Chapter 88: Pancreatic Cancer¶
Part 4: Oncology and Hematology · Part 4 – Oncology: Solid Tumors
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Pancreatic cancer is the third leading cause of cancer-related mortality in the United States with an overall 5-year survival of 13%.
- Cigarette smoking is the greatest risk factor, believed to cause 25 to 30% of pancreatic cancers.
- High BMI (≥30) is associated with a doubling of pancreatic cancer risk.
- KRAS mutations are seen in 90–95% of pancreatic adenocarcinomas; TP53 in ~75%; DPC4/SMAD4 in about half.
- Modified FOLFIRINOX is the standard adjuvant therapy with median survival of 54 months compared to 35 months for gemcitabine alone.
- Patients with BRCA1/2 or PALB2 germline variants should be considered for PARP inhibitor therapy in metastatic disease.
- CA19-9 is a serum marker but is nondetectable in Lewis antigen non-secretors, limiting its utility in that subgroup.
- Trousseau's syndrome (migratory superficial thrombophlebitis) and Virchow's node (supraclavicular lymphadenopathy) are classic signs of advanced disease.
- Neoadjuvant therapy is the standard approach for borderline resectable or locally advanced disease to assess tumor biology and downstage.
- Screening is not recommended for average-risk individuals but is indicated for high-risk groups (e.g., BRCA1/2, PALB2, family history).
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Epidemiology & Survival
- 1.2 Screening & High-Risk Populations
- 2. EPIDEMIOLOGY
- 2.1 Demographics & Trends
- 2.2 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Molecular Characteristics
- 3.2 Precursor Lesions
- 3.3 Location & Pathology
- 4. CLINICAL FEATURES
- 4.1 Symptoms & Signs
- 4.2 Physical Examination Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Painless Jaundice
- 5.2 Weight Loss & Epigastric Pain
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Imaging
- 6.2 Histologic Diagnosis & Markers
- 6.3 Staging
- 7. MANAGEMENT & TREATMENT
- 7.1 Resectable Disease
- 7.2 Locally Advanced Disease
- 7.3 Metastatic Disease
- 7.4 Adjuvant Therapy
- 7.5 Neoadjuvant Therapy
- 7.6 Molecularly Targeted Therapy
- 7.7 Supportive Care
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Survival by Stage
- 8.2 Complications
- 9. SPECIAL CONSIDERATIONS
- 9.1 Genetic Risk & Screening
- 9.2 Molecular Profile Considerations
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Exclusion Criteria
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Pancreatic cancer is the third leading cause of cancer-related mortality in the United States, with >66,000 Americans diagnosed and >51,000 dying from the disease each year. Pancreatic cancer is projected to be the second leading cause of death from cancer in the United States by 2030. Worldwide, pancreatic cancer is the eleventh most common cancer, with about half a million diagnoses per annum. Pancreatic cancer is the most lethal human cancer, with an overall 5-year survival of 13%. However, that situation is changing due to enhanced understanding of pathobiology, integration of multimodality therapy, and eligibility for targeted therapy beyond cytotoxic therapy.
1.1 Epidemiology & Survival¶
Pancreatic cancer accounts for 3% of all new cancer cases in the United States and ~8.3% of all deaths from cancer in the United States. The lifetime risk of developing pancreatic cancer is ~1.7%. The incidence has been increasing about 1.1% per year overall, but notably in people <55 years of age, it has been increasing 2.36% per year in women and 0.62% per year in men. Pancreatic cancer is more common with increasing age and slightly more common in men than in women. The 5-year survival rate for all stages has increased from 3% in 1975 to 13% in 2024. The latest information from the U.S. Surveillance, Epidemiology, and End Results (SEER) database predicts that the 5-year survival is about 44% for patients with localized pancreatic cancer, 16% for those with regional disease, and 3.2% for patients with metastatic disease.
1.2 Screening & High-Risk Populations¶
For an average-risk individual (without any known predisposing factors), there is currently no recommended screening. Knowing that an individual carries a BRCA1/2 or PALB2 germline variant or any of the above mutations requires referral of that person to an early detection or high-risk screening clinic. For patients with a BRCA1/2 or PALB2 pathogenic germline variant, a poly(ADP-ribose) polymerase (PARP) inhibitor should be considered as part of treatment for metastatic pancreatic cancer. Other pathogenic germline variants are under study to determine their increased risk of pancreatic cancer, including CFTR, PRSS2, CDK4, FANCC, APC, ATM, BRIP1, BRCA1, EPCAM, MEN1, MLH1, MSH2, MSH6, NF1, PMS2, SMAD4, TP53, TSC1, TSC2, and VHL. Some of these variants are also associated with pancreatic neuroendocrine tumors. In addition to recognized genetic syndromes from single gene variants, other individuals without any of these identifiable germline variants may be at higher risk for this cancer. For example, a family history of pancreatic cancer is associated with increased risk based on the number of affected relatives. Having one first-degree relative with pancreatic cancer, one's risk for developing the disease is increased 4.6-fold, having two first-degree relatives increases the risk 6.4-fold, and three or more first-degree relatives confers a 32-fold increased risk. The risk is increased if a relative developed pancreatic cancer at <55 years old and is further compounded by smoking.
