Chapter 47: Dysphagia¶
Section 6 Alterations in Gastrointestinal Function · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Dysphagia is defined as difficulty with swallowing, referring to problems with the transit of food or liquid from the mouth to the hypopharynx or through the esophagus.
- Dysphagia is subclassified by location (oral, pharyngeal, esophageal) and mechanism (structural vs. propulsive/motor).
- Intermittent dysphagia to solids implies structural dysphagia; constant dysphagia with both liquids and solids suggests an esophageal motor abnormality.
- Progressive dysphagia over weeks to months raises concern for neoplasia.
- Episodic dysphagia to solids that is unchanged or slowly progressive over years indicates a benign disease process (e.g., Schatzki ring, eosinophilic esophagitis).
- Hoarseness preceding dysphagia indicates a primary laryngeal lesion; hoarseness occurring after dysphagia suggests compromise of the recurrent laryngeal nerve by malignancy.
- Zenker's diverticulum is typically encountered in elderly patients and presents with regurgitation of particulate food debris, aspiration, and halitosis.
- Scleroderma commonly presents with absent peristalsis and a weakened LES, predisposing patients to peptic stricture formation.
- Fluoroscopy is necessary to evaluate functional abnormalities of the pharyngeal phase, requiring the patient to be conscious and cooperative.
- Immunocompromised states (e.g., AIDS) require consideration of opportunistic infections (Candida, HSV, CMV) and tumors (Kaposi's sarcoma, lymphoma).
- Atopy increases concerns for eosinophilic esophagitis, most prevalent in Caucasian male patients between ages 20 and 40 years.
- Cricopharyngeal bars are common radiographic findings; most patients with transient bars are asymptomatic, making it important to rule out alternative etiologies before treatment.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Terminology
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Physiology of Swallowing
- 3.2 Neuromuscular Apparatus
- 3.3 Pathophysiology of Dysphagia
- 4. CLINICAL FEATURES
- 4.1 Oral and Pharyngeal Dysphagia
- 4.2 Esophageal Dysphagia
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Structural Causes
- 5.2 Propulsive Causes
- 5.3 Myogenic Causes
- 5.4 Neurogenic Causes
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 History
- 6.2 Physical Examination
- 6.3 Imaging and Endoscopy
- 7. MANAGEMENT & TREATMENT
- 7.1 Structural Management
- 7.2 Motor Management
- 7.3 Infectious and Inflammatory Management
- 7.4 Neurogenic Management
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 9.1 Immunocompromised States
- 9.2 Atopy
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | shows an algorithm for the approach to a patient with dysphagia |
| 1 | 🖼 Figure | Sagittal and diagrammatic views of the musculature involved in enacting and the... |
| 2 | 🖼 Figure | Sagittal and diagrammatic views of the musculature involved in enacting and the... |
1. DEFINITION & OVERVIEW¶
Dysphagia—difficulty with swallowing—refers to problems with the transit of food or liquid from the mouth to the hypopharynx or through the esophagus. Severe dysphagia can compromise nutrition, cause aspiration, and reduce quality of life. Additional terminology pertaining to swallowing dysfunction is as follows.
1.1 Terminology¶
Harrison's defines these terms as follows:
2. EPIDEMIOLOGY¶
Epidemiology data not explicitly detailed in the provided source text.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Dysphagia can be subclassified both by location and by the circumstances in which it occurs. With respect to location, distinct considerations apply to oral, pharyngeal, or esophageal dysphagia. Normal transport of an ingested bolus depends on the consistency and size of the bolus, the caliber of the lumen, the integrity of peristaltic contraction, and deglutitive inhibition of both the UES and the LES. Dysphagia caused by an oversized bolus or a narrow lumen is called structural dysphagia, whereas dysphagia due to abnormalities of peristalsis or impaired sphincter relaxation after swallowing is called propulsive or motor dysphagia. More than one mechanism may be operative in a patient with dysphagia.
