Cough¶
Chapter 40 | Part 2: Cardinal Manifestations and Presentation of Diseases · Part 2 – Cardinal Manifestations & Presentation
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Cough is a protective reflex; impaired cough predisposes to retained secretions, infection, and atelectasis.
- Excessive coughing can lead to emesis, syncope, muscular pain, rib fractures, and urinary incontinence.
- Chronic cough is defined as lasting >8 weeks; common causes include ACE inhibitors, postnasal drainage, gastroesophageal reflux, and asthma.
- ACE inhibitor–induced cough occurs in 5–30% of patients, is not dose-dependent, and is caused by bradykinin accumulation.
- Cough hypersensitivity syndrome presents with a dry cough worsened by talking, laughing, or exertion; more common in women.
- Eosinophilic bronchitis is characterized by sputum eosinophilia >3% without airflow obstruction and responds to inhaled glucocorticoids.
- Postnasal drainage diagnosis relies on subjective information as quantitation is not possible; many with drainage do not cough.
- Failure to observe a decrease in cough after 1 month off ACE inhibitor therapy argues strongly against ACE inhibitor etiology.
- Impaired cough assessment can use peak expiratory flow or maximal expiratory pressure as surrogates for cough strength.
- Cough-variant asthma is common in children but rare in adults; diagnosis requires airflow obstruction or bronchoprovocation challenge.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Cough Mechanism
- 1.2 Impaired Cough
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Chronic Cough Hypersensitivity Syndrome
- 3.2 Eosinophilic Bronchitis
- 4. CLINICAL FEATURES
- 4.1 Chronic Cough with Normal Chest Radiograph
- 4.2 Physical Examination Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Acute Cough Etiologies
- 5.2 Chronic Cough Etiologies
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Testing for Chronic Cough
- 7. MANAGEMENT & TREATMENT
- 7.1 Management of ACE Inhibitor–Induced Cough
- 7.2 Management of Gastroesophageal Reflux
- 7.3 Management of Postnasal Drainage
- 7.4 Management of Asthma and Eosinophilic Bronchitis
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Complications of Impaired Cough
- 8.2 Complications of Excessive Cough
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🖼 Figure | Flow-volume curve shows spikes of high expiratory flow achieved with cough |
1. DEFINITION & OVERVIEW¶
Cough performs an essential protective function for human airways and lungs. Without an effective cough reflex, there is a risk for retained airway secretions and aspirated material predisposing to infection, atelectasis, and respiratory compromise. At the other extreme, excessive coughing can be exhausting and complicated by emesis, syncope, muscular pain, or rib fractures. It can aggravate low back pain, abdominal or inguinal hernias, and urinary incontinence, and is a major impediment to social interactions. Cough is often a clue to the presence of respiratory disease. In many instances, cough is an expected and accepted manifestation of disease, as in acute respiratory tract infection; however, persistent cough in the absence of other respiratory symptoms commonly causes patients to seek medical attention.
1.1 Cough Mechanism¶
Both chemical (e.g., capsaicin) and mechanical (e.g., mucus, particulates in air pollution) stimuli can initiate a cough. Cationic channels (e.g., transient receptor potential channels) and adenosine triphosphate–activated ion channels (P2X3) function as sensory neuronal receptors, with signals transmitted centrally via Aδ (mechanosensory) and C fibers (chemosensory). Afferent nerve endings richly innervate the pharynx, larynx, and airways to the level of the terminal bronchioles and extend into the lung parenchyma. They are also located in the external auditory canal (the auricular branch of the vagus nerve, or Arnold's nerve) and in the esophagus. Sensory signals travel via the vagus and superior laryngeal nerves to a region of the brainstem in the nucleus tractus solitarius. Integrated neural networks process this input into a conscious sensation referred to as the 'urge to cough.' The efferent limb of the cough reflex involves a highly orchestrated series of involuntary muscular actions, with the potential for input from cortical pathways as well, making possible voluntary cough. The vocal cords adduct, leading to transient upper-airway occlusion. Expiratory muscles contract, generating positive intrathoracic pressures as high as 300 mmHg. With sudden release of the laryngeal contraction, rapid expiratory flows are generated, exceeding the normal 'envelope' of maximal expiratory flow seen on the flow-volume curve. Bronchial smooth-muscle contraction together with dynamic compression of airways narrow airway lumens and maximize the velocity of exhalation. The kinetic energy available to dislodge mucus from the inside of airway walls is directly proportional to the square of the velocity of expiratory airflow. A deep breath preceding a cough optimizes the function of the expiratory muscles; a series of repetitive coughs at successively lower lung volumes sweeps the point of maximal expiratory velocity progressively further into the lung periphery.