Table 1 — Table 88-1 Germline Mutations, Familial Cancer Syndromes, and Fold Risk of Pancreatic Cancer¶
| Germline Mutation | Familial Cancer Syndrome | Estimated Increased Risk (Fold) of Pancreatic Cancer |
|---|---|---|
| BRCA2 | Familial breast/ovarian cancer and others | 3.5–10 |
| p16/CDKN2A | Familial atypical multiple mole melanoma (FAMMM) | 15–22 |
| PRSS1 or SPIN11b | Hereditary (familial) pancreatitis | 53 |
| STK11 (LKB1) | Peutz-Jeghers syndrome | 76–140 |
| ATM | Ataxia-telangiectasia | 6 |
| MLH1, MSH2, MSH6, PMS2 | Hereditary nonpolyposis colorectal syndrome or Lynch syndrome | 9–36 |
2. EPIDEMIOLOGY¶
Pancreatic cancer accounts for 3% of all new cancer cases in the United States and ~8.3% of all deaths from cancer in the United States. The lifetime risk of developing pancreatic cancer is ~1.7%. The incidence has been increasing about 1.1% per year overall, but notably in people 30% in the first 3 years (along with a decrease in their hemoglobin A1c and blood glucose level). Physical inactivity also has been associated with an increased risk of pancreatic cancer.
2.1 Demographics & Trends¶
Age is one of the strongest risk factors for pancreatic cancer with median age at diagnosis of 71 years (the disease is most frequently diagnosed in the 65–79 age group; for men, 65–69; for women, 75–79). The number of new cases per 100,000 persons and the number of deaths per 100,000 persons are higher for males and for black people of both sexes. People who have a non-O blood type are at higher risk of developing pancreatic cancer.
2.2 Risk Factors¶
Environment: The greatest risk factor for pancreatic cancer is cigarette smoking. The risk correlates with the increased number of cigarettes smoked and persists for at least 10 years following smoking cessation. Twenty-five to 30% of pancreatic cancers are believed to be caused by smoking. Exposure to cadmium as part of cigarette smoking or via exposure to welding, soldering, or dietary exposure has been weakly associated with an increased risk of pancreatic cancer. Dietary factors may contribute to risk, acknowledging confounding issues; however, high intake of fat or meat (particularly well-done barbequed meat) are risk factors. High intake of citrus fruits and vegetables are associated with a decreased risk of pancreatic cancer. Coffee and low-to-moderate alcohol consumption are not associated with an increased risk for pancreatic cancer, although consumption of sugary carbonated drinks has been associated with elevated risk. Hereditary Factors: Hereditary factors account for 10–16% of all pancreatic cancers. Family members of patients with pancreatic cancer and selected individuals with certain pathogenic germline variants should seek participation in an early detection program with genetic counseling, definition of risk, and if appropriate, periodic magnetic resonance imaging (MRI) screening and endoscopic ultrasound of the pancreas, ideally enrolled on a prospective registry.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Pancreatic cancer is the third leading cause of cancer-related mortality in the United States, with >66,000 Americans diagnosed and >51,000 dying from the disease each year. Pancreatic cancer is projected to be the second leading cause of death from cancer in the United States by 2030. Worldwide, pancreatic cancer is the eleventh most common cancer, with about half a million diagnoses per annum. Pancreatic cancer is the most lethal human cancer, with an overall 5-year survival of 13%. However, that situation is changing. In particular, (1) an enhanced understanding of the pathobiology and genomic landscape of pancreatic cancer is steadily giving rise to new therapeutic opportunities, (2) the integration of multimodality therapy for patients with localized disease has improved outcomes, and (3) increasingly more molecularly defined groups of patients are eligible for targeted therapy beyond cytotoxic therapy.
3.1 Molecular Characteristics¶
The mutational landscape of pancreatic ductal adenocarcinoma is characterized by alterations in four genes that are commonly mutated or inactivated. The most common of these is the KRAS oncogene (mutations primarily in codon 12). It is increasingly important to identify the specific mutant KRAS allele as novel drugs targeting specific alleles now exist and others are in development. KRAS mutations are seen in 90–95% of pancreatic adenocarcinomas. A subset of pancreatic cancers is termed "KRAS wildtype," where no alteration in KRAS is observed. This form of pancreatic cancer is more frequently observed in patients 90% of invasive pancreatic adenocarcinomas. TP53 is mutated in ~75% and DPC4/SMAD4 is mutated in about half of these tumors. As a reference point, the BRCA2 gene noted in Table 88-1 is mutated in 3.5–10% of pancreatic adenocarcinomas.
3.2 Precursor Lesions¶
Most pancreatic cancers are believed to arise from pancreatic intraepithelial neoplasia (PanINs), which have varying degrees of dysplasia designated as PanINs 1–3 (and constitute a progression model for pancreatic cancer). Genetic alterations become more frequent as the PanIN grade increases (e.g., grade 3). Most PanIN lesions will never progress to invasive malignancy. An alternate precursor lesion is an intraductal papillary neoplasm (IPMN), which is usually noninvasive. Unfortunately, even high-grade PanIN lesions are not detectable by currently available imaging modalities. In contrast, some pancreatic adenocarcinomas arise from noninvasive cystic epithelial precursor lesions. These lesions can be seen on magnetic resonance imaging (MRI) and computed tomography (CT) imaging, and thus detection may permit early diagnosis of pancreatic cancer. As compared to main pancreatic duct IPMN, a side branch duct IPMN is more likely to be noninvasive. MRI and endoscopic ultrasound are commonly used to assess malignant potential based on risk factors such as size, growth rate, main pancreatic duct size, and the presence of mural nodularity. One other rare pancreatic tumor is the mucinous cystic neoplasm; they may be seen as incidental findings on scans and are more common in the body and tail of the pancreas and tend to occur in women. These lesions are less likely to progress to malignancy. Clinical signs of concern include large size (>3 cm) and the presence of mural nodules and/or thickening. Even after rare progression to mucinous adenocarcinoma, they typically have a more favorable prognosis relative to typical ductal adenocarcinoma.
