Chapter 227 | Pneumocystis Infections¶
Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Fungal
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Pneumocystis jirovecii is an opportunistic fungal pathogen causing pneumonia primarily in immunocompromised hosts (HIV/AIDS, transplant, high-dose steroids).
- Diagnosis relies on demonstration of organisms in lung tissue or BAL fluid using specific stains (silver, immunofluorescence) or PCR; BAL is the gold standard.
- First-line treatment is Trimethoprim-Sulfamethoxazole (TMP-SMX) for 14 days (non-HIV mild) or 21 days (all other).
- Glucocorticoids are indicated for moderate to severe disease (PaO2 <70 mmHg or A-a gradient ≥35 mmHg) to reduce inflammation.
- CD4+ T-cell count 200/μL do not guarantee protection in non-HIV immunosuppression.
- A normal chest CT essentially rules out PCP; diffuse bilateral interstitial infiltrates are classic but not specific.
- TMP-SMX hypersensitivity is common in HIV; alternatives include Atovaquone, Clindamycin-Primaquine, or Pentamidine.
- Untreated PCP is invariably fatal; prognosis depends on underlying disease, need for intubation, and comorbidities.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Organism Biology
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Lung Pathology
- 4. CLINICAL FEATURES
- 4.1 Physical Examination & Oxygenation
- 4.2 Radiographic Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria & Thresholds
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Therapy
- 7.2 Treatment Failure & Switching
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Mortality Risk Factors
- 9. SPECIAL CONSIDERATIONS
- 9.1 Prophylaxis
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Direct microscopy of Pneumocystis pneumonia |
| 2 | 🖼 Figure | Direct microscopy of Pneumocystis pneumonia |
| 3 | 🖼 Figure | Radiographs in Pneumocystis pneumonia |
| 4 | 🖼 Figure | Radiographs in Pneumocystis pneumonia |
| 5 | 🖼 Figure | Direct microscopy of Pneumocystis pneumonia |
| 6 | 🖼 Figure | Radiographs in Pneumocystis pneumonia |
| 7 | 🖼 Figure | Direct microscopy of Pneumocystis pneumonia |
| 8 | 🖼 Figure | Radiographs in Pneumocystis pneumonia |
1. DEFINITION & OVERVIEW¶
📖 Harrison's defines this as:
Pneumocystis is an opportunistic pathogen that is an important cause of pneumonia in immunocompromised hosts, particularly those with HIV infection, organ transplants, or hematologic malignancies and those receiving high-dose glucocorticoids or certain immunosuppressive monoclonal antibodies.
- Pneumocystis is an opportunistic pathogen that is an important cause of pneumonia in immunocompromised hosts.
- Pneumocystis was discovered in rodents in 1909 and was initially believed to be a protozoan.
- Molecular techniques have demonstrated that the organism is actually a fungus.
- Formerly known as Pneumocystis carinii, the species specific to humans has been renamed Pneumocystis jirovecii.
- The species specific to rats is Pneumocystis carinii; there are multiple variants of Pneumocystis specific to other animals.
- Systemic infection occurs almost exclusively in immunocompromised hosts, especially those who have hematologic malignancies, are neutropenic, have received a solid organ or hematopoietic stem cell transplantation, or are receiving corticosteroids.
- Severe neutropenia is a major risk factor for disseminated disease.
- Myeloid phagocytes and their oxidative burst are critical for protection against Trichosporon (related context), but for Pneumocystis, CD4+ T cells are critical in host defense.
1.1 Organism Biology¶
- The life cycle of Pneumocystis likely involves both sexual and asexual reproduction.
- The organism exists as a trophic form, a cyst, and a precyst.
- Studies in rodents show that immunocompetent animals can serve as reservoirs for respiratory transmission of P. carinii (the infecting species in rats) to immunocompetent and immunosuppressed rats.
- Human Pneumocystis is thought to be transmitted by a respiratory route as well.
- P. jirovecii, like all pneumocystis species, is host-specific.
