Cestode Infections¶
Chapter 242 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Parasitic
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Neurocysticercosis diagnosis relies on imaging visualization of a scolex ('dot-in-hole') or specific serology (EITB); calcified lesions do not require antiparasitic therapy.
- Management of neurocysticercosis prioritizes seizure control and hydrocephalus management before initiating antiparasitic drugs to avoid worsening inflammation.
- Echinococcosis treatment is guided by WHO imaging classification (CE1-CE5); PAIR (aspiration, instillation, reaspiration) is preferred for small liver cysts, while surgery is required for multilocular disease.
- Paragonimiasis mimics tuberculosis; diagnosis requires detection of eggs in sputum/feces and history of raw freshwater crab consumption.
- Taenia solium eggs are immediately infective for humans; autoinfection can occur via ingestion of eggs from one's own feces.
- Praziquantel is the drug of choice for Taeniasis and Paragonimiasis; Albendazole is the primary agent for Echinococcosis.
- R. nana infection is unique among human cestodes as it does not require an intermediate host and causes autoinfection.
- Echinococcal cyst rupture can cause anaphylaxis; aspiration should only be performed by experienced practitioners with precautions.
- Diagnostic criteria for neurocysticercosis (Del Brutto) require one absolute criterion or specific combinations of major/minor neuroimaging and clinical/exposure criteria.
- Prevention of Taenia solium infection involves adequate cooking of pork (56°C for 5 min) or freezing at -10°C for 9 days.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 4. CLINICAL FEATURES
- 4.1 Neurocysticercosis
- 4.2 Echinococcosis
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Neurocysticercosis Diagnostic Criteria
- 6.2 Echinococcosis Imaging Classification
- 7. MANAGEMENT & TREATMENT
- 7.1 Neurocysticercosis Management
- 7.2 Echinococcosis Management
- 7.3 Drug Therapy
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- 11. WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- 12. WHAT EXCLUDES THE DIAGNOSIS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Management of cystic hydatid disease caused by Echinococcus radiographic appearance |
| 1 | 🖼 Figure | Neurocysticercosis is caused by Taenia solium |
| 2 | 🖼 Figure | Imaging studies of cystic echinococcosis |
1. DEFINITION & OVERVIEW¶
- Cestodes, or tapeworms, are members of the flatworm phylum (Platyhelminthes) and comprise the subphylum (Cestoda).
- Adult worms are segmented worms found in the gastrointestinal tract of the definitive host.
- Larval forms are typically cystic and found in the tissues of the intermediate host.
- Human cestode infections include both tapeworm and larval-form infections.
- For tapeworm infections, humans are the definitive hosts, with adult tapeworms living in the gastrointestinal tract (Taenia saginata, Dibothriocephalus latus, and Dipylidium caninum).
- Humans are an intermediate or dead-end host with larval-stage parasites living in the tissues for Echinococcus spp., Spirometra spp., and Taenia multiceps.
- Humans may be either the intermediate hosts or the definitive hosts for Taenia solium and are the hosts of both stages of Rodentolepis nana (formerly Hymenolepis nana).
- Tapeworm forms are typically elongated and ribbon-shaped and attach to the intestinal mucosa by means of sucking cups or hooks located on the scolex.
- A short, narrow neck is found at the base of the scolex from which proglottids (segments) form.
- As proglottids mature, they are displaced from the neck by the formation of new, less mature segments.
- The elongating chain of attached proglottids, called the strobila, constitutes the bulk of the tapeworm.
- Some tapeworms consist of more than 1000 proglottids and may be several meters long.
- Mature proglottids are hermaphroditic and produce eggs, which are intermittently released.
- Most human tapeworms require at least one intermediate host to complete the life cycle.
- After ingestion of the eggs or proglottids by an intermediate host, the eggs are activated to release the invasive larvae (oncospheres).
- The oncosphere penetrates the intestinal mucosa and migrates to tissues and develops into an encysted form known as a cysticercus (single scolex), a coenurus (multiple scolices), or a hydatid (cyst with daughter cysts, each containing multiple protoscolices).
- After ingestion of the cystic forms by the definitive host, the scolex evaginates and develops into a tapeworm.
- Echinococcosis (also known as hydatid disease) refers to infection by the larval stage of Echinococcus species (E. granulosus sensu lato, E. multilocularis, or E. vogeli).
- E. granulosus sensu lato parasites are found on all continents, with areas of high prevalence in western China, central Asia, the Middle East, the Mediterranean region, eastern Africa, and parts of South America.
- E. multilocularis causes multilocular or alveolar echinococcosis characterized by locally invasive lesions.
- Alveolar echinococcosis is prevalent in Alpine, sub-Arctic, and Arctic regions of the northern hemisphere, including western China, central Asia, central and northern Europe, and in isolated areas of North America.
- Neotropical echinococcosis (formerly termed polycystic hydatid disease) is caused by E. vogeli and E. oligarthrus, which are only found in limited foci in South America.
- Echinococcal species require both intermediate and definitive hosts.
- The definitive hosts are usually canines (dogs, foxes, wolves) that harbor the small tapeworms in the intestine and shed eggs in stool.
- Humans are a dead-end intermediate host and not part of the parasite's life cycle for Echinococcus.
- R. nana is the only human cestode that does not require an intermediate host.
- Both the larval and adult stages coexist in the intestine of infected persons.
- Hymenolepis diminuta is a cestode of rodents that occasionally causes infection in small children.
- Infection is acquired by ingesting uncooked cereal and other foods contaminated by fleas and other insects that serve as intermediate hosts for H. diminuta.
2. EPIDEMIOLOGY¶
- Taenia saginata is found in all countries where raw or undercooked beef is eaten.
- It is most prevalent in sub-Saharan African and Middle Eastern countries.
- Taenia asiatica is closely related to T. saginata and is found in Asia, with pigs as intermediate hosts.
- T. solium has a wide global distribution including all areas where pigs are raised with access to human feces.
- Cysticercosis is highly prevalent in Latin America, sub-Saharan Africa, China, India, and Southeast Asia.
- Cysticercosis also occurs in nonendemic nations due to the immigration of tapeworm carriers or cysticercosis-infected persons from endemic areas.
- Echinococcosis is prevalent worldwide in most areas where livestock is raised in association with dogs.
- E. granulosus sensu lato parasites are found on all continents.
- E. multilocularis is prevalent in Alpine, sub-Arctic, and Arctic regions of the northern hemisphere.
- Neotropical echinococcosis is found in limited foci in South America.
- R. nana infection is most often asymptomatic but may be associated with diarrhea, abdominal pain, and weight loss, particularly in children with the highest burden of infection.
- H. diminuta infection is acquired by ingesting uncooked cereal and other foods contaminated by fleas and other insects that serve as intermediate hosts.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Humans serve as the definitive host for the adult stage of T. saginata and T. asiatica.
- The scolex attaches to the small intestines and the strobila with 1000–2000 proglottids can reach 8 m in length.
- The scolex of T. asiatica has an unarmed (with no hooks) rostellum and four suckers, whereas T. saginata has no rostellum but attaches via four prominent suckers.
- Each gravid segment has 15–30 uterine branches (in contrast to 8–12 for T. solium).
- The eggs of the three human-infecting Taenia species are indistinguishable morphologically and are 30–40 μm in diameter, contain the oncosphere with six hooklets, and have a thick brown striated shell.
- Eggs can live for months to years on vegetation until they are ingested by cattle or other herbivores (T. saginata) or pigs (T. asiatica).
- After ingestion, the oncosphere egresses the egg, invades into the intestinal wall, and is distributed throughout the body via the bloodstream.
- The invasive larva transforms into the cysticercus (cystic forms) in muscle or viscera of the intermediate host.
- When raw or undercooked meat containing the larvae is ingested, the cysticercus evaginates and forms a tapeworm in the human intestines.
- The adult worm matures over several months to produce eggs.
- The proglottids or eggs are then shed intermittently with stool.
- T. solium resides primarily in the small intestines.
- The scolex attaches to the mucosa via sucking disks and the armed rostellum with two rows of hooklets.
- The mature tapeworm can reach a length of 3 m and have up to 1000 proglottids.
- Each mature proglottid may produce approximately 50,000 eggs.
- Proglottids are released from the terminal end of the tapeworm intermittently and excreted into the feces.
- The eggs are immediately infective for both humans and pigs.
- After ingestion of eggs by the intermediate host, the oncospheres are released, penetrate the intestinal wall, and are carried via the bloodstream to tissues.