3.1 Physiology of Swallowing¶
Swallowing begins with a voluntary (oral) phase that includes preparation during which food is masticated and mixed with saliva. This is followed by a transfer phase during which the bolus is pushed into the pharynx by the tongue. Bolus entry into the hypopharynx initiates the pharyngeal swallow response, which is centrally mediated and involves a complex series of actions, the net result of which is to propel food through the pharynx into the esophagus while preventing its entry into the airway. To accomplish this, the larynx is elevated and pulled forward, actions that also facilitate upper esophageal sphincter (UES) opening. Tongue pulsion then propels the bolus through the UES, followed by a peristaltic contraction that clears residue from the pharynx and through the esophagus. The lower esophageal sphincter (LES) relaxes as the food enters the esophagus and remains relaxed until the peristaltic contraction has delivered the bolus into the stomach. Peristaltic contractions elicited in response to a swallow are called primary peristalsis and involve sequenced inhibition followed by contraction of the musculature along the entire length of the esophagus.
3.2 Neuromuscular Apparatus¶
The musculature of the oral cavity, pharynx, UES, and cervical esophagus is striated and directly innervated by lower motor neurons carried in cranial nerves. Oral cavity muscles are innervated by the fifth (trigeminal) and seventh (facial) cranial nerves; the tongue, by the twelfth (hypoglossal) cranial nerve. Pharyngeal muscles are innervated by the ninth (glossopharyngeal) and tenth (vagus) cranial nerves. Physiologically, the UES consists of the cricopharyngeus muscle, the adjacent inferior pharyngeal constrictor, and the proximal portion of the cervical esophagus. UES innervation is derived from the vagus nerve, whereas the innervation to the musculature acting on the UES to facilitate its opening during swallowing comes from the fifth, seventh, and twelfth cranial nerves. The UES remains closed at rest owing to both its inherent elastic properties and neurogenically mediated contraction of the cricopharyngeus muscle. UES opening during swallowing involves both cessation of vagal excitation to the cricopharyngeus and simultaneous contraction of the suprahyoid and geniohyoid muscles that pull open the UES in conjunction with the upward and forward displacement of the larynx. The cervical esophagus, like the pharyngeal musculature, consists of striated muscle and is directly innervated by lower motor neurons of the vagus nerve. Peristalsis in the proximal esophagus is governed by the sequential activation of the vagal motor neurons in the nucleus ambiguus. In contrast, the distal esophagus and LES are composed of smooth muscle and are controlled by excitatory and inhibitory neurons within the esophageal myenteric plexus. Medullary preganglionic neurons from the dorsal motor nucleus of the vagus trigger peristalsis via these ganglionic neurons during primary peristalsis. Neurotransmitters of the excitatory ganglionic neurons are acetylcholine and substance P; those of the inhibitory neurons are vasoactive intestinal peptide and nitric oxide. Peristalsis results from the patterned activation of inhibitory followed by excitatory ganglionic neurons, with progressive dominance of the inhibitory neurons distally. Similarly, LES relaxation occurs with the onset of deglutitive inhibition and persists until the peristaltic sequence is complete. At rest, the LES is contracted because of excitatory ganglionic stimulation and its intrinsic myogenic tone, a property that distinguishes it from the adjacent esophagus. The function of the LES is supplemented by the surrounding muscle of the right diaphragmatic crus, which acts as an external sphincter during inspiration, cough, or abdominal straining.
