Infective Endocarditis¶
Chapter 133 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Infective endocarditis (IE) is a mass of platelets, fibrin, microorganisms, and scant inflammatory cells on heart valves or other endocardial surfaces.
- Acute IE is a hectically febrile illness that rapidly damages cardiac structures and progresses to death within weeks if untreated.
- Subacute IE follows an indolent course; causes structural cardiac damage only slowly, if at all; rarely metastasizes.
- Staphylococcus aureus is the most common bacterial species causing IE in developed countries.
- The Duke-ISCVID Criteria are the standard for diagnosis: Definite IE requires 2 major criteria, 1 major + 3 minor, or 5 minor criteria.
- Transthoracic echocardiography (TTE) fails to detect vegetations in 20–35% of patients with definite IE; Transesophageal echocardiography (TEE) detects vegetations in >90%.
- S. aureus bacteremia is associated with a high prevalence of IE and a resultant high risk for mortality; echocardiographic evaluation is recommended routinely.
- IE is rejected if an alternative diagnosis is established, if there is no recurrence despite therapy for <4 days, or if surgery/autopsy after <4 days yields no histologic evidence.
- Treatment requires prolonged parenteral antibiotics to achieve effective concentrations in the depths of the vegetation.
- Risk factors for IE have shifted from chronic rheumatic heart disease to injection drug use, degenerative valve disease, and intracardiac devices in developed countries.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification by Valve Type
- 1.2 Classification by Temporal Evolution
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Organisms Causing Major Clinical Forms of IE
- 3.2 Pathogenesis
- 4. CLINICAL FEATURES
- 4.1 Clinical and Laboratory Features
- 4.2 Manifestations with Specific Predisposing Conditions
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Mimickers of Culture-Negative IE
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Duke-ISCVID Criteria
- 6.2 Imaging Modalities
- 7. MANAGEMENT & TREATMENT
- 7.1 Antimicrobial Therapy
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Neurologic Complications
- 8.2 Renal and Splenic Complications
- 9. SPECIAL CONSIDERATIONS
- 9.1 People Who Inject Drugs (PWID)
- 9.2 Health Care–Associated IE
- 10. WHAT TO LOOK FOR — DIAGNOSTIC CLUES
- 10.1 Peripheral Manifestations
- 10.2 Embolic Risk Factors
- 11. WHAT EXCLUDES THE DIAGNOSIS
- 11.1 Rejection Criteria
- 11.2 Limitations of Testing
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | The diagnostic use of transesophageal and transthoracic (IE) or evidence of intracardiac... |
| 2 | 🖼 Figure | Vegetations (arrows) due to viridans streptococci endocarditis involving the mitral valve |
| 3 | 🖼 Figure | A |
| 4 | 🖼 Figure | A |
| 5 | 🖼 Figure | A |
1. DEFINITION & OVERVIEW¶
- The prototypic lesion of infective endocarditis (IE) is a mass of platelets, fibrin, microorganisms, and scant inflammatory cells.
- Infection most commonly involves heart valves but may also occur on the low-pressure side of a ventricular septal defect, on mural endocardium damaged by aberrant jets of blood or foreign bodies, or on intracardiac devices.
- The analogous process involving arteriovenous shunts, arterio-arterial shunts (patent ductus arteriosus), or a coarctation of the aorta is called infective endarteritis.
- IE can be classified according to the temporal evolution of disease, the site of infection, the cause of infection, or the predisposing risk factor (e.g., injection drug use, health care–associated).
- Acute IE is a hectically febrile illness that rapidly damages cardiac structures, seeds extracardiac sites, and, if untreated, progresses to death within weeks.
- Subacute IE follows an indolent course; causes structural cardiac damage only slowly, if at all; rarely metastasizes; and is gradually progressive unless complicated by a major embolic event or a ruptured mycotic aneurysm.
1.1 Classification by Valve Type¶
- Native-valve endocarditis (NVE).
- Prosthetic-valve infections (PVE).
- Infective endocarditis involving cardiovascular implantable electronic devices (CIED-IE).
- Transcatheter aortic valve replacement (TAVR)-PVE.
1.2 Classification by Temporal Evolution¶
- Acute IE: Rapidly febrile, rapid structural damage, death within weeks if untreated.
- Subacute IE: Indolent course, slow structural damage, rarely metastasizes.
2. EPIDEMIOLOGY¶
- In the United States and likely in other developed countries, the incidence of IE is estimated to be 15 cases per 100,000 population per year, with progressive increases during recent decades.
- While congenital heart diseases remain a constant predisposition, predisposing conditions in developed countries have shifted from chronic rheumatic heart disease (still common in developing countries) to injection drug use, degenerative valve disease, and intracardiac devices.
- Although the incidence of IE is increased among the elderly, recent data indicate age-adjusted mortality rates in people ≥55 years old have declined in the United States.
- Recently, however, there has been acceleration in mortality in people aged 25–44 years, likely associated with an increase in opioid use disorder (OUD) and injection drug use in this age group.
- In developed countries, 25–35% of cases of native-valve endocarditis (NVE) are health care–associated, and 16–30% of all cases are prosthetic-valve infections (PVE).
- The risk of PVE is greatest during the initial year after valve replacement; gradually declines to a low, stable rate thereafter; and is greater for bioprosthetic valves than mechanical valves.
- The incidence and rate of decline of transcatheter aortic valve replacement (TAVR)-PVE are similar to those for surgically implanted bioprosthetic aortic valves.
- IE involving cardiovascular implantable electronic devices (CIED-IE) occurs in 0.5–1.14 cases per 1000 recipients.
2.1 Risk Factors¶
- Congenital heart diseases.
- Injection drug use.
- Degenerative valve disease.
- Intracardiac devices.
- Health care–associated conditions.
- Immunocompromised state (e.g., HIV infection, malignancy).
- Age >60 years.
- Presence of aerobic bacteria.
- Sepsis at presentation.
- Symptom duration of >8 weeks.
- Abscess size >6 cm.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Although many species of bacteria and fungi cause sporadic episodes of IE, a few bacterial species cause the majority of cases.
- Recent large studies from developed areas identify Staphylococcus aureus as the most common bacterial species causing IE.
- The oral cavity, skin, and upper respiratory tract are the respective primary portals for viridans streptococci, staphylococci, and HACEK organisms.
- Streptococcus gallolyticus subspecies gallolyticus (formerly S. bovis biotype 1) originates from the gastrointestinal tract and is associated with colonic polyps and tumors.
- Enterococci enter the bloodstream primarily from the genitourinary tract.
- Health care–associated IE, most commonly caused by S. aureus, coagulase-negative staphylococci (CoNS), and enterococci, may have either a nosocomial onset (55%) or a community onset (45%).
- IE complicates 8–25% of episodes of catheter-associated bacteremia; the higher rates are detected in high-risk patients studied by transesophageal echocardiography (TEE).
- PVE arising within 2 months of valve surgery—i.e., early PVE—is generally nosocomial and is the result of intraoperative contamination of the prosthesis or a postoperative infection.
- PVE beginning >12 months after surgery—i.e., late PVE—are similar to those in community-acquired NVE.
- Regardless of the time of onset after surgery, the majority of CoNS strains that cause PVE are resistant to methicillin.
- CIED-IE involves the device or the endothelium at points of device contact. Occasionally, there is concurrent valvular infection.
