Ischemic Heart Disease¶
Chapter 284 | Harrison's 22e · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- See source text for full details
📑 Table of Contents¶
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Algorithm for management of a patient with ischemic heart disease |
| 2 | 🔀 Flowchart | Difference in the approach to the lesion with percutaneous coronary (PCI) and... |
| 1 | 🖼 Figure | Selecting appropriate testing patients with angina and suspected coronary artery disease (CAD) |
| 2 | 🖼 Figure | (Continued) |
| 3 | 🖼 Figure | (Continued) |
| 4 | 🖼 Figure | (Continued) |
| 5 | 🖼 Figure | (Continued) |
| 6 | 🖼 Figure | Cascade of mechanisms and manifestations of ischemia |
| 7 | 🖼 Figure | reason, methods for detecting coronary calcium have been developed as a measure... |
| 8 | 🖼 Figure | Macrocirculation and microcirculation across segments and sizes of the at the top |
| 9 | 🖼 Figure | Macrocirculation and microcirculation across segments and sizes of the at the top |
| 10 | 🖼 Figure | Macrocirculation and microcirculation across segments and sizes of the at the top |
RAW CONTENT¶
[PAGE 2090] 2090 PART 6 Disorders of the Cardiovascular System the general context of population growth and as a result of the increase Section 5 Coronary and Peripheral in the average age of the world’s population. With urbanization in Vascular Disease countries with emerging economies and a growing middle class, ele- ments of the energy-rich Western diet are being adopted. As a result, the prevalence of risk factors for IHD and the prevalence of IHD itself are both increasing rapidly, so that in analyses of the global burden 284 Ischemic Heart Disease of disease, there is a shift from communicable to noncommunicable diseases, and it is estimated that globally over 200 million people live Robert P. Giugliano, Elliott M. Antman, with IHD. Population subgroups that appear to be particularly affected Joseph Loscalzo are men in South Asian countries, especially India and the Middle East. IHD is a major contributor to the number of disability-adjusted life- years (DALYs) experienced globally. Ischemic heart disease (IHD) is a condition in which there is an inad- ■ PATHOPHYSIOLOGY equate supply of blood and oxygen to a portion of the myocardium; it typically occurs when there is an imbalance between myocardial Central to an understanding of the pathophysiology of myocardial oxygen supply and demand. The most common cause of myocardial ischemia is the concept of myocardial supply and demand. In normal ischemia is atherosclerotic disease of an epicardial coronary artery conditions, for any given level of a demand for oxygen, the myocar- (or arteries) sufficient to cause a regional reduction in myocardial dium will control the supply of oxygen-rich blood to prevent under- blood flow and inadequate perfusion of the myocardium supplied perfusion of myocytes and the subsequent development of ischemia by the involved coronary artery. This chapter focuses on the chronic and infarction. The major determinants of myocardial oxygen demand manifestations and treatment of IHD (sometimes referred to as chronic (MVO) are heart rate, myocardial contractility, and myocardial wall 2 coronary disease or chronic coronary syndrome), while the subsequent tension (stress). An adequate supply of oxygen to the myocardium chapters address the acute phases of IHD. requires a satisfactory level of oxygen-carrying capacity of the blood (determined by the inspired level of oxygen, pulmonary function, ■ EPIDEMIOLOGY AND GLOBAL TRENDS and hemoglobin concentration and function) and an adequate level IHD causes more deaths and disability and incurs greater economic of coronary blood flow. Blood flows through the coronary arteries in costs than any other illness in the developed world. IHD is the most a phasic fashion, with the majority occurring during diastole. About common, serious, chronic, life-threatening illness in the United States, 75% of the total coronary resistance to flow occurs across three sets where 20.5 million persons have IHD. Although there is regional of arteries: (1) large epicardial arteries (Resistance 1 = R), (2) prear- 1 variation, ~3–4% of the population has sustained a myocardial infarc- teriolar vessels (R), and (3) arteriolar and intramyocardial capillary 2 tion. Genetic factors, a high-fat and energy-rich diet, smoking, and a vessels (R). In the absence of significant flow-limiting atheroscle- 3 sedentary lifestyle are associated with the emergence of IHD. In the rotic obstructions, R is trivial; the major determinant of