Botulism¶
Chapter 158 | Part 5: Infectious Diseases · Part 5 – Infectious Diseases: Bacterial
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Botulism is a rare, life-threatening disease characterized by cranial nerve palsies and symmetric descending flaccid paralysis.
- Four naturally occurring forms: foodborne, infant, wound, and adult intestinal colonization.
- Botulinum neurotoxins (BoNTs) cleave SNARE-family proteins (SNAP-25, VAMP, syntaxin), inhibiting acetylcholine release.
- Clinical presentation typically begins with ptosis (81%), followed by descending paralysis (93%) and respiratory compromise.
- Diagnosis relies on clinical suspicion; mouse bioassay is the gold standard, with PCR/Endopep-MS as alternatives.
- Equine botulinum antitoxin (BAT) treats non-infants; human-derived antitoxin (BabyBIG) treats infants.
- Antitoxin prevents progression of paralysis but does not reverse existing paralysis.
- Honey should never be fed to infants ≤1 year of age due to risk of infant botulism.
- Foodborne botulism is the third most common form in the US; wound botulism is the second most common.
- Recovery requires regeneration of nerve endings; paralysis can last weeks to months.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Forms of Botulism
- 1.2 Pathophysiology
- 2. EPIDEMIOLOGY
- 2.1 Outbreak Statistics
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Toxin Mechanism
- 3.2 Bacterial Characteristics
- 4. CLINICAL FEATURES
- 4.1 Clinical Manifestations
- 4.2 Symptom Frequencies
- 4.3 Respiratory Compromise
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 GBS vs. Botulism
- 5.2 Stroke vs. Botulism
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Algorithm
- 6.2 Laboratory Confirmation
- 7. MANAGEMENT & TREATMENT
- 7.1 Antitoxin Therapy
- 7.2 Supportive Care
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Recovery Timeline
- 9. SPECIAL CONSIDERATIONS
- 9.1 Prevention
- 9.2 Global Considerations
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Exclusion Criteria
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Figure / Illustration |
1. DEFINITION & OVERVIEW¶
Botulism is a rare, life-threatening disease characterized by cranial nerve palsies and symmetric descending flaccid paralysis. The paralysis of botulism lasts for weeks or months—the time required for regeneration of affected nerve endings and recovery of voluntary muscle function. There are no sensory deficits; patients are fully conscious, with normal intellectual function, although cranial nerve palsies may give a mistaken impression of altered consciousness.
1.1 Forms of Botulism¶
Four forms of naturally occurring botulism have been described: - Foodborne botulism: Caused by ingestion of foods contaminated with preformed toxin. - Infant botulism: Caused by colonization of the intestinal tract of infants ≤1 year of age. - Wound botulism: Caused by germination and growth of C. botulinum spores in a wound or necrotic tissue. - Adult intestinal colonization: Similar to infant botulism but affects persons >1 year of age. Other forms include: - Iatrogenic botulism: Occurs when a patient given injections of BoNT experiences signs of systemic botulism. - Inhalational botulism: BoNTs can be aerosolized and used as a bioweapon.
1.2 Pathophysiology¶
BoNTs are metalloproteases composed of a light chain and a heavy chain. The light chain has catalytic activity, and the heavy chain contains a translocation domain and a receptor-binding domain. The receptor-binding domain mediates neurospecific binding, leading to internalization within endocytic compartments. Interaction of the translocation domain with the membrane of endocytic vesicles leads to translocation of the light chain into the cytosol. Once in the cytosol, the light chain cleaves specific SNARE-family proteins. Serotypes A and E cleave SNAP-25; serotypes B, D, F, and G cleave VAMP; and serotype C cleaves SNAP-25 and syntaxin. Cleavage of any of these proteins disrupts the assembly of synaptic fusion complexes, inhibiting the fusion of the membrane of the synaptic vesicle containing acetylcholine with the neuronal cell membrane. Clinically, the result is flaccid paralysis of voluntary muscles. The irreversible binding of BoNTs to their targets has a clinical consequence: once toxin binding has occurred, the resulting paralysis persists for weeks or months, until nerve endings have been regenerated.
2. EPIDEMIOLOGY¶
Foodborne Botulism: - In the United States, foodborne botulism is the third most common form of botulism. - From 2001 to 2019, 362 foodborne botulism cases were reported, with a mean of 19 cases per year. - Most cases (64%) were caused by serotype A BoNT, followed by serotype E (26%). - Serotypes B and F caused 7% and 2% of cases, respectively. - Outbreaks caused by serotype E usually had a shorter incubation period; those caused by type A had higher numbers of patients who required mechanical ventilation; those caused by type B had lower numbers of deaths. - Foodborne botulism cases are usually sporadic, but small and large outbreaks can occur. - Most foodborne botulism cases in the United States are due to home-canned vegetables and pickled vegetables (e.g., beets, green beans, carrots, mushrooms, asparagus, peppers, beans, mustard greens, corn, tomato sauce, olives, pumpkin butter), vegetables baked in aluminum foil (e.g., potatoes, beets), home-canned meat-based foods (e.g., tuna, pickled pigs' feet, stew, pasta in meat sauce), oil-based foods (e.g., pasta and jarred pesto, homemade garlic-infused oil), herbal deer antler tea, home-prepared fermented tofu, commercial clam chowder, or commercial grain and vegetable products. - In Alaska, traditional Alaskan Native foods linked to foodborne botulism cases have included seal oil, seal blubber, dried herring in seal oil, fermented seal flipper, stinkheads and other fermented fish heads, stinkfish, salmon eggs, beaver tail, whitefish, fish eggs, fermented beluga, and whale blubber. - Commercial food manufacturing processes include retort canning, in which high temperature and pressure destroy the highly resistant clostridial spores, and manipulations that inhibit bacterial growth, such as acidification or addition of growth inhibitors. - Pruno, an illicit prison-brewed alcoholic beverage, has caused multiple outbreaks (California 2004, Utah 2011, Arizona 2012, Mississippi 2016).
Wound Botulism: - Between 2001 and 2019, 452 cases of wound botulism were reported, with an average of 24 cases per year. - Most cases (92%) were caused by BoNT serotype A and by serotype B (5%). - Most cases (96%) were among persons who injected drugs (mainly black tar heroin), and the remaining 4% of cases were due to traumatic injuries. - Wound botulism is now the second most common form of botulism in the United States.
Infant Botulism: - Infant botulism is the most common form of botulism in the United States. - Between 2001 and 2019, 2172 infant botulism cases were reported. - BoNT serotypes A and B caused most cases (40% and 58%, respectively). - Only 2 cases were due to serotype E. - A small fraction (<1%) of cases were caused by serotype F. - 22 infant botulism cases were due to strains of C. botulinum that can produce two BoNT serotypes (A and B or B and F).