3.3 Pathophysiology of Dysphagia¶
Dysphagia can be subclassified both by location and by the circumstances in which it occurs. With respect to location, distinct considerations apply to oral, pharyngeal, or esophageal dysphagia. Normal transport of an ingested bolus depends on the consistency and size of the bolus, the caliber of the lumen, the integrity of peristaltic contraction, and deglutitive inhibition of both the UES and the LES. Dysphagia caused by an oversized bolus or a narrow lumen is called structural dysphagia, whereas dysphagia due to abnormalities of peristalsis or impaired sphincter relaxation after swallowing is called propulsive or motor dysphagia. More than one mechanism may be operative in a patient with dysphagia. Scleroderma commonly presents with absent peristalsis as well as a weakened LES that predisposes patients to peptic stricture formation. Likewise, radiation therapy for head and neck cancer may compound the functional deficits in the oropharyngeal swallowing attributable to the tumor and cause cervical esophageal stenosis. It is worth noting that in addition to bolus transit, symptom reporting of dysphagia is dependent upon intact sensory innervation and central nervous system perception. Chronicity of motor dysfunction in combination with defects in peripheral sensory perception may reduce indentation behind the lower third of the cricoid cartilage, is related to Zenker's diverticulum in that it involves limited distensibility of the cricopharyngeus and can lead to the formation of a Zenker's diverticulum. However, a cricopharyngeal bar is a common radiographic finding, and most patients with transient cricopharyngeal bars are asymptomatic, making it important to rule out alternative etiologies of dysphagia before treatment. Furthermore, cricopharyngeal bars may be secondary to other neuromuscular disorders that impair opening of the UES.
4. CLINICAL FEATURES¶
Dysphagia localized to neck, nasal regurgitation, aspiration, neck, food impaction, and associated ENT symptoms are hallmarks of oropharyngeal dysphagia. Dysphagia localized to chest or neck, food impaction, and associated ENT symptoms are hallmarks of oropharyngeal dysphagia. Dysphagia localized to chest is esophageal in origin. Nasal regurgitation and tracheobronchial aspiration manifest by coughing with swallowing are hallmarks of oropharyngeal dysphagia. Severe cough with swallowing may also be a sign of a tracheoesophageal fistula. The presence of hoarseness may be another important diagnostic clue. When hoarseness precedes dysphagia, the primary lesion is usually laryngeal; hoarseness that occurs after the development of dysphagia may result from compromise of the recurrent laryngeal nerve by a malignancy. The type of food causing dysphagia is an important consideration. Intermittent dysphagia that occurs only with solid food implies structural dysphagia, whereas constant dysphagia with both liquids and solids strongly suggests an esophageal motor abnormality. Two caveats to this pattern are that despite having a motor abnormality, patients with scleroderma generally develop mild dysphagia for solids only and that patients with oropharyngeal dysphagia often have greater difficulty managing liquids than solids. Dysphagia that is progressive over the course of weeks to months raises concern for neoplasia. Episodic dysphagia to solids that is unchanged or slowly progressive over years indicates a benign disease process such as a Schatzki ring or eosinophilic esophagitis. Food impaction with a prolonged inability to pass an ingested bolus even with ingestion of liquid is typical of structural dysphagia. Chest pain may accompany dysphagia whether it is prolonged history of heartburn preceding the onset of dysphagia is suggestive of peptic stricture and, infrequently, esophageal adenocarcinoma.
4.1 Oral and Pharyngeal Dysphagia¶
Oral-phase dysphagia is associated with poor bolus formation and control so that food has prolonged retention within the oral cavity and may seep out of the mouth. Drooling and difficulty in initiating swallowing are characteristic signs. Poor bolus control also may lead to premature spillage of food into the hypopharynx with resultant aspiration into the trachea, evident as swallow-induced cough or regurgitation into the nasal cavity. Pharyngeal-phase dysphagia is associated with retention of food in the pharynx due to poor tongue or pharyngeal propulsion or obstruction at the UES. Signs and symptoms of concomitant hoarseness or cranial nerve dysfunction may be associated with oropharyngeal dysphagia that is associated with neurologic disorders.