coronary 1 United States and Western Europe, IHD is growing among low-income resistance is found in R and R (Fig. 284-1). The normal coronary 2 3 groups, but primary prevention has delayed the disease to later in life circulation is dominated and controlled by the heart’s requirements across socioeconomic groups. Despite these sobering statistics, it is for oxygen. This need is met by the ability of the coronary vascular worth noting that epidemiologic data show a decline in the rate of bed to vary its resistance (and, therefore, blood flow) considerably deaths due to IHD, about half of which is attributable to treatments and while the myocardium extracts a high and relatively fixed percentage half to prevention by risk factor modification. of oxygen. Normally, intramyocardial resistance vessels demonstrate a Obesity, insulin resistance, and type 2 diabetes mellitus are increas- great capacity for dilation (R and R decrease). The changing oxygen 2 3 ing and are powerful risk factors for IHD. These trends are occurring in needs of the heart with exercise and emotional stress affect coronary Macrocirculation Microcirculation Segment Epicardial arteries >400 µm Small arteries 400 µm | Small arteries <400 µm Arterioles <100 µm Capillaries <10 µm Pressure Metabolites Regulation Exchange Flow Transport | | [/TABLE]
[PAGE 2091] Ischemic Heart Disease 2091 CHAPTER 284 vascular resistance and, in this manner, regulate the supply of oxygen the bloodstream. Upon exposure of the plaque contents to blood, two and substrate to the myocardium (metabolic regulation). The coronary important and interrelated processes are set in motion: (1) platelets resistance vessels also adapt to physiologic alterations in blood pres- are activated and aggregate, and (2) the coagulation cascade is acti- sure to maintain coronary blood flow at levels appropriate to myocar- vated, leading to deposition of fibrin strands. A thrombus composed dial needs (autoregulation). of platelet aggregates and fibrin strands traps red blood cells and can By reducing the lumen of the coronary arteries, atherosclerosis reduce coronary blood flow, leading to the clinical manifestations of limits appropriate increases in perfusion when the demand for more myocardial ischemia. coronary flow occurs. When the luminal reduction is severe, myocar- The location of the obstruction influences the quantity of myo- dial perfusion in the basal state is reduced. Coronary blood flow also cardium rendered ischemic and determines the severity of the clini- can be limited by spasm (see vasospastic angina in Chap. 285), arterial cal manifestations. Thus, critical obstructions in vessels, such as the thrombi, and, rarely, coronary emboli as well as by ostial narrowing left main coronary artery and the proximal left anterior descending due to aortitis. Congenital abnormalities such as the origin of the left coronary artery, are particularly hazardous. Chronic severe coronary anterior descending coronary artery from the pulmonary artery may narrowing and myocardial ischemia frequently are accompanied by the cause myocardial ischemia and infarction in infancy, but this cause is development of collateral vessels, especially when the narrowing devel- very rare in adults. ops gradually. When well developed, such vessels can by themselves Myocardial ischemia also can occur if myocardial oxygen demands provide sufficient blood flow to sustain the viability of the myocardium are markedly increased and particularly when coronary blood flow at rest but not during conditions of increased demand. may be limited, as occurs in severe left ventricular hypertrophy (LVH) With progressive worsening of a stenosis in a proximal epicardial due t
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
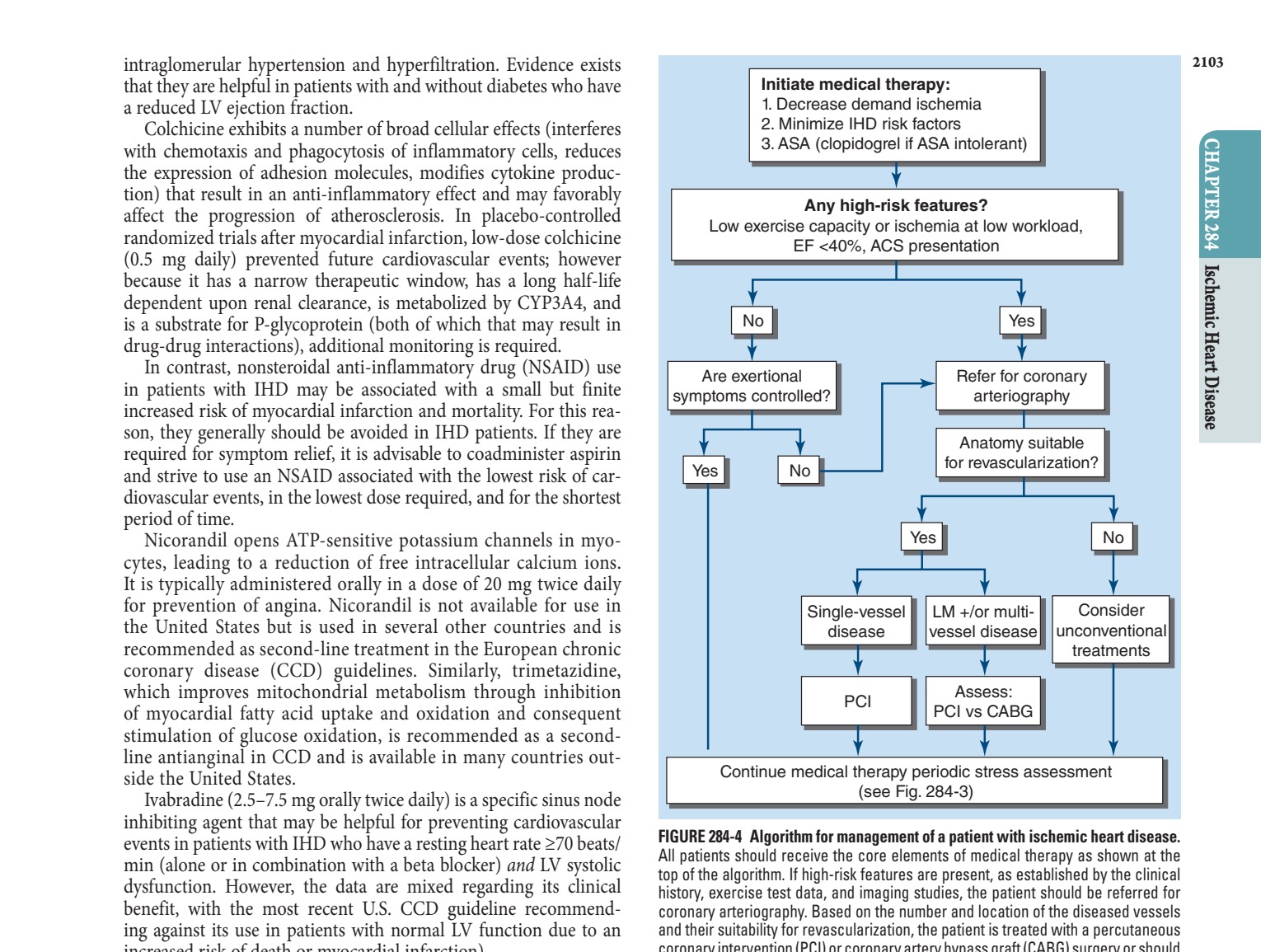
Caption: FIGURE 284-4 Algorithm for management of a patient with ischemic heart disease. All patients should receive the core elements of medical therapy as shown at the top of the algorithm. If high-risk features are present, as established by the clinical history, exercise test data, and imaging studies, the patient should be referred for coronary arteriography. Based on the number and location of the diseased vessels and their suitability for revascularization, the patient is treated with a percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) surgery or should be considered for unconventional treatments. See text for further discussion. ACS, acute coronary syndrome; ASA, aspirin; EF, ejection fraction; IHD, ischemic heart disease; LM, left main.
Flowchart 2¶

