Ischemic Stroke¶
Chapter 438 | Part 13: Neurologic Disorders · Part 13 – Neurologic Disorders
Detailed clinical reference synthesised from Harrison's Principles of Internal Medicine, 22nd Edition
🔑 Key Clinical Points¶
- The ischemic penumbra is defined as the ischemic but reversibly dysfunctional tissue surrounding a core area of infarction; saving the penumbra is the goal of revascularization therapy.
- IV thrombolysis with rtPA is indicated within 4.5 hours of onset (or 3 hours in US approval) if no hemorrhage is seen on CT; tenecteplase is an alternative bolus option.
- Endovascular thrombectomy improves clinical outcomes for large-vessel occlusions (ICA, MCA, basilar) up to 24 hours from onset if imaging shows a mismatch.
- Blood pressure should be reduced if it exceeds 220/120 mmHg, or >185/110 mmHg if thrombolytic therapy is anticipated; routine lowering below these limits may worsen outcomes.
- Aspirin is the only antiplatelet agent proven effective for acute treatment; dual antiplatelet therapy (aspirin + clopidogrel/ticagrelor) is used for 21-30 days after minor stroke or TIA.
- Nonvalvular atrial fibrillation is the most common cause of cardioembolic stroke; CHADS-VASc score is used to estimate stroke risk and guide anticoagulation.
- Cerebellar infarction can mimic labyrinthitis; even small amounts of edema can cause brainstem compression requiring emergency suboccipital decompression.
- Hemicraniectomy reduces mortality by 50% in patients with significant cerebral edema; older patients (>60 years) benefit less but still significantly.
- Paradoxical embolization occurs via a patent foramen ovale (PFO) or atrial septal defect; bubble-contrast echocardiography is highly sensitive for detection.
- Carotid atherosclerosis produces an estimated 10% of ischemic strokes; high-grade stenosis (>50%) requires endarterectomy regardless of infarct size.
📑 Table of Contents¶
- 1. DEFINITION & OVERVIEW
- 1.1 Clinical Diagnosis
- 2. EPIDEMIOLOGY
- 3. ETIOLOGY & PATHOPHYSIOLOGY
- 3.1 Pathophysiology Cascade
- 3.2 Mechanisms of Ischemic Stroke
- 4. CLINICAL FEATURES
- 4.1 Cardioembolic Stroke
- 4.2 Carotid Atherosclerosis
- 5. DIFFERENTIAL DIAGNOSIS
- 6. INVESTIGATIONS & DIAGNOSIS
- 6.1 Diagnostic Criteria for Thrombolysis
- 6.2 Imaging Findings
- 7. MANAGEMENT & TREATMENT
- 7.1 Medical Support
- 7.2 Thrombolysis
- 7.3 Endovascular Revascularization
- 7.4 Antithrombotic Treatment
- 7.5 Neuroprotection
- 7.6 Stroke Centers and Rehabilitation
- 8. PROGNOSIS & COMPLICATIONS
- 9. SPECIAL CONSIDERATIONS
- 9.1 Pregnancy
- 9.2 Pediatrics
- 9.3 Elderly
- 9.4 Renal/Hepatic Impairment
- 10. KEY PEARLS & CLINICAL TRAPS
- Flowcharts & Algorithms
- Figures & Illustrations
📋 Figures in This Chapter¶
1. DEFINITION & OVERVIEW¶
📖 Harrison's defines this as:
Another important concept is the ischemic penumbra, defined as the ischemic but reversibly dysfunctional tissue surrounding a core area of infarction.
- The clinical diagnosis of stroke is discussed in Chap. 437.
- Once this diagnosis is made and either a noncontrast computed tomography (CT) scan or magnetic resonance imaging (MRI) scan has been performed, rapid reversal of ischemia is paramount.
- This chapter will focus on the stroke treatment timeline and subsequent secondary stroke prevention.
- A transient ischemic attack (TIA) is defined as a clinical syndrome characterized by transient symptoms resulting from ischemia without infarction unless prolonged.
- The penumbra can be imaged by perfusion imaging using MRI or CT.
- The ischemic penumbra will eventually progress to infarction if no change in flow occurs, and hence, saving the ischemic penumbra is the goal of revascularization therapy.
- Restoration of blood flow provides oxygen and glucose to the penumbral tissue, preventing infarction not only by supplying fuel for metabolism but by reversing tissue acidosis, clearing glutamate and toxic oxygen species, and halting waves of cortical spreading depression emanating from the ischemic core that add metabolic stress to the tissue.
1.1 Clinical Diagnosis¶
- The clinical diagnosis of stroke is discussed in Chap. 437.
- Once this diagnosis is made and either a noncontrast computed tomography (CT) scan or magnetic resonance imaging (MRI) scan has been performed, rapid reversal of ischemia is paramount.
- This chapter will focus on the stroke treatment timeline and subsequent secondary stroke prevention.
2. EPIDEMIOLOGY¶
- Heart disease and stroke statistics-2023 update: A report from the American Heart Association (Tsao CW).
- Cardioembolic stroke is responsible for ~20% of all ischemic strokes.
- Carotid atherosclerosis produces an estimated 10% of ischemic stroke.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- Patients with atrial fibrillation have an average annual risk of stroke of ~5%.
3. ETIOLOGY & PATHOPHYSIOLOGY¶
- Acute occlusion of an intracranial vessel causes reduction in blood flow to the brain region it supplies.
- The magnitude of flow reduction is a function of collateral blood flow, and this depends on an individual's vascular anatomy (which may be altered by disease), the site of occlusion, and systemic blood pressure.
- A decrease in cerebral blood flow to zero causes death of brain tissue (neuron cell bodies, dendrites, axons, and glial cells) within 4–10 min.
- Values 11.1 mmol/L [200 mg/dL]).
- It is reasonable to suppress fever and prevent hyperglycemia during and after brain ischemia.
- The value of induced mild hypothermia to improve stroke outcomes has not been clearly demonstrated and remains the subject of continuing clinical research.
Table 1 — TABLE 438-2 Causes of Ischemic Stroke¶
| COMMON CAUSES | UNCOMMON CAUSES |
|---|---|
| Thrombosis | Hypercoagulable disorders |
| Lacunar stroke (small vessel) | Protein C deficiencya |
| Large-vessel thrombosis | Protein S deficiencya |
| Dehydration | Antithrombin III deficiencya |
| Embolic occlusion | Antiphospholipid syndrome |
| Artery-to-artery | Factor V Leiden mutationa |
| Carotid bifurcation | Prothrombin G20210A mutationa |
| Aortic arch | Systemic malignancy |
| Arterial dissection | Sickle cell anemia |
| Cardioembolic | β Thalassemia |
| Atrial fibrillation | Polycythemia vera |
| Mural thrombus | Systemic lupus erythematosus |
| Myocardial infarction | Homocysteinemia |
| Dilated cardiomyopathy | Thrombotic thrombocytopenic purpura |
| Valvular lesions | Disseminated intravascular coagulation |
| Mitral stenosis | Dysproteinemiasa |
| Mechanical valve | Nephrotic syndromea |
| Bacterial endocarditis | Inflammatory bowel diseasea |
| Paradoxical embolus | Oral contraceptives |
| Atrial septal defect | COVID-19 infection |
| Patent foramen ovale | Venous sinus thrombosisb |
| Atrial septal aneurysm | Fibromuscular dysplasia |
| Spontaneous echo contrast | Vasculitis |
| Stimulant drugs: cocaine, amphetamine | Systemic vasculitis (PAN, granulomatosis with polyangiitis, Takayasu's, giant cell arteritis) |
| Primary CNS vasculitis | Primary CNS vasculitis |
| Meningitis (syphilis, tuberculosis, fungal, bacterial, zoster) | Noninflammatory vasculopathy |
| Noninflammatory vasculopathy | Reversible vasoconstriction syndrome |
| Reversible vasoconstriction syndrome | Fabry's disease |
| Fabry's disease | Angiocentric lymphoma |
| Angiocentric lymphoma | Cardiogenic |
| Cardiogenic | Mitral valve calcification |
| Mitral valve calcification | Atrial myxoma |
| Atrial myxoma | Intracardiac tumor |
| Intracardiac tumor | Marantic endocarditis |
| Marantic endocarditis | Libman-Sacks endocarditis |
| Libman-Sacks endocarditis | Subarachnoid hemorrhage vasospasm |
| Subarachnoid hemorrhage vasospasm | Moyamoya disease |
| Moyamoya disease | Eclampsia |
3.1 Pathophysiology Cascade¶
- Arterial occlusion leads to energy failure, spreading depression, mitochondrial damage, PARP activation, glutamate release, Ca2+/Na+ influx, inflammatory response, iNOS, free oxygen species, proteolysis, leukocyte adhesion, lipolysis, membrane and cytoskeletal breakdown, arachidonic acid production, phospholipase activation, acid production, and cell death.