- In the pig, larvae usually mature in striated muscle of the neck, tongue, and trunk.
- By 60–90 days, the invasive larvae transform into the encysted larval stage.
- In the pigs, cysticerci typically survive for months to years, until the pig is slaughtered.
- Humans develop intestinal tapeworm infections after ingestion of contaminated pork.
- Human cysticercosis follows ingestion of T. solium eggs.
- Transmission is associated with close contact with a tapeworm carrier.
- The eggs are sticky and may be found under the fingernails of tapeworm carriers.
- The tapeworm carrier can also infect themselves by ingestion of ova, likely via the fecal-oral route.
- The adult tapeworms of E. granulosus sensu lato are small (5 mm long) and live for 5–20 months in the small intestine of dogs.
- Each tapeworm has only three proglottids: one immature, one mature, and one gravid.
- The latter are shed and release eggs that are morphologically similar to Taenia eggs.
- Heavy infections of dogs with many tapeworms are common in endemic areas.
- When humans ingest the eggs, the invasive oncospheres are released from eggs, penetrate the intestinal mucosa, enter the portal circulation, and are carried mostly to the liver and lungs.
- However, virtually any organ can be infected including kidneys, spleen, heart, bone, and brain.
- Larvae of E. granulosus sensu lato develop into fluid-filled unilocular hydatid cysts.
- The wall of the cystic lesion consists of an external membrane and an inner germinal layer, which are surrounded by the host's adventitial layer that may contain different patterns of inflammation and fibrosis.
- Daughter cysts and germinating cystic structures called brood capsules develop from the inner aspect of the germinal layer.
- New organisms, called protoscolices, develop in large numbers within the brood capsule.
- A protoscolex is an invaginated scolex with the capacity to form an adult tapeworm if ingested by a definitive host or form a new cystic lesion if released in the intermediate host's tissues.
- The cysts expand slowly over a period of years and may contain thousands of protoscolices.
- E. multilocularis has a life cycle involving wild canines such as foxes or wolves, which are the main definitive hosts.
- Domestic dogs can also serve as definitive hosts of these tapeworms.
- Small rodents are the main intermediate hosts.
- Humans are dead-end intermediate hosts that develop alveolar echinococcosis.
- The larval stage of this parasite forms multilocular, small irregular cysts with proliferating and invasive capacity.
- The parasite larvae invade the host tissue by peripheral extension of processes from the germinal layer.
- These lesions do not contain brood capsules or protoscolices.
- R. nana is the only human cestode that does not require an intermediate host.
- Both the larval and adult stages coexist in the intestine of infected persons.
- The adult tapeworm is only ~2 cm long and lives in the human proximal ileum.
- The tiny proglottids are rarely seen in the stool.
- They release spherical eggs, 30–44 μm in diameter, containing the invasive larvae termed oncosphere, which has six hooklets.
- The eggs are immediately infective after leaving the host and survive for ≤10 days in the environment.
- After the eggs are ingested, the oncosphere is released, penetrates the intestinal villi, and develops into the cysticercoid larval form within the epithelium.
- After a few days, these larvae reenter the intestinal lumen, attach to the mucosa, and mature into adult tapeworms over 10–12 days.
- The life span of adult R. nana worms is typically ~4–10 weeks.
- However, infection is perpetuated by cycles of reinfection and autoinfection in which some eggs hatch in the intestinal lumen and form the cysticercoid larva without leaving the host.
4. CLINICAL FEATURES¶
- The symptoms and signs of paragonimiasis are fever, cough, hemoptysis, and peripheral eosinophilia.
- Some patients with paragonimiasis and low parasite burdens may remain relatively asymptomatic for prolonged periods or may have recurrent attacks of cough, sputum production, fever, and night sweats that mimic tuberculosis.
- Infective metacercariae may migrate to extrapulmonary sites such as the brain (cerebral paragonimiasis).
- Pulmonary paragonimiasis is diagnosed by detection of parasite ova in sputum and/or feces.
- Serology can be helpful in egg-negative cases and in cerebral paragonimiasis.
- Anamnestic information about the consumption of raw or undercooked freshwater crabs by immigrants, expatriates, and returning travelers—and, in the United States, the consumption of raw or undercooked crayfish from freshwater river systems where P. kellicotti is endemic—is important in patients presenting with fever, cough, hemoptysis, pleural effusions, and peripheral eosinophilia.
- Patients may be asymptomatic or may note passing proglottids in their feces.
- Patients may note the sensation of something moving while the motile proglottids of T. saginata are passed.
- Patients occasionally note abdominal pain or discomfort, nausea, change in appetite, or weakness.
- Weight loss is unusual.
- Intestinal infections (taeniasis) with T. solium are often asymptomatic.
- Some patients note passage of proglottids in stool.
- The proglottids are typically off-white in color and 1–3 cm in length, 0.5–1 cm wide, and about 1 mm thick.
- The clinical manifestations of cysticercosis are variable.
- Cysticerci can be found anywhere in the body but are commonly detected in the central nervous system (CNS), skeletal muscle, subcutaneous tissue, or the eye.
- The clinical manifestations of human cysticercosis vary with the location of the cysticerci as well as with the extent of associated inflammatory responses or scarring.
- The most common clinical manifestations are neurologic symptoms.
- Headache is common with all CNS forms of disease.
- Seizures are the most frequent clinical manifestation and are associated with inflammation of the brain parenchyma surrounding the cysticercus.
- Seizures may be focal, focal with secondary generalization, or generalized.
- Another common clinical manifestation is with symptoms of hydrocephalus, which may result from CSF flow obstruction by cysticerci and/or accompanying inflammation or communicating hydrocephalus from arachnoiditis.
- The symptoms of increased intracranial pressure may include headache, nausea and vomiting, dizziness, and ataxia.
- Patients with hydrocephalus may present with altered mental status or papilledema with altered visual acuity.
- Some patients present with intermittent acute hydrocephalus (termed Bruns' syndrome) associated with change in position due to the cysticercus working as a ball valve.
- Cysticerci at the base of the brain or in the subarachnoid space may cause chronic meningitis or arachnoiditis, communicating hydrocephalus, mass lesions, hemorrhages, or strokes.
- Patients often have CSF pleocytosis with a predominance of lymphocytes, neutrophils, or eosinophils.
- The protein level in CSF may be elevated; the glucose concentration is usually normal but can be markedly reduced.
- Symptoms of hepatic cystic echinococcosis may include abdominal fullness or pain or a palpable mass in the right upper quadrant.
- A palpable mass in the right upper quadrant may be present.
- Physical examination may reveal liver enlargement and obstructive jaundice.
- The lesions may infiltrate adjoining organs (e.g., diaphragm, kidneys, or lungs) or may metastasize to the spleen, lungs, or brain.
- Compression of a bile duct or leakage of cyst fluid into the biliary tree may present with symptoms mimicking cholelithiasis.
- Jaundice can result from biliary obstruction.
- Rupture of or leakage from a hydatid cyst may present more acutely with symptoms including fever, pruritus, urticaria, eosinophilia, or anaphylaxis.
- Cystic echinococcosis in the lungs may present with chronic cough, shortness of breath, chest pain, or hemoptysis.
- Rupture into the bronchial tree leads to sudden expectoration of the cyst fluid and membranes.
- Rupture into the pleural cavity may produce pleuritic chest pain and hydatid empyema.
- Rupture of hydatid cysts, which can occur spontaneously, after trauma, or during surgery, may lead to release of protoscolices into the patient's tissues, each of which can form new cysts.
- Hydatid disease may also involve bone (invasion of the medullary cavity with bony erosion producing pathologic fractures), the CNS (space-occupying lesions), the heart (conduction defects, pericarditis), and the pelvis (pelvic mass).
- E. multilocularis characteristically presents as a slow-growing hepatic mass, which typically presents decades after the initial infection.
- The lesions resemble tumors causing progressive destruction of the liver and extension into adjoining structures.
- Frequent symptoms include upper-quadrant and epigastric discomfort.
- R. nana infection is most often asymptomatic.
- However, infection may be associated with diarrhea, abdominal pain, and weight loss, particularly in children with the highest burden of infection.
4.1 Neurocysticercosis¶
- Neurologic infection can be classified based on the location and viability of the parasites.
- Involvement of the brain, spine, or cerebrospinal fluid (CSF) is termed neurocysticercosis.
