Chapter 281 | Pericardial Disease¶
Part 6: Disorders of the Cardiovascular System · Part 6 – Cardiovascular Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- Acute pericarditis is defined by four principal features: chest pain, pericardial friction rub, ECG changes (ST elevation, PR depression), and pericardial effusion.
- Differentiation from AMI is critical: Pericarditis shows diffuse ST elevation with PR depression, whereas AMI shows convex ST elevation with reciprocal depression.
- Cardiac tamponade is diagnosed by Beck's triad (hypotension, JVD, soft heart sounds) and pulsus paradoxus (>10 mmHg inspiratory decline in systolic BP).
- Constrictive pericarditis is characterized by an M-shaped jugular venous pulse (prominent x and y descents) and square root sign in ventricular pressure pulses.
- Treatment of acute idiopathic pericarditis involves NSAIDs (aspirin, ibuprofen, indomethacin) plus colchicine (3 months).
- Glucocorticoids are reserved for refractory cases or contraindications to NSAIDs/colchicine due to higher recurrence risk.
- Pericardiocentesis is indicated for tamponade; subxiphoid approach is preferred.
- Pericardiectomy is the treatment of choice for chronic constrictive pericarditis.
- Uremic pericarditis is associated with severe renal dysfunction and may require intensified dialysis or pericardial window.
- Neoplastic pericarditis requires cytology of pericardial fluid and often biopsy for diagnosis.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Normal Functions of the Pericardium
- 1.2 Classification of Pericarditis
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Pathophysiology of Cardiac Tamponade
- 3.2 Pathophysiology of Constrictive Pericarditis
- 4. CLINICAL FEATURES
- 4.1 Acute Pericarditis Symptoms
- 4.2 Physical Examination Findings
- 5. DIFFERENTIAL DIAGNOSIS
- 5.1 Differentiation from AMI
- 5.2 Differentiation of Tamponade vs Constriction
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Electrocardiographic Findings
- 6.2 Echocardiographic Findings
- 7. MANAGEMENT & TREATMENT
- 7.1 Treatment of Acute Pericarditis
- 7.2 Treatment of Cardiac Tamponade
- 7.3 Treatment of Constrictive Pericarditis
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 9.1 Uremic Pericarditis
- 9.2 Neoplastic Pericarditis
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
| # | Type | Description |
|---|---|---|
| 1 | 🔀 Flowchart | Constrictive pericarditis |
| 1 | 🖼 Figure | A |
| 2 | 🖼 Figure | Pericardial inflammation by cardiac magnetic resonance imaging |
| 3 | 🖼 Figure | Figure / Illustration |
1. DEFINITION & OVERVIEW¶
The pericardium is a double-layered sac consisting of the visceral pericardium (serous membrane) and the parietal pericardium (fibrous sac). The normal pericardium exerts a restraining force to prevent sudden dilation of cardiac chambers, restricts anatomic position, and retards spread of infections. Acute pericarditis is the most common pathologic process involving the pericardium. It is characterized by inflammation of the pericardial layers. Chronic pericardial disease includes constrictive pericarditis and chronic pericardial effusions.
1.1 Normal Functions of the Pericardium¶
- The normal pericardium is a double-layered sac of the visceral pericardium and parietal pericardium.
- The visceral pericardium is a serous membrane separated from the fibrous parietal pericardium by a small quantity (15–50 mL) of fluid, an ultrafiltrate of plasma.
- The normal pericardium exerts a restraining force to prevent sudden dilation of the cardiac chambers, especially the right atrium and ventricle, e.g., during exercise.
- It restricts the anatomic position of the heart.
- It likely retards the spread of infections from the lungs and pleural cavities to the heart.
- Total absence of the pericardium, either congenital or after surgery, does not produce obvious clinical disease.
- Partial left pericardial defects may allow the main pulmonary artery and left atrium to bulge through the defect; rarely, herniation and subsequent strangulation of the left atrium may cause sudden death.
1.2 Classification of Pericarditis¶
Harrison's defines the classification of pericarditis as follows: - Clinical Classification: - I. Acute pericarditis (6 months) - A. Constrictive - B. Adhesive (nonconstrictive) - Etiologic Classification: - I. Infectious pericarditis - A. Viral (coxsackievirus A and B, echovirus, herpesviruses, mumps, adenovirus, hepatitis, HIV, post-acute COVID, mpox) - B. Pyogenic (pneumococcus, Streptococcus, Staphylococcus, Neisseria, Legionella, Chlamydia) - C. Tuberculous - D. Fungal (histoplasmosis, coccidioidomycosis, Candida, blastomycosis) - E. Other infections (syphilitic, protozoal, parasitic) - II. Noninfectious pericarditis - A. Acute idiopathic - B. Renal failure - C. Neoplasia - 1. Primary tumors (benign or malignant, mesothelioma) - 2. Tumors metastatic to pericardium (lung and breast cancer, lymphoma, leukemia) - D. Trauma (penetrating chest wall, nonpenetrating) - E. Aortic dissection (with leakage into pericardial sac) - F. Acute myocardial infarction - G. Postirradiation - H. Familial Mediterranean fever and other autoinflammatory syndromes - I. Familial pericarditis - 1. Mulibrey nanisma - J. Metabolic (myxedema, cholesterol) - III. Pericarditis presumably related to autoimmunity - A. Rheumatic fever - B. Collagen vascular disease (systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis, scleroderma, acute rheumatic fever, granulomatosis with polyangiitis, IgG4 disease) - C. Drug-induced (e.g., procainamide, hydralazine, phenytoin, isoniazid, minoxidil, anticoagulants, methysergide) - D. Postcardiac injury - 1. Postpericardiotomy - 2. Posttraumatic - 3. Postmyocardial infarction (Dressler's syndrome)
Table 1 — Table 281-1 Classification of Pericarditis¶
| Clinical Classification | Etiologic Classification |
|---|---|
| I. Acute pericarditis (<6 weeks) | I. Infectious pericarditis |
| A. Fibrinous | A. Viral (coxsackievirus A and B, echovirus, herpesviruses, mumps, adenovirus, hepatitis, HIV, post-acute COVID, mpox) |
| B. Effusive (serous or sanguineous) | B. Pyogenic (pneumococcus, Streptococcus, Staphylococcus, Neisseria, Legionella, Chlamydia) |
| II. Subacute pericarditis (6 weeks to 6 months) | C. Tuberculous |
| A. Effusive-constrictive | D. Fungal (histoplasmosis, coccidioidomycosis, Candida, blastomycosis) |
| B. Constrictive | E. Other infections (syphilitic, protozoal, parasitic) |
| III. Chronic pericarditis (>6 months) | II. Noninfectious pericarditis |
| A. Constrictive | A. Acute idiopathic |
| B. Adhesive (nonconstrictive) | B. Renal failure |
| C. Neoplasia | |
| 1. Primary tumors (benign or malignant, mesothelioma) | |
| 2. Tumors metastatic to pericardium (lung and breast cancer, lymphoma, leukemia) | |
| D. Trauma (penetrating chest wall, nonpenetrating) | |
| E. Aortic dissection (with leakage into pericardial sac) | |
| F. Acute myocardial infarction | |
| G. Postirradiation | |
| H. Familial Mediterranean fever and other autoinflammatory syndromes | |
| I. Familial pericarditis | |
| 1. Mulibrey nanisma | |
| J. Metabolic (myxedema, cholesterol) | |
| III. Pericarditis presumably related to autoimmunity | |
| A. Rheumatic fever | |
| B. Collagen vascular disease (systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis, scleroderma, acute rheumatic fever, granulomatosis with polyangiitis, IgG4 disease) | |
| C. Drug-induced (e.g., procainamide, hydralazine, phenytoin, isoniazid, minoxidil, anticoagulants, methysergide) | |
| D. Postcardiac injury | |
| 1. Postpericardiotomy | |
| 2. Posttraumatic | |
| 3. Postmyocardial infarction (Dressler's syndrome) |
2. EPIDEMIOLOGY¶
- Acute pericarditis occurs at all ages but is most common in young adult males.
