Acute Intestinal Obstruction¶
Chapter 341 | Part 10: Disorders of the Gastrointestinal System · Part 10 – Gastrointestinal Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Cardinal signs of acute obstruction: colicky abdominal pain, abdominal distention, emesis, and obstipation.
- Closed-loop obstruction (e.g., volvulus, hernia) carries a much higher risk of strangulation and ischemia compared to simple obstruction.
- Computed tomography (CT) sensitivity for detecting high-grade bowel obstruction is ~95% with specificity of 96%.
- Barium studies are contraindicated in patients with suspected complete or high-grade obstruction due to risk of barium concretions and need for surgery.
- Cecal diameter exceeding 10–12 cm in distal colonic obstruction is associated with ischemic necrosis and perforation risk.
- Neostigmine is the primary pharmacologic treatment for Ogilvie's syndrome (colonic pseudo-obstruction) but requires cardiac monitoring and atropine availability.
- Postoperative adhesions account for >50% of small-bowel obstruction cases in the United States and Europe.
- Patients with ileus typically lack colicky pain and may pass flatus/stool, distinguishing them from complete mechanical obstruction.
- Mesenteric venous gas, pneumatosis intestinalis, and pneumoperitoneum on CT are late findings indicating bowel necrosis.
- Neostigmine is contraindicated in patients with mechanical obstruction; it must be used only after mechanical obstruction is excluded.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification of Obstruction
- 1.2 Epidemiology Overview
- 2. EPIDEMIOLOGY
- 2.1 Incidence and Trends
- 2.2 Demographics and Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Etiologic Categories
- 3.2 Pathophysiologic Cascade
- 3.3 Incidence by Cause
- 4. CLINICAL FEATURES
- 4.1 Physical Examination Findings
- 4.2 Differentiating Ileus vs Obstruction
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Ileus vs Mechanical Obstruction
- 5.2 Causes of Ileus (Functional or Pseudo-Obstruction)
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Laboratory Findings
- 6.2 Imaging Studies
- 7. MANAGEMENT & TREATMENT
- 7.1 Initial Stabilization
- 7.2 Surgical Intervention
- 7.3 Specific Conditions
- 7.4 Postoperative Bowel Obstruction
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Complication Rates
- 8.2 Mortality
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy
- 9.2 Barium Contraindications
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Clinical Traps
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Acute intestinal obstruction occurs either mechanically from blockage or from intestinal dysmotility when there is no blockage. In the latter instance, the abnormality is functional. Mechanical bowel obstruction may be caused by extrinsic processes, intrinsic abnormalities of the bowel wall, or intraluminal abnormalities. Obstruction is also commonly described as being either 'simple' or, alternatively, 'strangulated' if vascular insufficiency and intestinal ischemia are evident.
1.1 Classification of Obstruction¶
- Mechanical obstruction: Caused by blockage from extrinsic, intrinsic, or intraluminal disease.
- Functional obstruction: Also known as ileus or pseudo-obstruction; present when dysmotility prevents intestinal contents from being propelled distally and no mechanical blockage exists.
- Simple obstruction: No vascular insufficiency or ischemia.
- Strangulated obstruction: Vascular insufficiency and intestinal ischemia are evident.
1.2 Epidemiology Overview¶
- Acute intestinal obstruction accounts for ~1–3% of all hospitalizations.
- Approximately 80% of cases involve the small bowel.
- About one-third of these patients show evidence of significant ischemia.
- The therapeutic mortality rate for patients with strangulation who are operated on within 24–30 h of the onset of symptoms is ~8% but triples shortly thereafter.
- Globally, although the incidence and prevalence of acute intestinal obstruction have increased over the past two decades, morbidity and mortality appear to be decreasing.
2. EPIDEMIOLOGY¶
Acute intestinal obstruction accounts for ~1–3% of all hospitalizations and a quarter of all urgent or emergent general surgery admissions. Approximately 80% of cases involve the small bowel, and about one-third of these patients show evidence of significant ischemia. The therapeutic mortality rate for patients with strangulation who are operated on within 24–30 h of the onset of symptoms is ~8% but triples shortly thereafter.
2.1 Incidence and Trends¶
- Globally, although the incidence and prevalence of acute intestinal obstruction have increased over the past two decades, morbidity and mortality appear to be decreasing.
- Diagnosis remains challenging.
- The extent of mechanical obstruction is typically described as partial, high grade, or complete—generally correlating with the risk of complications and the urgency with which the underlying disease process must be addressed.
2.2 Demographics and Risk Factors¶
- Risk factors for colonic volvulus include institutionalization, the presence of neuropsychiatric conditions requiring psychotropic medication, chronic constipation, and aging.