- The clinical manifestations of human cysticercosis vary with the location of the cysticerci as well as with the extent of associated inflammatory responses or scarring.
- The most common clinical manifestations are neurologic symptoms.
- Headache is common with all CNS forms of disease.
- Seizures are the most frequent clinical manifestation and are associated with inflammation of the brain parenchyma surrounding the cysticercus.
- Seizures may be focal, focal with secondary generalization, or generalized.
- Another common clinical manifestation is with symptoms of hydrocephalus, which may result from CSF flow obstruction by cysticerci and/or accompanying inflammation or communicating hydrocephalus from arachnoiditis.
- The symptoms of increased intracranial pressure may include headache, nausea and vomiting, dizziness, and ataxia.
- Patients with hydrocephalus may present with altered mental status or papilledema with altered visual acuity.
- Some patients present with intermittent acute hydrocephalus (termed Bruns' syndrome) associated with change in position due to the cysticercus working as a ball valve.
- Cysticerci at the base of the brain or in the subarachnoid space may cause chronic meningitis or arachnoiditis, communicating hydrocephalus, mass lesions, hemorrhages, or strokes.
4.2 Echinococcosis¶
- The liver is involved in two-thirds of E. granulosus sensu lato infections and nearly all E. multilocularis infections.
- The lungs are involved in about 20% of E. granulosus sensu lato infections.
- The parasites are often discovered incidentally on a routine x-ray or ultrasound study prior to onset of symptoms.
- Symptoms of hepatic cystic echinococcosis may include abdominal fullness or pain or a palpable mass in the right upper quadrant.
- Physical examination may reveal liver enlargement and obstructive jaundice.
- The lesions may infiltrate adjoining organs (e.g., diaphragm, kidneys, or lungs) or may metastasize to the spleen, lungs, or brain.
- Compression of a bile duct or leakage of cyst fluid into the biliary tree may present with symptoms mimicking cholelithiasis.
- Jaundice can result from biliary obstruction.
- Rupture of or leakage from a hydatid cyst may present more acutely with symptoms including fever, pruritus, urticaria, eosinophilia, or anaphylaxis.
- Cystic echinococcosis in the lungs may present with chronic cough, shortness of breath, chest pain, or hemoptysis.
- Rupture into the bronchial tree leads to sudden expectoration of the cyst fluid and membranes.
- Rupture into the pleural cavity may produce pleuritic chest pain and hydatid empyema.
- Rupture of hydatid cysts, which can occur spontaneously, after trauma, or during surgery, may lead to release of protoscolices into the patient's tissues, each of which can form new cysts.
- Hydatid disease may also involve bone (invasion of the medullary cavity with bony erosion producing pathologic fractures), the CNS (space-occupying lesions), the heart (conduction defects, pericarditis), and the pelvis (pelvic mass).
- E. multilocularis characteristically presents as a slow-growing hepatic mass, which typically presents decades after the initial infection.
- The lesions resemble tumors causing progressive destruction of the liver and extension into adjoining structures.
- Frequent symptoms include upper-quadrant and epigastric discomfort.
5. DIFFERENTIAL DIAGNOSIS¶
- Paragonimiasis mimics tuberculosis.
- Neurocysticercosis must be distinguished from other pathologies producing similar neuroimaging findings.
- Echinococcosis must be distinguished from other cystic liver lesions and tumors.
- Taeniasis must be distinguished from other causes of intestinal tapeworms.
- R. nana infection must be distinguished from other causes of intestinal tapeworms.
6. INVESTIGATIONS & DIAGNOSIS¶
- Diagnosis depends on detection of eggs or proglottids in the stool.
- Eggs may not be found by stool examination but are sometimes only present in the perianal area; thus, when suspected, the perianal region should be examined with use of a cellophane-tape swab (as in pinworm infection).
- Antigen-detection assays are more sensitive than microscopic examination but are not commercially available.
- Distinguishing T. saginata or T. asiatica from T. solium requires examination of mature proglottids or the scolex or via molecular tests.
- Eosinophilia and elevated levels of serum IgE are usually absent.
- Diagnosis of tapeworm infection with T. solium is made by the demonstration of eggs or proglottids, as described for T. saginata.
- However, eggs and proglottids are only shed intermittently, limiting the sensitivity of direct testing.
- Antigen-capture enzyme-linked immunosorbent assay (ELISA), polymerase chain reaction (PCR), and serology for tapeworm stage-specific antigens are more sensitive but are only available as research techniques.
- The diagnosis of neurocysticercosis can be difficult since the symptoms are nonspecific and there is no readily available material for demonstration of the parasite.
- A group of international experts proposed revised diagnostic criteria (Table 242-1).
- The diagnosis is only certain with definite demonstration of the parasite (absolute criteria).
- Definitive diagnosis is possible with histologic observation of the parasite in excised tissue, by funduscopic visualization of the parasite in the subretinal or vitreous spaces of the eye, or by neuroimaging demonstrating a cystic lesion containing a characteristic scolex (Fig. 242-1).
- With high-resolution neuroimaging, the scolex can often be identified.
- In other cases, a clinical diagnosis is based on a combination of clinical presentation, radiographic studies, exposure or evidence demonstrating presence of the parasites by antigen-detection, quantitative PCR, or even next-generation sequencing in spinal fluid.
- Neuroimaging is the primary major diagnostic method (Fig. 242-1).
- Demonstration of a cystic lesion with a mural nodule consistent with a scolex ('dot-in-hole') is diagnostic.
- Major findings include cystic lesions with or without enhancement (e.g., ring enhancement), one or more nodular calcifications (which may also have associated edema or enhancement), focal enhancing lesions, or cystic lesions in the subarachnoid space.
- Cysticerci in the brain parenchyma are usually 5–20 mm in diameter and round.
- Cystic lesions in the subarachnoid space or fissures may enlarge up to 6 cm in diameter and may be lobulated.
- The cyst wall for cysticerci in the subarachnoid space or ventricles is usually very thin, and the cyst fluid is often isodense with CSF.
- Thus, obstructive hydrocephalus or enhancement of the basilar meninges may be the only finding on computed tomography (CT) in extraparenchymal neurocysticercosis.
- However, since these findings are less specific, they are considered only minor criteria.
- Cysticerci in the ventricles or subarachnoid space are more readily identified by magnetic resonance imaging (MRI), especially fast imaging employing steady-state acquisition (FIESTA) or three-dimensional constructive interference in steady state (3D CISS).
- CT is more sensitive than MRI in identifying calcified lesions, whereas MRI is more sensitive than CT for identifying small cystic lesions, scolexes, and enhancement.
- Spontaneous resolution, resolution after albendazole therapy, or mobile cystic lesions within the ventricles are findings that can support the diagnosis of neurocysticercosis.
- Exposure history significantly modifies the interpretation of neuroimaging studies.
- Detection of specific antibodies to or antigens of T. solium are major exposure criteria.
- Antibody tests using unfractionated antigens (e.g., ELISAs using crude parasite antigen) have high rates of false-positive and false-negative results and should be avoided.
- An immunoblot assay (enzyme-linked immunoelectrotransfer blot [EITB]) using lentil lectin–purified glycoproteins is >99% specific and sensitive in patients with multiple cysts.
- However, patients with single cysticercosis or intracranial lesions or with calcifications may be seronegative.
- Serum samples are more sensitive than CSF using EITB.
- Each of the diagnostic antigens has been cloned, and assays using recombinant or synthetic antigens are in development.
- Assays using monoclonal antibodies to detect parasite antigen in the blood, CSF, or urine may also facilitate diagnosis and patient follow-up.
- Antigen-detection assays are currently the available commercially in Europe but not in the United States.
- More recently, real-time PCR has been employed for diagnosis and follow-up of extraparenchymal disease.
- Other major clinical/exposure criteria for neurocysticercosis include the presence of cysticerci outside the CNS (e.g., typical cigar-shaped calcifications in muscle) or exposure to a tapeworm carrier or a household member infected with T. solium.
- Minor clinical/exposure criteria include residence in an endemic village or clinical symptoms suggestive of neurocysticercosis (e.g., seizures or obstructive hydrocephalus).
- Studies from India validated clinical criteria for diagnosis in selected cases.
- In patients from endemic areas who had single enhancing lesions presenting with seizures, a normal physical examination, and no evidence of systemic disease (e.g., no fever, adenopathy, or chest radiographic abnormalities), the presence on CT of round lesions 5–20 mm in diameter with no midline shift was almost always caused by neurocysticercosis.