Adult Intestinal Colonization: - Similar to infant botulism, adult intestinal colonization is caused by spores of BoNT-producing species of Clostridium colonizing the large intestine, growing, and producing BoNT in situ. - Although spores are routinely ingested and excreted by humans, the adult intestinal tract does not support spore germination and toxin production under normal circumstances. - Adult intestinal colonization is usually associated with inborn anatomic abnormalities, gastrointestinal surgery, or prolonged use of antibiotics. - Between 2001 and 2019, 51 cases were reported as being of 'unknown or other etiology.' - Most of these cases were caused by serotype A (63%) and serotype F (27%). - Many were thought to be cases of adult intestinal colonization, although confirmation is not always possible.
2.1 Outbreak Statistics¶
Total Foodborne Botulism Outbreaks of 10 or More Cases Reported in the United States Between 2001 and 2019: - 2001: Texas, Chili, 16 cases. - 2007: Multistate, Commercially canned hot dog chili sauce, 10 cases. - 2015: Ohio, Home-canned potatoes used to prepare a potato salad, served at a church potluck, 27 cases. - 2016: Mississippi, Pruno, illegal alcoholic beverage consumed by persons who were incarcerated at a federal facility, 19 cases. - 2017: California, Commercially produced nacho cheese, sold at a convenience store, 10 cases.
Table 1 — Table 158-1 Total Foodborne Botulism Outbreaks of 10 or More Cases Reported in the United States Between 2001 and 2019¶
| YEAR | STATE | FOOD SOURCE | NO. OF CONFIRMED CASES |
|---|---|---|---|
| 2001 | Texas | Chili | 16 |
| 2007 | Multistate | Commercially canned hot dog chili sauce | 10 |
| 2015 | Ohio | Home-canned potatoes used to prepare a potato salad, served at a church potluck | 27 |
| 2016 | Mississippi | Pruno, illegal alcoholic beverage consumed by persons who were incarcerated at a federal facility | 19 |
| 2017 | California | Commercially produced nacho cheese, sold at a convenience store | 10 |
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Botulism is caused by botulinum neurotoxins (BoNTs), which are produced by Clostridium botulinum. Rare strains of Clostridium butyricum and Clostridium baratii can also produce BoNTs. Seven distinct serotypes of BoNT (A through G) are well characterized; serotypes A, B, E, and F reportedly cause disease in humans. Novel serotypes—BoNT/FA (or H or HA), BoNT/En, and BoNT/X—have been proposed, but the scientific community has not yet reached a consensus as to whether each represents a new serotype or a combination of known serotypes, as in the case of BoNT/FA (or H or HA), or whether they represent true toxins or botulinum-like proteins, as in the case of BoNT/En and BoNT/X. BoNTs are encoded by the bont gene, which is also diverse in its DNA sequence. At least 40 unique subtypes of BoNT have been identified within serotypes A, B, E, and F. By definition, a variant of BoNT represents a new subtype when its amino acid form sequence differs by at least 2.6% from those of all known subtypes within that particular serotype. Although 2.6% is an arbitrary threshold, this figure has provided the basis for genetic subtype designations. BoNTs are produced by C. botulinum and a few strains of C. butyricum and C. baratii, which are all gram-positive, rod-shaped, spore-forming, anaerobic bacteria. Under most environmental conditions, C. botulinum exists as spores that are heat-resistant and ubiquitous in soil. In general, C. botulinum spores require temperatures above boiling to ensure destruction; their thermal resistance increases with higher pH and lower salt content. Spores present in foods can survive most preservation methods and, if the conditions allow it, can germinate and produce BoNTs in significant amounts to cause disease. Commercial retort canning reliably destroys botulinal spores. BoNTs are among the most toxic substances known. Extremely small amounts of BoNT can cause severe disease and death. Severity of disease varies with dose, serotype, and route of exposure. The lethal dose of BoNT in humans is not known but can be estimated by extrapolation of toxicity data from animal studies. The estimated lethal dose of BoNT acquired via the IV or IM route is 0.1–1 ng/kg of body weight. The human lethal dose of BoNT acquired by inhalation of aerosolized toxin is estimated at 1–75 ng/kg. The degree of toxicity of BoNT acquired by the oral route is estimated to be much lower: 0.1–1 μg/kg.
3.1 Toxin Mechanism¶
Despite their structural variability, BoNTs all have a similar mechanism of action: they target neurons and block neurotransmission by cleaving SNARE-family proteins in the host, with consequent inhibition of acetylcholine release. BoNTs are metalloproteases composed of a light chain and a heavy chain. The light chain has catalytic activity, and the heavy chain contains a translocation domain and a receptor-binding domain. The receptor-binding domain of the heavy chain mediates the neurospecific binding of BoNTs, which leads to its internalization within endocytic compartments. Interaction of the translocation domain of the heavy chain with the membrane of endocytic vesicles leads to the translocation of the light chain into the cytosol. Once in the cytosol, the light chain cleaves specific SNARE-family proteins. Serotypes A and E cleave SNAP-25; serotypes B, D, F, and G cleave VAMP; and serotype C cleaves SNAP-25 and syntaxin. Cleavage of any of these proteins disrupts the assembly of synaptic fusion complexes, and this disruption inhibits the fusion of the membrane of the synaptic vesicle containing acetylcholine with the neuronal cell membrane. Clinically, the result is flaccid paralysis of voluntary muscles. The irreversible binding of BoNTs to their targets has a clinical consequence: once toxin binding has occurred, the resulting paralysis persists for weeks or months, until nerve endings have been regenerated.
3.2 Bacterial Characteristics¶
C. botulinum type E is commonly found in aquatic environments and in aquatic animals. Because the spores are found in many foods, improper preparation or storage may produce the confluence of conditions that allow germination and growth of BoNT-producing species of Clostridium, which in turn result in production of BoNT. Both historically and at the present time, canned foods are of concern because they create anaerobic environments. To render these foods safe, proper processing procedures in conditions of enough heat and pressure to inactivate Clostridium spores, along with sufficient acidity, salinity, or other preservative methods to limit the organism's growth and its production of BoNT, are required. Low-acidity foods, such as corn, peppers, potatoes, and beets, represent a higher risk.
