Chronic Kidney Disease¶
Chapter 322 | Part 9: Disorders of the Kidney and Urinary Tract · Part 9 – Renal & Urinary Tract Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- CKD is defined by a progressive decline in GFR and/or albuminuria, stratified by KDIGO criteria (GFR and Albuminuria).
- Staging (G1-G5) is based on eGFR; Albuminuria (A1-A3) adds risk stratification for mortality and progression.
- eGFR equations (CKD-EPI, MDRD) are preferred over timed collections; race-free equations are recommended but adjustments may be used in specific dosing contexts.
- Leading causes of CKD: Diabetic nephropathy, Glomerulonephritis, Hypertension-associated CKD, ADPKD, Other cystic/tubulointerstitial.
- Uremia involves accumulation of toxins, loss of homeostasis (fluid, electrolytes, hormones), and systemic inflammation.
- Metabolic Acidosis: Common in CKD; treat with oral sodium bicarbonate if serum bicarbonate <20-23 mmol/L.
- Hyperkalemia: Managed by diet, diuretics, and avoiding K+-sparing drugs; RAS inhibitors used cautiously with monitoring.
- Bone Disease: Secondary hyperparathyroidism (high turnover), Adynamic bone disease (low turnover), Osteomalacia (vitamin D deficiency).
- Vascular Calcification: Associated with hyperphosphatemia, low PTH, and high calcium load; independent risk factor for mortality.
- Genetic Factors: APOL1 variants increase risk in African ancestry; Monogenic causes include ADPKD, COL4A3/4/5, UMOD, HNF1B.
- Anemia: Due to reduced EPO production; treated with ESAs and iron.
- Dialysis Indication: Intractable hyperkalemia, volume overload, or uremic symptoms (stage 5 CKD).
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Pathophysiology of CKD
- 1.2 Staging of CKD
- 2. EPIDEMIOLOGY
- 2.1 Risk Factors for CKD
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Leading Categories of Etiologies
- 3.2 Pathophysiology of Uremia
- 4. CLINICAL FEATURES
- 4.1 Fluid, Electrolyte, and Acid-Base Disorders
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Distinguishing CKD from AKI
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Estimation of GFR
- 6.2 Diagnostic Criteria and Staging
- 7. MANAGEMENT & TREATMENT
- 7.1 Pharmacologic Management
- 7.2 Dialysis and Renal Replacement
- 8. PROGNOSIS & COMPLICATIONS
- 8.1 Prognostic Factors
- 9. SPECIAL CONSIDERATIONS
- 9.1 Genetic Risk Factors
- 10. KEY PEARLS & CLINICAL TRAPS
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
Chronic kidney disease (CKD) encompasses a spectrum of pathophysiologic processes associated with abnormal kidney function, often with a progressive decline in glomerular filtration rate (GFR). The risk of worsening CKD is closely linked to the GFR, its trajectory over time, and the quantity of urinary albumin excretion (albuminuria). The dispiriting term end-stage renal disease represents a stage of CKD where the accumulation of toxins, fluid, and electrolytes normally excreted by the kidneys leads to death unless the toxins are removed by renal replacement therapy by means of dialysis or kidney transplantation. End-stage renal disease will be supplanted in this chapter by the term stage 5 CKD.
1.1 Pathophysiology of CKD¶
The pathophysiology of CKD involves two broad mechanisms of damage: - Specific initiating mechanisms particular to the underlying etiology (e.g., genetic abnormalities in development, immune complex deposition, inflammation, metabolic, microvascular perturbation, or toxin exposure affecting vascular, glomerular, or tubulointerstitial compartments of the kidney). - Nonspecific mechanisms involving hyperfiltration and hypertrophy of the remaining viable nephrons, which are common consequences of long-term reduction of renal mass, irrespective of underlying etiology. - Responses to reduction in nephron number are mediated by vasoactive hormones, cytokines, and growth factors. - Eventually, the short-term adaptations of hyperfiltration and hypertrophy to maintain GFR become maladaptive as the increased pressure and flow within the nephron predispose to distortion of glomerular architecture, abnormal podocyte function, and disruption of the filtration barrier, leading to sclerosis and dropout of the remaining nephrons. - Increased intrarenal activity of the renin-angiotensin system (RAS) together with reduced tubuloglomerular feedback appears to contribute both to the initial compensatory hyperfiltration and to the subsequent maladaptive hypertrophy and sclerosis.
1.2 Staging of CKD¶
Staging of CKD is based on both GFR and on urinary albumin excretion rate and is key to understanding the emergence of symptoms, for determining the risk and rate of CKD progression and complications, and for determining indications for medical intervention. - GFR is estimated (eGFR) rather than directly measured, using equations that include serum creatinine concentration and various other individual patient parameters, in place of timed urine collections, which have proven cumbersome and unreliable. - U.S.-based national professional societies have recommended utilizing the equations shown in Table 322-3. - eGFR determination in CKD is valid only if the primary patient is in steady state, that is, the serum creatinine is neither rising nor falling over days. - The newly recommended equations no longer include a parameter that adjusts for differences in creatinine production based on continental ancestry (race-free eGFR estimation equations). However, in some situations where precise estimation of GFR might affect medication dosing or other individual clinical decisions, it is reasonable to include an estimated adjustment based on various parameters that could modify creatinine production downward (e.g., loss of a limb) or upward (increased muscle mass) or, in some cases, revert to measure timed creatinine production rates or use of the more costly and less widely available marker cystatin-C, which is not affected by variables that influence creatinine production. - The normal annual mean decline in GFR with age from the peak GFR (~120 mL/min per 1.73 m2) attained during the third decade of life is ~1 mL/min per year per 1.73 m2, reaching a mean value of 70 mL/min per 1.73 m2 at age 70, with considerable interindividual variability. - Although reduced GFR is expected with aging, the lower GFR signifies a true loss of kidney function with attendant consequences in terms of risk of CKD complications and requirement for dose adjustment of medications. - The mean GFR is lower in women than in men, though men are at greater risk for CKD than women. - A woman in her eighties with a laboratory report of serum creatinine in the normal range may have a GFR of <50 mL/min per 1.73 m2. - Relatedly, even a mild elevation in serum creatinine concentration often signifies a substantial reduction in GFR in older individuals. - It is not entirely clear as yet as to whether advancing age as a risk factor for progressive CKD is independent of such age-related reduction in the measure of eGFR.
2. EPIDEMIOLOGY¶
It has been estimated from population data that at least 6% of the adult population in the United States has CKD at stages 1 and 2. An additional 4.5% of the U.S. population is estimated to have stages 3 and 4 CKD. Table 322-4 lists the five most frequent clinical categories of CKD, cumulatively accounting for >90% of the CKD disease burden worldwide. The relative contribution of each category varies among different geographic regions. The most frequent cause of CKD is diabetic nephropathy, most often secondary to type 2 diabetes mellitus.
