Kidney Transplantation¶
Chapter 325 | Part 9: Disorders of the Kidney and Urinary Tract · Part 9 – Renal & Urinary Tract Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- 1-year allograft survival rates in the US: Living donor 98%, Deceased donor 93%.
- Kidney Donor Profile Index (KDPI) <20% allocated to recipients with highest expected posttransplant survival.
- Absolute contraindications: Active malignancy, active infection, psychosocial issues affecting adherence, chronic illness limiting survival <2 years.
- Induction therapy: Antithymocyte globulin (ATG) for high-risk/sensitized; Basiliximab for low-risk.
- Maintenance regimen: Calcineurin inhibitor (Tacrolimus/Cyclosporine) + Antimetabolite (Mycophenolate/Azathioprine) + Steroids.
- Antibody-mediated rejection hallmark: C4d deposition in peritubular capillaries + circulating donor-specific antibody.
- CMV prophylaxis: Valganciclovir for seronegative recipients of seropositive donors.
- Chronic allograft dysfunction causes: Chronic active antibody-mediated rejection, recurrent glomerular disease, hypertension, CNI nephrotoxicity.
- Malignancy incidence in transplant recipients: 5–6% (approx. 100x general population).
- DCD kidneys (Non-Heart-Beating Donors): Survival not shown to be inferior to deceased-donor kidneys from categories III and IV.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Historical Context & Current Status
- 1.2 Recent Activity & Results
- 2. EPIDEMIOLOGY
- 2.1 Survival Rates
- 2.2 Risk Factors
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Immunology of Rejection
- 3.2 Mechanisms of Chronic Lesions
- 4. CLINICAL FEATURES
- 4.1 Signs & Symptoms of Rejection
- 4.2 Signs & Symptoms of Infection
- 4.3 Signs & Symptoms of Malignancy
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Rejection vs. Toxicity vs. Recurrence
- 5.2 Infection Differential
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Donor Evaluation
- 6.2 Diagnostic Criteria & Algorithms
- 7. MANAGEMENT & TREATMENT
- 7.1 Induction Therapy
- 7.2 Maintenance Therapy
- 7.3 Treatment of Rejection
- 7.4 Management of Infection
- 7.5 Management of Chronic Complications
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Causes of Death
- 8.2 Chronic Allograft Dysfunction
- 9. SPECIAL CONSIDERATIONS
- 9.1 Living-Donor Evaluation
- 9.2 Deceased-Donor Evaluation
- 9.3 Clinical Course & Management
- 10. KEY PEARLS & CLINICAL TRAPS
- 10.1 Diagnostic Clues
- 10.2 Exclusion Criteria
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | CHAPTER 325 OF THE RECIPIENT tion agent is used |
| 1 | 🖼 Figure | Recognition pathways for major histocompatibility complex (MHC) receptors that bind to specific... |
1. DEFINITION & OVERVIEW¶
Kidney transplantation is the treatment of choice for patients with end-stage kidney disease (ESKD). It involves the surgical placement of a donor kidney into the recipient to restore renal function. The procedure has evolved from identical twin transplants in 1954 to complex organ sharing and xenotransplantation research. Current 1-year survival rates for living-donor and deceased-donor allografts are 98% and 93%, respectively, in the United States.
1.1 Historical Context & Current Status¶
- First successful kidney transplant performed in Boston in 1954 between identical twins.
- Introduction of immunosuppressive therapies (azathioprine, prednisone) in 1960s established transplantation across nonidentical individuals (allografts).
- 1970s and 1980s: Success rate at 1-year mark markedly improved after introduction of calcineurin inhibitors.
- Current 1-year survival rates: Living-donor 98%, Deceased-donor 93%.
- Long-term survival has not improved as much over time; average allograft survival time is 19 years for living-donor and 12 years for deceased-donor grafts.
- Age-related mortality rates after transplantation are highest in the first year due to surgical risks: 2% for ages 18–34 years, 3% for ages 35–49 years, and 6.8% for ages ≥50–60 years.
- Despite age-related risks, actual survival benefit of transplantation compared to chronic dialysis becomes apparent within days to months following transplantation.
1.2 Recent Activity & Results¶
- In 2022: >19,000 deceased-donor kidney transplants and approximately 6000 living-donor transplants performed in the United States.
- Ratio of deceased-donor to living-donor transplants remaining stable over past few years.
