Mitral Valve Prolapse¶
Chapter 276 | Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Mitral valve prolapse (MVP) is defined by systolic displacement of the mitral valve leaflet belly by at least 2 mm into the left atrium.
- The classic physical exam finding is a mid- or late systolic click followed by a crescendo-decrescendo murmur.
- MVP is more common in women (ages 15-30) and often benign; in older men (>50), MR is often more severe due to chordal rupture.
- Genetic loci associated with MVP include LMCD1, SPTBN1, LTBP2, TGFB2, NMB, and ALPK3.
- Sudden death is rare but occurs in patients with severe MR and depressed LV function or a flail leaflet.
- Transcatheter edge-to-edge repair (TEER) is approved for secondary MR and heart failure patients with reduced EF.
- Diagnostic maneuvers: Standing/Valsalva advances the click; squatting delays or eliminates it.
- ECG may show biphasic or inverted T waves in leads II, III, and aVF, or ventricular premature beats.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Synonyms & Classification
- 1.2 Pathology
- 2. EPIDEMIOLOGY
- 2.1 Age & Sex Distribution
- 2.2 Familial Patterns
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Genetic Factors
- 3.2 Associated Syndromes
- 4. CLINICAL FEATURES
- 4.1 Symptoms
- 4.2 Complications
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Chest Pain Mimics
- 5.2 Embolic Events
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Electrocardiography
- 6.2 Echocardiography
- 6.3 Exercise Testing
- 7. MANAGEMENT & TREATMENT
- 7.1 Medical Therapy
- 7.2 Transcatheter Repair (TEER)
- 7.3 Surgical Repair
- 7.4 Investigational Approaches
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Sudden Death Risk
- 8.2 Arrhythmia Risk
- 9. SPECIAL CONSIDERATIONS
- 9.1 Connective Tissue Disorders
- 9.2 Skeletal Deformities
- 9.3 Other Features
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Physical Exam Maneuvers
- 10.2 Murmur Radiation
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Barlow’s valve with classic mitral valve prolapse, as seen on transthoracic echocardiogram... |
| 2 | 🖼 Figure | Mitral valve prolapse |
| 3 | 🖼 Figure | Mitral valve prolapse |
| 4 | 🖼 Figure | Mitral valve prolapse |
| 5 | 🖼 Figure | Mitral valve prolapse |
1. DEFINITION & OVERVIEW¶
- Mitral valve prolapse (MVP), also variously termed the systolic click-murmur syndrome, Barlow’s syndrome, floppy-valve syndrome, or billowing mitral leaflet syndrome, is a relatively common but highly variable clinical syndrome resulting from diverse pathologic mechanisms affecting the mitral valve apparatus.
- Among these mechanisms are excessive or redundant mitral leaflet tissue, which is commonly associated with myxomatous degeneration and greatly increased concentrations of certain glycosaminoglycans.
- MVP is the most common abnormality leading to primary mitral regurgitation (MR) and mitral valve repair surgery.
- In most patients with MVP, the cause is unknown, but in some, it appears to be genetically determined.
- A reduction in the production of type III collagen has been implicated, and electron microscopy has revealed fragmentation of collagen fibrils.
- Prolapse can affect one or both leaflets, to varying degrees.
- The posterior mitral leaflet is usually more affected than the anterior, and the mitral valve annulus is often dilated.
- In many patients, elongated, redundant, or ruptured chordae tendineae cause or contribute to the regurgitation.
- MVP may also occur rarely as a sequel to acute rheumatic fever, in ischemic heart disease, and in various cardiomyopathies, as well as in 20% of patients with ostium secundum atrial septal defect.
- MVP may lead to excessive stress on the papillary muscles, leading to localized ischemia, infarction, and replacement fibrosis, which may be a nidus for ventricular arrhythmias.
- Rupture of chordae tendineae and progressive annular dilation and calcification contribute to valvular regurgitation, which then places more stress on the diseased mitral valve apparatus, thereby creating a vicious cycle.
