Chapter 374: Spondyloarthritis¶
Immune-Mediated, Inflammatory, and Rheumatologic Disorders · Part 11 – Rheumatology & Immunology
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Spondyloarthritis (SpA) is a family of immune-mediated inflammatory arthritis disorders characterized by inflammation-induced bone loss coexisting with pathologic new bone formation.
- Axial SpA (axSpA) is divided into radiographic (r-axSpA, ankylosing spondylitis) and nonradiographic (nr-axSpA) based on sacroiliitis grade on plain radiographs.
- Peripheral SpA (pSpA) includes psoriatic arthritis, reactive arthritis, IBD-associated arthritis, and undifferentiated SpA.
- HLA-B27 is the strongest genetic risk factor, present in 85–90% of r-axSpA and 50–90% of nr-axSpA patients.
- Inflammatory back pain (IBP) is characterized by insidious onset, improvement with exercise, and worsening with rest, distinguishing it from mechanical back pain.
- TNF-α and IL-17 are signature cytokines driving disease across all domains (gut, skin, joint, spine).
- Imaging: MRI is sensitive for early active inflammation (osteitis), while X-ray shows structural damage (sacroiliitis, syndesmophytes).
- Treatment hierarchy: NSAIDs first-line; Biologics (TNFi, IL-17i, IL-23i) or JAK inhibitors for refractory cases.
- Red flags for malignancy or infection: fever, weight loss, night pain, history of cancer, or advanced age.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Classification Spectrum
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Genetic Associations
- 3.2 Cytokine Pathways
- 4. CLINICAL FEATURES
- 4.1 Inflammatory Back Pain Characteristics
- 4.2 Extraarticular Manifestations
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria
- 6.2 Imaging Findings
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Interventions
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
- Spondyloarthritis (SpA) refers to a family of immune-mediated inflammatory arthritis disorders that share many clinical, genetic, and pathologic characteristics.
- Moll and Wright are credited in recognizing these diseases in 1974 as distinct from rheumatoid arthritis (RA).
- While axial skeletal involvement is hinted at in the word 'spondyloarthritis,' it is not mandatory.
- The musculoskeletal manifestations of SpA include sacroiliitis, inflammatory spinal lesions, peripheral inflammatory arthritis, enthesitis (inflammation at the attachment of tendons and ligaments to the bones), tendonitis, tenosynovitis, and dactylitis ('sausage digits').
- Other clinical manifestations include uveitis, skin psoriasis, inflammatory bowel disease (IBD, Crohn's, or ulcerative colitis), absence of rheumatoid factor (RF) and nodules (to differentiate from RA), familial correlation, and association with the gene human leukocyte antigen (HLA)-B27.
- The 2009 Assessment of Spondyloarthritis International Society (ASAS) classification criteria divided SpA under 'axial' (axSpA) and 'peripheral' (pSpA).
- 'Peripheral' SpA indicates that peripheral musculoskeletal features represent disease under treatment, which inevitably impacts histopathology.
- Obtaining synovial tissue from an array of joints such as knees, wrists, and small joints in fingers has become much more readily accessible through ultrasound-guided synovial tissue biopsy, which permits study of synovial tissue alterations in an early treatment-naïve stage.
- Patients with axSpA can have peripheral musculoskeletal manifestations, and patients with pSpA may have additional axial skeletal involvement at presentation or may develop it later in the course of their disease.
- Other conditions sometimes included under pSpA are SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome, acne-associated arthritis, and arthritis associated with hidradenitis suppurativa.
- Table 374-1 shows the full spectrum of conditions included under 'spondyloarthritis.'
- Pattern recognition is important for the diagnosis of SpA.
- Typical patterns include asymmetric, mono- or oligoarticular (four or less joints) inflammatory arthritis of large joints in the lower limb (usually knee), with enthesitis, tendonitis, and dactylitis.
- This contrasts with RA, where polyarticular symmetric involvement of metacarpophalangeal (MCP)/proximal interphalangeal (PIP) joints predominates.
- The cumulative prevalence of all conditions under SpA is 2–3% of the population, much more common than RA.
1.1 Classification Spectrum¶
- Table 374-1 Spectrum of Spondyloarthritis
- Axial Spondyloarthritis (axSpA): Radiographic (r-axSpA, also called ankylosing spondylitis [AS]) and Nonradiographic (nr-axSpA).
- Peripheral Spondyloarthritis (pSpA): Conditions commonly included (Psoriatic arthritis, IBD-associated arthritis, Reactive arthritis, Undifferentiated peripheral SpA) and Conditions sometimes included (SAPHO syndrome, Acne-associated arthritis, Hidradenitis suppurativa–associated arthritis).
- Radiographic axSpA (r-axSpA): Sacroiliitis grade 2 (bilateral), grade 3 or 4 (unilateral or bilateral).
- Nonradiographic axSpA (nr-axSpA): Sacroiliitis grade 1 (unilateral or bilateral) or grade 2 (unilateral).
- Psoriatic arthritis: Skin psoriasis and nail involvement usually preceding arthritis, enthesitis, dactylitis.
- IBD-associated arthritis: Crohn's disease or ulcerative colitis with inflammatory arthritis.
- Reactive arthritis: Urethritis, history of preceding infection with Salmonella, Shigella, Yersinia, Campylobacter, and Chlamydia, mucosal ulcers, conjunctivitis, keratoderma blennorrhagica.
- Undifferentiated peripheral SpA: Enthesitis, dactylitis, family history of SpA, HLA-B27, acute anterior uveitis, and not fitting in any of the other conditions mentioned above.
- SAPHO syndrome: Synovitis, acne, pustulosis, hyperostosis, and osteitis; typical involvement of anterior chest wall joints.
- Acne-associated arthritis: Acne conglobata, peripheral arthritis.
- Hidradenitis suppurativa–associated arthritis: Hidradenitis suppurativa, peripheral arthritis, rarely asymmetric sacroiliitis manifestations.
Table 1 — Table 374-1 Spectrum of Spondyloarthritis¶
| SPONDYLOARTHRITIS (SPA) | AXIAL SPONDYLOARTHRITIS (axSpA) | PERIPHERAL SPONDYLOARTHRITIS (pSpA) |
|---|---|---|
| Radiographic axSpA (r-axSpA, also called ankylosing spondylitis [AS]) | Sacroiliitis grade 2 (bilateral), grade 3 or 4 (unilateral or bilateral) | Psoriatic arthritis: Skin psoriasis and nail involvement usually preceding arthritis, enthesitis, dactylitis |
| Nonradiographic axSpA (nr-axSpA) | Sacroiliitis grade 1 (unilateral or bilateral) or grade 2 (unilateral) | Inflammatory bowel disease–associated arthritis: Crohn's disease or ulcerative colitis with inflammatory arthritis |
| Reactive arthritis | Urethritis, history of preceding infection with Salmonella, Shigella, Yersinia, Campylobacter, and Chlamydia, mucosal ulcers, conjunctivitis, keratoderma blennorrhagica | Undifferentiated peripheral SpA: Enthesitis, dactylitis, family history of SpA, HLA-B27, acute anterior uveitis, and not fitting in any of the other conditions mentioned above |
| SAPHO syndrome | Synovitis, acne, pustulosis, hyperostosis, and osteitis; typical involvement of anterior chest wall joints | Acne-associated arthritis: Acne conglobata, peripheral arthritis |
| Hidradenitis suppurativa–associated arthritis | Hidradenitis suppurativa, peripheral arthritis, rarely asymmetric sacroiliitis manifestations |
2. EPIDEMIOLOGY¶
- The male-to-female ratio is 2:1 for r-axSpA and 1:1 for nr-axSpA.