4. CLINICAL FEATURES¶
Botulism produces a syndrome characterized by bilateral cranial nerve palsies that may be followed by symmetric, descending flaccid paralysis that may cause respiratory arrest. There are no sensory deficits; patients are fully conscious, with normal intellectual function, although cranial nerve palsies may give a mistaken impression of altered consciousness. The paralysis of botulism lasts for weeks or months—the time required for regeneration of affected nerve endings and recovery of voluntary muscle function. The severity of disease varies greatly between patients and is probably governed by the dose of toxin to which they have been exposed. Without treatment, some patients do not progress beyond ptosis and mild palsy in one or two cranial nerves; others experience fulminant cranial nerve palsies and rapidly progressive descending flaccid paralysis eventually affecting most or all voluntary muscles as well as respiratory failure requiring intubation and mechanical ventilation within hours. The different BoNT serotypes are associated with variations in the botulism syndrome. BoNT type A is associated with more rapid disease progression, more frequent respiratory compromise and mechanical ventilation, and longer duration of paralysis. Type B is associated with a milder syndrome, with less severe and shorter-duration paralysis. Intoxication with the rarely occurring type F produces a syndrome of rapidly progressing paralysis that often leads to respiratory failure, with more rapid recovery than occurs with other toxin types. However, all toxin types causing human illness can cause severe disease; the clinical approach is the same for all. The paralysis of botulism can last for weeks or months—the time required for regeneration of affected nerve endings and recovery of voluntary muscle function. For severely affected patients with extensive paralysis, management consists of protracted intensive care, with detection and treatment of attendant risks not specific to botulism, such as ventilator-associated pneumonia, decubitus ulcers, and psychological trauma. More than 95% of noninfant botulism patients in the United States recover; hospital discharge is often followed by protracted rehabilitative care. The survival rate for infant botulism is near 100%.
4.1 Clinical Manifestations¶
In all botulism syndromes, the first neurologic manifestation usually is ptosis, which can be striking. Ocular findings of fuzzy vision or frank diplopia are caused by extraocular muscle paralysis due to palsies of cranial nerves III, IV, and VI. Flat, youthfully unlined, expressionless facies are produced by cranial nerve VII (facial nerve) palsy. Dysarthria is also a prominent manifestation. Oral and nasal regurgitation of foods or beverages is caused by cranial nerve IX (glossopharyngeal nerve) palsy. The autonomic system may be affected, producing anhidrosis manifesting as severe pharyngeal pain and erythema that has been mistaken for pharyngitis; paradoxically, other patients experience an inability to manage copious oral secretions. Autonomic dysfunction may produce hemodynamic instability requiring monitoring. Cranial nerve palsy may produce pharyngeal muscle flaccidity, causing airway collapse and respiratory arrest early in the course of illness, while reduction in diaphragmatic and accessory muscle function may cause respiratory compromise hours or days later. Cranial nerve palsies may be followed by descending symmetric flaccid paralysis of the muscles of the neck, shoulders, upper limbs, and lower limbs; proximal muscle groups of each limb are affected before distal muscle groups. Rarely, asymmetry of cranial nerve palsies or distal muscle paralysis is reported and, at least in some cases (especially those described in reports based on chart abstractions), may reflect an incomplete or incompletely recorded neurologic examination. Despite intact sensorium, symptoms such as ptosis, dysarthria, and gait instability may be mistaken for diminished consciousness and lack of coordination and may be erroneously attributed to intoxication from alcohol or other substances. Paresthesias have been reported in some patients; these sensations are not explained by the known activity of botulinum toxin. Paralysis of the diaphragm and accessory muscles of respiration may occur, producing respiratory compromise. Distal tendon reflexes diminish symmetrically. Constipation due to intestinal paralysis develops in almost all patients. Nausea and vomiting may occur in foodborne botulism, preceding neurologic symptoms. Whether these manifestations are due to BoNT, other products of BoNT-producing species of Clostridium, or other contaminants of spoiled food is unknown. These gastrointestinal symptoms have not been reported in wound botulism.
4.2 Symptom Frequencies¶
A recent analysis of 332 U.S. botulism cases found the following frequencies for patient-reported symptoms: - Difficulty swallowing: 86% - Fatigue: 85% - Blurred vision: 80% - Slurred speech: 78% - Double vision: 76% - Shortness of breath: 65% - Dry mouth: 62% The analysis also reported the following frequencies of observed signs: - Afebrile body temperature: 99% - Descending paralysis: 93% - Alert and oriented status: 93% - Ptosis: 81% - Limb weakness: 78% - Decreased palatal reflex: 54% - Facial palsy: 47% - Dilated pupils: 20% Sixty-six percent of patients were intubated and received mechanical ventilation.
4.3 Respiratory Compromise¶
Respiratory compromise occurs early in the course of disease in a substantial proportion of patients: the largest systematic literature review to date of foodborne and wound botulism cases (402 patients) reported that the average time from symptom onset to hospitalization was 2 days and that, at hospital admission, 42% of patients had respiratory symptoms; of these patients, 42% presented with no extremity weakness. In the same review, 87% of patients who required mechanical ventilation were intubated during the first 2 days of hospitalization. The combination of expressionless facies from cranial nerve paralysis and immobility from voluntary muscle paralysis may give patients with botulism a placid appearance that masks the agitation expected with respiratory distress.
5. DIFFERENTIAL DIAGNOSIS¶
Once a neurologic examination reveals the cranial nerve palsies of botulism and any additional bilateral flaccid paralysis, the differential diagnosis may include Guillain-Barré syndrome (GBS), myasthenia gravis, Lambert-Eaton syndrome, and tick paralysis. Less likely conditions include tetrodotoxin or shellfish poisoning, antimicrobial-associated paralysis, and rarer poisonings. A careful history and physical examination can further narrow the range of diagnoses. GBS is a rare (~1 case per 100,000 population per year in the United States) autoimmune demyelinating polyneuropathy that follows acute infection by Campylobacter jejuni, certain viruses, and other bacteria. In 95% of cases, GBS presents as an ascending paralysis. Recent reports from Peru indicate massive outbreaks of GBS of unknown cause, challenging the previously held notion that conditions causing flaccid paralysis other than botulism occur only as sporadic cases. The 5% of GBS cases presenting as the Miller Fisher variant are characterized by the triad of ophthalmoplegia, ataxia, and areflexia, which may resemble early descending paralysis. The CSF protein level is elevated in GBS, but the increase may take days after symptom onset; thus, normal CSF levels should be taken into account along with the duration of symptoms, and lumbar puncture may need to be repeated. Electromyography performed by an experienced operator may yield findings indicative of GBS and not botulism. Serological antibody tests or rapid nerve stimulation tests can confirm myasthenia gravis; borderline positive Tensilon tests have been reported in botulism patients. In most stroke patients, the physical examination should reveal asymmetric paralysis and upper motor neuron signs; brain imaging can help reveal rare basilar strokes that can produce symmetric bulbar palsies. The history and physical examination should rule out Lambert-Eaton syndrome, which is characterized by proximal limb weakness in patients with advanced cancer.