- It is often associated with pleural effusion and pneumonitis.
- The disease ordinarily runs its course in a few days to 4 weeks.
- Recurrent (relapsing) pericarditis occurs in approximately one-fourth of patients with acute idiopathic pericarditis.
- A smaller number of individuals have multiple recurrences.
- In aggregate, adults with congenital heart disease demonstrate both quality-of-life–limiting comorbidities and premature mortality far in excess of age-matched controls.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Acute pericarditis is often severe, retrosternal and/or left precordial, and referred to the neck, arms, or left shoulder.
- The pain is frequently pleuritic, consequent to accompanying pleural inflammation (i.e., pericarditis).
- Pain is often intensified by lying supine and relieved by sitting up and leaning forward.
- Pain is often absent in slowly developing tuberculous, postirradiation, neoplastic, and uremic pericarditis.
- Viral or idiopathic acute pericarditis occurs in association with or following illnesses of known or presumed viral origin and probably is caused by the same agent.
- There may be an antecedent infection of the respiratory tract, but viral isolation and serologic studies are usually negative.
- In some cases, coxsackievirus A or B or the virus of influenza, echovirus, mumps, herpes simplex, varicella-zoster, adenovirus, or cytomegalovirus has been isolated from pericardial fluid, and/or appropriate elevations in viral antibody titers have been observed.
- Frequently, a viral cause cannot be established, and the term idiopathic acute pericarditis is appropriate.
- Postcardiac injury syndrome may develop after a cardiac operation (postpericardiotomy syndrome), after blunt or penetrating cardiac trauma, or after perforation of the heart with a catheter; rarely, it follows AMI.
- The principal symptom is the pain of acute pericarditis, which usually develops 1–4 weeks after the cardiac injury.
- Pyogenic (purulent) pericarditis is usually secondary to cardiothoracic operations, by extension of infection from the lungs or pleural cavities, from rupture of the esophagus into the pericardial sac, or from rupture of a valvular ring abscess in a patient with infective endocarditis.
- Pericarditis of renal failure (uremic pericarditis) occurs in up to one-third of patients with severe renal dysfunction and is also seen in patients undergoing chronic dialysis who have normal levels of blood urea nitrogen (dialysis-associated pericarditis).
- Pericarditis due to neoplastic diseases results from extension or invasion of metastatic tumors (most commonly carcinoma of the lung and breast, malignant melanoma, lymphoma, and leukemia) to the pericardium.
- The basic physiologic abnormality in patients with chronic constrictive pericarditis is the inability of the ventricles to fill owing to the limitations imposed by the rigid, thickened pericardium.
- Ventricular filling is unimpeded during early diastole but is reduced abruptly when the elastic limit of the pericardium is reached, whereas in cardiac tamponade, ventricular filling is impeded throughout diastole.
- In both conditions, ventricular end-diastolic and stroke volumes are reduced and the end-diastolic pressures in both ventricles and the mean pressures in the atria, pulmonary veins, and systemic veins are all elevated to similar levels (i.e., within 5 mmHg of one another).
3.1 Pathophysiology of Cardiac Tamponade¶
- The accumulation of fluid in the pericardial space in a quantity sufficient to cause serious obstruction of the inflow of blood into the ventricles results in cardiac tamponade.
- This complication may be fatal if it is not recognized and treated promptly.
- The quantity of fluid necessary to produce cardiac tamponade may be as small as 200 mL when the fluid develops rapidly or be as much as >2000 mL in slowly developing effusions when the pericardium has had the opportunity to stretch and adapt to an increasing volume.
- The limitations to ventricular filling are responsible for reductions of cardiac output and arterial pressure.
- The three principal features of tamponade (Beck's triad) are hypotension, soft or absent heart sounds, and jugular venous distention with a prominent x (early systolic) descent but an absent y (early diastolic) descent.
- Paradoxical pulse also occurs in approximately one-third of patients with constrictive pericarditis, and in some cases of hypovolemic shock, acute and chronic obstructive airway disease, and pulmonary embolism.
- Right ventricular infarction may resemble cardiac tamponade with hypotension, elevated jugular venous pressure, a slow y descent in the jugular venous pulse, and, occasionally, a paradoxical pulse.
3.2 Pathophysiology of Constrictive Pericarditis¶
- Chronic constrictive pericarditis results when the healing of an acute fibrinous or serofibrinous pericarditis or the resorption of a chronic pericardial effusion is followed by obliteration of the pericardial cavity with the formation of granulation tissue.
- The latter gradually contracts and forms a firm scar encasing the heart, which may become calcified.
- In developing nations, a high percentage of cases are of tuberculous origin, but this is now an uncommon cause in North America or Western Europe.
- Chronic constrictive pericarditis may follow acute or relapsing viral or idiopathic pericarditis, trauma with organized blood clot, or cardiac surgery of any type, or results from mediastinal irradiation, purulent infection, histoplasmosis, neoplastic disease (especially breast cancer, lung cancer, and lymphoma), rheumatoid arthritis, SLE, or chronic renal failure treated by chronic dialysis.