- The role of the physical examination in the evaluation of patients with valvular heart disease is also considered in Chaps. 44 and 246; of electrocardiography (ECG) in Chap. 247; of echocardiography and other noninvasive imaging techniques in Chap. 241; and of cardiac catheterization and angiography in Chap. 249.
- The results of transthoracic and transesophageal echocardiographic imaging are critical to patient selection, along with an assessment of the adequacy of GDMT for heart failure.
- The use of TEER with a clip device in addition to medical therapy was shown to be superior to medical therapy alone in a trial involving symptomatic heart failure patients with reduced EF and at least moderately severe secondary MR followed through 5 years.
- Patients treated with the clip device had significantly lower rates of heart failure hospitalizations and all-cause mortality than those treated medically.
- This was the first randomized trial to show a survival benefit in patients with heart failure and secondary MR.
- Other transcatheter approaches to mitral valve repair have included the deployment of a device within the coronary sinus that can be adjusted to reduce mitral annular circumference leading to the effective orifice area of the valve much like a surgically implanted ring.
- Variations in the anatomic relationship of the coronary sinus to the mitral annulus and circumflex coronary artery have limited the applicability of this technique.
- Attempts to reduce the septal-lateral dimension of a dilated annulus using adjustable cords placed across the LV in a subvalvular location have been investigated.
- Construction of neochords to the mitral leaflets under TEE guidance using a system delivered via the cardiac apex has also been studied.
- Investigational experience with transcatheter mitral valve replacement systems remains in early clinical stages, although the field is evolving rapidly.
- Many high surgical risk patients are not candidates for transcatheter mitral valve repair, and thus, there is keen interest in refining this technology.
- Challenges with transseptal delivery and LV outflow tract obstruction from the devices used have prompted iterative changes in the systems utilized in early feasibility studies.
Table 1 — Table 276-1. Genetic Loci Associated with MVP¶
| Gene | Association |
|---|---|
| LMCD1 | MVP |
| SPTBN1 | MVP |
| LTBP2 | MVP |
| TGFB2 | MVP |
| NMB | MVP |
| ALPK3 | MVP |
| LMNA | Cardiomyopathy |
| FLNC | Cardiomyopathy |
| FLNA | Cardiomyopathy |
1.1 Synonyms & Classification¶
- Systolic click-murmur syndrome
- Barlow’s syndrome
- Floppy-valve syndrome
- Billowing mitral leaflet syndrome
1.2 Pathology¶
- Excessive or redundant mitral leaflet tissue
- Myxomatous degeneration
- Increased concentrations of certain glycosaminoglycans
- Fragmentation of collagen fibrils (reduction in type III collagen production)
- Elongated, redundant, or ruptured chordae tendineae
- Dilated mitral valve annulus
- Prolapse of one or both leaflets (posterior usually more affected than anterior)
2. EPIDEMIOLOGY¶
- MVP is a relatively common but highly variable clinical syndrome.
- MVP is more common in women than men.
- MVP occurs most frequently between the ages of 15 and 30 years.
- The clinical course is most often benign.
- MVP may also be observed in older (>50 years) patients, often men, in whom MR is often more severe because of chordal rupture and requires surgical treatment.
- There is an increased familial incidence for some patients, suggesting an autosomal dominant form of inheritance with incomplete penetrance.
- Myxomatous thickening and prolapse of the mitral valve can occur in isolation in 2–3% of the general population or may be associated with heritable connective tissue disorders, such as Marfan syndrome.
- MVP is a frequent finding in patients with heritable disorders of connective tissue, including Marfan syndrome, osteogenesis imperfecta, and Ehlers-Danlos syndrome.
- MVP may be associated with thoracic skeletal deformities similar to but not as severe as those in Marfan syndrome, such as a high-arched palate and alterations of the chest and thoracic spine, including kyphosis and the so-called straight back syndrome.
- Other associated features can include a history of inguinal hernias, joint dislocations, meniscal tears, and easy bruising.
2.1 Age & Sex Distribution¶
- Women > Men
- Peak incidence: 15-30 years
- Older patients (>50): Often men, more severe MR
2.2 Familial Patterns¶
- Increased familial incidence
- Autosomal dominant inheritance with incomplete penetrance
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- In most patients with MVP, the cause is unknown.