5.1 GBS vs. Botulism¶
In contrast to the findings in Guillain-Barré syndrome (GBS; see below), lumbar-puncture cerebrospinal fluid (CSF) values—and specifically the protein level—are usually normal in botulism. The CSF protein level may be very slightly elevated in a minority of botulism cases. The fact that botulism produces no abnormal findings on brain imaging may help rule out rare basilar strokes that produce nonlateralizing symptoms. Serological antibody tests and rapid nerve stimulation tests can rule out myasthenia gravis. Electromyography, when performed by an experienced practitioner, can provide support for the diagnosis. Botulism is indicated by findings consistent with neuromuscular junction blockage, normal axonal conduction, and potentiation with rapid repetitive stimulation in affected muscles.
5.2 Stroke vs. Botulism¶
In most stroke patients, the physical examination should reveal asymmetric paralysis and upper motor neuron signs; brain imaging can help reveal rare basilar strokes that can produce symmetric bulbar palsies. A possible cause of misdiagnosis is failure to perform a complete neurologic examination; indeed, review of some botulism patients' charts reveals documentation of the first neurologic examination, which suggested the correct diagnosis, days after hospital admission. As stated earlier, the combination of ptosis, dysarthria, and perceived gait instability from muscle paralysis in some cases may be misinterpreted as intoxication from alcohol or other substances. In other cases, rapidly progressing botulism may result in pharyngeal collapse and respiratory distress relatively early in the course, leading the clinical team to focus on airway management and primary respiratory diagnoses and thus delaying the neurologic evaluation.
6. INVESTIGATIONS & DIAGNOSIS¶
Rapid clinical diagnosis is essential. A diagnostic aid for botulism, 'Clinical Criteria to Trigger Suspicion of Botulism,' has been published by botulism consultants at the Centers for Disease Control and Prevention (CDC; accessible at academic.oup.com/cid/article/66/suppl_1/S38/4780423). The paralysis of botulism lasts for weeks or months, and administration of equine-source botulinum antitoxin (BAT)—the specific therapy to arrest the progression of paralysis—depends on the correct diagnosis. At this time, laboratory confirmation of botulism, which may require ≥24 h, must take place at a specialized public health laboratory. Therefore, effective, timely treatment relies on rapid clinical diagnosis of botulism in a patient with clinically compatible findings, without awaiting laboratory confirmation. A clinician suspecting noninfant botulism in a patient should immediately contact the state health department's emergency 24-h line. The state will connect the clinician with a botulism clinical consultant at the CDC (or, in Alaska, California, and Colorado, at the state health department), who will review the case with the clinician, assist in the shipping of appropriate specimens to a public health laboratory for definitive diagnosis, and, when indicated, arrange for immediate shipping of BAT from the federal stockpile at no charge. A clinician suspecting infant botulism in a patient should immediately contact the Infant Botulism Treatment and Prevention Program's on-call physician at (510)231-7600, who will provide consultation, assist with specimen collection, and, when indicated, assist with the provision of human-derived botulinum antitoxin (BabyBIG), a specific treatment licensed for treatment of infant botulism. The neurologic examination is the key to clinical diagnosis of botulism, as it readily uncovers the cranial nerve deficits that are invariably present in botulism and focuses the differential diagnosis. In principle, the distinct syndrome of bilateral cranial palsies and descending flaccid paralysis in a fully conscious patient should render the diagnosis and prompt treatment of botulism straightforward. The presentation of two or more patients with this syndrome is almost pathognomonic, since other illnesses considered during the differential diagnosis of botulism do not produce outbreaks. In practice, however, sporadic (lone) cases of botulism are misdiagnosed, and sometimes the diagnosis is missed even in the setting of an outbreak. In part, these failures may be due to the rarity of botulism and the clinician's unfamiliarity with its presentation. Standard clinical studies, including bloodwork and radiology, are not useful in diagnosing botulism. Laboratory testing confirms clinically diagnosed botulism cases and determines the BoNT serotype causing the disease. In addition, laboratory testing can confirm epidemiologic data by demonstrating presence of BoNT in the suspected food. Botulism cases are confirmed by the laboratory when BoNT is identified in serum or stool specimens or when a BoNT-producing species of Clostridium is isolated from stool specimens or wound cultures. Identification of preformed BoNT in food consumed by patients also confirms foodborne botulism. The gold standard for identification and serotyping of BoNT in clinical or food specimens is the mouse bioassay. The drawback is that this highly sensitive and specific method requires the use of animals. Specimens are injected IP into the mice with and without antitoxin; the mice are then observed for up to 96 h for signs of botulism. If the specimen contains BoNT at levels sufficient to affect the mice quickly, results may be available within 24 h of injection. Low levels of toxin may produce signs later, so mice should be monitored for 4 days after injection. Many in vitro methods have been developed for detection of BoNT and BoNT-producing species of Clostridium in clinical and food specimens. For instance, public health laboratories in the United States can use a real-time polymerase chain reaction test that detects bont genes encoding serotypes A through G. This test is a useful screening method to determine whether BoNT-producing species of Clostridium are present in cultures of clinical specimens, but positive results must be confirmed. Another in vitro method, the Endopep mass spectrometry (Endopep-MS) assay, is highly sensitive and specific and can detect BoNT in clinical specimens and foods. The advantage of Endopep-MS is that it detects active BoNT and therefore represents an ideal alternative to the mouse bioassay. Immune-based assays can provide rapid and sensitive results; their main limitation is that they detect antigens, which may not necessarily represent active BoNT. Cell-based in vitro assays are also a possible alternative to the mouse bioassay as they detect biologic activity of BoNT.
6.1 Diagnostic Algorithm¶
Step 1: Suspect botulism based on clinical criteria (Ptosis + Descending Paralysis + Conscious). Step 2: Contact state health department's emergency 24-h line immediately. Step 3: State connects clinician with botulism clinical consultant (CDC or state health department). Step 4: Consultant reviews case, assists in shipping appropriate specimens (Serum/Stool/Wound) to public health laboratory. Step 5: Laboratory confirms diagnosis via Mouse Bioassay (Gold Standard), PCR, or Endopep-MS. Step 6: If indicated, arrange for immediate shipping of BAT (non-infant) or BabyBIG (infant) from federal stockpile at no charge. Step 7: Administer antitoxin immediately upon suspicion, without awaiting lab confirmation if clinical suspicion is high.