1.2 Impaired Cough¶
Weak or ineffective cough compromises the ability to clear lower respiratory tract secretions, predisposing to more serious infections and their sequelae. Weakness or paralysis of the expiratory (abdominal and intercostal) muscles and pain in the chest wall or abdomen are among the most common causes of impaired cough. Cough strength is generally assessed qualitatively; peak expiratory flow or maximal expiratory pressure at the mouth can be used as a surrogate marker for cough strength. A variety of assistive devices and techniques have been developed to improve cough efficacy, running the gamut from simple (splinting of the abdominal muscles with a tightly held pillow to reduce postoperative pain while coughing) to complex (a mechanical cough-assist device supplied via face mask or tracheal tube that applies a cycle of positive pressure followed rapidly by negative pressure). Cough may fail to clear secretions completely despite a preserved ability to generate normal expiratory velocities; such failure may be due to abnormal airway secretions (e.g., abnormally viscous secretions of cystic fibrosis), ciliary dysfunction (e.g., primary ciliary dyskinesia), or structural abnormalities of the airways (e.g., tracheomalacia with excessive expiratory collapse of the trachea during cough).
Table 1 — Table 40-1 Causes of Impaired Cough and Airway Clearance¶
| Category | Specific Causes | |||
|---|---|---|---|---|
| Respiratory muscle weakness | Chest wall or abdominal pain | Chest wall deformity (e.g., severe kyphoscoliosis) | Impaired glottic closure or tracheostomy | Central respiratory depression (e.g., anesthesia, sedation, or neurologic disease) |
| Abnormal airway secretions | Ciliary dysfunction | Tracheobronchomalacia | Bronchiectasis | Tracheal or bronchial stenoses |
2. EPIDEMIOLOGY¶
The duration of cough is a clue to its etiology, at least retrospectively. Acute cough (8 weeks) may be caused by a wide variety of cardiopulmonary diseases, including those of inflammatory, infectious, neoplastic, and cardiovascular etiologies. Chronic cough in the absence of identifiable etiology has been recognized with increasing frequency, is thought to be due to exaggerated neurologic signaling via sensory cough-reflex pathways, and is referred to as 'chronic cough hypersensitivity syndrome.'
3. ETIOLOGY & PATHOPHYSIOLOGY¶
Cough alone as a manifestation of asthma is common among children but not among adults. Cough due to asthma in the absence of wheezing, shortness of breath, and chest tightness is referred to as 'cough-variant asthma.' A history suggestive of cough-variant asthma ties the onset of cough to an exposure that typically triggers asthma and the resolution of cough to discontinuation of the exposure. ACE inhibitor–induced cough occurs in 5–30% of patients taking these agents and is not dose-dependent. ACE metabolizes bradykinin and other tachykinins, such as substance P. The mechanism of ACE inhibitor–associated cough may involve sensitization of sensory nerve endings due to accumulation of bradykinin. Postnasal drainage of any etiology can cause cough as a response to stimulation of sensory receptors of the cough-reflex pathway in the hypopharynx or aspiration of draining secretions into the trachea. The term upper airway cough syndrome has been coined to encompass the concept that chronic inflammation in the nose and sinuses can cause cough even in the absence of physical drainage into the pharynx. It is thought that reflux of gastric contents into the lower esophagus may trigger cough via reflex pathways initiated in the esophageal mucosa. Reflux to the level of the pharynx (laryngopharyngeal reflux), with consequent aspiration of gastric contents, causes a chemical bronchitis and possibly pneumonitis that can elicit cough for days afterward, but it is an uncommon finding among persons with chronic cough.