- See Figure 438-1 for major steps in the cascade of cerebral ischemia.
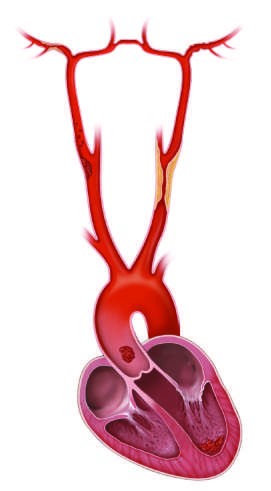
3.2 Mechanisms of Ischemic Stroke¶
- Occlusion of an intracranial vessel by an embolus (e.g., cardiogenic sources such as atrial fibrillation or artery-to-artery emboli from carotid atherosclerotic plaque), often affecting the large intracranial vessels.
- In situ thrombosis of an intracranial vessel, typically affecting the small penetrating arteries that arise from the major intracranial arteries.
- Hypoperfusion caused by flow-limiting stenosis of a major extracranial (e.g., internal carotid) or intracranial vessel, often producing 'watershed' ischemia.
4. CLINICAL FEATURES¶
- The clinical presentation and examination findings often establish the cause of stroke or the possibilities to a few.
- Judicious use of laboratory testing and imaging studies completes the initial evaluation.
- Nevertheless, nearly 30% of strokes remain unexplained despite extensive evaluation.
- Clinical examination should focus on the peripheral and cervical vascular system (measuring blood pressure), the heart (dysrhythmia, murmurs), extremities (peripheral emboli), and retina (effects of hypertension and cholesterol emboli [Hollenhorst plaques]).
- A complete neurologic examination is performed to localize the anatomic site of stroke.
- An imaging study of the brain is always indicated and is required for patients being considered for thrombolysis; it may be combined with CT- or MRI-based angiography to visualize the vasculature of the neck and intracranial vessels.
- A chest x-ray, electrocardiogram (ECG), urinalysis, complete blood count, erythrocyte sedimentation rate (ESR), serum electrolytes, blood urea nitrogen (BUN), creatinine, blood glucose, serum lipid profile, prothrombin time (PT), and partial thromboplastin time (PTT) are often useful and should be considered in all patients.
- An ECG, and subsequent cardiac telemetry, may demonstrate arrhythmias or reveal evidence of recent myocardial infarction (MI).
- Of all these studies, only brain imaging and finger stick blood glucose are necessary prior to IV thrombolysis; the results of other studies should not delay the rapid administration of IV thrombolysis if the patient is eligible.
- Embolic strokes tend to occur suddenly with maximum neurologic deficit present at onset.
- With reperfusion following more prolonged ischemia, petechial hemorrhages can occur within the ischemic territory.
- These are usually of no clinical significance and should be distinguished from frank intracranial hemorrhage into a region of ischemic stroke where the mass effect from the hemorrhage can cause a significant decline in neurologic function.
- Emboli large enough to occlude the stem of the MCA (3–4 mm) or internal carotid terminus lead to large infarcts that involve both deep gray and white matter and some portions of the cortical surface.
- A smaller embolus may occlude a small cortical or penetrating arterial branch.
- The location and size of an infarct within a vascular territory depend on the extent of the collateral circulation.
- Special vigilance is warranted for patients with cerebellar infarction.
- These strokes may mimic labyrinthitis because of prominent vertigo and vomiting; the presence of head or neck pain should alert the physician to consider cerebellar stroke due to vertebral artery dissection.
- Even small amounts of cerebellar edema can acutely increase intracranial pressure (ICP) by obstructing cerebrospinal fluid (CSF) flow leading to hydrocephalus or by directly compressing the brainstem.
- The resulting brainstem compression can manifest as coma and respiratory arrest and require emergency surgical decompression.
- Suboccipital decompression is recommended in patients with cerebellar infarcts who demonstrate neurologic deterioration and should be performed before significant brainstem compression occurs.
4.1 Cardioembolic Stroke¶
- Cardioembolism is responsible for ~20% of all ischemic strokes.
- Stroke caused by heart disease is primarily due to embolism of thrombotic material forming on the atrial or ventricular wall or the left heart valves.
- These thrombi then detach and embolize into the arterial circulation.
- The thrombus may fragment or lyse quickly, producing only a TIA.
- Alternatively, the arterial occlusion may last longer, producing stroke.
- Emboli from the heart most often lodge in the intracranial internal carotid artery, the MCA, the posterior cerebral artery (PCA), or one of their branches; infrequently, the anterior cerebral artery (ACA) is involved.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- MI, prosthetic valves, rheumatic heart disease, and ischemic cardiomyopathy are other considerations.
- Cardiac disorders causing brain embolism are discussed in the chapters on heart diseases, but a few pertinent aspects are highlighted here.
- Left atrial enlargement is an additional risk factor for formation of atrial thrombi.
- Paradoxical embolization occurs when venous thrombi migrate to the arterial circulation, usually via a patent foramen ovale (PFO) or atrial septal defect.
- Bubble-contrast echocardiography (IV injection of agitated saline coupled with either transthoracic or transesophageal echocardiography) can demonstrate a right-to-left cardiac shunt, revealing the conduit for paradoxical embolization.
- Alternatively, a right-to-left shunt is implied if immediately following IV injection of agitated saline, the ultrasound signature of bubbles is observed during transcranial Doppler insonation of the MCA; pulmonary arteriovenous malformations should be considered if this test is positive yet an echocardiogram fails to reveal an intracardiac shunt.
- Both techniques are highly sensitive for detection of right-to-left shunts.
- Besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
4.2 Carotid Atherosclerosis¶
- Atherosclerosis within the carotid artery occurs most frequently within the common carotid bifurcation and proximal internal carotid artery; the carotid siphon (portion within the cavernous sinus) is also vulnerable to atherosclerosis.
- Male gender, older age, smoking, hypertension, diabetes, and hypercholesterolemia are risk factors for carotid disease, as they are for stroke in general.
- Carotid atherosclerosis produces an estimated 10% of ischemic stroke.
- Carotid disease can be classified by whether the stenosis is symptomatic or asymptomatic and by the degree of stenosis (percent narrowing of the narrowest segment compared to a nondiseased segment).
- Symptomatic carotid disease implies that the patient has experienced a stroke or TIA.
- High-grade stenosis of the internal carotid artery, which may be associated with either cerebral emboli or flow-limiting ischemia, was identified in this patient.
5. DIFFERENTIAL DIAGNOSIS¶
- Perform an emergency noncontrast head CT scan to differentiate between ischemic stroke and hemorrhagic stroke.
- There are no reliable clinical findings that conclusively separate ischemia from hemorrhage, although a more depressed level of consciousness, higher initial blood pressure, or worsening of symptoms 1 hour after onset favor hemorrhage, and a deficit that is maximal at onset, or remits, suggests ischemia.
- Cerebellar infarction may mimic labyrinthitis because of prominent vertigo and vomiting.
- Meningitis (syphilis, tuberculosis, fungal, bacterial, zoster) may present with stroke-like symptoms.
- Subarachnoid hemorrhage vasospasm may mimic ischemic stroke.
- Moyamoya disease may present with ischemic symptoms.
- Eclampsia may present with stroke-like symptoms in pregnancy.
6. INVESTIGATIONS & DIAGNOSIS¶
- Perform an emergency noncontrast head CT scan to differentiate between ischemic stroke and hemorrhagic stroke.
- An imaging study of the brain is always indicated and is required for patients being considered for thrombolysis; it may be combined with CT- or MRI-based angiography to visualize the vasculature of the neck and intracranial vessels.
- Advanced neuroimaging techniques may help to select patients beyond the 4.5-h window who will benefit from thrombolysis.
- Two trials using MRI selection beyond 4.5 h have shown clinical benefit from IV rtPA.
- CT perfusion imaging increases the sensitivity for detecting ischemia and can measure the ischemic penumbra.
- MR perfusion can be combined with MR diffusion imaging to identify the ischemic penumbra as the mismatch between these two imaging sequences.
- The ischemic penumbra will eventually progress to infarction if no change in flow occurs, and hence, saving the ischemic penumbra is the goal of revascularization therapy.
- Restoration of blood flow provides oxygen and glucose to the penumbral tissue, preventing infarction not only by supplying fuel for metabolism but by reversing tissue acidosis, clearing glutamate and toxic oxygen species, and halting waves of cortical spreading depression emanating from the ischemic core that add metabolic stress to the tissue.