- In some, it appears to be genetically determined.
- A reduction in the production of type III collagen has been implicated.
- Electron microscopy has revealed fragmentation of collagen fibrils.
- Genome-wide association studies and 4884 MVP cases identified 14 genetic loci associated with MVP.
- Candidate genes included LMCD1, SPTBN1, LTBP2, TGFB2, NMB, and ALPK3.
- A polygenic risk score improved the performance of a clinical risk prediction model for patients with MR and/or leaflet thickening, although overall performance was modest.
- Other work has identified genetic associations with LMNA, FLNC, and FLNA, which are often expressed as cardiomyopathies.
- MVP is a frequent finding in patients with heritable disorders of connective tissue, including Marfan syndrome, osteogenesis imperfecta, and Ehlers-Danlos syndrome.
- MVP may occur rarely as a sequel to acute rheumatic fever, in ischemic heart disease, and in various cardiomyopathies, as well as in 20% of patients with ostium secundum atrial septal defect.
- Myxomatous degeneration of the valve predisposes to severe regurgitation and chordal rupture and is a frequent indication for mitral valve repair or replacement.
- MVP may lead to excessive stress on the papillary muscles, leading to localized ischemia, infarction, and replacement fibrosis.
- The latter, which may be a nidus for ventricular arrhythmias, may be visible on cardiac magnetic resonance imaging as late gadolinium enhancement and occurs in the absence of coronary artery disease.
- Rupture of chordae tendineae and progressive annular dilation and calcification contribute to valvular regurgitation, which then places more stress on the diseased mitral valve apparatus, thereby creating a vicious cycle.
3.1 Genetic Factors¶
- Unknown cause in most patients
- Genetically determined in some
- Reduced type III collagen production
- Fragmentation of collagen fibrils
3.2 Associated Syndromes¶
- Marfan syndrome
- Osteogenesis imperfecta
- Ehlers-Danlos syndrome
- Acute rheumatic fever (rare sequel)
- Ischemic heart disease (rare sequel)
- Cardiomyopathies
- Ostium secundum atrial septal defect (20% of cases)
4. CLINICAL FEATURES¶
- Most patients are asymptomatic and remain so for their entire lives.
- MVP is now the most common cause of isolated severe MR requiring surgical treatment in North America.
- Arrhythmias, most commonly ventricular premature contractions and paroxysmal supraventricular and ventricular tachycardia, as well as atrial fibrillation (AF), have been reported and may cause palpitations, light-headedness, and syncope.
- Sudden death is a very rare complication and occurs most often in patients with severe MR and depressed left ventricle (LV) systolic function, although it can occur in individuals with normal LV size and function.
- A small subset of MVP patients with high-grade ventricular ectopy has been identified with phenotypic features including electrocardiographic inferior-apical T-wave abnormalities, high-density premature ventricular complexes at rest, mitral annular disjunction (defined as abnormal atrial displacement of the mitral valve leaflet hinge point), and papillary muscle fibrosis on cardiac magnetic resonance imaging.
- In addition, there may be an excess risk of sudden death among patients with a flail leaflet.
- Most of these patients have severe MR.
- Many patients with MVP have chest pain that can be difficult to evaluate; it is often substernal, prolonged, and not related to exertion, and may rarely resemble angina pectoris.
- Transient cerebral ischemic attacks secondary to emboli from the mitral valve due to endothelial disruption have been reported.
- Infective endocarditis may occur in the development of MVP.
4.1 Symptoms¶
- Asymptomatic (most common)
- Palpitations (arrhythmias)
- Light-headedness
- Syncope
- Chest pain (substernal, prolonged, not related to exertion)
- Transient cerebral ischemic attacks (emboli)
- Angina-like pain (rare)
4.2 Complications¶
- Ventricular premature contractions
- Paroxysmal supraventricular tachycardia
- Ventricular tachycardia
- Atrial fibrillation
- Sudden death (rare)
- Infective endocarditis
5. DIFFERENTIAL DIAGNOSIS¶
- Chest pain in MVP may resemble angina pectoris.