- One-third of cases of CIED-IE present within 3 months after device implantation or manipulation, one-third between 3 and 12 months, and one-third >1 year.
- S. aureus and CoNS cause the majority of cases of CIED-IE.
- IE in people who inject drugs (PWID), especially that involving the tricuspid valve, is commonly caused by S. aureus, which is often resistant to methicillin.
- Left-sided valve infections in PWID have a more varied etiology.
- In addition to the usual causes of IE, infection due to Enterobacterales, Pseudomonas aeruginosa, Candida species, and sporadically by unusual organisms (Bacillus, Lactobacillus, Corynebacterium species) is encountered.
- About 5–15% of patients with IE have negative blood cultures; in one-third to one-half of these cases, cultures are negative because of prior antibiotic exposure.
- The remainder are infected by fastidious organisms, such as some streptococci; nutritionally variant bacteria now designated Granulicatella, Gemella, and Abiotrophia species; Coxiella burnetii; and Bartonella species.
- Some fastidious organisms occur in characteristic geographic settings (e.g., C. burnetii and Bartonella species in Europe, Brucella species in the Middle East).
- Tropheryma whipplei causes an indolent, culture-negative form of IE.
- C. burnetii has a predilection for prosthetic valves.
- Corynebacterium species and Cutibacterium acnes may involve intracardiac devices and be slow to grow in blood cultures.
- Mycobacterium chimaera, which may be difficult to recover from blood cultures unless special media is used, has caused a global outbreak of PVE and disseminated infection as a result of aerosols from contaminated heater-cooler machines used during cardiopulmonary bypass.
- Lastly, atrial myxoma, marantic endocarditis, and the antiphospholipid antibody syndrome may mimic culture-negative IE.
3.1 Organisms Causing Major Clinical Forms of IE¶
- Table 133-1 summarizes the proportion of cases for various organisms across different IE types.
- Streptococci (includes viridans streptococci; Streptococcus gallolyticus; other non–group A, groupable streptococci; and Abiotrophia and Granulicatella spp.) are common in NVE (40%) and PVE (13% in health care–associated).
- Enterococci (Primarily E. faecalis or nonspeciated isolates; occasionally E. faecium or other less likely species) are common in NVE (9%) and PVE (16% in health care–associated).
- Staphylococcus aureus (Includes methicillin-susceptible and -resistant isolates) is the most common cause of PVE (52% in health care–associated) and CIED-IE (36%).
- Coagulase-negative staphylococci are common in PVE (11% in community-acquired, 33% in early PVE).
- Fastidious gram-negative coccobacilli (HACEK group) includes Haemophilus spp., Aggregatibacter spp., Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae.
- Gram-negative bacilli are rare in NVE (1%) but more common in PVE (13% in health care–associated).
- Candida spp. are rare in NVE (<1%) but more common in PVE (1% in community-acquired, 8% in early PVE).
- Polymicrobial/miscellaneous infections occur in 3% of NVE and 3% of health care–associated NVE.
- Culture-negative IE occurs in 9% of NVE and 3% of health care–associated NVE.
Table 1 — Table 133-1 Organisms Causing Major Clinical Forms of Infective Endocarditis (IE)¶
| ORGANISM(S) | NATIVE-VALVE IE COMMUNITY-ACQUIRED (N = 1718) | NATIVE-VALVE IE HEALTH CARE–ASSOCIATED (N = 1110) | PROSTHETIC-VALVE IE <2 MONTHS (N = 144) | PROSTHETIC-VALVE IE >2-12 MONTHS (N = 31) | PROSTHETIC-VALVE IE >12 MONTHS (N = 194) | TAVR PVE (N = 295) | CIED-IE (N = 337) |
|---|---|---|---|---|---|---|---|
| Streptococci | 40 | 13 | 1 | 10 | 31 | 18 | 2 |
| Pneumococci | 2 | — | — | — | — | — | — |
| Enterococci | 9 | 16 | 8 | 13 | 11 | 24 | 4 |
| Staphylococcus aureus | 28 | 52 | 22 | 13 | 18 | 23 | 36 |
| Coagulase-negative staphylococci | 5 | 11 | 33 | 35 | 11 | 20 | 41 |
| Fastidious gram-negative coccobacilli (HACEK group) | 3 | — | — | — | 6 | — | — |
| Gram-negative bacilli | 1 | 1 | 13 | 3 | 6 | 1 | 6 |
| Candida spp. | <1 | 1 | 8 | 13 | 1 | 1 | 2 |
| Polymicrobial/miscellaneous | 3 | 3 | 3 | 6 | 5 | 8 | 2 |
| Diphtheroids | — | <1 | 6 | — | 3 | 1 | — |
| Culture-negative | 9 | 3 | 5 | 7 | 8 | 5 | 6 |
3.2 Pathogenesis¶
- The undamaged endothelium is resistant to infection by most bacteria.
- Endothelial injury (e.g., at the site of impact of high-velocity blood jets or on the low-pressure side of a cardiac structural lesion) allows either direct infection by virulent organisms or the development of a platelet–fibrin thrombus—a condition called nonbacterial thrombotic endocarditis (NBTE).
- This thrombus serves as a site of bacterial attachment during transient bacteremia.
- The cardiac conditions most commonly resulting in NBTE are mitral regurgitation, aortic stenosis, aortic regurgitation, ventricular septal defects, and complex congenital heart disease.
- NBTE also arises as a result of a hypercoagulable state; this phenomenon gives rise to marantic endocarditis (uninfected vegetations seen in patients with malignancy and chronic diseases) and to bland vegetations complicating systemic lupus erythematosus and antiphospholipid antibody syndrome.
- Organisms that cause IE enter the bloodstream from colonized body surfaces or sites of infection.
- S. aureus adherence to intact endothelium may be mediated by local inflammation inducing von Willebrand factor on endothelial cell surfaces with resulting adherence of both platelets and S. aureus.
- Alternatively, S. aureus adherence to injured endothelium may be mediated by local deposition of fibrin and circulating von Willebrand factor on exposed subendothelial tissue to which in turn S. aureus adhere directly.
- Other microorganisms in the blood adhere to NBTE.
- The organisms that commonly cause IE have surface adhesin molecules, collectively called microbial surface components recognizing adhesin matrix molecules (MSCRAMMs) that mediate adherence to NBTE sites or injured endothelium.
- Adherence is facilitated by fibronectin-binding proteins present on many gram-positive bacteria; by clumping factor (a fibrinogen- and fibrin-binding surface protein) on S. aureus; by fibrinogen-binding surface proteins or (Fss2), collagen-binding surface protein (Ace), and Ebp pili (the latter mediating platelet adherence) on Enterococcus faecalis; and by glucans or FimA (a member of the family of oral mucosal adhesins) on streptococci.
- Fibronectin-binding proteins are required for S. aureus invasion of intact endothelium; thus, these surface proteins may facilitate infection of previously normal valves.
- If resistant to the bactericidal activity of serum and the microbicidal peptides released locally by platelets, adherent organisms proliferate to form dense microcolonies.
- Microorganisms also induce platelet deposition and a localized procoagulant state by eliciting tissue factor from the endothelium and, in the case of S. aureus, from monocytes as well.
- Fibrin deposition combines with platelet aggregation and microorganism proliferation to generate an infected vegetation.