3.3 Location & Pathology¶
The posterior location of the pancreas in the abdomen is one of the issues that makes diagnosis more challenging. Cancers of the pancreas can be divided into neoplasms of the endocrine pancreas and those of the exocrine pancreas. The most common neoplasm of the exocrine pancreas and most lethal is ductal adenocarcinoma. These cancers arise in the head, body, or tail of the pancreas and are characterized by infiltrating desmoplastic stromal reactions. Other subtypes of nonneuroendocrine pancreatic cancers include acinar cell carcinoma (tumors of the exocrine enzyme producing cell), colloid carcinoma, medullary carcinoma, adenosquamous carcinoma, and other rare subtypes. Each of these is different in behavior and in their molecular characteristics and often requires other specific types of treatment. Occasionally, metastases to the pancreas occur secondarily to renal, breast, lung, and urothelial carcinomas, melanoma, lymphoma, and other malignancies.
4. CLINICAL FEATURES¶
A classic presentation for a patient with pancreatic cancer arising in the head of the gland is "painless" jaundice. Jaundice is visually detectable with a bilirubin of >2 mg/dL, and pruritus may also occur due to bile salt deposition in the skin. However, pain is also common in newly diagnosed patients and is typically mid epigastric (sometimes described as a "boring-like" pain) with radiation to the back (due to retroperitoneal invasion of the splanchnic nerve plexus). The pain may be exacerbated by eating or lying flat. In the presence of jaundice, light stool color from the absence of bile occurs (steatorrhea also causes malodorous stools). Other signs include the onset of diabetes (particularly with concomitant weight loss) or hyperglycemia/elevated hemoglobin A1c in the preceding 1–2 years. The association of pancreatic cancer with depression remains controversial. In addition to jaundice, physical signs of pancreatic cancer include evidence of weight loss, including loss of muscle mass, and a palpable gallbladder in the setting of biliary obstruction (Courvoisier's sign). Migratory superficial thrombophlebitis and presentation with both deep venous and arterial thromboses can occur (Trousseau's syndrome). Signs of late-stage disease include a lymph node palpable in the supraclavicular fossa (usually on the left where the thoracic duct enters the subclavian vein). This is referred to as Virchow's node. Occasionally, one can palpate subcutaneous metastases in the periumbilical area referred to as a Sister Mary Joseph's node—named after one of the operating room nurses from the Mayo Clinic who noted that when she prepped that area and felt those nodules, the patient often had peritoneal metastases. The history and symptoms noted above lead to imaging as the next step, including ultrasonography (jaundice) and CT or MRI.
4.1 Symptoms & Signs¶
History: A classic presentation for a patient with pancreatic cancer arising in the head of the gland is "painless" jaundice. Jaundice is visually detectable with a bilirubin of >2 mg/dL, and pruritus may also occur due to bile salt deposition in the skin. However, pain is also common in newly diagnosed patients and is typically mid epigastric (sometimes described as a "boring-like" pain) with radiation to the back (due to retroperitoneal invasion of the splanchnic nerve plexus). The pain may be exacerbated by eating or lying flat. In the presence of jaundice, light stool color from the absence of bile occurs (steatorrhea also causes malodorous stools). Other signs include the onset of diabetes (particularly with concomitant weight loss) or hyperglycemia/elevated hemoglobin A1c in the preceding 1–2 years. The association of pancreatic cancer with depression remains controversial.
4.2 Physical Examination Findings¶
Physical signs include evidence of weight loss, including loss of muscle mass, and a palpable gallbladder in the setting of biliary obstruction (Courvoisier's sign). Migratory superficial thrombophlebitis and presentation with both deep venous and arterial thromboses can occur (Trousseau's syndrome). Signs of late-stage disease include a lymph node palpable in the supraclavicular fossa (usually on the left where the thoracic duct enters the subclavian vein). This is referred to as Virchow's node. Occasionally, one can palpate subcutaneous metastases in the periumbilical area referred to as a Sister Mary Joseph's node—named after one of the operating room nurses from the Mayo Clinic who noted that when she prepped that area and felt those nodules, the patient often had peritoneal metastases.
5. DIFFERENTIAL DIAGNOSIS¶
The clinical presentation of pancreatic cancer often mimics other conditions. Painless jaundice in the context of pancreatic cancer must be distinguished from biliary obstruction due to choledocholithiasis (gallstones), which typically presents with pain and fever (Charcot's triad). Weight loss and epigastric pain may be seen in chronic pancreatitis, peptic ulcer disease, or gastric malignancy. New-onset diabetes or unexpected worsening of type 2 diabetes may be associated with pancreatic cancer, and research programs are evaluating screening in otherwise healthy individuals in this setting. The association of pancreatic cancer with depression remains controversial. Migratory superficial thrombophlebitis (Trousseau's syndrome) and deep venous/arterial thromboses must be distinguished from other causes of hypercoagulable states. Palpable supraclavicular lymphadenopathy (Virchow's node) suggests metastatic disease but may be seen in other malignancies. Palpable periumbilical nodules (Sister Mary Joseph's node) suggest peritoneal metastases but may be seen in other abdominal pathologies.
5.1 Painless Jaundice¶
Differential diagnosis includes choledocholithiasis, cholangiocarcinoma, ampullary carcinoma, and pancreatic head adenocarcinoma. Key distinguishing features include the presence of a palpable gallbladder (Courvoisier's sign) which suggests malignant obstruction rather than stones (unless the gallbladder is fibrotic).
5.2 Weight Loss & Epigastric Pain¶
Differential diagnosis includes chronic pancreatitis, peptic ulcer disease, gastric malignancy, and lymphoma. Key distinguishing features include the presence of steatorrhea (pancreatic insufficiency) and the specific radiation of pain to the back (retroperitoneal invasion).