- The population prevalence of axSpA depends on the prevalence of HLA-B27 in that geographic region.
- In Europe, HLA-B27 frequency in the population increases from south to north, and so does the prevalence of axSpA.
- For example, the prevalence of HLA-B27 in Spain and Norway is 7 and 9%, respectively, and the prevalence of AS and axSpA in these two countries is 0.1 and 0.56%.
- The 2009–2010 National Health and Nutritional Examination Survey (NHANES) estimated that in the United States, the population prevalence of HLA-B27 is 6% and that of axSpA is between 0.9 and 1.4%, of which 0.5% were reported to have AS.
- The population prevalence of axSpA in the rest of the world is not well studied and is believed to be between 0.02 and 1.5%.
- Diagnostic prevalence of axSpA in the United States, which includes only the diagnosed cases in a population, is one-tenth that of population prevalence, suggesting a large undiagnosed population.
- Based on insurance claims databases in the United States, the diagnostic prevalence of axSpA increased between 2006 to 2019, which could be attributed to increased disease awareness.
- The incidence rates of AS are 0.005–0.01 per 100 patient-years globally and are not available for nr-axSpA.
- The risk of axSpA is 5% in HLA-B27-positive people but increases to 20% in HLA-B27-positive first-degree relatives of affected individuals with axSpA.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- SpA is a prototypic chronic immune-mediated inflammatory disease that couples inflammation to structural damage.
- A unique feature of SpA is that inflammation-induced bone loss coexists with pathologic new bone formation, which occurs at specific sites in the skeleton.
- These sites include not only the sacroiliac joint but also the anterior spinal ligaments or at entheses in the peripheral skeleton.
- If uncontrolled, axSpA may ultimately lead to a complete ankylosis of the sacroiliac joints and the spine, termed 'bamboo spine.'
- With increasing awareness of SpA resulting from early diagnosis and treatment, there has been a steady decrease in the amount of structural damage observed over the past decades with a gradual shift of higher prevalence from r-AxSpA to nr-AxSpA.
- Although the exact mechanisms that initiate the disease are not fully delineated, genetic and environmental risk factors and molecular and cellular alterations at key disease sites have been implicated in the pathophysiology of SpA.
- At these sites, which include the axial and peripheral joints, entheses, skin, and gut, variation is seen in the disease mechanisms and perturbations of the key cytokine pathways.
- These tissue-based variations are most likely associated with the dissimilar clinical responses observed between the spine, peripheral joints, and gut during treatment with cytokine inhibitors.
- Genetic Associations: HLA-B27 is a major histocompatibility complex (MHC) class I allele that forms the strongest genetic risk factor for SpA and specifically axSpA.
- MHC class I molecules are expressed on the surface of nucleate cells and can present peptides to CD8+ T cells.
- HLA-B27 is present in 85–90% of the patients with r-axSpA and 50–90% in nr-axSpA, in contrast to about 5% of the healthy Caucasian population.
- Besides HLA-B27, other MHC class I genes and non-MHC coding genes have been identified in large genome-wide association studies (GWAS) in axSpA.
- Within the group of non-MHC coding genes, genes linked to innate immune processes, interleukin (IL)-23/IL-17 immunity, joint and bone remodeling, epithelial function, and antigen presentation are seen.
- Genetic epistatic interaction has been suggested between ERAP1, a peptide-trimming enzyme, of which single nucleotide polymorphisms (SNPs) are associated with AS and HLA-B27.
- The 'arthritogenic peptide' theory proposes that HLA-B27 presents pathological microbial peptides to CD8+ cytotoxic T cells that target cross-reactive human peptides leading to inflammation and resulting in molecular mimicry.
- Presumably, this first antigenic exposure could take place in the gut or at the urogenital tract.
- Several subtypes of HLA-B27 exist, but not all of them represent risk factors for axSpA. For example, HLA-B2704 and HLA-B2705 subtypes confer a genetic risk, whereas the HLA-B2706 and HLA-B2709 allotypes are not associated with axSpA even though they only differ in one peptide residue or amino acid.
- The second theory relates to the ability of HLA-B27 to homodimerize. These HLA-B27 homodimers can be expressed at the cell surface and interact with innate immune receptors, such as the KIR3DL2 receptor, on T and natural killer (NK) cells resulting in IL-17 production, one of the key pathogenic cytokines in axSpA.
- A third theory links HLA-B27 to unfolded protein responses (UPR) and autophagy, which may promote type 17 immune responses through release of IL-23.
- Mechanical Stress: Mechanical strain in entheses may lead to microdamage that leads to immune activation and tissue repair.
- Enthesitis occurs more often in the lower limbs, which are subject to higher mechanical strain.
- In patients with AS, exposure to physical labor was related to more structural damage.
- In mouse models, mechanical strain was shown to be causally related to development of enthesitis and SpA-related new bone formation through mechanisms that support chronicity of inflammation.
- Barrier Integrity Loss and the Intestinal Microbiota: Evidence supporting this mechanism has been the development of ReA following an infectious gastroenteritis with Salmonella typhimurium, Shigella enteritidis, Yersinia enterocolitica, or Campylobacter enteritidis.
- Studies have highlighted the loss of barrier integrity, which may facilitate translocation of bacteria and microbial peptides that can elicit an immune response.
- The human microbiome is shaped by genetic and environmental factors.
- Changes in diversity and composition of the gut microbiome have been identified in SpA, pinpointing an intestinal dysbiosis that is similar to patients with IBD.
- Germ-free HLA-B27 transgenic rats fail to develop SpA, suggesting a crucial pathogenic role for intestinal microbiota.
- In humans, microbiome profiling in stool and biopsy samples of HLA-B27–positive individuals found that HLA-B27 affects the gut microbiome even in the absence of disease.
- This supports the concept that in HLA-B27–positive individuals, intestinal dysbiosis occurs prior to the onset of clinical manifestations and may contribute to the risk of disease.
- Earlier research suggested that HLA-B27 may promote intracellular innate-like survival and persistence of pathogens such as Chlamydia trachomatis in monocytes, which could travel to joints and promote synovial inflammation.
- More recent studies indicate that not all preclinical models or of combined gut and joint disease mimicking SpA impact these sites similarly: in a tumor necrosis factor (TNF) cytokine-dependent model with Crohn's-like ileitis and peripheral arthritis, gut inflammation was found to be microbiota dependent but not joint inflammation.
