Tricuspid Valve Disease¶
Chapter 277 | Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Tricuspid stenosis (TS) is rare in North America and Western Europe, generally rheumatic in origin, and almost always associated with mitral stenosis (MS).
- Tricuspid regurgitation (TR) is common; >85% of cases are secondary (functional) due to annular dilation and leaflet tethering from RV remodeling.
- Carvallo's sign: A holosystolic murmur of TR that intensifies during inspiration and reduces during expiration or Valsalva maneuver.
- Surgical indication for TR: Annular dilation >40 mm on TTE or >70 mm intraoperatively, history of right heart failure, or PA hypertension.
- Transcatheter edge-to-edge repair (TEER) and transcatheter replacement are options for high/prohibitive surgical risk patients.
- Diuretics and aldosterone antagonists are useful for managing systemic venous congestion in severe TR.
- ECG in TS shows RA enlargement (tall P waves in lead II, upright P waves in V) without ECG evidence of RVH.
- TS does not occur as an isolated lesion; diagnosis is often missed unless associated MS is considered.
- Severe TR leads to RA enlargement, RV volume overload, and eventual systolic dysfunction.
- Perioperative mortality for isolated tricuspid valve surgery is high (~8–9%) and influenced by reoperation hazards.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Tricuspid Stenosis (TS)
- 1.2 Tricuspid Regurgitation (TR)
- 2. EPIDEMIOLOGY
- 2.1 Tricuspid Stenosis Epidemiology
- 2.2 Tricuspid Regurgitation Epidemiology
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Tricuspid Stenosis Pathophysiology
- 3.2 Tricuspid Regurgitation Pathophysiology
- 3.3 Etiologies of Tricuspid Valve Disease
- 4. CLINICAL FEATURES
- 4.1 Tricuspid Stenosis Clinical Features
- 4.2 Tricuspid Regurgitation Clinical Features
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Tricuspid Stenosis Differential Diagnosis
- 5.2 Tricuspid Regurgitation Differential Diagnosis
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Electrocardiography
- 6.2 Chest Radiography
- 6.3 Echocardiography
- 6.4 Cardiac Catheterization
- 7. MANAGEMENT & TREATMENT
- 7.1 Tricuspid Stenosis Treatment
- 7.2 Tricuspid Regurgitation Treatment
- 7.3 Surgical Indications
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Survival and Mortality
- 8.2 Complications
- 9. SPECIAL CONSIDERATIONS
- 9.1 Infective Endocarditis
- 9.2 Atrial Fibrillation
- 9.3 Mitral Valve Prolapse
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Exclusion Criteria
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Management of tricuspid regurgitation |
| 1 | 🖼 Figure | Tricuspid regurgitation |
| 2 | 🖼 Figure | Tricuspid regurgitation |
| 3 | 🖼 Figure | Transcatheter tricuspid valve (TV) repair and replacement |
| 4 | 🖼 Figure | Figure / Illustration |
| 5 | 🖼 Figure | Transcatheter tricuspid valve (TV) repair and replacement |
1. DEFINITION & OVERVIEW¶
Tricuspid valve disease encompasses tricuspid stenosis (TS) and tricuspid regurgitation (TR). TS is much less prevalent than mitral stenosis (MS) in North America and Western Europe. TR is more common than TS. TR is categorized as primary (organic, leaflet, or chordal related) or secondary (functional, atrial, and/or ventricular).
1.1 Tricuspid Stenosis (TS)¶
TS is generally rheumatic in origin and is more common in women than men. It does not occur as an isolated lesion and is usually associated with MS. Hemodynamically significant TS occurs in 5–10% of patients with severe MS; rheumatic TS is commonly associated with some degree of tricuspid regurgitation (TR). Nonrheumatic causes of TS are rare.
1.2 Tricuspid Regurgitation (TR)¶
More than 85% of TR cases encountered in clinical practice are secondary (functional) in nature and related to tricuspid annular dilation and leaflet tethering in the setting of RV remodeling caused by pressure or volume overload (or both), myocardial infarction (MI), or trauma. A third category of TR is that associated with cardiac implanted electronic device (CIED) leads from pacemakers or defibrillators. When placed across the tricuspid valve, the leads can result in leaflet entrapment or perforation. In addition, pacing from the right ventricular apex can result in dyssynchronous ventricular contraction and functional TR.
2. EPIDEMIOLOGY¶
Tricuspid stenosis (TS) is much less prevalent than mitral stenosis (MS) in North America and Western Europe. It is generally rheumatic in origin and is more common in women than men. Tricuspid regurgitation (TR) is more common than TS. More than 85% of TR cases encountered in clinical practice are secondary (functional) in nature.