- Transient cerebral ischemic attacks may be confused with other causes of embolic events.
- Infective endocarditis must be considered in patients with MVP and leaflet thickening.
- MVP may be associated with heritable connective tissue disorders (Marfan, Ehlers-Danlos, osteogenesis imperfecta).
- Differentiation from rheumatic valve disease: Chordae are focally thickened but are not fused as would be the case in rheumatic valve disease.
5.1 Chest Pain Mimics¶
- Angina pectoris
- MVP pain: Substernal, prolonged, not related to exertion
5.2 Embolic Events¶
- Transient cerebral ischemic attacks
- Mechanism: Emboli from mitral valve due to endothelial disruption
6. INVESTIGATIONS & DIAGNOSIS¶
- The ECG most commonly is normal but may show biphasic or inverted T waves in leads II, III, and aVF and, occasionally, ventricular or ventricular premature beats.
- Transthoracic echocardiography (TTE) is particularly effective in identifying the abnormal position and prolapse of the mitral valve leaflets.
- A useful echocardiographic definition of MVP is systolic displacement (in the parasternal long axis view) of the belly of the mitral valve leaflets by at least 2 mm into the left atrium (LA) superior to the plane of the mitral annulus.
- There can be prolapse of one or both leaflets.
- Color flow and continuous wave Doppler imaging is helpful to evaluate the associated MR and provide estimates of severity.
- The jet lesion of MR due to MVP is most often eccentric, and assessment of the effective regurgitant orifice area and regurgitant volume can be difficult with standard techniques.
- Both three-dimensional echocardiography and cardiac magnetic resonance imaging can provide more precise determinations of LV volumes.
- Transesophageal echocardiography (TEE) is indicated when more accurate anatomic information is required and is performed routinely for intraoperative guidance during surgical or transcatheter valve repair.
- Exercise testing can be performed when there is uncertainty regarding functional capacity.
- It is often combined with rest and immediate poststress TTE to assess LV and right ventricular (RV) function and the dynamic nature of MR and pulmonary artery pressures.
- Left ventriculography done at the time of cardiac catheterization can also be used.
Table 2 — Table 276-2. Echocardiographic Definition of MVP¶
| Criterion | Finding |
|---|---|
| View | Parasternal long axis view |
| Displacement | Systolic displacement of belly of mitral valve leaflets |
| Magnitude | At least 2 mm into left atrium (LA) |
| Location | Superior to the plane of the mitral annulus |
| Leaflets | Prolapse of one or both leaflets |
6.1 Electrocardiography¶
- Most commonly normal
- Biphasic or inverted T waves in leads II, III, and aVF
- Occasionally ventricular or ventricular premature beats
6.2 Echocardiography¶
- Transthoracic echocardiography (TTE): Primary modality
- Definition: Systolic displacement of belly of mitral valve leaflets by at least 2 mm into LA superior to plane of mitral annulus
- Color flow and continuous wave Doppler: Evaluate associated MR and severity
- Jet lesion: Most often eccentric
- Three-dimensional echocardiography: Precise LV volumes
- Cardiac magnetic resonance imaging: Precise LV volumes
- Transesophageal echocardiography (TEE): Intraoperative guidance, accurate anatomic information
6.3 Exercise Testing¶
- Indicated when uncertainty regarding functional capacity
- Combined with rest and immediate poststress TTE
- Assesses LV and RV function
- Assesses dynamic nature of MR and pulmonary artery pressures
7. MANAGEMENT & TREATMENT¶
- The results of transthoracic and transesophageal echocardiographic imaging are critical to patient selection, along with an assessment of the adequacy of GDMT for heart failure.
- The use of TEER with a clip device in addition to medical therapy was shown to be superior to medical therapy alone in a trial involving symptomatic heart failure patients with reduced EF and at least moderately severe secondary MR followed through 5 years.
- Patients treated with the clip device had significantly lower rates of heart failure hospitalizations and all-cause mortality than those treated medically.