- Definite or probable diagnosis can be made using the criteria and combinations of criteria listed in the footnote of Table 242-1.
- For cystic echinococcosis disease, a definitive diagnosis can also be made by the examination of aspirated fluids for protoscolices and/or hooklets.
- However, due to the potential risk of fluid leakage resulting in either dissemination of infection or, more rarely, anaphylactic reactions, aspiration should only be performed by experienced interventionists and following the precautions used for percutaneous treatment (see below).
- Serodiagnostic assays can be useful, but current serologic tests are insensitive and cannot be used to exclude the diagnosis of echinococcosis.
- ELISA and immunoblot assays for specific antibody are positive in ~90% of cases of hydatid liver disease.
- By contrast, the sensitivity is only ~50% for patients with cysts in the lungs.
- Imaging studies are the main diagnostic methods to detect and evaluate echinoccal cysts.
- Chest x-ray or CT can identify pulmonary cysts due to E. granulosus sensu lato, which appear as rounded masses of uniform density (Fig. 242-2).
- Ultrasound, CT, or MRI can be used to identify cystic echinococcosis lesions in solid organs of the abdomen, particularly in the liver.
- The ultrasound classification proposed by the World Health Organization Informal Working Group on Echinococcosis has diagnostic and management applications for liver cystic echinococcosis (Figs. 242-2 and 242-3).
- MRI can also be used to classify lesions.
- MRI and CT may be more useful than ultrasound to evaluate the presence of cyst complications, such as communication with the biliary tree, that preclude some management options.
- Imaging of cystic echinococcosis shows well-defined cysts walls and, in some cases, internal trabeculation, dense cyst material, and/or calcifications (Fig. 242-3).
- In some cases, the protoscolices and brood capsules of E. granulosus complex may be visible within the cysts as fine particles termed hydatid sand.
- Identification of daughter cysts within the larger cyst is diagnostic of cystic echinococcosis disease.
- Eggshell or mural calcification on CT is also diagnostic of E. granulosus infection.
- In contrast, ultrasound or CT of alveolar hydatid cysts often reveals an indistinct solid mass.
- Some cases will display central necrosis or plaque-like calcifications.
- Infection is diagnosed by finding the characteristic R. nana eggs in microscopy of the stool.
6.1 Neurocysticercosis Diagnostic Criteria¶
- Diagnosis is confirmed by one absolute criterion, by two major criteria or one major and one confirmatory neuroimaging criteria plus any clinical/exposure criterion, or by one major neuroimaging criterion plus two clinical/exposure criteria (including at least one major clinical/exposure criterion), together with the exclusion of other pathologies producing similar neuroimaging findings.
- A probable diagnosis is supported by one major neuroimaging criterion plus any two clinical/exposure criteria or by one minor neuroimaging criterion plus at least one major clinical/exposure criterion.
Table 1 — Table 242-1 Revised Diagnostic Criteria for Neurocysticercosis¶
| Category | Criteria | ||
|---|---|---|---|
| 1. Absolute criteria | a. Histologic demonstration of the parasite from biopsy of a brain or spinal cord lesion | b. Visualization of subretinal cysticercus | c. Conclusive demonstration of a scolex with a cystic lesion on neuroimaging studies |
| 2. Neuroimaging criteria | a. Major neuroimaging criteria: Cystic lesions without a discernible scolex, typical small enhancing lesions, multilobulated cystic lesions in the subarachnoid space, typical parenchymal brain calcifications | b. Confirmative neuroimaging criteria: Resolution of cystic lesions spontaneously or after cysticidal drug therapy; Migration of ventricular cysts documented on sequential neuroimaging studies | c. Minor neuroimaging criteria: Obstructive hydrocephalus or abnormal enhancement of basal leptomeninges |
| 3. Clinical/exposure criteria | a. Major clinical/exposure criteria: Detection of specific anticysticercal antibodies (e.g., by enzyme-linked immunoelectrotransfer blot [EITB]) or cysticercal antigens by well-standardized immunodiagnostic tests; Cysticercosis outside the central nervous system; Evidence of a household contact with T. solium infection | b. Minor clinical/exposure criteria: Clinical manifestations suggestive of neurocysticercosis; Individuals coming from or living in an area where cysticercosis is endemic |
6.2 Echinococcosis Imaging Classification¶
- Staging is done by imaging studies including ultrasound, CT, or MRI and includes lesions classified as active, transitional, and inactive.
- Active cysts include types CL (with a cystic lesion and no visible cyst wall), CE1 (with a visible cyst wall and internal echoes [snowflake sign]), and CE2 (with a visible cyst wall and internal septation).
- Transitional cysts may have detached laminar membranes (CE3a) or may be partially collapsed (CE3b).
- Inactive cysts include types CE4 (a nonhomogeneous mass) and CE5 (a cyst with a thick calcified wall).
Table 2 — Table 242-2 WHO Classification of Cystic Echinococcosis¶
| Stage | Description |
|---|---|
| CL | Cystic lesion and no visible cyst wall |
| CE1 | Visible cyst wall and internal echoes (snowflake sign) |
| CE2 | Visible cyst wall and internal septation |
| CE3a | Detached laminar membranes |
| CE3b | Partially collapsed |
| CE4 | Nonhomogeneous mass |
| CE5 | Cyst with a thick calcified wall |
7. MANAGEMENT & TREATMENT¶
- Food-Borne Trematode Infections: Praziquantel and triclabendazole are the two drugs of choice.
- All confirmed cases of human paragonimiasis should be treated with praziquantel (Table 241-2) to avoid the complications of extrapulmonary disease.
- Surgical management may be needed for pulmonary or cerebral lesions.
- Taeniasis saginata and Taeniasis asiatica: A single dose of praziquantel (10 mg/kg) is highly effective.
- Niclosamide (adult dose, 2 g; 1 g for children weighing 11−34 kg) is also effective but is less available.
- Nitazoxanide can also be used.
- Taeniasis solium and Cysticercosis: Tapeworm infection by T. solium infection is treated with a single dose of praziquantel (10 mg/kg).
- However, praziquantel may occasionally trigger an inflammatory response in the CNS if concomitant cryptic cysticercosis is present.
- Niclosamide (2 g) is also effective but is not as widely available.
- Initial management of neurocysticercosis should focus on treatment of seizures or hydrocephalus.
- Seizures can be controlled with antiseizure medications.
- Seizure medications can usually be tapered after 6 months in patients with single enhancing lesions in whom imaging normalizes and in whom there are no breakthrough seizures.
- Subjects with multiple parenchymal lesions require more prolonged therapy.
- However, antiseizure medications can often be tapered off after 2 years if lesions resolve without development of calcifications and patients remain free of seizures.
- Patients with calcified lesions are at higher risk of recurrent seizures, especially if the lesions are associated with perilesional edema or enhancement.
- For patients with hydrocephalus, the reduction of intracranial pressure should be the priority of the initial therapy.
- Patients with cysticerci in the cerebral ventricles typically present with obstructive hydrocephalus, and the preferred approach is removal of the cysticercus via neurosurgery.
- Cysticerci in the lateral or third ventricles should be removed via neuroendoscopy.
- Antiparasitic drugs make the cysticerci more friable and should be avoided prior to surgery.
- The cysticerci in the fourth ventricle can be approached by microdissection using a posterior approach or, in some cases, via neuroendoscopy.
- When complete removal of the cysticercus is not possible, a diverting procedure, such as ventriculoperitoneal shunting, can be used to manage hydrocephalus.
- Historically, shunt failure was a major problem.
- The risk of shunt failure may be limited by administration of antiparasitic drugs and glucocorticoids.
- Antiparasitic drug treatment is never an emergency in neurocysticercosis and should wait until patients are stabilized with antiseizure and anti-inflammatory medications and exclusion of intraocular disease.
- Antiparasitics do not hasten resolution of neuroradiologic abnormalities in parenchymal neurocysticercosis.
- Clinical benefits consist mainly of decreasing the number of recurrent generalized seizures.
- In viable parenchymal cysticercosis, most authorities recommend antiparasitic drugs, especially albendazole (15 mg/kg per day for 8–28 days).
- A combination of albendazole and praziquantel (50 mg/kg per day) is more effective in patients with more than two cystic lesions.
- A longer course or combination therapy is needed in patients with multiple subarachnoid cysticerci.
- Both antiparasitic agents may exacerbate the inflammatory response around the dying parasite, thereby exacerbating seizures or hydrocephalus.