- Thus, humans are not infected, for example, by P. carinii (rodents) or P. oryctolagi (rabbits), but are only infected by P. jirovecii, which is from other humans.
- Serologic and molecular studies have demonstrated that most humans are exposed to P. jirovecii and infected early in life.
- It was historically thought that Pneumocystis pneumonia usually developed from reactivation of latent infection.
- However, molecular evidence makes it clear that children and adults can develop PCP from primary infection or reinfection.
- The source of infection is thought to be either healthy or immunosuppressed individuals who themselves experienced recent infection or reinfection, or immunosuppressed persons with clinical PCP.
- Nosocomial outbreaks among immunosuppressed persons occur in inpatient and outpatient settings.
- The utility of drop or airborne isolation for preventing transmission from patients with PCP to other immunosuppressed individuals has been debated; no clear evidence exists, although it seems prudent to isolate patients with active PCP from other immunosuppressed patients using at least droplet precautions.
2. EPIDEMIOLOGY¶
- PCP came to medical attention in the early 1950s when pathologists in Czechoslovakia recognized Pneumocystis in the alveolar exudates of infants involved in nursery outbreaks of interstitial pneumonia.
- Outbreaks had been described in Europe since the 1920s.
- Among adults, PCP was rarely recognized until the populations of immunosuppressed adults increased due to the development of immunosuppressive therapies for solid-organ transplantation, bone marrow transplantation, cancer, and autoimmune disorders, and until the development of better pulmonary diagnostic techniques such as bronchoscopy.
- In 1981, PCP was first reported in men who had sex with men and in intravenous (IV) drug users who had no obvious cause of immunosuppression.
- These cases were subsequently recognized as the first cases of what came to be known as the acquired immunodeficiency syndrome (AIDS).
- The incidence of PCP increased dramatically as the AIDS epidemic grew.
- Without PCP chemoprophylaxis or antiretroviral therapy (ART), 80–90% of patients with HIV/AIDS in North America and Western Europe ultimately developed one or more episodes of PCP.
- While its incidence declined with the introduction of anti-Pneumocystis prophylaxis and durably effective ART, PCP has continued to be an important cause of AIDS-associated morbidity in the United States and Western Europe, particularly in individuals who do not know they are infected with HIV until they are profoundly immunosuppressed.
- PCP also develops in HIV-uninfected patients who are immunocompromised secondary to congenital immunodeficiencies, hemologic or malignant neoplasms, stem cell or solid-organ transplantation, and treatment with immunosuppressive medications.
- The incidence of PCP depends on the degree and duration of immunosuppression.
- PCP is increasingly reported among individuals receiving tumor necrosis factor α inhibitors and certain (but not all) immunosuppressive monoclonal antibodies for autoimmune, rheumatologic, or neoplastic diseases.
- In many health care systems, PCP occurs more often due to non-HIV-related immunosuppression than due to HIV infection.
- In some developing countries, the incidence of PCP among PLWH has been reported to be lower than that in more industrialized countries.
- This lower incidence may be due to competing mortality from infectious diseases such as tuberculosis and bacterial pneumonia, which typically occur before patients become immunosuppressed enough to develop PCP.
- Geographic variations in Pneumocystis exposure and underdiagnosis attributable to lack of diagnostic resources also may explain the apparent lower frequency of PCP in some countries.
2.1 Risk Factors¶
- HIV infection (CD4+ T-cell count <200/μL).
- Solid-organ transplantation.
- Hematopoietic stem cell transplantation.
- High-dose glucocorticoids.
- Certain immunosuppressive monoclonal antibodies (e.g., rituximab, alemtuzumab).
- Fludarabine, temozolomide, temsirolimus.
- Congenital immunodeficiencies.
- Neutropenia.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- CD4+ T cells are critical in host defense against Pneumocystis.
- Among PLWH, the incidence of PCP is inversely related to the CD4+ T-cell count: at least 80% of cases occur at counts of 200/μL in persons with HIV infection, but such occurrences are uncommon, especially with CD4+ T-cell counts substantially higher than 200/μL.