2.1 Risk Factors for CKD¶
Adults with such risk factors should be monitored yearly for urinary albumin excretion level, decline in estimated GFR (eGFR), and blood pressure, so that a clinical reno-protective management pathway can be planned. More recently, identified risk factors for which there is now a consensus include tobacco use, increased body mass index (BMI) and sedentary lifestyle, a past episode of clinically recovered acute kidney injury (AKI), and many forms of apparently recovered childhood and adolescent kidney disease. - There is also an increasing awareness of the role of genetic risk factors, which may account for up to 20% of adult-onset CKD, depending on the clinical phenotype, family background, demographic history, and population ancestry. - Many rare inherited forms of CKD follow a Mendelian inheritance pattern, sometimes as part of a systemic syndrome, with the most common in this category being autosomal dominant polycystic kidney disease (ADPKD). - In addition, it is now appreciated that many unique, kindred-specific, site-specific copy number variants and microdeletions, as well as functional single nucleotide variants at >300 genetic loci known to harbor systemic and kidney-only disease pathogenic mutations with high penetrance, also contribute to pleiotropic presentations of CKD. - Many of the genes with identified CKD-causing mutations are expressed in the podocytes of the glomeruli or in the glomerular basement membrane, but others are expressed in tubule segments associated with a primary tubulointerstitial process and secondary glomerular injury. - In addition to these high penetrance mutations, DNA sequence variants with partial penetrance for causation or progression of CKD have been identified and often require an acquired second hit for emergence of disease. - A striking example is the finding of allelic versions of the APOL1 gene, of sub-Saharan African population ancestry, which contributes to the several-fold higher frequency of certain common etiologies of nondiabetic CKD (e.g., focal segmental glomerulosclerosis, HIV- and SARS-CoV-2–associated nephropathy, CKD with hypertension, lupus nephritis) observed among African and Hispanic Americans in major regions of continental Africa and the global African diaspora. - The prevalence in West African populations seems to have arisen as an evolutionary adaptation conferring protection from tropical pathogens. - As in other common diseases with a heritable component, acquired triggers (e.g., increased levels of interferon-γ and other cytokines) can transform genetic risk into disease.
Table 1 — TABLE 322-1 Risk Factors for Chronic Kidney Disease (CKD)¶
| Category | Risk Factor |
|---|---|
| Noncommunicable Diseases | Diabetes |
| Noncommunicable Diseases | Increased BMI |
| Noncommunicable Diseases | Autoinflammatory disease (e.g., lupus, vasculitis, cancer immunotherapy) |
| Noncommunicable Diseases | Nephrotoxic exposure (including many antineoplastic therapies) |
| Noncommunicable Diseases | Hypertension (risk, cause, or consequence) |
| Communicable Diseases | Streptococcal infection |
| Communicable Diseases | Mycobacterial infection |
| Communicable Diseases | HIV infection (HIVAN) |
| Communicable Diseases | SARS-CoV-2 |
| Communicable Diseases | HBV, HCV |
| Demographic, Anthropomorphic, Ancestry, Geographic | Age |
| Demographic, Anthropomorphic, Ancestry, Geographic | Male sex |
| Demographic, Anthropomorphic, Ancestry, Geographic | Population ancestry |
| Demographic, Anthropomorphic, Ancestry, Geographic | Region-specific CKD risk of uncertain etiology (e.g., Central America, Sri Lanka, and indigenous peoples of Australia and New Zealand) |
| Demographic, Anthropomorphic, Ancestry, Geographic | Family history of kidney disease |
| Genetic | Monogenic inheritance with (1) high penetrance or (2) low to medium penetrance |
| Genetic | Polygenic risk factors |
| Childhood-Related Risk Factors | Premature and SGA birth |
| Childhood-Related Risk Factors | Persistent asymptomatic microscopic hematuria |
| Childhood-Related Risk Factors | Childhood kidney disease (even resolved) |
| Childhood-Related Risk Factors | Treated childhood cancer |
| Lifestyle | Tobacco use |
| Lifestyle | Sedentary lifestyle |
| Other | Prior acute kidney injury |
| Other | Preeclampsia |
| Other | Kidney donation (or other acquired nephrectomy) |
Table 2 — TABLE 322-2 Monogenic Risk Loci for Chronic Kidney Disease (CKD)¶
| Copy Number Variants Causative of Congenital Renal Anomalies | Five Most Predominant Causes of CKD with Mendelian Inheritance | Genes for type IV collagen-associated nephropathy | Genes for autosomal dominant tubulointerstitial kidney disease | Genes for nephronophthisis | Other |
|---|---|---|---|---|---|
| 1q21 | Genes for autosomal dominant polycystic kidney disease (ADPKD1, ADPKD2) | COL4A3, COL4A4, COL4A5 | UMOD, MUC1, HNF1B | NPHP genes | Genes with known common variants that confer increased risk with odds ratio exceeding 2 with non-Mendelian inheritance patterns (APOL1) |
| 4p16.1-p16.3 | |||||
| 16p11.2 | |||||
| 16p13.11 | |||||
| 17q12 | |||||
| 22q11.2 |
3. ETIOLOGY & PATHOPHYSIOLOGY¶
The most frequent cause of CKD is diabetic nephropathy, most often secondary to type 2 diabetes mellitus. Patients with newly diagnosed CKD often have hypertension. When no overt evidence for a primary glomerular or tubulointerstitial kidney disease process is present, CKD is frequently attributed to hypertension. However, it is now appreciated that some of these patients may have a subclinical primary glomerulopathy, such as focal segmental or global glomerulosclerosis, and the elevated blood pressure is a consequence of the kidney disease. In other patients, progressive nephrosclerosis and hypertension are the renal correlates of a systemic vascular disease, often also involving large and small vessels elsewhere, such as the heart and brain. This latter combination is especially common in older patients, among whom chronic kidney ischemia as a cause of CKD may be underdiagnosed.
3.1 Leading Categories of Etiologies¶
Table 322-4 lists the five most frequent clinical categories of CKD, cumulatively accounting for >90% of the CKD disease burden worldwide. The relative contribution of each category varies with geographic region and race.