4.2 Esophageal Dysphagia¶
The adult esophagus measures 18–26 cm in length and is anatomically divided into the cervical esophagus, extending from the pharyngoesophageal junction to the suprasternal notch, and the thoracic esophagus, which continues to the diaphragmatic hiatus. When distended, the esophageal lumen has internal dimensions of about 2 cm in the anteroposterior plane and 3 cm in the lateral plane. Solid food dysphagia becomes common when the lumen is narrowed to <13 mm, but also can occur with larger diameters in the setting of poorly masticated food or motor dysfunction. Circumferential lesions are more likely to cause dysphagia than are lesions that involve only a partial circumference of the esophageal wall. The most common structural causes of dysphagia are Schatzki's rings, eosinophilic esophagitis, and peptic strictures. Dysphagia also occurs in the setting of gastroesophageal reflux disease without a stricture, perhaps on the basis of altered esophageal sensation, reduced esophageal mural distensibility, or motor dysfunction. Propulsive disorders leading to esophageal dysphagia result from abnormalities of peristalsis and/or deglutitive inhibition, potentially affecting the cervical or thoracic esophagus. Since striated muscle pathology usually involves both the oropharynx and the cervical esophagus, the clinical manifestations usually are dominated by oropharyngeal dysphagia. Diseases affecting smooth muscle involve both the thoracic esophagus and the LES. A dominant manifestation of this, absent peristalsis, refers to either the complete absence of swallow-induced contraction (absent contractility) or the presence of nonperistaltic, disordered contractions. Absent peristalsis and failure of deglutitive LES relaxation are the defining features of achalasia. In distal esophageal spasm (DES), LES function is normal, with the disordered motility restricted to the esophageal body. Absent contractility combined with severe weakness of the LES is a pattern commonly found in patients with scleroderma.
5. DIFFERENTIAL DIAGNOSIS¶
Oropharyngeal dysphagia may be due to neurologic, muscular, structural, iatrogenic, infectious, and metabolic causes. Iatrogenic, neurologic, and structural pathologies are most common. Iatrogenic causes include surgery and radiation, often in the setting of head and neck cancer. Neurogenic dysphagia resulting from cerebrovascular accidents, Parkinson's disease, and amyotrophic lateral sclerosis is a major source of morbidity related to aspiration and malnutrition. Oropharyngeal structural lesions causing dysphagia include Zenker's diverticulum, cricopharyngeal bar, and neoplasia. Esophageal dysphagia etiologies include structural, propulsive, and structural causes. Structural causes include Schatzki's rings, eosinophilic esophagitis, peptic strictures, Zenker's diverticulum, cricopharyngeal bar, neoplasia, cervical web, osteophytes, congenital abnormalities, post head and neck surgery, chemotherapy mucositis, radiation, corrosive injury, infection, cerebral palsy, brainstem tumor, Guillain-Barré, paraneoplastic, scleroderma, surgical stenosis, hiatal hernia, lichen planus, ringed esophagus, congenital esophageal stenosis. Propulsive causes include cerebral vascular accident, polymyositis, myasthenia gravis, achalasia (primary and secondary), diffuse esophageal spasm, eosinophilic esophagitis, Behcet's syndrome, bullous pemphigoid, Crohn's disease, mixed connective tissue disorders, oculopharyngeal muscular dystrophy, Huntington's chorea syndrome, sarcoidosis, radiation esophagitis, multiple sclerosis, myotonic dystrophy, post-polio syndrome, and esophageal web. Myogenic causes include myasthenia gravis, polymyositis, oculopharyngeal muscular dystrophy, Huntington's chorea syndrome, and myotonic dystrophy. Neurogenic causes include cerebrovascular accident, Parkinson's disease, amyotrophic lateral sclerosis, brainstem tumor, Guillain-Barré, multiple sclerosis, and post-polio syndrome.
5.1 Structural Causes¶
Zenker's diverticulum, cricopharyngeal bar, neoplasia, Schatzki's rings, eosinophilic esophagitis, peptic strictures, cervical web, osteophytes, congenital abnormalities, post head and neck surgery, chemotherapy mucositis, radiation, corrosive injury, infection, cerebral palsy, brainstem tumor, Guillain-Barré, paraneoplastic, scleroderma, surgical stenosis, hiatal hernia, lichen planus, ringed esophagus, congenital esophageal stenosis.