2.1 Tricuspid Stenosis Epidemiology¶
TS is rare. It is generally rheumatic in origin. It is more common in women than men. It does not occur as an isolated lesion and is usually associated with MS.
2.2 Tricuspid Regurgitation Epidemiology¶
TR is common. >85% of cases are secondary (functional). Primary TR is less common. Primary TR results from congenitally deformed tricuspid valves, defects of the atrioventricular canal, Ebstein's malformation, carcinoid heart disease, endomyocardial fibrosis, radiation, infective endocarditis, and leaflet trauma.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Tricuspid valve disease etiologies are classified by valve lesion (stenosis vs regurgitation) and cause (primary vs secondary). TS is rheumatic. TR is secondary (functional) or primary (organic). Pathophysiology of TS involves a diastolic pressure gradient between the right atrium (RA) and right ventricle (RV). Pathophysiology of TR involves backward flow from RV to RA dependent on driving pressure and orifice size.
3.1 Tricuspid Stenosis Pathophysiology¶
A diastolic pressure gradient between the right atrium (RA) and right ventricle (RV) defines TS. It is augmented when the transvalvular blood flow increases during inspiration and declines during expiration. A mean diastolic pressure gradient of 4 mmHg is usually sufficient to elevate the mean RA pressure to levels that result in systemic venous congestion. Unless sodium intake has been restricted and diuretics administered, this venous congestion is associated with hepatomegaly, ascites, and edema, sometimes severe. In patients with sinus rhythm, the RA a wave may be extremely tall and may even approach the level of the RV systolic pressure. The y descent is prolonged. The cardiac output (CO) at rest is usually depressed, and it fails to rise during exercise. The low CO is responsible for the normal or only slightly elevated left atrial (LA), pulmonary artery (PA), and RV systolic pressures despite the presence of MS. Thus, the presence of TS can mask the hemodynamic and clinical features of any associated MS.
3.2 Tricuspid Regurgitation Pathophysiology¶
The incompetent tricuspid valve allows blood to flow backward from the RV into the RA, the volume of which is dependent on the driving pressure (i.e., RV systolic pressure) and the size of the regurgitant orifice. The severity and physical signs of TR can vary as a function of PA systolic pressure (in the absence of RV outflow tract stenosis), the dimensions of the tricuspid valve annulus, the respiratory cycle-dependent changes in RV preload, and RA compliance. RV filling is increased during inspiration. With TR, forward CO is reduced and does not augment with exercise. Significant degrees of TR will lead to RA enlargement and elevation of the RA and jugular venous pressures with prominent c-v waves in the pulse tracings. Progressively severe TR can lead to "ventricularization" of the RA wave form. Severe TR is also characterized by RV dilation (RV volume overload) and eventual systolic dysfunction, the progression of which can be accelerated by a concomitant pressure load from PA hypertension or by myocardial fibrosis from previous injury.
3.3 Etiologies of Tricuspid Valve Disease¶
Tricuspid stenosis etiologies include Rheumatic and Congenital causes. Tricuspid regurgitation etiologies include Rheumatic, Endocarditis, Myxomatous (TVP), Carcinoid, Radiation, Congenital (Ebstein's), Trauma (including that due to RV endomyocardial biopsy), and CIED related causes. Secondary TR is caused by RV and/or tricuspid annular dilation due to multiple causes (e.g., long-standing pulmonary HTN, remodeling post-RV MI, left-sided heart disease, cardiomyopathy, AF).
Table 1 — Table 277-1 Causes of Tricuspid Valve Diseases¶
| VALVE LESION | ETIOLOGIES | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Tricuspid stenosis | Rheumatic | Congenital | |||||||
| Tricuspid regurgitation | Rheumatic | Endocarditis | Myxomatous (TVP) | Carcinoid | Radiation | Congenital (Ebstein's) | Trauma (including that due to RV endomyocardial biopsy) | CIED related | Leaflet impingement, adherence, laceration, perforation, avulsion; chordal entrapment |
4. CLINICAL FEATURES¶
Patients with TS generally exhibit marked systemic venous congestion; salt restriction, bed rest, and diuretic therapy are required during the preoperative period. Characteristically, patients with severe TS complain of relatively little dyspnea for the degree of hepatomegaly, ascites, and edema that they have. However, fatigue secondary to a low CO and discomfort due to signs of right-sided congestion such as hepatomegaly and ascites are common in patients with advanced TS and/or TR. In some patients, TS may be suspected for the first time when symptoms of right-sided failure persist after an adequate mitral commissurotomy. Mild or moderate degrees of TR are usually well tolerated in the absence of other hemodynamic disturbances. Because TR often coexists with left-sided valve lesions, LV dysfunction, and/or PA hypertension, symptoms related to these lesions may dominate the clinical picture. Atrial functional TR due to atrial fibrillation is usually accompanied by palpitations. Fatigue and exertional dyspnea owing to reduced forward CO are early symptoms of isolated, severe TR. As the disease progresses and RV function declines, patients may report cervical pulsations, abdominal fullness/bloating, diminished appetite, and muscle wasting, although with progressive weight gain and painful swelling of the lower extremities.