3.1 Chronic Cough Hypersensitivity Syndrome¶
It presents with a dry or minimally productive cough and a tickle or sensitivity in the throat and is made worse with talking, laughing, or exertion. It is more common in women than men and can last for years. Specific diagnostic criteria are lacking; the diagnosis is suspected when alternative etiologies are excluded by diagnostic testing or failed therapeutic trials. It is uncertain whether persistent daily coughing elicits an inflammatory response and is thereby self-perpetuating.
3.2 Eosinophilic Bronchitis¶
This uncommon condition is characterized by sputum eosinophilia in excess of 3% without airflow obstruction or bronchial hyperresponsiveness and is successfully treated with inhaled glucocorticoids. Measurement of an elevated concentration of nitric oxide in exhaled breath has the potential to detect eosinophilic airway inflammation (in asthma or eosinophilic bronchitis) and predict a favorable response to inhaled steroids in persons with chronic cough.
4. CLINICAL FEATURES¶
Except for our ability to detect the sound of excess airway secretions, details as to the resonance of the cough, its time of occurrence during the day, and the pattern of coughing (e.g., occurring in paroxysms) infrequently provide useful etiologic clues. Regardless of cause, cough often worsens upon first lying down at night, with talking, or with the hyperpnea of exercise; it frequently improves with sleep. An exception may involve the cough that occurs only with certain allergic exposures or exercise in cold air, as in asthma. Useful historical questions include what circumstances surrounded the onset of cough, what makes the cough better or worse, and whether the cough produces sputum. The physical examination seeks clues suggesting the presence of cardiopulmonary disease, including findings such as wheezing or crackles on chest examination. Examination of the auditory canals and tympanic membranes (for irritation of the latter resulting in stimulation of Arnold's nerve), the nasal passageways (for rhinitis or polyps), and the nails (for clubbing) may also provide etiologic clues. Because cough can be a manifestation of a systemic disease such as sarcoidosis or vasculitis, a thorough general examination is likewise important.
4.1 Chronic Cough with Normal Chest Radiograph¶
In virtually all instances, evaluation of chronic cough merits a chest radiograph. The list of diseases that can cause persistent cough without other symptoms and without detectable abnormalities on physical examination is long. It includes serious illnesses such as sarcoidosis or Hodgkin's disease in young adults, lung cancer in older patients, and (worldwide) pulmonary tuberculosis. An abnormal chest film prompts an evaluation aimed at explaining the radiographic abnormality. In a patient with chronic productive cough, examination of expectorated sputum is warranted, because determining the cause of mucus hypersecretion is a crucial clue to etiology. Purulent-appearing sputum should be sent for routine bacterial culture and, in certain circumstances, mycobacterial culture as well. Cytologic examination of mucoid sputum may be useful to assess for malignancy and oropharyngeal aspiration and to distinguish neutrophilic from eosinophilic bronchitis. Expectoration of blood—whether streaks of blood, blood mixed with airway secretions, or pure blood—deserves a special approach to assessment and management.