6.2 Laboratory Confirmation¶
Laboratory testing confirms clinically diagnosed botulism cases and determines the BoNT serotype causing the disease. In addition, laboratory testing can confirm epidemiologic data by demonstrating presence of BoNT in the suspected food. Botulism cases are confirmed by the laboratory when BoNT is identified in serum or stool specimens or when a BoNT-producing species of Clostridium is isolated from stool specimens or wound cultures. Identification of preformed BoNT in food consumed by patients also confirms foodborne botulism. The gold standard for identification and serotyping of BoNT in clinical or food specimens is the mouse bioassay. The drawback is that this highly sensitive and specific method requires the use of animals. Specimens are injected IP into the mice with and without antitoxin; the mice are then observed for up to 96 h for signs of botulism. If the specimen contains BoNT at levels sufficient to affect the mice quickly, results may be available within 24 h of injection. Low levels of toxin may produce signs later, so mice should be monitored for 4 days after injection. Many in vitro methods have been developed for detection of BoNT and BoNT-producing species of Clostridium in clinical and food specimens. For instance, public health laboratories in the United States can use a real-time polymerase chain reaction test that detects bont genes encoding serotypes A through G. This test is a useful screening method to determine whether BoNT-producing species of Clostridium are present in cultures of clinical specimens, but positive results must be confirmed. Another in vitro method, the Endopep mass spectrometry (Endopep-MS) assay, is highly sensitive and specific and can detect BoNT in clinical specimens and foods. The advantage of Endopep-MS is that it detects active BoNT and therefore represents an ideal alternative to the mouse bioassay. Immune-based assays can provide rapid and sensitive results; their main limitation is that they detect antigens, which may not necessarily represent active BoNT. Cell-based in vitro assays are also a possible alternative to the mouse bioassay as they detect biologic activity of BoNT.
7. MANAGEMENT & TREATMENT¶
Treatment for botulism consists of two components: meticulous monitoring and supportive care, including admittance to the intensive care unit when indicated, and administration of botulinum antitoxin, the only specific therapy for botulism, as quickly as possible. Paralysis from botulism can be rapidly progressive. Vital capacity, and often hemodynamic parameters, should be frequently monitored and mechanical ventilation instituted immediately if needed. Paralysis induced by BoNT lasts weeks or months, and patients with extensive paralysis require painstaking care to avoid complications associated with protracted immobilization, including respirator-dependent pneumonia, decubitus ulcers, and psychological trauma. Patients who have recovered from severe botulism report that their appearance and immobility often led caregivers to assume they were unconscious; as a consequence, patients were sometimes subjected to painful procedures without warning and to insensitive comments. Signage should remind all caregivers that botulism patients are conscious but 'locked in.' Psychological support should be instituted for intubated botulism patients from the outset. With proper supportive care, >95% of botulism patients in the United States recover, even without antitoxin therapy; however, the antitoxin, if promptly administered, can substantially reduce the extent and duration of illness (see below). Botulinum antitoxin is the only specific treatment for botulism. The antitoxin prevents the progression of paralysis but does not reverse existing paralysis. If given early enough in the course of disease, it may avert respiratory compromise, obviate mechanical intubation, and forestall protracted paralysis and hospitalization along with associated complications. Accordingly, it is essential to administer antitoxin as soon as possible. A recent systematic literature review and meta-analysis covering nearly a century of the published literature in noninfant botulism patients confirmed long-known findings from smaller studies by showing significantly reduced mortality rates among patients treated with equine antitoxin, especially when treatment was administered within 48 h of symptom onset. Another large systematic literature review of pediatric noninfant botulism recently showed significantly reduced mortality risk among children treated with equine antitoxin. Published studies have demonstrated a substantial reduction in the duration and severity of illness among patients with infant botulism who are treated with human-derived botulinum antitoxin. There is no prophylactic treatment for botulism. Persons who may have been exposed to botulinum toxin should be evaluated by a physician and carefully observed for the development of symptoms of botulism. If symptoms appear, the patient should be treated immediately with botulinum antitoxin.
7.1 Antitoxin Therapy¶
The equine botulinum antitoxin used to treat noninfant botulism consists of antibodies produced in horses immunized with botulinum toxoids (inactivated toxins) and toxins. The antibodies are type-specific (anti-A neutralizes BoNT type A and so forth). The currently licensed antitoxin product in the United States, heptavalent botulinum antitoxin (BAT), contains antibodies to BoNT types A, B, C, D, E, F, and G. These equine antibodies have undergone despeciation to reduce antigenicity and the risk of anaphylaxis to foreign protein. A recent systematic literature review, along with studies of BAT use, indicated that <2% of recipients experience serious adverse reactions. Administration of one vial of BAT elicits circulating antitoxin concentrations sufficient to neutralize toxin levels one to two orders of magnitude higher than those found in the serum of most botulism patients. As noted earlier, clinicians suspecting botulism in a patient should immediately call their state health department's emergency contact to be put in touch with a botulism clinical consultant who will review the case and assist in its management, including shipment of BAT from the federal stockpile at no charge. The botulinum antitoxin used to treat infants, BabyBIG, consists of human antibodies obtained from hyperimmunized volunteers. The product is licensed for treatment of infant botulism due to BoNT types A and B and, as noted earlier, can be obtained through the Infant Botulism Treatment and Prevention Program.
7.2 Supportive Care¶
Treatment for botulism consists of two components: meticulous monitoring and supportive care, including admittance to the intensive care unit when indicated, and administration of botulinum antitoxin, the only specific therapy for botulism, as quickly as possible. Paralysis from botulism can be rapidly progressive. Vital capacity, and often hemodynamic parameters, should be frequently monitored and mechanical ventilation instituted immediately if needed. Paralysis induced by BoNT lasts weeks or months, and patients with extensive paralysis require painstaking care to avoid complications associated with protracted immobilization, including respirator-dependent pneumonia, decubitus ulcers, and psychological trauma. Patients who have recovered from severe botulism report that their appearance and immobility often led caregivers to assume they were unconscious; as a consequence, patients were sometimes subjected to painful procedures without warning and to insensitive comments. Signage should remind all caregivers that botulism patients are conscious but 'locked in.' Psychological support should be instituted for intubated botulism patients from the outset. With proper supportive care, >95% of botulism patients in the United States recover, even without antitoxin therapy; however, the antitoxin, if promptly administered, can substantially reduce the extent and duration of illness (see below).