- Patients with colonic volvulus typically present in their seventies or eighties.
- Colonic volvulus is more common in Eastern Europe, Russia, and Africa than it is the United States.
- It is rare for adhesions or hernias to obstruct the colon.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Mechanical bowel obstruction may be caused by extrinsic processes, intrinsic abnormalities of the bowel wall, or intraluminal abnormalities. Within each of these broad categories are many diseases that can impede intestinal propulsion. Intrinsic diseases that can cause intestinal obstruction are usually congenital, inflammatory, neoplastic, or traumatic in origin, although intussusception and radiation injury can also be etiologic. Functional obstruction, also known as ileus and pseudo-obstruction, is present when dysmotility prevents intestinal contents from being propelled distally and no mechanical blockage exists.
3.1 Etiologic Categories¶
- Extrinsic diseases most commonly cause mechanical obstruction of the small intestine.
- Intrinsic diseases are usually congenital, inflammatory, neoplastic, or traumatic.
- Intraluminal abnormalities include bezoars, feces, foreign bodies, gallstones, and enteroliths.
- Functional obstruction (ileus/pseudo-obstruction) involves dysmotility without blockage.
Table 1 — Table 341-1 Most Common Causes of Acute Intestinal Obstruction¶
| Category | Specific Causes |
|---|---|
| Extrinsic Disease | Adhesions (especially due to previous abdominal surgery), internal or external hernias, neoplasms (including carcinomatosis and extraintestinal malignancies, mostly commonly ovarian), endometriosis or intraperitoneal abscesses, and idiopathic sclerosis |
| Intrinsic Disease | Congenital (e.g., malrotation, atresia, stenosis, intestinal duplication, cyst formation, and congenital bands—the latter rarely in adults) Inflammation (e.g., inflammatory bowel disease, especially Crohn's disease, but also diverticulitis, radiation, tuberculosis, lymphogranuloma venereum, and schistosomiasis) Neoplasia (note: primary small-bowel cancer is rare; obstructive colon cancer may mimic small-bowel obstruction if the ileocecal valve is incompetent) Traumatic (e.g., hematoma formation, anastomotic strictures) Other, including intussusception (where the lead point is typically a polyp or tumor in adults), volvulus, obstruction of duodenum by superior mesenteric artery, radiation or ischemic injury, and aganglionosis, which is Hirschsprung's disease |
| Intraluminal Abnormalities | Bezoars, feces, foreign bodies including inspissated barium, gallstones (entering the lumen via a cholecystoenteric fistula), enteroliths |
3.2 Pathophysiologic Cascade¶
- Increased intestinal contractility occurs proximally and distal to the obstruction.
- Subsequently, intestinal peristalsis slows as the intestine or stomach proximal to the point of obstruction dilates and fills with gastrointestinal secretions and swallowed air.
- Intraluminal dilation also increases intraluminal pressure.
- When luminal pressure exceeds venous pressure, venous and lymphatic drainage is impeded.
- Edema ensues, and the bowel wall proximal to the site of blockage may become hypoxemic.
- Epithelial necrosis can be identified within 12 h of obstruction.
- Ultimately, arterial blood supply may become so compromised that full-thickness ischemia, necrosis, and perforation result.
- Stasis increases bacteria counts within the jejunum and ileum.
- Bacteria, such as Escherichia coli, Streptococcus faecalis, and Klebsiella, and other pathogens may be recovered from intestinal cultures, mesenteric lymph nodes, the bloodstream, and other sites.
- Inflammatory edema eventually increases the production of reactive oxygen species and activates neutrophils and macrophages, which accumulate within the bowel wall.
- Their accumulation, along with changes in innate immunity, disrupts secretory and neuromotor processes.
- Dehydration is caused by loss of the normal intestinal absorptive capacity as well as fluid accumulation in the gastric or intestinal wall and intraperitoneally.
- Anorexia and emesis tend to exacerbate intravascular volume depletion.
- In the worst-case scenario after high-grade distal obstruction, emesis leads to losses of gastric potassium, hydrogen, and chloride, while dehydration stimulates proximal renal tubule bicarbonate reabsorption.
- Intraperitoneal fluid accumulation, especially in patients with severe distal bowel obstruction, may increase intraabdominal pressure enough to elevate the diaphragm, inhibit respiration, impede systemic venous return, and promote vascular instability.
- Severe hemodynamic compromise may elicit a systemic inflammatory response and generalized microvascular leakage.
- Closed-loop obstruction results when the proximal and distal openings of a given bowel segment are both occluded, for example, due to volvulus or a hernia.