- This was the first randomized trial to show a survival benefit in patients with heart failure and secondary MR.
- Other transcatheter approaches to mitral valve repair have included the deployment of a device within the coronary sinus that can be adjusted to reduce mitral annular circumference leading to the effective orifice area of the valve much like a surgically implanted ring.
- Variations in the anatomic relationship of the coronary sinus to the mitral annulus and circumflex coronary artery have limited the applicability of this technique.
- Attempts to reduce the septal-lateral dimension of a dilated annulus using adjustable cords placed across the LV in a subvalvular location have been investigated.
- Construction of neochords to the mitral leaflets under TEE guidance using a system delivered via the cardiac apex has also been studied.
- Investigational experience with transcatheter mitral valve replacement systems remains in early clinical stages, although the field is evolving rapidly.
- Many high surgical risk patients are not candidates for transcatheter mitral valve repair, and thus, there is keen interest in refining this technology.
- Challenges with transseptal delivery and LV outflow tract obstruction from the devices used have prompted iterative changes in the systems utilized in early feasibility studies.
- The TEER system is also approved for the treatment of heart failure patients with secondary MR.
7.1 Medical Therapy¶
- Adequacy of GDMT for heart failure assessed
- Medical therapy alone used in some trials
7.2 Transcatheter Repair (TEER)¶
- Clip device in addition to medical therapy
- Superior to medical therapy alone in symptomatic heart failure patients with reduced EF and at least moderately severe secondary MR
- Significantly lower rates of heart failure hospitalizations and all-cause mortality
- First randomized trial to show survival benefit in patients with heart failure and secondary MR
7.3 Surgical Repair¶
- Mitral valve repair surgery is a frequent indication for myxomatous degeneration
- High surgical risk patients may not be candidates for transcatheter mitral valve repair
7.4 Investigational Approaches¶
- Deployment of device within coronary sinus
- Adjustable cords placed across LV in subvalvular location
- Construction of neochords to mitral leaflets under TEE guidance
- Transcatheter mitral valve replacement systems (early clinical stages)
8. PROGNOSIS & COMPLICATIONS¶
- The clinical course is most often benign.
- Sudden death is a very rare complication and occurs most often in patients with severe MR and depressed left ventricle (LV) systolic function, although it can occur in individuals with normal LV size and function.
- A small subset of MVP patients with high-grade ventricular ectopy has been identified with phenotypic features including electrocardiographic inferior-apical T-wave abnormalities, high-density premature ventricular complexes at rest, mitral annular disjunction (defined as abnormal atrial displacement of the mitral valve leaflet hinge point), and papillary muscle fibrosis on cardiac magnetic resonance imaging.
- In addition, there may be an excess risk of sudden death among patients with a flail leaflet.
- Most of these patients have severe MR.
- In many patients, the condition progresses over years or decades; in others, it worsens rapidly as a result of chordal rupture or endocarditis.
- MVP may lead to excessive stress on the papillary muscles, leading to localized ischemia, infarction, and replacement fibrosis.
- The latter, which may be a nidus for ventricular arrhythmias, may be visible on cardiac magnetic resonance imaging as late gadolinium enhancement and occurs in the absence of coronary artery disease.
- Rupture of chordae tendineae and progressive annular dilation and calcification contribute to valvular regurgitation, which then places more stress on the diseased mitral valve apparatus, thereby creating a vicious cycle.
8.1 Sudden Death Risk¶
- Very rare complication
- Most often in patients with severe MR and depressed LV systolic function
- Can occur in individuals with normal LV size and function
- Excess risk in patients with a flail leaflet
- Most of these patients have severe MR
8.2 Arrhythmia Risk¶
- Ventricular premature contractions
- Paroxysmal supraventricular tachycardia
- Ventricular tachycardia
- Atrial fibrillation
- Nidus for ventricular arrhythmias (papillary muscle fibrosis)
9. SPECIAL CONSIDERATIONS¶
- MVP is a frequent finding in patients with heritable disorders of connective tissue, including Marfan syndrome, osteogenesis imperfecta, and Ehlers-Danlos syndrome.
