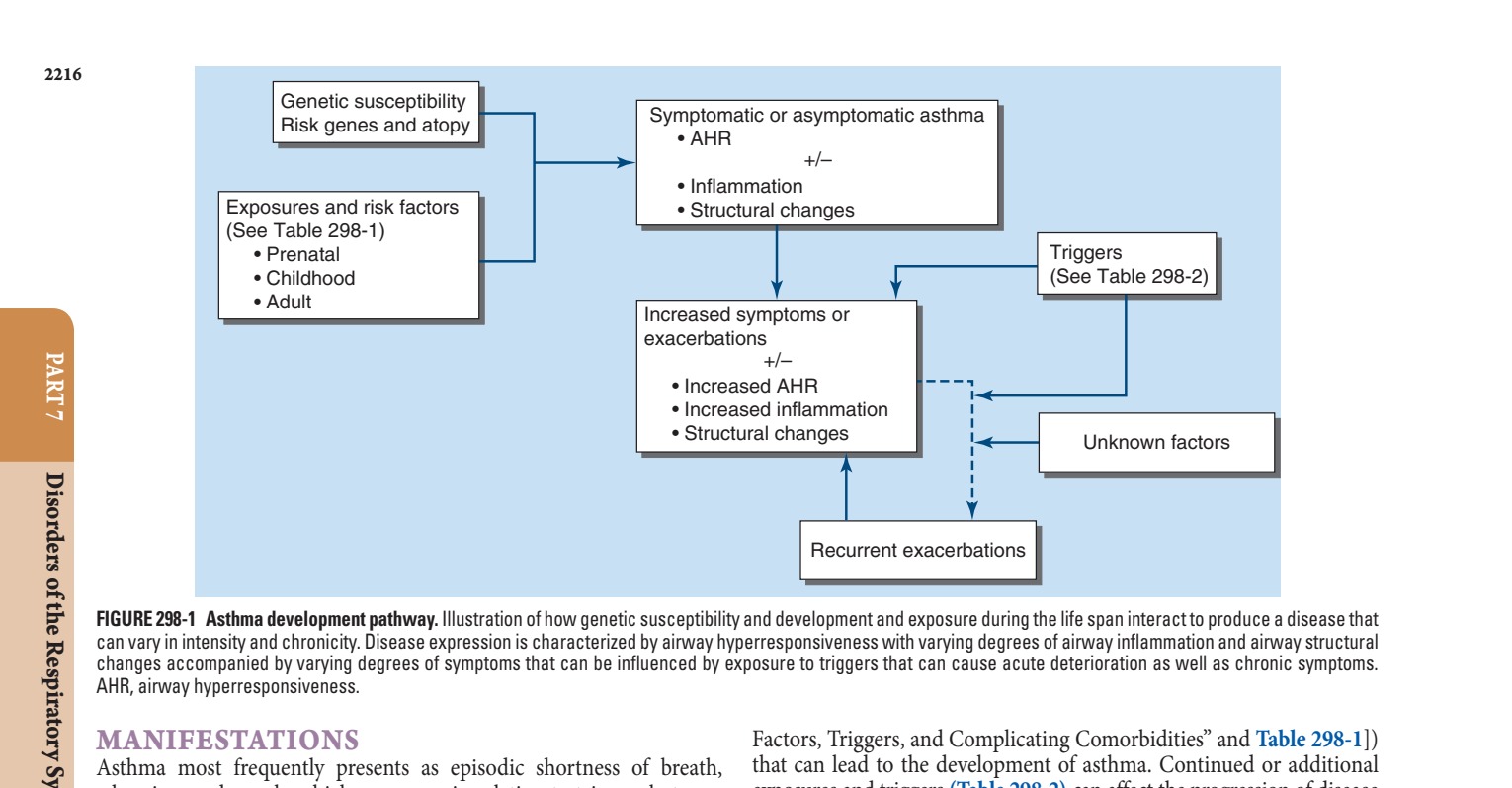
Caption: FIGURE 298-1 Asthma development pathway. Illustration of how genetic susceptibility can vary in intensity and chronicity. Disease expression is characterized by airway changes accompanied by varying degrees of symptoms that can be influenced by AHR, airway hyperresponsiveness. MANIFESTATIONS Asthma most frequently presents as episodic shortness of breath, wheezing, and cough, which can occur in relation to triggers but may also occur spontaneously. These symptoms can occur in combination or separately. Other symptoms can include chest tightness and/or
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
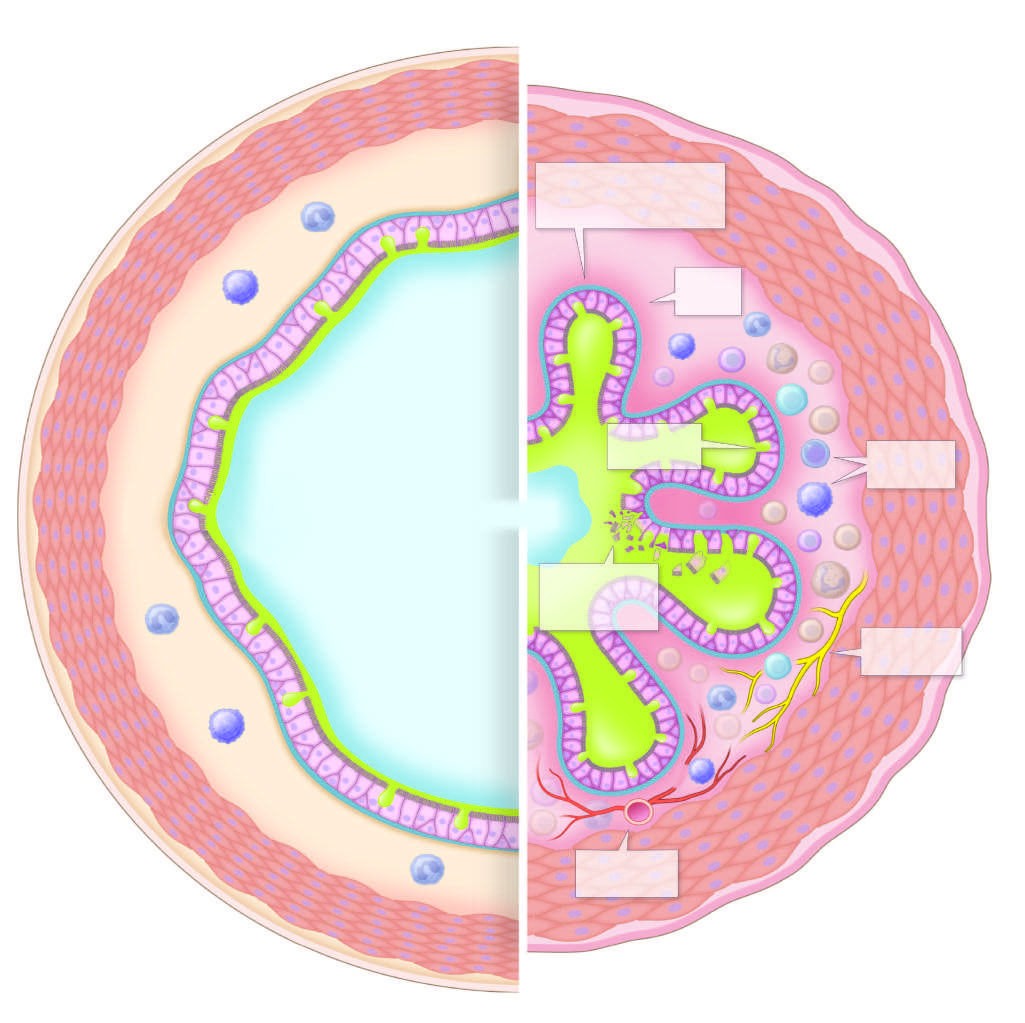
Caption: FIGURE 298-2 Pathologic changes that can be seen in asthmatic airways. Illustrated is airway, and the right represents an asthmatic airway highlighting the pathologic muscle contraction and hypertrophy, mucus in the airway lumen, and thickening of the to increase in size with smooth-muscle relaxation may be impaired by deposition of proliferation. All these changes may not be present in one individual, and certain patients — Figure 298-2: Pathologic changes in asthmatic airways. Cross-sectional illustration of a bronchus comparing normal airway (left) to asthmatic airway (right). The asthmatic airway shows reduced lumen due to smooth-muscle contraction and hypertrophy, mucus in the lumen, thickening of the submucosa due to edema and cellular infiltration, collagen deposition, epithelial disruption, and vascular/neuronal proliferation.