- It is the most common precursor for strangulation, but not every closed loop strangulates.
- The risk of vascular insufficiency, systemic inflammation, hemodynamic compromise, irreversible intestinal ischemia is much greater in patients with closed-loop obstruction.
- Pathologic changes may occur rapidly, such that emergent intervention is indicated.
- Irreversible bowel ischemia may progress to transmural necrosis even if obstruction is relieved.
3.3 Incidence by Cause¶
- Postoperative adhesions: >50% overall.
- Neoplasms: ~20%.
- Hernias (especially ventral or internal types, where the risk of strangulation is increased): ~10%.
- Inflammatory bowel disease, other inflammation (obstruction may resolve if acute inflammation and edema subside): ~5%.
- Intussusception, volvulus, other miscellaneous diseases: <15%.
Table 2 — Table 341-2 Acute Small-Intestinal and Colonic Obstruction Incidences¶
| Cause | Incidence |
|---|---|
| Postoperative adhesions | >50% overall |
| Neoplasms | ~20% |
| Hernias (especially ventral or internal types, where the risk of strangulation is increased) | ~10% |
| Inflammatory bowel disease, other inflammation (obstruction may resolve if acute inflammation and edema subside) | ~5% |
| Intussusception, volvulus, other miscellaneous diseases | <15% |
4. CLINICAL FEATURES¶
The cardinal signs are colicky abdominal pain, abdominal distention, emesis, and obstipation. More intraluminal fluid accumulates in patients with distal obstruction, which typically leads to greater distention, more discomfort, and delayed emesis. This emesis is feculent when there is bacterial overgrowth. Patients with more proximal obstruction commonly present with less abdominal distention but more pronounced vomiting. Elements of the history that might be helpful include any prior history of surgery, including herniorrhaphy, as well as any history of cancer or inflammatory bowel disease. Most patients, even those with simple obstruction, appear to be critically ill. Many may be oliguric, hypotensive, and tachycardic because of severe intravascular volume depletion. Fever is worrisome for strangulation or systemic inflammation.
4.1 Physical Examination Findings¶
- Bowel sounds and bowel activity are notoriously difficult to interpret.
- Classically, many patients with early small-bowel obstruction will have high-pitched, 'musical' tinkling bowel sounds and peristaltic 'rushes' known as borborygmi.
- Later in the course of the disease, the bowel sounds may be absent or hypoactive as peristaltic activity decreases.
- This contrasts with the common findings in patients with ileus or pseudo-obstruction where bowel sounds are typically absent or hypoactive from the beginning.
- All surgical incisions should be examined.
- The presence of a tender abdominal or groin mass strongly suggests that an incarcerated hernia may be the cause of obstruction.
- The presence of tenderness should increase the concern about the presence of complications such as ischemia, necrosis, or localized peritonitis.
- Severe pain with localization or signs of peritoneal irritation is suspicious for strangulated or closed-loop obstruction.
- Asymmetrical abdominal distension and a tympanic mass may be evident.
- Patients with ileus or pseudo-obstruction may have signs and symptoms like those with bowel obstruction. Although abdominal distention is present, colicky abdominal pain is typically absent, and patients may not have nausea or emesis.
- Ongoing, regular discharge of stool or flatus can sometimes help distinguish patients with ileus from those with complete mechanical bowel obstruction.
4.2 Differentiating Ileus vs Obstruction¶
- Ileus: Dysmotility prevents intestinal contents from being propelled distally and no mechanical blockage exists.
- Postoperative ileus is the most commonly known form of functional bowel obstruction.
- Patients with ileus typically lack colicky pain.
- Patients with ileus may pass flatus/stool.
- Obstruction: Mechanical blockage exists.
- Patients with complete mechanical obstruction typically have obstipation.
- Patients with partial blockage may continue to pass flatus and stool.
- Patients with ileus or pseudo-obstruction may have signs and symptoms like those with bowel obstruction. Although abdominal distention is present, colicky abdominal pain is typically absent, and patients may not have nausea or emesis.
5. DIFFERENTIAL DIAGNOSIS¶
The overall functional risk of ileus appears to be less in patients who undergo laparoscopic procedures. Patients with ileus or pseudo-obstruction may have signs and symptoms like those with bowel obstruction. Although abdominal distention is present, colicky abdominal pain is typically absent, and patients may not have nausea or emesis. Ongoing, regular discharge of stool or flatus can sometimes help distinguish patients with ileus from those with complete mechanical bowel obstruction. The overall functional risk of ileus appears to be less in patients who undergo laparoscopic procedures.
5.1 Ileus vs Mechanical Obstruction¶
- Ileus: Dysmotility prevents intestinal contents from being propelled distally and no mechanical blockage exists.