- Skin Barrier: The skin, as the outer barrier of the body, is also vulnerable to the development of immune-mediated inflammatory disease.
- Alterations in the cutaneous microbiome of patients with psoriasis and PsA have been described with striking similarities between nonlesional and lesional skin.
- However, the functional impact of skin microbiota on the disease trajectory is still ill defined.
3.1 Genetic Associations¶
- HLA-B27 is a major histocompatibility complex (MHC) class I allele that forms the strongest genetic risk factor for SpA and specifically axSpA.
- MHC class I molecules are expressed on the surface of nucleate cells and can present peptides to CD8+ T cells.
- HLA-B27 is present in 85–90% of the patients with r-axSpA and 50–90% in nr-axSpA, in contrast to about 5% of the healthy Caucasian population.
- Other MHC class I genes and non-MHC coding genes have been identified in large genome-wide association studies (GWAS) in axSpA.
- Genes linked to innate immune processes, interleukin (IL)-23/IL-17 immunity, joint and bone remodeling, epithelial function, and antigen presentation are seen.
- Genetic epistatic interaction has been suggested between ERAP1, a peptide-trimming enzyme, of which single nucleotide polymorphisms (SNPs) are associated with AS and HLA-B27.
- HLA-B2704 and HLA-B2705 subtypes confer a genetic risk, whereas the HLA-B2706 and HLA-B2709 allotypes are not associated with axSpA.
3.2 Cytokine Pathways¶
- Regardless of the route of disease initiation, several common effector pathways have emerged, with TNF and IL-17 representing signature cytokines in the immunologic basis of axSpA.
- TNF-α is an important activator and product of macrophages that stimulates cytokine production in immune cells and activates fibroblasts.
- TNF-α can also be made by neutrophils and activated T cells in the inflamed synovium, enthesis, and intestine.
- By activating osteoclasts, it promotes inflammation-induced bone loss and bone erosions in SpA.
- IL-17A blockade is effective in axSpA, whereas IL-23 inhibition does not provide benefit.
- Conversely, IL-23 blockers are approved in IBD, but agents targeting IL-17A are contraindicated in active IBD, due to the barrier protective roles of IL-17.
- In PsA, IL-23 and IL-17 inhibitors both appear to be effective.
- Several IL-17A–producing cell types, including T17 cells (consisting of both CD4+ T 17 and CD8+ Tc17 cells), γ/δ T cells, and ILC3, are present at entheseal sites in steady-state conditions.
- In synovial fluid of SpA patients, innate-like T cells such as γδ T cells were found to be the major T-cell source of IL-17 in the presence or absence of IL-23.
- Janus kinase (JAK) inhibitors, which block signaling of several cytokines, are effective in a wide range of SpA including all clinical domains.
4. CLINICAL FEATURES¶
- Axial SpA is a chronic, immune-mediated inflammatory disorder predominantly involving the axial skeleton (sacroiliac joints and the spine) and also the peripheral skeleton.
- The axial skeleton is always involved, and involvement of the peripheral joints occurs in ~30–40% of patients.
- The hips, historically considered 'root joints,' are the most common nonspinal joints affected.
- Enthesitis in the axial and peripheral skeleton is a common feature, but dactylitis is relatively rare.
- Extraarticular manifestations include psoriasis, acute anterior uveitis, and IBD.
- Some patients with axSpA experience gradual spinal bony fusion over several years, which leads to reduced spine and neck flexibility.
- Despite these osteoproliferative changes in the skeleton, osteoporosis is a common morbidity.
- AxSpA significantly affects patients' well-being, function, productivity, and health-related quality of life.
- The most common first manifestation of axSpA is low back, hip, or buttock pain, which starts before the age of 40–45 years, usually in the 20s to 30s.
- The typical characteristics of this back pain include any combination of the following: insidious onset, chronicity (>3 months' duration), age of onset 30 min) morning stiffness.
- Back pain with these characteristics is termed 'inflammatory back pain' (IBP) to differentiate it from the common 'mechanical back pain'.
- Rarely, thoracic or neck pain can be a presenting feature, and when present, it is more commonly seen in women.
- Fatigue and stiffness are the two most bothersome symptoms after back pain in axSpA.
- Fatigue is multifactorial, secondary to sleep disturbance, active inflammation, and anemia, and may also indicate underlying depression and anxiety of chronic disease.
- Peripheral arthritis is seen in 30–40% of patients with axSpA.
- Typically, this is an asymmetric, oligoarticular inflammatory arthritis involving the large joints of the lower extremities and rarely the small joints of hands and feet.
- Hip involvement, presenting as pain in the groin with radiation to medial thigh or the knee, is common and is associated with significant functional impairment.
- Enthesitis is a common manifestation of axSpA.
- Enthesitis may present as heel pain (plantar fasciitis, Achilles tendon insertion pain), chest wall pain, intercostal muscle insertions, medial or lateral epicondylitis, quadriceps or patellar tendon insertion pain around knees, or pelvic rim pain.
- Dactylitis is an uncommon manifestation of axSpA.
- Persistent axial inflammation may lead to bony fusion of sacroiliac joints, apophyseal joints, and development of syndesmophytes by osteoproliferation in the outer fibers of the annulus fibrosus of the intervertebral disks.
- These bony changes lead to limitation of spinal, including neck, mobility in all directions and are a major cause of significant functional impairment in late stages of the disease.
- Extramusculoskeletal manifestations of axSpA, such as psoriasis, IBD, and acute anterior uveitis, can also be the presenting symptom of axSpA in some patients, and such patients may first present to a dermatologist, gastroenterologist, or an ophthalmologist.
- Uveitis, the most common extramusculoskeletal manifestation, is seen in 40% of patients with axSpA and presents as eye discomfort followed by redness, pain, photophobia, and miosis.
- The typical phenotype of uveitis associated with axSpA is acute, anterior, unilateral, and episodic.
- While frank IBD is seen in 10%, histologic evidence of subclinical gut inflammation is seen in up to 50% of patients.
- Psoriasis is seen in 10%, and osteoporosis can be present in 40%.
- AxSpA can affect multiple organ systems.
- The two renal manifestations of axSpA are IgA nephropathy, which can present at any time in the disease course as microscopic hematuria, and nephrotic syndrome secondary to renal (AA) amyloidosis, which is a late complication seen after prolonged uncontrolled inflammation.
- Conduction abnormalities (heart blocks) can be seen at any stage of the disease, whereas aortic valve insufficiency and cauda equina syndrome presenting as urinary hesitancy and/or saddle anesthesia are late complications.
- Pulmonary manifestations of axSpA include apical fibrosis, cavitary lung lesion, or fibrotic parenchymal lesions.
- Sleep apnea syndrome and restrictive lung disease seen in late-stage axSpA are mostly related to osteoproliferative structural changes of the cervical spine and rib cage.
- The course of axSpA can be variable, with close to 50% of patients with nonradiographic to radiographic stage over 20 years and <10% progressing to significant spinal involvement with bamboo spine.