- As of 2022: Nearly 139,000 adult kidney transplant candidates on the waiting list, with 25,000 patients being transplanted yearly.
- New allocation system implemented in 2014 in the United States to offer opportunity for transplantation to patients highly sensitized while allowing patients expected to survive longest to receive best-quality deceased donor organs.
- Kidney Donor Profile Index (KDPI) score ranges from 0 to 100% to estimate potential risk of graft failure after kidney transplant based on 10 donor factors.
- KDPI 85% kidneys (previously expanded criteria donor [ECD]) directed toward patients expected to fare less well on dialysis.
- 2021 new distance-based kidney allocation policy: Deceased-donor kidneys offered first to candidates listed at transplant hospitals within 250 nautical miles.
- Donor pool expansion strategies: Use of kidneys from donors after cardiac death (DCD) now commonly used, consisting of 30% of total deceased kidney transplants.
- HCV-positive donors to HCV-positive or -negative recipients: Practice becoming more common since 2017, consisting of 9% of deceased kidney transplants.
- HOPE Act: Authorized organ donation from HIV-positive candidates; >100 transplants performed.
- Blood group B candidates: Eligible for allograft from A blood type donors if low anti-A titer, helping reduce wait time disparities for African-American ESKD population.
- Xenotransplantation: Experimental kidney transplants into brain-dead recipients performed in 2022 using genetically engineered pigs; issues include xenoimmunity, transmission of zoonosis, and ethical challenges.
2. EPIDEMIOLOGY¶
Kidney transplantation is performed worldwide with tens of thousands of transplants annually. In the United States, >220,000 patients are living with a functioning kidney transplant. The incidence of malignancy in patients on immunosuppressive therapy is 5–6%, or approximately 100 times greater than that in the general population. Cardiovascular events (29%), infection (18%), and malignancy (17%) are the major causes of death in kidney transplant recipients.
2.1 Survival Rates¶
- 1-Year Follow-Up: Deceased donor grafts 94%, Patients 95%; Living donor grafts 98%, Patients 99%.
- 5-Year Follow-Up: Deceased donor grafts 76%, Patients 77%; Living donor grafts 87%, Patients 87%.
- 10-Year Follow-Up: Deceased donor grafts 54%, Patients 67%; Living donor grafts 70%, Patients 83%.
- Allograft survival is higher for living-donor recipients at 1-year mark, likely related to less ischemic injury.
- At 5- and 10-year follow-up, steeper decline in survival of those with deceased-donor kidneys remains.
2.2 Risk Factors¶
- Non-modifiable: Age, race (African-American ESKD population has higher prevalence of blood type B), genetic factors (APOL1 risk alleles).
- Modifiable: Diabetes, cardiovascular status, hypertension, obesity, active substance abuse, psychosocial issues affecting adherence.
- Donor factors: Elderly donor, acute kidney injury, prolonged ischemia, high KDPI score.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
The pathogenesis of allograft loss due to chronic process consists of interstitial fibrosis, tubular atrophy, vasculopathy, and glomerulopathy. This is likely a combination of an alloimmune response, drug toxicity, and the result of a variety of other insults. Rejection mechanisms involve T cell–mediated and antibody-mediated effector mechanisms. Immunosuppressive agents suppress all immune responses nonspecifically, including those to exogenous pathogens and malignant tumors.
3.1 Immunology of Rejection¶
- T cell–mediated rejection: Caused by recipient T lymphocytes responding to donor HLA antigens expressed within the transplanted MHC II.
- CD4+ lymphocytes respond to class II (HLA-DR) incompatibility by proliferating and releasing proinflammatory cytokines.
- CD8+ cytotoxic lymphocytes respond primarily to class I (HLA-A, -B) antigens and mature into cytotoxic effector cells causing organ damage through direct contact and lysis.
- Full T-cell activation requires T-cell receptor binding to alloantigens and engagement of costimulatory molecules (CD28 on T cells and CD80/CD86 on antigen-presenting cells).
- Antibody-mediated rejection: Caused by circulating antibodies against donor antigens. Donor-derived antigens delivered to recipient's draining lymph nodes activate alloimmune response.
- Follicular helper T cells (Tfh) activated and promote differentiation of B cells into antibody-secreting plasma cells.