6. INVESTIGATIONS & DIAGNOSIS¶
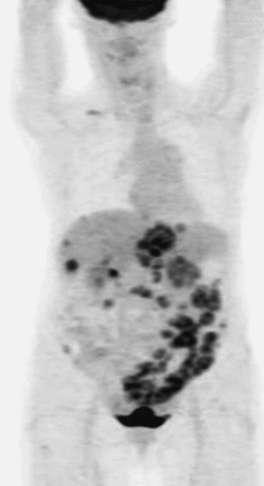
A key diagnostic tool is the use of a dual-phase contrast-enhanced CT using a pancreas cancer protocol, which allows arterial phase enhancement and portal venous phase enhancement and detailed visualization of tumor–blood vessel relationships to inform both resectability and staging. Figure 88-2 demonstrates such a CT scan (with vascular involvement). Figure 88-3 demonstrates the use of an 18F-glucose positron emission tomography (PET) scan that can aid in the detection of otherwise occult metastatic disease. A histologic (tissue) diagnosis is essential upfront and should be obtained with a Tru-Cut biopsy needle (fine-needle aspiration cytology is an acceptable but less preferred alternative). Obtaining adequate tissue not only secures a histologic/cytologic diagnosis but also facilitates molecular testing (next-generation sequencing for genomic alterations including KRAS) and microsatellite status. Increasingly subsets of patients based on genomic characterization are being identified and for whom therapies are available, making the need for adequate tissue sampling increasingly relevant to patient management. A core needle (18- to 22-gauge) biopsy can be obtained via endoscopic ultrasound-guided technique for a tumor localized to the pancreas. To biopsy the liver or a lymph node, a larger (16- to 18-gauge) percutaneous needle biopsy by an interventional radiologist is typically undertaken. Before treatment and, ideally, once the bilirubin level has normalized (biliary obstruction is associated with elevated CA19-9), a serum sample should be obtained for level of CA19-9, carcinoembryonic antigen (CEA), and CA125 (can be helpful for the 8–15% of patients with nondetectable CA19-9–Lewis antigen nonsecretors). Trends of these tumor markers over time can inform therapeutic decision-making.
6.1 Imaging¶
Imaging: A key diagnostic tool is the use of a dual-phase contrast-enhanced CT using a pancreas cancer protocol, which allows arterial phase enhancement and portal venous phase enhancement and detailed visualization of tumor–blood vessel relationships to inform both resectability and staging. Figure 88-2 demonstrates such a CT scan (with vascular involvement). Figure 88-3 demonstrates the use of an 18F-glucose positron emission tomography (PET) scan that can aid in the detection of otherwise occult metastatic disease. For optimal staging, a laparoscopy is selectively indicated either before or at the time of definitive surgery. If metastatic disease is identified at laparoscopy, curative intent surgery is not undertaken.
6.2 Histologic Diagnosis & Markers¶
Histologic Diagnosis: A histologic (tissue) diagnosis is essential upfront and should be obtained with a Tru-Cut biopsy needle (fine-needle aspiration cytology is an acceptable but less preferred alternative). Obtaining adequate tissue not only secures a histologic/cytologic diagnosis but also facilitates molecular testing (next-generation sequencing for genomic alterations including KRAS) and microsatellite status. Increasingly subsets of patients based on genomic characterization are being identified and for whom therapies are available, making the need for adequate tissue sampling increasingly relevant to patient management. A core needle (18- to 22-gauge) biopsy can be obtained via endoscopic ultrasound-guided technique for a tumor localized to the pancreas. To biopsy the liver or a lymph node, a larger (16- to 18-gauge) percutaneous needle biopsy by an interventional radiologist is typically undertaken. Serum Markers: Before treatment and, ideally, once the bilirubin level has normalized (biliary obstruction is associated with elevated CA19-9), a serum sample should be obtained for level of CA19-9, carcinoembryonic antigen (CEA), and CA125 (can be helpful for the 8–15% of patients with nondetectable CA19-9–Lewis antigen nonsecretors). Trends of these tumor markers over time can inform therapeutic decision-making.
6.3 Staging¶
Clinical Staging: The clinical staging of pancreatic cancer according to the American Joint Commission on Cancer staging is presented in Table 88-2. Table 88-3 presents another clinical way to express extent of disease as well as therapeutic approaches (to be discussed later). For optimal staging, a laparoscopy is selectively indicated either before or at the time of definitive surgery. If metastatic disease is identified at laparoscopy, curative intent surgery is not undertaken.