- Organisms deep in vegetations are metabolically inactive (nongrowing) and relatively resistant to killing by antimicrobial agents.
- Proliferating surface organisms are shed into the bloodstream continuously.
4. CLINICAL FEATURES¶
- The clinical manifestations of IE—other than constitutional symptoms, which probably result from cytokine production—arise from damage to intracardiac structures; embolization of vegetation fragments leading to infection or infarction of remote tissues; hematogenous infection of sites during bacteremia; and tissue injury due to the deposition of circulating immune complexes or immune responses to deposited bacterial antigens.
- The highly variable clinical IE syndrome spans a continuum between acute and subacute presentations.
- Most forms of IE share clinical and laboratory features (Table 133-2).
- In patients with subacute presentations, fever is typically low-grade, rarely exceeding 39.4°C (103°F); in contrast, temperatures of 39.4°–40°C (103°–104°F) are often noted in acute IE.
- Fever may be blunted in patients who are elderly, are severely debilitated, or have renal failure.
- Although heart murmurs are usually indicative of the predisposing cardiac pathology rather than of IE, valvular damage and ruptured chordae may result in new regurgitant murmurs.
- In acute IE involving a normal valve, murmurs may be absent initially but ultimately are detected in 85% of cases.
- Congestive heart failure (CHF) resulting from valve dysfunction or, occasionally, intracardiac fistulae develop in 30–40% of patients.
- Extension of leaflet infection into adjacent annular or myocardial tissue results in paravalvular abscesses, which in turn may cause intracardiac fistulae with new murmurs.
- Aortic paravalvular infection may burrow into the upper ventricular septum and interrupt the conduction system, leading to varying degrees of heart block.
- Mitral paravalvular abscesses are more distant from the conduction system and rarely cause conduction abnormalities.
- Coronary artery emboli occur in 2% of patients and may result in myocardial infarction.
- The classic nonsuppurative peripheral manifestations of subacute IE (e.g., Janeway lesions; Fig. 133-2A) are related to prolonged infection; with early diagnosis and treatment, these have become infrequent.
- In contrast, septic embolization mimicking some of these lesions (subungual hemorrhage, Osler’s nodes) is common in patients with acute S. aureus IE (Fig. 133-2B).
- Musculoskeletal pain usually remits promptly with treatment but must be distinguished from focal metastatic infections (e.g., spondylodiscitis), which may complicate 10–15% of cases.
- Hematogenously seeded focal infection occurs most often in the skin, spleen, kidneys, skeletal system, and meninges.
- Arterial emboli, one-half of which precede the diagnosis of IE, are clinically apparent in up to 50% of patients.
- S. aureus IE, mobile vegetations >10 mm in diameter, and infection involving the mitral valve anterior leaflet are independently associated with an increased risk of embolization.
- Embolic arterial occlusion causes regional pain or ischemia-induced organ dysfunction (e.g., of the kidney, spleen, bowel, extremity).
- Cerebrovascular emboli presenting as strokes or occasionally as encephalopathy complicate 15–35% of cases; however, evidence of clinically asymptomatic emboli is found on magnetic resonance imaging (MRI) in 30–65% of patients with left-sided IE.
- The frequency of stroke is 8 per 1000 patient-days during the week prior to diagnosis and decreases to 4.8 and 1.7 per 1000 patient-days during the first and second weeks of effective antimicrobial therapy, respectively.
- Only 3% of strokes occur after 1 week of effective therapy.
- Emboli occurring late during or after effective therapy do not in themselves constitute evidence of failed antimicrobial treatment.
- Other neurologic complications include aseptic or purulent meningitis, intracranial hemorrhage due to hemorrhagic infarcts or ruptured mycotic aneurysms, and seizures.
- Mycotic aneurysms are focal dilations of arteries occurring at points in the artery wall that have been weakened by infection in the vasa vasorum or where septic emboli have lodged.
- Microabscesses in the brain and meninges occur commonly in S. aureus IE; intracerebral abscesses requiring surgical drainage are infrequent.
- Immune complex deposition on the glomerular basement membrane causes diffuse hypocomplementemic glomerulonephritis and renal dysfunction, which typically improve with effective antimicrobial therapy.
- Embolic renal infarcts cause flank pain and hematuria but rarely renal dysfunction.
- Splenic infarcts or abscess can manifest as left upper abdominal, pleuritic chest, or left shoulder pain.
- Among PWID, 35–60% of IE is limited to the tricuspid valve and presents with fever with faint or no murmur and without peripheral manifestations.
- Septic pulmonary emboli, which are common with tricuspid IE, cause cough, pleuritic chest pain, nodular pulmonary infiltrates, and occasionally empyema or pyopneumothorax.
- Infection of the aortic or mitral valve presents with the typical clinical features of IE, including peripheral manifestations.
- Health care–associated IE has typical manifestations unless associated with an intracardiac device or masked by the symptoms of concurrent illness.
- CIED-IE may be associated with obvious (especially within 6 months of device manipulation) or cryptic generator pocket infection or arise through bacteremic seeding without pocket infection.
- Fever, sepsis, minimal murmur, and occasionally pulmonary symptoms due to septic emboli are seen.
- Late-onset PVE and TAVR-PVE present with typical clinical features.
- In early PVE, symptoms may be masked by recent surgery.
- In both early and late PVE, paravalvular infection is common and often results in partial valve dehiscence, regurgitant murmurs, CHF, or disruption of the conduction system.
4.1 Clinical and Laboratory Features¶
- Table 133-2 summarizes the frequency of clinical and laboratory features of IE.
- Fever is present in 80–90% of cases.
- Chills and sweats are present in 40–75% of cases.
- Anorexia, weight loss, and malaise are present in 25–50% of cases.
- Myalgias and arthralgias are present in 15–30% of cases.
- Back pain is present in 7–15% of cases.
- Heart murmur is present in 80–85% of cases.
- New or worsened regurgitant murmur is present in 20–50% of cases.
- Arterial emboli are present in 20–50% of cases.
- Splenomegaly is present in 15–50% of cases.
- Clubbing is present in 10–20% of cases.
- Neurologic manifestations are present in 20–40% of cases.
- Peripheral manifestations (Osler’s nodes, subungual hemorrhages, Janeway lesions, Roth’s spots) are present in 2–15% of cases.
- Petechiae are present in 10–40% of cases.
- Anemia is present in 70–90% of cases.
- Leukocytosis is present in 20–30% of cases.
- Microscopic hematuria is present in 30–50% of cases.
- Elevated erythrocyte sedimentation rate is present in 60–90% of cases.
- Elevated C-reactive protein level is present in 90% of cases.
- Rheumatoid factor is present in 50% of cases.
- Circulating immune complexes are present in 65–100% of cases.
- Decreased serum complement is present in 5–40% of cases.