- Plasma cells produce donor-targeting antibodies against HLA and non-HLA antigens, depositing in allograft kidney and causing injury via complement-dependent and independent mechanisms.
- C4d deposition in peritubular capillaries and glomerular basement membrane is a footprint of complement activation and diagnostic criterion of antibody-mediated rejection.
- Non-HLA minor antigens: Relatively weak initially, suppressible by conventional immunosuppressive therapy unless prior exposure/priming occurred.
- Eplet matching: Short sequences of polymorphic amino acids on surface of HLA antigens recognized by HLA antibodies; eplet mismatches in class II HLA DQ loci are important risk factors for acute rejection.
3.2 Mechanisms of Chronic Lesions¶
- Chronic renal transplant dysfunction caused by chronic active antibody-mediated rejection, recurrent glomerular disease, hypertension, CNI nephrotoxicity, secondary focal glomerulosclerosis, or combination of these pathophysiologies.
- Chronic vascular changes: Intimal proliferation and medial hypertrophy.
- Control of systemic and intrarenal hypertension with calcium channel blockers thought to have beneficial influence on rate of progression of chronic allograft dysfunction.
- CNI nephrotoxicity: Nephrotoxicity presents a serious management problem; drug levels should be monitored.
- Recurrent glomerular disease: Kidney allograft biopsy can distinguish subacute cellular rejection from recurrent disease or secondary focal sclerosis.
4. CLINICAL FEATURES¶
Early diagnosis of rejection allows prompt institution of therapy to preserve allograft function and prevent irreversible damage. Clinical evidence of rejection is rarely characterized by fever, swelling, and tenderness over the allograft. Rejection may present only with a rise in serum creatinine, with or without a reduction in urine volume. The focus should be on ruling out other causes of functional deterioration, such as acute tubular injury, calcineurin toxicity, BK nephropathy, and recurrent glomerular diseases.
4.1 Signs & Symptoms of Rejection¶
- Rise in serum creatinine.
- Reduction in urine volume.
- Rarely: Fever, swelling, tenderness over the allograft.
- Postoperative diuresis: Large amounts of sodium, potassium, and water may be lost postoperatively due to acute tubular injury from ischemia.
- Slow recovery or oliguria: Should prompt allograft biopsy because superimposition of rejection on acute tubular injury is common and difficult to distinguish without biopsy.
4.2 Signs & Symptoms of Infection¶
- Signs and symptoms of infection may be atypical due to immunosuppression.
- Opportunistic infections should be considered based on clinical presentation.
- CMV infection: Presentation varies from asymptomatic CMV viremia to systemic syndrome (fever, leukopenia) and tissue-specific manifestation (hepatitis, gastroenteritis, retinopathy).
- Pneumocystis jirovecii: Rare but critical opportunistic infection; aggressive diagnostic procedures including transbronchial and open-lung biopsy frequently indicated.
- Tissue-invasive fungal infections: Require treatment with systemic agents such as fluconazole or newer antifungal agents.
- Aspergillus, Nocardia, Candida: Specific treatments required.
4.3 Signs & Symptoms of Malignancy¶
- Incidence of tumors in patients on immunosuppressive therapy is 5–6%.
- Approximately 100 times greater than that in the general population.
- Major causes of death: Cardiovascular events (29%), infection (18%), malignancy (17%).
5. DIFFERENTIAL DIAGNOSIS¶
The focus should be on ruling out other causes of functional deterioration when rejection is suspected. Differential diagnosis includes acute tubular injury, calcineurin toxicity, BK nephropathy, and recurrent glomerular diseases. Allograft biopsy is the gold standard for diagnosis of acute T cell–mediated and antibody-mediated rejection. Diagnostic measures such as culture (blood, urine, drain fluids), viral load in plasma, and imaging (allograft ultrasound and computed tomography [CT]) should be obtained for infection workup.
5.1 Rejection vs. Toxicity vs. Recurrence¶
- Acute T cell–mediated rejection: Diagnosed by presence of immune cell infiltration in interstitial, tubular, or vascular compartments according to Banff classification.
- Antibody-mediated rejection: Evidence present when endothelial injury and deposition of complement component C4d is detected in peritubular capillaries, accompanied by detection of circulating donor-specific antibody.
- Calcineurin toxicity: Presents as functional deterioration; drug levels should be monitored.