4.2 Physical Examination Findings¶
On speculum examination of the nose, excess mucoid or purulent secretions, inflamed and edematous nasal mucosa, and/or polyps may be seen; in addition, secretions or a cobblestoned appearance of the mucosa along the posterior pharyngeal wall may be noted. Unfortunately, there is no means by which to quantitate postnasal drainage. In many instances, this diagnosis must rely on subjective information provided by the patient. Furthermore, this assessment must also be counterbalanced by the fact that many people who have chronic postnasal drainage do not experience cough. Linking gastroesophageal reflux to chronic cough poses similar challenges. Retrosternal burning after meals or on recumbency, frequent eructation, hoarseness, and throat pain may be indicative of gastroesophageal reflux. Nevertheless, reflux may also elicit minimal or no symptoms. Glottic inflammation detected on laryngoscopy may be a manifestation of recurrent reflux to the level of the throat, but it is a nonspecific finding.
5. DIFFERENTIAL DIAGNOSIS¶
It is commonly held that (alone or in combination) the use of an ACE inhibitor; postnasal drainage; gastroesophageal reflux; and asthma account for >90% of cases of chronic cough with a normal or noncontributory chest radiograph; however, clinical experience does not support this contention. Strict adherence to this concept discourages the search for alternative explanations by both clinicians and researchers. In recent years, the concept of a distinct 'cough hypersensitivity syndrome' has emerged, emphasizing the putative role of sensitized sensory nerve endings and afferent neural pathways in causing chronic refractory cough, akin to chronic neuropathic pain.
5.1 Acute Cough Etiologies¶
Acute cough (<3 weeks) is most commonly due to a respiratory tract infection, aspiration, or inhalation of noxious chemicals or smoke.
5.2 Chronic Cough Etiologies¶
Chronic cough (>8 weeks) may be caused by a wide variety of cardiopulmonary diseases, including those of inflammatory, infectious, neoplastic, and cardiovascular etiologies. Patient's with excessive nasopharyngeal drainage, and medications (angiotensin-converting enzyme [ACE] inhibitors) are the most common identifiable causes of chronic cough.
6. INVESTIGATIONS & DIAGNOSIS¶
In a patient with chronic productive cough, examination of expectorated sputum is warranted, because determining the cause of mucus hypersecretion is a crucial clue to etiology. Purulent-appearing sputum should be sent for routine bacterial culture and, in certain circumstances, mycobacterial culture as well. Cytologic examination of mucoid sputum may be useful to assess for malignancy and oropharyngeal aspiration and to distinguish neutrophilic from eosinophilic bronchitis. In a patient capable of taking reliable measurements, home expiratory peak flow monitoring can be a cost-effective method to support or discount a diagnosis of asthma. Objective testing can establish the diagnosis of asthma (airflow obstruction on spirometry that varies over time or reverses in response to a bronchodilator) or exclude it with certainty (a negative response to a bronchoprovocation challenge—e.g., with methacholine).
6.1 Diagnostic Testing for Chronic Cough¶
Evaluation of chronic cough merits a chest radiograph. An abnormal chest film prompts an evaluation aimed at explaining the radiographic abnormality. Quantification of the frequency and level of reflux requires a somewhat invasive procedure to measure esophageal pH (either nasopharyngeal placement of a catheter with a pH probe into the esophagus for 24 h or endoscopic placement of a radiotransmitter capsule into the esophagus) and, with newer techniques, esophageal pressures (manometry) and nonacid reflux. The precise interpretation of test results that permits an etiologic linking of reflux events and cough remains debated.
7. MANAGEMENT & TREATMENT¶
Treatment of chronic cough in a patient with a normal chest radiograph is often empirical and is targeted at the most likely cause(s) of cough as determined by history, physical examination, and possibly pulmonary function testing. Therapy for postnasal drainage depends on the presumed etiology (infection, allergy, or vasomotor rhinitis) and may include systemic antihistamines; decongestants; antibiotics; nasal saline irrigation; and nasal pump sprays with glucocorticoids, antihistamines, or anticholinergics. Antacids, histamine type 2 (H) receptor antagonists, and proton pump inhibitors are used to neutralize or decrease the production of gastric acid in gastroesophageal reflux disease; dietary changes, elevation of the head and torso during sleep, and medications to improve gastric emptying or impede the flow of refluxate (e.g., alginates) are additional therapeutic measures. Cough-variant asthma typically responds well to inhaled glucocorticoids and intermittent use of inhaled β-agonist bronchodilators. Any patient with chronic unexplained cough who is taking an ACE inhibitor should have a trial period off the medication, regardless of the timing of the onset and of cough relative to the initiation of ACE inhibitor therapy. In most instances, a safe alternative is available; angiotensin receptor blockers do not cause cough. Failure to observe a decrease in cough after 1 month off medication argues strongly against this etiology.