- A chest x-ray, electrocardiogram (ECG), urinalysis, complete blood count, erythrocyte sedimentation rate (ESR), serum electrolytes, blood urea nitrogen (BUN), creatinine, blood glucose, serum lipid profile, prothrombin time (PT), and partial thromboplastin time (PTT) are often useful and should be considered in all patients.
- An ECG, and subsequent cardiac telemetry, may demonstrate arrhythmias or reveal evidence of recent myocardial infarction (MI).
- Of all these studies, only brain imaging and finger stick blood glucose are necessary prior to IV thrombolysis; the results of other studies should not delay the rapid administration of IV thrombolysis if the patient is eligible.
Table 2 — TABLE 438-1 Administration of Intravenous Recombinant Tissue Plasminogen Activator (rtPA) or Tenecteplase for Acute Ischemic Stroke (AIS)¶
| INDICATION | CONTRAINDICATION |
|---|---|
| Clinical diagnosis of stroke | Sustained BP >185/110 mmHg despite treatment |
| Onset of symptoms to time of drug administration ≤4.5 h | Bleeding diathesis |
| CT scan showing no hemorrhage, and no edema > 1/3 of the MCA territory | Recent head injury or intracerebral hemorrhage |
| Age ≥18 years | Major surgery in preceding 14 days |
| Administration of stroke thrombolysis | Gastrointestinal bleeding in preceding 21 days |
| IV access with two peripheral IV lines (avoid arterial or central line placement) | Recent myocardial infarction |
| Review eligibility for stroke thrombolysis | Administration of stroke thrombolysis |
| Administer 0.9 mg/kg IV (maximum 90 mg) rtPA IV as 10% of total dose by bolus, followed by remainder of total dose over 1 h | No other antithrombotic treatment for 24 h |
| Or Administer 0.25 mg/kg IV (maximum 25 mg) tenecteplase IV push over 5 s | For decline in neurologic status or uncontrolled BP, stop infusion, give cryoprecipitate, and reimage brain emergently |
| Frequent cuff BP monitoring | Avoid urethral catheterization for ≥2 h |
6.1 Diagnostic Criteria for Thrombolysis¶
- Clinical diagnosis of stroke.
- Onset of symptoms to time of drug administration ≤4.5 h.
- CT scan showing no hemorrhage, and no edema > 1/3 of the MCA territory.
- Age ≥18 years.
- Sustained BP >185/110 mmHg despite treatment is a contraindication.
- Bleeding diathesis is a contraindication.
- Recent head injury or intracerebral hemorrhage is a contraindication.
- Major surgery in preceding 14 days is a contraindication.
- Gastrointestinal bleeding in preceding 21 days is a contraindication.
- Recent myocardial infarction is a contraindication.
6.2 Imaging Findings¶
- Noncontrast head CT scan: Differentiates ischemic stroke from hemorrhagic stroke.
- CTA: Confirms large-vessel occlusion (ICA, MCA, basilar).
- CTP: Identifies ischemic penumbra (mismatch).
- MRI DWI: Shows residual brain infarction.
- Hyperdensity in the left MCA on CT is highly specific for MCA occlusion but is poorly sensitive, as only 20% of patients with MCA occlusion show hyperdensity.
7. MANAGEMENT & TREATMENT¶
- After the clinical diagnosis of stroke is made, an orderly and prompt process of evaluation and treatment should follow.
- The first goal is to prevent or reverse brain injury.
- Attend to the patient's airway, breathing, and circulation (ABCs), and treat hypoglycemia or hyperglycemia if identified by finger stick testing.
- Perform an emergency noncontrast head CT scan to differentiate between ischemic stroke and hemorrhagic stroke.
- There are no reliable clinical findings that conclusively separate ischemia from hemorrhage, although a more depressed level of consciousness, higher initial blood pressure, or worsening of symptoms 1 hour after onset favor hemorrhage, and a deficit that is maximal at onset, or remits, suggests ischemia.
- Treatments designed to reverse or lessen the amount of tissue infarction and improve clinical outcome fall within six categories: (1) medical support, (2) IV thrombolysis, and (3) endovascular revascularization, (4) antithrombotic treatment, (5) neuroprotection, and (6) stroke centers and rehabilitation.
- Between 5 and 10% of patients develop enough cerebral edema to cause obtundation and brain herniation.
- Edema peaks on the second or third day but can cause mass effect for ~10 days.
- The larger the infarct, the greater the likelihood that clinically significant edema will develop.
- Water restriction and IV mannitol or hypertonic saline may be used to raise the serum osmolarity, but hypovolemia should be avoided because this may contribute to hypotension and worsening infarction.
- Combined analysis of three randomized European trials of hemicraniectomy (craniotomy and temporary removal of part of the skull) shows that hemicraniectomy reduces mortality by 50%, and the clinical outcomes of survivors are significantly improved.
- Older patients (age >60 years) benefit less but still significantly.
- The size of the diffusion-weighted imaging volume of brain infarction during the acute stroke is a predictor of future deterioration requiring hemicraniectomy.
- Special vigilance is warranted for patients with cerebellar infarction.
- These strokes may mimic labyrinthitis because of prominent vertigo and vomiting; the presence of head or neck pain should alert the physician to consider cerebellar stroke due to vertebral artery dissection.
- Even small amounts of cerebellar edema can acutely increase intracranial pressure (ICP) by obstructing cerebrospinal fluid (CSF) flow leading to hydrocephalus or by directly compressing the brainstem.
- The resulting brainstem compression can manifest as coma and respiratory arrest and require emergency surgical decompression.
- Suboccipital decompression is recommended in patients with cerebellar infarcts who demonstrate neurologic deterioration and should be performed before significant brainstem compression occurs.
- For decline in neurologic status or uncontrolled BP, stop infusion, give cryoprecipitate, and reimage brain emergently.
- Avoid urethral catheterization for ≥2 h.
Table 3 — TABLE 438-3 Recommendations on Chronic Use of Antithrombotics for Various Cardiac Conditions¶
| CONDITION | RECOMMENDATION |
|---|---|
| Nonvalvular atrial fibrillation | Calculate CHADS-VASc score |
| • CHA2DS2-VASc score of 0 | Aspirin or no antithrombotic |
| • CHADS-VASc score of 1 | Aspirin or OAC |
| • CHADS-VASc score of ≥2 | OAC |
| Rheumatic mitral valve disease | • With atrial fibrillation, previous OAC or left atrial diameter >55 mm: OAC |
| • Embolization or appendage clot despite OAC plus aspirin | OAC generally precludes use of anticoagulation or thrombolytics. |
| • Mitral valve prolapse | Asymptomatic: No therapy |
| • With otherwise cryptogenic stroke or TIA | Aspirin |
| • Atrial fibrillation | OAC |
| • Asymptomatic | No therapy |
| • With atrial fibrillation | OAC |
| • Otherwise cryptogenic stroke or TIA | Aspirin or OAC |
| • Recurrent embolization despite aspirin | OAC |
| • With atrial fibrillation | OAC |
| • Aortic valve calcification | Asymptomatic: No therapy |
| • Otherwise cryptogenic stroke or TIA | Aspirin or OAC |
| • With atrial fibrillation | OAC |
| • Asymptomatic | No therapy |
| • Otherwise cryptogenic ischemic stroke or TIA | Aspirin or closure with device |
| • Carotid disease | Indication for OAC (deep-venous thrombosis or hypercoagulable state): OAC |
| • Mechanical heart valve | Aortic position, bileaflet or Medtronic Hall VKA INR 2.5, range 2–3 |
| • Atrial septal defect | Otherwise cryptogenic ischemic stroke or TIA: Aspirin or closure with device |
7.1 Medical Support¶
- Attend to the patient's airway, breathing, and circulation (ABCs).
- Treat hypoglycemia or hyperglycemia if identified by finger stick testing.
- Blood pressure should be reduced if it exceeds 220/120 mmHg, if there is malignant hypertension or concomitant myocardial ischemia, or if blood pressure is >185/110 mmHg and thrombolytic therapy is anticipated.
- When faced with the competing demands of myocardium and brain, lowering the heart rate with a β-adrenergic blocker (such as esmolol) can be a first step to decrease cardiac work and maintain blood pressure.
- Routine lowering of blood pressure below the limits listed above has the potential to worsen outcomes.
- Fever is detrimental and should be treated with antipyretics and surface cooling.
- Serum glucose should be monitored and kept <10.0 mmol/L (180 mg/dL), and above at least 3.3 mmol/L (60 mg/dL); a more intensive glucose control strategy does not improve outcome.
- Use of pneumatic compression stockings is of proven benefit in reducing risk of DVT and is a safe alternative to heparin.
7.2 Thrombolysis¶
- The National Institute of Neurological Disorders and Stroke (NINDS) Recombinant Tissue Plasminogen Activator (rtPA) Stroke Study showed a clear benefit for IV rtPA in selected patients with acute stroke.