- In constrictive pericarditis, the right and left atrial pressure pulses display an M-shaped contour, with prominent x and y descents.
- The y descent, which is absent or diminished in cardiac tamponade, is the most prominent deflection in constrictive pericarditis; it reflects rapid early filling of the ventricles.
- The y descent is interrupted by a rapid rise in atrial pressure during early diastole, when ventricular filling is impeded by the constricting pericardium.
- These characteristic changes are transmitted to the jugular veins where they may be recognized by inspection.
- In constrictive pericarditis, the ventricular pressure pulses in both ventricles exhibit the characteristic "square root" sign during diastole.
4. CLINICAL FEATURES¶
- Weakness, fatigue, weight gain, increased abdominal girth, abdominal discomfort, and edema are common.
- The patient often appears chronically ill, and in advanced cases, anasarca, skeletal muscle wasting, and cachexia may be present.
- Exertional dyspnea is common, and orthopnea may occur, although it is usually not severe.
- The neck veins are distended and may remain so even after intensive diuretic treatment, and venous pressure may fail to decline during inspiration (Kussmaul's sign).
- The latter is common in chronic pericarditis but may also occur in tricuspid stenosis, right ventricular infarction, and restrictive cardiomyopathy.
- The pulse pressure is normal or reduced.
- A paradoxical pulse can be detected in about one-third of cases.
- Congestive hepatomegaly is pronounced, may impair hepatic function, and may cause jaundice; ascites is common and is usually more prominent than dependent edema.
- Pleural effusions and splenomegaly may also be present.
- The apical pulse is reduced and may retract in systole (Broadbent's sign).
- The heart sounds may be distant; an early third heart sound (i.e., a pericardial knock) occurring at the cardiac apex with the abrupt cessation of ventricular filling is often conspicuous.
- The ECG frequently displays low voltage of the QRS complexes and diffuse flattening or inversion of the T waves.
- Atrial fibrillation is present in about one-third of patients.
- The chest roentgenogram shows enlargement of the cardiac silhouette, with a "water bottle" configuration, but may be normal in patients with small effusions.
- Ewart's sign: The base of the left lung may be compressed by pericardial fluid, producing a patch of dullness, increased fremitus, and egophony beneath the angle of the left scapula.
4.1 Acute Pericarditis Symptoms¶
- Chest pain is usually present in acute infectious pericarditis and in many of the forms presumed to be related to hypersensitivity.
- The pain of acute pericarditis is often severe, retrosternal and/or left precordial, and referred to the neck, arms, or left shoulder.
- Frequently the pain is pleuritic, consequent to accompanying pleural inflammation (i.e., pericarditis).
- At times, it is steady, radiates to the trapezius ridge or into either arm, and resembles that of myocardial ischemia.
- Pain is often intensified by lying supine and relieved by sitting up and leaning forward.
- Pain is often absent in slowly developing tuberculous, postirradiation, neoplastic, and uremic pericarditis.
4.2 Physical Examination Findings¶
- Pericardial friction rub is audible at some point in the illness in approximately 85% of patients with acute pericarditis.
- The rub may have up to three components per cardiac cycle and is described as rasping, scratching, or grating.
- It is heard most frequently at end expiration with the patient upright and leaning forward.
- Pericardial effusion is usually associated with pain and/or the ECG changes mentioned above and, if the effusion is large, with electrical alternans.
- Pericardial effusion is especially important clinically when it develops within a relatively short time because it may lead to cardiac tamponade.
- Differentiation from cardiac enlargement on physical examination may be difficult, but heart sounds may be fainter with large pericardial effusion.
- The friction rub and the apex impulse may disappear.
- The base of the left lung may be compressed by pericardial fluid, producing Ewart's sign, a patch of dullness, increased fremitus, and egophony beneath the angle of the left scapula.
5. DIFFERENTIAL DIAGNOSIS¶
- A common diagnostic error is mistaking acute viral or idiopathic pericarditis for AMI and vice versa.
- Pericarditis secondary to postcardiac injury is differentiated from acute idiopathic pericarditis chiefly by timing.
- If it occurs within a few days or weeks of a chest blow, a cardiac perforation, a cardiac operation, or an AMI, the two are probably related.
- It is important to distinguish pericarditis due to collagen vascular disease from acute idiopathic pericarditis.
- Most important in the differential diagnosis is the pericarditis due to systemic lupus erythematosus (SLE) or drug-induced (hydralazine or procainamide) lupus.
- When pericarditis occurs in the absence of any obvious underlying disorder, the diagnosis of SLE may be suggested by a rise in the titer of antinuclear antibodies.
- Acute pericarditis is an occasional complication of rheumatoid arthritis, scleroderma, and polyarteritis nodosa, and other evidence of these diseases is usually obvious at the time of presentation with acute pericarditis.
- Pyogenic (purulent) pericarditis is usually secondary to cardiothoracic operations, by extension of infection from the lungs or pleural cavities, from rupture of the esophagus into the pericardial sac, or from rupture of a valvular ring abscess in a patient with infective endocarditis.
- It may also complicate the viral, bacterial, mycobacterial, and fungal infections that occur with HIV infection.
- It is generally accompanied by fever, chills, septicemia, and evidence of infection elsewhere, and generally has a poor prognosis.
- The diagnosis is made by examination of the pericardial fluid.
- It requires immediate drainage as well as vigorous antibiotic treatment.
5.1 Differentiation from AMI¶
- Differentiation of AMI from acute pericarditis may be challenging when, with the latter, serum biomarkers of myocardial damage rise, presumably because of concomitant involvement of the epicardium in the inflammatory process (an epi-myocarditis) with resulting myocyte necrosis.
- If they occur, however, these elevations are quite modest compared to those in AMI, given the superficial subepicardial injury despite often extensive electrocardiographic ST-segment elevation in pericarditis.
- This dissociation is useful in differentiating between these conditions.
- In AMI, ST elevations are upwardly convex, and reciprocal depression is usually more prominent; these changes may return to normal within a day or two.
- In pericarditis, ST elevations are upwardly concave, and reciprocal depression is usually less prominent.
5.2 Differentiation of Tamponade vs Constriction¶
- Table 281-2 lists the features that distinguish acute cardiac tamponade from constrictive pericarditis and similar clinical disorders.
- Pulsus paradoxus is always present in tamponade, usually present in constrictive pericarditis, rare in restrictive cardiomyopathy, and present in right ventricular infarction.