- Patients receiving these drugs should be carefully monitored.
- High-dose glucocorticoids should always be used during treatment (e.g., dexamethasone 0.1–0.4 mg/kg per day or prednisone 60 mg/d).
- For patients with subarachnoid cysts or giant cysticerci, anti-inflammatory medications such as glucocorticoids are needed to reduce arachnoiditis and accompanying vasculitis.
- Most authorities recommend prolonged courses of antiparasitic drugs as well as shunting when hydrocephalus is present.
- Patients typically require prolonged anti-inflammatory treatment along with antiparasitics.
- Methotrexate and, in some cases, tumor necrosis factor inhibitors produce cystic hydatid disease or cystic echinococcosis, which are prevalent worldwide in most areas where livestock is raised in association with dogs.
- In patients with diffuse cerebral edema and elevated intracranial pressure due to multiple inflamed parenchymal lesions, glucocorticoids are the mainstay of therapy, and antiparasitic drugs should be avoided.
- For ocular and spinal lesions, drug-induced inflammation may cause irreversible damage.
- Intraocular disease should be managed surgically.
- Recent data suggest that spinal disease is best managed using both medical and surgical therapy.
- Prevention of T. solium tapeworm infection consists of precautions in handling pork, as described for T. asiatica, and thoroughly cooking or freezing pork to destroy the cysticerci.
- Pork inspections and condemnation of infected meat prevent transmission.
- The prevention of cysticercosis involves good personal hygiene including handwashing, effective disposal of feces, and treatment and prevention of human intestinal infections.
- Optimal eradication programs to eradicate T. solium in endemic areas include mass chemotherapy administered to human and porcine populations and vaccinations of pigs.
- A vaccine for porcine infection is licensed in India and a few other countries.
- For cystic echinococcosis disease, optimal treatment varies depending on the size, stage, location, and clinical manifestations of cysts.
- In the past, surgery was the main treatment method, but numerous studies have demonstrated that other treatment modalities may be just as effective and lead to less morbidity.
- Staging is recommended for cystic echinococcosis of the liver, which allows assessment of the cyst size and viability (Fig. 242-3).
- CL, CE1, and CE3a lesions 10 cm), or superficial cysts, which are more likely to rupture and spill protoscolices.
- Albendazole (15 mg/kg daily in two divided doses) should be initiated at least 2 days before the procedure and continued for at least 4 weeks afterward.
- Fine-needle ultrasound or CT-guided aspiration should enter the cyst through solid tissues to limit spillage of cyst fluid.
- Aspiration can confirm the diagnosis by microscopic demonstration of protoscolices or hooks.
- After aspiration, bilirubin should be measured in the cyst fluid using a dipstick, or contrast material should be injected to detect occult communications with the biliary tract.
- If no bile is found and no communication is visualized, instillation of scolicidal agents (usually hypertonic saline) and reaspiration are performed.
- PAIR, when performed by a skilled practitioner, results in cure and relapse rates equivalent to surgery, with less perioperative morbidity and shorter hospitalization.
- In some centers, CE2 lesions have been treated by modified catheter drainage, including puncture of each daughter cyst within the primary cyst.
- Patients with treatment failure can often be treated again successfully with PAIR or additional courses of medical therapy.
- Response to treatment is best assessed by serial imaging studies, with attention to cyst size and consistency.
- Cysts may not demonstrate complete radiologic resolution even though no viable protoscolices are present.
- Those cysts classified as CE4 or CE5 are considered nonviable and require periodic reevaluations to assess for reactivation.
- Surgery remains the treatment of choice for complicated cystic echinococcosis (e.g., cysts communicating with the biliary tract), for most thoracic and intracranial cysts, and when PAIR is not possible.
- Liver cysts should be removed via a pericystectomy, in which the entire cyst and the surrounding fibrous tissue are removed to prevent spillage and recurrence.
- Recent reports demonstrate that, in experienced hands, cysts can often be safely removed by laparoscopic or robotic surgery.
- The risks posed by leakage of fluid during surgery or PAIR include anaphylaxis and dissemination of protoscolices.
- Spillage can be minimized by careful dissection and using surgical draping soaked in hypertonic saline.
- Infusion of scolicidal agents is no longer recommended because of problems with hypernatremia, intoxication, or sclerosing cholangitis.
- Albendazole should be administered adjunctively, beginning several days to weeks before resection of the liver cyst and continuing for several weeks afterwards.
- Surgical resection is required to attempt cure of E. multilocularis disease.
- Complete removal of the parasite continues to offer the best chance for cure.
- Patients who have undergone presumed curative resection should be treated with albendazole for at least 2 years after presumptively curative surgery.
- Positron emission tomography can be used to follow disease activity.
- Unfortunately, most cases are only diagnosed at a stage in which complete resection is impossible; in these cases, albendazole treatment should be continued indefinitely, with careful monitoring.
- In some cases of larger lesions, complete removal of the liver followed by liver transplantation has been performed.
- R. nana Infection: The treatment of choice for R. nana is praziquantel (25 mg/kg once), which is active against both the adult worms and the cysticercoids in the intestinal wall.
- Nitazoxanide (500 mg twice a day for 3 days) has been used as an alternative treatment.
- Hymenolepiasis diminuta: Infection is diagnosed by detection of eggs.
7.1 Neurocysticercosis Management¶
- Initial management of neurocysticercosis should focus on treatment of seizures or hydrocephalus.
- Seizures can be controlled with antiseizure medications.
- Seizure medications can usually be tapered after 6 months in patients with single enhancing lesions in whom imaging normalizes and in whom there are no breakthrough seizures.
- Subjects with multiple parenchymal lesions require more prolonged therapy.
- However, antiseizure medications can often be tapered off after 2 years if lesions resolve without development of calcifications and patients remain free of seizures.
- Patients with calcified lesions are at higher risk of recurrent seizures, especially if the lesions are associated with perilesional edema or enhancement.
- For patients with hydrocephalus, the reduction of intracranial pressure should be the priority of the initial therapy.
- Patients with cysticerci in the cerebral ventricles typically present with obstructive hydrocephalus, and the preferred approach is removal of the cysticercus via neurosurgery.
- Cysticerci in the lateral or third ventricles should be removed via neuroendoscopy.
- Antiparasitic drugs make the cysticerci more friable and should be avoided prior to surgery.
- The cysticerci in the fourth ventricle can be approached by microdissection using a posterior approach or, in some cases, via neuroendoscopy.
- When complete removal of the cysticercus is not possible, a diverting procedure, such as ventriculoperitoneal shunting, can be used to manage hydrocephalus.
- Historically, shunt failure was a major problem.
- The risk of shunt failure may be limited by administration of antiparasitic drugs and glucocorticoids.
- Antiparasitic drug treatment is never an emergency in neurocysticercosis and should wait until patients are stabilized with antiseizure and anti-inflammatory medications and exclusion of intraocular disease.
- Antiparasitics do not hasten resolution of neuroradiologic abnormalities in parenchymal neurocysticercosis.
- Clinical benefits consist mainly of decreasing the number of recurrent generalized seizures.
- In viable parenchymal cysticercosis, most authorities recommend antiparasitic drugs, especially albendazole (15 mg/kg per day for 8–28 days).
- A combination of albendazole and praziquantel (50 mg/kg per day) is more effective in patients with more than two cystic lesions.
- A longer course or combination therapy is needed in patients with multiple subarachnoid cysticerci.
- Both antiparasitic agents may exacerbate the inflammatory response around the dying parasite, thereby exacerbating seizures or hydrocephalus.
- Patients receiving these drugs should be carefully monitored.
- High-dose glucocorticoids should always be used during treatment (e.g., dexamethasone 0.1–0.4 mg/kg per day or prednisone 60 mg/d).
- For patients with subarachnoid cysts or giant cysticerci, anti-inflammatory medications such as glucocorticoids are needed to reduce arachnoiditis and accompanying vasculitis.
- Most authorities recommend prolonged courses of antiparasitic drugs as well as shunting when hydrocephalus is present.
- Patients typically require prolonged anti-inflammatory treatment along with antiparasitics.
- Methotrexate and, in some cases, tumor necrosis factor inhibitors produce cystic hydatid disease or cystic echinococcosis, which are prevalent worldwide in most areas where livestock is raised in association with dogs.
- In patients with diffuse cerebral edema and elevated intracranial pressure due to multiple inflamed parenchymal lesions, glucocorticoids are the mainstay of therapy, and antiparasitic drugs should be avoided.