- The NINDS study used IV rtPA (0.9 mg/kg to a 90-mg maximum; 10% as a bolus, then the remainder over 60 min) versus placebo in ischemic stroke within 3 h of onset.
- One-half of the patients were treated within 90 min.
- Symptomatic intracranial hemorrhage occurred in 6.4% of patients on rtPA and 0.6% on placebo.
- In the rtPA group, there was a significant 12% absolute increase in the number of patients with only minimal disability (32% on placebo and 44% on rtPA) and a nonsignificant 4% reduction in mortality (21% on placebo and 17% on rtPA).
- Thus, despite an increased incidence of symptomatic intracranial hemorrhage, treatment with IV rtPA within 3 h of the onset of ischemic stroke improved clinical outcome.
- Three subsequent trials of IV rtPA did not confirm this benefit, perhaps because of the dose of rtPA used, the timing of its delivery, and small sample size.
- When data from all randomized IV rtPA trials were combined, however, efficacy was confirmed in the 80 years and diabetic patients with a previous stroke were excluded.
- In this 821-patient randomized study, efficacy was again confirmed, although the treatment effect was less robust than in the 0- to 3-h time window.
- In the rtPA group, 52.4% of patients achieved a good outcome at 90 days, compared to 45.2% of the placebo group (odds ratio [OR] 1.34, p = .04).
- The symptomatic intracranial hemorrhage rate was 2.4% in the rtPA group and 0.2% in the placebo group (p = .008).
- Based on these data, rtPA is approved in the 3- to 4.5-h window in Europe and Canada but is only approved for 0–3 h in the United States.
- A dose of 0.6 mg/kg is typically used in Japan and other Asian countries based on observation of >600 patients given this lower dose and observing similar outcomes to historical controls and a lower rate of intracranial hemorrhage.
- This dose also mitigates concerns that patients of Asian descent have a higher propensity to bleed from most antithrombotic and thrombolytic medications.
- The plasminogen activator tenecteplase (0.25 mg/kg IV bolus over 5 s with a maximum dose of 25 mg) has been directly compared to rtPA and is being adopted by many centers because it is given without need for a 1-h infusion.
- This improves the efficiency of transferring patients to comprehensive stroke centers for thrombectomy because the IV infusion required for IV rtPA is not required for tenecteplase, thus obviating need for critical care transport.
- Several trials using tenecteplase prior to endovascular therapy have found it to be safe.
7.3 Endovascular Revascularization¶
- Ischemic stroke from large-vessel intracranial occlusion results in high rates of mortality and morbidity.
- Occlusions in such large vessels (middle cerebral artery [MCA], intracranial internal carotid artery, and the basilar artery) generally involve a large clot burden and often fail to open with IV thrombolysis alone.
- Endovascular mechanical thrombectomy has been studied as an alternative or adjunctive treatment of acute stroke in patients who are ineligible for, or have contraindications to, thrombolytics or in those who failed to achieve vascular recanalization with IV thrombolysis.
- In 2015, the results of six randomized trials were published, all demonstrating that endovascular therapy improved clinical outcomes for internal carotid and MCA occlusions proven by CT angiography (CTA), under 6 h from stroke onset, with or without pretreatment with IV tissue plasminogen activator (tPA).
- One study concluded that patients were home nearly 2 months earlier if they received endovascular therapy.
- A combined meta-analysis of all patients in these trials confirmed a large benefit with endovascular therapy (OR, 2.49; 95% confidence interval [CI], 1.76–3.53; p <.001).
- The percentage of patients who achieved modified Rankin scores of 0–2 (normal or symptomatic but independent) was 46% in the endovascular group and 26.5% in the medical arm.
- A more recent meta-analysis reveals a mortality benefit with thrombectomy as well.
- As with IV rtPA treatment, clinical outcome is dependent on time to effective therapy.
- The odds of a good outcome exceed 3 if groin puncture occurs within 2 h of symptom onset but is only 2 if 8 h elapse.
- Over 80% of patients who had vessel opening within 1 h of arrival to the emergency department had a good outcome, whereas only one-third had a good outcome if 6 h elapsed.
- The outcomes from endovascular therapy are likely improved with IV rtPA treatment prior to thrombectomy if the patient is eligible for rtPA and it is safe to administer.
- Recent data support replacing IV rtPA with IV tenecteplase because its simple bolus administration makes transporting the patient to an endovascular center less cumbersome.
- Extending the time window beyond 6 h appears to be effective if the patient has specific imaging findings demonstrating good vascular collaterals (CT perfusion or magnetic resonance [MR] perfusion techniques) and can be treated within 24 h.
- The Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN) trial reported good outcomes more frequently with endovascular therapy than with medical care alone (47 vs 13%, p <.0001).
- The Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3 (DEFUSE-3) trial confirmed these results (45 vs 17%, p <.001).
- Now that endovascular stroke therapy is proven to be effective, the creation of comprehensive stroke centers designed to rapidly identify and treat patients with large-vessel cerebral ischemia has been a major focus internationally.
- Creating regional systems of care whereby stroke patients are first evaluated at acute stroke ready hospitals or primary stroke centers (which can administer IV rtPA or tenecteplase) then transferred to thrombectomy-capable or comprehensive stroke centers if needed, or directly triaged to thrombectomy-capable or comprehensive centers based on field assessment, appears to be an effective strategy to improve outcomes.
7.4 Antithrombotic Treatment¶
- Aspirin is the only antiplatelet agent that has been proven to be effective for the acute treatment of ischemic stroke; there are several antiplatelet agents proven for the secondary prevention of stroke.
- Two large trials, the International Stroke Trial (IST) and the Chinese Acute Stroke Trial (CAST), found that the use of aspirin within 48 h of stroke onset reduced both stroke recurrence risk and mortality minimally.
- Among 19,435 patients in IST, those allocated to aspirin, 300 mg/d, had slightly fewer deaths within 14 days (9.0 vs 9.4%), significantly fewer recurrent ischemic strokes (2.8 vs 3.9%), no excess of hemorrhagic strokes (0.9 vs 0.8%), and a trend toward a reduction in death or dependence at 6 months (61.2 vs 63.5%).
- In CAST, 21,106 patients with ischemic stroke received 160 mg/d of aspirin or a placebo for up to 4 weeks.
- In the aspirin group, there were very small reductions in early mortality (3.3 vs 3.9%), recurrent ischemic strokes (1.6 vs 2.1%), and dependency at discharge or death (30.5 vs 31.6%).
- These trials demonstrate that the use of aspirin in the treatment of acute ischemic stroke is safe and produces a small net benefit.
- For every 1000 acute strokes treated with aspirin, ~9 deaths or nonfatal stroke recurrences will be prevented in the first few weeks, and ~13 fewer patients will be dead or dependent at 6 months.
- The short-term combination of aspirin with clopidogrel or with ticagrelor following minor stroke or TIA is effective at preventing early second stroke.
- Numerous clinical trials have failed to demonstrate any benefit of routine anticoagulation in the primary treatment of atherothrombotic cerebral ischemia and have also shown an increase in the risk of brain and systemic hemorrhage.
- Therefore, the routine use of heparin or other anticoagulants for patients with atherothrombotic stroke is not warranted.
- Heparin and oral anticoagulation are likely no more effective than aspirin for stroke.
- There may be benefit of anticoagulation for halting progression of dural sinus thrombosis.
- Platelet Inhibition: Aspirin is the only antiplatelet agent that has been proven to be effective for the acute treatment of ischemic stroke.
- Dual antiplatelet agents aspirin (81 mg) and either clopidogrel (600 mg-load, followed by 75 mg daily) or ticagrelor (180-mg load, followed by 90 mg twice daily) daily for 21–30 days then continue aspirin at 81 mg daily.
- Ticagrelor has the advantage of not being affected by common polymorphisms of CYP2C19 that limit efficacy of clopidogrel in significant proportions of patients, particularly those of Asian descent.
- If the CTA revealed significant intracranial atherosclerosis or other precranial vessel stenosis within the vascular territory of the infarct (lumen caliber reduced by >50%), we continue dual antiplatelet agents for at least 3 months and then convert to a single agent.
- Unless contraindicated, all patients receive a high-intensity statin such as atorvastatin 80 mg or rosuvastatin 40 mg, with goal low-density lipoprotein level of <70 mg/dL unless the stroke has a nonatherothrombotic cause.
- Patients who are statin intolerant can receive PCSK9 inhibitors.
- Blood pressure control should target systolic blood pressure <120 mmHg long term, but we allow permissive hypertension for the first few days or weeks to help with collateral flow to the brain.