4.1 Tricuspid Stenosis Clinical Features¶
Severe TS is associated with marked hepatic congestion, often resulting in cirrhosis, jaundice, serious malnutrition, anasarca, and ascites. Congestive hepatomegaly and, in cases of severe tricuspid valve disease, splenomegaly are present. The jugular veins are distended, and in patients with sinus rhythm, there may be giant a waves. The v waves are less conspicuous, and because tricuspid obstruction impedes RA emptying during diastole, there is a slow y descent. In patients with sinus rhythm, there may be prominent presystolic pulsations of the enlarged liver as well.
4.2 Tricuspid Regurgitation Clinical Features¶
The neck veins in patients with severe TR are distended with prominent c-v waves and rapid y descents (in the absence of TS). TR is more often diagnosed by examination of the neck veins than by auscultation of the heart sounds. Other findings may include marked hepatomegaly with systolic pulsations, ascites, pleural effusions, edema, and a positive hepatojugular reflux sign. A prominent RV pulsation in the left parasternal region and a blowing holosystolic murmur along the lower left sternal margin, which may be intensified during inspiration (Carvallo's sign) and reduced during expiration or the strain phase of the Valsalva maneuver, are characteristic findings. The murmur of TR may sometimes be confused with that of mitral regurgitation (MR) unless attention is paid to its variation during the respiratory cycle and the extent of RV enlargement is appreciated. AF may be the driver of TR or may emerge later in the disease with ventricular and atrial remodeling.
5. DIFFERENTIAL DIAGNOSIS¶
The murmur of TS has many of the qualities of the diastolic murmur of MS, and because TS almost always occurs in the presence of MS, it may be missed. However, the tricuspid murmur is generally heard best along the left lower sternal border and over the xiphoid process and is most prominent during presystole in patients with sinus rhythm. The murmur of TS is augmented during inspiration, and it is reduced during expiration and particularly during the strain phase of the Valsalva maneuver, when tricuspid transvalvular flow is reduced. The murmur of TR may sometimes be confused with that of mitral regurgitation (MR) unless attention is paid to its variation during the respiratory cycle and the extent of RV enlargement is appreciated. AF may be the driver of TR or may emerge later in the disease with ventricular and atrial remodeling.
5.1 Tricuspid Stenosis Differential Diagnosis¶
TS is generally rheumatic in origin. It does not occur as an isolated lesion and is usually associated with MS. The diagnosis may be missed unless it is considered. Severe TS is associated with marked hepatic congestion, often resulting in cirrhosis, jaundice, serious malnutrition, anasarca, and ascites. Congestive hepatomegaly and, in cases of severe tricuspid valve disease, splenomegaly are present.
5.2 Tricuspid Regurgitation Differential Diagnosis¶
TR can often emerge in the setting of new-onset atrial fibrillation (AF), particularly in older patients (atrial functional TR). Rheumatic fever may produce primary TR, often associated with TS. Tricuspid valve prolapse, carcinoid heart disease, endomyocardial fibrosis, radiation, infective endocarditis, and leaflet trauma can also produce primary TR. Less commonly, primary TR results from congenitally deformed tricuspid valves and can occur with defects of the atrioventricular canal, as well as with Ebstein's malformation of the tricuspid valve. A third category of TR is that associated with cardiac implanted electronic device (CIED) leads from pacemakers or defibrillators. When placed across the tricuspid valve, the leads can result in leaflet entrapment or perforation. In addition, pacing from the right ventricular apex can result in dyssynchronous ventricular contraction and functional TR.