- Prominent y descent is absent in tamponade, usually present in constrictive pericarditis, rare in restrictive cardiomyopathy, and present in right ventricular infarction.
- Prominent x descent is always present in tamponade, usually present in constrictive pericarditis, always present in restrictive cardiomyopathy, and present in right ventricular infarction.
- Kussmaul's sign is absent in tamponade, always present in constrictive pericarditis, rare in restrictive cardiomyopathy, and present in right ventricular infarction.
- Pericardial knock is absent in tamponade, usually present in constrictive pericarditis, absent in restrictive cardiomyopathy, and absent in right ventricular infarction.
- Low ECG voltage is always present in tamponade, usually present in constrictive pericarditis, rare in restrictive cardiomyopathy, and present in right ventricular infarction.
- Electrical alternans is always present in tamponade, absent in constrictive pericarditis, absent in restrictive cardiomyopathy, and absent in right ventricular infarction.
- Thickened pericardium is absent in tamponade, always present in constrictive pericarditis, absent in restrictive cardiomyopathy, and present in effusive constrictive pericarditis.
- Pericardial calcification is absent in tamponade, usually present in constrictive pericarditis, absent in restrictive cardiomyopathy, and absent in effusive constrictive pericarditis.
- Pericardial effusion is always present in tamponade, absent in constrictive pericarditis, absent in restrictive cardiomyopathy, and present in effusive constrictive pericarditis.
- RV size is usually small in tamponade, usually normal in constrictive pericarditis, usually normal in restrictive cardiomyopathy, enlarged in right ventricular infarction, and usually normal in effusive constrictive pericarditis.
Table 2 — Table 281-2 Features That Distinguish Cardiac Tamponade from Constrictive Pericarditis and Similar Clinical Disorders¶
| Characteristic | Tamponade | Constrictive Pericarditis | Restrictive Cardiomyopathy | Right Ventricular Infarction | Effusive Constrictive Pericarditis | |
|---|---|---|---|---|---|---|
| Pulsus paradoxus | +++ | + | + | + | +++ | |
| Jugular veins | ||||||
| Prominent y descent | – | ++ | + | + | – | |
| Prominent x descent | +++ | ++ | +++ | + | +++ | |
| Kussmaul's sign | – | +++ | + | +++ | ++ | |
| Third heart sound | – | – | + | + | + | |
| Pericardial knock | – | ++ | – | – | – | |
| Electrocardiogram | ||||||
| Low ECG voltage | ++ | ++ | + | – | + | |
| Electrical alternans | ++ | – | – | – | + | |
| Echocardiogram | ||||||
| Thickened pericardium | – | +++ | – | – | ++ | |
| Pericardial calcification | – | ++ | – | – | _ | |
| Pericardial effusion | +++ | – | – | – | ++ | |
| RV size | Usually small | Usually normal | Usually normal | Enlarged | Usually normal | |
| Exaggerated respiratory variation in flow velocity | +++ | +++ | – | +++ | + | |
| CT/MRI | ||||||
| Thickened pericardium | – | +++ | – | ++ | ||
| Equalization of diastolic pressures | +++ | +++ | – | ++ | ++ |
6. INVESTIGATIONS & DIAGNOSIS¶
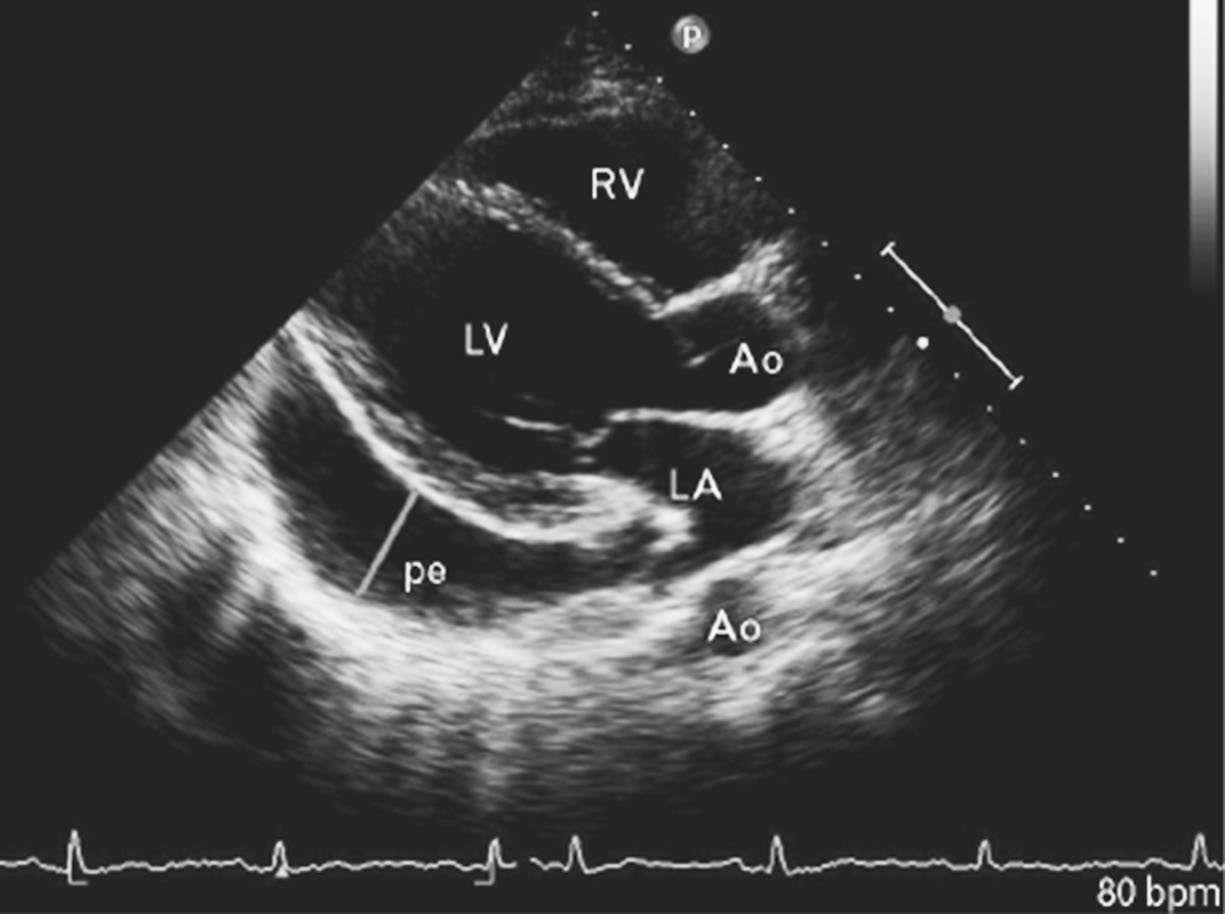
- Echocardiography is the most widely used imaging technique. It is sensitive, specific, simple, and noninvasive; it may be performed at the bedside; and it allows localization and estimation of the quantity of pericardial fluid.