Table 2 — Table 133-2 Clinical and Laboratory Features of Infective Endocarditis¶
| FEATURE | FREQUENCY, % |
|---|---|
| Fever | 80–90 |
| Chills and sweats | 40–75 |
| Anorexia, weight loss, malaise | 25–50 |
| Myalgias, arthralgias | 15–30 |
| Back pain | 7–15 |
| Heart murmur | 80–85 |
| New/worsened regurgitant murmur | 20–50 |
| Arterial emboli | 20–50 |
| Splenomegaly | 15–50 |
| Clubbing | 10–20 |
| Neurologic manifestations | 20–40 |
| Peripheral manifestations (Osler’s nodes, subungual hemorrhages, Janeway lesions, Roth’s spots) | 2–15 |
| Petechiae | 10–40 |
| Anemia | 70–90 |
| Leukocytosis | 20–30 |
| Microscopic hematuria | 30–50 |
| Elevated erythrocyte sedimentation rate | 60–90 |
| Elevated C-reactive protein level | 90 |
| Rheumatoid factor | 50 |
| Circulating immune complexes | 65–100 |
| Decreased serum complement | 5–40 |
4.2 Manifestations with Specific Predisposing Conditions¶
- Among PWID, 35–60% of IE is limited to the tricuspid valve and presents with fever with faint or no murmur and without peripheral manifestations.
- Septic pulmonary emboli, which are common with tricuspid IE, cause cough, pleuritic chest pain, nodular pulmonary infiltrates, and occasionally empyema or pyopneumothorax.
- Infection of the aortic or mitral valve presents with the typical clinical features of IE, including peripheral manifestations.
- Health care–associated IE has typical manifestations unless associated with an intracardiac device or masked by the symptoms of concurrent illness.
- CIED-IE may be associated with obvious (especially within 6 months of device manipulation) or cryptic generator pocket infection or arise through bacteremic seeding without pocket infection.
- Fever, sepsis, minimal murmur, and occasionally pulmonary symptoms due to septic emboli are seen.
- Late-onset PVE and TAVR-PVE present with typical clinical features.
- In early PVE, symptoms may be masked by recent surgery.
- In both early and late PVE, paravalvular infection is common and often results in partial valve dehiscence, regurgitant murmurs, CHF, or disruption of the conduction system.
5. DIFFERENTIAL DIAGNOSIS¶
- Atrial myxoma, marantic endocarditis, and the antiphospholipid antibody syndrome may mimic culture-negative IE.
- Focal metastatic infections (e.g., spondylodiscitis) must be distinguished from peripheral manifestations of IE.
- Septic embolization mimicking some of these lesions (subungual hemorrhage, Osler’s nodes) is common in patients with acute S. aureus IE.
- Musculoskeletal pain usually remits promptly with treatment but must be distinguished from focal metastatic infections (e.g., spondylodiscitis), which may complicate 10–15% of cases.
5.1 Mimickers of Culture-Negative IE¶
- Atrial myxoma.
- Marantic endocarditis.
- Antiphospholipid antibody syndrome.
6. INVESTIGATIONS & DIAGNOSIS¶
- Careful clinical, microbiologic, and echocardiographic evaluations should be pursued when febrile patients have IE predispositions, cardiac or noncardiac (e.g., stroke or splenic infarct) features of IE, or blood cultures yielding an IE-associated organism.
- The Duke-ISCVID Criteria reiterate that multiple blood cultures are the gold standard for diagnosing IE.
- Collection of three cultures from separate venipuncture sites is still recommended but is no longer required.
- Further, the bacterial species considered 'typical' for causing IE are defined as those whose recovery from blood has been strongly associated with IE; the pathogen list has been expanded to include all streptococcal species except S. pneumoniae and S. pyogenes, S. lugdunensis, E. faecalis regardless of the primary source, and 'streptococcus-like bacteria' (e.g., Granulicatella spp., Abiotrophia spp., and Gemella spp.).
- To fulfill a major criterion, a typical organism that causes IE (e.g., those listed previously plus S. aureus and HACEK organisms) must be recovered in two or more blood culture sets; other organisms, considered 'nontypical' must grow in three or more blood culture sets and the clinical presentation must be unexplained by an extracardiac focus of infection.
- In patients with intracardiac prosthetic material, CoNS, Corynebacterium striatum, Corynebacterium jeikeium, C. acnes, Serratia marcescens, Pseudomonas aeruginosa, nontuberculous mycobacteria (e.g., M. chimaerae), and Candida species should be considered 'typical.'
- Otherwise these organisms must be found in three or more blood culture sets to satisfy a major criterion.
- In patients with suspected NVE, PVE, TAVR-PVE, or CIED-IE who have not received antibiotics during the prior 2 weeks, three two-bottle blood culture sets containing the appropriate volume of blood (10 mL per bottle) should be obtained, ideally from different venipuncture sites.
- If the cultures remain negative after 48–72 h, two or three additional blood culture sets should be obtained, and the laboratory should be consulted for advice regarding optimal culture techniques.
- Pending culture results, empirical antimicrobial therapy should be withheld initially from hemodynamically and clinically stable patients with suspected subacute IE, especially those who have received antibiotics within the preceding 2 weeks.
- The delay allows blood for additional cultures to be obtained without the confounding effect of empirical treatment.
- Patients with sepsis or deteriorating hemodynamics who may require urgent surgery should receive empirical treatment immediately after the initial three sets of blood cultures are obtained.
- Non–blood culture laboratory criteria have been added to microbiologic major criteria in the Duke-ISCVID Criteria to implicate organisms that are difficult to recover by blood culture.
- These include polymerase chain reaction (PCR) or other nucleic acid–based techniques identifying C. burnetii, Bartonella spp., or T. whipplei from the blood and indirect immunofluorescence assays for IgM and IgG antibodies to Bartonella henselae or B. quintana with IgG titer ≥1:800.
- Next-generation (shotgun metagenomic) sequencing of pathogen DNA from serum has emerged as a novel nonculture technology capable of identifying a wide array of organisms in blood culture–negative IE.
- However, Duke-ISCVID Criteria recommend that results from such testing that yield organisms other than C. burnetii be considered minor criteria at this time.
- In vegetations recovered at surgery or by embolectomy, pathogens can be identified by culture and histopathologic examination with special stains.
- A sample of the vegetation should be collected using sterile technique and saved for molecular testing using PCR with organism-specific primers (e.g., C. burnetii, Bartonella, T. whipplei, C. acnes, Mycoplasma hominis) or broad-range PCR targeting 16S ribosomal RNA (or 28S rRNA, if fungi are suspected) followed by sequencing for organism identification.
- Histopathology may inform the selection of specific molecular tests.
- Molecular testing is a useful diagnostic technology when the histopathology of a vegetation is consistent with IE; however, it cannot be used to establish the viability of residual bacteria in vegetations.
- Additionally, molecular testing is only moderately sensitive, and thus, a negative test cannot exclude IE.
- When tissue is limited, molecular testing should be prioritized over culture.
- Echocardiography or cardiac CT showing vegetation, valvular/leaflet perforation/aneurysm, abscess, pseudoaneurysm or intracardiac fistula is a major criterion.
- New valvular regurgitation (new/worsening murmur is NOT sufficient; requires echocardiographic evidence) is a major criterion.
- New prosthetic valve dehiscence/insufficiency is a major criterion.
- FDG-PET/CT with abnormal metabolic activity involving a native or prosthetic valve, ascending aortic graft, intracardiac device leads, or other prosthetic material is a major criterion.
- Evidence of IE documented by direct inspection during heart surgery is a major criterion.
- Minor criteria include predisposition (previous history of IE, injection drug use, prosthetic valve, previous valve repair, congenital heart disease (e.g., bicuspid AV), CIED, more than mild regurgitation or stenosis, hypertrophic cardiomyopathy).