5.2 Propulsive Causes¶
Cerebral vascular accident, polymyositis, myasthenia gravis, achalasia (primary and secondary), diffuse esophageal spasm, eosinophilic esophagitis, Behcet's syndrome, bullous pemphigoid, Crohn's disease, mixed connective tissue disorders, oculopharyngeal muscular dystrophy, Huntington's chorea syndrome, sarcoidosis, radiation esophagitis, multiple sclerosis, myotonic dystrophy, post-polio syndrome, and esophageal web.
5.3 Myogenic Causes¶
Myasthenia gravis, polymyositis, oculopharyngeal muscular dystrophy, Huntington's chorea syndrome, and myotonic dystrophy.
5.4 Neurogenic Causes¶
Cerebrovascular accidents, Parkinson's disease, amyotrophic lateral sclerosis, brainstem tumor, Guillain-Barré, multiple sclerosis, and post-polio syndrome.
6. INVESTIGATIONS & DIAGNOSIS¶
The patient history is extremely valuable in making a presumptive diagnosis or at least substantially limiting the differential diagnoses in most patients. Key elements of the history are the localization of dysphagia, the circumstances in which dysphagia is experienced, other symptoms associated with dysphagia, and progression. Dysphagia that localizes to the suprasternal notch may indicate either an oropharyngeal or an esophageal etiology as distal dysphagia is referred proximally about 30% of the time. Dysphagia that localizes to the chest is esophageal in origin. Nasal regurgitation and tracheobronchial aspiration manifest by coughing with swallowing are hallmarks of oropharyngeal dysphagia. Severe cough with swallowing may also be a sign of a tracheoesophageal fistula. The presence of hoarseness may be another important diagnostic clue. When hoarseness precedes dysphagia, the primary lesion is usually laryngeal; hoarseness that occurs after the development of dysphagia may result from compromise of the recurrent laryngeal nerve by a malignancy. The type of food causing dysphagia is an important consideration. Intermittent dysphagia that occurs only with solid food implies structural dysphagia, whereas constant dysphagia with both liquids and solids strongly suggests an esophageal motor abnormality. Two caveats to this pattern are that despite having a motor abnormality, patients with scleroderma generally develop mild dysphagia for solids only and that patients with oropharyngeal dysphagia often have greater difficulty managing liquids than solids. Dysphagia that is progressive over the course of weeks to months raises concern for neoplasia. Episodic dysphagia to solids that is unchanged or slowly progressive over years indicates a benign disease process such as a Schatzki ring or eosinophilic esophagitis. Food impaction with a prolonged inability to pass an ingested bolus even with ingestion of liquid is typical of structural dysphagia. Chest pain may accompany dysphagia whether it is prolonged history of heartburn preceding the onset of dysphagia is suggestive of peptic stricture and, infrequently, esophageal adenocarcinoma. A history of prolonged nasogastric intubation, esophageal or head and neck surgery, ingestion of caustic agents or pills, previous radiation or chemotherapy, or associated mucocutaneous diseases may help isolate the cause of dysphagia. With accompanying odynophagia, which usually is indicative of ulceration, infectious or pill-induced esophagitis should be suspected. In patients with AIDS or other immunocompromised states, esophagitis due to opportunistic infections such as Candida, herpes simplex virus, or cytomegalovirus and to tumors such as Kaposi's sarcoma and lymphoma should be considered. A history of atopy increases concerns for eosinophilic esophagitis, which is most prevalent in Caucasian male patients between the ages of 20 and 40 years. Medication use should identify agents associated with pill esophagitis and narcotics that are associated with opioid-induced esophageal dysmotility. Physical examination is important in the evaluation of oral and pharyngeal dysphagia because dysphagia is usually only one of many manifestations of a more global disease process. Signs of bulbar or pseudobulbar palsy, including dysarthria, dysphonia, ptosis, and regurgitation, aspiration, neck, food impaction, and associated ENT symptoms are hallmarks of oropharyngeal dysphagia. Adequate fluoroscopic examination requires that the patient be conscious and cooperative. The study incorporates recordings of swallow sequences during ingestion of food and liquids of varying consistencies. The pharynx is examined to detect bolus retention, regurgitation into the nose, or aspiration into the trachea. Timing and integrity of pharyngeal contraction and opening of the UES with a swallow are analyzed to assess both aspiration risk and the potential for swallow therapy. Structural abnormalities of the oropharynx, especially those that may require biopsies, also should be assessed by direct laryngoscopic examination.