- Risk factors for osteoproliferation include male sex, persistent body inflammation (seen on magnetic resonance imaging [MRI] of sacroiliac joints and spine, high C-reactive protein [CRP]), syndesmophytes, presence of HLA-B27, and smoking.
- AS is thought to be a disease of males, and back pain and enthesitis in women are commonly mistaken for fibromyalgia. This delays the diagnosis in females even further.
- Lower prevalence of HLA-B27 in nonwhite populations also adds to the delay in diagnosis.
- The diagnosis of axSpA is based on pattern recognition, ruling out common causes for the symptoms, and clinical reasoning.
4.1 Inflammatory Back Pain Characteristics¶
- Table 374-4 Clinical Features of Inflammatory Versus Mechanical Back Pain
- Age at onset: Inflammatory (30 min) vs Mechanical (Less than 30 min).
- Pain at night: Inflammatory (Yes, usually after midnight) vs Mechanical (No, usually late in the day).
- Exercise/activity: Inflammatory (Improves pain and stiffness) vs Mechanical (Worsens pain).
- Rest/inactivity: Inflammatory (Worsens pain and stiffness) vs Mechanical (Improves pain).
- Duration: Inflammatory (Chronic) vs Mechanical (Acute or chronic).
- Response to NSAIDs: Inflammatory (More than 50% relief in 48 hours) vs Mechanical (Limited relief).
Table 2 — Table 374-4 Clinical Features of Inflammatory Versus Mechanical Back Pain¶
| FEATURE | INFLAMMATORY BACK PAIN | MECHANICAL BACK PAIN |
|---|---|---|
| Age at onset | Before 40–45 years | 20–65 years |
| Onset | Insidious | Acute or insidious |
| Morning stiffness | Prolonged (more than 30 min) | Less than 30 min |
| Pain at night | Yes, usually after midnight | No, usually late in the day |
| Exercise/activity | Improves pain and stiffness | Worsens pain |
| Rest/inactivity | Worsens pain and stiffness | Improves pain |
| Duration | Chronic | Acute or chronic |
| Response to NSAIDs | More than 50% relief in 48 hours | Limited relief |
4.2 Extraarticular Manifestations¶
- Uveitis: Seen in 40% of patients with axSpA. Presents as eye discomfort followed by redness, pain, photophobia, and miosis. Typical phenotype is acute, anterior, unilateral, and episodic.
- Psoriasis: Seen in 10%.
- Osteoporosis: Can be present in 40%.
- Renal: IgA nephropathy (microscopic hematuria) and nephrotic syndrome (renal AA amyloidosis).
- Cardiac: Conduction abnormalities (heart blocks) at any stage; aortic valve insufficiency and cauda equina syndrome (urinary hesitancy, saddle anesthesia) as late complications.
- Pulmonary: Apical fibrosis, cavitary lung lesion, fibrotic parenchymal lesions, sleep apnea syndrome, restrictive lung disease.
5. DIFFERENTIAL DIAGNOSIS¶
- Chronic nonspecific 'mechanical' back pain is common in the general population, and axSpA is the etiology in only 4–5% of such patients.
- Mechanical causes of back pain therefore should be considered first in a patient presenting with chronic back pain.
- The so-called 'red flag' signs of fever, weight loss, advanced age, and past history of malignancy should alert the examiner to look for osteomyelitis, osteoporotic fracture, or metastatic disease.
- In young patients with generalized body pain, fibromyalgia, central sensitization, hypermobility, hypothyroidism, and hypovitaminosis D may be considered.
- Abnormalities on incidental imaging in a patient with or even without chronic back pain lead to other differential diagnoses such as diffuse idiopathic skeletal hyperostosis (DISH) or osteitis condensans ilii (OCI).
- DISH is a noninflammatory, degenerative condition affecting the spine, with exuberant new bone formation in the form of anterior and posterior longitudinal ligament ossification of at least four contiguous vertebral bodies and bulky 'flowing' osteophytes typically on the right side of the thoracic spine, but normal sacroiliac joints.
- It is generally seen in obese, diabetic males, often older than 50 years of age.
- DISH is sometimes mistaken for bamboo spine of AS.
- OCI is usually an asymptomatic condition of multiparous women characterized by radiographic findings of a triangular area of dense sclerosis on the lower and inferior part of the iliac side of the sacroiliac joints.
- This can be mistaken for sacroiliitis, and in early stages, MRI of the sacroiliac joints may be indistinguishable from that of axSpA.
- Lack of erosions should help distinguish OCI from axSpA.
- OCI can be seen in nulliparous women and even men.
- While DISH and OCI are generally asymptomatic, some patients with either condition may present with chronic back pain.
- Inflammatory back pain with sclerotic changes on sacroiliac joint radiographs can also be seen in conditions such as postpartum insufficiency fracture of the sacrum; septic sacroiliitis from tuberculosis, brucellosis, fungi, and other infectious agents; and rarely, malignancies.
- As a result, the U.S. Food and Drug Administration (FDA) suggests reserving certain diagnostic or therapeutic approaches for specific contexts.
6. INVESTIGATIONS & DIAGNOSIS¶
- Elevated inflammatory markers, erythrocyte sedimentation rate (ESR), and CRP help in making the diagnosis of axSpA, but these tests are neither sensitive (seen in only 30–40% of patients with active axSpA) nor specific for axSpA.
- Imaging plays a very important role in the diagnosis of axSpA.
- A single anteroposterior (AP) view or a Ferguson view x-ray of the pelvis is sufficient to image sacroiliac joints.
- Multiple views (e.g., oblique) of the sacroiliac joints add little in making the diagnosis; in addition, they increase radiation risk to gonads.
- Radiographic features of sacroiliitis include marginal sclerosis, erosions, narrowing and widening of the joints, and in late stages, fusion.
- As a general rule, plain radiographs of the spine should be avoided in patients with chronic back pain.
- However, there are some characteristic changes of axSpA seen in the lateral radiograph of the spine, and they include Romanus lesions or the shiny corner sign and squaring of the vertebral body seen as a result of erosions at the attachments of the spinal ligaments at the vertebral corners.
- Andersson lesion is an uncommon finding and is characterized by vertebral body erosion and sclerosis at the intervertebral disk level.
- In the late stages, ossification of the outer layer of annulus fibrosus leads to syndesmophyte formation.
- Typical syndesmophyte orientation is vertical, differentiating it from the horizontal orientation of osteophytes, which is commonly seen with osteoarthritis (OA) of the spine.
- Bamboo spine, or ankylosis of the entire spine, is seen in a very small percentage of late-stage AS patients.
- Low-dose computed tomography (CT) of the sacroiliac joints and spine in the diagnosis of axSpA is emerging as an alternative to plain radiography for diagnosis and assessing progression.
- Magnetic resonance imaging (MRI) of the sacroiliac joints and spine has evolved as an important tool in making the diagnosis of axSpA.
- During the early stage of disease, MRI of the sacroiliac joints may show evidence of active inflammation, or 'osteitis,' and that may be the only abnormality.
- As time passes, the active inflammatory changes transition to fatty metaplasia, and this may further transform to new bone formation.