Figure 2¶
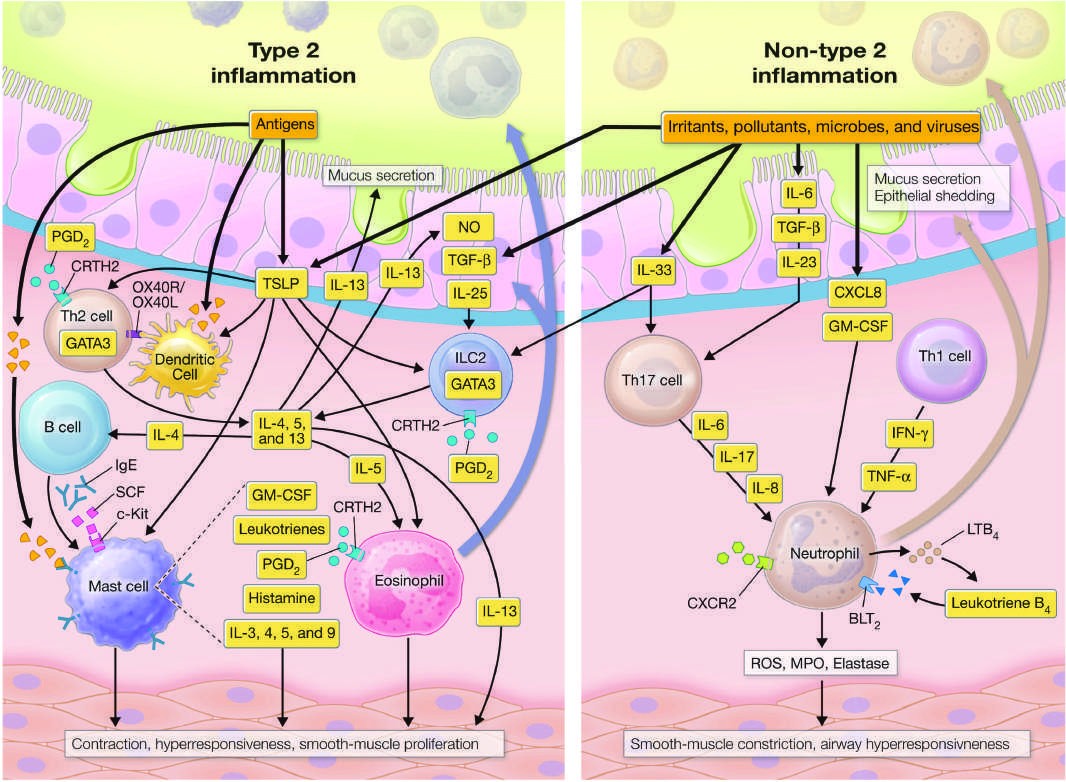
Caption: FIGURE 298-3 Inflammatory cells and mediators involved in type 2 and non–type 2 inflammatory cells and release of mediators that are responsible for recruiting and hyperresponsiveness and fibroblast proliferation and matrix deposition. BLT2, receptor); CXCL8, CXC motif chemokine ligand 8; CXCR2, CXC chemokine receptor 2; factor; IFN-γ, interferon gamma; IL, interleukin; ILC2, innate lymphoid type 2 cells; c-Kit, NO, nitric oxide; OX40L/OX40R, OX40 ligand/OX40 receptor; PGD2, prostaglandin D2; factor β; Th, T helper; TNF-α, tumor necrosis factor α; TSLP, thymic stromal — Figure 298-3: Inflammatory cells and mediators involved in type 2 and non–type 2 inflammation. Diagram illustrating the activation of inflammatory cells (mast cells, eosinophils, T2 cells, ILC2s) by allergens and nonallergic stimuli, leading to release of mediators (cytokines, leukotrienes, chemokines) that affect airway smooth muscle, fibroblast proliferation, and matrix deposition.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.