- Minor criteria include fever (T > 38.0°C (100.4°F)).
- Minor criteria include vascular phenomenon (arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhage, Janeway lesions, cerebral/splenic abscesses, purulent purpura).
- Minor criteria include immunologic phenomena (glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor).
- Minor criteria include microbiologic evidence (positive blood cultures not meeting above criteria, positive culture, PCR, or other nucleic acid-based test for an organism consistent with IE from a non-endovascular site, or single finding of a skin bacterium by PCR on a valve or wire without additional clinical or microbiological supporting evidence).
- Minor criteria include imaging criteria (abnormal metabolic activity on FDG-PET/CT within 3 months of implantation of a prosthetic valve, ascending aortic graft, intracardiac device lead).
- Minor criteria include physical exam criteria (New valvular regurgitation on auscultation).
- Definite IE: 1. Pathologic criteria (microorganisms or active endocarditis identified in a vegetation/intra-cardiac abscess from cardiac tissue, prosthetic material, arterial embolus) 2. Clinical criteria (2 major or 1 major + 3 minor or 5 minor).
- Possible IE: 1 major + 1 minor or 3 minor.
- Rejected IE: does not meet above criteria or firm alternative dx or lack of recurrence with 90% of patients with definite IE; nevertheless, initial studies may yield false-positive results in 6–18% of IE patients, especially in TAVR-PVE.
- A negative TEE, when IE is likely, does not exclude the diagnosis but rather warrants repeating the study in 7–10 days.
- TEE is sometimes augmented by three-dimensional TEE, which can better visualize vegetations and perivalvular extension of infection.
- Other imaging should be pursued when anatomic confirmation is contraindicated or is not confirmatory, and in suspected PVE.
- Electrocardiographic-gated multislice cardiac CT angiogram (CTA), which is less sensitive than TEE in detection of vegetations, valvular perforation, and paravalvular leakage but superior in defining pseudoaneurysm or abscess, may be definitive.
- Further, it can be used in lieu of preoperative cardiac catheterization to assess coronary artery patency in patients at low to intermediate risk of coronary disease.
- 18F-Fluorodeoxyglucose positron emission tomography (FDG-PET)/CT is less sensitive than TEE or CTA in detecting intracardiac pathology in NVE or CIED-IE but provides increased sensitivity in assessing suspected PVE, including TAVR-PVE, infection of ascending aorta grafts, extracardiac complications, left ventricular assist device (LVAD) infection, and CIED pocket and lead infection.
- As 18F-fluorodeoxyglucose positron emission tomography (FDG-PET)/CT is a whole-body image, findings may modify therapy in 25% of NVE and PVE patients.
- However, FDG-PET/CT is costly, requires preprocedure patient preparation, can have false-positive results in patients with recent valve surgery (<3 months), and requires experienced radiographers for interpretation.
- Findings indicative of IE on CTA and FDG-PET/CT are major criteria and considered equivalent to echocardiography in the Duke-ISCVID schema.
- In population-based studies and large series (using various diagnostic criteria), IE occurs frequently among patients who have monomicrobial bacteremia due to those gram-positive organisms that are commonly associated with IE.
- For example, 12–17% of patients with blood cultures growing E. faecalis have IE; 7% of patients with blood cultures growing non–β-hemolytic streptococci have IE; and 8–14% of patients with blood cultures growing S. aureus have IE.
- Among patients with one or more positive monomicrobial blood culture, IE risk-prediction scoring systems have been developed to identify patients who are at sufficient risk of IE to justify echocardiographic assessment (Table 133-4).
- Because S. aureus bacteremia is associated with a high prevalence of IE and a resultant high risk for mortality, echocardiographic evaluation (high-quality TTE or preferably TEE) is recommended routinely.
- Prediction scores suggest that with S. aureus bacteremia, a patient with any of the features listed in Table 133-4 incurs at least a 6% risk of IE, with risk increasing when multiple features are present.
- Thus, when present, these findings are a strong indication for early TEE.
- In their absence, TTE should suffice unless other findings suggest IE.
- Among patients with either monomicrobial E. faecalis or non–β-hemolytic streptococcal bacteremia, any three of the respective listed features (Table 133-4) are associated with a significant frequency of IE.
- For these patients, the estimated number needed to test with TEE to detect IE is 2.4 and 3.6, respectively.
- While these predictive scoring systems need further evaluation and should be used with clinical judgment, they appear to have a high sensitivity and therefore a high negative predictive value, which allows identification of patients at low risk of IE where echocardiography, particularly TEE, can be omitted.
- An approach to echocardiographic evaluation of patients with suspected IE is illustrated in Fig. 133-3.
- Resonance angiography (MRA) should be obtained in patients with neurologic signs or symptoms, including unusual headache, to assess for emboli, hemorrhage, or mycotic aneurysms.
- The findings can support the IE diagnosis as well as provide evidence requiring changes in planned surgical treatment.
- Patients with recalcitrant back pain or focal spine tenderness should undergo spine MRI targeted to the appropriate level based on symptoms to assess for osteomyelitis and epidural abscess.
- Contrast-enhanced whole-body tomography to detect silent emboli in patients without localizing symptoms is not likely to enhance diagnostic accuracy and is associated with significant risk of kidney injury due to contrast media exposure; thus, it should not be performed routinely.
6.1 Duke-ISCVID Criteria¶
- The diagnosis of IE is established with certainty only when vegetations are examined histologically and microbiologically.
- Nevertheless, a common clinical approach utilizes a diagnostic schema based on clinical, laboratory, and echocardiographic findings common to patients with IE (Table 133-3).
- Now known as the Duke–International Society for Cardiovascular Infectious Diseases (Duke-ISCVID) Criteria for IE, the criteria were updated in 2023 to encompass new epidemiologic data and microbiologic testing and imaging methodologies; these modifications have been validated in at least four bacteremia cohorts and show sensitivity in the 80–93% range.
- Clinical judgment must be exercised to use the criteria effectively.
- A clinical diagnosis of definite IE requires two major criteria, one major and three minor criteria, or five minor criteria.
- IE is rejected if an alternative diagnosis is established, if there is no recurrence despite therapy for <4 days, or if surgery or autopsy after <4 days of antimicrobial therapy yields no histologic evidence of IE.
- Cases not classified as definite or rejected are considered possible IE when either one major and one minor criterion or three minor criteria are fulfilled.
- Absent extenuating circumstances, patients with definite and possible IE are treated as having IE.