Table 3 — TABLE 322-4 Leading Categories of Etiologies of Chronic Kidney Disease (CKD)¶
| Etiology Category |
|---|
| Diabetic nephropathy |
| Glomerulonephritis |
| Hypertension-associated CKD (includes vascular and ischemic kidney disease and primary glomerular disease with associated hypertension) |
| Autosomal dominant polycystic kidney disease |
| Other cystic and tubulointerstitial nephropathy |
3.2 Pathophysiology of Uremia¶
Uremia is the syndrome with symptoms, signs, and accompanying disturbances in laboratory measurements that result from reduced kidney function. Although serum urea and creatinine concentrations rise with reduced excretory capacity of the kidneys, accumulation of these two molecules themselves does not account for the symptoms and signs that characterize the uremic syndrome. Large numbers of solutes that accumulate when GFR declines have been implicated. These include water-soluble, hydrophobic, protein-bound, charged, and uncharged nitrogen-containing nonvolatile products of metabolism. It is thus evident that the serum concentrations of urea and creatinine should be viewed as being readily measured but very incomplete surrogate markers for retained toxins, and monitoring the levels of urea and creatinine in the patient with impaired kidney function represents a vast oversimplification of the uremic state. - The uremic syndrome involves more than renal excretory failure. A host of metabolic and endocrine functions normally performed by the kidneys are also impaired and can result in anemia, malnutrition, and abnormal metabolism of carbohydrates, fats, and proteins. - Furthermore, plasma levels of many hormones, including PTH, FGF-23, insulin, glucagon, steroid hormones including vitamin D and sex hormones, and prolactin change with CKD as a result of reduced excretion, decreased degradation, or abnormal regulation. - Finally, CKD is associated with increased systemic inflammation. Elevated levels of C-reactive protein are detected along with other acute-phase reactants, whereas levels of so-called negative acute-phase reactants, such as albumin and fetuin, decline. - Thus, the inflammation associated with CKD is important in the malnutrition-inflammation-atherosclerosis/calcification syndrome, which contributes in turn to the acceleration of vascular disease and morbidity associated with advanced kidney disease. - In summary, the pathophysiology of the uremic syndrome can be divided into manifestations in three spheres of dysfunction: (1) those consequent to the accumulation of toxins that normally undergo renal excretion; (2) those consequent to the loss of other kidney functions, such as fluid and electrolyte homeostasis and hormone regulation; and (3) progressive systemic inflammation and its vascular and nutritional consequences.
4. CLINICAL FEATURES¶
Stages 1 and 2 CKD are usually asymptomatic, such that the recognition of CKD occurs more often as a result of laboratory testing in clinical settings other than suspicion of kidney disease. Moreover, in the absence of the risk factors noted above, population-wide screening is not recommended. With progression to CKD stages 3 and 4, clinical and laboratory complications become more prominent. Virtually all organ systems are affected, but the most evident complications include anemia with easy fatigability; decreased appetite with progressive malnutrition; abnormalities in calcium, phosphorus, and mineral-regulating hormones, such as 1,25(OH)D (calcitriol), parathyroid hormone (PTH), and fibroblast growth factor 23 (FGF-23); and abnormalities in sodium, potassium, water, and acid-base homeostasis. Many patients, especially older individuals, will have eGFR values compatible with stage 2 or 3 CKD. However, the majority of these patients will show no further deterioration of kidney function. In this setting, it is advised to recheck kidney function, and if it is stable and not associated with proteinuria, the patient can usually be followed with interval repeat testing without referral to a nephrologist. If repeat testing shows declining GFR, albuminuria, or uncontrolled hypertension, referral to a nephrologist is appropriate. If the patient progresses to stage 5 CKD (GFR <15 mL/min), toxins accumulate such that patients usually experience a disturbance in their activities of daily living, well-being, nutritional status, and water and electrolyte homeostasis, eventuating in the uremic syndrome.
4.1 Fluid, Electrolyte, and Acid-Base Disorders¶
Sodium and Water Homeostasis - With normal kidney function, excretion of filtered sodium and water matches intake. - Many forms of kidney disease disrupt this balance such that dietary intake of sodium exceeds its excretion, leading to sodium retention and attendant extra-cellular fluid volume (ECFV) expansion. - This expansion may contribute to hypertension, which itself can accelerate nephron hyperfiltration and injury. - As long as water intake does not exceed the capacity for renal water clearance, the ECFV expansion will be isonatric and the patient will have a normal plasma sodium concentration. - Hyponatremia is not commonly seen in CKD patients, but when present, often responds to water restriction. - The patient with ECFV expansion should be counseled regarding salt restriction. - While the thiazide diuretic chlorthalidone alone has been shown to reduce elevated blood pressure and in some patients even with stage 4 CKD, administration of loop diuretics, including furosemide, bumetanide, or torsemide, may be needed to manage sodium accumulation. - Resistance to loop diuretics in CKD often mandates use of higher doses than those used in patients with normal GFR. The combination of loop diuretics with metolazone may be helpful. - Diuretic resistance with intractable edema and hypertension in advanced CKD may serve as an indication to initiate dialysis. - Rarely, patients with CKD may have impaired renal conservation of sodium and water. When an extrarenal cause for fluid loss, such as gastrointestinal (GI) loss, is present, these patients may be prone to ECFV depletion because of the inability of the failing kidney to reclaim filtered sodium adequately. - Any depletion of ECFV, whether due to GI losses, renal sodium loss, or overzealous diuretic therapy, can further compromise kidney function through hypoperfusion, or a "prerenal" state, leading to acute-on-chronic kidney failure. - In this setting, holding or adjusting the diuretic dose or rarely even cautious volume repletion with normal saline may return the ECFV to normal and restore renal function to baseline. - Many patients are given a "sick day" warning, wherein should they experience volume depletion, for example from vomiting or diarrhea, they are told to not take their diuretics or other antihypertensive medications until they resume eating and drinking normally.
Potassium Homeostasis - In CKD, the decline in GFR is not necessarily accompanied by a parallel decline in urinary potassium excretion, which is predominantly mediated by aldosterone-dependent secretion in the distal nephron. - Another defense against potassium retention in these patients is augmented potassium excretion in the GI tract. - Notwithstanding these two homeostatic responses, hyperkalemia may be precipitated in certain settings. These include increased dietary potassium intake, hemolysis, transfusion of stored red blood cells, and metabolic acidosis. - Importantly, a host of medications can inhibit renal potassium excretion and lead to hyperkalemia. The most important medications in this respect include the RAS inhibitors and spironolactone and other potassium-sparing diuretics such as amiloride, eplerenone, and triamterene, as well as the new nonsteroidal mineralocorticoid receptor antagonists. - As will be outlined below, several of these are major agents in the medical management armamentarium to slow or prevent progression of CKD. The benefits of the RAS inhibitors in ameliorating hyperfiltration and progression of CKD and mitigating cardiovascular complications very often favor their cautious and judicious use with very close monitoring of plasma potassium concentrations. - Coadministration of potassium-lowering agents may allow for the use of RAS inhibitors with reduced risk of hyperkalemia. - Gratifyingly, the gliflozin diuretics, administrated even in advanced stages of CKD, seem to have counterbalancing effects on kidney potassium handling that result in net preservation of potassium homeostasis. - Certain causes of CKD can be associated with earlier and more severe disruption of potassium secretory mechanisms in the distal nephron, out of proportion to the decline in GFR. These include conditions associated with hyporeninemic hypoaldosteronism, such as diabetes, and renal diseases that preferentially affect the distal nephron, such as obstructive uropathy and sickle cell nephropathy. - Hypokalemia is not common in CKD and usually reflects markedly reduced dietary potassium intake, especially in association with excessive diuretic therapy or concurrent GI losses. - The use of potassium supplements and potassium-sparing diuretics may be risky in patients with impaired renal function and needs to be monitored closely.