Caption: FIGURE 284-5 Difference in the approach to the lesion with percutaneous coronary (PCI) and coronary artery bypass grafting (CABG). PCI is targeted at the “culprit” lesion whereas CABG is directed at the epicardial vessel, including the culprit lesion or lesions culprits, proximal to the insertion of the vein graft, a difference that may account for the of CABG, at least in the intermediate term, in patients with multivessel disease. New England Journal of Medicine, Quantitative Determinants of the Outcome of Mitral Regurgitation, M Enriquez-Sarano et al. 352, 2235. Copyright © 2005. Society. Reprinted with permission from Massachusetts Medical Society.)
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

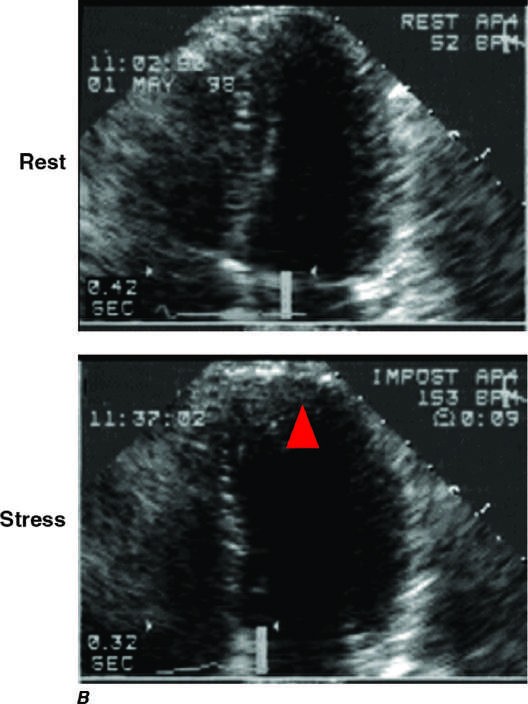
Caption: FIGURE 284-3 Selecting appropriate testing patients with angina and suspected coronary artery disease (CAD). On the left of the figure is an algorithm for selecting from among testing options. In patients who are at low risk, in whom prior testing was equivocal, or in whom the diagnosis of is CAD uncertain, noninvasive functional stress testing with imaging for myocardial ischemia or computed tomography angiography (CTA) is reasonable to establish the diagnosis of CAD prior to initiation of treatment. Patients with a high clinical likelihood of CAD, patients with symptoms despite antianginal therapy or with low-level activities, and patients with high-risk features based on the initial clinical evaluation may proceed directly to invasive coronary angiography without further diagnostic testing. (Adapted from J Knuuti et al: 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 41:407, 2020.) Panels A–F are examples of the data obtained with electrocardiogram (ECG) monitoring and specialized imaging procedures. CMR, cardiac magnetic resonance; EBCT, electron beam computed tomography; ECHO, echocardiography; FFR, fractional flow reserve; IHD, ischemic heart disease; iwFR, instantaneous wave-free ration; MIBI, methoxyisobutyl isonitrite; MR, magnetic resonance; PET, positron emission tomography. A. Lead V at rest (top panel) and after 4.5 min of exercise (bottom panel). There is 3 mm (0.3 mV) of horizontal ST-segment depression, indicating a 4 positive test for ischemia. (Adapted from BR Chaitman, in E Braunwald et al [eds]: Heart Disease, 8th ed, Philadelphia, Saunders, 2008.) B. A 45-year-old avid jogger who began experiencing classic substernal chest pressure underwent an exercise echo study. With exercise, the patient’s heart rate increased from 52 to 153 beats/min. The
Figure 2¶
Caption: FIGURE 284-3 (Continued)
Figure 3¶