- MVP may be associated with thoracic skeletal deformities similar to but not as severe as those in Marfan syndrome, such as a high-arched palate and alterations of the chest and thoracic spine, including kyphosis and the so-called straight back syndrome.
- Other associated features can include a history of inguinal hernias, joint dislocations, meniscal tears, and easy bruising.
- MVP may also be observed in older (>50 years) patients, often men, in whom MR is often more severe because of chordal rupture and requires surgical treatment.
9.1 Connective Tissue Disorders¶
- Marfan syndrome
- Osteogenesis imperfecta
- Ehlers-Danlos syndrome
9.2 Skeletal Deformities¶
- High-arched palate
- Alterations of chest and thoracic spine
- Kyphosis
- Straight back syndrome
9.3 Other Features¶
- Inguinal hernias
- Joint dislocations
- Meniscal tears
- Easy bruising
10. KEY PEARLS & CLINICAL TRAPS¶
- Auscultation: A frequent finding is the mid- or late (nonejection) systolic click, which occurs 0.14 s or more after S and is thought to be generated by the sudden tensing of slack, elongated chordae tendineae or by the prolapsing mitral leaflet when it reaches its maximal excursion.
- Systolic clicks may be multiple and may be followed by a high-pitched, mid-late systolic crescendo–decrescendo murmur, which occasionally is “whooping” or “honking” and is heard best at the apex.
- Radiation of the murmur will depend on the involved leaflet. With posterior leaflet prolapse, the jet of MR is directed anteriorly and the murmur will radiate to the base of the heart. With anterior leaflet involvement, the jet of MR is directed posteriorly and the murmur will radiate to the axilla and back.
- The click and murmur occur earlier with standing, during the strain phase of the Valsalva maneuver and with any intervention that decreases LV volume (preload), exaggerating the propensity of the leaflet to prolapse.
- Conversely, squatting and isometric exercises, which increase LV volume, diminish MVP; the click-murmur complex is delayed, moves away from S, and may even disappear.
- Some patients have a mid-systolic click without a murmur; others have a murmur without a click. Still others have both sounds at different times.
- ECG: The ECG most commonly is normal but may show biphasic or inverted T waves in leads II, III, and aVF and, occasionally, ventricular or ventricular premature beats.
10.1 Physical Exam Maneuvers¶
- Standing/Valsalva: Click and murmur occur earlier
- Decreased LV volume (preload): Exaggerates propensity of leaflet to prolapse
- Squatting/Isometric exercises: Diminish MVP
- Increased LV volume: Click-murmur complex delayed, moves away from S, may disappear
10.2 Murmur Radiation¶
- Posterior leaflet prolapse: Jet directed anteriorly, murmur radiates to base of heart
- Anterior leaflet involvement: Jet directed posteriorly, murmur radiates to axilla and back
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
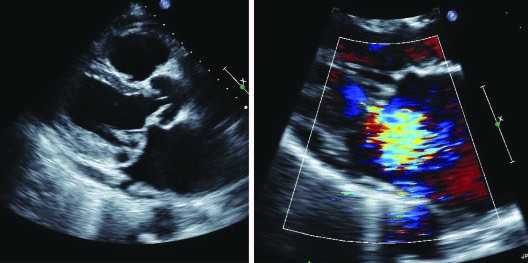
Caption: FIGURE 276-2 Barlow’s valve with classic mitral valve prolapse, as seen on transthoracic echocardiogram in parasternal long-axis windows. Left: parasternal long-axis window, showing both myxomatous leaflets (arrows) billowing into the left to atrium in late systole. Right: same window with color Doppler showing significant mitral regurgitation (arrow) in systole. (Courtesy of Justina Wu, MD, PhD.) — Figure 276-1A: Three-dimensional transesophageal echocardiogram showing a myxomatous mitral valve from the left atrial en face aspect. There is billowing and prolapse of the entire middle scallop of the posterior leaflet (asterisk).