7.5 Neuroprotection¶
- Neuroprotection is the concept of providing a treatment that prolongs the brain's tolerance to ischemia.
- Drugs that block the excitatory amino acid pathways have been shown to protect neurons and glia in animals, but despite multiple clinical trials, they have not yet been proven to be beneficial in humans.
- Hypothermia is a powerful neuroprotective treatment in patients with cardiac arrest and is neuroprotective in animal models of stroke, but it has not been adequately studied in patients with ischemic stroke and is the subject of ongoing research.
- Hypothermia combined with hemicraniectomy is no more effective than hemicraniectomy with euthermia.
7.6 Stroke Centers and Rehabilitation¶
- Patient care in stroke units followed by rehabilitation services improves neurologic outcomes and reduces mortality.
- Use of clinical priorities of acute stroke consultation: Once stroke is suspected, the first priorities are to assess airway and blood pressure, followed by establishing the time last seen normal.
- Patients with disabling neurologic deficits (particularly with National Institutes of Health Stroke Scale >5) may be eligible for thrombolytic and/or endovascular therapy.
- Based on the onset time, we follow the protocol shown in the figure.
- Following acute treatments, if any, we proceed with establishing the cause of the ischemic stroke.
- If atrial fibrillation is established or newly discovered, we favor use of apixaban 5 mg twice daily (or a reduced dose of 2.5 mg twice daily for impaired glomerular filtration rate) lifelong.
- If atrial fibrillation is not detected during the hospital encounter, we obtain an ambulatory electrocardiogram monitor to surveil for intermittent atrial fibrillation while treating with antiplatelet agents, then convert to oral anticoagulation if intermittent atrial fibrillation is detected.
- If we identify significant internal carotid stenosis, we refer for carotid endarterectomy during the same hospitalization regardless of infarct size.
- For all else, we use the dual antiplatelet agents aspirin (81 mg) and either clopidogrel (600 mg-load, followed by 75 mg daily) or ticagrelor (180-mg load, followed by 90 mg twice daily) daily for 21–30 days then continue aspirin at 81 mg daily.
- Proper rehabilitation of the stroke patient includes early physical, occupational, and speech therapy.
- It is directed toward educating the patient and family about the patient's neurologic deficit, preventing the complications of immobility (e.g., pneumonia, DVT and pulmonary embolism, pressure sores of the skin, and muscle contractures), and providing encouragement and instruction in overcoming the deficit.
- Use of pneumatic compression stockings is of proven benefit in reducing risk of DVT and is a safe alternative to heparin.
- The goal of rehabilitation is to return the patient home and to maximize recovery by providing a safe, progressive regimen suited to the individual patient.
- Additionally, the use of constrained movement therapy (immobilizing the unaffected side) has been associated with arterial dissection.
- However, there may be benefit of constrained movement therapy to improve hemiparesis following stroke, even years after the stroke, suggesting that physical therapy can recruit unused neural pathways.
- Controversy exists regarding whether selective serotonin uptake inhibitors improve motor recovery, but they may be helpful in preventing poststroke depression.
- Newer robotic therapies and neuromodulation approaches using transcranial magnetic stimulation or transcranial direct current stimulation are under active investigation.
- The human nervous system is more adaptable than previously thought, and developing physical and pharmacologic strategies to enhance long-term neural recovery are associated with an increase in pneumonia rates that could adversely impact stroke outcomes.
8. PROGNOSIS & COMPLICATIONS¶
- Combined analysis of three randomized European trials of hemicraniectomy (craniotomy and temporary removal of part of the skull) shows that hemicraniectomy reduces mortality by 50%, and the clinical outcomes of survivors are significantly improved.
- Older patients (age >60 years) benefit less but still significantly.
- The size of the diffusion-weighted imaging volume of brain infarction during the acute stroke is a predictor of future deterioration requiring hemicraniectomy.
- Between 5 and 10% of patients develop enough cerebral edema to cause obtundation and brain herniation.
- Edema peaks on the second or third day but can cause mass effect for ~10 days.
- The larger the infarct, the greater the likelihood that clinically significant edema will develop.
- Water restriction and IV mannitol or hypertonic saline may be used to raise the serum osmolarity, but hypovolemia should be avoided because this may contribute to hypotension and worsening infarction.
- Special vigilance is warranted for patients with cerebellar infarction.
- These strokes may mimic labyrinthitis because of prominent vertigo and vomiting; the presence of head or neck pain should alert the physician to consider cerebellar stroke due to vertebral artery dissection.
- Even small amounts of cerebellar edema can acutely increase intracranial pressure (ICP) by obstructing cerebrospinal fluid (CSF) flow leading to hydrocephalus or by directly compressing the brainstem.
- The resulting brainstem compression can manifest as coma and respiratory arrest and require emergency surgical decompression.
- Suboccipital decompression is recommended in patients with cerebellar infarcts who demonstrate neurologic deterioration and should be performed before significant brainstem compression occurs.
- For decline in neurologic status or uncontrolled BP, stop infusion, give cryoprecipitate, and reimage brain emergently.
- Avoid urethral catheterization for ≥2 h.
- The percentage of patients who achieved modified Rankin scores of 0–2 (normal or symptomatic but independent) was 46% in the endovascular group and 26.5% in the medical arm.
- A more recent meta-analysis reveals a mortality benefit with thrombectomy as well.
- As with IV rtPA treatment, clinical outcome is dependent on time to effective therapy.
- The odds of a good outcome exceed 3 if groin puncture occurs within 2 h of symptom onset but is only 2 if 8 h elapse.
- Over 80% of patients who had vessel opening within 1 h of arrival to the emergency department had a good outcome, whereas only one-third had a good outcome if 6 h elapsed.
- The outcomes from endovascular therapy are likely improved with IV rtPA treatment prior to thrombectomy if the patient is eligible for rtPA and it is safe to administer.
- Recent data support replacing IV rtPA with IV tenecteplase because its simple bolus administration makes transporting the patient to an endovascular center less cumbersome.
- Extending the time window beyond 6 h appears to be effective if the patient has specific imaging findings demonstrating good vascular collaterals (CT perfusion or magnetic resonance [MR] perfusion techniques) and can be treated within 24 h.
- The Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN) trial reported good outcomes more frequently with endovascular therapy than with medical care alone (47 vs 13%, p <.0001).
- The Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3 (DEFUSE-3) trial confirmed these results (45 vs 17%, p <.001).
- Now that endovascular stroke therapy is proven to be effective, the creation of comprehensive stroke centers designed to rapidly identify and treat patients with large-vessel cerebral ischemia has been a major focus internationally.
- Creating regional systems of care whereby stroke patients are first evaluated at acute stroke ready hospitals or primary stroke centers (which can administer IV rtPA or tenecteplase) then transferred to thrombectomy-capable or comprehensive stroke centers if needed, or directly triaged to thrombectomy-capable or comprehensive centers based on field assessment, appears to be an effective strategy to improve outcomes.
- For every 1000 acute strokes treated with aspirin, ~9 deaths or nonfatal stroke recurrences will be prevented in the first few weeks, and ~13 fewer patients will be dead or dependent at 6 months.
- The short-term combination of aspirin with clopidogrel or with ticagrelor following minor stroke or TIA is effective at preventing early second stroke.
9. SPECIAL CONSIDERATIONS¶
- The value of induced mild hypothermia to improve stroke outcomes has not been clearly demonstrated and remains the subject of continuing clinical research.
- Hypothermia combined with hemicraniectomy is no more effective than hemicraniectomy with euthermia.
- Hypothermia is a powerful neuroprotective treatment in patients with cardiac arrest and is neuroprotective in animal models of stroke, but it has not been adequately studied in patients with ischemic stroke and is the subject of ongoing research.
- Hypothermia combined with hemicraniectomy is no more effective than hemicraniectomy with euthermia.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
- The presence of a venous source of embolus, besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- MI, prosthetic valves, rheumatic heart disease, and ischemic cardiomyopathy are other considerations.
- Cardiac disorders causing brain embolism are discussed in the chapters on heart diseases, but a few pertinent aspects are highlighted here.
- Left atrial enlargement is an additional risk factor for formation of atrial thrombi.
- Paradoxical embolization occurs when venous thrombi migrate to the arterial circulation, usually via a patent foramen ovale (PFO) or atrial septal defect.
- Bubble-contrast echocardiography (IV injection of agitated saline coupled with either transthoracic or transesophageal echocardiography) can demonstrate a right-to-left cardiac shunt, revealing the conduit for paradoxical embolization.
- Alternatively, a right-to-left shunt is implied if immediately following IV injection of agitated saline, the ultrasound signature of bubbles is observed during transcranial Doppler insonation of the MCA; pulmonary arteriovenous malformations should be considered if this test is positive yet an echocardiogram fails to reveal an intracardiac shunt.