- CD4+ T-cell counts are less useful in predicting the risk of PCP in patients who are immunosuppressed for reasons other than HIV infection.
- In these populations, a CD4+ T-cell count 200/μL in many populations does not imply protection.
- For patients who are immunosuppressed as a result of factors other than HIV infection, the CD4+ T-cell counts 200/μL are not a reliable marker of protection from PCP.
- For these patients who are immunosuppressed due to causes other than HIV infection, the period of susceptibility is usually estimated on the basis of experience with the underlying disease and the specific immunosuppressive regimen.
- Cessation of prophylaxis has been associated with clusters of cases in certain patient populations, such as solid-organ transplant recipients, where the period of susceptibility is not well-defined.
- Patients receiving a prolonged course of high-dose glucocorticoids predispose patients to PCP.
3.1 Lung Pathology¶
- Pneumocystis has a unique tropism for the lung.
- Organisms are presumably inhaled into the alveolar space after being exhaled by another human.
- Clinically apparent pneumonia occurs only if an individual is immunocompromised.
- Pneumocystis proliferates in the lung, provoking a mononuclear cell response.
- The alveoli become filled with proteinaceous material, and alveolar damage results in increased alveolar-capillary injury and surfactant abnormalities.
- While clinical disease due to Pneumocystis in immunocompetent hosts has not been clearly documented, studies have shown that Pneumocystis organisms can cause subclinical infection among children and adults who are not immunocompromised and can be associated with pulmonary pathology.
- The relevance of these organisms to acute or chronic clinical syndromes, such as chronic obstructive pulmonary disease (COPD), in immunocompetent patients is being investigated.
- Stained lung sections typically show foamy, vacuolated alveolar exudates composed largely of viable and nonviable organisms.
- Interstitial edema and fibrosis may develop, and organisms can be seen in the alveolar space with silver or other stains.
- The organisms can also be seen when tissue is subjected to colorimetric or immunofluorescent staining.
4. CLINICAL FEATURES¶
- PCP presents as acute or subacute pneumonia that may initially be characterized by a vague sense of dyspnea alone, but that subsequently manifests as fever and nonproductive cough with progressive shortness of breath.
- Patients may ultimately progress to respiratory failure and death.
- Extrapulmonary manifestations of PCP are rare, but can include involvement of almost any organ, most notably the lymph nodes, spleen, and liver.
- The physical examination findings in PCP are nonspecific.
- Patients have decreased oxygen saturation—at rest or with exertion—that, without treatment, progresses to severe hypoxemia.
- Patients may initially have a normal chest examination and no adventitious sounds, but later develop diffuse rales and signs of consolidation.
- Untreated, PCP is invariably fatal.
- Patients with HIV infection often have an indolent course that may present early as mild exercise intolerance or chest tightness without fever or cough and a normal or nearly normal posterior–anterior chest radiograph.
- However, this process progresses over days, weeks, or even a few months to fever, cough, diffuse alveolar infiltrates, and profound hypoxemia.
- Some patients with HIV infection and most patients with other types of immunosuppression have more acute disease that progresses over a few days to respiratory failure.
- Rare patients also develop distributive shock due to PCP.
- A few unusual patients present with extrapulmonary manifestations in the skin or soft tissue, retina, brain, liver, kidney, or spleen.
- Extrapulmonary disease is nonspecific in presentation and can be diagnosed only by histology.
- When there is extrapulmonary clinical disease in a patient with PCP, the priority is to determine what other concurrent infectious or neoplastic process might be present, given the rarity of extrapulmonary pneumocystosis.
4.1 Physical Examination & Oxygenation¶
- Decreased oxygen saturation at rest or with exertion.
- Progression to severe hypoxemia without treatment.
- Normal chest examination initially, later diffuse rales and signs of consolidation.
4.2 Radiographic Findings¶
- The initial chest radiograph may be normal when patients have mild symptoms.
- The classic radiographic appearance of symptomatic PCP consists of diffuse bilateral interstitial infiltrates that are perihilar and symmetric.