- BK nephropathy: Reactivation of BK virus in setting of immunosuppression; renal biopsy useful for examining interstitial nephritis, tubular cytopathic changes of BK nephropathy, and viral antigens.
- Recurrent glomerular disease: Kidney allograft biopsy can distinguish subacute cellular rejection from recurrent disease or secondary focal sclerosis.
5.2 Infection Differential¶
- Pneumocystis jirovecii: Critical opportunistic infection.
- CMV: Serious complication after kidney transplantation associated with increased morbidity and mortality.
- Fungal infections: Tissue-invasive fungal infections require treatment with systemic agents.
- Bacterial infections: Nocardia, Candida, Aspergillus.
6. INVESTIGATIONS & DIAGNOSIS¶
Recipient evaluation is critical in identifying patients at risk. It involves a multidisciplinary approach requiring thorough medical, surgical, social, and psychosocial evaluations. Cardiovascular risk assessment is crucial during perioperative and postoperative periods. Diagnostic ultrasound is helpful in identifying urinary obstruction or presence of perirenal collections of urine (urinoma), blood (hematoma), or lymph (lymphocele). Doppler ultrasonography is useful in ascertaining changes in allograft vasculature and blood flow. Allograft biopsy is the gold standard for diagnosis of acute T cell–mediated and antibody-mediated rejection.
6.1 Donor Evaluation¶
- Living-donor evaluation: Basic principle of 'first, do no harm' important. Donor evaluation must take every effort to exclude any medical conditions that may cause morbidity and mortality after kidney donation, such as hypertension, diabetes, and/or proteinuria.
- Risk of ESKD after kidney donation: Not greater than that of general population, but absolute donation associated with small but significant potential lifetime risk of ESKD (0.3–0.4%).
- Mechanism of premature renal failure: Increased blood flow and hyperfiltration injury in remaining kidney.
- Deceased-donor evaluation: Should be free of malignant neoplastic disease, hepatitis, and HIV owing to possible transmission to recipient.
- Ischemic time: Generally, an ischemic time of <24 h is preferred.
- Tissue typing: Molecular typing of HLA by genomic sequencing almost universally used.
- Cross-matching: Positive cytotoxic crossmatch of recipient serum with donor T lymphocytes indicates presence of preformed donor-specific anti-HLA class I antibodies and is usually predictive of hyperacute rejection.
- Flow cytometric crossmatch: Detects presence of anti-HLA IgG on antibodies not necessarily detected on cytotoxic crossmatch; may not be absolute contraindication.
6.2 Diagnostic Criteria & Algorithms¶
- KDPI Score: Ranges from 0 to 100% to estimate potential risk of graft failure after kidney transplant based on 10 donor factors.
- KDPI 85%: Directed toward patients expected to fare less well on dialysis.
- DCD Categories: I (Brought in dead), II (Unsuccessful resuscitation), III (Awaiting cardiac arrest), IV (Cardiac arrest after brainstem death), V (Cardiac arrest in a hospital patient).
- DCD Usage: Kidneys can be used for transplantation from categories II–V but are commonly only used from categories III and IV.
- Posttransplant Management Algorithm: High-risk recipients (high %PRA, prior transplant, autoimmune GN, donor cold ischemia >24h, donor age >60, high KDPI) receive Antithymocyte globulin induction. Low-risk recipients (PRA <10%, first transplant, donor age 15–35, cold ischemia <12h, low KDPI) receive Basiliximab induction.
- Rejection Management: If kidney function remains inadequate or low, allograft biopsy indicated. If no rejection, adjust CNI dose. If acute rejection, IV steroid (methylprednisolone 0.5–1 g/d × 3 days) or antithymocyte globulin.
7. MANAGEMENT & TREATMENT¶
Kidney transplant recipients need to take immunosuppressive drugs for life, except identical twins or simultaneous bone marrow–kidney transplant recipients. Immunosuppressive agents are divided into induction and maintenance agents. Induction therapy is given to most kidney transplant recipients in the United States at the time of transplant to reduce risk of early acute rejection and to minimize or eliminate use of either steroids or calcineurin inhibitors and their associated toxicities. Maintenance therapy typically consists of a calcineurin inhibitor (CNI), usually tacrolimus, and an antimetabolite, usually mycophenolic acid, with or without early steroid withdrawal.