Table 2 — Table 88-2 Definition of Primary Tumor (T)¶
| T Category | T Criteria |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ. This includes high-grade pancreatic intraepithelial neoplasia (PanIn-3), intraductal papillary mucinous neoplasm with high-grade dysplasia, intraductal tubulopapillary neoplasm with high-grade dysplasia, and mucinous cystic neoplasm with high-grade dysplasia |
| T1 | Tumor ≤2 cm in greatest dimension |
| T1a | Tumor ≤0.5 cm in greatest dimension |
| T1b | Tumor >0.5 cm and <1 cm in greatest dimension |
| T1c | Tumor 1–2 cm in greatest dimension |
| T2 | Tumor >2 cm and ≤4 cm in greatest dimension |
| T3 | Tumor >4 cm in greatest dimension |
| T4 | Tumor involves celiac axis, superior mesenteric artery, and/or common hepatic artery, regardless of size |
Table 3 — Table 88-2 N and M Category Criteria¶
| Category | Criteria |
|---|---|
| N Category | NX: Regional lymph nodes cannot be assessed; N0: No regional lymph node metastases; N1: Metastasis in one to three regional lymph nodes; N2: Metastasis in four or more regional lymph nodes |
| M Category | M0: No distant metastasis; M1: Distant metastasis |
Table 4 — Table 88-2 AJCC Prognostic Stage Groups¶
| T Category | N Category | M Category | Stage Group |
|---|---|---|---|
| Tis | N0 | M0 | 0 |
| T1 | N0 | M0 | IA |
| T1 | N1 | M0 | IIB |
| T1 | N2 | M0 | III |
| T2 | N0 | M0 | IB |
| T2 | N1 | M0 | IIB |
| T2 | N2 | M0 | III |
| T3 | N0 | M0 | IIA |
| T3 | N1 | M0 | IIB |
| T3 | N2 | M0 | III |
| T4 | Any N | M0 | III |
| Any T | Any N | M1 | IV |
7. MANAGEMENT & TREATMENT¶
For all patients with localized pancreatic cancer, multidisciplinary evaluation should be undertaken. A standard approach for resectable disease (10–15% of patients; as defined in Table 88-3) is surgery followed by adjuvant therapy. Neoadjuvant therapy (systemic therapy prior to surgery) is an option for patients with resectable disease. The rationales for preoperative chemotherapy include the following: (1) to control micrometastatic disease; (2) to assess tumor biology and response to the selected chemotherapy regimen (this allows patients with progressive disease to avoid nontherapeutic, morbid surgery); (3) to assure delivery of systemic therapy because therapy is better tolerated in the preoperative setting and is not subject to omission of drugs or altering doses due to delayed postoperative recovery; and (4) to achieve tumor downstaging to enhance the potential for a margin-negative surgical resection. The type of surgery for patients with tumors in the pancreatic head, neck, or uncinate process is typically a pancreaticoduodenectomy with or without pylorus preservation. For tumors in the body or tail, a distal subtotal pancreatectomy and splenectomy are performed. These operations may be performed using a traditional "open" surgical technique or using minimally invasive techniques. Clinical and pathologic findings of the resection are defined as either an R0 resection (no macroscopic or microscopic disease left after surgery) or an R1 resection, which refers to microscopic residual disease at the surgical margin. An R2 resection refers to gross residual disease remaining after surgery and is a highly undesirable oncologic outcome. The best outcomes are achieved in patients with a small tumor (<2 cm), no lymph node involvement (N0), and R0 (stage I), in whom 5-year survival ranges from 50 to 90% depending on actual tumor size and grade. Overall, only a small fraction of tumors are diagnosed when stage I; however, a key goal of screening is to "stage migrate" and increase the proportion of tumors that are diagnosed as early stage I lesions. Several approaches are designed to maximize outcome for localized pancreatic cancer. Patients with metastatic pancreatic cancer may have a hypercoagulable state and frequently have thrombophlebitis (Trousseau's sign) and deep vein thrombosis with pulmonary emboli and/or more rarely arterial thrombotic events. Anticoagulation using either a direct oral anticoagulant or low-molecular-weight heparin is required in these setting in the absence of a contraindication to anticoagulation. Control of pain or of active cancer-related symptomatology including anorexia, weight loss, and malabsorption should be proactively treated. Pancreatic enzyme replacement therapy (PERT) is a critical measure to address symptoms of malabsorption, including abdominal cramping, bloating, steatorrhea, excess flatus, and weight loss. Early involvement of a supportive care team can help maximize symptom control, facilitate treatment readiness, and extend a better quality of life.
7.1 Resectable Disease¶
Designation: Resectable (localized). Median Survival: 18–23 mo. Therapeutic Approaches: Surgery followed by adjuvant therapy (mFOLFIRINOX or gemcitabine +/- capecitabine or nab-paclitaxel). Neoadjuvant chemotherapy followed by surgery. Criteria: No solid tumor contact with celiac axis, hepatic artery, or superior mesenteric artery (SMA), contact with superior mesenteric–portal veins of <180°, Patent superior mesenteric–portal veins, No extrapancreatic disease.
Table 5 — Table 88-3 Extent of Disease and Therapeutic Approach (Resectable)¶
| Designation | Median Survival | Therapeutic Approaches |
|---|---|---|
| Resectable (localized) | 18–23 mo | Surgery followed by adjuvant therapy (mFOLFIRINOX or gemcitabine +/- capecitabine or nab-paclitaxel); Neoadjuvant chemotherapy followed by surgery |
7.2 Locally Advanced Disease¶
Designation: Locally advanced. Median Survival: 6–18 mo. Therapeutic Approaches: Chemotherapy +/- radiation. Criteria: Arterial involvement of >180° (superior mesenteric artery, others); Venous occlusion (superior mesenteric vein [SMV] or portal); No extrapancreatic disease. Typical treatment paradigms for locally advanced disease include systemic chemotherapy with or without radiation therapy. A proportion of patients with locally advanced disease (~20%) may be rendered operable following neoadjuvant therapy.
Table 6 — Table 88-3 Extent of Disease and Therapeutic Approach (Locally Advanced)¶
| Designation | Median Survival | Therapeutic Approaches |
|---|---|---|
| Locally advanced | 6–18 mo | Chemotherapy +/- radiation |
7.3 Metastatic Disease¶
Designation: Metastatic. Median Survival: 6–12 mo. Therapeutic Approaches: Chemotherapy with special consideration for tumors with specific targets (e.g., mismatch repair high, BRCA1/2, BRAF, etc.). The mainstay of treatment for metastatic pancreatic cancer is systemic chemotherapy. Several treatment regimens including FOLFIRINOX, gemcitabine, albumin-bound paclitaxel, and, more recently, NALIFIRINOX (nanoliposomal irinotecan, 5-fluorouracil, leucovorin, oxaliplatin; NAPOLI-3) have all demonstrated a survival advantage compared to prior standards in untreated metastatic pancreatic cancer. In a previously treated setting, liposomal irinotecan and infusional 5-fluorouracil and leucovorin (NAPOLI-1) regimen has been shown to improve survival. Predictors of outcome in the metastatic setting include good physical functioning (performance status), favorable nutritional status, the absence of liver metastases, lung-only metastases, and the presence of select pathogenic germline variants. Table 88-4 details combination regimens that have further improved survival modestly. Median overall survival ranges from 6 to 12 months. However, 1-year survival is improving, with subsets of patients whose survival with metastatic disease can reach a couple of years or longer.