- For ocular and spinal lesions, drug-induced inflammation may cause irreversible damage.
- Intraocular disease should be managed surgically.
- Recent data suggest that spinal disease is best managed using both medical and surgical therapy.
7.2 Echinococcosis Management¶
- Optimal treatment of cystic echinococcosis varies depending on the size, stage, location, and clinical manifestations of cysts.
- In the past, surgery was the main treatment method, but numerous studies have demonstrated that other treatment modalities may be just as effective and lead to less morbidity.
- Staging is recommended for cystic echinococcosis of the liver, which allows assessment of the cyst size and viability (Fig. 242-3).
- CL, CE1, and CE3a lesions 10 cm), or superficial cysts, which are more likely to rupture and spill protoscolices.
- Albendazole (15 mg/kg daily in two divided doses) should be initiated at least 2 days before the procedure and continued for at least 4 weeks afterward.
- Fine-needle ultrasound or CT-guided aspiration should enter the cyst through solid tissues to limit spillage of cyst fluid.
- Aspiration can confirm the diagnosis by microscopic demonstration of protoscolices or hooks.
- After aspiration, bilirubin should be measured in the cyst fluid using a dipstick, or contrast material should be injected to detect occult communications with the biliary tract.
- If no bile is found and no communication is visualized, instillation of scolicidal agents (usually hypertonic saline) and reaspiration are performed.
- PAIR, when performed by a skilled practitioner, results in cure and relapse rates equivalent to surgery, with less perioperative morbidity and shorter hospitalization.
- In some centers, CE2 lesions have been treated by modified catheter drainage, including puncture of each daughter cyst within the primary cyst.
- Patients with treatment failure can often be treated again successfully with PAIR or additional courses of medical therapy.
- Response to treatment is best assessed by serial imaging studies, with attention to cyst size and consistency.
- Cysts may not demonstrate complete radiologic resolution even though no viable protoscolices are present.
- Those cysts classified as CE4 or CE5 are considered nonviable and require periodic reevaluations to assess for reactivation.
- Surgery remains the treatment of choice for complicated cystic echinococcosis (e.g., cysts communicating with the biliary tract), for most thoracic and intracranial cysts, and when PAIR is not possible.
- Liver cysts should be removed via a pericystectomy, in which the entire cyst and the surrounding fibrous tissue are removed to prevent spillage and recurrence.
- Recent reports demonstrate that, in experienced hands, cysts can often be safely removed by laparoscopic or robotic surgery.
- The risks posed by leakage of fluid during surgery or PAIR include anaphylaxis and dissemination of protoscolices.
- Spillage can be minimized by careful dissection and using surgical draping soaked in hypertonic saline.
- Infusion of scolicidal agents is no longer recommended because of problems with hypernatremia, intoxication, or sclerosing cholangitis.
- Albendazole should be administered adjunctively, beginning several days to weeks before resection of the liver cyst and continuing for several weeks afterwards.
- Surgical resection is required to attempt cure of E. multilocularis disease.
- Complete removal of the parasite continues to offer the best chance for cure.
- Patients who have undergone presumed curative resection should be treated with albendazole for at least 2 years after presumptively curative surgery.
- Positron emission tomography can be used to follow disease activity.
- Unfortunately, most cases are only diagnosed at a stage in which complete resection is impossible; in these cases, albendazole treatment should be continued indefinitely, with careful monitoring.
- In some cases of larger lesions, complete removal of the liver followed by liver transplantation has been performed.
7.3 Drug Therapy¶
- Food-Borne Trematode Infections: Praziquantel and triclabendazole are the two drugs of choice.
- All confirmed cases of human paragonimiasis should be treated with praziquantel (Table 241-2) to avoid the complications of extrapulmonary disease.
- Surgical management may be needed for pulmonary or cerebral lesions.
- Taeniasis saginata and Taeniasis asiatica: A single dose of praziquantel (10 mg/kg) is highly effective.
- Niclosamide (adult dose, 2 g; 1 g for children weighing 11−34 kg) is also effective but is less available.
- Nitazoxanide can also be used.
- Taeniasis solium and Cysticercosis: Tapeworm infection by T. solium infection is treated with a single dose of praziquantel (10 mg/kg).
- However, praziquantel may occasionally trigger an inflammatory response in the CNS if concomitant cryptic cysticercosis is present.
- Niclosamide (2 g) is also effective but is not as widely available.
- R. nana Infection: The treatment of choice for R. nana is praziquantel (25 mg/kg once), which is active against both the adult worms and the cysticercoids in the intestinal wall.
- Nitazoxanide (500 mg twice a day for 3 days) has been used as an alternative treatment.
- Echinococcosis: Albendazole (15 mg/kg daily in two divided doses) should be initiated at least 2 days before the procedure and continued for at least 4 weeks afterward.
- A combination of albendazole and praziquantel (50 mg/kg per day) is more effective in patients with more than two cystic lesions.
- A longer course or combination therapy is needed in patients with multiple subarachnoid cysticerci.
- Both antiparasitic agents may exacerbate the inflammatory response around the dying parasite, thereby exacerbating seizures or hydrocephalus.
- Patients receiving these drugs should be carefully monitored.
- High-dose glucocorticoids should always be used during treatment (e.g., dexamethasone 0.1–0.4 mg/kg per day or prednisone 60 mg/d).
- For patients with subarachnoid cysts or giant cysticerci, anti-inflammatory medications such as glucocorticoids are needed to reduce arachnoiditis and accompanying vasculitis.
- Most authorities recommend prolonged courses of antiparasitic drugs as well as shunting when hydrocephalus is present.
- Patients typically require prolonged anti-inflammatory treatment along with antiparasitics.
8. PROGNOSIS & COMPLICATIONS¶
- Cysts may not demonstrate complete radiologic resolution even though no viable protoscolices are present.
- Those cysts classified as CE4 or CE5 are considered nonviable and require periodic reevaluations to assess for reactivation.
- Patients with calcified lesions are at higher risk of recurrent seizures, especially if the lesions are associated with perilesional edema or enhancement.
- The risk of shunt failure may be limited by administration of antiparasitic drugs and glucocorticoids.
- Infusion of scolicidal agents is no longer recommended because of problems with hypernatremia, intoxication, or sclerosing cholangitis.
- The risks posed by leakage of fluid during surgery or PAIR include anaphylaxis and dissemination of protoscolices.
- Spontaneous resolution, resolution after albendazole therapy, or mobile cystic lesions within the ventricles are findings that can support the diagnosis of neurocysticercosis.
- E. multilocularis characteristically presents as a slow-growing hepatic mass, which typically presents decades after the initial infection.
- The lesions resemble tumors causing progressive destruction of the liver and extension into adjoining structures.
- Frequent symptoms include upper-quadrant and epigastric discomfort.
9. SPECIAL CONSIDERATIONS¶
- Prevention of T. solium tapeworm infection consists of precautions in handling pork, as described for T. asiatica, and thoroughly cooking or freezing pork to destroy the cysticerci.
- Pork inspections and condemnation of infected meat prevent transmission.
- The prevention of cysticercosis involves good personal hygiene including handwashing, effective disposal of feces, and treatment and prevention of human intestinal infections.
- Optimal eradication programs to eradicate T. solium in endemic areas include mass chemotherapy administered to human and porcine populations and vaccinations of pigs.
- A vaccine for porcine infection is licensed in India and a few other countries.
- Prevention of T. solium tapeworm infection consists of precautions in handling pork, as described for T. asiatica, and thoroughly cooking or freezing pork to destroy the cysticerci.
- Pork inspections and condemnation of infected meat prevent transmission.
- The prevention of cysticercosis involves good personal hygiene including handwashing, effective disposal of feces, and treatment and prevention of human intestinal infections.
- Optimal eradication programs to eradicate T. solium in endemic areas include mass chemotherapy administered to human and porcine populations and vaccinations of pigs.
- A vaccine for porcine infection is licensed in India and a few other countries.
- Since R. nana is acquired by the fecal-oral route, improved sanitation and personal hygiene can be used to eliminate infection.
- Hand washing in the household and school is important.
- Mass chemotherapy and improved hygiene have been used to control epidemics.
10. KEY PEARLS & CLINICAL TRAPS¶
- Neurocysticercosis diagnosis relies on imaging visualization of a scolex ('dot-in-hole') or specific serology (EITB); calcified lesions do not require antiparasitic therapy.