7.1 Induction Therapy¶
- Depleting Agents: Antithymocyte globulin (ATG) is a lymphocyte-depleting agent. Peripheral human lymphocytes, thymocytes, or lymphocytes from spleens or thoracic duct fistulas are injected into horses or rabbits to produce antilymphocyte serum, from which the immunoglobulin fraction is then separated.
- Monoclonal antibodies: Alemtuzumab directed against CD52, widely expressed on immune cells such as B and T cells, natural killer cells, macrophages, and some granulocytes.
- Nondepleting Agents: Target 55-kDa alpha chain of IL-2 receptor, expressed only on activated T cells. Used as prophylaxis for (but not treatment of) acute rejection in immediate posttransplant period.
- Steroids: Methylprednisolone 250–500 mg given immediately before or at time of transplantation, dose tapered to 20 mg within a week. Most patients whose renal function is stable after 6 months or a year do not require large doses of prednisone; maintenance doses of 5–10 mg per day are the rule.
- Basiliximab: Used for low-risk recipients.
7.2 Maintenance Therapy¶
- Glucocorticoids: Prednisone/prednisolone. Mechanism: Binds cytosolic receptors and heat shock proteins. Blocks transcription of IL-1, -2, -3, -6, TNF-α, and IFN-γ. Side effects: Hypertension, glucose intolerance, dyslipidemia, osteoporosis.
- Cyclosporine (CsA): Lipid-soluble polypeptide. Mechanism: Trimolecular complex with cyclophilin and calcineurin → block in cytokine (e.g., IL-2) production; however, stimulates TGF-β production. Side effects: Nephrotoxicity, hypertension, dyslipidemia, glucose intolerance, hirsutism/hyperplasia of gums.
- Tacrolimus: Macrolide, well absorbed. Mechanism: Trimolecular complex with FKBP-12 and calcineurin → block in cytokine (e.g., IL-2) production; may stimulate TGF-β production. Side effects: Similar to CsA, but hirsutism/hyperplasia of gums unusual, and diabetes more likely.
- Azathioprine: Mercaptopurine prodrug. Mechanism: Hepatic metabolites inhibit purine synthesis. Side effects: Marrow suppression (WBC > RBC > platelets).
- Mycophenolate mofetil/sodium: Metabolized to mycophenolic acid. Mechanism: Inhibits purine synthesis via inosine monophosphate dehydrogenase. Side effects: Diarrhea/cramps; dose-related liver and marrow suppression is uncommon.
- Sirolimus/everolimus: Macrolide, poor oral bioavailability. Mechanism: Complexes with FKBP-12 and then blocks p70 S6 kinase in IL-2 receptor pathway for proliferation. Side effects: Hyperlipidemia, thrombocytopenia.
- Belatacept: Fusion protein, intravenous injections. Mechanism: Binds CD80 and CD86, prevents CD28 binding and T-cell activation. Side effects: Posttransplant lymphoproliferative disease (PTLD).
- Monitoring: Drug level of CNIs should be monitored, and drug–drug interactions should be carefully examined. Antibiotics and antifungals (e.g., erythromycin, ketoconazole, fluconazole) and nondihydropyridine calcium channel blockers (e.g., diltiazem, verapamil) inhibit activity of cytochrome P450 C3A enzyme and cause elevated levels of CNIs. Antiepileptics (e.g., phenytoin, carbamazepine) increase metabolism, resulting in lower levels.
- TPMT Genotyping: U.S. Food and Drug Administration (FDA) recommends TPMT genotyping or phenotyping before starting treatment with azathioprine. Patients with two nonfunctional TPMT alleles experience life-threatening myelosuppression when treated with azathioprine.
- Allopurinol: Concomitant use best avoided and, if used, very carefully monitored, owing to inhibition of xanthine oxidase.
7.3 Treatment of Rejection¶
- T cell–mediated rejection: Treatment involves high-dose steroid, e.g., IV administration of methylprednisolone, 500–1000 mg daily for 3 days.
- Failure to respond: Indication for antibody therapy, usually with ATG.
- Antibody-mediated rejection: Treatment remains a challenge. Aggressive use of plasmapheresis, IVIG, anti-CD20 monoclonal antibody (rituximab) to target B lymphocytes, and bortezomib to target antibody-producing plasma cells indicated.