- The presence of pericardial fluid is recorded by two-dimensional transthoracic echocardiography as a relatively echo-free space between the posterior pericardium and left ventricular epicardium and/or as a space between the anterior right ventricle and the parietal pericardium just beneath the anterior chest wall.
- The diagnosis of pericardial fluid or thickening may be confirmed by computed tomography (CT) or magnetic resonance imaging (MRI).
- These techniques may be superior to echocardiography in detecting loculated pericardial effusions and pericardial thickening, and in the identification of pericardial masses.
- MRI is also helpful in detecting pericardial inflammation.
- Pericardial fluid obtained from an effusion may have the physical characteristics of an exudate.
- In developed nations, bloody fluid is most commonly due to neoplasm, renal failure, or cardiac trauma.
- In developing nations, tuberculosis may also cause exudative and/or bloody effusion.
- The pericardial fluid should be analyzed for red and white blood cells and cytology for neoplastic cells.
- Cultures should be obtained.
- The presence of DNA of Mycobacterium tuberculosis determined by the polymerase chain reaction and/or of an elevated adenosine deaminase strongly supports the diagnosis of tuberculous pericarditis; however, it is often necessary to obtain pericardial tissue to make this diagnosis.
- Echocardiography shows that tricuspid and pulmonic valve flow velocities increase markedly during inspiration, whereas pulmonic vein, mitral, and aortic flow velocities decrease (as in constrictive pericarditis, see below) in tamponade.
- In tamponade, there is late diastolic inward motion (collapse) of the right ventricular free wall and the right atrium.
- Transesophageal echocardiography, CT, or cardiac MRI may be necessary to diagnose a loculated effusion responsible for cardiac tamponade.
6.1 Electrocardiographic Findings¶
- The electrocardiogram (ECG) in acute pericarditis without massive effusion usually displays changes secondary to acute subepicardial inflammation.
- Typically, it evolves through four stages.
- In stage 1, there is widespread elevation of the ST segments, often with upward concavity, involving two or three standard limb leads and V–V6.
- In addition, there is depression of the PR segment below the TP segment, reflecting atrial involvement, an early change that may occur prior to ST segment elevation.
- Usually there are no significant changes in QRS complexes unless a large pericardial effusion develops.
- After several days, the ST segments return to normal (stage 2), and only then, or even later, do the T waves become inverted (stage 3).
- Weeks or months after the onset of acute pericarditis, the ECG returns to normal (stage 4).
- In contrast, in AMI, ST elevations are upwardly convex, and reciprocal depression is usually more prominent; these changes may return to normal within a day or two.
6.2 Echocardiographic Findings¶
- Echocardiography is the most widely used imaging technique.
- It is sensitive, specific, simple, and noninvasive.
- It may be performed at the bedside.
- It allows localization and estimation of the quantity of pericardial fluid.
- The presence of pericardial fluid is recorded by two-dimensional transthoracic echocardiography as a relatively echo-free space between the posterior pericardium and left ventricular epicardium and/or as a space between the anterior right ventricle and the parietal pericardium just beneath the anterior chest wall.
- In tamponade, there is late diastolic inward motion (collapse) of the right ventricular free wall and the right atrium.
- Transesophageal echocardiography, CT, or cardiac MRI may be necessary to diagnose a loculated effusion responsible for cardiac tamponade.
7. MANAGEMENT & TREATMENT¶
- There is no specific therapy for acute idiopathic pericarditis, but bed rest may be recommended, and anti-inflammatory treatment with aspirin (2–4 g/d) or nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (600–800 mg tid) or indomethacin (25–50 mg tid), should be administered along with gastric protection (e.g., omeprazole 20 mg/d).
- In responsive patients, these doses should be continued for 1–2 weeks and then tapered over several weeks.
- In addition, colchicine (0.5 to 0.6 mg qd [70 kg]) should be administered for 3 months.
- Colchicine enhances the response to NSAIDs and also aids in reducing the risk of recurrent pericarditis.
- This drug is concentrated in and interferes with the migration of neutrophils, may cause diarrhea and other gastrointestinal side effects, and is contraindicated in patients with hepatic or renal dysfunction.
- Glucocorticoids (e.g., prednisone 1 mg/kg per day) usually suppress the clinical manifestations of acute pericarditis in patients who have failed therapy with or do not tolerate NSAIDs and colchicine.
- However, since they increase the risk of subsequent recurrence, full-dose corticosteroids should be given for only 2–4 days and then tapered.
- Anticoagulants should be avoided because their use could cause bleeding into the pericardial cavity and tamponade.
- In patients with multiple, frequent, and disabling recurrences that continue for >2 years, are not prevented by continuing colchicine and other NSAIDs, and are not controlled by glucocorticoids, treatment with azathioprine or anakinra (an interleukin 1β receptor antagonist) has been reported to be of benefit.
- Rarely, pericardial stripping may be necessary; however, this procedure may not always terminate the recurrences.
- The majority of patients with acute pericarditis can be managed as outpatients with careful follow-up.
- However, when specific causes (tuberculosis, neoplastic disease, bacterial infection) are suspected, or if any of the predictors of poor prognosis (fever >38°C, subacute onset, large pericardial effusion, immunosuppression, or pericardial knock) are present, hospitalization is advisable.
- If manifestations of tamponade appear, pericardiocentesis using an apical, parasternal, or, most commonly, subxiphoid approach must be carried out at once because if left untreated, tamponade may be rapidly fatal.
- Whenever possible, this procedure should be carried out under echocardiographic guidance.
- Intravenous saline may be administered as the patient is being readied for the procedure, but the pericardiocentesis must not be delayed.
- If possible, intrapericardial pressure should be measured before fluid is withdrawn, and the pericardial cavity should be drained as completely as possible.
- A small, multiholed catheter may be advanced over the needle inserted into the pericardial cavity and left in place to allow draining of the pericardial space if fluid reaccumulates.
- Surgical drainage through a limited (subxiphoid) thoracotomy may be required in recurrent tamponade to remove loculated effusions and/or when it is necessary to obtain tissue for diagnosis.