Caption: FIGURE 284-3 (Continued)
Figure 4¶

Caption: FIGURE 284-3 (Continued)
Figure 5¶

Caption: FIGURE 284-3 (Continued)
Figure 6¶

Caption: FIGURE 284-2 Cascade of mechanisms and manifestations of ischemia. (Reproduced knowledge. J Am Coll Cardiol 54:1561, 2009.)
Figure 7¶

Caption: reason, methods for detecting coronary calcium have been developed as a measure of the presence of coronary atherosclerosis. These meth- ods involve CT applications that achieve rapid acquisition of images (electron beam [EBCT] and multidetector [MDCT] detection). Coro- nary calcium detected by these imaging techniques most commonly is quantified by using the Agatston score, which is based on the area and density of calcification. FIGURE 284-3 (Continued) in
Figure 8¶

Caption: FIGURE 284-1 Macrocirculation and microcirculation across segments and sizes of the at the top. Vasomotion of the arterial segments occurs in response to the stimuli shown. depiction of the relative resistance to antegrade flow. (Adapted from J Knuuti et al: 2019 Eur Heart J 41:407, 2020/.)
Figure 9¶

Caption: FIGURE 284-1 Macrocirculation and microcirculation across segments and sizes of the at the top. Vasomotion of the arterial segments occurs in response to the stimuli shown. depiction of the relative resistance to antegrade flow. (Adapted from J Knuuti et al: 2019 Eur Heart J 41:407, 2020/.)
Figure 10¶

Caption: FIGURE 284-1 Macrocirculation and microcirculation across segments and sizes of the at the top. Vasomotion of the arterial segments occurs in response to the stimuli shown. depiction of the relative resistance to antegrade flow. (Adapted from J Knuuti et al: 2019 Eur Heart J 41:407, 2020/.)
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.