7.1 Management of ACE Inhibitor–Induced Cough¶
ACE inhibitor–induced cough occurs in 5–30% of patients taking these agents and is not dose-dependent. The mechanism of ACE inhibitor–associated cough may involve sensitization of sensory nerve endings due to accumulation of bradykinin. Any patient with chronic unexplained cough who is taking an ACE inhibitor should have a trial period off the medication, regardless of the timing of the onset and of cough relative to the initiation of ACE inhibitor therapy. In most instances, a safe alternative is available; angiotensin receptor blockers do not cause cough.
7.2 Management of Gastroesophageal Reflux¶
Antacids, histamine type 2 (H) receptor antagonists, and proton pump inhibitors are used to neutralize or decrease the production of gastric acid in gastroesophageal reflux disease; dietary changes, elevation of the head and torso during sleep, and medications to improve gastric emptying or impede the flow of refluxate (e.g., alginates) are additional therapeutic measures.
7.3 Management of Postnasal Drainage¶
Therapy for postnasal drainage depends on the presumed etiology (infection, allergy, or vasomotor rhinitis) and may include systemic antihistamines; decongestants; antibiotics; nasal saline irrigation; and nasal pump sprays with glucocorticoids, antihistamines, or anticholinergics.
7.4 Management of Asthma and Eosinophilic Bronchitis¶
Cough-variant asthma typically responds well to inhaled glucocorticoids and intermittent use of inhaled β-agonist bronchodilators. Eosinophilic bronchitis is successfully treated with inhaled glucocorticoids.
8. PROGNOSIS & COMPLICATIONS¶
Without an effective cough reflex, we are at risk for retained airway secretions and aspirated material predisposing to infection, atelactasis, and respiratory compromise. At the other extreme, excessive coughing can be exhausting; can be complicated by emesis, syncope, muscular pain, or rib fractures; can aggravate low back pain, abdominal or inguinal hernias, and urinary incontinence; and can be a major impediment to social interactions.
8.1 Complications of Impaired Cough¶
Weak or ineffective cough compromises the ability to clear lower respiratory tract secretions, predisposing to more serious infections and their sequelae.
8.2 Complications of Excessive Cough¶
Excessive coughing can be complicated by emesis, syncope, muscular pain, or rib fractures. It can aggravate low back pain, abdominal or inguinal hernias, and urinary incontinence.
9. SPECIAL CONSIDERATIONS¶
The text does not explicitly detail special considerations for pregnancy, pediatrics, elderly, renal/hepatic impairment, or immunocompromised states in the provided source text.
10. KEY PEARLS & CLINICAL TRAPS¶
Cough hypersensitivity syndrome is more common in women than men and can last for years. It presents with a dry or minimally productive cough and a tickle or sensitivity in the throat and is made worse with talking, laughing, or exertion. It is uncertain whether persistent daily coughing elicits an inflammatory response and is thereby self-perpetuating. Many people with symptomatic reflux do not experience chronic cough. The precise interpretation of test results that permits an etiologic linking of reflux events and cough remains debated.