- The structural changes of sclerosis, fat metaplasia, erosions, fat metaplasia in an erosion cavity (backfill), and new bone formation, in addition to the inflammatory changes seen on MRI, aid in making the diagnosis of axSpA.
- Sole presence of inflammatory lesions in early stages or sole presence of ankylosis in very late stage may be enough for the diagnosis of axSpA, but as a general rule, multiple types of inflammatory and structural lesions increase the suspicion of axSpA.
- In the spine, multiple corner inflammatory lesions and/or multiple corner fatty lesions increase the confidence of axSpA diagnosis.
- MRI is a very sensitive imaging technique, and mechanical stress on the sacroiliac joints in professional athletes, postpartum women, and even in normal individuals, especially above the age of 40, may show changes of osteitis.
- Fat metaplasia-type changes in the sacroiliac joints are also seen in degenerative arthritis as well as in normal individuals.
- Inappropriate utilization of MRI can lead to overdiagnosis.
- Table 374-2 Modified New York Classification Criteria for Ankylosing Spondylitis (AS).
- Clinical Criteria: 1. Low back pain >3 months, Improved with exercise, Not relieved by rest. 2. Limited lumbar motion in frontal and lateral planes. 3. Reduced chest expansion.
- Radiographic Criteria: 1. Bilateral grade >2 sacroiliitis on x-ray. 2. Unilateral or bilateral grade 3 or 4 on x-ray.
- Definite AS requires ≥1 clinical criterion plus 1 radiographic criterion.
- Figure 374-2 Schema for the diagnosis of axial spondyloarthritis in a patient complaining of chronic back pain (back pain lasting >3 months).
- Figure 374-3 Radiographic axial spondyloarthritis. A. Bilateral sacroiliitis (modified New York grade 3) with sclerosis and erosions. B. Lateral view cervical spine in advanced radiographic axial spondyloarthritis showing anterior syndesmophytes and fused facet joints.
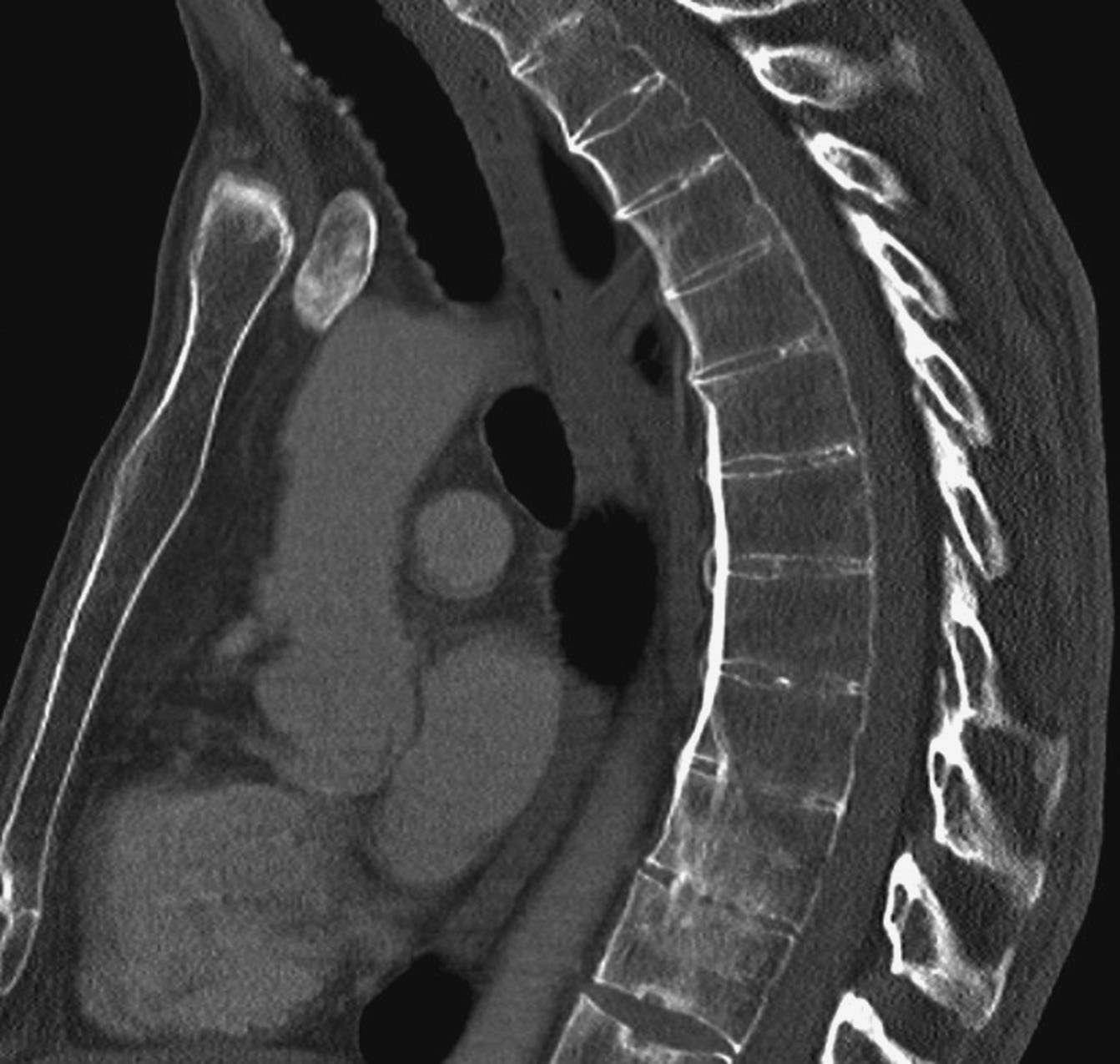
- Figure 374-4 Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes.
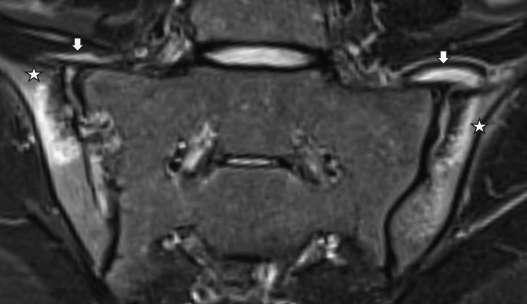
- Figure 374-5 Magnetic resonance images of spondyloarthritis. A. T1-weighted image of sacroiliac joints with bilateral erosions (left-sided erosions marked by ), left fatty metaplasia (single ), and right bone marrow edema (marked with white arrows). B. Short tau inversion recovery (STIR) image with bilateral bone marrow edema suggestive of joint space inflammation (shown by ) and anterior capsulitis (shown by a white arrow).
- Table 374-3 Grading of Sacroiliitis.
- Grade 0: Normal.
- Grade 1: Suspicious change.
- Grade 2: Minimum abnormality (small, localized areas with erosions or sclerosis, without alterations in the joint width).
- Grade 3: Unequivocal abnormality (moderate or advanced sacroiliitis with evidence of sclerosis, widening, narrowing, or partial ankylosis).