- The interstitial infiltrates can progress to alveolar filling.
- High-resolution chest computed tomography (CT) shows diffuse ground-glass opacities in virtually all patients with PCP, often before a routine chest radiograph becomes abnormal.
- A normal chest CT essentially rules out the diagnosis of PCP.
- Pneumatoceles and pneumothoraces are characteristic chest radiographic findings, especially in patients with HIV infection.
- A wide variety of atypical radiographic findings have been described, including asymmetric patterns, upper-lobe infiltrates, mediastinal adenopathy, nodules, cavities, and effusions.
5. DIFFERENTIAL DIAGNOSIS¶
- Differential diagnosis includes other causes of diffuse bilateral interstitial infiltrates.
- Other concurrent infectious or neoplastic processes must be considered in the presence of extrapulmonary manifestations.
- Congestive heart failure, pulmonary emboli, pulmonary hypertension, drug toxicity, or a neoplastic process are causes of pulmonary dysfunction that must be ruled out if PCP treatment fails.
6. INVESTIGATIONS & DIAGNOSIS¶
- The optimal sample for a specific microbiologic diagnostic examination depends on how ill the patient is and what resources are available.
- Before the 1990s, diagnoses of PCP were usually established by open lung biopsy; later, transbronchial lung biopsy was employed.
- Hematoxylin and eosin (H and E) staining of pulmonary tissue demonstrates a foamy alveolar filling and a mononuclear interstitial infiltrate. This appearance is pathognomonic for PCP even though the organisms cannot be specifically identified with this H and E stain.
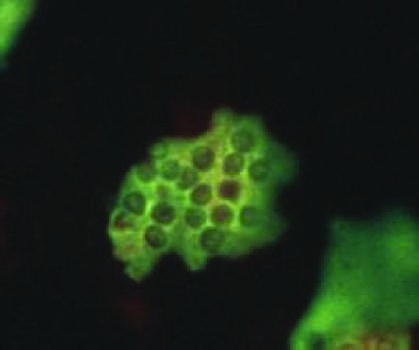
- Since human pneumocystis has never been successfully cultured, the diagnosis is typically established in lung tissue or pulmonary secretions by staining of the cyst and or trophozoite with methenamine silver, toluidine blue O, or Giemsa—or by staining with a specific immunofluorescent antibody.
- Since the 1990s, bronchoalveolar lavage (BAL) has become the most common method for obtaining a sample of respiratory secretions in which to detect Pneumocystis organisms.
- The demonstration of organisms in BAL fluid is almost 100% sensitive and specific for PCP.
- The organisms are identified in pulmonary secretions with the specific stains indicated above for lung biopsy.
- While expectorated sputum or throat swabs have very low sensitivity, an induced sputum sample obtained and interpreted by an experienced provider can be highly sensitive and specific; however, the sensitivity is dependent on both the characteristics of the patient, the quality of the sputum sample, and the experience of the center conducting the test and is widely variable (55–90%).
- Many laboratories offer polymerase chain reaction (PCR) testing of respiratory specimens for Pneumocystis in preference to direct microscopy of stained respiratory secretions.
- However, PCR tests are so sensitive that it is difficult to distinguish patients with colonization (i.e., those whose acute lung disease is due to some other process but who have low levels of Pneumocystis DNA in their lungs) from those with acute pneumonia due to Pneumocystis.
- The PCR cycle number is probably helpful, i.e., the lower the cycle number, the more DNA was detected. However, PCR tests for PCP are not standardized and specimen collection can vary considerably resulting in variable quality of the specimens assessed.
- Therefore, there is no specific PCR threshold that can be deemed to be especially convincing.
- Such PCR tests on appropriate samples may be more useful for ruling out a diagnosis of PCP if they are negative than for definitively attributing the disease to Pneumocystis if they are positive.
- There has been considerable interest in serologic tests, such as assays for (1→3)-β-d-glucan, a component of the fungal cell wall.
- Serum (1→3)-β-d-glucan levels are frequently elevated in patients with PCP.