Metabolic Acidosis - Metabolic acidosis is a common disturbance in CKD. - The majority of patients can still acidify the urine, but they produce less ammonia and, therefore, cannot excrete the quantity of protons required to maintain acid-base balance in most diets. - Hyperkalemia, if present, further depresses ammonia production. - The combination of hyperkalemia and hyperchloremic metabolic acidosis is often present, even at earlier stages of CKD, in patients with diabetic nephropathy or in those with predominant tubulointerstitial disease including obstructive uropathy. - With further declining GFR, the total urinary net daily acid excretion may be severely limited to <30–40 mmol, and the accumulation of anions of retained organic acids can then lead to an anion-gap metabolic acidosis. - Thus, the non-anion-gap metabolic acidosis seen in earlier stages of CKD may be complicated by the addition of an anion-gap metabolic acidosis as CKD progresses. - In most patients, the metabolic acidosis is mild; the pH is rarely <7.32 and can usually be corrected with oral sodium bicarbonate supplementation. - Studies have suggested that even modest degrees of metabolic acidosis may be associated with the development of protein catabolism and progression of CKD. - Recent studies suggest that bicarbonate supplementation in stages 3–5 CKD was also associated with slower progression to dialysis. - The sodium load in sodium bicarbonate supplementation needs to be taken into account when ECFV expansion is present.
5. DIFFERENTIAL DIAGNOSIS¶
The differential diagnosis of CKD primarily involves distinguishing the underlying etiology (e.g., diabetic nephropathy, glomerulonephritis, hypertension-associated CKD, ADPKD, other cystic and tubulointerstitial nephropathy) and distinguishing CKD from acute kidney injury (AKI) or prerenal azotemia. Prerenal azotemia, with the exception of the cardiorenal and hepatorenal syndromes, and postrenal azotemia carry a better prognosis than most cases of intrinsic AKI. The kidneys may recover even after severe, dialysis-requiring AKI. Survivors of an episode of AKI requiring temporary dialysis, however, are at extremely high risk for progressive CKD, and up to 10% may develop ESKD requiring dialysis or transplantation. AKI and CKD are increasingly seen as interrelated and syndromes: CKD is a major risk factor for the development of AKI, and AKI is a risk factor for the future development of CKD. Measurement of albuminuria after an AKI episode can help predict the risk of kidney disease progression and can serve as a valuable risk-stratification tool.
5.1 Distinguishing CKD from AKI¶
- CKD is defined by a progressive decline in GFR and/or albuminuria.
- AKI is defined by an abrupt decrease in GFR (e.g., increase in serum creatinine by ≥0.3 mg/dL within 48 hours or ≥1.5 times baseline within 7 days).
- Measurement of albuminuria after an AKI episode can help predict the risk of kidney disease progression.
- Postdischarge care after AKI under the supervision of a nephrologist for aggressive secondary prevention of kidney disease is prudent.
6. INVESTIGATIONS & DIAGNOSIS¶
Measurement of albuminuria is also helpful for monitoring nephron injury and the response to therapy in many forms of CKD, especially chronic glomerular diseases. The cumbersome 24-h urine collection has been replaced by measurement of urinary albumin-to-creatinine ratio (UACR) in one and preferably several spot first-morning urine samples as a measure pointing to glomerular injury. Even in patients with negative conventional urinary dipstick tests for protein, persistent UACR >2.5 mg/mmol (male) or >3.5 mg/mmol (female) on two to three occasions serves as a marker not only for early detection of kidney disease but for systemic microvascular disease as well. A Kidney Failure Risk (KFR) equation has been devised to predict the risk of progression to stage 5 dialysis-dependent kidney disease. The equation is available on many sites online (for example, www.kidneyfailurerisk.com) and uses age, sex, region (North American or non–North American), GFR, and UACR. It has been validated in several cohorts around the world, although the risk for progression appears to be greater in North America, accounting for the regional adjustment in the equation.
6.1 Estimation of GFR¶
GFR is estimated (eGFR) rather than directly measured, using equations that include serum creatinine concentration and various other individual patient parameters, in place of timed urine collections, which have proven cumbersome and unreliable. - U.S.-based national professional societies have recommended utilizing the equations shown in Table 322-3. - eGFR determination in CKD is valid only if the primary patient is in steady state, that is, the serum creatinine is neither rising nor falling over days. - The newly recommended equations no longer include a parameter that adjusts for differences in creatinine production based on continental ancestry (race-free eGFR estimation equations). However, in some situations where precise estimation of GFR might affect medication dosing or other individual clinical decisions, it is reasonable to include an estimated adjustment based on various parameters that could modify creatinine production downward (e.g., loss of a limb) or upward (increased muscle mass) or, in some cases, revert to measure timed creatinine production rates or use of the more costly and less widely available marker cystatin-C, which is not affected by variables that influence creatinine production.
Table 4 — TABLE 322-3 Recommended Equations for Estimation of Glomerular Filtration Rate (GFR) Using Serum Creatinine Concentration (SCr), Age, Sex, Race, and Body Weight¶
| Equation | Formula | Adjustments |
|---|---|---|
| Modification of Diet in Renal Disease (MDRD) Study | Estimated GFR (mL/min per 1.73 m2) = 1.86 × (SCr)−1.154 × (age)−0.203 | Multiply by 0.742 for women Multiply by 1.21 for African ancestry (currently under review) |
| CKD-EPI Equation | GFR = 141 × min(SCr/kappa, 1)α × max(SCr/kappa, 1)–1.209 × 0.993Age | Multiply by 1.018 for women Multiply by 1.159 for African ancestry (currently under review) where SCr is serum creatinine in mg/dL, kappa is 0.7 for females and 0.9 for males, α is –0.329 for females and –0.411 for males, min indicates the minimum of SCr/kappa or 1, and max indicates the maximum of SCr/kappa or 1. |
6.2 Diagnostic Criteria and Staging¶
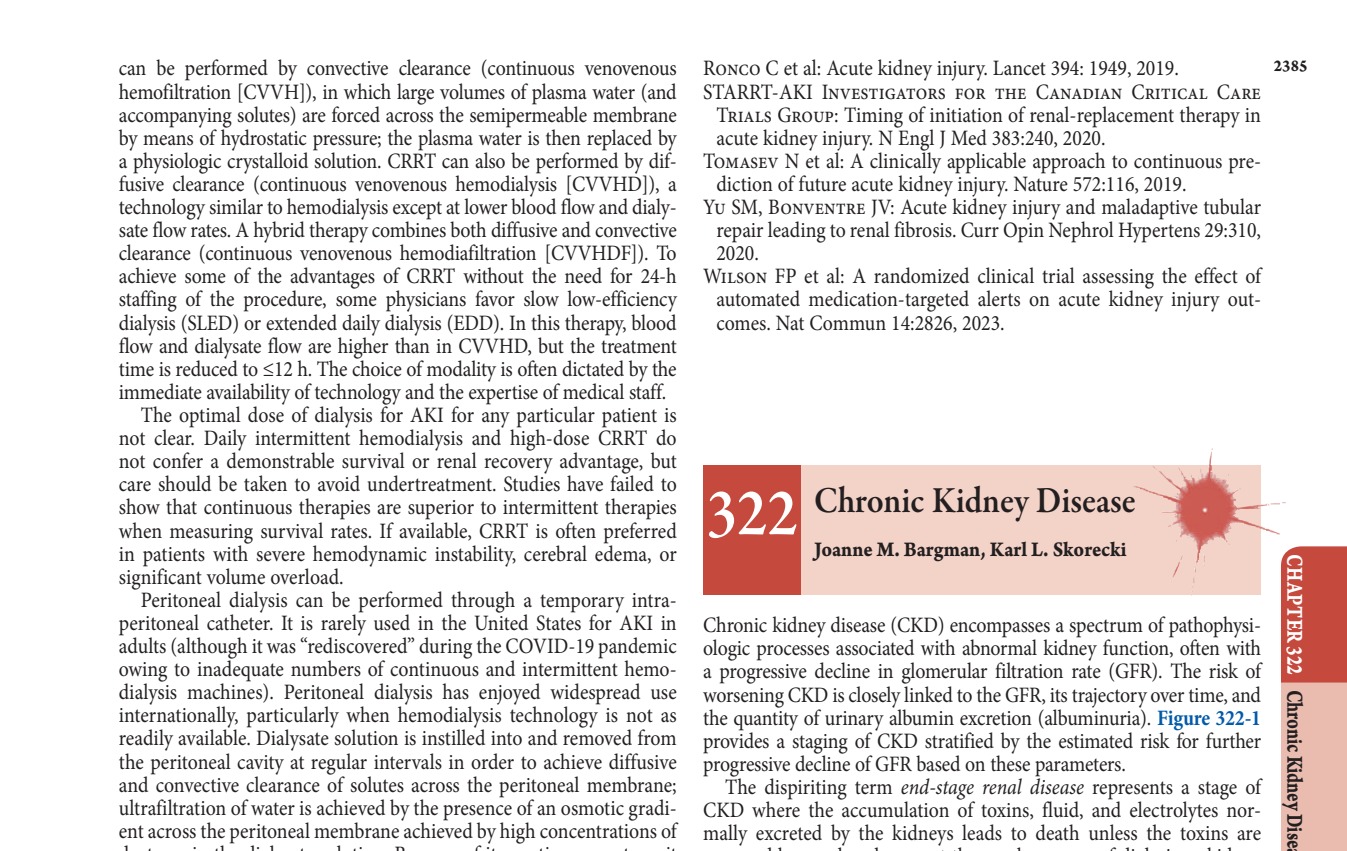