- Management of neurocysticercosis prioritizes seizure control and hydrocephalus management before initiating antiparasitic drugs to avoid worsening inflammation.
- Echinococcosis treatment is guided by WHO imaging classification (CE1-CE5); PAIR (aspiration, instillation, reaspiration) is preferred for small liver cysts, while surgery is required for multilocular disease.
- Paragonimiasis mimics tuberculosis; diagnosis requires detection of eggs in sputum/feces and history of raw freshwater crab consumption.
- Taenia solium eggs are immediately infective for humans; autoinfection can occur via ingestion of eggs from one's own feces.
- R. nana infection is unique among human cestodes as it does not require an intermediate host and causes autoinfection.
- Echinococcal cyst rupture can cause anaphylaxis; aspiration should only be performed by experienced practitioners with precautions.
- Diagnostic criteria for neurocysticercosis (Del Brutto) require one absolute criterion or specific combinations of major/minor neuroimaging and clinical/exposure criteria.
- Prevention of Taenia solium infection involves adequate cooking of pork (56°C for 5 min) or freezing at -10°C for 9 days.
- Calcified lesions in neurocysticercosis do not require antiparasitic treatment.
11. WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- Demonstration of a cystic lesion with a mural nodule consistent with a scolex ('dot-in-hole') is diagnostic for neurocysticercosis.
- Cysticerci in the brain parenchyma are usually 5–20 mm in diameter and round.
- Cystic lesions in the subarachnoid space or fissures may enlarge up to 6 cm in diameter and may be lobulated.
- The cyst wall for cysticerci in the subarachnoid space or ventricles is usually very thin, and the cyst fluid is often isodense with CSF.
- Identification of daughter cysts within the larger cyst is diagnostic of cystic echinococcosis disease.
- Eggshell or mural calcification on CT is also diagnostic of E. granulosus infection.
- In contrast, ultrasound or CT of alveolar hydatid cysts often reveals an indistinct solid mass.
- Some cases will display central necrosis or plaque-like calcifications.
- For cystic echinococcosis disease, a definitive diagnosis can also be made by the examination of aspirated fluids for protoscolices and/or hooklets.
- In patients from endemic areas who had single enhancing lesions presenting with seizures, a normal physical examination, and no evidence of systemic disease (e.g., no fever, adenopathy, or chest radiographic abnormalities), the presence on CT of round lesions 5–20 mm in diameter with no midline shift was almost always caused by neurocysticercosis.
- An immunoblot assay (enzyme-linked immunoelectrotransfer blot [EITB]) using lentil lectin–purified glycoproteins is >99% specific and sensitive in patients with multiple cysts.
- However, patients with single cysticercosis or intracranial lesions or with calcifications may be seronegative.
- Serum samples are more sensitive than CSF using EITB.
- Each of the diagnostic antigens has been cloned, and assays using recombinant or synthetic antigens are in development.
- Assays using monoclonal antibodies to detect parasite antigen in the blood, CSF, or urine may also facilitate diagnosis and patient follow-up.
- Antigen-detection assays are currently the available commercially in Europe but not in the United States.
- More recently, real-time PCR has been employed for diagnosis and follow-up of extraparenchymal disease.
- Other major clinical/exposure criteria for neurocysticercosis include the presence of cysticerci outside the CNS (e.g., typical cigar-shaped calcifications in muscle) or exposure to a tapeworm carrier or a household member infected with T. solium.
- Minor clinical/exposure criteria include residence in an endemic village or clinical symptoms suggestive of neurocysticercosis (e.g., seizures or obstructive hydrocephalus).
- Studies from India validated clinical criteria for diagnosis in selected cases.
- Infection is diagnosed by finding the characteristic R. nana eggs in microscopy of the stool.
12. WHAT EXCLUDES THE DIAGNOSIS¶
- Diagnosis is only certain with definite demonstration of the parasite (absolute criteria).
- Definitive diagnosis is possible with histologic observation of the parasite in excised tissue, by funduscopic visualization of the parasite in the subretinal or vitreous spaces of the eye, or by neuroimaging demonstrating a cystic lesion containing a characteristic scolex (Fig. 242-1).
- With high-resolution neuroimaging, the scolex can often be identified.
- In other cases, a clinical diagnosis is based on a combination of clinical presentation, radiographic studies, exposure or evidence demonstrating presence of the parasites by antigen-detection, quantitative PCR, or even next-generation sequencing in spinal fluid.
- Neuroimaging is the primary major diagnostic method (Fig. 242-1).
- Demonstration of a cystic lesion with a mural nodule consistent with a scolex ('dot-in-hole') is diagnostic.
- Major findings include cystic lesions with or without enhancement (e.g., ring enhancement), one or more nodular calcifications (which may also have associated edema or enhancement), focal enhancing lesions, or cystic lesions in the subarachnoid space.
- Cysticerci in the brain parenchyma are usually 5–20 mm in diameter and round.
- Cystic lesions in the subarachnoid space or fissures may enlarge up to 6 cm in diameter and may be lobulated.
- The cyst wall for cysticerci in the subarachnoid space or ventricles is usually very thin, and the cyst fluid is often isodense with CSF.
- Thus, obstructive hydrocephalus or enhancement of the basilar meninges may be the only finding on computed tomography (CT) in extraparenchymal neurocysticercosis.
- However, since these findings are less specific, they are considered only minor criteria.
- Cysticerci in the ventricles or subarachnoid space are more readily identified by magnetic resonance imaging (MRI), especially fast imaging employing steady-state acquisition (FIESTA) or three-dimensional constructive interference in steady state (3D CISS).
- CT is more sensitive than MRI in identifying calcified lesions, whereas MRI is more sensitive than CT for identifying small cystic lesions, scolexes, and enhancement.
- Spontaneous resolution, resolution after albendazole therapy, or mobile cystic lesions within the ventricles are findings that can support the diagnosis of neurocysticercosis.
- Exposure history significantly modifies the interpretation of neuroimaging studies.
- Detection of specific antibodies to or antigens of T. solium are major exposure criteria.
- Antibody tests using unfractionated antigens (e.g., ELISAs using crude parasite antigen) have high rates of false-positive and false-negative results and should be avoided.
- An immunoblot assay (enzyme-linked immunoelectrotransfer blot [EITB]) using lentil lectin–purified glycoproteins is >99% specific and sensitive in patients with multiple cysts.
- However, patients with single cysticercosis or intracranial lesions or with calcifications may be seronegative.
- Serum samples are more sensitive than CSF using EITB.
- Each of the diagnostic antigens has been cloned, and assays using recombinant or synthetic antigens are in development.
- Assays using monoclonal antibodies to detect parasite antigen in the blood, CSF, or urine may also facilitate diagnosis and patient follow-up.
- Antigen-detection assays are currently the available commercially in Europe but not in the United States.
- More recently, real-time PCR has been employed for diagnosis and follow-up of extraparenchymal disease.
- Other major clinical/exposure criteria for neurocysticercosis include the presence of cysticerci outside the CNS (e.g., typical cigar-shaped calcifications in muscle) or exposure to a tapeworm carrier or a household member infected with T. solium.
- Minor clinical/exposure criteria include residence in an endemic village or clinical symptoms suggestive of neurocysticercosis (e.g., seizures or obstructive hydrocephalus).
- Studies from India validated clinical criteria for diagnosis in selected cases.
- In patients from endemic areas who had single enhancing lesions presenting with seizures, a normal physical examination, and no evidence of systemic disease (e.g., no fever, adenopathy, or chest radiographic abnormalities), the presence on CT of round lesions 5–20 mm in diameter with no midline shift was almost always caused by neurocysticercosis.
- Definite or probable diagnosis can be made using the criteria and combinations of criteria listed in the footnote of Table 242-1.
- For cystic echinococcosis disease, a definitive diagnosis can also be made by the examination of aspirated fluids for protoscolices and/or hooklets.
- However, due to the potential risk of fluid leakage resulting in either dissemination of infection or, more rarely, anaphylactic reactions, aspiration should only be performed by experienced interventionists and following the precautions used for percutaneous treatment (see below).
- Serodiagnostic assays can be useful, but current serologic tests are insensitive and cannot be used to exclude the diagnosis of echinococcosis.
- ELISA and immunoblot assays for specific antibody are positive in ~90% of cases of hydatid liver disease.
- By contrast, the sensitivity is only ~50% for patients with cysts in the lungs.