6.1 History¶
Key elements of the history are the localization of dysphagia, the circumstances in which dysphagia is experienced, other symptoms associated with dysphagia, and progression. Dysphagia that localizes to the suprasternal notch may indicate either an oropharyngeal or an esophageal etiology as distal dysphagia is referred proximally about 30% of the time. Dysphagia that localizes to the chest is esophageal in origin. Nasal regurgitation and tracheobronchial aspiration manifest by coughing with swallowing are hallmarks of oropharyngeal dysphagia. Severe cough with swallowing may also be a sign of a tracheoesophageal fistula. The presence of hoarseness may be another important diagnostic clue. When hoarseness precedes dysphagia, the primary lesion is usually laryngeal; hoarseness that occurs after the development of dysphagia may result from compromise of the recurrent laryngeal nerve by a malignancy. The type of food causing dysphagia is an important consideration. Intermittent dysphagia that occurs only with solid food implies structural dysphagia, whereas constant dysphagia with both liquids and solids strongly suggests an esophageal motor abnormality. Two caveats to this pattern are that despite having a motor abnormality, patients with scleroderma generally develop mild dysphagia for solids only and that patients with oropharyngeal dysphagia often have greater difficulty managing liquids than solids. Dysphagia that is progressive over the course of weeks to months raises concern for neoplasia. Episodic dysphagia to solids that is unchanged or slowly progressive over years indicates a benign disease process such as a Schatzki ring or eosinophilic esophagitis. Food impaction with a prolonged inability to pass an ingested bolus even with ingestion of liquid is typical of structural dysphagia. Chest pain may accompany dysphagia whether it is prolonged history of heartburn preceding the onset of dysphagia is suggestive of peptic stricture and, infrequently, esophageal adenocarcinoma. A history of prolonged nasogastric intubation, esophageal or head and neck surgery, ingestion of caustic agents or pills, previous radiation or chemotherapy, or associated mucocutaneous diseases may help isolate the cause of dysphagia. With accompanying odynophagia, which usually is indicative of ulceration, infectious or pill-induced esophagitis should be suspected. In patients with AIDS or other immunocompromised states, esophagitis due to opportunistic infections such as Candida, herpes simplex virus, or cytomegalovirus and to tumors such as Kaposi's sarcoma and lymphoma should be considered. A history of atopy increases concerns for eosinophilic esophagitis, which is most prevalent in Caucasian male patients between the ages of 20 and 40 years. Medication use should identify agents associated with pill esophagitis and narcotics that are associated with opioid-induced esophageal dysmotility.
6.2 Physical Examination¶
Physical examination is important in the evaluation of oral and pharyngeal dysphagia because dysphagia is usually only one of many manifestations of a more global disease process. Signs of bulbar or pseudobulbar palsy, including dysarthria, dysphonia, ptosis, and regurgitation, aspiration, neck, food impaction, and associated ENT symptoms are hallmarks of oropharyngeal dysphagia.
6.3 Imaging and Endoscopy¶
Adequate fluoroscopic examination requires that the patient be conscious and cooperative. The study incorporates recordings of swallow sequences during ingestion of food and liquids of varying consistencies. The pharynx is examined to detect bolus retention, regurgitation into the nose, or aspiration into the trachea. Timing and integrity of pharyngeal contraction and opening of the UES with a swallow are analyzed to assess both aspiration risk and the potential for swallow therapy. Structural abnormalities of the oropharynx, especially those that may require biopsies, also should be assessed by direct laryngoscopic examination.