Table 3 — Table 133-3 The Modified Duke Criteria for the Clinical Diagnosis of Infective Endocarditis (IE)¶
| CRITERIA | DESCRIPTION |
|---|---|
| Major Criteria | A. Microbiologic Criteria: 1. Positive blood culture: Microorganism that commonly cause IE in 2 or more separate blood culture sets (Typical—i.e., S. aureus, S. lugdunensis, E. faecalis, all streptococcal species except S. pneumoniae and S. pyogenes, Granulicatella spp., Abiotrophia spp., Gemella spp., HACEK group organisms and in the setting of intracardiac prosthetic material, CoNS, C. striatum, C. jeikeium, S. marcescens, P. aeruginosa, C. acnes, nontuberculosis mycobacteria, Candida spp.) OR Microorganisms that occasionally or rarely cause IE isolated from 3 or more separate blood culture sets (Nontypical). 2. Positive laboratory tests: Positive polymerase chain reaction (PCR) for Coxiella burnetii, Bartonella spp., or Tropheryma whipplei from blood OR Single blood culture growing C. burnetii or phase I IgG Ab titer ≥ 1:800 OR Indirect immunofluorescence assays (IFA) for IgM Ab and IgG Ab to B. henselae or B. quintana with IgG Ab titer ≥ 1:800. |
| Major Criteria | B. Imaging Criteria: 1. Echocardiography or cardiac CT showing vegetation, valvular/leaflet perforation/aneurysm, abscess, pseudoaneurysm or intracardiac fistula OR New valvular regurgitation (new/worsening murmur is NOT sufficient; requires echocardiographic evidence) OR New prosthetic valve dehiscence/insufficiency. 2. FDG-PET/CT with abnormal metabolic activity involving a native or prosthetic valve, ascending aortic graft, intracardiac device leads, or other prosthetic material. |
| Major Criteria | C. Surgical Criteria: Evidence of IE documented by direct inspection during heart surgery. |
| Minor Criteria | A. Predisposition: previous history of IE, injection drug use, prosthetic valve, previous valve repair, congenital heart disease (e.g., bicuspid AV), CIED, more than mild regurgitation or stenosis, hypertrophic cardiomyopathy. |
| Minor Criteria | B. Fever: T > 38.0°C (100.4°F). |
| Minor Criteria | C. Vascular phenomenon: arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhage, Janeway lesions, cerebral/splenic abscesses, purulent purpura. |
| Minor Criteria | D. Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, positive rheumatoid factor. |
| Minor Criteria | E. Microbiologic evidence: positive blood cultures (not meeting above criteria) OR Positive culture, PCR, or other nucleic acid-based test for an organism consistent with IE from a non-endovascular site or single finding of a skin bacterium by PCR on a valve or wire without additional clinical or microbiological supporting evidence. |
| Minor Criteria | F. Imaging criteria: abnormal metabolic activity on FDG-PET/CT within 3 months of implantation of a prosthetic valve, ascending aortic graft, intracardiac device lead. |
| Minor Criteria | G. Physical exam criteria: New valvular regurgitation on auscultation. |
| Diagnosis | Definite IE: 1. Pathologic criteria (microorganisms or active endocarditis identified in a vegetation/intra-cardiac abscess from cardiac tissue, prosthetic material, arterial embolus) 2. Clinical criteria (2 major or 1 major + 3 minor or 5 minor). Possible IE: 1 major + 1 minor or 3 minor. Rejected IE: does not meet above criteria or firm alternative dx or lack of recurrence with <4 days of antibiotics or no evidence on autopsy. |
6.2 Imaging Modalities¶
- Transthoracic echocardiography (TTE) is exceptionally specific; however, in 20% of patients, the images are inadequate.
- TTE fails to detect vegetations in 20–35% of patients with definite clinical IE, missing vegetations 90% of patients with definite IE; nevertheless, initial studies may yield false-positive results in 6–18% of IE patients, especially in TAVR-PVE.
- A negative TEE, when IE is likely, does not exclude the diagnosis but rather warrants repeating the study in 7–10 days.
- TEE is sometimes augmented by three-dimensional TEE, which can better visualize vegetations and perivalvular extension of infection.
- Other imaging should be pursued when anatomic confirmation is contraindicated or is not confirmatory, and in suspected PVE.
- Electrocardiographic-gated multislice cardiac CT angiogram (CTA), which is less sensitive than TEE in detection of vegetations, valvular perforation, and paravalvular leakage but superior in defining pseudoaneurysm or abscess, may be definitive.
- Further, it can be used in lieu of preoperative cardiac catheterization to assess coronary artery patency in patients at low to intermediate risk of coronary disease.
- 18F-Fluorodeoxyglucose positron emission tomography (FDG-PET)/CT is less sensitive than TEE or CTA in detecting intracardiac pathology in NVE or CIED-IE but provides increased sensitivity in assessing suspected PVE, including TAVR-PVE, infection of ascending aorta grafts, extracardiac complications, left ventricular assist device (LVAD) infection, and CIED pocket and lead infection.
- As 18F-fluorodeoxyglucose positron emission tomography (FDG-PET)/CT is a whole-body image, findings may modify therapy in 25% of NVE and PVE patients.
- However, FDG-PET/CT is costly, requires preprocedure patient preparation, can have false-positive results in patients with recent valve surgery (<3 months), and requires experienced radiographers for interpretation.
- Findings indicative of IE on CTA and FDG-PET/CT are major criteria and considered equivalent to echocardiography in the Duke-ISCVID schema.
7. MANAGEMENT & TREATMENT¶
- To cure IE, all bacteria in the vegetation must be killed.
- This is difficult because local host defenses are deficient and because the bacteria are largely nongrowing and metabolically inactive and thus are less easily killed by antibiotics.
- Consequently, therapy must be prolonged.
- Antibiotics are generally given parenterally to achieve serum concentrations that, through passive diffusion, result in effective concentrations in the depths of the vegetation.
- The decision to initiate treatment empirically must balance the need to establish a microbiologic diagnosis against the potential disease progression or the need to control infection prior to urgent surgery.
- Infection at other sites (such as the meninges), allergies, end-organ dysfunction, interactions with concomitantly administered medications, and risks of adverse events must be considered in the selection of therapy.
- The regimens recommended for the treatment of PVE (except that caused by staphylococci), although given for several weeks longer, are similar to those used to treat NVE (Table 133-5).
- Recommended antibiotic dosing and duration of therapy, which are not fully detailed in the provided text, should be followed based on specific pathogen and patient factors.
7.1 Antimicrobial Therapy¶
- Antibiotics are generally given parenterally to achieve serum concentrations that, through passive diffusion, result in effective concentrations in the depths of the vegetation.
- The decision to initiate treatment empirically must balance the need to establish a microbiologic diagnosis against the potential disease progression or the need to control infection prior to urgent surgery.
- Infection at other sites (such as the meninges), allergies, end-organ dysfunction, interactions with concomitantly administered medications, and risks of adverse events must be considered in the selection of therapy.
- The regimens recommended for the treatment of PVE (except that caused by staphylococci), although given for several weeks longer, are similar to those used to treat NVE (Table 133-5).
- Recommended antibiotic dosing and duration of therapy, which are not fully detailed in the provided text, should be followed based on specific pathogen and patient factors.
8. PROGNOSIS & COMPLICATIONS¶
- Arterial emboli, one-half of which precede the diagnosis of IE, are clinically apparent in up to 50% of patients.
- S. aureus IE, mobile vegetations >10 mm in diameter, and infection involving the mitral valve anterior leaflet are independently associated with an increased risk of embolization.
- Embolic arterial occlusion causes regional pain or ischemia-induced organ dysfunction (e.g., of the kidney, spleen, bowel, extremity).
- Cerebrovascular emboli presenting as strokes or occasionally as encephalopathy complicate 15–35% of cases; however, evidence of clinically asymptomatic emboli is found on magnetic resonance imaging (MRI) in 30–65% of patients with left-sided IE.
- The frequency of stroke is 8 per 1000 patient-days during the week prior to diagnosis and decreases to 4.8 and 1.7 per 1000 patient-days during the first and second weeks of effective antimicrobial therapy, respectively.
- Only 3% of strokes occur after 1 week of effective therapy.