- Postoperative ileus is the most commonly known form of functional bowel obstruction.
- Patients with ileus typically lack colicky pain.
- Patients with ileus may pass flatus/stool.
- Obstruction: Mechanical blockage exists.
- Patients with complete mechanical obstruction typically have obstipation.
- Patients with partial blockage may continue to pass flatus and stool.
5.2 Causes of Ileus (Functional or Pseudo-Obstruction)¶
- Intraabdominal procedures, lumbar spinal injuries, or surgical procedures on the lumbar spine and pelvis.
- Metabolic or electrolyte abnormalities, especially hypokalemia and hypomagnesemia, but also hyponatremia, uremia, and severe hyperglycemia.
- Drugs such as opiates, antihistamines, and some psychotropic (e.g., haloperidol, tricyclic antidepressants) and anticholinergic agents.
- Intestinal ischemia.
- Intraabdominal or retroperitoneal inflammation or hemorrhage.
- Lower lobe pneumonias.
- Intraoperative radiation (likely due to smooth muscle damage).
- Systemic sepsis.
- Hyperparathyroidism.
- Pseudo-obstruction (Ogilvie's syndrome).
- Ileus secondary to hereditary or acquired visceral myopathies and neuropathies that disrupt myocellular neural coordination.
- Some collagen vascular diseases such as lupus erythematosus or scleroderma.
Table 3 — Table 341-3 Most Common Causes of Ileus (Functional or Pseudo-Obstruction of the Intestine)¶
| Category | Specific Causes |
|---|---|
| Procedural/Injury | Intraabdominal procedures, lumbar spinal injuries, or surgical procedures on the lumbar spine and pelvis |
| Metabolic/Electrolyte | Metabolic or electrolyte abnormalities, especially hypokalemia and hypomagnesemia, but also hyponatremia, uremia, and severe hyperglycemia |
| Drugs | Drugs such as opiates, antihistamines, and some psychotropic (e.g., haloperidol, tricyclic antidepressants) and anticholinergic agents |
| Ischemia | Intestinal ischemia |
| Inflammation | Intraabdominal or retroperitoneal inflammation or hemorrhage Lower lobe pneumonias |
| Systemic | Systemic sepsis Hyperparathyroidism |
| Pseudo-obstruction | Pseudo-obstruction (Ogilvie's syndrome) |
| Myopathy/Neuropathy | Ileus secondary to hereditary or acquired visceral myopathies and neuropathies that disrupt myocellular neural coordination |
| Collagen Vascular | Some collagen vascular diseases such as lupus erythematosus or scleroderma |
6. INVESTIGATIONS & DIAGNOSIS¶
Laboratory testing should include a complete blood count and serum electrolyte and creatinine measurements. Serial assessments are often useful. Mild hemoconcentration and slight elevation of the white blood cell count commonly occur after simple bowel obstruction. Emesis and dehydration may cause hypokalemia, hypochloremia, elevated blood urea nitrogen–to–creatinine ratios, and metabolic alkalosis. Patients may be hyponatremic on admission because many have attempted to rehydrate themselves with hypotonic fluids. The presence of guaiac-positive stools and iron-deficiency anemia are strongly suggestive of malignancy. Higher white blood cell counts with the presence of immature forms and the presence of metabolic acidosis are worrisome for severe volume depletion or ischemic necrosis and sepsis. Presently, no laboratory tests are especially useful for identifying the presence of simple or strangulated obstruction, although increases in serum d-lactate, creatine kinase BB isoenzymes, or intestinal fatty acid binding protein levels may be suggestive of the latter. Recommendations for diagnostic imaging continue to evolve. In all cases, the key is not to delay operative intervention unnecessarily when the patient's signs or symptoms strongly suggest that high-grade or complete obstruction or bowel compromise is present.
6.1 Laboratory Findings¶
- Complete blood count and serum electrolyte and creatinine measurements.
- Mild hemoconcentration and slight elevation of the white blood cell count commonly occur after simple bowel obstruction.
- Emesis and dehydration may cause hypokalemia, hypochloremia, elevated blood urea nitrogen–to–creatinine ratios, and metabolic alkalosis.
- Patients may be hyponatremic on admission because many have attempted to rehydrate themselves with hypotonic fluids.
- The presence of guaiac-positive stools and iron-deficiency anemia are strongly suggestive of malignancy.
- Higher white blood cell counts with the presence of immature forms and the presence of metabolic acidosis are worrisome for severe volume depletion or ischemic necrosis and sepsis.
- Increases in serum d-lactate, creatine kinase BB isoenzymes, or intestinal fatty acid binding protein levels may be suggestive of strangulated obstruction.