- Both techniques are highly sensitive for detection of right-to-left shunts.
- Besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
- The presence of a venous source of embolus, besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- MI, prosthetic valves, rheumatic heart disease, and ischemic cardiomyopathy are other considerations.
- Cardiac disorders causing brain embolism are discussed in the chapters on heart diseases, but a few pertinent aspects are highlighted here.
- Left atrial enlargement is an additional risk factor for formation of atrial thrombi.
- Paradoxical embolization occurs when venous thrombi migrate to the arterial circulation, usually via a patent foramen ovale (PFO) or atrial septal defect.
- Bubble-contrast echocardiography (IV injection of agitated saline coupled with either transthoracic or transesophageal echocardiography) can demonstrate a right-to-left cardiac shunt, revealing the conduit for paradoxical embolization.
- Alternatively, a right-to-left shunt is implied if immediately following IV injection of agitated saline, the ultrasound signature of bubbles is observed during transcranial Doppler insonation of the MCA; pulmonary arteriovenous malformations should be considered if this test is positive yet an echocardiogram fails to reveal an intracardiac shunt.
- Both techniques are highly sensitive for detection of right-to-left shunts.
- Besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
9.1 Pregnancy¶
- Eclampsia may present with stroke-like symptoms in pregnancy.
9.2 Pediatrics¶
- Sickle cell anemia is an uncommon cause of ischemic stroke in children.
9.3 Elderly¶
- Older patients (age >60 years) benefit less but still significantly from hemicraniectomy.
- Patients aged >80 years were excluded in ECASS III study.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
9.4 Renal/Hepatic Impairment¶
- Use of apixaban 5 mg twice daily (or a reduced dose of 2.5 mg twice daily for impaired glomerular filtration rate) lifelong if atrial fibrillation is established or newly discovered.
10. KEY PEARLS & CLINICAL TRAPS¶
- The ischemic penumbra is defined as the ischemic but reversibly dysfunctional tissue surrounding a core area of infarction.
- Saving the ischemic penumbra is the goal of revascularization therapy.
- Restoration of blood flow provides oxygen and glucose to the penumbral tissue, preventing infarction not only by supplying fuel for metabolism but by reversing tissue acidosis, clearing glutamate and toxic oxygen species, and halting waves of cortical spreading depression emanating from the ischemic core that add metabolic stress to the tissue.
- Blood pressure should be reduced if it exceeds 220/120 mmHg, if there is malignant hypertension or concomitant myocardial ischemia, or if blood pressure is >185/110 mmHg and thrombolytic therapy is anticipated.
- Routine lowering of blood pressure below the limits listed above has the potential to worsen outcomes.
- Fever is detrimental and should be treated with antipyretics and surface cooling.
- Serum glucose should be monitored and kept 11.1 mmol/L [200 mg/dL]) worsens brain injury during ischemia.
- It is reasonable to suppress fever and prevent hyperglycemia during and after brain ischemia.
- The value of induced mild hypothermia to improve stroke outcomes has not been clearly demonstrated and remains the subject of continuing clinical research.
- Hemicraniectomy reduces mortality by 50%, and the clinical outcomes of survivors are significantly improved.
- Older patients (age >60 years) benefit less but still significantly from hemicraniectomy.
- The size of the diffusion-weighted imaging volume of brain infarction during the acute stroke is a predictor of future deterioration requiring hemicraniectomy.
- Special vigilance is warranted for patients with cerebellar infarction.
- These strokes may mimic labyrinthitis because of prominent vertigo and vomiting; the presence of head or neck pain should alert the physician to consider cerebellar stroke due to vertebral artery dissection.
- Even small amounts of cerebellar edema can acutely increase intracranial pressure (ICP) by obstructing cerebrospinal fluid (CSF) flow leading to hydrocephalus or by directly compressing the brainstem.
- The resulting brainstem compression can manifest as coma and respiratory arrest and require emergency surgical decompression.
- Suboccipital decompression is recommended in patients with cerebellar infarcts who demonstrate neurologic deterioration and should be performed before significant brainstem compression occurs.
- For decline in neurologic status or uncontrolled BP, stop infusion, give cryoprecipitate, and reimage brain emergently.
- Avoid urethral catheterization for ≥2 h.
- Aspirin is the only antiplatelet agent that has been proven to be effective for the acute treatment of ischemic stroke.
- Dual antiplatelet agents aspirin (81 mg) and either clopidogrel (600 mg-load, followed by 75 mg daily) or ticagrelor (180-mg load, followed by 90 mg twice daily) daily for 21–30 days then continue aspirin at 81 mg daily.
- Ticagrelor has the advantage of not being affected by common polymorphisms of CYP2C19 that limit efficacy of clopidogrel in significant proportions of patients, particularly those of Asian descent.
- If the CTA revealed significant intracranial atherosclerosis or other precranial vessel stenosis within the vascular territory of the infarct (lumen caliber reduced by >50%), we continue dual antiplatelet agents for at least 3 months and then convert to a single agent.
- Unless contraindicated, all patients receive a high-intensity statin such as atorvastatin 80 mg or rosuvastatin 40 mg, with goal low-density lipoprotein level of <70 mg/dL unless the stroke has a nonatherothrombotic cause.
- Patients who are statin intolerant can receive PCSK9 inhibitors.
- Blood pressure control should target systolic blood pressure <120 mmHg long term, but we allow permissive hypertension for the first few days or weeks to help with collateral flow to the brain.
- The percentage of patients who achieved modified Rankin scores of 0–2 (normal or symptomatic but independent) was 46% in the endovascular group and 26.5% in the medical arm.
- A more recent meta-analysis reveals a mortality benefit with thrombectomy as well.
- As with IV rtPA treatment, clinical outcome is dependent on time to effective therapy.
- The odds of a good outcome exceed 3 if groin puncture occurs within 2 h of symptom onset but is only 2 if 8 h elapse.
- Over 80% of patients who had vessel opening within 1 h of arrival to the emergency department had a good outcome, whereas only one-third had a good outcome if 6 h elapsed.
- The outcomes from endovascular therapy are likely improved with IV rtPA treatment prior to thrombectomy if the patient is eligible for rtPA and it is safe to administer.
- Recent data support replacing IV rtPA with IV tenecteplase because its simple bolus administration makes transporting the patient to an endovascular center less cumbersome.
- Extending the time window beyond 6 h appears to be effective if the patient has specific imaging findings demonstrating good vascular collaterals (CT perfusion or magnetic resonance [MR] perfusion techniques) and can be treated within 24 h.
- The Clinical Mismatch in the Triage of Wake Up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN) trial reported good outcomes more frequently with endovascular therapy than with medical care alone (47 vs 13%, p <.0001).
- The Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3 (DEFUSE-3) trial confirmed these results (45 vs 17%, p <.001).
- Now that endovascular stroke therapy is proven to be effective, the creation of comprehensive stroke centers designed to rapidly identify and treat patients with large-vessel cerebral ischemia has been a major focus internationally.
- Creating regional systems of care whereby stroke patients are first evaluated at acute stroke ready hospitals or primary stroke centers (which can administer IV rtPA or tenecteplase) then transferred to thrombectomy-capable or comprehensive stroke centers if needed, or directly triaged to thrombectomy-capable or comprehensive centers based on field assessment, appears to be an effective strategy to improve outcomes.
- For every 1000 acute strokes treated with aspirin, ~9 deaths or nonfatal stroke recurrences will be prevented in the first few weeks, and ~13 fewer patients will be dead or dependent at 6 months.
- The short-term combination of aspirin with clopidogrel or with ticagrelor following minor stroke or TIA is effective at preventing early second stroke.
- Numerous clinical trials have failed to demonstrate any benefit of routine anticoagulation in the primary treatment of atherothrombotic cerebral ischemia and have also shown an increase in the risk of brain and systemic hemorrhage.
- Therefore, the routine use of heparin or other anticoagulants for patients with atherothrombotic stroke is not warranted.
- Heparin and oral anticoagulation are likely no more effective than aspirin for stroke.
- There may be benefit of anticoagulation for halting progression of dural sinus thrombosis.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- MI, prosthetic valves, rheumatic heart disease, and ischemic cardiomyopathy are other considerations.
- Cardiac disorders causing brain embolism are discussed in the chapters on heart diseases, but a few pertinent aspects are highlighted here.
- Left atrial enlargement is an additional risk factor for formation of atrial thrombi.
- Paradoxical embolization occurs when venous thrombi migrate to the arterial circulation, usually via a patent foramen ovale (PFO) or atrial septal defect.
- Bubble-contrast echocardiography (IV injection of agitated saline coupled with either transthoracic or transesophageal echocardiography) can demonstrate a right-to-left cardiac shunt, revealing the conduit for paradoxical embolization.