- Emboli occurring late during or after effective therapy do not in themselves constitute evidence of failed antimicrobial treatment.
- Other neurologic complications include aseptic or purulent meningitis, intracranial hemorrhage due to hemorrhagic infarcts or ruptured mycotic aneurysms, and seizures.
- Mycotic aneurysms are focal dilations of arteries occurring at points in the artery wall that have been weakened by infection in the vasa vasorum or where septic emboli have lodged.
- Microabscesses in the brain and meninges occur commonly in S. aureus IE; intracerebral abscesses requiring surgical drainage are infrequent.
- Immune complex deposition on the glomerular basement membrane causes diffuse hypocomplementemic glomerulonephritis and renal dysfunction, which typically improve with effective antimicrobial therapy.
- Embolic renal infarcts cause flank pain and hematuria but rarely renal dysfunction.
- Splenic infarcts or abscess can manifest as left upper abdominal, pleuritic chest, or left shoulder pain.
- Among PWID, 35–60% of IE is limited to the tricuspid valve and presents with fever with faint or no murmur and without peripheral manifestations.
- Septic pulmonary emboli, which are common with tricuspid IE, cause cough, pleuritic chest pain, nodular pulmonary infiltrates, and occasionally empyema or pyopneumothorax.
- Infection of the aortic or mitral valve presents with the typical clinical features of IE, including peripheral manifestations.
- Health care–associated IE has typical manifestations unless associated with an intracardiac device or masked by the symptoms of concurrent illness.
- CIED-IE may be associated with obvious (especially within 6 months of device manipulation) or cryptic generator pocket infection or arise through bacteremic seeding without pocket infection.
- Fever, sepsis, minimal murmur, and occasionally pulmonary symptoms due to septic emboli are seen.
- Late-onset PVE and TAVR-PVE present with typical clinical features.
- In early PVE, symptoms may be masked by recent surgery.
- In both early and late PVE, paravalvular infection is common and often results in partial valve dehiscence, regurgitant murmurs, CHF, or disruption of the conduction system.
8.1 Neurologic Complications¶
- Cerebrovascular emboli presenting as strokes or occasionally as encephalopathy complicate 15–35% of cases.
- Evidence of clinically asymptomatic emboli is found on magnetic resonance imaging (MRI) in 30–65% of patients with left-sided IE.
- The frequency of stroke is 8 per 1000 patient-days during the week prior to diagnosis and decreases to 4.8 and 1.7 per 1000 patient-days during the first and second weeks of effective antimicrobial therapy, respectively.
- Only 3% of strokes occur after 1 week of effective therapy.
- Emboli occurring late during or after effective therapy do not in themselves constitute evidence of failed antimicrobial treatment.
- Other neurologic complications include aseptic or purulent meningitis, intracranial hemorrhage due to hemorrhagic infarcts or ruptured mycotic aneurysms, and seizures.
- Mycotic aneurysms are focal dilations of arteries occurring at points in the artery wall that have been weakened by infection in the vasa vasorum or where septic emboli have lodged.
- Microabscesses in the brain and meninges occur commonly in S. aureus IE; intracerebral abscesses requiring surgical drainage are infrequent.
8.2 Renal and Splenic Complications¶
- Immune complex deposition on the glomerular basement membrane causes diffuse hypocomplementemic glomerulonephritis and renal dysfunction, which typically improve with effective antimicrobial therapy.
- Embolic renal infarcts cause flank pain and hematuria but rarely renal dysfunction.
- Splenic infarcts or abscess can manifest as left upper abdominal, pleuritic chest, or left shoulder pain.
9. SPECIAL CONSIDERATIONS¶
- Among PWID, 35–60% of IE is limited to the tricuspid valve and presents with fever with faint or no murmur and without peripheral manifestations.
- Septic pulmonary emboli, which are common with tricuspid IE, cause cough, pleuritic chest pain, nodular pulmonary infiltrates, and occasionally empyema or pyopneumothorax.
- Infection of the aortic or mitral valve presents with the typical clinical features of IE, including peripheral manifestations.
- Health care–associated IE has typical manifestations unless associated with an intracardiac device or masked by the symptoms of concurrent illness.
- CIED-IE may be associated with obvious (especially within 6 months of device manipulation) or cryptic generator pocket infection or arise through bacteremic seeding without pocket infection.
- Fever, sepsis, minimal murmur, and occasionally pulmonary symptoms due to septic emboli are seen.
- Late-onset PVE and TAVR-PVE present with typical clinical features.
- In early PVE, symptoms may be masked by recent surgery.
- In both early and late PVE, paravalvular infection is common and often results in partial valve dehiscence, regurgitant murmurs, CHF, or disruption of the conduction system.
9.1 People Who Inject Drugs (PWID)¶
- Among PWID, 35–60% of IE is limited to the tricuspid valve and presents with fever with faint or no murmur and without peripheral manifestations.
- Septic pulmonary emboli, which are common with tricuspid IE, cause cough, pleuritic chest pain, nodular pulmonary infiltrates, and occasionally empyema or pyopneumothorax.
- Left-sided valve infections in PWID have a more varied etiology.
- In addition to the usual causes of IE, infection due to Enterobacterales, Pseudomonas aeruginosa, Candida species, and sporadically by unusual organisms (Bacillus, Lactobacillus, Corynebacterium species) is encountered.
9.2 Health Care–Associated IE¶
- Health care–associated IE has typical manifestations unless associated with an intracardiac device or masked by the symptoms of concurrent illness.
- CIED-IE may be associated with obvious (especially within 6 months of device manipulation) or cryptic generator pocket infection or arise through bacteremic seeding without pocket infection.
- Fever, sepsis, minimal murmur, and occasionally pulmonary symptoms due to septic emboli are seen.
- Late-onset PVE and TAVR-PVE present with typical clinical features.
- In early PVE, symptoms may be masked by recent surgery.
- In both early and late PVE, paravalvular infection is common and often results in partial valve dehiscence, regurgitant murmurs, CHF, or disruption of the conduction system.
10. WHAT TO LOOK FOR — DIAGNOSTIC CLUES¶
- The classic nonsuppurative peripheral manifestations of subacute IE (e.g., Janeway lesions; Fig. 133-2A) are related to prolonged infection; with early diagnosis and treatment, these have become infrequent.
- In contrast, septic embolization mimicking some of these lesions (subungual hemorrhage, Osler’s nodes) is common in patients with acute S. aureus IE (Fig. 133-2B).
- Janeway lesions are non-tender, erythematous macules on the palms and soles.
- Osler’s nodes are tender, erythematous nodules on the pads of fingers and toes.
- Roth’s spots are retinal hemorrhages with pale centers.
- S. aureus IE, mobile vegetations >10 mm in diameter, and infection involving the mitral valve anterior leaflet are independently associated with an increased risk of embolization.
- Embolic arterial occlusion causes regional pain or ischemia-induced organ dysfunction (e.g., of the kidney, spleen, bowel, extremity).
- Cerebrovascular emboli presenting as strokes or occasionally as encephalopathy complicate 15–35% of cases; however, evidence of clinically asymptomatic emboli is found on magnetic resonance imaging (MRI) in 30–65% of patients with left-sided IE.
- The frequency of stroke is 8 per 1000 patient-days during the week prior to diagnosis and decreases to 4.8 and 1.7 per 1000 patient-days during the first and second weeks of effective antimicrobial therapy, respectively.