Staging of CKD (Fig. 322-1) is based on both GFR and on urinary albumin excretion rate and is key to understanding the emergence of symptoms, for determining the risk and rate of CKD progression and complications, and for determining indications for medical intervention. - GFR categories (G1-G5) are defined by eGFR thresholds. - Albuminuria categories (A1-A3) are defined by UACR thresholds. - Figure 322-1 illustrates the KDIGO classification of CKD, showing that Glomerular filtration rate (GFR) and Increasing albuminuria correspond to increasing risk of All-Cause Mortality, Cardiovascular Mortality, and Progression of CKD.
7. MANAGEMENT & TREATMENT¶
Treatment of CKD focuses on slowing progression, managing complications, and treating the underlying cause. Management includes dietary modifications, pharmacologic therapy, and monitoring. - Dietary salt restriction and the use of loop diuretics, occasionally in combination with metolazone, may be needed to maintain euvolemia. Water restriction is indicated only if there is hyponatremia. - Hyperkalemia often responds to dietary restriction of potassium, the use of kaliuretic diuretics, and both avoidance of potassium supplements (including occult sources, such as dietary salt substitutes) and monitoring with dose adjustment, or at times avoidance of potassium-retaining medications, which are often prescribed to slow CKD progression or afford cardioprotection (RAS inhibitors, steroidal or nonsteroidal mineralocorticoid antagonists). - Kaliuretic diuretics promote urinary potassium excretion, whereas potassium-sparing diuretics promote potassium loss through the GI tract and may reduce the incidence of hyperkalemia. - Intractable hyperkalemia is an indication (although uncommon) to consider institution of dialysis in a CKD patient. - Metabolic acidosis can usually be corrected with oral sodium bicarbonate supplementation. Recent studies suggest that bicarbonate supplementation in stages 3–5 CKD was also associated with slower progression to dialysis. - Calcium, Phosphorus, and the Cardiovascular System: There is a strong association between hyperphosphatemia and increased cardiovascular mortality in patients with CKD. Hyperphosphatemia and hypercalcemia are associated with increased vascular calcification, but it is unclear whether the excessive mortality is mediated by this mechanism. Studies using computed tomography (CT) and electron-beam CT scanning show that CKD patients have calcification in the media of coronary arteries and heart valves that appears to be orders of magnitude greater than that in patients without kidney disease. The magnitude of the calcification is proportional to age and hyperphosphatemia and is also associated with low PTH levels and low bone turnover. It is possible that in CKD patients, ingested calcium cannot be incorporated into bones with low turnover, and therefore, is deposited at the soft tissues. - Bone Manifestations of CKD: The major disorders of bone disease can be classified into those associated with high bone turnover with increased PTH levels (including osteitis fibrosa cystica, the classic lesion of secondary hyperparathyroidism), osteomalacia due to reduced vitamin D effect, and low bone turnover with low or normal PTH levels (adynamic bone disease) or often some combination of the foregoing. - The pathophysiology of secondary hyperparathyroidism and the consequent high-turnover bone disease is related to abnormal mineral metabolism through the following series of interrelated mechanisms: (1) declining GFR leads to reduced excretion of phosphate and, thus, phosphate retention; (2) the retained phosphate stimulates increased synthesis of both FGF-23 by osteocytes and of PTH and also stimulates growth of parathyroid gland mass; and (3) decreased levels of ionized calcium, which results from decreased levels of renal calcitriol production due to phosphate retention and elevated levels of FGF-23, which also increases degradation of calcitriol. Low calcitriol levels contribute to hyperparathyroidism, both by leading to hypocalcemia and also by a direct effect on PTH gene transcription. In addition, the normal inhibitory effect of FGF-23 on PTH production, which is Klotho-dependent, is also attenuated in CKD. These changes start to occur when the GFR falls below 60 mL/min, though some studies point to retention of phosphate as an event antedating measurable reduction in GFR, together with early elevation of FGF-23 as well. - FGF-23 is part of a family of phosphatonins that promotes phosphate excretion, and high levels of FGF-23 are an independent risk factor for left ventricular hypertrophy and are associated with increased mortality in CKD, dialysis, and kidney transplant patients. - Hyperparathyroidism stimulates bone turnover and leads to osteitis fibrosa cystica. Bone histology shows abnormal osteoid, bone and bone marrow fibrosis, and, in advanced stages, the formation of bone cysts, sometimes with hemorrhagic elements so that they appear brown in color; hence, the term brown tumor. Clinical manifestations of severe hyperparathyroidism include bone pain and fragility, brown tumors with compression syndromes, and resistance to erythropoiesis-stimulating agents (ESA) in part related to the bone marrow fibrosis. - Furthermore, PTH itself is considered a uremic toxin, and high levels are associated with muscle weakness, fibrosis of cardiac muscle, and constitutional symptoms. - Adynamic bone disease is increasing in prevalence, especially among diabetics and older patients. It is characterized by reduced bone volume and mineralization and may result from excessive suppression of PTH production, chronic inflammation, or both. Suppression of PTH can result from the use of vitamin D preparations or from excessive calcium exposure in the form of calcium-containing phosphate binding resins, such as calcium resonium, sodium polystyrene, or the newer agents patiromer and calcium zirconium cyclosilicate, promote potassium loss through the GI tract and may reduce the incidence of hyperkalemia. - Complications of adynamic bone disease include an increased incidence of fracture and bone pain and an association with increased vascular and cardiac calcification. Occasionally, the calcium will precipitate in the soft tissues into large concretions termed tumoral calcinosis (Fig. 322-3). Patients with adynamic bone disease often experience the most severe symptoms