- Alternatively, a right-to-left shunt is implied if immediately following IV injection of agitated saline, the ultrasound signature of bubbles is observed during transcranial Doppler insonation of the MCA; pulmonary arteriovenous malformations should be considered if this test is positive yet an echocardiogram fails to reveal an intracardiac shunt.
- Both techniques are highly sensitive for detection of right-to-left shunts.
- Besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
- The presence of a venous source of embolus, besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- MI, prosthetic valves, rheumatic heart disease, and ischemic cardiomyopathy are other considerations.
- Cardiac disorders causing brain embolism are discussed in the chapters on heart diseases, but a few pertinent aspects are highlighted here.
- Left atrial enlargement is an additional risk factor for formation of atrial thrombi.
- Paradoxical embolization occurs when venous thrombi migrate to the arterial circulation, usually via a patent foramen ovale (PFO) or atrial septal defect.
- Bubble-contrast echocardiography (IV injection of agitated saline coupled with either transthoracic or transesophageal echocardiography) can demonstrate a right-to-left cardiac shunt, revealing the conduit for paradoxical embolization.
- Alternatively, a right-to-left shunt is implied if immediately following IV injection of agitated saline, the ultrasound signature of bubbles is observed during transcranial Doppler insonation of the MCA; pulmonary arteriovenous malformations should be considered if this test is positive yet an echocardiogram fails to reveal an intracardiac shunt.
- Both techniques are highly sensitive for detection of right-to-left shunts.
- Besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
- The presence of a venous source of embolus, besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The most significant cause of cardioembolic stroke in most of the world is nonrheumatic (often called nonvalvular) atrial fibrillation.
- MI, prosthetic valves, rheumatic heart disease, and ischemic cardiomyopathy are other considerations.
- Cardiac disorders causing brain embolism are discussed in the chapters on heart diseases, but a few pertinent aspects are highlighted here.
- Left atrial enlargement is an additional risk factor for formation of atrial thrombi.
- Paradoxical embolization occurs when venous thrombi migrate to the arterial circulation, usually via a patent foramen ovale (PFO) or atrial septal defect.
- Bubble-contrast echocardiography (IV injection of agitated saline coupled with either transthoracic or transesophageal echocardiography) can demonstrate a right-to-left cardiac shunt, revealing the conduit for paradoxical embolization.
- Alternatively, a right-to-left shunt is implied if immediately following IV injection of agitated saline, the ultrasound signature of bubbles is observed during transcranial Doppler insonation of the MCA; pulmonary arteriovenous malformations should be considered if this test is positive yet an echocardiogram fails to reveal an intracardiac shunt.
- Both techniques are highly sensitive for detection of right-to-left shunts.
- Besides venous clot, fat and tumor emboli, bacterial endocarditis, IV air, and amniotic fluid emboli at childbirth may occasionally be responsible for paradoxical embolization.
- The importance of a PFO as a cause of stroke is debated, particularly because they are present in ~15% of the general population.
Flowcharts & Algorithms¶
Reproduced from Harrison's 22nd Edition.
Flowchart 1¶

Caption: FIGURE 438-2 Management of acute stroke (pathway followed by the authors). For the destination hospital. This allows early “stroke code” activation to prepare for an time seen normal, we expedite a noncontrast head CT scan, and if free of hemorrhage is administered in the CT scanner. (For IV tissue PA [tPA], the bolus is given and infusion (CTA) from left atrium to skull vertex is performed to identify an eligible target lesion for is not considered, and the decision to perform thrombectomy is based on perfusion Priorities of Acute Stroke Consultation: Once stroke is suspected, the first priorities seen normal. Patients with disabling neurologic deficits (particularly with National therapy. Based on the onset time, we follow the protocol shown in the figure. Following stroke. If atrial fibrillation is established or newly discovered, we favor use of apixaban 5 filtration rate) lifelong. If atrial fibrillation is not detected during the hospital encounter,
Figures & Illustrations¶
Reproduced from Harrison's 22nd Edition.
Figure 1¶
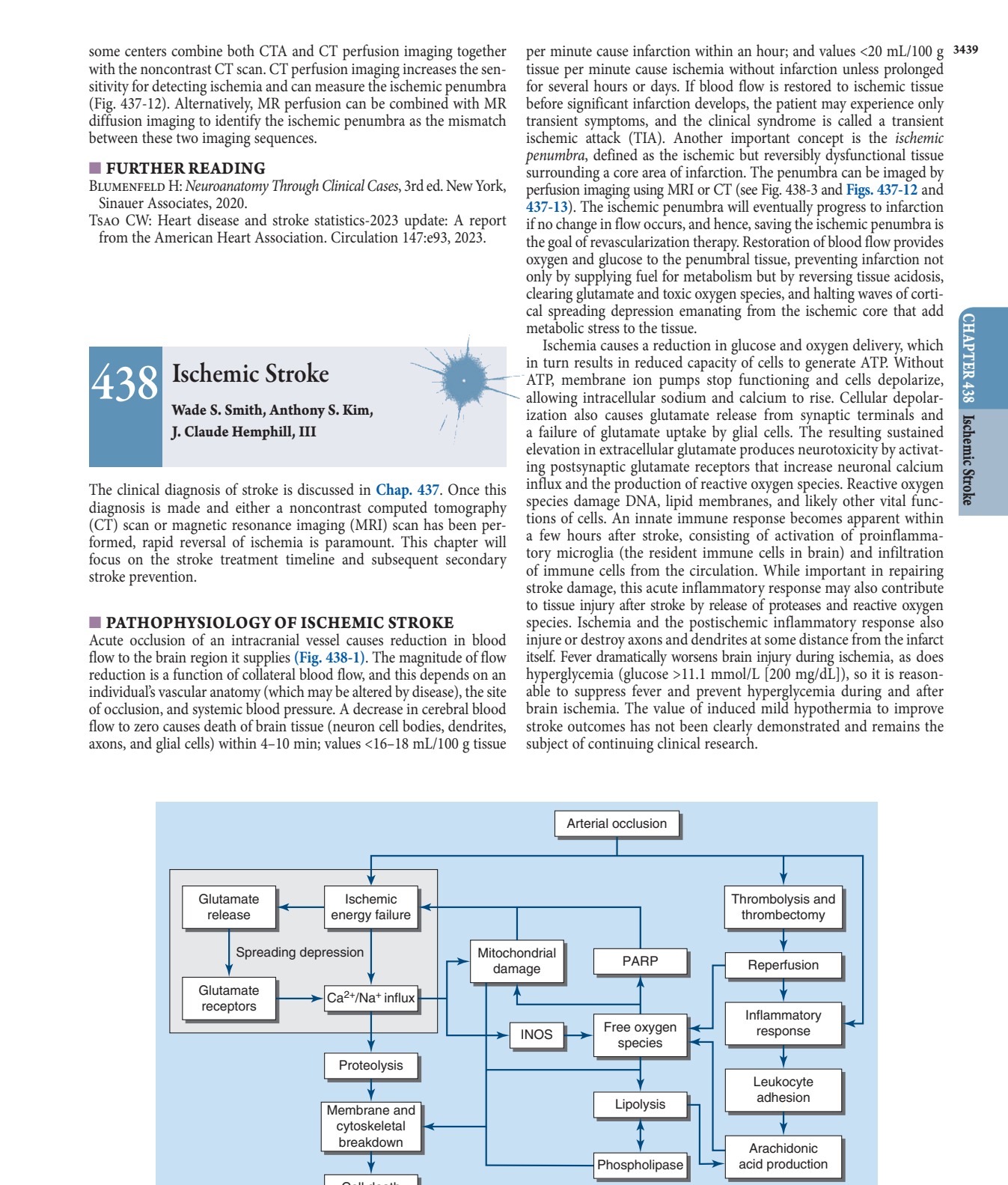
Caption: FIGURE 438-1 Major steps in the cascade of cerebral ischemia. See text for details. — Figure 438-1: Major steps in the cascade of cerebral ischemia, illustrating the progression from arterial occlusion to cell death via glutamate release, calcium influx, mitochondrial damage, and inflammatory response.