- However, serum or BAL (1→3)-β-d-glucan levels are not perfectly sensitive or highly specific for PCP.
- There are increasing numbers of studies of serum PCR tests for Pneumocystis, but such serum tests are not yet useful for establishing the presence or absence of PCP.
6.1 Diagnostic Criteria & Thresholds¶
- BAL fluid demonstration of organisms: Almost 100% sensitive and specific.
- H&E stain: Pathognomonic appearance (foamy alveolar filling, mononuclear infiltrate) even without specific organism identification.
- Silver/Giemsa/Immunofluorescent stains: Required for specific organism identification.
- Induced sputum: Variable sensitivity (55–90%) depending on patient characteristics and provider experience.
- Serum (1→3)-β-d-glucan: Frequently elevated but not perfectly sensitive or specific.
- Normal chest CT: Essentially rules out the diagnosis of PCP.
7. MANAGEMENT & TREATMENT¶
- The treatment of choice for PCP is trimethoprim-sulfamethoxazole (TMP-SMX), given either IV or PO.
- Duration: 14 days to non-HIV-infected patients with mild disease and for 21 days to all other patients.
- TMP-SMX interferes with the organism's folate metabolism.
- TMP-SMX is at least as effective as alternative agents and is better tolerated.
- TMP-SMX can cause leukopenia, hepatitis, rash, fever, elevation of potassium and creatinine, and anaphylactic and anaphylactoid reactions.
- Patients with HIV infection have an unusually high incidence of hypersensitivity to TMP-SMX.
- Monitoring of serum drug levels is useful if renal function or toxicities are issues in order to enhance the likelihood that therapy will be effective and toxicity will be avoided.
- Maintenance of a 2-h post-dose serum sulfamethoxazole level of 100–150 μg/mL has been associated with a successful outcome.
- Resistance to TMP-SMX cannot be measured by organism growth inhibition in the laboratory because human Pneumocystis cannot be successfully cultured.
- However, mutations in the target gene for sulfamethoxazole that confer in vitro sulfa resistance when found in other organisms have been recognized in Pneumocystis.
- The clinical relevance of these mutations for the response to therapy is uncertain.
- Sulfadiazine plus pyrimethamine, an oral regimen more often used for treatment of toxoplasmosis, also is highly effective.
- For PLWH who present with PCP before the initiation of ART, ART should be started within the first 2 weeks of therapy for PCP in most situations.
- Immune reconstitution inflammatory syndrome (IRIS) can occur, and the decision to initiate ART thus requires considerable clinical judgement that factors in the severity of pneumonia, the response of PCP to therapy, and concurrent medical conditions.
- Some authorities would switch from TMP-SMX to either IV pentamidine or IV clindamycin plus oral primaquine.
- Clindamycin-primaquine is certainly less toxic than IV pentamidine.
- Some authorities would add the second drug or drug combination to TMP-SMX rather than switching regimens.
- If patients are not already receiving them, glucocorticoids should be added to the regimen; the dosage and regimen are usually chosen empirically and depend on what glucocorticoid regimen (if any) the patient was receiving when PCP therapy was begun.
- Therapy with glucocorticoids should be the standard of care for patients with HIV infection and moderate to severe PCP.
- Therapy with glucocorticosteroids is also probably effective for patients with other immunodeficiencies who have moderate to severe PCP.
- This treatment should be started for moderate or severe disease when therapy for PCP is initiated, even if the diagnosis is suspected but has not yet been confirmed.
- If PLWH or HIV-uninfected patients are receiving high-dose glucocorticoids when they develop PCP, there are theoretical advantages to decreasing the steroid dose to improve immune function, but there is no convincing evidence on which to base any specific strategy.
- No definitive trials have identified the best therapeutic algorithm for patients in whom TMP-SMX treatment for PCP is failing.
- If no other treatable infectious or noninfectious processes are detected and pulmonary dysfunction appears to be due to PCP alone, many authorities would switch from TMP-SMX to either IV pentamidine or IV clindamycin plus oral primaquine.