of musculoskeletal pain, owing to the inability to repair the microfractures that occur normally as a part of healthy skeletal homeostasis with regular physical activity. - Patients with advanced CKD experience more frequent fractures than their age-matched controls. Osteomalacia is a distinct process, consequent to reduced production and action of 1,25(OH)D, leading to the accumulation of nonmineralized osteoid. - Tenapanor is a sodium-proton inhibitor that decreases GI phosphate absorption and may be useful to manage hyperphosphatemia in CKD and dialysis patients. - Calcitriol exerts a direct suppressive effect on PTH secretion and also indirectly suppresses PTH secretion by raising the concentration of ionized calcium. However, calcitriol therapy may result in hypercalcemia and/or hyperphosphatemia through increased GI absorption of these minerals. Certain analogues of calcitriol are available (e.g., paricalcitol) that suppress PTH secretion with less attendant hypercalcemia. - Recognition of the role of the extracellular calcium-sensing receptor has led to the development of calcimimetic agents that enhance the sensitivity of parathyroid cells to the suppressive effect of calcium. This class of drug, which includes cinacalcet and etelcalcetide, produces a dose-dependent reduction in PTH and plasma calcium concentration in some patients. - Current National Kidney Foundation KDOQI guidelines recommend that phosphate binders be used to maintain serum phosphorus levels within the normal range for age and race.
7.1 Pharmacologic Management¶
- RAS Inhibitors: The benefits of the RAS inhibitors in ameliorating hyperfiltration and progression of CKD and mitigating cardiovascular complications very often favor their cautious and judicious use with very close monitoring of plasma potassium concentrations. Coadministration of potassium-lowering agents may allow for the use of RAS inhibitors with reduced risk of hyperkalemia.
- Gliflozin Diuretics: The gliflozin diuretics, administrated even in advanced stages of CKD, seem to have counterbalancing effects on kidney potassium handling that result in net preservation of potassium homeostasis.
- Phosphate Binders: Calcium, calcium-containing phosphate binding resins (calcium resonium, sodium polystyrene), and newer agents (patiromer, calcium zirconium cyclosilicate) promote potassium loss through the GI tract and may reduce the incidence of hyperkalemia. Tenapanor is a sodium-proton inhibitor that decreases GI phosphate absorption and may be useful to manage hyperphosphatemia in CKD and dialysis patients.
- Vitamin D Analogs: Calcitriol exerts a direct suppressive effect on PTH secretion and also indirectly suppresses PTH secretion by raising the concentration of ionized calcium. However, calcitriol therapy may result in hypercalcemia and/or hyperphosphatemia through increased GI absorption of these minerals. Certain analogues of calcitriol are available (e.g., paricalcitol) that suppress PTH secretion with less attendant hypercalcemia.
- Calcimimetics: Recognition of the role of the extracellular calcium-sensing receptor has led to the development of calcimimetic agents that enhance the sensitivity of parathyroid cells to the suppressive effect of calcium. This class of drug, which includes cinacalcet and etelcalcetide, produces a dose-dependent reduction in PTH and plasma calcium concentration in some patients.
- Bicarbonate Supplementation: Metabolic acidosis can usually be corrected with oral sodium bicarbonate supplementation. Recent studies suggest that bicarbonate supplementation in stages 3–5 CKD was also associated with slower progression to dialysis. The sodium load in sodium bicarbonate supplementation needs to be taken into account when ECFV expansion is present.
7.2 Dialysis and Renal Replacement¶
- Continuous Renal Replacement Therapy (CRRT) can be performed by convective clearance (continuous venovenous hemofiltration [CVVH]), in which large volumes of plasma water (and accompanying solutes) are forced across the semipermeable membrane by means of hydrostatic pressure; the plasma water is then replaced by a physiologic crystalloid solution. CRRT can also be performed by diffusive clearance (continuous venovenous hemodialysis [CVVHD]), a technology similar to hemodialysis except at lower blood flow and dialysate flow rates. A hybrid therapy combines both diffusive and convective clearance (continuous venovenous hemodiafiltration [CVVHDF]).
- To achieve some of the advantages of CRRT without the need for 24-h staffing of the procedure, some physicians favor slow low-efficiency automated dialysis (SLED) or extended daily dialysis (EDD). In this therapy, blood flow and dialysate flow are higher than in CVVHD, but the treatment time is reduced to ≤12 h. The choice of modality is often dictated by the immediate availability of technology and the expertise of medical staff.
- The optimal dose of dialysis for AKI for any particular patient is not clear. Daily intermittent hemodialysis and high-dose CRRT do not confer a demonstrable survival or renal recovery advantage, but care should be taken to avoid undertreatment. Studies have failed to show that continuous therapies are superior to intermittent therapies when measuring survival rates. If available, CRRT is often preferred in patients with severe hemodynamic instability, cerebral edema, or significant volume overload.
- Peritoneal dialysis can be performed through a temporary intraperitoneal catheter. It is rarely used in the United States for AKI in adults (although it was "rediscovered" during the COVID-19 pandemic owing to inadequate numbers of continuous and intermittent hemodialysis machines). Peritoneal dialysis has enjoyed widespread use internationally, particularly when hemodialysis technology is not as readily available. Dialysate solution is instilled into and removed from the peritoneal cavity at regular intervals in order to achieve diffusive and convective clearance of solutes across the peritoneal membrane; ultrafiltration of water is achieved by the presence of an osmotic gradient across the peritoneal membrane achieved by high concentrations of dextrose in the dialysate solution. Because of its continuous nature, it is often better tolerated than intermittent procedures like hemodialysis in hypotensive patients. Peritoneal dialysis may not be sufficient for hypercatabolic patients due to inherent limitations in dialysis efficacy.