- Grade 4: Severe abnormality (total ankylosis).
- Source: Reproduced with permission from S van der Linden et al: Evaluation of diagnostic criteria for ankylosing spondylitis. Arthritis Rheum 27:361, 1984.
6.1 Diagnostic Criteria¶
- Modified New York Classification Criteria for Ankylosing Spondylitis (AS)
- Clinical Criteria: 1. Low back pain >3 months, Improved with exercise, Not relieved by rest. 2. Limited lumbar motion in frontal and lateral planes. 3. Reduced chest expansion.
- Radiographic Criteria: 1. Bilateral grade >2 sacroiliitis on x-ray. 2. Unilateral or bilateral grade 3 or 4 on x-ray.
- Definite AS requires ≥1 clinical criterion plus 1 radiographic criterion.
- Grading of Sacroiliitis
- Grade 0: Normal.
- Grade 1: Suspicious change.
- Grade 2: Minimum abnormality (small, localized areas with erosions or sclerosis, without alterations in the joint width).
- Grade 3: Unequivocal abnormality (moderate or advanced sacroiliitis with evidence of sclerosis, widening, narrowing, or partial ankylosis).
- Grade 4: Severe abnormality (total ankylosis).
Table 3 — Table 374-2 Modified New York Classification Criteria for Ankylosing Spondylitis (AS)¶
| Clinical Criteria | 1. Low back pain >3 months | Improved with exercise | Not relieved by rest | 2. Limited lumbar motion in frontal and lateral planes | 3. Reduced chest expansion |
|---|---|---|---|---|---|
| Radiographic Criteria | 1. Bilateral grade >2 sacroiliitis on x-ray | 2. Unilateral or bilateral grade 3 or 4 on x-ray | Definite AS requires ≥1 clinical criterion plus 1 radiographic criterion |
Table 4 — Table 374-3 Grading of Sacroiliitis¶
| GRADE | DESCRIPTION |
|---|---|
| Grade 0 | Normal |
| Grade 1 | Suspicious change |
| Grade 2 | Minimum abnormality (small, localized areas with erosions or sclerosis, without alterations in the joint width) |
| Grade 3 | Unequivocal abnormality (moderate or advanced sacroiliitis with evidence of sclerosis, widening, narrowing, or partial ankylosis) |
| Grade 4 | Severe abnormality (total ankylosis) |
6.2 Imaging Findings¶
- X-ray: Single AP view or Ferguson view x-ray of the pelvis is sufficient to image sacroiliac joints.
- Radiographic features of sacroiliitis: Marginal sclerosis, erosions, narrowing and widening of the joints, and in late stages, fusion.
- Lateral radiograph of the spine: Romanus lesions or the shiny corner sign and squaring of the vertebral body seen as a result of erosions at the attachments of the spinal ligaments at the vertebral corners.
- Andersson lesion: Vertebral body erosion and sclerosis at the intervertebral disk level.
- Syndesmophyte formation: Ossification of the outer layer of annulus fibrosus leads to syndesmophyte formation.
- Syndesmophyte orientation: Typical is vertical, differentiating it from the horizontal orientation of osteophytes seen with osteoarthritis (OA) of the spine.
- Bamboo spine: Ankylosis of the entire spine, seen in a very small percentage of late-stage AS patients.
- CT: Low-dose CT of the sacroiliac joints and spine is emerging as an alternative to plain radiography for diagnosis and assessing progression.
- MRI: MRI of the sacroiliac joints and spine has evolved as an important tool in making the diagnosis of axSpA.
- Early stage MRI: Evidence of active inflammation, or 'osteitis,' and that may be the only abnormality.
- Progression: Active inflammatory changes transition to fatty metaplasia, and this may further transform to new bone formation.
- Structural changes: Sclerosis, fat metaplasia, erosions, fat metaplasia in an erosion cavity (backfill), and new bone formation.
- Multiple lesions: Multiple corner inflammatory lesions and/or multiple corner fatty lesions increase the confidence of axSpA diagnosis.
- False positives: Mechanical stress on the sacroiliac joints in professional athletes, postpartum women, and even in normal individuals, especially above the age of 40, may show changes of osteitis.
- Fat metaplasia: Also seen in degenerative arthritis as well as in normal individuals.
- DISH: Diffuse idiopathic skeletal hyperostosis. Noninflammatory, degenerative condition affecting the spine, with exuberant new bone formation in the form of anterior and posterior longitudinal ligament ossification of at least four contiguous vertebral bodies and bulky 'flowing' osteophytes typically on the right side of the thoracic spine, but normal sacroiliac joints.
- OCI: Osteitis condensans ilii. Usually an asymptomatic condition of multiparous women characterized by radiographic findings of a triangular area of dense sclerosis on the lower and inferior part of the iliac side of the sacroiliac joints.
- Distinguishing OCI from axSpA: Lack of erosions should help distinguish OCI from axSpA.
7. MANAGEMENT & TREATMENT¶
- The American College of Rheumatology (ACR), Spondylitis Association of America (SAA), Spondyloarthritis Research and Treatment Network (SPARTAN) treatment guidelines, and ASAS-EULAR (European Alliance of Associations for Rheumatology) treatment recommendations have many commonalities regarding the order of treatments, choices of agents, and precautions.
- Table 374-5 outlines pharmacologic interventions for the treatment of axSpA.
- The use of immunosuppressive biologics and tsDMARDs has been associated with an increased risk of serious infections.
- While bacterial infections are seen in both classes, herpes zoster is mostly seen with JAK inhibitors (JAKis), and reactivation of latent tuberculosis is mostly seen with TNF inhibitors (TNFis).
- Mucosal and skin Candida infections are associated with IL-17 inhibitor (IL-17i) use.
- Other side effects of biologic therapy include injection-site reactions with subcutaneous injections or infusion reactions with intravenous (IV) medication.
- TNFi adverse effects include development of demyelinating disease, worsening of congestive heart failure, and paradoxical development of psoriasis-like skin lesions.
- Adverse events associated with IL-17i therapy include leukopenia and development or worsening of IBD.
- JAKis have a higher risk of major cardiovascular adverse events and cancers (lymphoma and lung cancers), especially in patients aged 65 years or older and in those with current or past history of smoking, with history of cardiovascular disease, or with malignancy.
- Physical therapy improves fatigue, mobility, and posture.
- Smoking cessation is encouraged in all patients.
- Patients with renal tubular acidosis should receive sodium bicarbonate by mouth (0.5–2 mmol/kg in four divided doses).
- Gluocorticoids and monoclonal antibody to CD20 (rituximab) appear to be effective in patients with systemic disease, particularly in those with purpura and persistent arthritis.
- Novel monoclonal antibodies targeting the CD40L/CD40 costimulatory pathway or the BAFF receptor or sequential treatment of belimumab and rituximab seem to be promising therapeutic strategies.
- Data for a beneficial role of other conventional immunosuppressants are limited.
- Treatment of lymphoma in the setting of Sjögren's disease follows the general guidelines for lymphoma management in the general population.