Table 7 — Table 88-3 Extent of Disease and Therapeutic Approach (Metastatic)¶
| Designation | Median Survival | Therapeutic Approaches |
|---|---|---|
| Metastatic | 6–12 mo | Chemotherapy with special consideration for tumors with specific targets (e.g., mismatch repair high, BRCA1/2, BRAF, etc.) |
7.4 Adjuvant Therapy¶
A standard of care is 24 weeks of adjuvant treatment with the modified FOLFIRINOX regimen (folinic acid, 5-fluorouracil, irinotecan, oxaliplatin). The median survival was 54 months for modified FOLFIRINOX compared to 35 months for gemcitabine alone (hazard ratio [HR] 0.64; 95% confidence interval [CI] 0.48–0.86; p = .003) in the definitive trial supporting this therapy. Main side effects included fatigue, gastrointestinal toxicity, myelosuppression, and neuropathy.
7.5 Neoadjuvant Therapy¶
Neoadjuvant therapy is the standard approach for patients with borderline resectable or locally advanced disease. The rationales for preoperative chemotherapy include the following: (1) to control micrometastatic disease; (2) to assess tumor biology and response to the selected chemotherapy regimen (this allows patients with progressive disease to avoid nontherapeutic, morbid surgery); (3) to assure delivery of systemic therapy because therapy is better tolerated in the preoperative setting and is not subject to omission of drugs or altering doses due to delayed postoperative recovery; and (4) to achieve tumor downstaging to enhance the potential for a margin-negative surgical resection.
7.6 Molecularly Targeted Therapy¶
PARP inhibitors have activity in patients with pathogenic germline or somatic (tumor-based) BRCA2, BRCA1, or PALB2 (i.e., defective DNA repair proteins) variants. In addition, these tumors might be more sensitive to specific combinations of chemotherapy that include platinum agents (gemcitabine and cisplatin or FOLFIRINOX). About 1% of pancreatic cancers have microsatellite instability, typically with high numbers of mutations in their tumors, and these tumors are likely to benefit from immune checkpoint blockade with anti-PD-1 (pembrolizumab, nivolumab) and anti-CTLA-4 inhibitors. KRAS mutations occur ubiquitously in pancreatic cancer. Current treatment guidelines include drugs targeting KRAS G12C (~1% of pancreatic cancers).
7.7 Supportive Care¶
Control of pain or of active cancer-related symptomatology including anorexia, weight loss, and malabsorption should be proactively treated. Pancreatic enzyme replacement therapy (PERT) is a critical measure to address symptoms of malabsorption, including abdominal cramping, bloating, steatorrhea, excess flatus, and weight loss. Early involvement of a supportive care team can help maximize symptom control, facilitate treatment readiness, and extend a better quality of life. Patients with metastatic pancreatic cancer may have a hypercoagulable state and frequently have thrombophlebitis (Trousseau's sign) and deep vein thrombosis with pulmonary emboli and/or more rarely arterial thrombotic events. Anticoagulation using either a direct oral anticoagulant or low-molecular-weight heparin is required in these setting in the absence of a contraindication to anticoagulation.
8. PROGNOSIS & COMPLICATIONS¶
The best outcomes are achieved in patients with a small tumor (180° and/or venous contact that does not permit resection/reconstruction), the median survival is poor (6–18 months). Complications from local disease progression can be significant and include pain, biliary and duodenal obstruction, vascular thromboses, varices, bleeding, and infection/sepsis. The mainstay of treatment for metastatic pancreatic cancer is systemic chemotherapy. Median overall survival ranges from 6 to 12 months. However, 1-year survival is improving, with subsets of patients whose survival with metastatic disease can reach a couple of years or longer. Patients with metastatic pancreatic cancer may have a hypercoagulable state and frequently have thrombophlebitis (Trousseau's sign) and deep vein thrombosis with pulmonary emboli and/or more rarely arterial thrombotic events.
8.1 Survival by Stage¶
Localized: 5-year survival about 44%. Regional: 5-year survival 16%. Metastatic: 5-year survival 3.2%. Overall 5-year survival: 13%. Resectable disease median survival: 18–23 mo. Locally advanced disease median survival: 6–18 mo. Metastatic disease median survival: 6–12 mo.
8.2 Complications¶
Local disease progression complications: Pain, biliary and duodenal obstruction, vascular thromboses, varices, bleeding, and infection/sepsis. Hypercoagulable state: Thrombophlebitis (Trousseau's sign), deep vein thrombosis with pulmonary emboli, arterial thrombotic events. Malabsorption: Abdominal cramping, bloating, steatorrhea, excess flatus, weight loss (addressed with PERT).
9. SPECIAL CONSIDERATIONS¶
Screening: For an average-risk individual (without any known predisposing factors), there is currently no recommended screening. Knowing that an individual carries a BRCA1/2 or PALB2 germline variant or any of the above mutations requires referral of that person to an early detection or high-risk screening clinic. For patients with a BRCA1/2 or PALB2 pathogenic germline variant, a poly(ADP-ribose) polymerase (PARP) inhibitor should be considered as part of treatment for metastatic pancreatic cancer. Other pathogenic germline variants are under study to determine their increased risk of pancreatic cancer, including CFTR, PRSS2, CDK4, FANCC, APC, ATM, BRIP1, BRCA1, EPCAM, MEN1, MLH1, MSH2, MSH6, NF1, PMS2, SMAD4, TP53, TSC1, TSC2, and VHL. Some of these variants are also associated with pancreatic neuroendocrine tumors. In addition to recognized genetic syndromes from single gene variants, other individuals without any of these identifiable germline variants may be at higher risk for this cancer. For example, a family history of pancreatic cancer is associated with increased risk based on the number of affected relatives. Having one first-degree relative with pancreatic cancer, one's risk for developing the disease is increased 4.6-fold, having two first-degree relatives increases the risk 6.4-fold, and three or more first-degree relatives confers a 32-fold increased risk. The risk is increased if a relative developed pancreatic cancer at <55 years old and is further compounded by smoking. Hereditary factors account for 10–16% of all pancreatic cancers. Family members of patients with pancreatic cancer and selected individuals with certain pathogenic germline variants should seek participation in an early detection program with genetic counseling, definition of risk, and if appropriate, periodic magnetic resonance imaging (MRI) screening and endoscopic ultrasound of the pancreas, ideally enrolled on a prospective registry.