- Treatment with an NSAID and intensification of dialysis are usually adequate for uremic pericarditis.
- Occasionally, tamponade occurs and pericardiocentesis is required.
- When the pericarditis of renal failure is recurrent or persistent, a pericardial window should be created or pericardiectomy may be necessary.
- Pericardiectomy may be required in patients with recurrence of chronic pericardial effusion.
- Intrapericardial instillation of sclerosing agents may be used to prevent reaccumulation of fluid, most commonly in recurrent neoplastic effusions.
7.1 Treatment of Acute Pericarditis¶
- Bed rest may be recommended.
- Anti-inflammatory treatment with aspirin (2–4 g/d) or nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (600–800 mg tid) or indomethacin (25–50 mg tid), should be administered along with gastric protection (e.g., omeprazole 20 mg/d).
- In responsive patients, these doses should be continued for 1–2 weeks and then tapered over several weeks.
- Colchicine (0.5 to 0.6 mg qd [70 kg]) should be administered for 3 months.
- Colchicine enhances the response to NSAIDs and also aids in reducing the risk of recurrent pericarditis.
- This drug is concentrated in and interferes with the migration of neutrophils, may cause diarrhea and other gastrointestinal side effects, and is contraindicated in patients with hepatic or renal dysfunction.
- Glucocorticoids (e.g., prednisone 1 mg/kg per day) usually suppress the clinical manifestations of acute pericarditis in patients who have failed therapy with or do not tolerate NSAIDs and colchicine.
- However, since they increase the risk of subsequent recurrence, full-dose corticosteroids should be given for only 2–4 days and then tapered.
- Anticoagulants should be avoided because their use could cause bleeding into the pericardial cavity and tamponade.
- In patients with multiple, frequent, and disabling recurrences that continue for >2 years, are not prevented by continuing colchicine and other NSAIDs, and are not controlled by glucocorticoids, treatment with azathioprine or anakinra (an interleukin 1β receptor antagonist) has been reported to be of benefit.
- Rarely, pericardial stripping may be necessary; however, this procedure may not always terminate the recurrences.
7.2 Treatment of Cardiac Tamponade¶
- If manifestations of tamponade appear, pericardiocentesis using an apical, parasternal, or, most commonly, subxiphoid approach must be carried out at once because if left untreated, tamponade may be rapidly fatal.
- Whenever possible, this procedure should be carried out under echocardiographic guidance.
- Intravenous saline may be administered as the patient is being readied for the procedure, but the pericardiocentesis must not be delayed.
- If possible, intrapericardial pressure should be measured before fluid is withdrawn, and the pericardial cavity should be drained as completely as possible.
- A small, multiholed catheter may be advanced over the needle inserted into the pericardial cavity and left in place to allow draining of the pericardial space if fluid reaccumulates.
- Surgical drainage through a limited (subxiphoid) thoracotomy may be required in recurrent tamponade to remove loculated effusions and/or when it is necessary to obtain tissue for diagnosis.
7.3 Treatment of Constrictive Pericarditis¶
- Pericardiectomy is the treatment of choice for chronic constrictive pericarditis.
- Pericardiectomy may be required in patients with recurrence of chronic pericardial effusion.
- Intrapericardial instillation of sclerosing agents may be used to prevent reaccumulation of fluid, most commonly in recurrent neoplastic effusions.
8. PROGNOSIS & COMPLICATIONS¶
- The natural history of Eisenmenger Syndrome is variable, and although there is significant morbidity, in general, adults with ES appear to survive longer than those with other forms of pulmonary arterial hypertension.
- The most frequent complication is recurrent (relapsing) pericarditis, which occurs in approximately one-fourth of patients with acute idiopathic pericarditis.
- A smaller number of individuals have multiple recurrences.
- In aggregate, adults with congenital heart disease demonstrate both quality-of-life–limiting comorbidities and premature mortality far in excess of age-matched controls.
- The reported prevalence of pain, anxiety, depression, dyspnea, and fatigue appears similar to that reported for adults who are decades older and engaged in palliative care for acquired cardiovascular disease at end of life (EOL).
9. SPECIAL CONSIDERATIONS¶
- Selective pulmonary vasodilators, such as bosentan or sildenafil, and are efficacious in Eisenmenger Syndrome.
- Select patients may be candidates for combined heart–lung transplantation or preferably lung transplantation with concomitant repair of the intracardiac defect, if feasible.
- Contraception for women with ES who are of childbearing age is strongly recommended, avoiding use of estrogen, which may be thrombogenic.
- Pregnancy is contraindicated in these women due to the high risk of maternal mortality.
- Congenital heart disease care centers that contain an ACHD specialty care program has been associated with improved overall survival.
- Care for adults with CHD within medical care centers that contain an ACHD specialty care program has been associated with improved overall survival.
- However, current analyses suggest that the majority of adults with CHD seek and receive their medical care outside of such ACHD specialty care centers and within the hands of the general practitioner, internist, and cardiologist.
- Under a surface of adaptability and determination, adults with CHD present a wide spectrum of cognitive and functional performance, multiple organ system comorbidities, abnormalities of systemic and pulmonary vasculature, and a near universal presence of heart failure.
- Palliative care specialists who are embedded within or aligned with ACHD care teams can play an important and iterative role in defining and addressing alignment of patient and clinician goals within the boundaries of frequently complex care decisions over the adult life span.
- In a retrospective study of ACHD patients who died during a hospital admission, only a minority had engaged in EOL discussions with their providers.
- Surveys of both adults with CHD and their providers suggest that the overwhelming majority of patients wish to participate in advanced care planning and discussion of palliative care; this contrasts with statements from ACHD care providers noting their uncertainties regarding EOL prognostication and concerns over discussion about EOL.
9.1 Uremic Pericarditis¶
- Pericarditis of renal failure (uremic pericarditis) occurs in up to one-third of patients with severe renal dysfunction and is also seen in patients undergoing chronic dialysis who have normal levels of blood urea nitrogen (dialysis-associated pericarditis).
- These two forms of pericarditis may be fibrinous and are generally associated with serosanguinous effusions; frank hemorrhagic effusions may be seen in some cases of uremic pericarditis prior to the onset of dialysis.
- A pericardial friction rub is common, but pain is usually absent or mild.
- Treatment with an NSAID and intensification of dialysis are usually adequate.
- Occasionally, tamponade occurs and pericardiocentesis is required.
- When the pericarditis of renal failure is recurrent or persistent, a pericardial window should be created or pericardiectomy may be necessary.