- Imaging studies are the main diagnostic methods to detect and evaluate echinoccal cysts.
- Chest x-ray or CT can identify pulmonary cysts due to E. granulosus sensu lato, which appear as rounded masses of uniform density (Fig. 242-2).
- Ultrasound, CT, or MRI can be used to identify cystic echinococcosis lesions in solid organs of the abdomen, particularly in the liver.
- The ultrasound classification proposed by the World Health Organization Informal Working Group on Echinococcosis has diagnostic and management applications for liver cystic echinococcosis (Figs. 242-2 and 242-3).
- MRI can also be used to classify lesions.
- MRI and CT may be more useful than ultrasound to evaluate the presence of cyst complications, such as communication with the biliary tree, that preclude some management options.
- Imaging of cystic echinococcosis shows well-defined cysts walls and, in some cases, internal trabeculation, dense cyst material, and/or calcifications (Fig. 242-3).
- In some cases, the protoscolices and brood capsules of E. granulosus complex may be visible within the cysts as fine particles termed hydatid sand.
- Identification of daughter cysts within the larger cyst is diagnostic of cystic echinococcosis disease.
- Eggshell or mural calcification on CT is also diagnostic of E. granulosus infection.
- In contrast, ultrasound or CT of alveolar hydatid cysts often reveals an indistinct solid mass.
- Some cases will display central necrosis or plaque-like calcifications.
- Infection is diagnosed by finding the characteristic R. nana eggs in microscopy of the stool.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
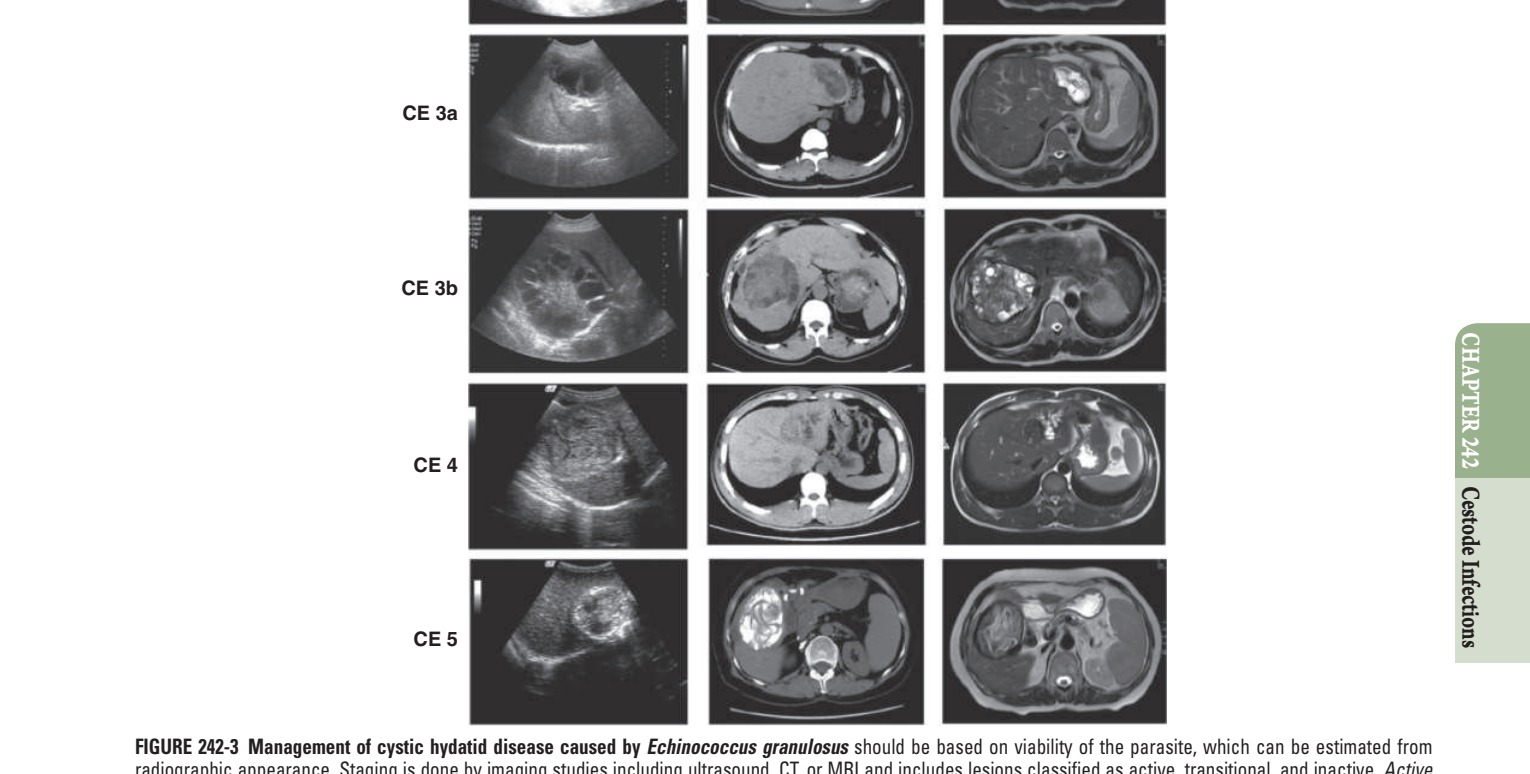
Caption: FIGURE 242-3 Management of cystic hydatid disease caused by Echinococcus radiographic appearance. Staging is done by imaging studies including ultrasound, CT, cysts include types CL (with a cystic lesion and no visible cyst wall), CE1 (with a wall and internal septation). Transitional cysts may have detached laminar (a nonhomogeneous mass) and CE5 (a cyst with a thick calcified wall).
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 242-1 Neurocysticercosis is caused by Taenia solium. Neurologic infection Parenchymal viable cysts (FLAIR MRI sequence). Upper center: Parenchymal viable (postcontrast T1 MRI sequence). Bottom left: Extensive basal subarachnoid in the fourth ventricle (FLAIR MRI sequence). Bottom right: Intraparenchymal brain fluid-attenuated inversion recovery. (Modified with permission from White AC Jr, 2018;31(5):377-382. Lippincott Williams & Wilkins.) — Figure 242-1: Neurocysticercosis imaging demonstrating various lesion types. Upper left: Parenchymal viable cysts on FLAIR MRI. Upper center: Parenchymal viable cysts on postcontrast T1 MRI. Upper right: Single enhancing lesion on postcontrast T1 MRI. Bottom left: Extensive basal subarachnoid neurocysticercosis in the anterior fossa on FLAIR MRI. Bottom center: Viable cyst in the fourth ventricle on FLAIR MRI. Bottom right: Intraparenchymal brain calcifications on noncontrasted CT scan. Lesions are marked with arrowheads.
Figure 2¶
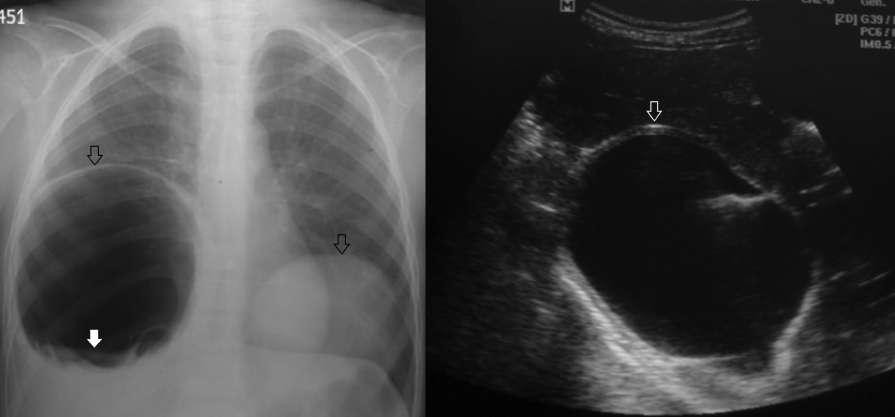
Caption: FIGURE 242-2. Imaging studies of cystic echinococcosis. A. Chest x-ray film of a complicated right chest cyst and an intact left chest cyst. B. Liver ultrasound of a patient — Figure 242-2: Imaging studies of cystic echinococcosis. A: Chest x-ray film showing bilateral cysts with well-defined cyst walls (hollow arrows). B: Liver ultrasound showing CE1 cysts with a well-defined bilayer cyst wall (hollow arrow).
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.