6. INVESTIGATIONS & DIAGNOSIS¶
The electrocardiogram (ECG) features of RA enlargement (see Fig. 247-8) include tall, peaked P waves in lead II, as well as prominent, upright P waves in lead V. The absence of ECG evidence of RV hypertrophy (RVH) in a patient with right-sided heart failure who is believed to have MS should suggest associated tricuspid valve disease. The chest x-ray in patients with combined TS and MS shows particular prominence of the RA and superior vena cava without much enlargement of the PA and with less evidence of pulmonary vascular congestion than occurs in patients with isolated MS; engorgement of the azygos vein can often be appreciated. On transthoracic echocardiographic (TTE) examination, the tricuspid valve is usually thickened and domes in diastole; the transvalvular gradient can be estimated by continuous wave Doppler echocardiography. Severe TS is characterized by a valve area ≤1 cm2 or pressure half-time of ≥190 ms. The RA and inferior vena cava (IVC) are enlarged. TTE provides additional information regarding the severity of any associated TR, mitral valve structure and function, left ventricular (LV) and RV size and function, and PA pressure. Cardiac catheterization is not routinely necessary for assessment of TS. TTE is usually definitive with demonstration of RA dilation and RV volume overload and prolapsing, flail, scarred, or displaced/tethered tricuspid leaflets with annular dilation; the diagnosis and assessment of TR can be made by color flow Doppler imaging. Severe TR is accompanied by hepatic vein systolic flow reversal. Continuous wave Doppler of the TR velocity profile is useful in estimating PA systolic pressure, except when the TR is very severe and the jet velocity is blunted by rapidly increasing RA pressure. Accurate assessment of TR severity, PA pressures, and RV size and systolic function with TTE can be quite challenging in many patients. Real-time three-dimensional echocardiography and cardiac magnetic resonance (CMR) imaging provide alternative imaging modalities to aid in the assessment of TR severity, although they are not widely available. In patients with severe TR, the CO is usually markedly reduced, and the RA pressure pulse may not exhibit an x descent during early systole but rather show a prominent c-v wave with a rapid y descent. The mean RA and RV end-diastolic pressures are often elevated. Exercise testing can be used to assess functional capacity in patients with asymptomatic severe TR. The prognostic significance of exercise-induced changes in TR severity and RV function has not been well studied.
6.1 Electrocardiography¶
ECG features of RA enlargement include tall, peaked P waves in lead II, as well as prominent, upright P waves in lead V. The absence of ECG evidence of RV hypertrophy (RVH) in a patient with right-sided heart failure who is believed to have MS should suggest associated tricuspid valve disease. The ECG may show changes characteristic of the lesion responsible for the TR, e.g., an inferior Q-wave MI suggestive of a prior RV MI, RVH, or a bizarre right bundle branch block–type pattern with preexcitation in patients with Ebstein's anomaly. ECG signs of RA enlargement may be present in patients with sinus rhythm; AF is frequently noted.
6.2 Chest Radiography¶
The chest x-ray in patients with combined TS and MS shows particular prominence of the RA and superior vena cava without much enlargement of the PA and with less evidence of pulmonary vascular congestion than occurs in patients with isolated MS; engorgement of the azygos vein can often be appreciated. The chest x-ray may show RA and RV enlargement, depending on the chronicity and severity of TR.
6.3 Echocardiography¶
TTE is usually definitive with demonstration of RA dilation and RV volume overload and prolapsing, flail, scarred, or displaced/tethered tricuspid leaflets with annular dilation; the diagnosis and assessment of TR can be made by color flow Doppler imaging. Severe TR is accompanied by hepatic vein systolic flow reversal. Continuous wave Doppler of the TR velocity profile is useful in estimating PA systolic pressure, except when the TR is very severe and the jet velocity is blunted by rapidly increasing RA pressure. Accurate assessment of TR severity, PA pressures, and RV size and systolic function with TTE can be quite challenging in many patients. Real-time three-dimensional echocardiography and cardiac magnetic resonance (CMR) imaging provide alternative imaging modalities to aid in the assessment of TR severity, although they are not widely available. Severe TS is characterized by a valve area ≤1 cm2 or pressure half-time of ≥190 ms.
6.4 Cardiac Catheterization¶
Cardiac catheterization is not routinely necessary for assessment of TS. Of right and left heart catheterization is rarely necessary but can also show prolapse of the posterior and sometimes of both mitral valve leaflets.