6.2 Imaging Studies¶
- Abdominal radiography, which must include upright or cross-table lateral views, can be completed quickly and may indicate the need for emergency surgical intervention in patients who are not in the immediate postoperative period.
- A 'staircasing' pattern of dilated air and fluid-filled small-bowel loops >2.5 cm in diameter with little or no air seen in the colon are classical findings in patients with small-bowel obstruction.
- Little bowel gas appears in patients with proximal bowel obstruction or in patients whose intestinal lumens are filled with fluid.
- Upright plain films of the abdomen of patients with large-bowel obstruction typically show colon dilatation.
- Small-bowel air-fluid levels may not be obvious if the ileocecal valve is incompetent.
- Although it can be difficult to distinguish from ileus, small-bowel obstruction is more likely when air-fluid levels are seen without significant colonic distension.
- Free air suggests that perforation has occurred in patients who have not recently undergone surgical procedures.
- A gas-filled, 'coffee bean'–shaped dilated shadow may be seen in patients with volvulus.
- Computed tomography (CT) is the most frequently used imaging modality.
- Its sensitivity for detecting bowel obstruction is ~95% (78–100%) in patients with high-grade obstruction, with a specificity of 96% and an accuracy of ≥95%.
- Its accuracy in diagnosing closed-loop obstruction is much lower (60%).
- CT may also provide useful information regarding location or to identify circumstances where surgical intervention is urgently needed.
- Patients who have evidence of contrast appearing within the cecum within 4–24 h of oral administration of water-soluble contrast can be expected to improve with high sensitivity and specificity (~95% each).
- Contrast studies may demonstrate a 'bird's beak,' a 'c-loop,' or 'whorl' deformity on CT imaging at the site where twisting obstructs the lumen when a colonic volvulus is present.
- Abdominal radiography, unlike CT imaging, may not accurately distinguish obstruction from other causes of colonic dysmotility.
- Ultrasonographic evaluations are especially difficult to interpret but may be sensitive and appropriate studies to evaluate patients who are pregnant or for whom x-ray exposure is otherwise contraindicated or inappropriate.
- CT imaging with enteral and IV contrast can also identify ischemia.
- Altered bowel wall enhancement is the most specific early finding, but its sensitivity is low.
- Mesenteric venous gas, pneumoperitoneum, and pneumatosis intestinalis are late findings indicating the presence of bowel necrosis.
- CT scanning after a water-soluble contrast enema may help distinguish ileus or pseudo-obstruction from distal large-bowel obstruction in patients who present with evidence of small-bowel and colonic distention.
- CT enteroclysis, though now rarely performed, can accurately identify neoplasia as a cause of bowel obstruction.
- Contrast enemas or colonoscopies are almost always needed to identify causes of acute colonic obstruction.
- Barium studies are generally contraindicated in patients with evidence of complete or high-grade bowel obstruction, especially when they present acutely.
- Barium should never be given orally to a patient with possible obstruction until that diagnosis has been excluded.
- In every other instance, such investigations should only be performed in exceptional circumstances and with great caution because patients with significant obstruction may develop barium concretions as an additional source of blockage and some who would have otherwise recovered will require operative intervention.
- Barium opacification also renders cross-sectional imaging studies or angiography uninterpretable.
7. MANAGEMENT & TREATMENT¶
An improved understanding of the pathophysiology of bowel obstruction and the importance of fluid resuscitation, electrolyte repletion, intestinal decompression, and the selected use of antibiotics has likely contributed to a reduction in mortality from acute bowel obstruction. Patients should be stabilized as quickly as possible. Nasogastric tube suction decompresses the stomach, minimizes further distention from swallowed air, improves patient comfort, and reduces the risk of aspiration. Urine output should be assessed to using a Foley catheter. In some cases, for example, in patients with cardiac disease, central venous pressures should be monitored. The use of antibiotics is controversial, although prophylactic administration may be warranted if operation is anticipated. Complete bowel obstruction is an indication for intervention. Stenting may be possible and warranted for some patients with high-grade obstruction due to unresectable stage IV malignancies. Stenting may also allow elective mechanical bowel preparation before operation. Because treatment options are so variable, it is helpful to make as precise a diagnosis as possible preoperatively. An improved understanding of the pathophysiology of bowel obstruction and the importance of fluid resuscitation, electrolyte repletion, intestinal decompression, and the selected use of antibiotics has likely contributed to a reduction in mortality from acute bowel obstruction. Patients should be stabilized as quickly as possible. Nasogastric tube suction decompresses the stomach, minimizes further distention from swallowed air, improves patient comfort, and reduces the risk of aspiration. Urine output should be assessed to using a Foley catheter. In some cases, for example, in patients with cardiac disease, central venous pressures should be monitored. The use of antibiotics is controversial, although prophylactic administration may be warranted if operation is anticipated. Complete bowel obstruction is an indication for intervention. Stenting may be possible and warranted for some patients with high-grade obstruction due to unresectable stage IV malignancies. Stenting may also allow elective mechanical bowel preparation before operation.