Figure 2¶

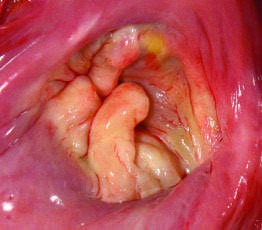
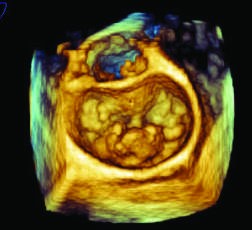
Caption: FIGURE 276-1 Mitral valve prolapse. Myxomatous thickening and prolapse of the mitral valve can occur in isolation in 2–3% of the general population or may be associated with heritable connective tissue disorders, such as Marfan syndrome. Myxomatous degeneration of the valve predisposes to severe regurgitation and chordal rupture and is a frequent indication for mitral valve repair or replacement. Prolapse can affect one or both leaflets, to varying degrees. A. Three-dimensional transesophageal echocardiogram showing a myxomatous mitral valve from the left atrial en face aspect. There is billowing and prolapse of the entire middle scallop of the posterior leaflet (asterisk). (Figure courtesy of Douglas C. Shook, MD, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital.) B. The posterior leaflet of the mitral valve demonstrates marked — Figure 276-1B: The posterior leaflet of the mitral valve demonstrates marked prolapse and hooding in all segments and severe redundancy in this postmortem photograph taken from the vantage point of the left atrium.
Figure 3¶
Caption: FIGURE 276-1 Mitral valve prolapse. Myxomatous thickening and prolapse of the mitral valve can occur in isolation in 2–3% of the general population or may be associated with heritable connective tissue disorders, such as Marfan syndrome. Myxomatous degeneration of the valve predisposes to severe regurgitation and chordal rupture and is a frequent indication for mitral valve repair or replacement. Prolapse can affect one or both leaflets, to varying degrees. A. Three-dimensional transesophageal echocardiogram showing a myxomatous mitral valve from the left atrial en face aspect. There is billowing and prolapse of the entire middle scallop of the posterior leaflet (asterisk). (Figure courtesy of Douglas C. Shook, MD, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital.) B. The posterior leaflet of the mitral valve demonstrates marked — Figure 276-1C: Opening the left heart reveals prominent mitral leaflet hooding (arrows). The chordae are focally thickened but are not fused as would be the case in rheumatic valve disease.
Figure 4¶
Caption: FIGURE 276-1 Mitral valve prolapse. Myxomatous thickening and prolapse of the mitral valve can occur in isolation in 2–3% of the general population or may be associated with heritable connective tissue disorders, such as Marfan syndrome. Myxomatous degeneration of the valve predisposes to severe regurgitation and chordal rupture and is a frequent indication for mitral valve repair or replacement. Prolapse can affect one or both leaflets, to varying degrees. A. Three-dimensional transesophageal echocardiogram showing a myxomatous mitral valve from the left atrial en face aspect. There is billowing and prolapse of the entire middle scallop of the posterior leaflet (asterisk). (Figure courtesy of Douglas C. Shook, MD, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital.) B. The posterior leaflet of the mitral valve demonstrates marked — Figure 276-2 Left: Parasternal long-axis window on transthoracic echocardiogram showing both myxomatous leaflets (arrows) billowing into the left atrium in late systole.
Figure 5¶
Caption: FIGURE 276-1 Mitral valve prolapse. Myxomatous thickening and prolapse of the mitral valve can occur in isolation in 2–3% of the general population or may be associated with heritable connective tissue disorders, such as Marfan syndrome. Myxomatous degeneration of the valve predisposes to severe regurgitation and chordal rupture and is a frequent indication for mitral valve repair or replacement. Prolapse can affect one or both leaflets, to varying degrees. A. Three-dimensional transesophageal echocardiogram showing a myxomatous mitral valve from the left atrial en face aspect. There is billowing and prolapse of the entire middle scallop of the posterior leaflet (asterisk). (Figure courtesy of Douglas C. Shook, MD, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital.) B. The posterior leaflet of the mitral valve demonstrates marked — Figure 276-2 Right: Same parasternal long-axis window with color Doppler showing significant mitral regurgitation (arrow) in systole.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.