8. PROGNOSIS & COMPLICATIONS¶
The paralysis of botulism lasts for weeks or months—the time required for regeneration of affected nerve endings and recovery of voluntary muscle function. For severely affected patients with extensive paralysis, management consists of protracted intensive care, with detection and treatment of attendant risks not specific to botulism, such as ventilator-associated pneumonia, decubitus ulcers, and psychological trauma. More than 95% of noninfant botulism patients in the United States recover; hospital discharge is often followed by protracted rehabilitative care. The survival rate for infant botulism is near 100%. Death in untreated patients during the first hours to days of illness is caused by airway obstruction resulting from pharyngeal muscle paralysis and inadequate tidal volume resulting from paralysis of diaphragmatic and accessory respiratory muscles. The combination of expressionless facies from cranial nerve paralysis and immobility from voluntary muscle paralysis may give patients with botulism a placid appearance that masks the agitation expected with respiratory distress. Respiratory compromise occurs early in the course of disease in a substantial proportion of patients: the largest systematic literature review to date of foodborne and wound botulism cases (402 patients) reported that the average time from symptom onset to hospitalization was 2 days and that, at hospital admission, 42% of patients had respiratory symptoms; of these patients, 42% presented with no extremity weakness. In the same review, 87% of patients who required mechanical ventilation were intubated during the first 2 days of hospitalization. The severity of disease varies greatly between patients and is probably governed by the dose of toxin to which they have been exposed. Without treatment, some patients do not progress beyond ptosis and mild palsy in one or two cranial nerves; others experience fulminant cranial nerve palsies and rapidly progressive descending flaccid paralysis eventually affecting most or all voluntary muscles as well as respiratory failure requiring intubation and mechanical ventilation within hours.
8.1 Recovery Timeline¶
The paralysis of botulism lasts for weeks or months—the time required for regeneration of affected nerve endings and recovery of voluntary muscle function. For severely affected patients with extensive paralysis, management consists of protracted intensive care, with detection and treatment of attendant risks not specific to botulism, such as ventilator-associated pneumonia, decubitus ulcers, and psychological trauma. More than 95% of noninfant botulism patients in the United States recover; hospital discharge is often followed by protracted rehabilitative care. The survival rate for infant botulism is near 100%.
9. SPECIAL CONSIDERATIONS¶
Botulism of Other Etiologies: Between 2001 and 2019, 51 cases were reported as being of 'unknown or other etiology.' This category includes laboratory-confirmed botulism cases that do not meet the definition of foodborne, infant, or wound botulism. Most of these cases were caused by serotype A (63%) and serotype F (27%). Many were thought to be cases of adult intestinal colonization, although confirmation of this form of botulism is not always possible. Most foodborne botulism cases in the United States are due to a wide variety of home-canned vegetables and pickled vegetables (e.g., beets, green beans, carrots, mushrooms, asparagus, peppers, beans, mustard greens, corn, tomato sauce, olives, pumpkin butter), vegetables baked in aluminum foil (e.g., potatoes, beets), home-canned meat-based foods (e.g., tuna, pickled pigs' feet, stew, pasta in meat sauce), oil-based foods (e.g., pasta and jarred pesto, homemade garlic-infused oil), herbal deer antler tea, home-prepared fermented tofu, commercial clam chowder, or commercial grain and vegetable products. In Alaska, traditional Alaskan Native foods linked to foodborne botulism cases have included seal oil, seal blubber, dried herring in seal oil, fermented seal flipper, stinkheads and other fermented fish heads, stinkfish, salmon eggs, beaver tail, whitefish, fish eggs, fermented beluga, and whale blubber. Commercial food manufacturing processes include retort canning, in which high temperature and pressure destroy the highly resistant clostridial spores, and manipulations that inhibit bacterial growth, such as acidification or addition of growth inhibitors that prevent germination and growth of BoNT-producing species of Clostridium and the production of BoNT. However, commercial foods occasionally still cause botulism if safe manufacturing processes are not followed or fail or if foods are stored or used inappropriately by the retailer or consumer. For instance, an outbreak of 10 cases associated with commercially canned hot dog chili sauce occurred in 2007 as a result of deficiencies in the canning process. Other commercial food-associated outbreaks that occurred in the United States between 2001 and 2019 include a 2001 outbreak of 16 cases linked to chili that was stored at inappropriate temperatures and later served at a church event in Texas and a 2006 outbreak linked to commercial carrot juice, which included four cases in the United States and two cases in Canada. The investigation of the latter outbreak led to an international product recall. The juice, which had no added sugar, salt, or preservatives, was stored at inappropriate temperatures. Pruno, an illicit prison-brewed alcoholic beverage, first caused a botulism outbreak in a California prison in 2004, affecting 4 prisoners. In 2011, a second outbreak due to pruno was reported and involved 8 patients at a prison in Utah. In 2012, 2 outbreaks associated with pruno occurred in a single prison in Arizona, with 4 and 8 cases, respectively. The largest outbreak from pruno occurred in 2016 in a Mississippi prison; 31 cases were identified, including 19 confirmed and 12 suspected. Wound botulism was once rare in the United States, but its frequency has been increasing for decades, and it is now the second most common form of botulism. Between 2001 and 2019, 452 cases of wound botulism were reported, with an average of 24 cases per year. Most cases (92%) were caused by BoNT serotype A and by serotype B (5%). Most cases (96%) were among persons who injected drugs (mainly black tar heroin), and the remaining 4% of cases were due to traumatic injuries. Infant botulism is the most common form of botulism in the United States. Between 2001 and 2019, 2172 infant botulism cases were reported. BoNT serotypes A and B caused most cases (40% and 58%, respectively). Only 2 cases were due to serotype E. Of these 2 cases, 1 was due to C. botulinum type E and the other to C. butyricum type E; both cases represented the first report anywhere in this country of infant botulism due to those respective organisms. A small fraction (<1%) of cases were caused by serotype F. Of note, 22 infant botulism cases were due to strains of C. botulinum that can produce two BoNT serotypes (A and B or B and F).
9.1 Prevention¶
No vaccine is licensed for the prevention of botulism. In the United States, a botulinum toxoid vaccine was available through the CDC until 2011, but it was discontinued because of a decline in immunogenicity of some serotypes and an increase in occurrence of moderate local reactions. Several vaccine candidates are currently in clinical trials. Because most foodborne botulism cases are caused by home-canned or home-preserved foods, the prevention of foodborne botulism depends mainly on proper preparation and preservation that ensures the destruction of spores of BoNT-producing species of Clostridium that may be present in the food or on the creation of an environment that will not allow the germination and growth of these spores, such as low pH or low water activity. Water activity is a measure of how much water is free, unbound, and thus available to microorganisms to use for growth. If foods have low water activity, it means they do not have much free water, and growth of C. botulinum will be limited or inhibited. Using pressure canners and properly cleaning items employed in the canning process can reduce the risk of foodborne botulism. Among other resources, the USDA Complete Guide to Home Canning provides a detailed description of safe home-canning practices. Other ways of preventing foodborne botulism include refrigerating homemade oils infused with garlic or herbs and discarding any of these oils that have not been used after 4 days; maintaining baked potatoes or similar foods wrapped in aluminum foil at temperatures above 140°F until served and then refrigerating leftovers; refrigerating canned or pickled foods after opening; and boiling home-canned foods before eating, especially those foods that are low in acid. Wound botulism largely affects people who inject drugs, especially black tar heroin. Using safe injection practices may help prevent wound botulism and many other infections, such as HIV and hepatitis C virus infections. Thus, educating injection drug users on the prevention of wound botulism and other infections is vital in protecting their health. As wound botulism can also follow traumatic injuries, keeping wounds clean is key. The risk factors for infant botulism are not fully understood, but possible sources of spores of BoNT-producing species of Clostridium include foods and dust. In most cases of infant botulism, no source of spores is identified. Honey is the only food that has been identified as an epidemiologically associated reservoir of spores of BoNT-producing species of Clostridium. Honey should not be fed to infants ≤1 year of age.