9.1 Genetic Risk & Screening¶
Germline Variants: BRCA2, p16/CDKN2A, PRSS1 or SPIN11b, STK11 (LKB1), ATM, MLH1, MSH2, MSH6, PMS2. Syndromes: Familial breast/ovarian cancer, Familial atypical multiple mole melanoma (FAMMM), Peutz-Jeghers syndrome, Hereditary (familial) pancreatitis, Ataxia-telangiectasia, Hereditary nonpolyposis colorectal syndrome or Lynch syndrome. Risk: BRCA2 (3.5–10 fold), p16/CDKN2A (15–22 fold), PRSS1/SPIN11b (53 fold), STK11 (76–140 fold), ATM (6 fold), MLH1/MSH2/MSH6/PMS2 (9–36 fold). Screening: Periodic MRI and endoscopic ultrasound for high-risk individuals. Average-risk: No recommended screening.
9.2 Molecular Profile Considerations¶
KRAS: Mutations in 90–95% of pancreatic adenocarcinomas. Targeted therapy: Drugs targeting KRAS G12C (~1% of pancreatic cancers). BRCA1/2/PALB2: PARP inhibitors. MSI-High: Immune checkpoint blockade (anti-PD-1, anti-CTLA-4). BRAF: Targetable fusions (NRG-1, NTRK1-3).
10. KEY PEARLS & CLINICAL TRAPS¶
Board-exam favorites, common diagnostic pitfalls, must-not-miss diagnoses, useful mnemonics. Pancreatic cancer is the third leading cause of cancer-related mortality in the United States. Painless jaundice is a classic presentation for pancreatic cancer arising in the head of the gland. A palpable gallbladder in the setting of biliary obstruction is Courvoisier's sign. Migratory superficial thrombophlebitis is Trousseau's syndrome. A lymph node palpable in the supraclavicular fossa is Virchow's node. Subcutaneous metastases in the periumbilical area is a Sister Mary Joseph's node. High BMI (≥30) is associated with a doubling of pancreatic cancer risk. Cigarette smoking is the greatest risk factor, believed to cause 25 to 30% of pancreatic cancers. CA19-9 is nondetectable in Lewis antigen non-secretors. Modified FOLFIRINOX is the standard adjuvant therapy with median survival of 54 months compared to 35 months for gemcitabine alone. Neoadjuvant therapy is the standard approach for borderline resectable or locally advanced disease.
10.1 Diagnostic Clues¶
Painless jaundice with bilirubin >2 mg/dL. Pruritus due to bile salt deposition. Mid epigastric pain radiating to the back. Light stool color (steatorrhea). Palpable gallbladder (Courvoisier's sign). Migratory superficial thrombophlebitis (Trousseau's syndrome). Supraclavicular lymphadenopathy (Virchow's node). Periumbilical nodules (Sister Mary Joseph's node).
10.2 Exclusion Criteria¶
CA19-9 is nondetectable in Lewis antigen non-secretors. This makes the diagnosis of pancreatic cancer using CA19-9 as a marker unlikely in this subgroup. Other causes of jaundice (choledocholithiasis) typically present with pain and fever (Charcot's triad) rather than painless jaundice.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 88-1 A. Note the relationship of the pancreas to the major vessels of the stromal component (white arrows). (Part A is courtesy of Mary Kay Washington, MD, Genomics Research Institute [TGen].) — Figure 88-1A: Anatomical relationship of the pancreas to the major vessels of the retroperitoneum, including the splenic artery, hepatic artery, portal vein, common bile duct, superior mesenteric artery, and superior mesenteric vein.
Figure 2¶

Caption: FIGURE 88-1 A. Note the relationship of the pancreas to the major vessels of the stromal component (white arrows). (Part A is courtesy of Mary Kay Washington, MD, Genomics Research Institute [TGen].) — Figure 88-1B: Histology of ductal adenocarcinoma of the pancreas showing the tumor (black arrows) with an intense stromal component (white arrows).
Figure 3¶
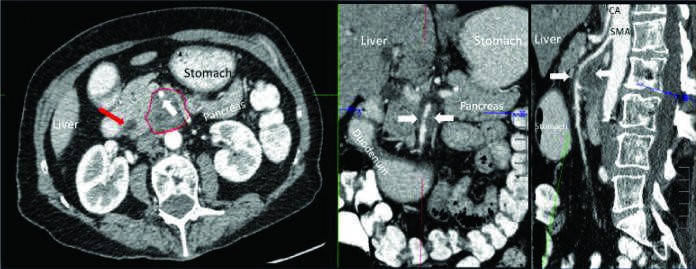
Caption: Pancreatic Cancer FIGURE 88-2 Selected images from contrast-enhanced computed tomography (CT) in patients with locally advanced adenocarcinoma of the pancreas. A high-quality contrast-enhanced CT scan (arterial phase in panels A–C and portal venous phase in panels D–F) is required for optimal staging of pancreas cancer. Panel A demonstrates the typical features of adenocarcinoma of the pancreas on arterial phase axial CT scans (dotted outline) with tumor encasement of the superior mesenteric artery (white arrow). Note the dilatation of the common bile duct (red arrow). Panels B (magnified coronal) and C (sagittal) show reconstruction of CT images into additional orthogonal planes with exquisite details to confirm the unresectable nature of the tumor due to vascular encasement. Panel D demonstrates the typical features of adenocarcinoma of the pancreas on portal venous phase axial CT scans in a different subject. The dotted line outlines a pancreas cancer lesion in the pancreatic head, which is encasing the portal splenic confluence (dotted outline). Panels E (white arrow) and F show the pinched appearance of the portal splenic confluence by tumor abutment and invasion of the superior mesenteric vein (white arrow) on coronal and sagittal views. Note the presence of a stent in the common bile duct (red arrow) to help relieve biliary obstruction caused by the tumor. CA, celiac axis; SMA, superior mesenteric artery. ■ CLINICAL FEATURES arterial phase enhancement and portal venous phase enhancement and — Figure 88-2A: Contrast-enhanced CT scan (arterial phase) demonstrating typical features of adenocarcinoma of the pancreas with tumor encasement of the superior mesenteric artery and dilatation of the common bile duct.