- Diuretic resistance with intractable edema and hypertension in advanced CKD may serve as an indication to initiate dialysis.
- Intractable hyperkalemia is an indication (although uncommon) to consider institution of dialysis in a CKD patient.
8. PROGNOSIS & COMPLICATIONS¶
The development of AKI is associated with a significantly increased risk of in-hospital and long-term mortality, longer length of stay, and increased costs. AKI is also associated with an increased risk of later cardiovascular disease events, though the mechanisms are not well understood. Prerenal azotemia, with the exception of the cardiorenal and hepatorenal syndromes, and postrenal azotemia carry a better prognosis than most cases of intrinsic AKI. The kidneys may recover even after severe, dialysis-requiring AKI. Survivors of an episode of AKI requiring temporary dialysis, however, are at extremely high risk for progressive CKD, and up to 10% may develop ESKD requiring dialysis or transplantation. AKI and CKD are increasingly seen as interrelated and syndromes: CKD is a major risk factor for the development of AKI, and AKI is a risk factor for the future development of CKD. Measurement of albuminuria after an AKI episode can help predict the risk of kidney disease progression and can serve as a valuable risk-stratification tool. - Figure 322-1 illustrates the KDIGO classification of CKD, showing that Glomerular filtration rate (GFR) and Increasing albuminuria correspond to increasing risk of All-Cause Mortality, Cardiovascular Mortality, and Progression of CKD. - High levels of FGF-23 are an independent risk factor for left ventricular hypertrophy and are associated with increased mortality in CKD, dialysis, and kidney transplant patients. - Hyperparathyroidism stimulates bone turnover and leads to osteitis fibrosa cystica. Bone histology shows abnormal osteoid, bone and bone marrow fibrosis, and, in advanced stages, the formation of bone cysts, sometimes with hemorrhagic elements so that they appear brown in color; hence, the term brown tumor. Clinical manifestations of severe hyperparathyroidism include bone pain and fragility, brown tumors with compression syndromes, and resistance to erythropoiesis-stimulating agents (ESA) in part related to the bone marrow fibrosis. - Adynamic bone disease is increasing in prevalence, especially among diabetics and older patients. It is characterized by reduced bone volume and mineralization and may result from excessive suppression of PTH production, chronic inflammation, or both. Complications of adynamic bone disease include an increased incidence of fracture and bone pain and an association with increased vascular and cardiac calcification. - Patients with advanced CKD experience more frequent fractures than their age-matched controls. Osteomalacia is a distinct process, consequent to reduced production and action of 1,25(OH)D, leading to the accumulation of nonmineralized osteoid. - There is a strong association between hyperphosphatemia and increased cardiovascular mortality in patients with CKD. Hyperphosphatemia and hypercalcemia are associated with increased vascular calcification, but it is unclear whether the excessive mortality is mediated by this mechanism. Studies using computed tomography (CT) and electron-beam CT scanning show that CKD patients have calcification in the media of coronary arteries and heart valves that appears to be orders of magnitude greater than that in patients without kidney disease. The magnitude of the calcification is proportional to age and hyperphosphatemia and is also associated with low PTH levels and low bone turnover.
8.1 Prognostic Factors¶
- GFR and Albuminuria: Figure 322-1 illustrates the KDIGO classification of CKD, showing that Glomerular filtration rate (GFR) and Increasing albuminuria correspond to increasing risk of All-Cause Mortality, Cardiovascular Mortality, and Progression of CKD.
- FGF-23: High levels of FGF-23 are an independent risk factor for left ventricular hypertrophy and are associated with increased mortality in CKD, dialysis, and kidney transplant patients.
- AKI History: Survivors of an episode of AKI requiring temporary dialysis are at extremely high risk for progressive CKD, and up to 10% may develop ESKD requiring dialysis or transplantation.
- Inflammation: CKD is associated with increased systemic inflammation. Elevated levels of C-reactive protein are detected along with other acute-phase reactants, whereas levels of so-called negative acute-phase reactants, such as albumin and fetuin, decline. Thus, the inflammation associated with CKD is important in the malnutrition-inflammation-atherosclerosis/calcification syndrome, which contributes in turn to the acceleration of vascular disease and morbidity associated with advanced kidney disease.
9. SPECIAL CONSIDERATIONS¶
- Genetic Factors: There is also an increasing awareness of the role of genetic risk factors, which may account for up to 20% of adult-onset CKD, depending on the clinical phenotype, family background, demographic history, and population ancestry. Many rare inherited forms of CKD follow a Mendelian inheritance pattern, sometimes as part of a systemic syndrome, with the most common in this category being autosomal dominant polycystic kidney disease (ADPKD). In addition, it is now appreciated that many unique, kindred-specific, site-specific copy number variants and microdeletions, as well as functional single nucleotide variants at >300 genetic loci known to harbor systemic and kidney-only disease pathogenic mutations with high penetrance, also contribute to pleiotropic presentations of CKD. Many of the genes with identified CKD-causing mutations are expressed in the podocytes of the glomeruli or in the glomerular basement membrane, but others are expressed in tubule segments associated with a primary tubulointerstitial process and secondary glomerular injury. In addition to these high penetrance mutations, DNA sequence variants with partial penetrance for causation or progression of CKD have been identified and often require an acquired second hit for emergence of disease. A striking example is the finding of allelic versions of the APOL1 gene, of sub-Saharan African population ancestry, which contributes to the several-fold higher frequency of certain common etiologies of nondiabetic CKD (e.g., focal segmental glomerulosclerosis, HIV- and SARS-CoV-2–associated nephropathy, CKD with hypertension, lupus nephritis) observed among African and Hispanic Americans in major regions of continental Africa and the global African diaspora. The prevalence in West African populations seems to have arisen as an evolutionary adaptation conferring protection from tropical pathogens. As in other common diseases with a heritable component, acquired triggers (e.g., increased levels of interferon-γ and other cytokines) can transform genetic risk into disease.
- Pregnancy: Preeclampsia is listed as a risk factor in Table 322-1. The text notes that certain causes of CKD can be associated with earlier and more severe disruption of potassium secretory mechanisms in the distal nephron, out of proportion to the decline in GFR. These include conditions associated with hyporeninemic hypoaldosteronism, such as diabetes, and renal diseases that preferentially affect the distal nephron, such as obstructive uropathy and sickle cell nephropathy.
- Pediatric/Childhood-Related: Childhood-Related Risk Factors include Premature and SGA birth, Persistent asymptomatic microscopic hematuria, Childhood kidney disease (even resolved), and Treated childhood cancer.
9.1 Genetic Risk Factors¶
- APOL1: A striking example is the finding of allelic versions of the APOL1 gene, of sub-Saharan African population ancestry, which contributes to the several-fold higher frequency of certain common etiologies of nondiabetic CKD (e.g., focal segmental glomerulosclerosis, HIV- and SARS-CoV-2–associated nephropathy, CKD with hypertension, lupus nephritis) observed among African and Hispanic Americans in major regions of continental Africa and the global African diaspora.