9.2 Global Considerations¶
Botulism has been reported from all parts of the world. The European Centre for Disease Prevention and Control has reported an average of 110 botulism cases each year from 2007 to 2018. During that period, the majority of cases were foodborne. The most common serotypes were A and B. Wound botulism was also reported, particularly in association with injection drug use. Infant botulism was reported in several countries, with honey identified as a risk factor in some cases. The incidence of botulism varies by region and is influenced by local food preservation practices and environmental factors.
10. KEY PEARLS & CLINICAL TRAPS¶
The presentation of two or more patients with this syndrome is almost pathognomonic, since other illnesses considered during the differential diagnosis of botulism do not produce outbreaks. In practice, however, sporadic (lone) cases of botulism are misdiagnosed, and sometimes the diagnosis is missed even in the setting of an outbreak. In part, these failures may be due to the rarity of botulism and the clinician's unfamiliarity with its presentation. A possible cause of misdiagnosis is failure to perform a complete neurologic examination; indeed, review of some botulism patients' charts reveals documentation of the first neurologic examination, which suggested the correct diagnosis, days after hospital admission. As stated earlier, the combination of ptosis, dysarthria, and perceived gait instability from muscle paralysis in some cases may be misinterpreted as intoxication from alcohol or other substances. In other cases, rapidly progressing botulism may result in pharyngeal collapse and respiratory distress relatively early in the course, leading the clinical team to focus on airway management and primary respiratory diagnoses and thus delaying the neurologic evaluation. Standard clinical studies, including bloodwork and radiology, are not useful in diagnosing botulism. Laboratory testing confirms clinically diagnosed botulism cases and determines the BoNT serotype causing the disease. In addition, laboratory testing can confirm epidemiologic data by demonstrating presence of BoNT in the suspected food. Botulism cases are confirmed by the laboratory when BoNT is identified in serum or stool specimens or when a BoNT-producing species of Clostridium is isolated from stool specimens or wound cultures. Identification of preformed BoNT in food consumed by patients also confirms foodborne botulism. The gold standard for identification and serotyping of BoNT in clinical or food specimens is the mouse bioassay. The drawback is that this highly sensitive and specific method requires the use of animals. Specimens are injected IP into the mice with and without antitoxin; the mice are then observed for up to 96 h for signs of botulism. If the specimen contains BoNT at levels sufficient to affect the mice quickly, results may be available within 24 h of injection. Low levels of toxin may produce signs later, so mice should be monitored for 4 days after injection. Many in vitro methods have been developed for detection of BoNT and BoNT-producing species of Clostridium in clinical and food specimens. For instance, public health laboratories in the United States can use a real-time polymerase chain reaction test that detects bont genes encoding serotypes A through G. This test is a useful screening method to determine whether BoNT-producing species of Clostridium are present in cultures of clinical specimens, but positive results must be confirmed. Another in vitro method, the Endopep mass spectrometry (Endopep-MS) assay, is highly sensitive and specific and can detect BoNT in clinical specimens and foods. The advantage of Endopep-MS is that it detects active BoNT and therefore represents an ideal alternative to the mouse bioassay. Immune-based assays can provide rapid and sensitive results; their main limitation is that they detect antigens, which may not necessarily represent active BoNT. Cell-based in vitro assays are also a possible alternative to the mouse bioassay as they detect biologic activity of BoNT. There is no prophylactic treatment for botulism. Persons who may have been exposed to botulinum toxin should be evaluated by a physician and carefully observed for the development of symptoms of botulism. If symptoms appear, the patient should be treated immediately with botulinum antitoxin. Treatment for botulism consists of two components: meticulous monitoring and supportive care, including admittance to the intensive care unit when indicated, and administration of botulinum antitoxin, the only specific therapy for botulism, as quickly as possible. Paralysis from botulism can be rapidly progressive. Vital capacity, and often hemodynamic parameters, should be frequently monitored and mechanical ventilation instituted immediately if needed. Paralysis induced by BoNT lasts weeks or months, and patients with extensive paralysis require painstaking care to avoid complications associated with protracted immobilization, including respirator-dependent pneumonia, decubitus ulcers, and psychological trauma. Patients who have recovered from severe botulism report that their appearance and immobility often led caregivers to assume they were unconscious; as a consequence, patients were sometimes subjected to painful procedures without warning and to insensitive comments. Signage should remind all caregivers that botulism patients are conscious but 'locked in.' Psychological support should be instituted for intubated botulism patients from the outset. With proper supportive care, >95% of botulism patients in the United States recover, even without antitoxin therapy; however, the antitoxin, if promptly administered, can substantially reduce the extent and duration of illness (see below). Botulinum antitoxin is the only specific treatment for botulism. The antitoxin prevents the progression of paralysis but does not reverse existing paralysis. If given early enough in the course of disease, it may avert respiratory compromise, obviate mechanical intubation, and forestall protracted paralysis and hospitalization along with associated complications. Accordingly, it is essential to administer antitoxin as soon as possible. A recent systematic literature review and meta-analysis covering nearly a century of the published literature in noninfant botulism patients confirmed long-known findings from smaller studies by showing significantly reduced mortality rates among patients treated with