- If patients are not already receiving them, glucocorticoids should be added to the regimen.
7.1 Pharmacologic Therapy¶
- First-Line Agent: TMP-SMX (Trimethoprim-Sulfamethoxazole).
- Dose: TMP (5 mg/kg) plus SMX (25 mg/kg) q6–8h PO or IV (i.e., 2 double-strength tablets tid or qid).
- Duration: 14 days (non-HIV mild) or 21 days (all other).
- Adverse Effects: Fever, rash, cytopenias, hepatitis, hyperkalemia.
- Alternative Agents:
- Atovaquone: 750 mg bid PO. Adverse Effects: Rash, fever, hepatitis.
- Clindamycin plus Primaquine: Clindamycin 300–450 mg q6h PO or 600 mg q6–8h IV; Primaquine 15–30 mg qd PO. Adverse Effects: Hemolysis (G6PD deficiency), methemoglobinemia, neutropenia, rash.
- Pentamidine: 3–4 mg/kg qd IV. Adverse Effects: Hypotension, azotemia, cardiac arrhythmias (torsades des pointes), pancreatitis, dysglycemias, hypocalcemia, neutropenia, hepatitis.
- Adjunctive Agent: Prednisone or methylprednisolone.
- Dose: 40 mg bid × 5 d, 40 mg qd × 5 d, 20 mg qd × 11 d; PO or IV.
- Adverse Effects: Peptic ulcer disease, hyperglycemia, mood alteration, hypertension.
7.2 Treatment Failure & Switching¶
- Some patients do not respond to therapy for 4–8 days.
- Supportive care for a minimum of 10 days is a reasonable consideration if such support is compatible with the patient's wishes and the prognosis of comorbidities.
- In fact, if patients of any level of severity are treated with specific therapy but without corticosteroids, they often deteriorate during the first few days, presumably due to enhanced inflammation induced by dying organisms.
- Patients whose condition continues to deteriorate after 3 or 4 days or have not improved after 7–10 days should be reevaluated to determine whether other infectious processes are present (either having been missed on initial evaluation or having developed during treatment), whether initial anti-Pneumocystis treatment has failed, or whether noninfectious processes (e.g., congestive heart failure, pulmonary emboli, pulmonary hypertension, drug toxicity, or a neoplastic process) are causing pulmonary dysfunction.
8. PROGNOSIS & COMPLICATIONS¶
- Untreated, PCP is invariably fatal.
- Factors that influence mortality risk of PCP include the patient's age and degree of immunosuppression as well as the presence of preexisting lung disease, the need for mechanical ventilation, and the development of a pneumothorax.
- With advances in supportive critical care, the prognosis for patients with PCP who require intubation and respiratory support has improved and now depends to a large extent on comorbidities and the prognosis of the underlying disease.
- Some patients do not respond to therapy for 4–8 days.
- Rare patients also develop distributive shock due to PCP.
- A few unusual patients present with extrapulmonary manifestations in the skin or soft tissue, retina, brain, liver, kidney, or spleen.
- Extrapulmonary disease is nonspecific in presentation and can be diagnosed only by histology.
8.1 Mortality Risk Factors¶
- Patient's age.
- Degree of immunosuppression.
- Presence of preexisting lung disease.
- Need for mechanical ventilation.
- Development of a pneumothorax.
9. SPECIAL CONSIDERATIONS¶
- For patients with HIV infection, CD4+ T-cell counts are a reliable marker of susceptibility, and counts 200/μL are not a reliable marker of protection from PCP.
- For these patients who are immunosuppressed due to causes other than HIV infection, the period of susceptibility is usually estimated on the basis of experience with the underlying disease and the specific immunosuppressive regimen.
- Cessation of prophylaxis has been associated with clusters of cases in certain patient populations, such as solid-organ transplant recipients, where the period of susceptibility is not well-defined.
- Patients receiving a prolonged course of high-dose glucocorticoids predispose patients to PCP.