7. MANAGEMENT & TREATMENT¶
Patients with TS generally exhibit marked systemic venous congestion; salt restriction, bed rest, and diuretic therapy are required during the preoperative period. Such a preparatory period may diminish hepatic congestion and thereby improve hepatic function sufficiently so that the risks of operation, particularly bleeding, are diminished. Surgical relief of the TS should be carried out, preferably at the time of surgical mitral commissurotomy or mitral valve replacement (MVR) for mitral valve disease, in patients with moderate or severe TS who have mean diastolic pressure gradients exceeding ~4 mmHg and tricuspid orifice areas 40 mm), a history of right heart failure, or PA hypertension. Diuretics can be useful for patients with severe TR and signs of right heart failure. An aldosterone antagonist may be particularly helpful because many patients have secondary hyperaldosteronism from marked hepatic congestion. Therapies to reduce elevated PA pressures and/or pulmonary vascular resistance, including those targeted at left-sided heart disease, can also be considered for patients with PA hypertension and severe secondary TR. Tricuspid valve surgery is recommended for patients with severe TR who are undergoing left-sided valve surgery and is also undertaken frequently for treatment of even moderate TR in patients undergoing left-sided valve surgery especially those with tricuspid annular dilation (>40 mm), a history of right heart failure, or PA hypertension. In a randomized trial of tricuspid valve annuloplasty surgery at the time of mitral valve surgery for degenerative MR in patients with moderate TR or mild TR with annular dilation, there was a significant reduction in the 2-year incidence of a composite end-point of reoperation, progression of TR, or all-cause death among those who underwent tricuspid surgery versus those who had mitral valve surgery alone. The composite endpoint was driven by a reduction in the progression of TR. Surgery may also infrequently be required for treatment of severe, primary TR with right heart failure not responsive to standard medical therapy or because of progressively declining RV systolic function. Reported perioperative mortality rates for isolated tricuspid valve surgery (repair and replacement) are high (~8–9%) and likely are influenced by the hazards encountered during reoperation on patients who have undergone previous left-sided valve surgery and have reduced RV function. There have been several recent advances in the application of transcatheter tricuspid valve repair and replacement techniques in patients with severe TR and high or prohibitive surgical risk. In a randomized trial of percutaneous transcatheter edge-to-edge repair versus medical therapy, clip repair resulted in a significant reduction in TR severity and improvement in quality-of-life scores, but no differences in all-cause mortality or hospitalization for heart failure over 1-year follow-up. The U.S. Food and Drug Administration approved the use of a transcatheter tricuspid valve replacement system in early 2024 based on favorable hemodynamic, echocardiographic, clinical, and quality-of-life results from prospective single-arm studies. Infective endocarditis prophylaxis is indicated for patients with a prior history of endocarditis. Beta blockers sometimes relieve chest pain and control palpitations. Decisions regarding anticoagulation for stroke prevention in AF should be based on the CHADS-VASc score and an assessment of bleeding risk. If the patient is symptomatic from severe MR, mitral valve repair is indicated. Most often, the MR will be reduced in severity but not eliminated. Nevertheless, symptom status and indices of LV size and function can be improved with this approach, which is now offered at >540 specialized sites in the United States. Reported hospital mortality rates following the procedure are <2%. Transcatheter replacement devices remain under active investigation but are not yet approved for use in the United States.
7.1 Tricuspid Stenosis Treatment¶
Patients with TS generally exhibit marked systemic venous congestion; salt restriction, bed rest, and diuretic therapy are required during the preoperative period. Such a preparatory period may diminish hepatic congestion and thereby improve hepatic function sufficiently so that the risks of operation, particularly bleeding, are diminished. Surgical relief of the TS should be carried out, preferably at the time of surgical mitral commissurotomy or mitral valve replacement (MVR) for mitral valve disease, in patients with moderate or severe TS who have mean diastolic pressure gradients exceeding ~4 mmHg and tricuspid orifice areas <1.5–2 cm2. TS is almost always accompanied by significant TR. Operative repair may permit substantial improvement of tricuspid valve function. If repair cannot be accomplished, the tricuspid valve may have to be replaced. Meta-analysis has shown no difference in overall survival between mechanical and tissue valve replacement. Mechanical valves in the tricuspid position are more prone to thromboembolic complications than in other positions. Percutaneous tricuspid balloon commissurotomy for isolated severe TS without significant TR is very rarely performed.
7.2 Tricuspid Regurgitation Treatment¶
Diuretics can be useful for patients with severe TR and signs of right heart failure. An aldosterone antagonist may be particularly helpful because many patients have secondary hyperaldosteronism from marked hepatic congestion. Therapies to reduce elevated PA pressures and/or pulmonary vascular resistance, including those targeted at left-sided heart disease, can also be considered for patients with PA hypertension and severe secondary TR. Tricuspid valve surgery is recommended for patients with severe TR who are undergoing left-sided valve surgery and is also undertaken frequently for treatment of even moderate TR in patients undergoing left-sided valve surgery especially those with tricuspid annular dilation (>40 mm), a history of right heart failure, or PA hypertension. In a randomized trial of tricuspid valve annuloplasty surgery at the time of mitral valve surgery for degenerative MR in patients with moderate TR or mild TR with annular dilation, there was a significant reduction in the 2-year incidence of a composite end-point of reoperation, progression of TR, or all-cause death among those who underwent tricuspid surgery versus those who had mitral valve surgery alone. The composite endpoint was driven by a reduction in the progression of TR. Surgery may also infrequently be required for treatment of severe, primary TR with right heart failure not responsive to standard medical therapy or because of progressively declining RV systolic function. Reported perioperative mortality rates for isolated tricuspid valve surgery (repair and replacement) are high (~8–9%) and likely are influenced by the hazards encountered during reoperation on patients who have undergone previous left-sided valve surgery and have reduced RV function. There have been several recent advances in the application of transcatheter tricuspid valve repair and replacement techniques in patients with severe TR and high or prohibitive surgical risk. In a randomized trial of percutaneous transcatheter edge-to-edge repair versus medical therapy, clip repair resulted in a significant reduction in TR severity and improvement in quality-of-life scores, but no differences in all-cause mortality or hospitalization for heart failure over 1-year follow-up. The U.S. Food and Drug Administration approved the use of a transcatheter tricuspid valve replacement system in early 2024 based on favorable hemodynamic, echocardiographic, clinical, and quality-of-life results from prospective single-arm studies.