equine antitoxin, especially when treatment was administered within 48 h of symptom onset. Another large systematic literature review of pediatric noninfant botulism recently showed significantly reduced mortality risk among children treated with equine antitoxin. Published studies have demonstrated a substantial reduction in the duration and severity of illness among patients with infant botulism who are treated with human-derived botulinum antitoxin. The equine botulinum antitoxin used to treat noninfant botulism consists of antibodies produced in horses immunized with botulinum toxoids (inactivated toxins) and toxins. The antibodies are type-specific (anti-A neutralizes BoNT type A and so forth). The currently licensed antitoxin product in the United States, heptavalent botulinum antitoxin (BAT), contains antibodies to BoNT types A, B, C, D, E, F, and G. These equine antibodies have undergone despeciation to reduce antigenicity and the risk of anaphylaxis to foreign protein. A recent systematic literature review, along with studies of BAT use, indicated that <2% of recipients experience serious adverse reactions. Administration of one vial of BAT elicits circulating antitoxin concentrations sufficient to neutralize toxin levels one to two orders of magnitude higher than those found in the serum of most botulism patients. As noted earlier, clinicians suspecting botulism in a patient should immediately call their state health department's emergency contact to be put in touch with a botulism clinical consultant who will review the case and assist in its management, including shipment of BAT from the federal stockpile at no charge. The botulinum antitoxin used to treat infants, BabyBIG, consists of human antibodies obtained from hyperimmunized volunteers. The product is licensed for treatment of infant botulism due to BoNT types A and B and, as noted earlier, can be obtained through the Infant Botulism Treatment and Prevention Program. No vaccine is licensed for the prevention of botulism. In the United States, a botulinum toxoid vaccine was available through the CDC until 2011, but it was discontinued because of a decline in immunogenicity of some serotypes and an increase in occurrence of moderate local reactions. Several vaccine candidates are currently in clinical trials. Because most foodborne botulism cases are caused by home-canned or home-preserved foods, the prevention of foodborne botulism depends mainly on proper preparation and preservation that ensures the destruction of spores of BoNT-producing species of Clostridium that may be present in the food or on the creation of an environment that will not allow the germination and growth of these spores, such as low pH or low water activity. Water activity is a measure of how much water is free, unbound, and thus available to microorganisms to use for growth. If foods have low water activity, it means they do not have much free water, and growth of C. botulinum will be limited or inhibited. Using pressure canners and properly cleaning items employed in the canning process can reduce the risk of foodborne botulism. Among other resources, the USDA Complete Guide to Home Canning provides a detailed description of safe home-canning practices. Other ways of preventing foodborne botulism include refrigerating homemade oils infused with garlic or herbs and discarding any of these oils that have not been used after 4 days; maintaining baked potatoes or similar foods wrapped in aluminum foil at temperatures above 140°F until served and then refrigerating leftovers; refrigerating canned or pickled foods after opening; and boiling home-canned foods before eating, especially those foods that are low in acid. Wound botulism largely affects people who inject drugs, especially black tar heroin. Using safe injection practices may help prevent wound botulism and many other infections, such as HIV and hepatitis C virus infections. Thus, educating injection drug users on the prevention of wound botulism and other infections is vital in protecting their health. As wound botulism can also follow traumatic injuries, keeping wounds clean is key. The risk factors for infant botulism are not fully understood, but possible sources of spores of BoNT-producing species of Clostridium include foods and dust. In most cases of infant botulism, no source of spores is identified. Honey is the only food that has been identified as an epidemiologically associated reservoir of spores of BoNT-producing species of Clostridium. Honey should not be fed to infants ≤1 year of age.
10.1 Diagnostic Clues¶
- The presentation of two or more patients with this syndrome is almost pathognomonic.
- In all botulism syndromes, the first neurologic manifestation usually is ptosis, which can be striking.
- The combination of ptosis, dysarthria, and perceived gait instability from muscle paralysis in some cases may be misinterpreted as intoxication from alcohol or other substances.
- Standard clinical studies, including bloodwork and radiology, are not useful in diagnosing botulism.
- The fact that botulism produces no abnormal findings on brain imaging may help rule out rare basilar strokes that produce nonlateralizing symptoms.
10.2 Exclusion Criteria¶
- Standard clinical studies, including bloodwork and radiology, are not useful in diagnosing botulism.
- In contrast to the findings in Guillain-Barré syndrome (GBS; see below), lumbar-puncture cerebrospinal fluid (CSF) values—and specifically the protein level—are usually normal in botulism.
- The CSF protein level may be very slightly elevated in a minority of botulism cases.
- The fact that botulism produces no abnormal findings on brain imaging may help rule out rare basilar strokes that produce nonlateralizing symptoms.
- Serological antibody tests and rapid nerve stimulation tests can rule out myasthenia gravis.
- In most stroke patients, the physical examination should reveal asymmetric paralysis and upper motor neuron signs; brain imaging can help reveal rare basilar strokes that can produce symmetric bulbar palsies.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
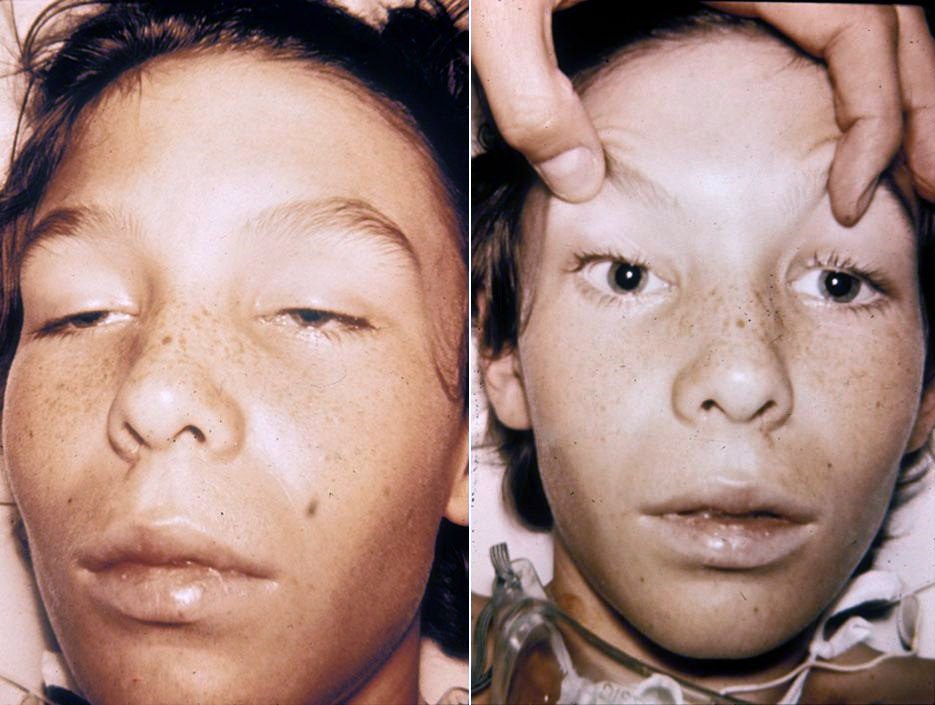
Caption: Clinical manifestations of botulism: The image likely depicts the characteristic descending flaccid paralysis and cranial nerve palsies (ptosis, diplopia, dysarthria) associated with botulism, illustrating the symmetric nature of the paralysis and the preserved consciousness of the patient.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.