9.2 Neoplastic Pericarditis¶
- Pericarditis due to neoplastic diseases results from extension or invasion of metastatic tumors (most commonly carcinoma of the lung and breast, malignant melanoma, lymphoma, and leukemia) to the pericardium.
- The pain of pericarditis, tamponade, and atrial arrhythmias are complications that occur occasionally.
- Diagnosis is made by pericardial fluid cytology or pericardial biopsy.
- Mediastinal irradiation for neoplasm may cause acute pericarditis and/or chronic constrictive pericarditis.
- Intrapericardial instillation of sclerosing agents may be used to prevent reaccumulation of fluid, most commonly in recurrent neoplastic effusions.
10. KEY PEARLS & CLINICAL TRAPS¶
- A high index of suspicion for cardiac tamponade is required because in many instances no obvious cause for pericardial disease is apparent.
- This diagnosis should be considered in any patient with otherwise unexplained sudden enlargement of the cardiac silhouette, hypotension, and elevation of jugular venous pressure.
- Reductions in amplitude of the QRS complexes and electrical alternans of the P, QRS, or T waves should also raise the suspicion of cardiac tamponade.
- The pain of acute pericarditis is often severe, retrosternal and/or left precordial, and referred to the neck, arms, or left shoulder.
- Frequently the pain is pleuritic, consequent to accompanying pleural inflammation (i.e., pericarditis).
- At times, it is steady, radiates to the trapezius ridge or into either arm, and resembles that of myocardial ischemia.
- For this reason, confusion with acute myocardial infarction (AMI) is common.
- Characteristically, pericardial pain may be intensified by lying supine and relieved by sitting up and leaning forward.
- Pain is often absent in slowly developing tuberculous, postirradiation, neoplastic, and uremic pericarditis.
- The differentiation of AMI from acute pericarditis may be challenging when, with the latter, serum biomarkers of myocardial damage rise, presumably because of concomitant involvement of the epicardium in the inflammatory process (an epi-myocarditis) with resulting myocyte necrosis.
- If they occur, however, these elevations are quite modest compared to those in AMI, given the superficial subepicardial injury despite often extensive electrocardiographic ST-segment elevation in pericarditis.
- This dissociation is useful in differentiating between these conditions.
- In AMI, ST elevations are upwardly convex, and reciprocal depression is usually more prominent; these changes may return to normal within a day or two.
- In pericarditis, ST elevations are upwardly concave, and reciprocal depression is usually less prominent.
- A pericardial friction rub is audible at some point in the illness in approximately 85% of patients with acute pericarditis.
- The rub may have up to three components per cardiac cycle and is described as rasping, scratching, or grating.
- It is heard most frequently at end expiration with the patient upright and leaning forward.
- Pericardial effusion is usually associated with pain and/or the ECG changes mentioned above and, if the effusion is large, with electrical alternans.
- Pericardial effusion is especially important clinically when it develops within a relatively short time because it may lead to cardiac tamponade.
- Differentiation from cardiac enlargement on physical examination may be difficult, but heart sounds may be fainter with large pericardial effusion.
- The friction rub and the apex impulse may disappear.
- The base of the left lung may be compressed by pericardial fluid, producing Ewart's sign, a patch of dullness, increased fremitus, and egophony beneath the angle of the left scapula.
- The ECG frequently displays low voltage of the QRS complexes and diffuse flattening or inversion of the T waves.
- Atrial fibrillation is present in about one-third of patients.
- The chest roentgenogram shows enlargement of the cardiac silhouette, with a "water bottle" configuration, but may be normal in patients with small effusions.
- Ewart's sign: The base of the left lung may be compressed by pericardial fluid, producing a patch of dullness, increased fremitus, and egophony beneath the angle of the left scapula.
- The diagnosis of pericardial fluid or thickening may be confirmed by computed tomography (CT) or magnetic resonance imaging (MRI).
- These techniques may be superior to echocardiography in detecting loculated pericardial effusions and pericardial thickening, and in the identification of pericardial masses.
- MRI is also helpful in detecting pericardial inflammation.
- Pericardial fluid obtained from an effusion may have the physical characteristics of an exudate.
- In developed nations, bloody fluid is most commonly due to neoplasm, renal failure, or cardiac trauma.
- In developing nations, tuberculosis may also cause exudative and/or bloody effusion.
- The pericardial fluid should be analyzed for red and white blood cells and cytology for neoplastic cells.
- Cultures should be obtained.
- The presence of DNA of Mycobacterium tuberculosis determined by the polymerase chain reaction and/or of an elevated adenosine deaminase strongly supports the diagnosis of tuberculous pericarditis; however, it is often necessary to obtain pericardial tissue to make this diagnosis.
- Echocardiography shows that tricuspid and pulmonic valve flow velocities increase markedly during inspiration, whereas pulmonic vein, mitral, and aortic flow velocities decrease (as in constrictive pericarditis, see below) in tamponade.
- In tamponade, there is late diastolic inward motion (collapse) of the right ventricular free wall and the right atrium.
- Transesophageal echocardiography, CT, or cardiac MRI may be necessary to diagnose a loculated effusion responsible for cardiac tamponade.
- The three principal features of tamponade (Beck's triad) are hypotension, soft or absent heart sounds, and jugular venous distention with a prominent x (early systolic) descent but an absent y (early diastolic) descent.
- The limitations to ventricular filling are responsible for reductions of cardiac output and arterial pressure.
- The quantity of fluid necessary to produce cardiac tamponade may be as small as 200 mL when the fluid develops rapidly or be as much as >2000 mL in slowly developing effusions when the pericardium has had the opportunity to stretch and adapt to an increasing volume.
- The limitations to ventricular filling are responsible for reductions of cardiac output and arterial pressure.
- The three principal features of tamponade (Beck's triad) are hypotension, soft or absent heart sounds, and jugular venous distention with a prominent x (early systolic) descent but an absent y (early diastolic) descent.
- The limitations to ventricular filling are responsible for reductions of cardiac output and arterial pressure.
- The quantity of fluid necessary to produce cardiac tamponade may be as small as 200 mL when the fluid develops rapidly or be as much as >2000 mL in slowly developing effusions when the pericardium has had the opportunity to stretch and adapt to an increasing volume.
- Paradoxical pulse also occurs in approximately one-third of patients with constrictive pericarditis, and in some cases of hypovolemic shock, acute and chronic obstructive airway disease, and pulmonary embolism.
- Right ventricular infarction may resemble cardiac tamponade with hypotension, elevated jugular venous pressure, a slow y descent in the jugular venous pulse, and, occasionally, a paradoxical pulse.