7. MANAGEMENT & TREATMENT¶
Dysphagia related to motor disorders, structural disorders, or reflux disease. A Figure 47-2 shows an algorithm for the approach to a patient with dysphagia. Management depends on the underlying etiology. Structural causes may require dilation (Schatzki ring), surgery (Zenker's diverticulum, cricopharyngeal bar), or treatment of underlying malignancy. Motor disorders may require pharmacologic therapy (e.g., for achalasia) or surgical intervention (e.g., Heller myotomy). Reflux disease may require acid suppression. Pill esophagitis requires cessation of offending agents. Caustic injury requires supportive care. Radiation esophagitis requires supportive care. Infectious esophagitis requires antifungal or antiviral therapy. Neoplasia requires oncologic management. Opioid-induced dysmotility requires cessation of opioids. Eosinophilic esophagitis requires dietary modification and/or topical steroids. Achalasia may require pneumatic dilation, botulinum toxin injection, or Heller myotomy. Scleroderma management focuses on acid suppression and monitoring for strictures. Peptic stricture may require dilation. Crohn's disease requires medical management of the underlying condition. Behcet's syndrome requires immunosuppression. Bullous pemphigoid requires immunosuppression. Lichen planus requires topical steroids. Hiatal hernia may require surgical repair. Congenital esophageal stenosis may require dilation. Extrinsic compression may require surgical decompression. Radiation esophagitis requires supportive care. Multiple sclerosis, myotonic dystrophy, post-polio syndrome, and other neurogenic causes require management of the underlying neurologic condition.
7.1 Structural Management¶
Schatzki ring: Dilation. Zenker's diverticulum: Surgery. Cricopharyngeal bar: Dilation or myotomy. Peptic stricture: Dilation. Caustic injury: Supportive care. Neoplasia: Oncologic management.
7.2 Motor Management¶
Achalasia: Pneumatic dilation, botulinum toxin injection, Heller myotomy. Distal esophageal spasm: Calcium channel blockers, nitrates. Scleroderma: Acid suppression, monitoring for strictures. Diffuse esophageal spasm: Calcium channel blockers, nitrates.
7.3 Infectious and Inflammatory Management¶
Candida esophagitis: Antifungal therapy. Herpes simplex virus esophagitis: Antiviral therapy. Cytomegalovirus esophagitis: Antiviral therapy. Kaposi's sarcoma: Chemotherapy/immunotherapy. Lymphoma: Chemotherapy/immunotherapy. Eosinophilic esophagitis: Dietary modification, topical steroids. Pill esophagitis: Cessation of offending agents. Opioid-induced dysmotility: Cessation of opioids.
7.4 Neurogenic Management¶
Cerebrovascular accident: Swallow therapy. Parkinson's disease: Swallow therapy, medication optimization. Amyotrophic lateral sclerosis: Swallow therapy, nutritional support. Myasthenia gravis: Acetylcholinesterase inhibitors, immunosuppression. Polymyositis: Immunosuppression. Oculopharyngeal muscular dystrophy: Supportive care. Huntington's chorea syndrome: Supportive care. Myotonic dystrophy: Supportive care. Multiple sclerosis: Disease-modifying therapy. Post-polio syndrome: Supportive care.
8. PROGNOSIS & COMPLICATIONS¶
Severe dysphagia can compromise nutrition, cause aspiration, and reduce quality of life. Neurogenic dysphagia resulting from cerebrovascular accidents, Parkinson's disease, and amyotrophic lateral sclerosis is a major source of morbidity related to aspiration and malnutrition. Chronicity of motor dysfunction in combination with defects in peripheral sensory perception may reduce indentation behind the lower third of the cricoid cartilage, is related to Zenker's diverticulum in that it involves limited distensibility of the cricopharyngeus and can lead to the formation of a Zenker's diverticulum. However, a cricopharyngeal bar is a common radiographic finding, and most patients with transient cricopharyngeal bars are asymptomatic, making it important to rule out alternative etiologies of dysphagia before treatment. Furthermore, cricopharyngeal bars may be secondary to other neuromuscular disorders that impair opening of the UES.