- Monogenic Inheritance: Many rare inherited forms of CKD follow a Mendelian inheritance pattern, sometimes as part of a systemic syndrome, with the most common in this category being autosomal dominant polycystic kidney disease (ADPKD). In addition, it is now appreciated that many unique, kindred-specific, site-specific copy number variants and microdeletions, as well as functional single nucleotide variants at >300 genetic loci known to harbor systemic and kidney-only disease pathogenic mutations with high penetrance, also contribute to pleiotropic presentations of CKD.
- Gene Expression: Many of the genes with identified CKD-causing mutations are expressed in the podocytes of the glomeruli or in the glomerular basement membrane, but others are expressed in tubule segments associated with a primary tubulointerstitial process and secondary glomerular injury.
- Acquired Triggers: As in other common diseases with a heritable component, acquired triggers (e.g., increased levels of interferon-γ and other cytokines) can transform genetic risk into disease.
10. KEY PEARLS & CLINICAL TRAPS¶
- eGFR Validity: eGFR determination in CKD is valid only if the primary patient is in steady state, that is, the serum creatinine is neither rising nor falling over days.
- Race-Free Equations: The newly recommended equations no longer include a parameter that adjusts for differences in creatinine production based on continental ancestry (race-free eGFR estimation equations). However, in some situations where precise estimation of GFR might affect medication dosing or other individual clinical decisions, it is reasonable to include an estimated adjustment based on various parameters that could modify creatinine production downward (e.g., loss of a limb) or upward (increased muscle mass) or, in some cases, revert to measure timed creatinine production rates or use of the more costly and less widely available marker cystatin-C, which is not affected by variables that influence creatinine production.
- UACR Thresholds: Even in patients with negative conventional urinary dipstick tests for protein, persistent UACR >2.5 mg/mmol (male) or >3.5 mg/mmol (female) on two to three occasions serves as a marker not only for early detection of kidney disease but for systemic microvascular disease as well.
- Metabolic Acidosis Treatment: Recent studies suggest that bicarbonate supplementation in stages 3–5 CKD was also associated with slower progression to dialysis. The sodium load in sodium bicarbonate supplementation needs to be taken into account when ECFV expansion is present.
- Hyperkalemia Management: Coadministration of potassium-lowering agents may allow for the use of RAS inhibitors with reduced risk of hyperkalemia. The gliflozin diuretics, administrated even in advanced stages of CKD, seem to have counterbalancing effects on kidney potassium handling that result in net preservation of potassium homeostasis.
- Intractable Hyperkalemia: Intractable hyperkalemia is an indication (although uncommon) to consider institution of dialysis in a CKD patient.
- Adynamic Bone Disease: Complications of adynamic bone disease include an increased incidence of fracture and bone pain and an association with increased vascular and cardiac calcification. Occasionally, the calcium will precipitate in the soft tissues into large concretions termed tumoral calcinosis (Fig. 322-3). Patients with adynamic bone disease often experience the most severe symptoms of musculoskeletal pain, owing to the inability to repair the microfractures that occur normally as a part of healthy skeletal homeostasis with regular physical activity.
- Tumoral Calcinosis: Patients with adynamic bone disease often experience the most severe symptoms of musculoskeletal pain, owing to the inability to repair the microfractures that occur normally as a part of healthy skeletal homeostasis with regular physical activity. Occasionally, the calcium will precipitate in the soft tissues into large concretions termed tumoral calcinosis (Fig. 322-3).
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶

Caption: FIGURE 322-1 Kidney Disease Improving Global Outcome (KDIGO) classification of albuminuria correspond to increasing risk of All-Cause Mortality (A), Cardiovascular JAMA 330:1266, 2023.) Adults with such risk factors should be monitored yearly for urinary albumin excretion level, decline in estimated GFR (eGFR), and blood pressure, so that a clinical reno-protective management pathway can be planned. More recently, identified risk factors for which there is now a consensus include tobacco use, increased body mass index (BMI) and sedentary lifestyle, a past episode of clinically recovered acute kidney injury (AKI), and many forms of apparently recovered childhood and — FIGURE 322-1 KDIGO classification of chronic kidney disease (CKD). Glomerular filtration rate (GFR) and increasing albuminuria correspond to increasing risk of All-Cause Mortality, Cardiovascular Mortality, and Progression of CKD. Stages are defined by GFR categories (G1-G5) and Albuminuria categories (A1-A3).
Figure 2¶
Caption: Kidney Disease Figure 322-1 risk for further a stage of electrolytes nor- the toxins are dialysis or kidney Chaps. 323 and chapter by the — FIGURE 322-2 Schematic representation of the effect of intraglomerular hypertension on nephron survival. Shows Ang II constricting afferent arteriole leading to increased intraglomerular pressure, causing glomerular injury and sclerosis.
Figure 3¶

Caption: FIGURE 322-2 Schematic representation of the effect of intraglomerular hypertension on — FIGURE 322-3 Tumoral calcinosis. Clinical photograph of a patient on hemodialysis with a large, extensively calcified, enlarging painful mass on the arm due to chronic severe hyperphosphatemia and nonadherence to dietary restrictions.
Figure 4¶

Caption: FIGURE 322-5 The postulated role of the gliflozins in generating tubuloglomerular from DZ Cherney et al: Cherney et al: Circulation 129:587, 2014.) — FIGURE 322-4 (Implied from text context regarding fluid/electrolyte): Schematic of sodium and water homeostasis disruption in CKD leading to ECFV expansion and hypertension.
Figure 5¶

Caption: FIGURE 322-4 Calciphylaxis. This peritoneal dialysis patient was on chronic warfarin therapy for atrial fibrillation. She noticed a small painful nodule on the abdomen that was followed by progressive skin necrosis and ulceration of the anterior abdominal wall. She was treated with hyperbaric oxygen, intravenous thiosulfate, and discontinuation of warfarin, with slow resolution of the ulceration. extraosseous sites, such as the vascular bed and soft tissues. There is a similar association between osteoporosis and vascular calcification in the general population. Finally, hyperphosphatemia can induce a — FIGURE 322-5 (Implied from text context regarding bone): Histology or schematic of bone manifestations in CKD (Osteitis fibrosa cystica, Adynamic bone disease, Osteomalacia).
Figure 6¶

Caption: FIGURE 322-3 Tumoral calcinosis. This patient was on hemodialysis for many years and was nonadherent to dietary phosphorus restriction or the use of phosphate binders. He was chronically severely hyperphosphatemic. He developed an of enlarging painful mass on his arm that was extensively calcified. — FIGURE 322-6 (Implied from text context regarding vascular): CT or schematic showing vascular calcification in coronary arteries and heart valves in CKD patients compared to non-CKD.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.