7.1 Initial Stabilization¶
- Patients should be stabilized as quickly as possible.
- Nasogastric tube suction decompresses the stomach, minimizes further distention from swallowed air, improves patient comfort, and reduces the risk of aspiration.
- Urine output should be assessed to using a Foley catheter.
- In some cases, for example, in patients with cardiac disease, central venous pressures should be monitored.
- The use of antibiotics is controversial, although prophylactic administration may be warranted if operation is anticipated.
7.2 Surgical Intervention¶
- Complete bowel obstruction is an indication for intervention.
- At operation, dilation proximal to the site of blockage with distal collapse is a defining feature of bowel obstruction.
- Intraoperative strategies depend on the underlying problem and range from lysis of adhesions to resection with or without diverting ostomy to primary resection with anastomosis.
- Resection is warranted when there is concern about the bowel's viability after the obstructive process is relieved.
- Laparoscopic approaches can be useful for patients with early obstruction when extensive adhesions are not expected to be present.
- Some patients with high-grade obstruction secondary to malignant disease that is not amendable to resection will benefit from bypass procedures.
- Primary resection is prudent.
- Careful manual reduction of any involved bowel may limit the amount of intestine that needs to be removed.
- A proximal ostomy may be required if unprepped colon is involved.
- The most common site of intestinal obstruction in patients with gallstone 'ileus' is the ileum (60% of patients).
- The gallstone enters the intestinal tract most often via a cholecystoduodenal fistula.
- It can usually be removed by operative enterolithotomy.
- Addressing gallbladder disease during urgent or emergent surgery is not recommended.
- Patients with sigmoid volvulus can often be decompressed using a flexible tube inserted through a rigid proctoscope or using a flexible sigmoidoscope.
- Successful decompression results in sudden release of gas and fluid with evidence of decreased abdominal distension and allows definitive correction to be scheduled electively.
- Cecal volvulus most often requires laparotomy or laparoscopic correction.
7.3 Specific Conditions¶
- Ileus: Patients with ileus are treated supportively with IV fluids and nasogastric decompression while any underlying pathology is treated, taking care to optimize the use of narcotics.
- Pharmacologic treatments continue to be evaluated with some studies showing that treatment with peripherally active μ-opioid receptor antagonists (e.g., alvimopan and methylnaltrexone) or 5-HT4 agonists that stimulate the release of acetylcholine from enteric neurons (e.g., mosapride and prucalopride) may accelerate gastrointestinal recovery in some patients who have undergone abdominal surgery.
- Colonic Pseudo-obstruction (Ogilvie's Disease): Neostigmine is an acetylcholinesterase inhibitor that increases cholinergic (parasympathetic) activity, which can stimulate colonic motility.
- Some studies have shown it to be moderately effective in alleviating acute colonic pseudo-obstruction.
- It is the most common therapeutic approach and can be used once it is certain that there is no mechanical obstruction.
- Cardiac monitoring is required, and atropine should be immediately available.
- Intravenous administration induces defecation and flatus within 10 min in the majority of patients who will respond.
- Sympathetic blockade by epidural anesthesia can successfully ameliorate pseudo-obstruction in some patients.
- Volvulus: Patients with sigmoid volvulus can often be decompressed using a flexible tube inserted through a rigid proctoscope or using a flexible sigmoidoscope.
- Successful decompression results in sudden release of gas and fluid with evidence of decreased abdominal distension and allows definitive correction to be scheduled electively.
- Cecal volvulus most often requires laparotomy or laparoscopic correction.
- Gallstone Ileus: The most common site of intestinal obstruction in patients with gallstone 'ileus' is the ileum (60% of patients). The gallstone enters the intestinal tract most often via a cholecystoduodenal fistula. It can usually be removed by operative enterolithotomy. Addressing gallbladder disease during urgent or emergent surgery is not recommended.
7.4 Postoperative Bowel Obstruction¶
- Early postoperative mechanical bowel obstruction is that which occurs within the first 6 weeks of operation.
- Although it tends to respond and behave differently from classic mechanical bowel obstruction and may be very difficult to distinguish from postoperative ileus, most are partial and can be expected to resolve spontaneously.