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
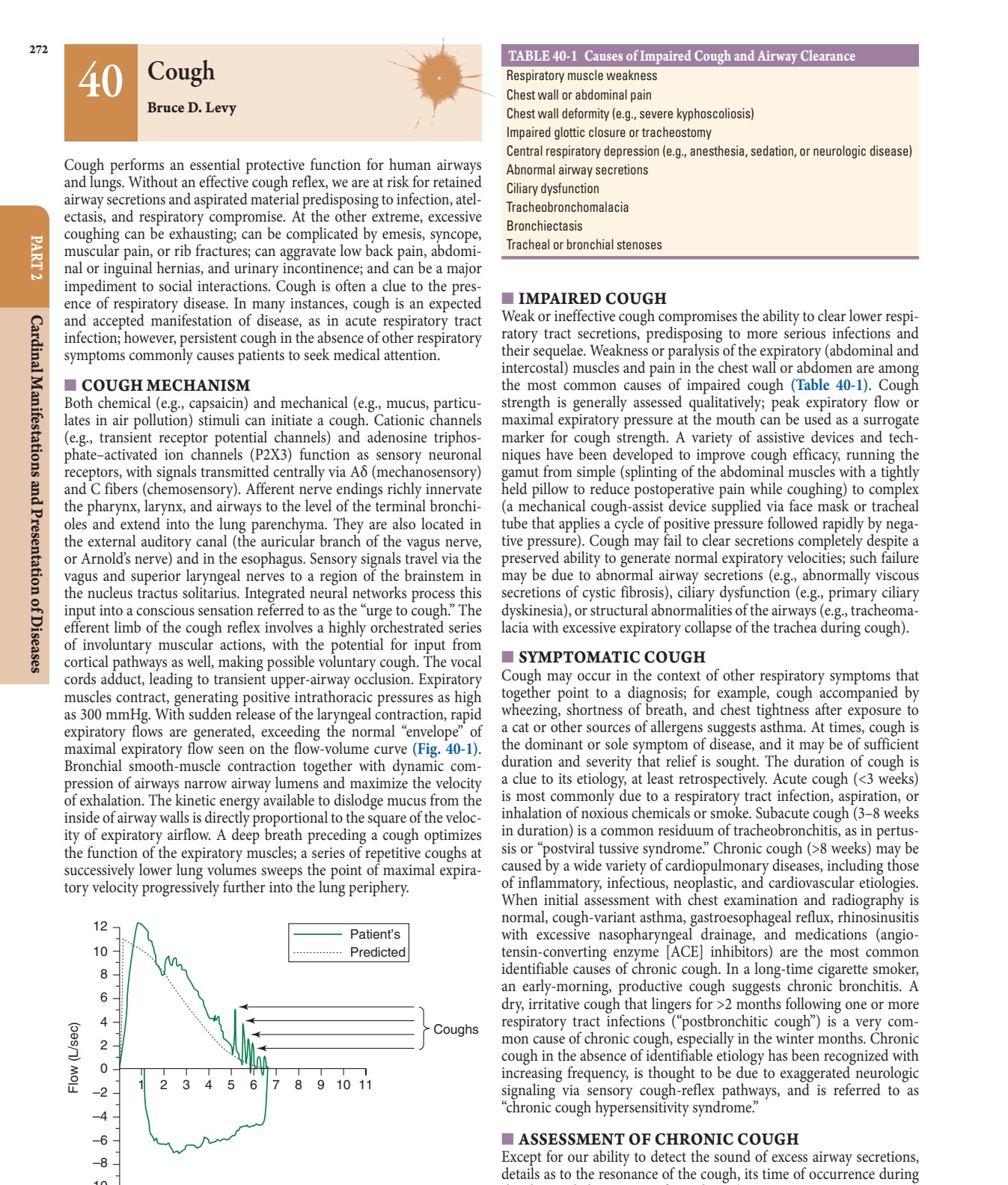
Caption: FIGURE 40-1 Flow-volume curve shows spikes of high expiratory flow achieved with cough. — Figure 40-1: Flow-volume curve demonstrating spikes of high expiratory flow achieved during cough, exceeding the normal maximal expiratory flow envelope.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.