- Noninvasive biomarkers: Circulating donor-derived cell-free DNA, urine chemokine markers (e.g., CXCL9), and characterization of urine exosome used as adjunct diagnostic markers for rejection.
7.4 Management of Infection¶
- Pneumocystis jirovecii: Prophylaxis against P. jirovecii with daily low-dose TMP-SMX for 6 months is effective.
- Candida: Oropharynx involvement with Candida may be treated with local nystatin.
- Systemic fungal infections: Require treatment with systemic agents such as fluconazole or one of newer antifungal agents.
- CMV infection: Valganciclovir has proved effective in both prophylaxis and treatment of CMV disease. Acyclovir is effective therapy for herpes simplex virus infections.
- BK virus: Reactivation of BK, if left untreated, will lead to progressive fibrosis and loss of the graft within 1 year in most cases. In most cases, BK infection can be managed by regular testing of BK viral load and judicious reduction of maintenance immunosuppression.
- Therapies for BK: Leflunomide, cidofovir, and quinolone antibiotics (which are effective against polyoma helicase) and IVIG have been tried but with inconsistent results.
7.5 Management of Chronic Complications¶
- Cardiovascular events: Major cause of death (29%).
- Infection: Major cause of death (18%).
- Malignancy: Major cause of death (17%).
- Hypertension: Control of systemic and intrarenal hypertension with calcium channel blockers thought to have beneficial influence on rate of progression of chronic allograft dysfunction.
- Malignancy: Incidence of tumors in patients on immunosuppressive therapy is 5–6%, or approximately 100 times greater than that in the general population.
- Belatacept: 7-year follow-up of BENEFIT trial showed improved patient and graft survival for belatacept-treated group compared to patients treated with cyclosporine, despite short-term risks of higher rates of acute rejection.
8. PROGNOSIS & COMPLICATIONS¶
Overall results of transplantation are presented in Table 325-2. While the loss of kidney transplant due to acute rejection is now a rare event, most allografts eventually succumb at varying rates to a chronic process consisting of interstitial fibrosis, tubular atrophy, vasculopathy, and glomerulopathy. The overall results of transplantation are presented in Table 325-2. Age-related mortality rates after transplantation are highest in the first year due to the surgical risks: 2% for ages 18–34 years, 3% for ages 35–49 years, and 6.8% for ages ≥50–60 years. Despite this, the actual survival benefit of transplantation compared to chronic dialysis becomes apparent within days to months following transplantation, even after risk adjustments for age, diabetes, and cardiovascular status.
8.1 Causes of Death¶
- Cardiovascular events (29%).
- Infection (18%).
- Malignancy (17%).
- Typical time courses of opportunistic infections after transplantation are shown in Table 325-4 (referenced in text).
8.2 Chronic Allograft Dysfunction¶
- Most recipients experience progressive decline in kidney function over time thereafter.
- Causes: Chronic active antibody-mediated rejection, recurrent glomerular disease, hypertension, CNI nephrotoxicity, secondary focal glomerulosclerosis, or combination of these pathophysiologies.
- Vascular changes: Intimal proliferation and medial hypertrophy commonly found.
- Diagnosis: Kidney allograft biopsy can distinguish subacute cellular rejection from recurrent disease or secondary focal sclerosis.
9. SPECIAL CONSIDERATIONS¶
Recipient evaluation is critical in identifying patients at risk. It involves a multidisciplinary approach that requires thorough medical, surgical, social, and psychosocial evaluations to identify the risk factors that prohibit transplantation or mandate treatment before proceeding, as well as ensuring the appropriate use of limited organs. There are a few absolute contraindications to kidney transplantation: chronic illness that limits predicted survival for <2 years, active malignancy, active infection, psychosocial issues affecting adherence to the medical care, and active substance abuse. Cardiovascular risk assessment is crucial during both the perioperative and postoperative periods. Patients with ESKD are at higher cardiovascular mortality risk and need thorough cardiovascular evaluation for coronary artery diseases, valvular diseases, and heart failure.
9.1 Living-Donor Evaluation¶
- Living kidney donors experience immediate risk of surgery and long-term potential risk of developing kidney dysfunction prematurely.
- Basic principle of 'first, do no harm' important.
- Donor evaluation must take every effort to exclude any medical conditions that may cause morbidity and mortality after kidney donation, such as hypertension, diabetes, and/or proteinuria.