Figure 2¶
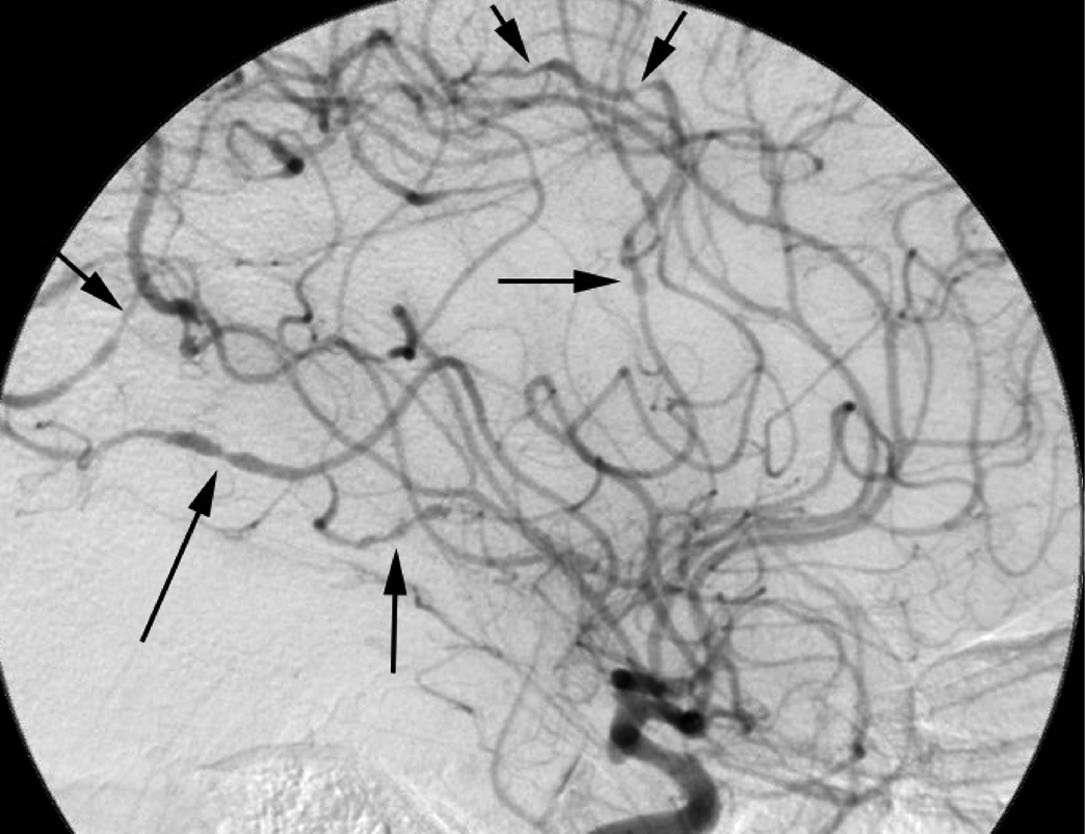
Caption: Ischemic Stroke 438 FIGURE 438-6 Cerebral angiogram from a 32-year-old male with central nervous system vasculopathy. Dramatic beading (arrows) typical of vasculopathy is shown. central nervous system vasculitis is rare; small or medium-sized ves- sels are usually affected, without apparent systemic vasculitis. The differential diagnosis includes other inflammatory vasculopathies including infection (tuberculous, fungal), sarcoidosis, angiocentric lymphoma, carcinomatous meningitis, and noninflammatory causes such as atherosclerosis, emboli, connective tissue disease, vasospasm, migraine-associated vasculopathy, and drug-associated causes. Some — Figure 438-2: Management of acute stroke pathway, showing the decision tree for prehospital call, CT scan, thrombolysis eligibility, CTA/CTP, and thrombectomy based on onset time and perfusion imaging.
Figure 3¶

Caption: FIGURE 438-3 (A) Noncontrast head computed tomography (CT) scan of a 78-year-old and awoke with right hemiparesis and expressive aphasia. The head CT shows no last seen normal time was 8 h prior. Head CT also shows hyperdensity in the left middle is poorly sensitive, as only 20% of patients with MCA occlusion show hyperdensity. (B) session reveals an occlusion of a secondary branch of the left MCA (arrow). (C) CT in the left image) but a large region (green shading in the right image) of ischemic tissue the occluded branch of the left MCA (arrow) and (E) restored flow after successful clot residual brain infarction. CBF, cerebral blood flow. onset, with or without pretreatment with IV tissue plasminogen — Figure 438-3 A: Noncontrast head CT scan of a patient with right hemiparesis and expressive aphasia showing no intracerebral hemorrhage but hyperdensity in the left MCA indicating occlusion.
Figure 4¶

Caption: FIGURE 438-4 Pathophysiology of ischemic stroke. A. Diagram illustrating the three major by an embolus (e.g., cardiogenic sources such as atrial fibrillation or artery-to-artery vessels; (2) in situ thrombosis of an intracranial vessel, typically affecting the small caused by flow-limiting stenosis of a major extracranial (e.g., internal carotid) or reformatted computed tomography angiogram of the common, internal, and external associated with either cerebral emboli or flow-limiting ischemia, was identified in this — Figure 438-3 B: CT angiography (CTA) confirming occlusion of a secondary branch of the left MCA, demonstrating the target lesion for thrombectomy.
Figure 5¶

Caption: FIGURE 438-4 Pathophysiology of ischemic stroke. A. Diagram illustrating the three major by an embolus (e.g., cardiogenic sources such as atrial fibrillation or artery-to-artery vessels; (2) in situ thrombosis of an intracranial vessel, typically affecting the small caused by flow-limiting stenosis of a major extracranial (e.g., internal carotid) or reformatted computed tomography angiogram of the common, internal, and external associated with either cerebral emboli or flow-limiting ischemia, was identified in this — Figure 438-3 C: CT perfusion imaging showing no core infarct but a large region of ischemic tissue (mismatch) that will die if revascularization is not achieved.
Figure 6¶
Caption: FIGURE 438-4 Pathophysiology of ischemic stroke. A. Diagram illustrating the three major by an embolus (e.g., cardiogenic sources such as atrial fibrillation or artery-to-artery vessels; (2) in situ thrombosis of an intracranial vessel, typically affecting the small caused by flow-limiting stenosis of a major extracranial (e.g., internal carotid) or reformatted computed tomography angiogram of the common, internal, and external associated with either cerebral emboli or flow-limiting ischemia, was identified in this — Figure 438-3 D: Catheter angiography showing the occluded branch of the left MCA prior to intervention.
Figure 7¶

Caption: FIGURE 438-5 Diagrams and reformatted computed tomography (CT) angiograms in the the deep penetrating arteries involved in small-vessel strokes. In the anterior circulation, a called lenticulostriates arise from the proximal portion of the anterior and middle cerebral subcortical structures (upper panels). In the posterior circulation, similar arteries arise and basilar arteries to supply the brainstem (lower panels). Occlusion of a single in a discrete area of infarct (pathologically termed a “lacune,” or lake). Note that these visualized on CT angiography. — Figure 438-3 E: Restoration of flow after successful clot removal during endovascular therapy.
Figure 8¶

Caption: FIGURE 438-5 Diagrams and reformatted computed tomography (CT) angiograms in the the deep penetrating arteries involved in small-vessel strokes. In the anterior circulation, a called lenticulostriates arise from the proximal portion of the anterior and middle cerebral subcortical structures (upper panels). In the posterior circulation, similar arteries arise and basilar arteries to supply the brainstem (lower panels). Occlusion of a single in a discrete area of infarct (pathologically termed a “lacune,” or lake). Note that these visualized on CT angiography. — Figure 438-3 F: Post-procedure imaging showing restored flow in the previously occluded vessel.
Figure 9¶
Caption: FIGURE 438-5 Diagrams and reformatted computed tomography (CT) angiograms in the the deep penetrating arteries involved in small-vessel strokes. In the anterior circulation, a called lenticulostriates arise from the proximal portion of the anterior and middle cerebral subcortical structures (upper panels). In the posterior circulation, similar arteries arise and basilar arteries to supply the brainstem (lower panels). Occlusion of a single in a discrete area of infarct (pathologically termed a “lacune,” or lake). Note that these visualized on CT angiography. — Figure 438-3 G: Subsequent diffusion-weighted imaging (DWI) scan showing a very small residual brain infarction following successful reperfusion.
Figure 10¶

Caption: FIGURE 438-5 Diagrams and reformatted computed tomography (CT) angiograms in the the deep penetrating arteries involved in small-vessel strokes. In the anterior circulation, a called lenticulostriates arise from the proximal portion of the anterior and middle cerebral subcortical structures (upper panels). In the posterior circulation, similar arteries arise and basilar arteries to supply the brainstem (lower panels). Occlusion of a single in a discrete area of infarct (pathologically termed a “lacune,” or lake). Note that these visualized on CT angiography. — Figure 438-4: Pathophysiology of ischemic stroke illustrating three major mechanisms: (1) embolus occlusion, (2) in situ thrombosis, and (3) hypoperfusion; plus reformatted CT angiogram of carotid arteries showing high-grade stenosis.
Generated from Harrison's Principles of Internal Medicine, 22nd Edition.