- The most effective method for preventing PCP is to eliminate the cause of immunosuppression by withdrawing immunosuppressive therapy or treating the underlying cause (e.g., HIV infection).
- Patients who are susceptible to PCP benefit from chemoprophylaxis during the period of susceptibility.
- For patients who are immunosuppressed as a result of factors other than HIV infection, the period of susceptibility is usually estimated on the basis of experience with the underlying disease and the specific immunosuppressive regimen.
- Cessation of prophylaxis has been associated with clusters of cases in certain patient populations, such as solid-organ transplant recipients, where the period of susceptibility is not well-defined.
9.1 Prophylaxis¶
- First-Choice Agent: TMP-SMX.
- Dose: 1 tablet (double- or single-strength) qd PO.
- Comments: Incidence of hypersensitivity is high. Rechallenge for non-life-threatening hypersensitivity; consider dose-escalation protocol.
- Alternative Agents:
- Dapsone plus Pyrimethamine plus Leucovorin: Dapsone 50 mg bid or 100 mg qd PO; Pyrimethamine 50 mg weekly PO; Leucovorin 25 mg weekly PO. Comments: Leucovorin ameliorates cytopenias due to pyrimethamine. Hemolysis is associated with G6PD deficiency.
- Dapsone 200 mg weekly PO plus Pyrimethamine 75 mg weekly PO plus Leucovorin 25 mg weekly PO.
- Pentamidine: 300 mg monthly via Aerosol (Respirgard II nebulizer). Comments: Aerosol may cause bronchospasm. Pentamidine is probably less effective than TMP-SMX or dapsone regimens.
- Atovaquone: 1500 mg qd PO. Comments: Requires fatty meal for optimal absorption.
- Echinocandins: There is some evidence for activity of echinocandins against the cyst form (but not the trophozoite form) of Pneumocystis, but the role for echinocandins as part of combination therapy is currently uncertain, and these drugs should never be used as single drug therapy for PCP.
10. KEY PEARLS & CLINICAL TRAPS¶
- A normal chest CT essentially rules out the diagnosis of PCP.
- PCP can occur at CD4+ T-cell counts >200/μL in persons with HIV infection, but such occurrences are uncommon, especially with CD4+ T-cell counts substantially higher than 200/μL.
- CD4+ T-cell counts >200/μL in many populations does not imply protection in non-HIV immunosuppression.
- A normal LDH level does not rule out PCP, nor is an elevated LDH value specific for PCP.
- The demonstration of organisms in BAL fluid is almost 100% sensitive and specific for PCP.
- PCR tests for PCP are not standardized and specimen collection can vary considerably resulting in variable quality of the specimens assessed.
- Therefore, there is no specific PCR threshold that can be deemed to be especially convincing.
- Such PCR tests on appropriate samples may be more useful for ruling out a diagnosis of PCP if they are negative than for definitively attributing the disease to Pneumocystis if they are positive.
- Serum (1→3)-β-d-glucan levels are frequently elevated in patients with PCP, but serum or BAL (1→3)-β-d-glucan levels are not perfectly sensitive or highly specific for PCP.
- Therapy with glucocorticoids should be the standard of care for patients with HIV infection and moderate to severe PCP.
- Therapy with glucocorticosteroids is also probably effective for patients with other immunodeficiencies who have moderate to severe PCP.
- This treatment should be started for moderate or severe disease when therapy for PCP is initiated, even if the diagnosis is suspected but has not yet been confirmed.
- If PLWH or HIV-uninfected patients are receiving high-dose glucocorticoids when they develop PCP, there are theoretical advantages to decreasing the steroid dose to improve immune function, but there is no convincing evidence on which to base any specific strategy.
- Maintenance of a 2-h post-dose serum sulfamethoxazole level of 100–150 μg/mL has been associated with a successful outcome.
- Resistance to TMP-SMX cannot be measured by organism growth inhibition in the laboratory because human Pneumocystis cannot be successfully cultured.
- However, mutations in the target gene for sulfamethoxazole that confer in vitro sulfa resistance when found in other organisms have been recognized in Pneumocystis.