- Risk of ESKD after kidney donation: Not greater than that of general population, but absolute donation associated with small but significant potential lifetime risk of ESKD (0.3–0.4%).
- Mechanism of premature renal failure: Increased blood flow and hyperfiltration injury in remaining kidney.
- Reports of development of hypertension, proteinuria, and even lesions of focal segmental sclerosis in donors over long-term follow-up.
- Family members of type 1 diabetics: Anti-insulin and anti-islet cell antibodies should be measured, and a glucose tolerance test should be performed.
- African-American donors: Higher risk of ESKD after donation (in line with their higher risk of kidney failure in general).
- Genetic screening: Screening for APOL1 risk alleles may be appropriate.
- Surgical perspective: Selective renal arteriography is essential to reveal any anatomic anomaly and to assess size imbalance and laterality of donor kidneys.
- Donor nephrectomy: Performed laparoscopically to minimize surgical scar and to enhance faster postsurgical recovery.
- Conflicts of interest: Financial and nonfinancial conflicts of interest between kidney donors and recipients strictly prohibited.
- Legislative efforts: Ongoing to protect kidney donors.
9.2 Deceased-Donor Evaluation¶
- Deceased donors should be free of malignant neoplastic disease, hepatitis, and HIV owing to possible transmission to the recipient.
- Under certain circumstances, HCV- and HIV-positive organs may be used.
- Increased risk of graft failure exists when donor is elderly or has acute kidney injury or when kidney experiences prolonged period of ischemia.
- DCD Categories: I (Brought in dead), II (Unsuccessful resuscitation), III (Awaiting cardiac arrest), IV (Cardiac arrest after brainstem death), V (Cardiac arrest in a hospital patient).
- DCD Usage: Kidneys can be used for transplantation from categories II–V but are commonly only used from categories III and IV.
- Survival: Survival of these kidneys has not been shown to be inferior to that of deceased-donor kidneys.
- KDPI: Kidneys with KDPI >85% have been shown to have poorer survival.
- High KDPI kidneys: Generally utilized for patients for whom benefits of being transplanted earlier outweigh associated risks of using lower-quality kidney.
9.3 Clinical Course & Management¶
- Adequate hemodialysis should be performed within 48 h prior to surgery as needed to control serum potassium to prevent cardiac arrhythmias.
- Surgery: Kidney allograft usually placed in recipient's iliac fossa using retroperitoneal approach.
- Anastomosis: Donor renal artery to recipient external iliac artery and donor renal vein to recipient external iliac vein.
- Donor ureter: Anastomosed to recipient bladder mucosa.
- Native kidney nephrectomy: Rarely performed except in case of extremely enlarged polycystic kidney or chronic pyelonephritis.
- Urine production: Allograft often starts to produce urine immediately after anastomosis.
- Acute tubular injury: Accounts for postoperative diuresis.
- Recovery: Recipient's serum creatinine should start to fall as allograft starts to function, and recovery usually occurs within 2 weeks, although periods as long as 6 weeks have been reported.
- Slow recovery or oliguria: Should prompt allograft biopsy because superimposition of rejection on acute tubular injury is common and difficult to distinguish without allograft biopsy.
- Induction immunosuppression therapy and maintenance steroids and antimetabolites start on day of surgery.
- CNI introduction: Usually safe to delay introduction of a CNI for a few days if a lymphocyte-depleting induction agent is used.
10. KEY PEARLS & CLINICAL TRAPS¶
The presence of antibodies against donor antigens, either HLA or non-HLA, can be a potential cause of allograft injury after transplantation, and hence, it is important to perform crossmatching prior to transplantation. A positive cytotoxic crossmatch of recipient serum with donor T lymphocytes indicates the presence of preformed donor-specific anti-HLA class I antibodies and is usually predictive of an acute vasculitic event termed hyperacute rejection. This finding represents the only widely accepted absolute immunologic contraindication for kidney transplantation. Desensitization prior to transplantation by reducing the level of anti-donor antibodies utilizing plasmapheresis and/or the administration of pooled immunoglobulin (IV immunoglobulin [IVIG]) has been useful in reducing the risk of hyperacute rejection following transplantation. Kidney paired donation programs where living donor kidneys are swapped so each recipient receives a compatible transplant organ are increasingly popular to transplant presensitized candidates safely.