- The basic physiologic abnormality in patients with chronic constrictive pericarditis is the inability of the ventricles to fill owing to the limitations imposed by the rigid, thickened pericardium.
- Ventricular filling is unimpeded during early diastole but is reduced abruptly when the elastic limit of the pericardium is reached, whereas in cardiac tamponade, ventricular filling is impeded throughout diastole.
- In both conditions, ventricular end-diastolic and stroke volumes are reduced and the end-diastolic pressures in both ventricles and the mean pressures in the atria, pulmonary veins, and systemic veins are all elevated to similar levels (i.e., within 5 mmHg of one another).
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶
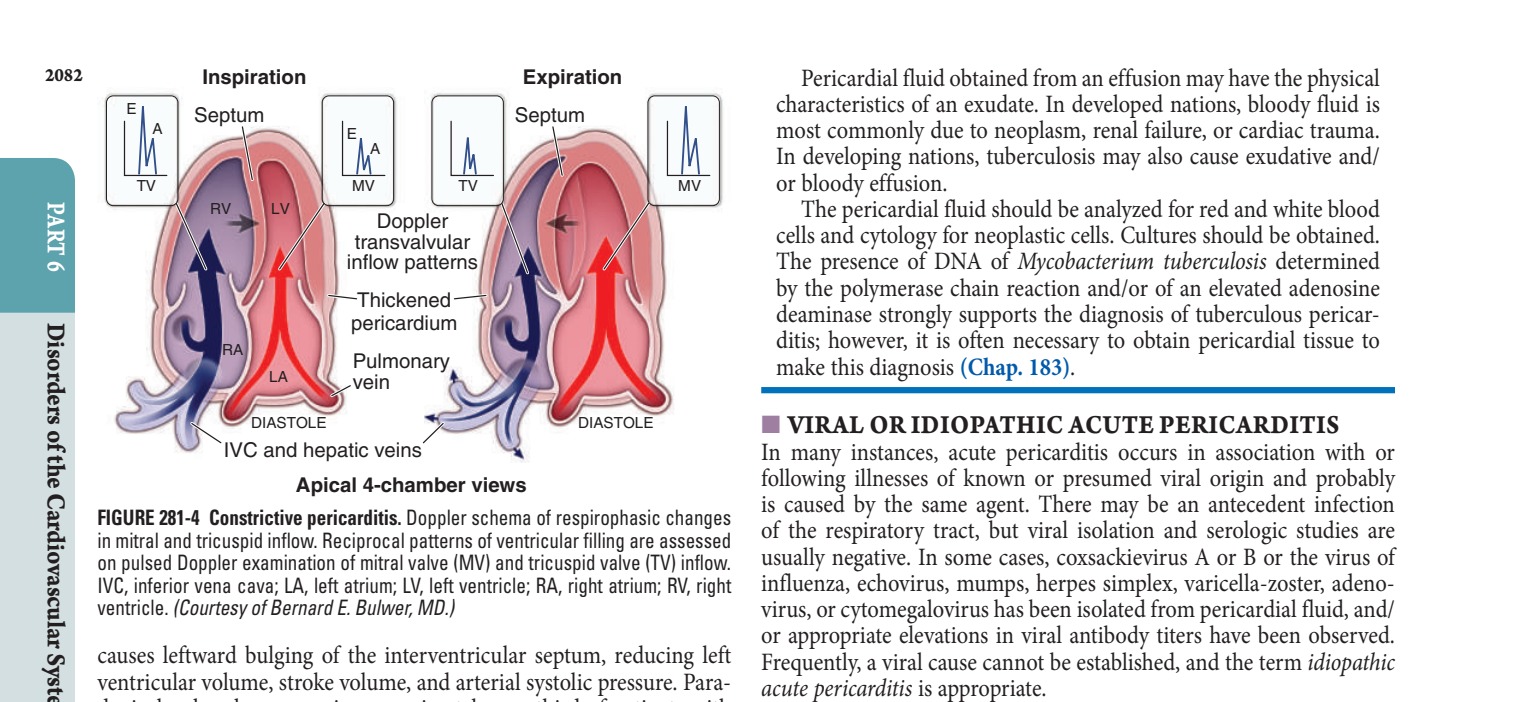
Caption: FIGURE 281-4 Constrictive pericarditis. Doppler schema of respirophasic changes of in mitral and tricuspid inflow. Reciprocal patterns of ventricular filling are assessed on pulsed Doppler examination of mitral valve (MV) and tricuspid valve (TV) inflow. IVC, inferior vena cava; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. (Courtesy of Bernard E. Bulwer, MD.) causes leftward bulging of the interventricular septum, reducing left ventricular volume, stroke volume, and arterial systolic pressure. Para- doxical pulse also occurs in approximately one-third of patients with constrictive pericarditis (see below), and in some cases of hypovolemic shock, acute and chronic obstructive airway disease, and pulmonary
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
Caption: FIGURE 281-1 A. Acute pericarditis. There are diffuse ST-segment elevations in leads I, II, current. B. Electrical alternans. This tracing was obtained from a patient with a large patients, these doses should be continued for 1–2 weeks and then tapered over several weeks. In addition, colchicine (0.5 to 0.6 mg qd [70 kg]) should be adminis- tered for 3 months. Colchicine enhances the response to NSAIDs — Figure 281-1: Electrocardiogram showing (A) diffuse ST-segment elevations with PR-segment depression in acute pericarditis, and (B) electrical alternans in a patient with large pericardial effusion and cardiac tamponade.
Figure 2¶

Caption: FIGURE 281-3 Pericardial inflammation by cardiac magnetic resonance imaging. A. Short thickened white line denoted by arrow. B. Long axis view. Late gadolinium enhancement of ventricle. (From RY Kwong: Cardiovascular magnetic resonance imaging, in Braunwald’s ■ CARDIAC TAMPONADE The accumulation of fluid in the pericardial space in a quantity suf- ficient to cause serious obstruction of the inflow of blood into the ventricles results in cardiac tamponade. This complication may be fatal if it is not recognized and treated promptly. The most common causes — Figure 281-2: Two-dimensional echocardiogram in lateral view demonstrating a large pericardial effusion (echo-free space) between the posterior pericardium and left ventricular epicardium.
Figure 3¶

Caption: Figure 281-3: Cardiac magnetic resonance imaging showing (A) short axis view with thickened, enhanced pericardium on T2 images and (B) long axis view with late gadolinium enhancement of the inflamed pericardium.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.