7.3 Surgical Indications¶
Tricuspid valve surgery is recommended for patients with severe TR who are undergoing left-sided valve surgery and is also undertaken frequently for treatment of even moderate TR in patients undergoing left-sided valve surgery especially those with tricuspid annular dilation (>40 mm), a history of right heart failure, or PA hypertension. Annular dilation is defined by >40 mm on transthoracic echocardiography (>21 mm/m2) or >70 mm on direct intraoperative measurement. Surgery can also be considered for low-risk asymptomatic patients in whom a successful and durable repair can be achieved with at least 95% likelihood by an expert surgeon. Mitral valve repair is preferred over replacement in patients with MVP or flail mitral leaflet. Repair of isolated posterior leaflet prolapse is usually straightforward, but increasingly more complex pathologies (e.g., anterior leaflet prolapse, bileaflet prolapse, Barlow's deformity) require advanced skills. Careful pre- and intraoperative TEE imaging is an important component of patient evaluation and surgical planning. Transcatheter edge-to-edge repair (TEER) using one of two commercially available systems to grasp the anterior and posterior leaflets together can be considered for treatment of symptomatic patients at prohibitive or high surgical risk with severe primary MR due to MVP.
8. PROGNOSIS & COMPLICATIONS¶
Meta-analysis has shown no difference in overall survival between mechanical and tissue valve replacement. Mechanical valves in the tricuspid position are more prone to thromboembolic complications than in other positions. Reported perioperative mortality rates for isolated tricuspid valve surgery (repair and replacement) are high (~8–9%) and likely are influenced by the hazards encountered during reoperation on patients who have undergone previous left-sided valve surgery and have reduced RV function. In a randomized trial of percutaneous transcatheter edge-to-edge repair versus medical therapy, clip repair resulted in a significant reduction in TR severity and improvement in quality-of-life scores, but no differences in all-cause mortality or hospitalization for heart failure over 1-year follow-up. The composite endpoint was driven by a reduction in the progression of TR.
8.1 Survival and Mortality¶
Meta-analysis has shown no difference in overall survival between mechanical and tissue valve replacement. Reported perioperative mortality rates for isolated tricuspid valve surgery (repair and replacement) are high (~8–9%) and likely are influenced by the hazards encountered during reoperation on patients who have undergone previous left-sided valve surgery and have reduced RV function.
8.2 Complications¶
Mechanical valves in the tricuspid position are more prone to thromboembolic complications than in other positions. Surgery may also infrequently be required for treatment of severe, primary TR with right heart failure not responsive to standard medical therapy or because of progressively declining RV systolic function.
9. SPECIAL CONSIDERATIONS¶
Infective endocarditis prophylaxis is indicated for patients with a prior history of endocarditis. Beta blockers sometimes relieve chest pain and control palpitations. Decisions regarding anticoagulation for stroke prevention in AF should be based on the CHADS-VASc score and an assessment of bleeding risk. If the patient is symptomatic from severe MR, mitral valve repair is indicated. Most often, the MR will be reduced in severity but not eliminated. Nevertheless, symptom status and indices of LV size and function can be improved with this approach, which is now offered at >540 specialized sites in the United States. Reported hospital mortality rates following the procedure are <2%. Transcatheter replacement devices remain under active investigation but are not yet approved for use in the United States.
9.1 Infective Endocarditis¶
Infective endocarditis prophylaxis is indicated for patients with a prior history of endocarditis.
9.2 Atrial Fibrillation¶
Decisions regarding anticoagulation for stroke prevention in AF should be based on the CHADS-VASc score and an assessment of bleeding risk. Atrial functional TR due to atrial fibrillation is usually accompanied by palpitations.
9.3 Mitral Valve Prolapse¶
If the patient is symptomatic from severe MR, mitral valve repair is indicated. Most often, the MR will be reduced in severity but not eliminated. Nevertheless, symptom status and indices of LV size and function can be improved with this approach, which is now offered at >540 specialized sites in the United States. Reported hospital mortality rates following the procedure are <2%.