9. SPECIAL CONSIDERATIONS¶
In patients with AIDS or other immunocompromised states, esophagitis due to opportunistic infections such as Candida, herpes simplex virus, or cytomegalovirus and to tumors such as Kaposi's sarcoma and lymphoma should be considered. A history of atopy increases concerns for eosinophilic esophagitis, which is most prevalent in Caucasian male patients between the ages of 20 and 40 years.
9.1 Immunocompromised States¶
AIDS or other immunocompromised states: Esophagitis due to opportunistic infections such as Candida, herpes simplex virus, or cytomegalovirus and to tumors such as Kaposi's sarcoma and lymphoma should be considered.
9.2 Atopy¶
Atopy: Increases concerns for eosinophilic esophagitis, which is most prevalent in Caucasian male patients between the ages of 20 and 40 years.
10. KEY PEARLS & CLINICAL TRAPS¶
Dysphagia that is progressive over the course of weeks to months raises concern for neoplasia. Episodic dysphagia to solids that is unchanged or slowly progressive over years indicates a benign disease process such as a Schatzki ring or eosinophilic esophagitis. Food impaction with a prolonged inability to pass an ingested bolus even with ingestion of liquid is typical of structural dysphagia. Chest pain may accompany dysphagia whether it is prolonged history of heartburn preceding the onset of dysphagia is suggestive of peptic stricture and, infrequently, esophageal adenocarcinoma. Most patients with transient cricopharyngeal bars are asymptomatic, making it important to rule out alternative etiologies of dysphagia before treatment. Hoarseness that precedes dysphagia, the primary lesion is usually laryngeal; hoarseness that occurs after the development of dysphagia may result from compromise of the recurrent laryngeal nerve by a malignancy.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶

Caption: Figure 47-2 shows an algorithm for the approach to a patient with dysphagia. HISTORY The patient history is extremely valuable in making a presumptive diagnosis or at least substantially limiting the differential diagnoses in most patients. Key elements of the history are the localization of dysphagia, the circumstances in which dysphagia is experienced, other symptoms associated with dysphagia, and progression. Dys- phagia that localizes to the suprasternal notch may indicate either
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
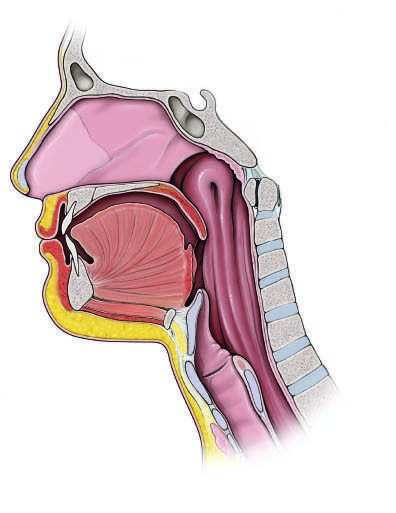
Caption: FIGURE 47-1 Sagittal and diagrammatic views of the musculature involved in enacting and the intimate relationship between the entrance to the larynx (airway) and the transiently reconfigured such that the esophageal inlet is open and the laryngeal inlet [eds]: Dysphagia: Diagnosis and Treatment. New York, Igaku-Shoin Medical Publishers, — Sagittal and diagrammatic views of the musculature involved in enacting oropharyngeal swallowing. Note the dominance of the tongue in the sagittal view and the intimate relationship between the entrance to the larynx (airway) and the esophagus. In the resting configuration illustrated, the esophageal inlet is closed. This is transiently reconfigured such that the esophageal inlet is open and the laryngeal inlet closed during swallowing.
Figure 2¶

Caption: FIGURE 47-1 Sagittal and diagrammatic views of the musculature involved in enacting and the intimate relationship between the entrance to the larynx (airway) and the transiently reconfigured such that the esophageal inlet is open and the laryngeal inlet [eds]: Dysphagia: Diagnosis and Treatment. New York, Igaku-Shoin Medical Publishers, — Approach to the patient with dysphagia. Etiologies in bold print are the most common. ENT, ear, nose, and throat; GERD, gastroesophageal reflux disease.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.