- Only 3% of strokes occur after 1 week of effective therapy.
- Mycotic aneurysms are focal dilations of arteries occurring at points in the artery wall that have been weakened by infection in the vasa vasorum or where septic emboli have lodged.
- Microabscesses in the brain and meninges occur commonly in S. aureus IE; intracerebral abscesses requiring surgical drainage are infrequent.
10.1 Peripheral Manifestations¶
- Janeway lesions: Non-tender, erythematous macules on the palms and soles.
- Osler’s nodes: Tender, erythematous nodules on the pads of fingers and toes.
- Roth’s spots: Retinal hemorrhages with pale centers.
- Subungual hemorrhages: Bleeding under the nails.
10.2 Embolic Risk Factors¶
- S. aureus IE.
- Mobile vegetations >10 mm in diameter.
- Infection involving the mitral valve anterior leaflet.
11. WHAT EXCLUDES THE DIAGNOSIS¶
- IE is rejected if an alternative diagnosis is established.
- IE is rejected if there is no recurrence despite therapy for <4 days.
- IE is rejected if surgery or autopsy after <4 days of antimicrobial therapy yields no histologic evidence of IE.
- Cases not classified as definite or rejected are considered possible IE when either one major and one minor criterion or three minor criteria are fulfilled.
- Absent extenuating circumstances, patients with definite and possible IE are treated as having IE.
- A negative TEE, when IE is likely, does not exclude the diagnosis but rather warrants repeating the study in 7–10 days.
- Molecular testing is only moderately sensitive, and thus, a negative test cannot exclude IE.
11.1 Rejection Criteria¶
- Alternative diagnosis established.
- No recurrence despite therapy for <4 days.
- Surgery or autopsy after <4 days of antimicrobial therapy yields no histologic evidence of IE.
11.2 Limitations of Testing¶
- A negative TEE, when IE is likely, does not exclude the diagnosis but rather warrants repeating the study in 7–10 days.
- Molecular testing is only moderately sensitive, and thus, a negative test cannot exclude IE.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
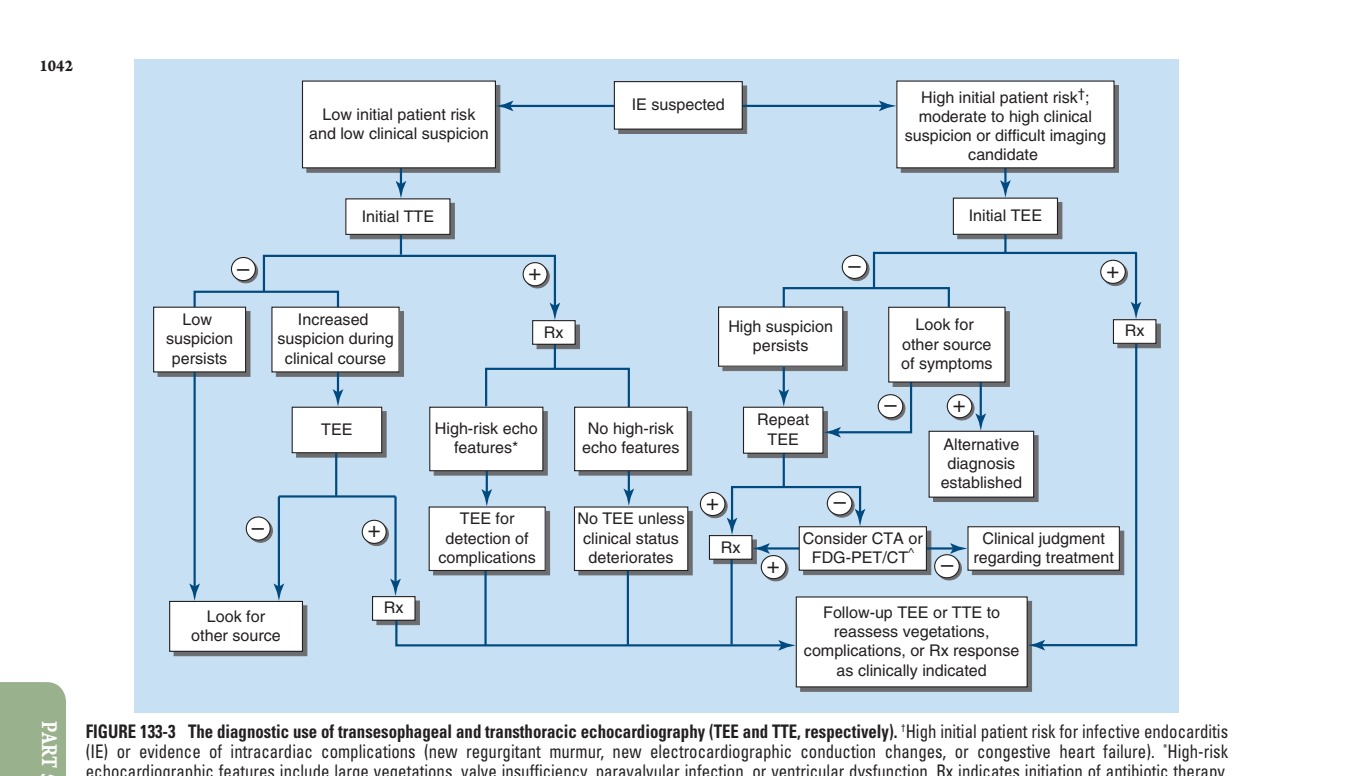
Caption: FIGURE 133-3 The diagnostic use of transesophageal and transthoracic (IE) or evidence of intracardiac complications (new regurgitant murmur, new echocardiographic features include large vegetations, valve insufficiency, paravalvular CTA, electrocardiogram-gated cardiac computed tomography (CT) angiogram; of these modalities. (Reproduced with permission from AS Bayer: Diagnosis and Figure 1.) — Figure 133-1: Vegetations (arrows) due to viridans streptococci endocarditis involving the mitral valve.
Figure 2¶

Caption: FIGURE 133-1 Vegetations (arrows) due to viridans streptococci endocarditis involving the mitral valve. — Figure 133-2 A: Janeway lesions on the toe (left) and plantar surface (right) of the foot in subacute Neisseria mucosa infective endocarditis (IE).
Figure 3¶

Caption: FIGURE 133-2 A. Janeway lesions on the toe (left) and plantar surface (right) of the Rachel Baden, MD.) B. Septic emboli with hemorrhage and infarction due to acute — Figure 133-2 B: Septic emboli with hemorrhage and infarction due to acute Staphylococcus aureus IE.
Figure 4¶

Caption: FIGURE 133-2 A. Janeway lesions on the toe (left) and plantar surface (right) of the Rachel Baden, MD.) B. Septic emboli with hemorrhage and infarction due to acute — Figure 133-3: Approach to echocardiographic evaluation of patients with suspected IE (illustrated in text).
Figure 5¶

Caption: FIGURE 133-2 A. Janeway lesions on the toe (left) and plantar surface (right) of the Rachel Baden, MD.) B. Septic emboli with hemorrhage and infarction due to acute — Figure 133-4: Representative transesophageal echocardiography (TEE) image showing vegetation on a prosthetic valve (inferred from text discussion of TEE utility).
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.