10. KEY PEARLS & CLINICAL TRAPS¶
TS does not occur as an isolated lesion and is usually associated with MS. TS is almost always accompanied by significant TR. TS is generally rheumatic in origin and is more common in women than men. TR is more common than TS. More than 85% of TR cases encountered in clinical practice are secondary (functional) in nature. Carvallo's sign is a characteristic finding. The murmur of TR may sometimes be confused with that of mitral regurgitation (MR) unless attention is paid to its variation during the respiratory cycle and the extent of RV enlargement is appreciated. AF may be the driver of TR or may emerge later in the disease with ventricular and atrial remodeling. The absence of ECG evidence of RV hypertrophy (RVH) in a patient with right-sided heart failure who is believed to have MS should suggest associated tricuspid valve disease. The diagnosis may be missed unless it is considered. Severe TS is associated with marked hepatic congestion, often resulting in cirrhosis, jaundice, serious malnutrition, anasarca, and ascites. Congestive hepatomegaly and, in cases of severe tricuspid valve disease, splenomegaly are present. The jugular veins are distended, and in patients with sinus rhythm, there may be giant a waves. The v waves are less conspicuous, and because tricuspid obstruction impedes RA emptying during diastole, there is a slow y descent. In patients with sinus rhythm, there may be prominent presystolic pulsations of the enlarged liver as well. The neck veins in patients with severe TR are distended with prominent c-v waves and rapid y descents (in the absence of TS). TR is more often diagnosed by examination of the neck veins than by auscultation of the heart sounds. Other findings may include marked hepatomegaly with systolic pulsations, ascites, pleural effusions, edema, and a positive hepatojugular reflux sign. A prominent RV pulsation in the left parasternal region and a blowing holosystolic murmur along the lower left sternal margin, which may be intensified during inspiration (Carvallo's sign) and reduced during expiration or the strain phase of the Valsalva maneuver, are characteristic findings.
10.1 Diagnostic Clues¶
Carvallo's sign: A holosystolic murmur of TR that intensifies during inspiration and reduces during expiration or Valsalva maneuver. RA enlargement on ECG (tall P waves in lead II, upright P waves in V). Hepatic congestion signs (hepatomegaly, ascites, edema). Giant a waves in sinus rhythm. Slow y descent in TS. Prominent c-v waves and rapid y descents in TR (absence of TS).
10.2 Exclusion Criteria¶
TS does not occur as an isolated lesion. TS is almost always accompanied by significant TR. Nonrheumatic causes of TS are rare. TS is generally rheumatic in origin. TS is more common in women than men. TS is much less prevalent than mitral stenosis (MS) in North America and Western Europe.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
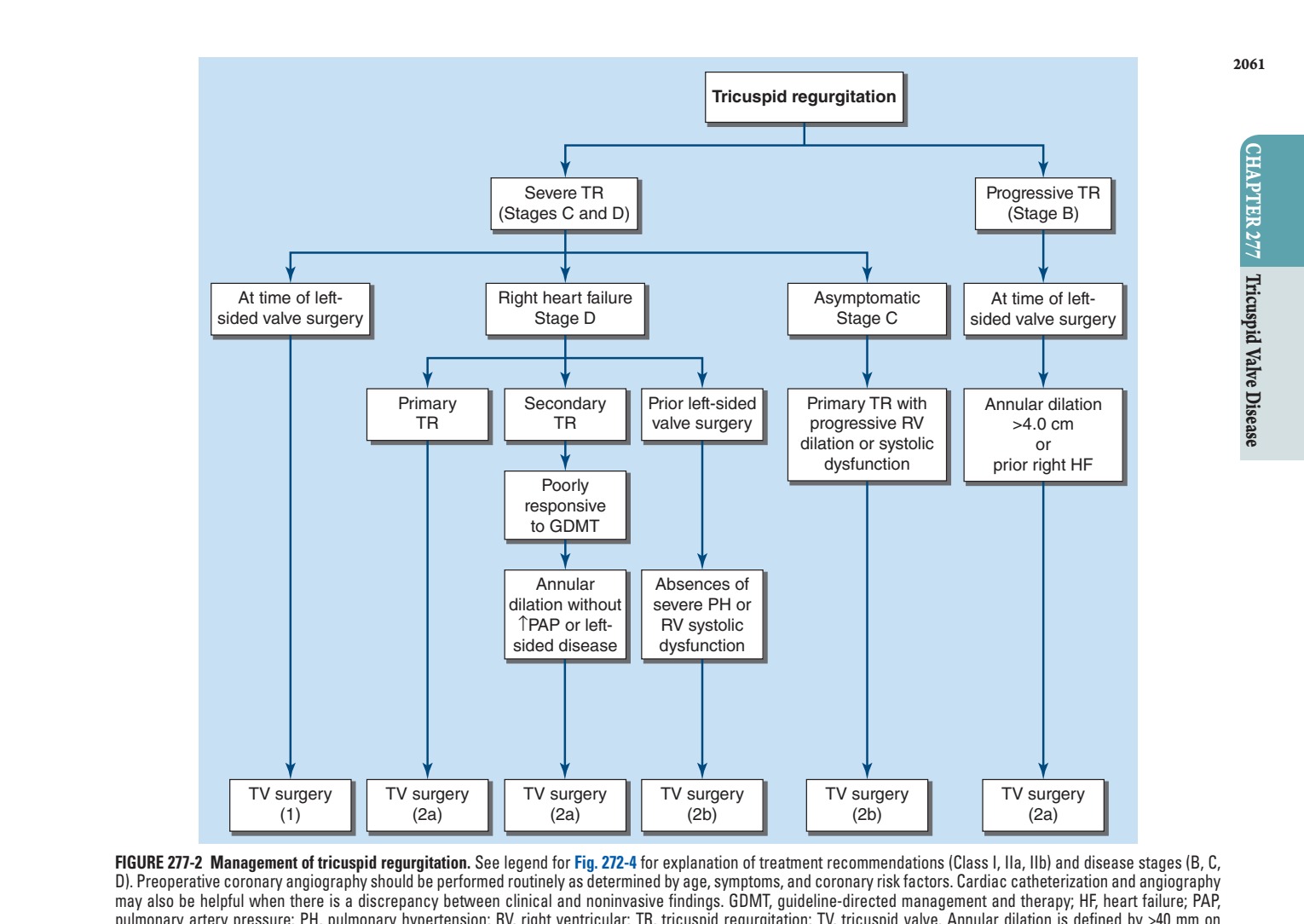