- The clinical relevance of these mutations for the response to therapy is uncertain.
- Untreated, PCP is invariably fatal.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
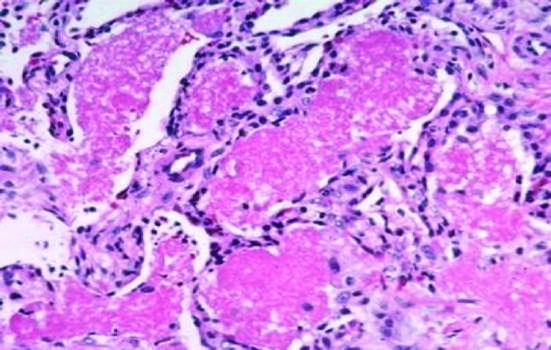
Caption: FIGURE 227-1 Direct microscopy of Pneumocystis pneumonia. A. Transbronchial lung B. Methenamine silver–stained bronchoalveolar lavage (BAL) fluid. C. Giemsa-stained — Figure 227-1A: Transbronchial lung biopsy stained with hematoxylin and eosin showing eosinophilic alveolar filling and mononuclear interstitial infiltrate.
Figure 2¶

Caption: FIGURE 227-1 Direct microscopy of Pneumocystis pneumonia. A. Transbronchial lung B. Methenamine silver–stained bronchoalveolar lavage (BAL) fluid. C. Giemsa-stained — Figure 227-1B: Methenamine silver–stained bronchoalveolar lavage (BAL) fluid demonstrating Pneumocystis organisms.
Figure 3¶

Caption: FIGURE 227-2 Radiographs in Pneumocystis pneumonia. A. Posterior–anterior chest radiograph showing symmetric alveolar infiltrates (courtesy of Alison Morris). C. ground-glass opacities. D. CT image showing symmetric interstitial infiltrates, — Figure 227-1C: Giemsa-stained BAL fluid showing Pneumocystis organisms.
Figure 4¶

Caption: FIGURE 227-2 Radiographs in Pneumocystis pneumonia. A. Posterior–anterior chest radiograph showing symmetric alveolar infiltrates (courtesy of Alison Morris). C. ground-glass opacities. D. CT image showing symmetric interstitial infiltrates, — Figure 227-1D: Immunofluorescent stain of BAL fluid highlighting Pneumocystis organisms.
Figure 5¶
Caption: FIGURE 227-1 Direct microscopy of Pneumocystis pneumonia. A. Transbronchial lung B. Methenamine silver–stained bronchoalveolar lavage (BAL) fluid. C. Giemsa-stained — Figure 227-2A: Posterior–anterior chest radiograph showing symmetric interstitial infiltrates typical of Pneumocystis pneumonia.
Figure 6¶

Caption: FIGURE 227-2 Radiographs in Pneumocystis pneumonia. A. Posterior–anterior chest radiograph showing symmetric alveolar infiltrates (courtesy of Alison Morris). C. ground-glass opacities. D. CT image showing symmetric interstitial infiltrates, — Figure 227-2B: Posterior–anterior chest radiograph showing symmetric alveolar infiltrates progressing from interstitial disease.
Figure 7¶

Caption: FIGURE 227-1 Direct microscopy of Pneumocystis pneumonia. A. Transbronchial lung B. Methenamine silver–stained bronchoalveolar lavage (BAL) fluid. C. Giemsa-stained — Figure 227-2C: Computed tomography (CT) image demonstrating symmetric interstitial infiltrates and ground-glass opacities.
Figure 8¶

Caption: FIGURE 227-2 Radiographs in Pneumocystis pneumonia. A. Posterior–anterior chest radiograph showing symmetric alveolar infiltrates (courtesy of Alison Morris). C. ground-glass opacities. D. CT image showing symmetric interstitial infiltrates, — Figure 227-2D: CT image showing symmetric interstitial infiltrates, ground-glass opacities, and pneumatoceles.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.