- A higher index of suspicion for a definitive site of obstruction is warranted for patients who undergo laparoscopic surgical procedures.
- Patients who first had ileus and then subsequently develop obstructive symptoms after an initial return of normal bowel function are more likely to have true postoperative small-bowel obstruction.
- The longer it takes for a patient's obstructive symptoms to resolve after hospitalization, the more likely the patient is to require surgical intervention.
8. PROGNOSIS & COMPLICATIONS¶
The frequency of major complications after operation ranges from 12 to 47%, with greater risk being attributed to resection therapies and the patient's overall health. Risk is increased for patients with American Society of Anesthesiologists (ASA) physical status of class III or higher. The therapeutic mortality rate for patients with strangulation who are operated on within 24–30 h of the onset of symptoms is ~8% but triples shortly thereafter.
8.1 Complication Rates¶
- The frequency of major complications after operation ranges from 12 to 47%.
- Greater risk is attributed to resection therapies and the patient's overall health.
- Risk is increased for patients with American Society of Anesthesiologists (ASA) physical status of class III or higher.
8.2 Mortality¶
- The therapeutic mortality rate for patients with strangulation who are operated on within 24–30 h of the onset of symptoms is ~8%.
- Mortality triples shortly thereafter.
9. SPECIAL CONSIDERATIONS¶
Ultrasonographic evaluations are especially difficult to interpret but may be sensitive and appropriate studies to evaluate patients who are pregnant or for whom x-ray exposure is otherwise contraindicated or inappropriate. Barium studies are generally contraindicated in patients with evidence of complete or high-grade bowel obstruction, especially when they present acutely. Barium should never be given orally to a patient with possible obstruction until that diagnosis has been excluded. In every other instance, such investigations should only be performed in exceptional circumstances and with great caution because patients with significant obstruction may develop barium concretions as an additional source of blockage and some who would have otherwise recovered will require operative intervention. Barium opacification also renders cross-sectional imaging studies or angiography uninterpretable.
9.1 Pregnancy¶
- Ultrasonographic evaluations may be sensitive and appropriate studies to evaluate patients who are pregnant.
- X-ray exposure is otherwise contraindicated or inappropriate in pregnancy.
9.2 Barium Contraindications¶
- Barium studies are generally contraindicated in patients with evidence of complete or high-grade bowel obstruction.
- Barium should never be given orally to a patient with possible obstruction until that diagnosis has been excluded.
- Patients with significant obstruction may develop barium concretions as an additional source of blockage.
- Barium opacification also renders cross-sectional imaging studies or angiography uninterpretable.
10. KEY PEARLS & CLINICAL TRAPS¶
- Closed-loop obstruction results when the proximal and distal openings of a given bowel segment are both occluded, for example, due to volvulus or a hernia. It is the most common precursor for strangulation, but not every closed loop strangulates.
- The risk of vascular insufficiency, systemic inflammation, hemodynamic compromise, irreversible intestinal ischemia is much greater in patients with closed-loop obstruction.
- Pathologic changes may occur rapidly, such that emergent intervention is indicated.
- Irreversible bowel ischemia may progress to transmural necrosis even if obstruction is relieved.
- Patients with distal obstruction whose ileocecal valves are competent may present with closed-loop obstruction. In this instance, the cecum may progressively dilate such that ischemic necrosis results in perforation, especially when the cecal diameter exceeds 10–12 cm.
- Patients with distal colonic obstruction whose ileocecal valves are incompetent tend to present later in the course of disease and mimic patients with distal findings in patients with ileus or pseudo-obstruction where bowel sounds are typically absent or hypoactive from the beginning.
- Patients with partial blockage may continue to pass flatus and stool.
- Patients with ileus or pseudo-obstruction may have signs and symptoms like those with bowel obstruction. Although abdominal distention is present, colicky abdominal pain is typically absent, and patients may not have nausea or emesis.
- Ongoing, regular discharge of stool or flatus can sometimes help distinguish patients with ileus from those with complete mechanical bowel obstruction.
- Neostigmine is contraindicated in patients with mechanical obstruction; it must be used only after mechanical obstruction is excluded.
- Barium studies are generally contraindicated in patients with evidence of complete or high-grade bowel obstruction, especially when they present acutely.
- Barium should never be given orally to a patient with possible obstruction until that diagnosis has been excluded.
10.1 Diagnostic Clues¶
- Closed-loop obstruction: Proximal and distal openings occluded (volvulus, hernia).
- Cecal diameter >10–12 cm: Risk of ischemic necrosis and perforation.
- Barium studies: Contraindicated in complete/high-grade obstruction.
- Neostigmine: Contraindicated in mechanical obstruction.