Caption: FIGURE 277-2 Management of tricuspid regurgitation. See legend for Fig. 272-4 for D). Preoperative coronary angiography should be performed routinely as determined by may also be helpful when there is a discrepancy between clinical and noninvasive pulmonary artery pressure; PH, pulmonary hypertension; RV, right ventricular; TR, transthoracic echocardiography (>21 mm/m2) or >70 mm on direct intraoperative for management of patients with valvular heart disease: A report of the American Circulation 143:e72, 2021.)
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 277-1 Tricuspid regurgitation. A. Transthoracic apical two-chamber view (white arrows) traversing the tricuspid valve. The plane of tricuspid valve closure is shows a broad jet of severe tricuspid regurgitation (between the yellow arrows) refluxing — Transthoracic echocardiographic apical two-chamber view showing the right atrium and right ventricle with a pacemaker lead traversing the tricuspid valve.
Figure 2¶

Caption: FIGURE 277-1 Tricuspid regurgitation. A. Transthoracic apical two-chamber view (white arrows) traversing the tricuspid valve. The plane of tricuspid valve closure is shows a broad jet of severe tricuspid regurgitation (between the yellow arrows) refluxing — Corresponding color flow Doppler image in systole showing a broad jet of severe tricuspid regurgitation refluxing into the right atrium.
Figure 3¶

Caption: FIGURE 277-3 Transcatheter tricuspid valve (TV) repair and replacement. A. Shown is a clip device that can be used to grasp the leading edges of the TV leaflets to reduce the severity of tricuspid regurgitation (TR) by decreasing the effective orifice area of the valve. (TriClip is a trademark of Abbott or its related companies.) B. Bioprosthetic heart valve replacement approved for percutaneous treatment of severe TR is selected for high or prohibitive surgical risk patients. (EVOQUE is a trademark of Edwards Lifesciences.) — Management algorithm for tricuspid regurgitation illustrating treatment recommendations for primary and secondary TR across disease stages B, C, and D.
Figure 4¶

Caption: Transcatheter tricuspid valve repair using a clip device to grasp the leading edges of the tricuspid valve leaflets to reduce regurgitation severity.
Figure 5¶

Caption: FIGURE 277-3 Transcatheter tricuspid valve (TV) repair and replacement. A. Shown is a clip device that can be used to grasp the leading edges of the TV leaflets to reduce the severity of tricuspid regurgitation (TR) by decreasing the effective orifice area of the valve. (TriClip is a trademark of Abbott or its related companies.) B. Bioprosthetic heart valve replacement approved for percutaneous treatment of severe TR is selected for high or prohibitive surgical risk patients. (EVOQUE is a trademark of Edwards Lifesciences.) — Bioprosthetic heart valve replacement selected for percutaneous treatment of severe tricuspid regurgitation in high or prohibitive surgical risk patients.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.