10.1 Diagnostic Clues¶
- C4d deposition in peritubular capillaries and glomerular basement membrane is a footprint of complement activation and one of the diagnostic criteria of antibody-mediated rejection.
- Rise in serum creatinine with or without reduction in urine volume is the primary presentation of rejection.
- Fever, swelling, and tenderness over the allograft are rarely characteristic of rejection.
- Circulating donor-derived cell-free DNA, urine chemokine markers (e.g., CXCL9), and characterization of urine exosome used as adjunct diagnostic markers for rejection.
10.2 Exclusion Criteria¶
- Absolute contraindications: Chronic illness that limits predicted survival for <2 years, active malignancy, active infection, psychosocial issues affecting adherence to the medical care, and active substance abuse.
- Positive cytotoxic crossmatch: Represents the only widely accepted absolute immunologic contraindication for kidney transplantation.
- Preformed antibodies against donor kidney at time of anticipated transplant: Can cause hyperacute rejection.
- Natural antibodies against ABO blood group antigens and antibodies against HLA class I (A, B, C) or class II (DR, DQ, DP) antigens: Harmful antibodies routinely excluded by proper screening of candidate's ABO compatibility and direct cytotoxic cross-matching of candidate's serum with lymphocytes of the donor.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
Caption: CHAPTER 325 OF THE RECIPIENT tion agent is used. Figure 325-2 illustrates a typical algorithm followed by transplant centers for early posttransplant management of recipients Adequate hemodialysis should be performed within 48 h prior to at high or low risk of early renal dysfunction. the surgery as needed to control serum potassium to prevent cardiac arrhythmias. During the transplantation surgery, the kidney allograft is usually placed in the recipient’s iliac fossa using a retroperitoneal ■ MANAGEMENT OF REJECTION approach. An anastomosis is made between donor renal artery and Early diagnosis of rejection allows prompt institution of therapy to recipient external iliac artery and donor renal vein to recipient external preserve allograft function and prevent irreversible damage. Clinical
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
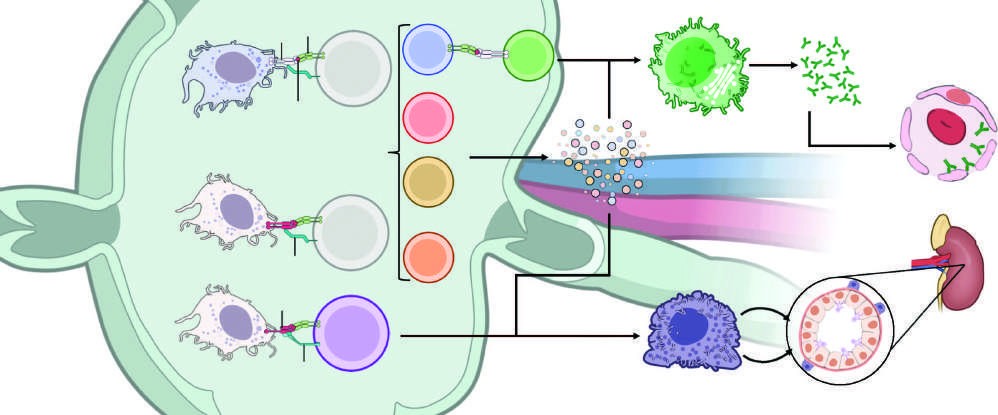
Caption: FIGURE 325-1 Recognition pathways for major histocompatibility complex (MHC) receptors that bind to specific complexes of peptides and MHC class II molecules on responses, there are two sets of T-cell clones involved in rejection. In the direct pathway, to the intact MHC molecule, and class I MHC allogeneic cells are recognized by CD8 T the incompatible MHC molecules are processed into peptides that are presented by the physiologic process in T-cell recognition of foreign antigens. Once T cells are H helper effects on macrophages, TC, and B cells. (Courtesy of Andrew Badoui and Nadim — Figure 325-1: Recognition pathways for major histocompatibility complex (MHC) antigens. Illustrates direct pathway (CD4 T cells bind class II MHC of donor APCs; CD8 T cells bind class I MHC allogeneic cells) and indirect pathway (incompatible MHC molecules processed into peptides presented by self-APCs of recipient). Shows Tfh cell activation, B cell differentiation into plasma cells, and antibody-mediated rejection mechanisms including C4d deposition and complement activation.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.