Figure 4¶

Caption: Pancreatic Cancer FIGURE 88-2 Selected images from contrast-enhanced computed tomography (CT) in patients with locally advanced adenocarcinoma of the pancreas. A high-quality contrast-enhanced CT scan (arterial phase in panels A–C and portal venous phase in panels D–F) is required for optimal staging of pancreas cancer. Panel A demonstrates the typical features of adenocarcinoma of the pancreas on arterial phase axial CT scans (dotted outline) with tumor encasement of the superior mesenteric artery (white arrow). Note the dilatation of the common bile duct (red arrow). Panels B (magnified coronal) and C (sagittal) show reconstruction of CT images into additional orthogonal planes with exquisite details to confirm the unresectable nature of the tumor due to vascular encasement. Panel D demonstrates the typical features of adenocarcinoma of the pancreas on portal venous phase axial CT scans in a different subject. The dotted line outlines a pancreas cancer lesion in the pancreatic head, which is encasing the portal splenic confluence (dotted outline). Panels E (white arrow) and F show the pinched appearance of the portal splenic confluence by tumor abutment and invasion of the superior mesenteric vein (white arrow) on coronal and sagittal views. Note the presence of a stent in the common bile duct (red arrow) to help relieve biliary obstruction caused by the tumor. CA, celiac axis; SMA, superior mesenteric artery. ■ CLINICAL FEATURES arterial phase enhancement and portal venous phase enhancement and — Figure 88-2D: Contrast-enhanced CT scan (portal venous phase) demonstrating a pancreas cancer lesion in the pancreatic head encasing the portal splenic confluence.
Figure 5¶
Caption: Pancreatic Cancer FIGURE 88-2 Selected images from contrast-enhanced computed tomography (CT) in patients with locally advanced adenocarcinoma of the pancreas. A high-quality contrast-enhanced CT scan (arterial phase in panels A–C and portal venous phase in panels D–F) is required for optimal staging of pancreas cancer. Panel A demonstrates the typical features of adenocarcinoma of the pancreas on arterial phase axial CT scans (dotted outline) with tumor encasement of the superior mesenteric artery (white arrow). Note the dilatation of the common bile duct (red arrow). Panels B (magnified coronal) and C (sagittal) show reconstruction of CT images into additional orthogonal planes with exquisite details to confirm the unresectable nature of the tumor due to vascular encasement. Panel D demonstrates the typical features of adenocarcinoma of the pancreas on portal venous phase axial CT scans in a different subject. The dotted line outlines a pancreas cancer lesion in the pancreatic head, which is encasing the portal splenic confluence (dotted outline). Panels E (white arrow) and F show the pinched appearance of the portal splenic confluence by tumor abutment and invasion of the superior mesenteric vein (white arrow) on coronal and sagittal views. Note the presence of a stent in the common bile duct (red arrow) to help relieve biliary obstruction caused by the tumor. CA, celiac axis; SMA, superior mesenteric artery. ■ CLINICAL FEATURES arterial phase enhancement and portal venous phase enhancement and — Figure 88-2E/F: Coronal and sagittal CT views showing the pinched appearance of the portal splenic confluence by tumor abutment and invasion of the superior mesenteric vein.
Figure 6¶

Caption: Pancreatic Cancer FIGURE 88-2 Selected images from contrast-enhanced computed tomography (CT) in patients with locally advanced adenocarcinoma of the pancreas. A high-quality contrast-enhanced CT scan (arterial phase in panels A–C and portal venous phase in panels D–F) is required for optimal staging of pancreas cancer. Panel A demonstrates the typical features of adenocarcinoma of the pancreas on arterial phase axial CT scans (dotted outline) with tumor encasement of the superior mesenteric artery (white arrow). Note the dilatation of the common bile duct (red arrow). Panels B (magnified coronal) and C (sagittal) show reconstruction of CT images into additional orthogonal planes with exquisite details to confirm the unresectable nature of the tumor due to vascular encasement. Panel D demonstrates the typical features of adenocarcinoma of the pancreas on portal venous phase axial CT scans in a different subject. The dotted line outlines a pancreas cancer lesion in the pancreatic head, which is encasing the portal splenic confluence (dotted outline). Panels E (white arrow) and F show the pinched appearance of the portal splenic confluence by tumor abutment and invasion of the superior mesenteric vein (white arrow) on coronal and sagittal views. Note the presence of a stent in the common bile duct (red arrow) to help relieve biliary obstruction caused by the tumor. CA, celiac axis; SMA, superior mesenteric artery. ■ CLINICAL FEATURES arterial phase enhancement and portal venous phase enhancement and — Figure 88-3: Positron emission tomography (PET) scan demonstrating metastatic disease at baseline and partial resolution of liver metastases after 6 weeks of chemotherapy.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.