7.1 Pharmacologic Interventions¶
- NSAIDs: First-line therapy.
- Biologics: TNF inhibitors (TNFis), IL-17 inhibitors (IL-17i), IL-23 inhibitors.
- JAK Inhibitors (JAKis): Effective across all domains.
- Side Effects: TNFis (demyelinating disease, worsening congestive heart failure, paradoxical psoriasis), IL-17i (leukopenia, worsening IBD), JAKis (major cardiovascular adverse events, cancers).
- Infections: Herpes zoster (JAKis), reactivation of latent tuberculosis (TNFis), mucosal and skin Candida infections (IL-17i).
- Injection/Infusion Reactions: Injection-site reactions with subcutaneous injections or infusion reactions with intravenous (IV) medication.
8. PROGNOSIS & COMPLICATIONS¶
- AxSpA significantly affects patients' well-being, function, productivity, and health-related quality of life.
- The course of axSpA can be variable, with close to 50% of patients with nonradiographic to radiographic stage over 20 years and <10% progressing to significant spinal involvement with bamboo spine.
- Risk factors for osteoproliferation include male sex, persistent body inflammation (seen on magnetic resonance imaging [MRI] of sacroiliac joints and spine, high C-reactive protein [CRP]), syndesmophytes, presence of HLA-B27, and smoking.
- Osteoporosis is a common morbidity despite osteoproliferative changes.
- Renal complications: IgA nephropathy (microscopic hematuria) and nephrotic syndrome (renal AA amyloidosis).
- Cardiac complications: Conduction abnormalities (heart blocks) at any stage; aortic valve insufficiency and cauda equina syndrome (urinary hesitancy, saddle anesthesia) as late complications.
- Pulmonary complications: Apical fibrosis, cavitary lung lesion, fibrotic parenchymal lesions, sleep apnea syndrome, restrictive lung disease.
- Lymphoma risk: The use of immunosuppressive biologics and tsDMARDs has been associated with an increased risk of serious infections, including lymphoma.
9. SPECIAL CONSIDERATIONS¶
- Lower prevalence of HLA-B27 in nonwhite populations also adds to the delay in diagnosis.
- AS is thought to be a disease of males, and back pain and enthesitis in women are commonly mistaken for fibromyalgia. This delays the diagnosis in females even further.
- DISH is generally seen in obese, diabetic males, often older than 50 years of age.
- OCI is usually an asymptomatic condition of multiparous women characterized by radiographic findings of a triangular area of dense sclerosis on the lower and inferior part of the iliac side of the sacroiliac joints.
- OCI can be seen in nulliparous women and even men.
- While DISH and OCI are generally asymptomatic, some patients with either condition may present with chronic back pain.
- Inflammatory back pain with sclerotic changes on sacroiliac joint radiographs can also be seen in conditions such as postpartum insufficiency fracture of the sacrum; septic sacroiliitis from tuberculosis, brucellosis, fungi, and other infectious agents; and rarely, malignancies.
- As a result, the U.S. Food and Drug Administration (FDA) suggests reserving certain diagnostic or therapeutic approaches for specific contexts.
10. KEY PEARLS & CLINICAL TRAPS¶
- Red flags for malignancy or infection: Fever, weight loss, advanced age, and past history of malignancy.
- In young patients with generalized body pain, consider fibromyalgia, central sensitization, hypermobility, hypothyroidism, and hypovitaminosis D.
- HLA-B27 testing is useful for diagnosis but does not rule out axSpA in HLA-B27-negative patients.
- MRI is sensitive for early active inflammation but can show changes in normal individuals or those with mechanical stress.
- Pattern recognition is important for the diagnosis of SpA.
- Typical patterns include asymmetric, mono- or oligoarticular (four or less joints) inflammatory arthritis of large joints in the lower limb (usually knee), with enthesitis, tendonitis, and dactylitis.
- This contrasts with RA, where polyarticular symmetric involvement of metacarpophalangeal (MCP)/proximal interphalangeal (PIP) joints predominates.
- The cumulative prevalence of all conditions under SpA is 2–3% of the population, much more common than RA.
- Smoking cessation is encouraged in all patients.
- Physical therapy improves fatigue, mobility, and posture.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶

Caption: FIGURE 373-3 Diagnostic algorithm for Sjögren’s disease. 1Defined as a positive troublesome dry eyes for more than 3 months? (b) Do you have a recurrent sensation of day? (d) Have you had a daily feeling of dry mouth for more than 3 months? (e) Do you in Whitcher et al. van Bijsterveld score described in van Bijsterveld et al. 3Focus score protocol described in Daniels et al. ILD, interstitial lung disease; MS, multiple sclerosis.
Flowchart 2¶

Caption: seen in up to 50% of patients. Psoriasis is seen in 10%, and osteoporosis common causes for the symptoms, and clinical reasoning. Figure 374-2 can be present in 40%. shows a schema for the diagnosis of axSpA in a patient complaining of AxSpA can affect multiple organ systems. The two renal manifesta- chronic (>3 months) back pain. While elevated inflammatory mark- tions of axSpA are IgA nephropathy, which can present at any time in ers, erythrocyte sedimentation rate (ESR), and CRP help in making the disease course as microscopic hematuria, and nephrotic syndrome the diagnosis of axSpA, these tests are neither sensitive (seen in only secondary to renal (AA) amyloidosis, which is a late complication only 30–40% of patients with active axSpA) nor specific for axSpA. seen after prolonged uncontrolled inflammation. Conduction abnor- Imaging plays a very important role in the diagnosis of axSpA. A malities (heart blocks) can be seen at any stage of the disease, whereas single anteroposterior (AP) view or a Ferguson view x-ray of the pelvis aortic valve insufficiency and cauda equina syndrome presenting as is sufficient to image sacroiliac joints. Multiple views (e.g., oblique) of
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
Caption: FIGURE 374-4 Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes. ■ DIFFERENTIAL DIAGNOSIS Chronic nonspecific “mechanical” back pain is common in the general population, and axSpA is the etiology in only 4–5% of such patients. Mechanical causes of back pain therefore should be considered first in a patient presenting with chronic back pain. The so-called “red flag” — Figure 374-1: Pathogenesis and signature cytokines across different disease domains in spondyloarthritis (SpA). Diagram illustrating genetic predisposition, mechanical stress, and barrier integrity loss leading to cytokine crosstalk (TNF-α, IL-17) involving innate and adaptive immune cells.