10.2 Clinical Traps¶
- Closed-loop obstruction is the most common precursor for strangulation.
- Patients with ileus may mimic obstruction (distention present, but pain/flatus absent).
- Barium concretions may require surgery if obstruction develops.
- Neostigmine can cause bradycardia; atropine must be available.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
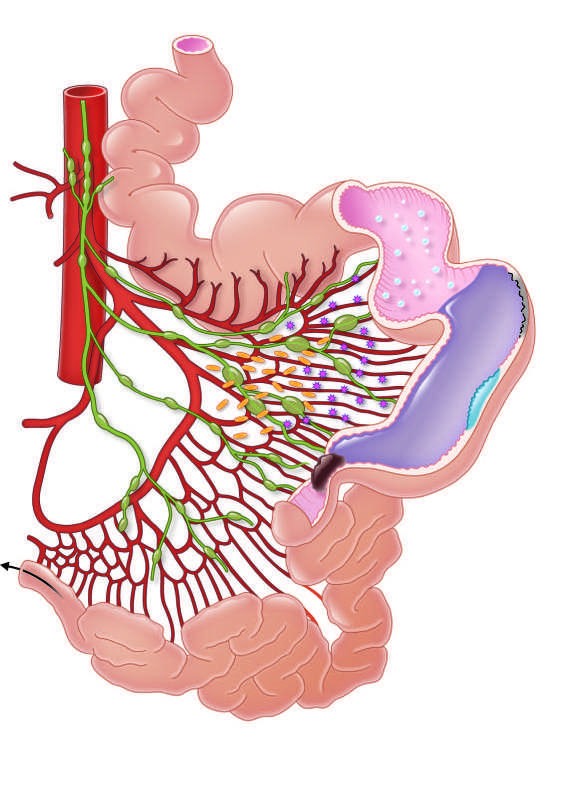
Caption: FIGURE 341-1 Pathophysiologic changes of small-bowel obstruction. — Figure 341-1: Pathophysiologic changes of small-bowel obstruction showing proximal bowel dilatation, fluid accumulation, ischemia, and necrosis at the point of obstruction with collapsed bowel distal to the block.
Figure 2¶

Caption: FIGURE 341-2 Computed tomography with oral and intravenous contrast demonstrating (A) evidence of small-bowel dilatation with air-fluid levels consistent with a small-bowel obstruction; (B) a partial small-bowel obstruction from an incarcerated ventral hernia (arrow); and (C) decompressed bowel seen distal to the hernia (arrow). (Reproduced with permission from D Longo et al: Harrison’s Principles of Internal Medicine, 18th ed. New York: McGraw-Hill; 2012.) or — Figure 341-2A: Computed tomography demonstrating small-bowel dilatation with air-fluid levels consistent with small-bowel obstruction.
Figure 3¶
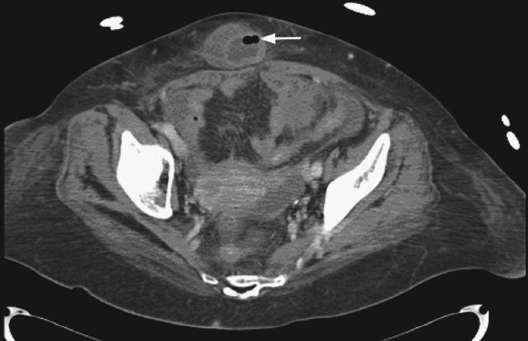
Caption: FIGURE 341-2 Computed tomography with oral and intravenous contrast demonstrating (A) evidence of small-bowel dilatation with air-fluid levels consistent with a small-bowel obstruction; (B) a partial small-bowel obstruction from an incarcerated ventral hernia (arrow); and (C) decompressed bowel seen distal to the hernia (arrow). (Reproduced with permission from D Longo et al: Harrison’s Principles of Internal Medicine, 18th ed. New York: McGraw-Hill; 2012.) or — Figure 341-2B: Computed tomography showing a partial small-bowel obstruction from an incarcerated ventral hernia (arrow).
Figure 4¶

Caption: FIGURE 341-2 Computed tomography with oral and intravenous contrast demonstrating (A) evidence of small-bowel dilatation with air-fluid levels consistent with a small-bowel obstruction; (B) a partial small-bowel obstruction from an incarcerated ventral hernia (arrow); and (C) decompressed bowel seen distal to the hernia (arrow). (Reproduced with permission from D Longo et al: Harrison’s Principles of Internal Medicine, 18th ed. New York: McGraw-Hill; 2012.) or — Figure 341-2C: Computed tomography showing decompressed bowel seen distal to the hernia (arrow).
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.