Figure 2¶
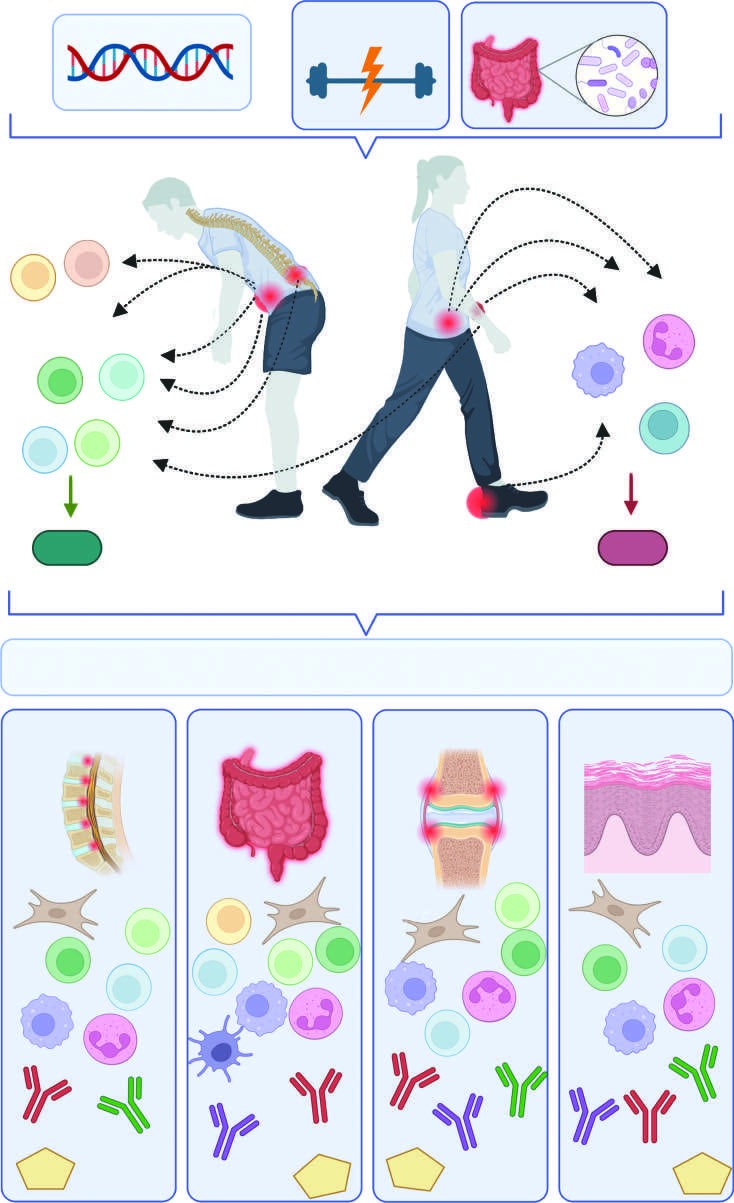
Caption: FIGURE 374-1 Pathogenesis and signature cytokines across different disease domains from mechanical stress, a well-known disease precipitator in psoriatic arthritis and axial (skin) surfaces culminating in a cytokine crosstalk characterized by both tumor necrosis include cells of both innate and adaptive immune system, along with tissue-resident overlapping (e.g., TNF-α) but also distinct (e.g., IL-17, IL-23) signature cytokines, which with signaling of several cytokines, are effective across all domains. — Figure 374-2: Schema for the diagnosis of axial spondyloarthritis (axSpA) in a patient with chronic back pain. Flowchart showing differentiation between radiographic (r-axSpA) and nonradiographic (nr-axSpA) based on imaging and clinical features.
Figure 3¶

Caption: FIGURE 374-4 Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes. ■ DIFFERENTIAL DIAGNOSIS Chronic nonspecific “mechanical” back pain is common in the general population, and axSpA is the etiology in only 4–5% of such patients. Mechanical causes of back pain therefore should be considered first in a patient presenting with chronic back pain. The so-called “red flag” — Figure 374-3: Radiographic axial spondyloarthritis. A. Bilateral sacroiliitis (modified New York grade 3) with sclerosis and erosions. B. Lateral view cervical spine in advanced radiographic axial spondyloarthritis showing anterior syndesmophytes and fused facet joints.
Figure 4¶

Caption: FIGURE 374-6 A. X-ray of the feet in psoriatic arthritis. These images show interphalangeal joint of great toes, and right fifth MTP joint. There are changes of pencil-in-cup deformity in the left fifth MTP joint. B. X-ray of the hands in psoriatic with ). Right third finger has dactylitis and shows periosteal new bone formation in the with ) and distal interphalangeal joints (marked with ). This combination of periosteal — Figure 374-4: Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes.
Figure 5¶

Caption: FIGURE 374-6 A. X-ray of the feet in psoriatic arthritis. These images show interphalangeal joint of great toes, and right fifth MTP joint. There are changes of pencil-in-cup deformity in the left fifth MTP joint. B. X-ray of the hands in psoriatic with ). Right third finger has dactylitis and shows periosteal new bone formation in the with ) and distal interphalangeal joints (marked with ). This combination of periosteal — Figure 374-5: Magnetic resonance images of spondyloarthritis. A. T1-weighted image of sacroiliac joints with bilateral erosions and fatty metaplasia. B. Short tau inversion recovery (STIR) image with bilateral bone marrow edema suggestive of joint space inflammation and anterior capsulitis.
Figure 6¶

Caption: FIGURE 374-6 A. X-ray of the feet in psoriatic arthritis. These images show interphalangeal joint of great toes, and right fifth MTP joint. There are changes of pencil-in-cup deformity in the left fifth MTP joint. B. X-ray of the hands in psoriatic with ). Right third finger has dactylitis and shows periosteal new bone formation in the with ) and distal interphalangeal joints (marked with ). This combination of periosteal — Figure 374-1 (Variant): Detailed view of pathogenesis diagram highlighting the role of HLA-B27, intestinal microbiota, and mechanical stress in disease initiation.
Figure 7¶

Caption: FIGURE 374-4 Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes. ■ DIFFERENTIAL DIAGNOSIS Chronic nonspecific “mechanical” back pain is common in the general population, and axSpA is the etiology in only 4–5% of such patients. Mechanical causes of back pain therefore should be considered first in a patient presenting with chronic back pain. The so-called “red flag” — Figure 374-2 (Variant): Detailed view of diagnostic schema highlighting the decision nodes for HLA-B27 status and MRI findings.
Figure 8¶

Caption: FIGURE 374-4 Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes. ■ DIFFERENTIAL DIAGNOSIS Chronic nonspecific “mechanical” back pain is common in the general population, and axSpA is the etiology in only 4–5% of such patients. Mechanical causes of back pain therefore should be considered first in a patient presenting with chronic back pain. The so-called “red flag” — Figure 374-3 (Variant): Detailed view of radiographic features including Romanus lesions and syndesmophyte orientation differentiating from osteoarthritis.
Figure 9¶
Caption: FIGURE 374-4 Computed tomography of the thoracic spine sagittal view in radiographic axial spondyloarthritis showing anterior and posterior syndesmophytes. ■ DIFFERENTIAL DIAGNOSIS Chronic nonspecific “mechanical” back pain is common in the general population, and axSpA is the etiology in only 4–5% of such patients. Mechanical causes of back pain therefore should be considered first in a patient presenting with chronic back pain. The so-called “red flag” — Figure 374-5 (Variant): Detailed view of MRI findings showing osteitis, fatty metaplasia, and new bone formation progression in sacroiliac joints.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.